Poor Sensitivity of Fecal Gluten Immunogenic Peptides and Serum Antibodies to Detect Duodenal Mucosal Damage in Celiac Disease Monitoring

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Subjects and Methods
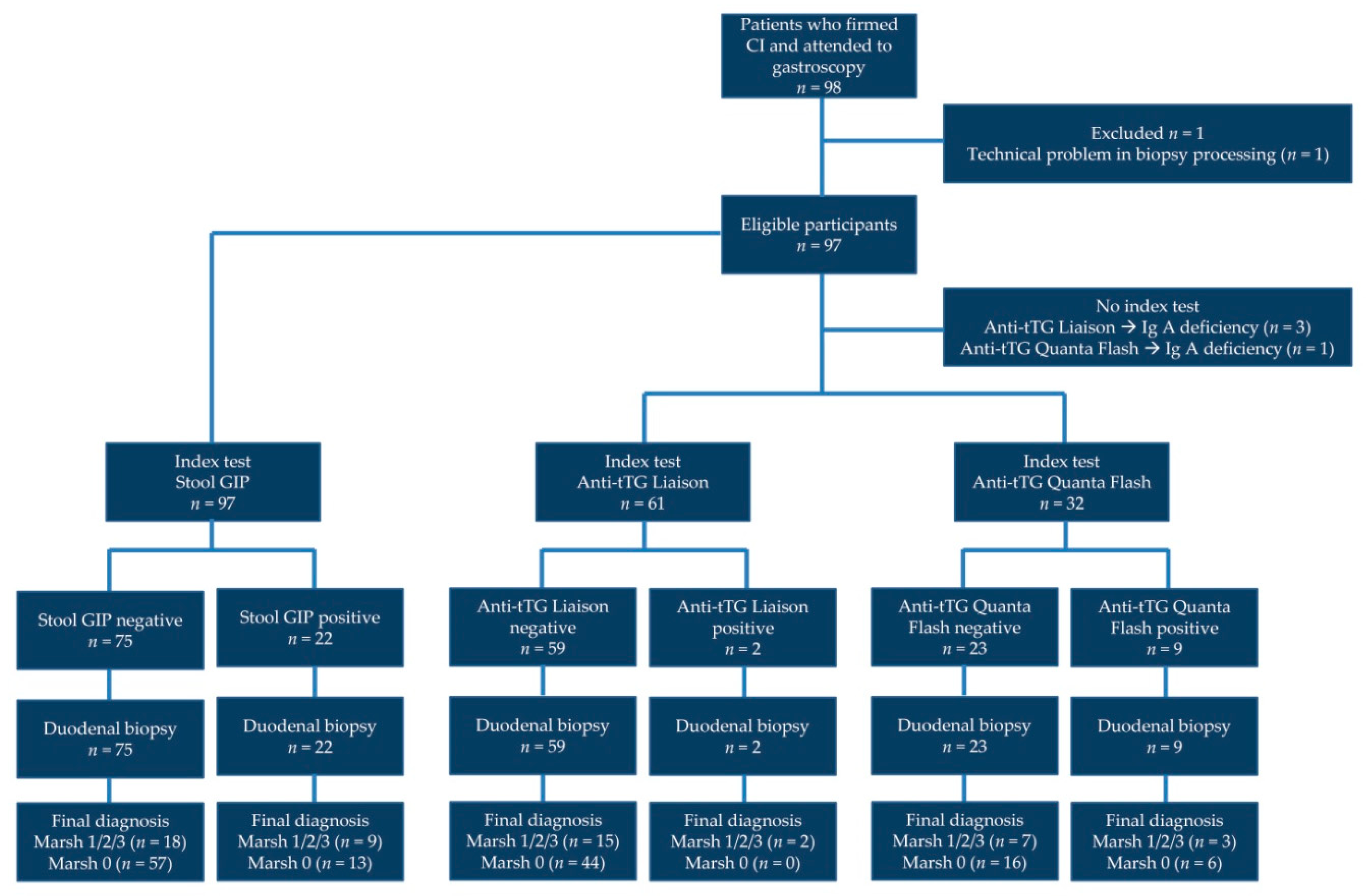
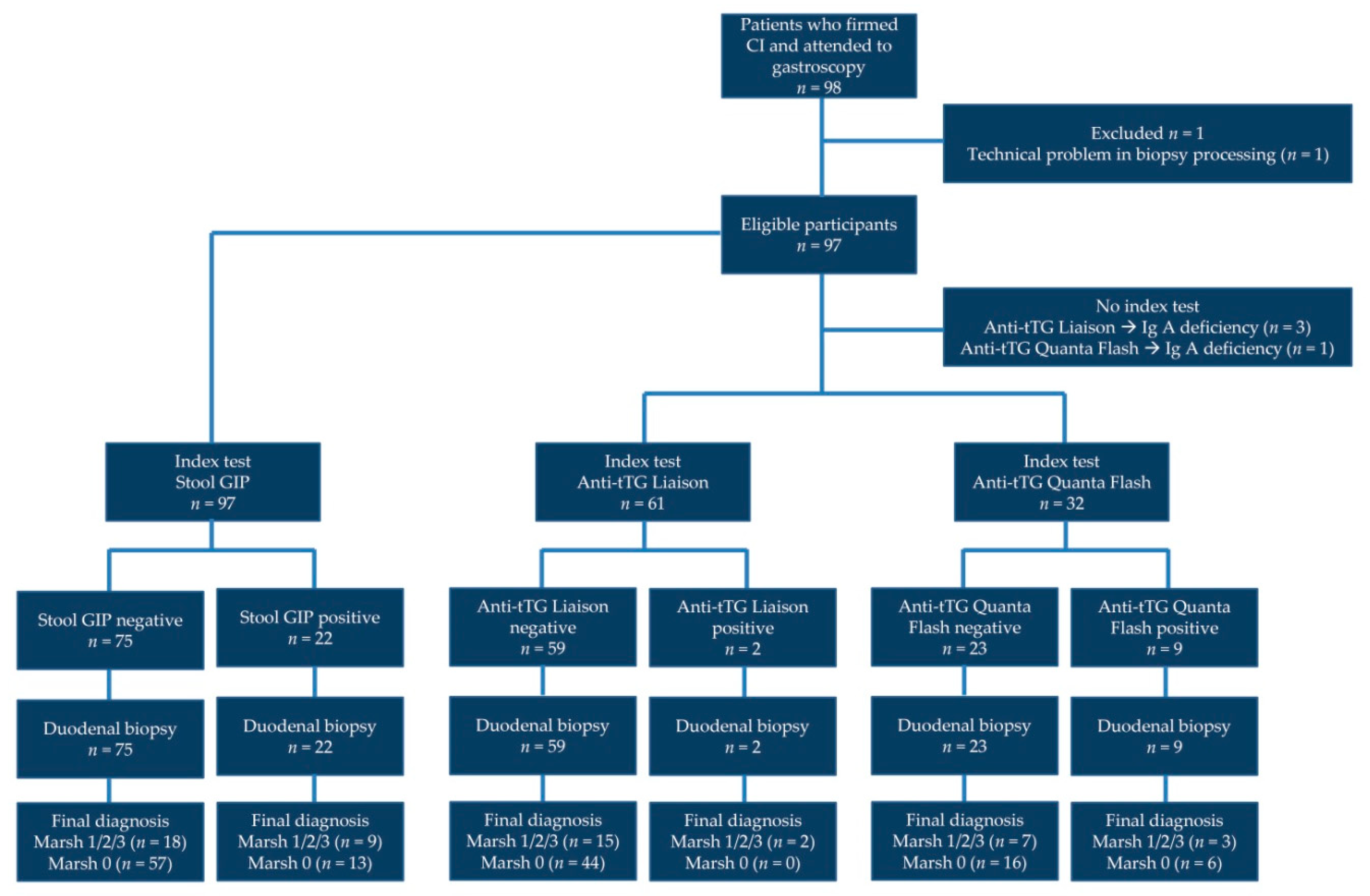
2.1. Study Design and Reporting
2.2. Study Population
2.3. Upper Endoscopy and Duodenal Biopsies
2.4. Measurement of GIPs
2.5. Measurement of Anti-tTG IgA
2.6. Gluten-Free-Diet Adherence and HRQoL Questionnaires
2.7. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics of Patients
3.2. Performance of GIP Detection in Stool Samples to Identify Mucosal Damage
3.3. Performance of Serum Anti-tTG IgA Antibodies to Detect Mucosal Damage
3.4. Association between Serum Antibodies and GIP Results
3.5. Patients’ Scores from Questionnaires and Relationship with Demographics, Mucosal Damage, and Laboratory Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac disease: A comprehensive current review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvester, J.A.; Graff, L.A.; Rigaux, L.; Walker, J.R.; Duerksen, D.R. Symptomatic suspected gluten exposure is common among patients with coeliac disease on a gluten-free diet. Aliment. Pharmacol. Ther. 2016, 44, 612–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanzini, A.; Lanzarotto, F.; Villanacci, V.; Mora, A.; Bertolazzi, S.; Turini, D.; Carella, G.; Malagoli, A.; Ferrante, G.; Cesana, B.M.; et al. Complete recovery of intestinal mucosa occurs very rarely in adult coeliac patients despite adherence to gluten-free diet. Aliment. Pharmacol. Ther. 2009, 29, 1299–1308. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, B.; Granath, F.; Ekbom, A.; Montgomery, S.M.; Murray, J.A.; Rubio-Tapia, A.; Green, P.H.R.; Ludvigsson, J.F. Mucosal healing and mortality in coeliac disease. Aliment. Pharmacol. Ther. 2013, 37, 332–339. [Google Scholar] [CrossRef] [Green Version]
- Galli, G.; Esposito, G.; Lahner, E.; Pilozzi, E.; Corleto, V.D.; Di Giulio, E.; Aloe Spiriti, M.A.; Annibale, B. Histological recovery and gluten-free diet adherence: A prospective 1-year follow-up study of adult patients with coeliac disease. Aliment. Pharmacol. Ther. 2014, 40, 639–647. [Google Scholar] [CrossRef] [Green Version]
- Lebwohl, B.; Michaëlsson, K.; Green, P.H.R.; Ludvigsson, J.F. Persistent mucosal damage and risk of fracture in celiac disease. J. Clin. Endocrinol. Metab. 2014, 99, 609–616. [Google Scholar] [CrossRef] [Green Version]
