Effects of Yeast Mannan Which Promotes Beneficial Bacteroides on the Intestinal Environment and Skin Condition: A Randomized, Double-Blind, Placebo-Controlled Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Subjects
2.3. Test Tablets
2.4. Fecal Microbiota Analysis
2.5. Measurement of Fecal Samples
2.6. Stool Properties and Bowel Habits
2.7. Urinal Equol
2.8. Skin Condition
2.9. Safety Evaluation
2.10. Statistical Analysis
3. Results
3.1. Characteristics of the Subjects
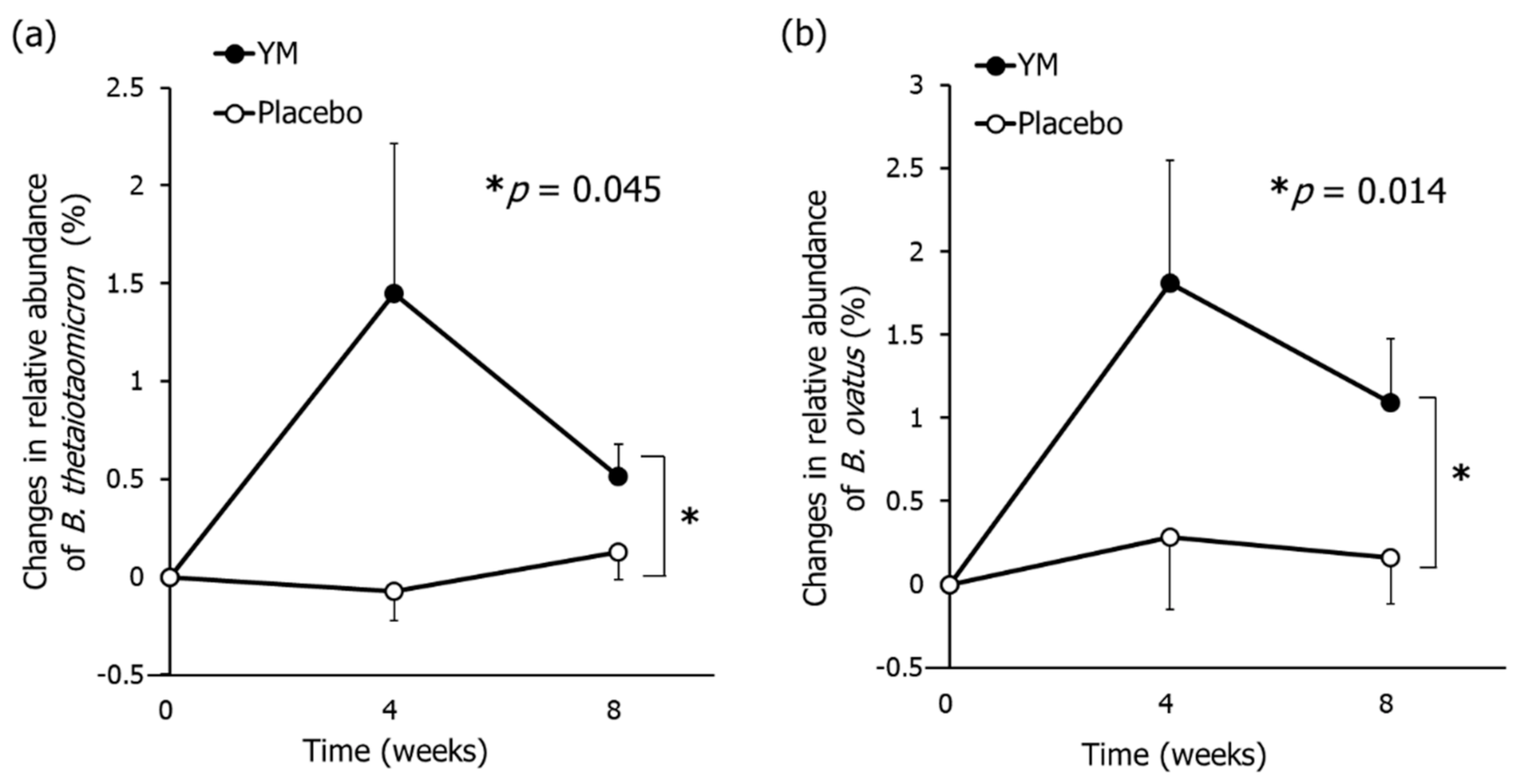
3.2. Fecal Microbiota
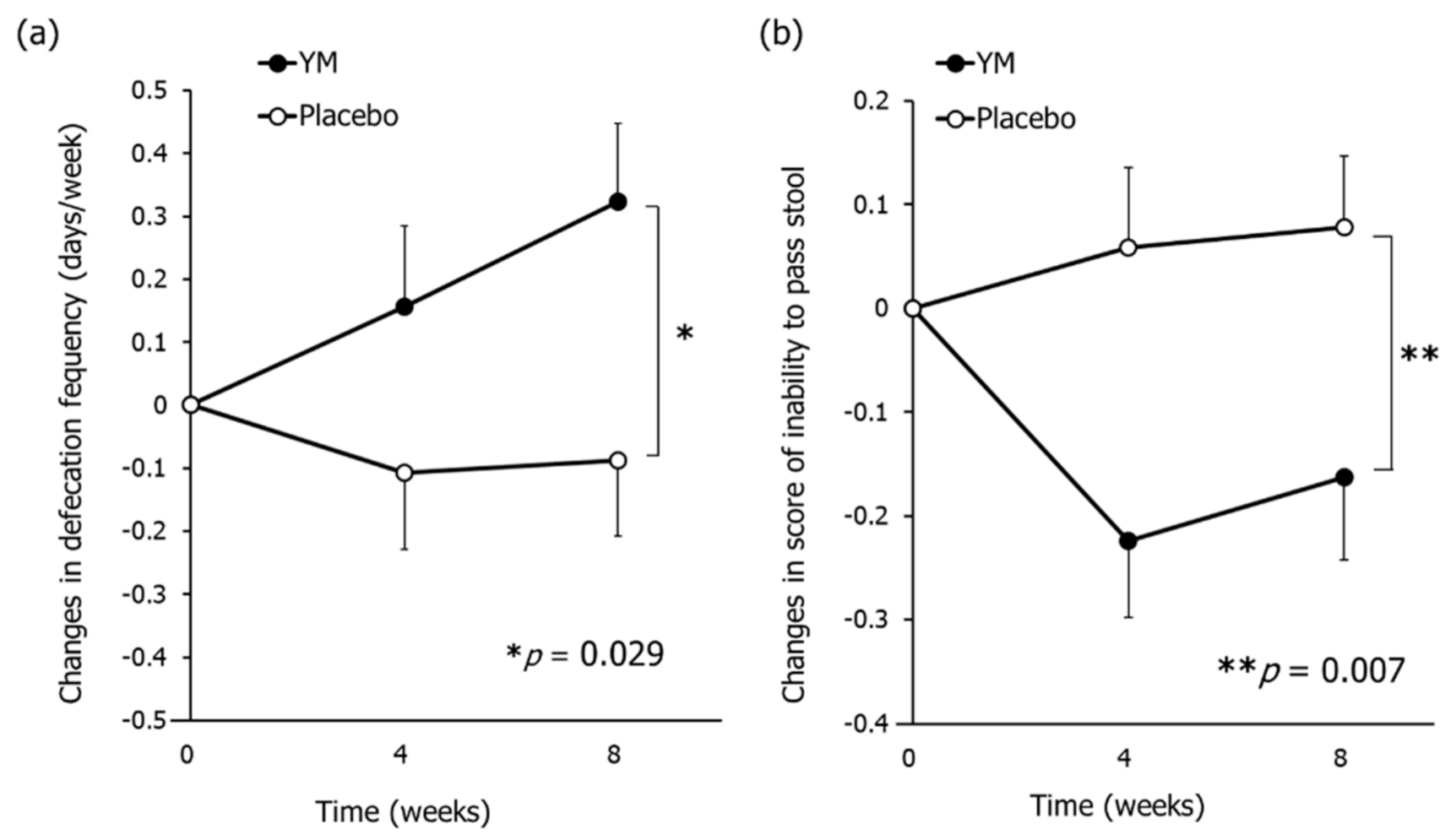
3.3. Bowel Habits and Constipation Symptoms
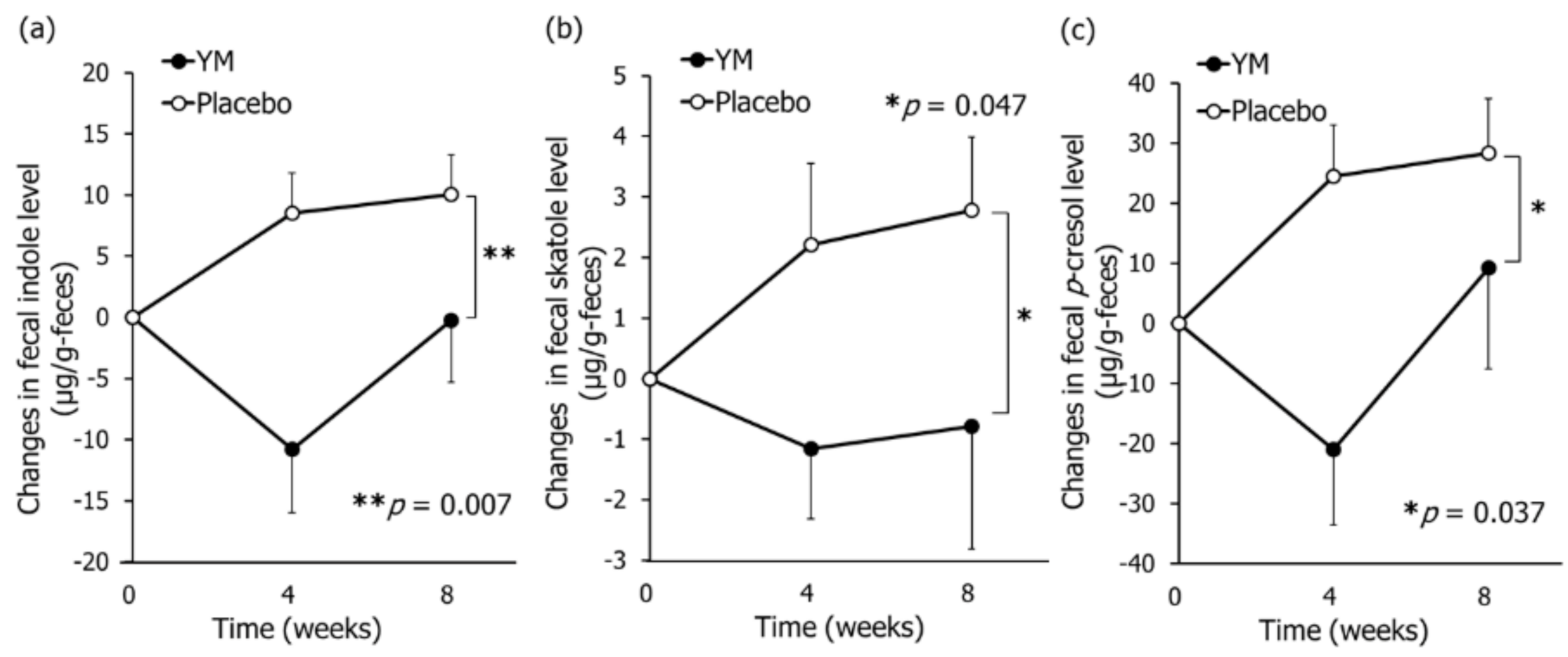
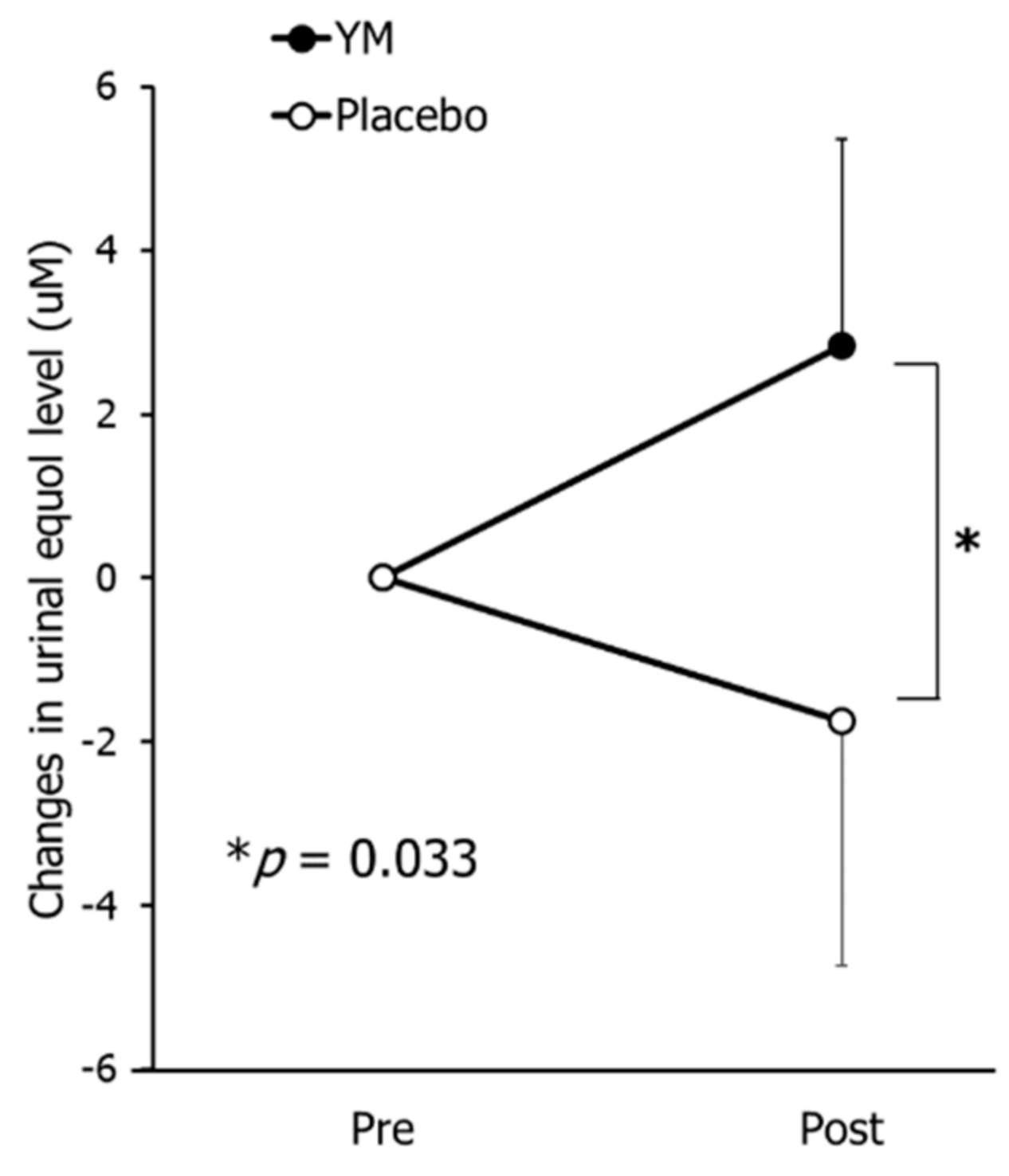
