Effects of a Fermented Dairy Drink Containing Lacticaseibacillus paracasei subsp. paracasei CNCM I-1518 (Lactobacillus casei CNCM I-1518) and the Standard Yogurt Cultures on the Incidence, Duration, and Severity of Common Infectious Diseases: A Systematic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Inclusion and Exclusion Criteria
2.3. Data Extraction and Assessment of Study Quality
2.4. Statistical Analysis
3. Results
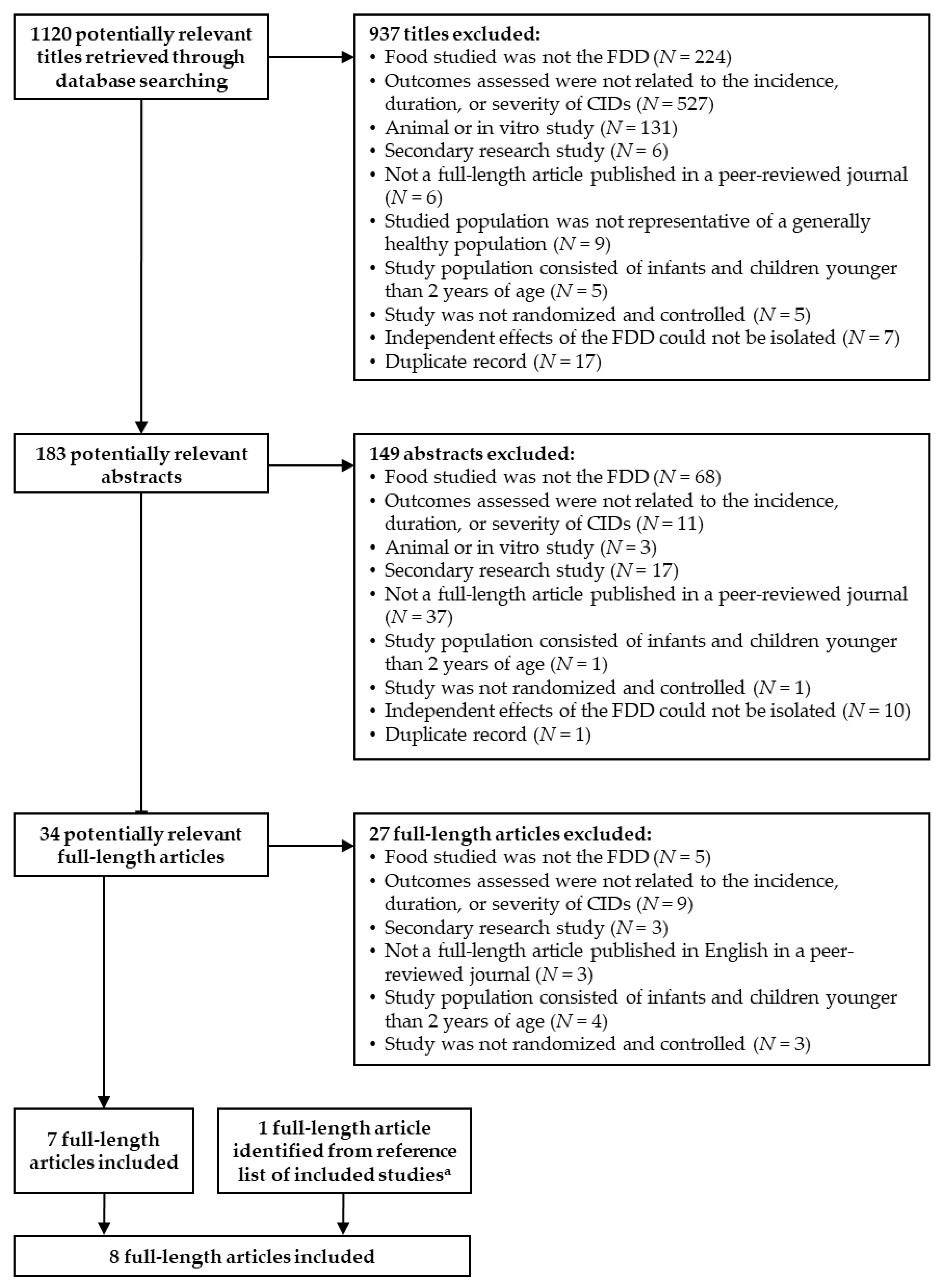
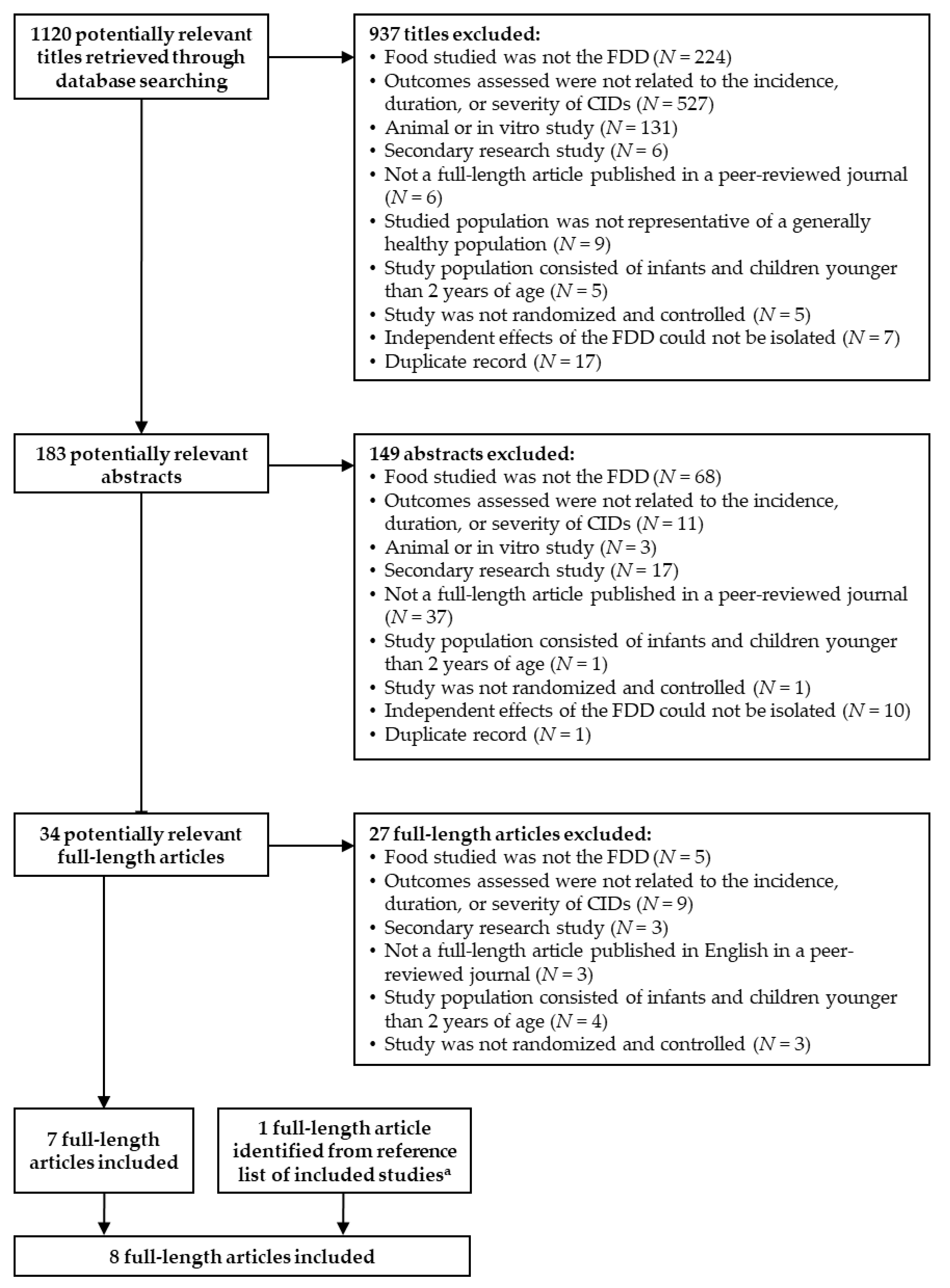
3.1. Identification of Literature
3.2. Children
3.3. Adults
3.4. Elderly
3.5. Meta-Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- GBD. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Prodeus, A.; Niborski, V.; Schrezenmeir, J.; Gorelov, A.; Shcherbina, A.; Rumyantsev, A. Fermented milk consumption and common infections in children attending day-care centers: A randomized trial. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 534–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majowicz, S.E.; McNab, W.B.; Sockett, P.; Henson, T.S.; Doré, K.; Edge, V.L.; Buffett, M.C.; Fazil, A.; Read, S.; McEwen, S.; et al. Burden and cost of gastroenteritis in a Canadian community. J. Food Prot. 2006, 69, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Kawai, K.; O’Brien, M.A.; Goveia, M.G.; Mast, T.C.; El Khoury, A.C. Burden of rotavirus gastroenteritis and distribution of rotavirus strains in Asia: A systematic review. Vaccine 2012, 30, 1244–1254. [Google Scholar] [CrossRef]
- Dicpinigaitis, P.V.; Eccles, R.; Blaiss, M.S.; Wingertzahn, M.A. Impact of cough and common cold on productivity, absenteeism, and daily life in the United States: ACHOO Survey. Curr. Med. Res. Opin. 2015, 31, 1519–1525. [Google Scholar] [CrossRef]