- Lebwohl, B.; Granath, F.; Ekbom, A.; Smedby, K.E.; Murray, J.A.; Neugut, A.I.; Green, P.H.R.; Ludvigsson, J.F. Mucosal healing and risk for lymphoproliferative malignancy in celiac disease: A population-based cohort study. Ann. Intern. Med. 2013, 159, 169–175. [Google Scholar] [CrossRef] [Green Version]
- Nachman, F.; del Campo, M.P.; González, A.; Corzo, L.; Vázquez, H.; Sfoggia, C.; Smecuol, E.; Pinto Sanchez, M.I.; Niveloni, S.; Sugai, E. Long-Term deterioration of quality of life in adult patients with celiac disease is associated with treatment noncompliance. Dig. Liver Dis. 2010, 42, 685–691. [Google Scholar] [CrossRef]
- Rubio-Tapia, A.; Hill, I.D.; Kelly, C.P.; Calderwood, A.H.; Murray, J.A. ACG clinical guidelines: Diagnosis and management of celiac disease. Am. J. Gastroenterol. 2013, 108, 656–676. [Google Scholar] [CrossRef] [Green Version]
- Pietzak, M.M. Follow-Up of patients with celiac disease: Achieving compliance with treatment. Gastroenterology 2005, 128, S135–S141. [Google Scholar] [CrossRef] [Green Version]
- Rubio-Tapia, A.; Rahim, M.W.; See, J.A.; Lahr, B.D.; Wu, T.-T.; Murray, J.A. Mucosal recovery and mortality in adults with celiac disease after treatment with a gluten-free diet. Am. J. Gastroenterol. 2010, 105, 1412–1420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaukinen, K.; Peräaho, M.; Lindfors, K.; Partanen, J.; Woolley, N.; Pikkarainen, P.; Karvonen, A.-L.; Laasanen, T.; Sievanen, H.; Maki, M.; et al. Persistent small bowel mucosal villous atrophy without symptoms in coeliac disease. Aliment. Pharmacol. Ther. 2007, 25, 1237–1245. [Google Scholar] [CrossRef]
- Sharkey, L.M.; Corbett, G.; Currie, E.; Lee, J.; Sweeney, N.; Woodward, J.M. Optimising delivery of care in coeliac disease—Comparison of the benefits of repeat biopsy and serological follow-up. Aliment. Pharmacol. Ther. 2013, 38, 1278–1291. [Google Scholar] [CrossRef]
- Silvester, J.A.; Kurada, S.; Szwajcer, A.; Kelly, C.P.; Leffler, D.A.; Duerksen, D.R. Tests for Serum Transglutaminase and Endomysial Antibodies Do Not Detect Most Patients with Celiac Disease and Persistent Villous Atrophy on Gluten-free Diets: A Meta-Analysis. Gastroenterology 2017, 153, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Morón, B.; Cebolla, A.; Manyani, H.; Alvarez-Maqueda, M.; Megías, M.; Thomas, M.D.C.; Carlos Lopez, M.; Sousa, C. Sensitive detection of cereal fractions that are toxic to celiac disease patients by using monoclonal antibodies to a main immunogenic wheat peptide. Am. J. Clin. Nutr. 2008, 87, 405–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comino, I.; Real, A.; Vivas, S.; Síglez, M.