3.4. Fecal and Urinal Metabolites
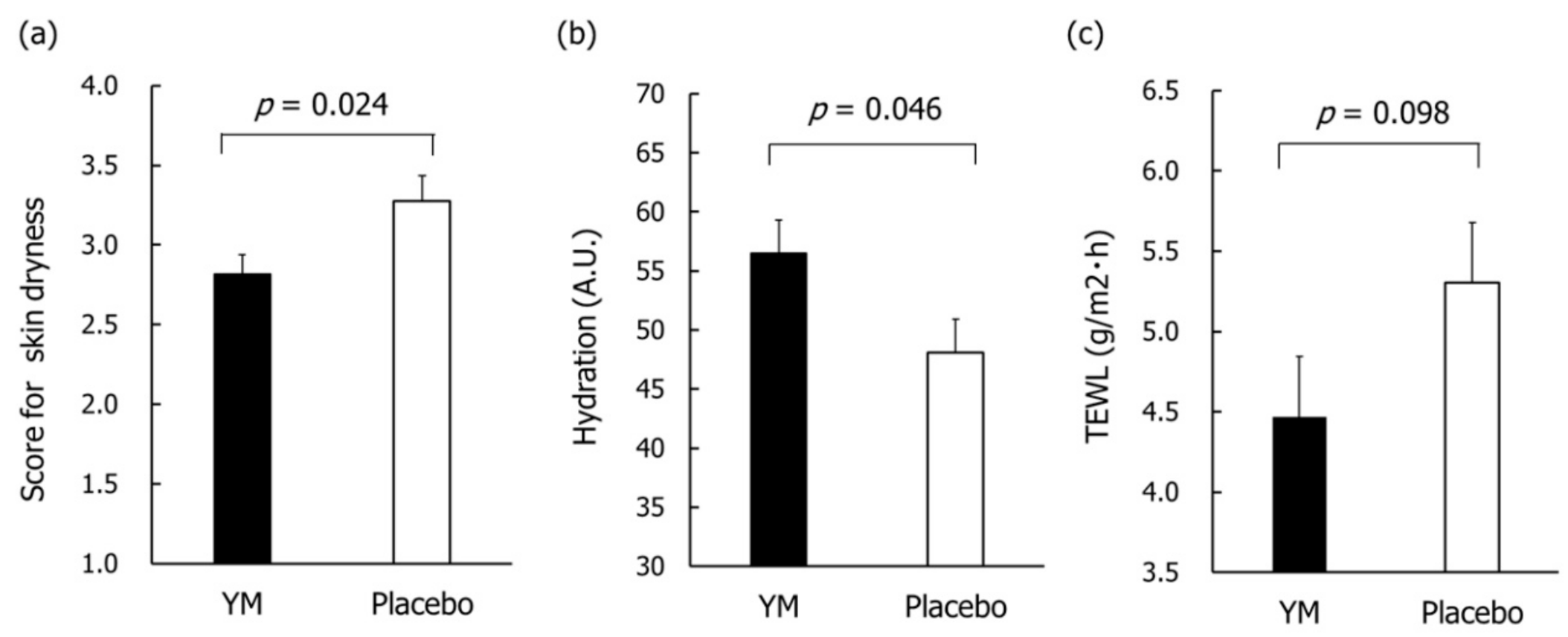
3.5. Skin Condition
3.6. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Liu, H.Z.; Liu, L.; Hui, H.; Wang, Q. Structural characterization and antineoplastic activity of Saccharomyces cerevisiae mannoprotein. Int. J. Food Prop. 2015, 18, 359–371. [Google Scholar] [CrossRef]
- Kocourek, J.; Ballou, C.E. Method for fingerprinting yeast cell wall mannans. J. Bacteriol. 1969, 100, 1175–1181. [Google Scholar] [CrossRef]
- Scheller, H.V.; Ulvskov, P. Hemicelluloses. Annu. Rev. Plant Biol. 2010, 61, 263–289. [Google Scholar] [CrossRef]
- Oba, S.; Washida, K.; Shimada, Y.; Sunagawa, T.; Tanihiro, R.; Sugiyama, H.; Nakamura, Y. Yeast mannan increases