- Chen, Y.; Ford, L.; Hall, G.; Dobbins, T.; Kirk, M. Healthcare utilization and lost productivity due to infectious gastroenteritis, results from a national cross-sectional survey Australia 2008–2009. Epidemiol. Infect. 2016, 144, 241–246. [Google Scholar] [CrossRef]
- Taylor, S.; Lopez, P.; Weckx, L.; Borja-Tabora, C.; Ulloa-Gutierrez, R.; Lazcano-Ponce, E.; Kerdpanich, A.; Angel Rodriguez Weber, M.; Mascareñas de Los Santos, A.; Tinoco, J.C.; et al. Respiratory viruses and influenza-like illness: Epidemiology and outcomes in children aged 6 months to 10 years in a multi-country population sample. J. Infect. 2017, 74, 29–41. [Google Scholar] [CrossRef]
- Putri, W.; Muscatello, D.J.; Stockwell, M.S.; Newall, A.T. Economic burden of seasonal influenza in the United States. Vaccine 2018, 36, 3960–3966. [Google Scholar] [CrossRef]
- Neuzil, K.M.; Hohlbein, C.; Zhu, Y. Illness among schoolchildren during influenza season: Effect on school absenteeism, parental absenteeism from work, and secondary illness in families. Arch. Pediatr. Adolesc. Med. 2002, 156, 986–991. [Google Scholar] [CrossRef] [Green Version]
- Linder, J.A.; Singer, D.E. Health-related quality of life of adults with upper respiratory tract infections. J. Gen. Intern. Med. 2003, 18, 802–807. [Google Scholar] [CrossRef] [Green Version]
- Diez Domingo, J.; Patrzalek, M.; Cantarutti, L.; Arnould, B.; Meunier, J.; Soriano-Gabarro, M.; Meyer, N.; Pirçon, J.Y.; Holl, K. The impact of childhood acute rotavirus gastroenteritis on the parents’ quality of life: Prospective observational study in European primary care medical practices. BMC Pediatr. 