Á.; Caminero, A.; Nistal, E.; Casqueiro, J.; Rodriguez-Herrera, A.; Cebolla, A.; Sousa, C. Monitoring of gluten-free diet compliance in celiac patients by assessment of gliadin 33-mer equivalent epitopes in feces. Am. J. Clin. Nutr. 2012, 95, 670–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Loudres Moreno, M.; Cebolla, Á.; Muñoz-Suano, A.; Carrillo-Carrion, C.; Comino, I.; Pizarro, Á.; Leon, F.; Rodriguez-Herrera, A.; Sousa, C. Detection of gluten immunogenic peptides in the urine of patients with coeliac disease reveals transgressions in the gluten-free diet and incomplete mucosal healing. Gut 2017, 66, 250–257. [Google Scholar] [CrossRef] [Green Version]
- Syage, J.A.; Kelly, C.P.; Dickason, M.A.; Ramirez, A.C.; Leon, F.; Dominguez, R.; Sealey-Voyksner, J.A. Determination of gluten consumption in celiac disease patients on a gluten-free diet. Am. J. Clin. Nutr. 2018, 107, 201–207. [Google Scholar] [CrossRef]
- Silvester, J.A.; Comino, I.; Kelly, C.P.; Sousa, C.; Duerksen, D.R. DOGGIE BAG Study Group. Most Patients with Celiac Disease on Gluten-Free Diets Consume Measurable Amounts of Gluten. Gastroenterology 2020, 158, 1497–1499. [Google Scholar] [CrossRef]
- Stefanolo, J.P.; Tálamo, M.; Dodds, S.; de la Paz Temprano, M.; Costa, A.F.; Moreno, M.L.; Pinto-Sanchez, M.I.; Smecuol, E.; Vasquez, H.; Gonzales, A.; et al. Real-World Gluten Exposure in Patients with Celiac Disease on Gluten-Free Diets, Determined from Gliadin Immunogenic Peptides in Urine and Fecal Samples. Clin. Gastroenterol. Hepatol. 2021. [Google Scholar] [CrossRef]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; de Vet, H.C.W.; et al. STARD 2015: An Updated List of Essential Items for Reporting Diagnostic Accuracy Studies. Clin. Chem. 2015, 61, 1446–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludvigsson, J.F.; Bai, J.C.; Biagi, F.; Card, T.R.; Ciacci, C.; Ciclitira, P.J.; Green, P.H.R.; Hadjivassiliou, M.; Holdoway, A.; van Heel, D.A.; et al. Diagnosis and management of adult coeliac disease: Guidelines from the British Society of Gastroenterology. Gut 2014, 63, 1210–1228. [Google Scholar] [CrossRef] [PubMed]
- Marsh, M.N. Gluten, major histocompatibility complex, and the small intestine. A molecular and immunobiologic approach to the spectrum of gluten sensitivity (‘celiac sprue’). Gastroenterology 1992, 102, 330–354. [Google Scholar] [CrossRef]