Bacteroides thetaiotaomicron abundance and suppresses putrefactive compound production in in vitro fecal microbiota fermentation. Biosci. Biotechnol. Biochem. 2020, 84, 2174–2178. [Google Scholar] [CrossRef]
- Oba, S.; Sunagawa, T.; Tanihiro, R.; Awashima, K.; Sugiyama, H.; Odani, T.; Nakamura, Y.; Kondo, A.; Sasaki, D.; Sasaki, K. Prebiotic effects of yeast mannan, which selectively promotes Bacteroides thetaiotaomicron and Bacteroides ovatus in a human colonic microbiota model. Sci. Rep. 2020, 10, 17351. [Google Scholar] [CrossRef] [PubMed]
- Cuskin, F.; Lowe, E.C.; Temple, M.J.; Zhu, Y.; Cameron, E.; Pudlo, N.A.; Porter, N.T.; Urs, K.; Thompson, A.J.; Cartmell, A.; et al. Human gut Bacteroidetes can utilize yeast mannan through a selfish mechanism. Nature 2015, 517, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Martens, E.C.; Lowe, E.C.; Chiang, H.; Pudlo, N.A.; Wu, M.; McNulty, N.; Abbott, D.W.; Henrissat, B.; Gilbert, H.J.; Bolam, D.N. Recognition and degradation of plant cell wall polysaccharides by two human gut symbionts. PLoS Biol. 2011, 9, e1001221. [Google Scholar] [CrossRef] [PubMed]
- A Phase I Randomized, Double-Blind, Placebo-Controlled Study to Assess the Safety and Tolerability of (Thetanix™) Bacteroides thetaiotaomicron in Adolescents with Stable Crohn’s Disease. Available online: https://www.4dpharmaplc.com/application/files/1815/5824/8886/Thetanix_DDW_poster_2019.pdf (accessed on 5 November 2020).
- Tan, H.; Yu, Z.; Wang, C.; Zhang, Q.; Zhao, J.; Zhang, H.; Zhai, Q.; Chen, W. Pilot Safety Evaluation of a Novel Strain of Bacteroides ovatus. Front. Genet. 2018, 9, 539. [Google Scholar] [CrossRef]
- Varyukhina, S.; Freitas, M.; Bardin, S.; Robillard, E.; Tavan, E.; Sapin, C.; Grill, J.; Trugnan, G. Glycan-modifying bacteria-derived soluble factors from Bacteroides thetaiotaomicron and Lactobacillus casei inhibit rotavirus infection in human intestinal cells. Microbes. Infect. 2012, 14, 273–278. [Google Scholar] [CrossRef]
- López-Boado, Y.S.; Wilson, C.L.; Hooper, L.V.; Gordon, J.I.; Hultgren, S.J.; Parks, W.C. Bacterial exposure induces and activates matrilysin in mucosal epithelial cells. J. Cell Biol. 2000, 148, 1305–1315. [Google Scholar] [CrossRef]
- Delday, M.; Mulder, I.; Logan, E.T.; Grant, G. Bacteroides thetaiotaomicron Ameliorates Colon Inflammation in Preclinical Models of Crohn’s Disease. Inflamm. Bowel Dis. 2019, 25, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Ulsemer, P.; Henderson, G.; Toutounian, K.; Löffler, A.; Schmidt, J.; Karsten, U.; Blaut, M.; Goletz, S. Specific humoral immune response to the Thomsen-Friedenreich tumor antigen (CD176) in mice after vaccination with the commensal bacterium Bacteroides ovatus D-6. Cancer Immunol. Immunother. 2013, 62, 875–887. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.; Zhao, J.; Zhang, H.; Zhai, Q.; Chen, W. Novel strains of Bacteroides fragilis and Bacteroides ovatus alleviate the LPS-induced inflammation in mice. Appl. Microbiol. Biotechnol. 2019, 103, 2353–2365. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Wang, J.H.; Liu, X. Metabolism of dietary soy isoflavones to equol by human intestinal microflora—Implications for health. Mol. Nutr. Food Res. 2007, 51, 765–781. [Google Scholar] [CrossRef] [PubMed]
- Ishiwata, N.; Melby, M.K.; Mizuno, S.; Watanabe, S. New equol supplement for relieving menopausal symptoms: Randomized, placebo-controlled trial of Japanese women. Menopause 2009, 16, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Takeda, T.; Shiina, M.; Chiba, Y. Effectiveness of natural S-equol supplement for premenstrual symptoms: Protocol of a randomised, double-blind, placebo-controlled trial. BMJ Open 2018, 8, e023314. [Google Scholar] [CrossRef]
- Oyama, A.; Ueno, T.; Uchiyama, S.; Aihara, T.; Miyake, A.; Kondo, S.; Matsunaga, K. The effects of natural S-equol supplementation on skin aging in postmenopausal women: A pilot randomized placebo controlled trial. Menopause 2012, 19, 202–210. [Google Scholar] [CrossRef]
- Bakke, O. Studies on the degradation of tyrosine by rat caecal contents. Scand. J. Gastroenterol. 1969, 4, 603–608. [Google Scholar]
- Miyazaki, K.; Masuoka, N.; Kano, M.; Iizuka, R. Bifidobacterium fermented milk and galacto-oligosaccharides lead to improved skin health by decreasing phenols production by gut microbiota. Benef. Microbes 2014, 5, 121–128. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Hatanaka, M.; Yamamoto, K.; Suzuki, N.; Iio, S.; Takara, T.; Morita, H.; Takimoto, T.; Nakamura, T. Effect of Bacillus subtilis C-3102 on loose stools in healthy volunteers. Benef. Microbes 2018, 9, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Tong, J.; Liu, C.; Summanen, P.; Xu, H.; Finegold, S. Application of quantitative real-time PCR for rapid identification of Bacteroides fragilis group and related organisms in human wound samples. Anaerobe 2011, 17, 64–68. [Google Scholar] [CrossRef]
- Furet, J.; Firmesse, O.; Gourmelon, M.; Bridonneau, C.; Tap, J.; Mondot, S.; Dor´e, J.; Corthier, G. Comparative assessment of human and farm animal faecal microbiota using real-time quantitative PCR. FEMS Microbiol. Ecol. 2009, 68, 351–362. [Google Scholar] [CrossRef] [PubMed]
- Imoto, N.; Morita, H.; Amanuma, F.; Maruyama, H.; Watanabe, S.; Hashiguchi, N. Maternal antimicrobial use at delivery has a stronger impact than mode of delivery on bifidobacterial colonization in infants: A pilot study. J. Perinatol. 2018, 38, 1174–1181. [Google Scholar] [CrossRef] [PubMed]
- Caporaso, J.G.; Kuczynski, J.; Stombaugh, J.; Bittinger, K.; Bushman, F.D.; Costello, E.K.; Fierer, N.; Peña, A.G.; Goodrich, J.K.; Gordon, J.I.; et al. QIIME allows analysis of high-throughput community sequencing data. Nat. Methods 2010, 7, 335–336. [Google Scholar] [CrossRef]
- The Greengenes Database. Available online: http://greengenes.secondgenome.com/?prefix=downloads/greengenes_database/gg_13_5/ (accessed on 5 November 2020).