- Oberhuber, G.; Granditsch, G.; Vogelsang, H. The histopathology of coeliac disease: Time for a standardized report scheme for pathologists. Eur. J. Gastroenterol. Hepatol. 1999, 11, 1185–1194. [Google Scholar] [CrossRef]
- Casellas, F.; Rodrigo, L.; Molina-Infante, J.; Vivas, S.; Lucendo, A.J.; Rosinach, M.; Duenas, C.; Fernandez-Banares, F.; Lopez-Vivancos, J. Transcultural adaptation and validation of the Celiac Disease Quality of Life (CD-QOL) Survey, a specific questionnaire to measure quality of life in patients with celiac disease. Revista Espanola de Enfermedades Digestivas 2013, 105, 585–593. [Google Scholar] [CrossRef] [Green Version]
- Fueyo-Díaz, R.; Gascón-Santos, S.; Asensio-Martínez, Á.; Sánchez-Calavera, M.A.; Magallón-Botaya, R. Transcultural adaptation and validation of the Celiac Dietary Adherence Test. A simple questionnaire to measure adherence to a gluten-free diet. Revista Espanola de Enfermedades Digestivas 2016, 108, 138–144. [Google Scholar] [CrossRef] [Green Version]
- Pinto-Sanchez, M.I.; Bai, J.C. Toward New Paradigms in the Follow Up of Adult Patients with Celiac Disease on a Gluten-Free Diet. Front. Nutr. 2019, 6, 153. [Google Scholar] [CrossRef]
- Bai, J.C.; Fried, M.; Corazza, G.R.; Schuppan, D.; Farthing, M.; Catassi, C.; Greco, L.; Cohen, H.; Ciacci, C.; Eliakim, R.; et al. World Gastroenterology Organisation global guidelines on celiac disease. J. Clin. Gastroenterol. 2013, 47, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Mooney, P.D.; Evans, K.E.; Singh, S.; Sanders, D.S. Treatment failure in coeliac disease: A practical guide to investigation and treatment of non-responsive and refractory coeliac disease. J. Gastrointest. Liver Dis. 2012, 21, 197–203. [Google Scholar]
- Szakács, Z.; Gede, N.; Gyöngyi, Z.; Solymár, M.; Csupor, D.; Erőss, B.; Vincze, A.; Miko, A.; Vasas, A.; Szapary, L.; et al. A Call for Research on the Prognostic Role of Follow-Up Histology in Celiac Disease: A Systematic Review. Front. Physiol. 2019, 10, 1408. [Google Scholar] [CrossRef]
- Fang, H.; King, K.S.; Larson, J.J.; Snyder, M.R.; Wu, T.T.; Gandhi, M.J.; Murray, J.A. Undetectable negative tissue transglutaminase IgA antibodies predict mucosal healing in treated coeliac disease patients. Aliment. Pharmacol. Ther. 2017, 46, 681–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuire, I.; Marja-Leena, L.; Teea, S.; Katri, H.; Jukka, P.; Päivi, S.; Heini, H.; Marrku, M.; Pekka, C.; Katri, K. Persistent duodenal intraepithelial lymphocytosis despite a long-term strict gluten-free diet in celiac disease. Am. J. Gastroenterol. 2012, 107, 1563–1569. [Google Scholar] [CrossRef] [PubMed]