- Aoe, S.; Nakamura, F.; Fujiwara, S. Effects of wheat bran on fecal butyrate-producing bacteria and wheat bran combined with barley on Bacteroides abundance in Japanese healthy adults. Nutrients 2018, 10, 1980. [Google Scholar] [CrossRef]
- Ikeda, N.; Saito, Y.; Shimizu, J.; Ochi, A.; Mizutani, J.; Watabe, J. Variations in concentrations of bacterial metabolites, enzyme activities, moisture, pH and bacterial composition between and within individuals in faeces of seven healthy adults. J. Appl. Bacteriol. 1994, 77, 185–194. [Google Scholar] [CrossRef]
- O’Donnell, L.J.; Virjee, J.; Heaton, K.W. Detection of pseudodiarrhoea by simple clinical assessment of intestinal transit rate. BMJ 1990, 300, 439–440. [Google Scholar] [CrossRef]
- Nagaviroj, K.; Yong, W.C.; Fassbender, K.; Zhu, G.; Oneschuk, D. Comparison of the constipation assessment scale and plain abdominal radiography in the assessment of constipation in advanced cancer patients. J. Pain Symptom Manag. 2011, 42, 222–228. [Google Scholar] [CrossRef]
- Fukai, K.; Sugita, A.; Tanaka, M. A developmental study of the Japanese version of the constipation assessment scale. JJNS 1995, 28, 201–207. [Google Scholar]
- Redruelloa, B.; Guadamurob, L.; Cuestaa, I.; Álvarez-Buyllaa, J.R.; Mayob, B.; Delgado, S. A novel UHPLC method for the rapid and simultaneous determination of daidzein, genistein and equol in human urine. J. Chromatogr. B 2015, 1005, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Likert, R. A technique for the measurement of attitudes. Arch. Psychol. 1932, 22, 5–55. [Google Scholar]
- Shilnikova, I.I.; Dmitrieva, N.V. Evaluation of antibiotic susceptibility of Bacteroides, Prevotella and Fusobacterium species isolated from patients of the N. N. Blokhin Cancer Research Center, Moscow, Russia. Anaerobe 2015, 31, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.; Amin, N.E.; Davies, T.; Appelbaum, P.C.; Edlund, C. gyrA mutations associated with quinolone resistance in Bacteroides fragilis group strains. Antimicrob. Agents Chemother. 2001, 45, 1977–1981. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, J. Carbonhydrate fermentation in the colon. J. Intest. Microbiol. 2005, 19, 169–177. [Google Scholar]
- Roberfroid, M.; Gibson, G.R.; Hoyles, L.; McCartney, A.L.; Rastall, R.; Rowland, I.; Wolvers, D.; Watzl, B.; Szajewska, H.; Stahl, B.; et al. Prebiotic effects: Metabolic and health benefits. Br. J. Nutr. 2010, 104, S1–S63. [Google Scholar] [CrossRef]
- Tzianabos, A.O.; Onderdonk, A.B.; Rosner, B.; Cisneros, R.L.; Kasper, D.L. Structural features of polysaccharides that induce intra-abdominal abscesses. Science 1993, 262, 416–419. [Google Scholar] [CrossRef]
- Bamba, T.; Matsuda, H.; Endo, M.; Fujiyama, Y. The pathogenic role of Bacteroides vulgatus in patients with ulcerative colitis. J. Gastroenterol. 1995, 30, 45–47. [Google Scholar]
- François, I.E.J.A.; Lescroart, O.; Veraverbeke, W.S.; Marzorati, M.; Possemiers, S.; Evenepoel, P.; Hamer, H.; Houben, E.; Windey, K.; Welling, G.W.; et al. Effects of a wheat bran extract containing arabinoxylan oligosaccharides on gastrointestinal health parameters in healthy adult human volunteers: A double-blind, randomised, placebo-controlled, cross-over trial. Br. J. Nutr. 2012, 108, 2229–2242. [Google Scholar] [CrossRef]
- Li, L.; Xiong, Q.; Zhao, J.; Lin, X.; He, S.; Wu, N.; Yao, Y.; Liang, W.; Zuo, X.; Ying, C. Inulin-type fructan intervention restricts the increase in gut microbiome-generated indole in patients with peritoneal dialysis: A randomized crossover study. Am. J. Clin. Nutr. 2020, 111, 1087–1099. [Google Scholar] [CrossRef]
- Okubo, T.; Ishihara, N.; Takahashi, H.; Fujisawa, T.; Kim, M.; Yamamoto, T.; Mitsuoka, T. Effects of partially hydrolyzed guar gum intake on human intestinal microflora and its metabolism. Biosci. Biotechnol. Biochem. 1994, 58, 1364–1369. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhi, F. Lower level of Bacteroides in the gut microbiota is associated with inflammatory bowel disease: A meta-analysis. Biomed. Res. Int. 2016, 5828959. [Google Scholar] [CrossRef] [PubMed]
- Png, C.W.; Lindén, S.W.; Gilshenan, K.S.; Zoetendal, E.G.; McSweeney, C.S.; Sly, L.I.; McGuckin, M.A.; Florin, T.H.J. Mucolytic bacteria with increased prevalence in IBD mucosa augment in vitro utilization of mucin by other bacteria. Am. J. Gastroenterol. 2010, 105, 2420–2428. [Google Scholar] [CrossRef] [PubMed]
- Ji, M.; Du, H.; Xu, Y. Structural and metabolic performance of p-cresol producing microbiota in different carbon sources. Food Res. Int. 2020, 132, 109049. [Google Scholar] [CrossRef]
- Amaretti, A.; Gozzoli, C.; Simone, M.; Raimondi, S.; Righini, L.; Pérez-Brocal, V.; Rodrigo García-López, R.; Moya, A.; Rossi, M. Profiling of protein degraders in cultures of human gut microbiota. Front Microbiol. 2019, 15, 2614. [Google Scholar] [CrossRef]
- Matsumoto, M.; Iino, H.; Suganuma, H. Intestinal Microbiota Correlate to Menstrual Cycle-Dependent Complaints and Plasma Levels of Female Hormones. In Proceedings of the Annual Meeting of Intestinal Microbiology, Tokyo, Japan, 9 June 2016; Volume A-7, p. 95. Available online: https://bifidus-fund.jp/meeting/pdf/20th/A1-7.pdf (accessed on 27 November 2020).
- Tamura, M.; Hori, S.; Nakagawa, H. Impact of dietary polydextrose on the daidzein metabolism in adult mice. Biosci. Microflora 2010, 29, 185–190. [Google Scholar] [CrossRef][Green Version]
- Tamura, M.; Kurusu, Y.; Hori, S. Effect of dietary L-arabinose on the intestinal microbiota and metabolism of dietary daidzein in adult mice. Biosci. Microbiota Food Health 2012, 31, 59–65. [Google Scholar] [CrossRef]
- Tamura, M.; Hoshi, C.; Hori, S. Xylitol affects the intestinal microbiota and metabolism of daidzein in adult male mice Int. J. Mol. Sci. 2013, 14, 23993–24007. [Google Scholar] [CrossRef]
- Salem, I.; Ramser, A.; Isham, N.; Ghannoum, M.A. The gut microbiome as a major regulator of the gut-skin axis. Front Microbiol. 2018, 9, 1459. [Google Scholar] [CrossRef]
- Leveque, J.L.; Corcuff, P.; De Rigal, J.; Agache, P. In vivo studies of the evolution of physical properties of the human skin with age. Int. J. Dermatol. 1984, 23, 322–329. [Google Scholar] [CrossRef]
- Darlenski, R.; Sassning, S.; Tsankov, N.; Fluhr, J.W. Non-invasive in vivo methods for investigation of the skin barrier. Eur. J. Pharm. Biopharm. 2009, 72, 295–303. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Events | Pretrial Test | Period of Time (Weeks) | The End of the Examination | |||
|---|---|---|---|---|---|---|
| –2 | 0 | 4 | 8 | |||
| Visit | ● | ● | ● | ● | ● | |
| Test-samples intake |  | |||||
| Soy-isoflavone intake |  | | ||||
| Urine sampling | ● | ● | ||||
| Feces sampling | ● | ● | ● | |||
| CAS | ● | ● | ● | |||
| Measurement of skin | ● | ● | ● | |||
| Questionnaire of skin | ● | ● | ||||
| Blood sampling | ● | ● | ||||
| Medical interview | ● | ● | ● | ● | ● | |
| Diary |  | |||||
| Parameters | Unit | YM Group | Placebo Group | p-Value |
|---|---|---|---|---|
| Age | years | 40.7 ± 5.6 | 40.7 ± 5.7 | 0.995 |
| Body mass index (BMI) | kg/m2 | 20.5 ± 2.2 | 21.0 ± 2.8 | 0.298 |
| Systolic blood pressure | mmHg | 108.7 ± 10.9 | 110.4 ± 12.6 | 0.461 |