- Hære, P.; Høie, O.; Schulz, T.; Schönhardt, I.; Raki, M.; Lundin, K.E.A. Long-Term mucosal recovery and healing in celiac disease is the rule—Not the exception. Scand. J. Gastroenterol. 2016, 51, 1439–1446. [Google Scholar] [CrossRef] [PubMed]
- Zanini, B.; Marullo, M.; Villanacci, V.; Salemme, M.; Lanzarotto, F.; Ricci, C.; Lanzini, A. Persistent Intraepithelial Lymphocytosis in Celiac Patients Adhering to Gluten-Free Diet Is Not Abolished Despite a Gluten Contamination Elimination Diet. Nutrients 2016, 8, 525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Meensel, B.; Hiele, M.; Hoffman, I.; Vermeire, S.; Rutgeerts, P.; Geboes, K.; Bossuyt, X. Diagnostic accuracy of ten second-generation (human) tissue transglutaminase antibody assays in celiac disease. Clin. Chem. 2004, 50, 2125–2135. [Google Scholar] [CrossRef] [PubMed]
- Sugai, E.; Nachman, F.; Váquez, H.; González, A.; Andrenacci, P.; Czech, A.; Niveloni, S.; Mazure, R.; Smecuol, E.; Cabanne, A.; et al. Dynamics of celiac disease-specific serology after initiation of a gluten-free diet and use in the assessment of compliance with treatment. Dig. Liver Dis. 2010, 42, 352–358. [Google Scholar] [CrossRef]
- Laserna-Mendieta, E.J.; Pineda-Tenor, D.; Timón-Zapata, J.; Carretero-Gómez, J.F.; Valle-Muñoz, J.; Gómez-Serranillos, M. A proposed reference change value for an IgA anti-tissue transglutaminase immunoassay to improve interpretation of serial results in celiac patients. Clin. Chim. Acta 2013, 421, 12–16. [Google Scholar] [CrossRef]
- Nachman, F.; Sugai, E.; Vázquez, H.; González, A.; Andrenacci, P.; Niveloni, S.; Mazure, R.; Smecuol, E.; Moreno, M.L.; Hwang, H.J.; et al. Serological tests for celiac disease as indicators of long-term compliance with the gluten-free diet. Eur. J. Gastroenterol. Hepatol. 2011, 23, 473–480. [Google Scholar] [CrossRef]
- Ruiz-Carnicer, Á.; Garzón-Benavides, M.; Fombuena, B.; Segura, V.; García-Fernández, F.; Sobrino-Rodríguez, S.; Gomez-Isquierdo, L.; Montes-Cano, M.A.; Rodriguez-Herrera, A.; Millan, R.; et al. Negative predictive value of the repeated absence of gluten immunogenic peptides in the urine of treated celiac patients in predicting mucosal healing: New proposals for follow-up in celiac disease. Am. J. Clin. Nutr. 2020, 112, 1240–1251. [Google Scholar] [CrossRef]
- Porcelli, B.; Ferretti, F.; Cinci, F.; Biviano, I.; Santini, A.; Grande, E.; Quagliarella, F.; Terzuoli, L.; Bacarelli, M.R.; Bizzaro, N.; et al. Fecal gluten immunogenic peptides as indicators of dietary compliance in celiac patients. Minerva Gastroenterologica e Dietologica 2020, 66, 201–207. [Google Scholar] [CrossRef]
- Akobeng, A.K.; Thomas, A.G. Systematic review: Tolerable amount of gluten for people with coeliac disease. Aliment. Pharmacol. Ther. 2008, 27, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Porcelli, B.; Ferretti, F.; Biviano, I.; Santini, A.; Cinci, F.; Vascotto, M.; Grande, E.; Quagliarella, F.; Terzuoli, L.; Bizzaro, N.; et al. Testing for fecal gluten immunogenic peptides: A useful tool to evaluate compliance with gluten-free diet by celiacs. Ann. Gastroenterol. 2020, 33, 631–637. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Total | HGT | HUP | p | ||
|---|---|---|---|---|---|
| Patients | 97 | 64 | 33 | ||
| Sex | Female | 75 (77.3%) | 48 (75.0%) | 27 (81.8%) | 0.477 |
| Male | 22 (22.7%) | 16 (25.0%) | 6 (18.2%) | ||
| Age (years) | 39.7 ± 18.0 (14–77) | 38.0 ± 19.2 (14–75) | 43.2 ± 15.1 (20–77) | 0.180 | |
| Age (years) at diagnosis | 31.0 ± 19.9 (0–72) | 29.1 ± 21.1 (1–68) | 34.6 ± 17.1 (0–72) | 0.168 | |
| Months in GFD | 104.9 ± 89.7 (12–362) | 106.3 ± 84.4 (12–362) | 102.1 ± 100.6 (12–318) | 0.826 | |
| Marsh type at diagnosis (%) | Marsh 3 | 60 (61.9%) | 38 (59.4%) | 22 (66.7%) | 0.313 |
| Marsh 2 | 9 (9.3%) | 8 (12.5%) | 1 (3.0%) | ||
| Marsh 1 | 11 (11.3%) | 7 (10.9%) | 4 (12.1%) | ||
| Unknown | 17 (17.5%) | 11 (17.2%) | 6 (18.2%) | ||
| Marsh type currently (%) a | Marsh 3 | 3 (3.1%) | 0 | 3 (9.1%) | 0.695 |
| Marsh 2 | 3 (3.1%) | 3 (4.7%) | 0 | ||
| Marsh 1 | 21 (21.6%) | 14 (21.9%) | 7 (21.2%) | ||
| Marsh 0 | 70 (72.2%) | 47 (73.4%) | 23 (69.7%) | ||
| Positive fecal GIPs (%) b | 22 (22.7%) [54.5%] | 15 (23.4%) [53.3%] | 7 (21.2%) [57.1%] | 0.804 | |
| Positive serum anti-tTG IgA (%) c | 11 (11.8%) | 2 (3.3%) | 9 (28.1%) | 0.001 | |
| Health-related quality of life score d | 71.6 ± 12.1 (39–96) | 71.0 ± 12.7 (39–96) | 72.7 ± 10.9 (40–89) | 0.520 | |
| CDAT score e | 12.2 ± 4.0 (7–27) | 12.2 ± 3.9 (7–24) | 12.1 ± 4.3 (7–27) | 0.910 | |
| Self-reported gluten consumption (%) f | 17 (17.5%) | 15 (23.4%) | 2 (6.1%) | 0.033 | |
| Marsh0 | Marsh1/2/3 | Total | AUC | AG | SE | SP | PPV | NPV | |
|---|---|---|---|---|---|---|---|---|---|