| Diastolic blood pressure | mmHg | 66.0 ± 8.4 | 67.8 ± 9.6 | 0.310 |
| Pulse rate | bpm | 71.0 ± 8.0 | 73.3 ± 10.6 | 0.219 |
| Hydration level (inner forearm) | - | 30.3 ± 4.0 | 29.4 ± 4.1 | 0.295 |
| TEWL (inner forearm) | g/m2h | 6.0 ± 1.0 | 5.9 ± 1.1 | 0.905 |
| Genus | Groups | Relative Abundance (%) | p-Value | ||
|---|---|---|---|---|---|
| Baseline | 4 Weeks | 8 Weeks | |||
| Bifidobacterium | YM | 9.1 ± 1.4 | 6.7 ± 1.1 | 6.6 ± 1.0 | 0.062 |
| Placebo | 6.2 ± 0.8 | 4.2 ± 0.6 | 5.1 ± 0.9 | ||
| Bacteroides | YM | 20.1 ± 1.9 | 27.7 ± 2.5 | 26.8 ± 2.1 | 0.076 |
| Placebo | 17.8 ± 1.8 | 21.8 ± 1.8 | 22.9 ± 1.9 | ||
| Parabacteroides | YM | 1.4 ± 0.3 | 2.0 ± 0.5 | 2.3 ± 0.4 | 0.064 |
| Placebo | 1.2 ± 0.2 | 1.3 ± 0.2 | 1.3 ± 0.1 | ||
| Rikenellaceae;g | YM | 1.4 ± 0.2 | 1.7 ± 0.4 | 2.0 ± 0.4 | 0.392 |
| Placebo | 2.1 ± 0.5 | 2.0 ± 0.3 | 2.2 ± 0.4 | ||
| Clostridiales;f;g * | YM | 0.8 ± 0.2 | 0.4 ± 0.1 | 0.9 ± 0.3 | 0.018 |
| Placebo | 1.9 ± 0.5 | 1.9 ± 0.5 | 2.5 ± 0.6 | ||
| Lachnospiraceae;g | YM | 4.3 ± 0.6 | 4.7 ± 0.6 | 4.6 ± 0.6 | 0.693 |
| Placebo | 4.7 ± 0.4 | 4.9 ± 0.4 | 4.7 ± 0.4 | ||
| Blautia | YM | 11.8 ± 1.4 | 8.7 ± 1.0 | 8.0 ± 1.2 | 0.942 |
| Placebo | 11.2 ± 1.2 | 8.3 ± 0.9 | 8.7 ± 0.9 | ||
| Coprococcus | YM | 5.6 ± 0.8 | 4.6 ± 0.6 | 4.6 ± 0.7 | 0.082 |
| Placebo | 7.2 ± 0.8 | 6.0 ± 0.7 | 5.9 ± 0.6 | ||
| Roseburia | YM | 4.0 ± 0.8 | 3.0 ± 0.5 | 3.1 ± 0.5 | 0.343 |
| Placebo | 4.3 ± 0.7 | 3.7 ± 0.6 | 3.9 ± 0.6 | ||
| Lachnospiraceae;g[Ruminococcus] | YM | 4.0 ± 0.8 | 2.8 ± 0.4 | 2.4 ± 0.3 | 0.340 |
| Placebo | 2.5 ± 0.5 | 2.6 ± 0.3 | 2.7 ± 0.4 | ||
| Ruminococcaceae;g ** | YM | 0.8 ± 0.2 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.008 |
| Placebo | 1.6 ± 0.4 | 2.1 ± 0.4 | 1.9 ± 0.4 | ||
| Faecalibacterium | YM | 14.5 ± 1.4 | 14.1 ± 1.4 | 14.1 ± 1.3 | 0.844 |
| Placebo | 14.6 ± 1.2 | 15.8 ± 1.1 | 13.2 ± 1.0 | ||
| Oscillospira | YM | 2.1 ± 0.3 | 1.9 ± 0.2 | 2.4 ± 0.3 | 0.424 |
| Placebo | 2.2 ± 0.2 | 2.4 ± 0.2 | 2.4 ± 0.2 | ||
| Ruminococcus * | YM | 2.3 ± 0.4 | 2.2 ± 0.3 | 2.5 ± 0.4 | 0.015 |
| Placebo | 3.2 ± 0.4 | 3.4 ± 0.4 | 3.8 ± 0.4 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanihiro, R.; Sakano, K.; Oba, S.; Nakamura, C.; Ohki, K.; Hirota, T.; Sugiyama, H.; Ebihara, S.; Nakamura, Y. Effects of Yeast Mannan Which Promotes Beneficial Bacteroides on the Intestinal Environment and Skin Condition: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients 2020, 12, 3673. https://doi.org/10.3390/nu12123673
Tanihiro R, Sakano K, Oba S, Nakamura C, Ohki K, Hirota T, Sugiyama H, Ebihara S, Nakamura Y. Effects of Yeast Mannan Which Promotes Beneficial Bacteroides on the Intestinal Environment and Skin Condition: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients. 2020; 12(12):3673. https://doi.org/10.3390/nu12123673
Chicago/Turabian StyleTanihiro, Reiko, Katsuhisa Sakano, Shunsuke Oba, Chikako Nakamura, Kohji Ohki, Tatsuhiko Hirota, Hiroshi Sugiyama, Shukuko Ebihara, and Yasunori Nakamura. 2020. "Effects of Yeast Mannan Which Promotes Beneficial Bacteroides on the Intestinal Environment and Skin Condition: A Randomized, Double-Blind, Placebo-Controlled Study" Nutrients 12, no. 12: 3673. https://doi.org/10.3390/nu12123673
APA StyleTanihiro, R., Sakano, K., Oba, S., Nakamura, C., Ohki, K., Hirota, T., Sugiyama, H., Ebihara, S., & Nakamura, Y. (2020). Effects of Yeast Mannan Which Promotes Beneficial Bacteroides on the Intestinal Environment and Skin Condition: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients, 12(12), 3673. https://doi.org/10.3390/nu12123673