| GIP (iVYCHECK, Biomedal) | |||||||||
| Positive (>0.15 µg/g) | 13 | 9 | 22 | - | 68.0% | 33.3% | 81.4% | 40.9% | 76.0% |
| Negative (<0.15 µg/g) | 57 | 18 | 75 | ||||||
| Anti-tTG IgA (Liaison, Diasorin) | |||||||||
| Positive (>8 UA/mL) | 0 | 2 | 2 | 0.549 | 75.4% | 11.8% | 100% | 100% | 74.6% |
| Negative (<8 UA/mL) | 44 | 15 | 59 | ||||||
| Anti-tTG IgA (Quanta Flash, Werfen) | |||||||||
| Positive (>20 UA/mL) | 6 | 3 | 9 | 0.564 | 59.4% | 30.0% | 72.7% | 33.3% | 69.6% |
| Negative (<20 UA/mL) | 16 | 7 | 23 | ||||||
| Biopsy | Centre | Sex | Age (y) | GFD Duration (m) | Marsh (dx) | GIPs | Anti-tTG IgA (UA/mL) | IgA (mg/dL) | HRQoL Score | CDAT Score | Gluten Intake |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Marsh 2 | HGT | Female | 18 | 194 | Marsh 3 | Neg | 2.0 | 305 | 80 | 17 | Yes |
| 16 | 38 | Pos | 1.6 | 205 | 64 | 11 | |||||
| Male | 19 | 77 | 14.2 | 329 | 58 | 17 | |||||
| Marsh 3 | HUP | Female | 63 | 41 | Marsh 3 | Neg | 169.9 | 258 | 62 | 19 | No |
| 39 | 56 | 4.1 | 212 | 86 | 9 | ||||||
| 26 | 302 | Unknown | <1.9 | 172 | 85 | 14 |
| GIP Negative | GIP Positive | Total | |
|---|---|---|---|
| Gluten consumption | 8 (47.1%) | 9 (52.9%) | 17 |
| No gluten consumption | 67 (83.7%) | 13 (16.3%) | 80 |
| 75 | 22 | 97 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laserna-Mendieta, E.J.; Casanova, M.J.; Arias, Á.; Arias-González, L.; Majano, P.; Mate, L.A.; Gordillo-Vélez, C.H.; Jiménez, M.; Angueira, T.; Tébar-Romero, E.; et al. Poor Sensitivity of Fecal Gluten Immunogenic Peptides and Serum Antibodies to Detect Duodenal Mucosal Damage in Celiac Disease Monitoring. Nutrients 2021, 13, 98. https://doi.org/10.3390/nu13010098
Laserna-Mendieta EJ, Casanova MJ, Arias Á, Arias-González L, Majano P, Mate LA, Gordillo-Vélez CH, Jiménez M, Angueira T, Tébar-Romero E, et al. Poor Sensitivity of Fecal Gluten Immunogenic Peptides and Serum Antibodies to Detect Duodenal Mucosal Damage in Celiac Disease Monitoring. Nutrients. 2021; 13(1):98. https://doi.org/10.3390/nu13010098
Chicago/Turabian StyleLaserna-Mendieta, Emilio J., María José Casanova, Ángel Arias, Laura Arias-González, Pedro Majano, Luis Alberto Mate, Carlos Humberto Gordillo-Vélez, Mirella Jiménez, Teresa Angueira, Emilia Tébar-Romero, and et al. 2021. "Poor Sensitivity of Fecal Gluten Immunogenic Peptides and Serum Antibodies to Detect Duodenal Mucosal Damage in Celiac Disease Monitoring" Nutrients 13, no. 1: 98. https://doi.org/10.3390/nu13010098