2012, 12, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marlow, R.; Finn, A.; Trotter, C. Quality of life impacts from rotavirus gastroenteritis on children and their families in the UK. Vaccine 2015, 33, 5212–5216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, B.C.; Ma, S.S.; Goldenberg, J.Z.; Thorlund, K.; Vandvik, P.O.; Loeb, M.; Guyatt, G.H. Probiotics for the prevention of Clostridium difficile-associated diarrhea: A systematic review and meta-analysis. Ann. Intern. Med. 2012, 157, 878–888. [Google Scholar] [CrossRef] [PubMed]
- King, S.; Glanville, J.; Sanders, M.E.; Fitzgerald, A.; Varley, D. Effectiveness of probiotics on the duration of illness in healthy children and adults who develop common acute respiratory infectious conditions: A systematic review and meta-analysis. Br. J. Nutr. 2014, 112, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Caffarelli, C.; Cardinale, F.; Povesi-Dascola, C.; Dodi, I.; Mastrorilli, V.; Ricci, G. Use of probiotics in pediatric infectious diseases. Expert Rev. Anti. Infect. Ther. 2015, 13, 1517–1535. [Google Scholar] [CrossRef]
- Goldenberg, J.Z.; Lytvyn, L.; Steurich, J.; Parkin, P.; Mahant, S.; Johnston, B.C. Probiotics for the prevention of pediatric antibiotic-associated diarrhea. Cochrane Database Syst. Rev. 2015, 11, CD004827.pub4. [Google Scholar] [CrossRef]
- Hao, Q.; Dong, B.R.; Wu, T. Probiotics for preventing acute upper respiratory tract infections. Cochrane Database Syst. Rev. 2015, 2, CD006895. [Google Scholar] [CrossRef]
- McFarland, L.V. Probiotics for the Primary and Secondary prevention of C. difficile infections: A meta-analysis and systematic review. Antibiotics 2015, 4, 160–178. [Google Scholar] [CrossRef] [Green Version]
- Amaral, M.A.; Guedes, G.; Epifanio, M.; Wagner, M.B.; Jones, M.H.; Mattiello, R. Network meta-analysis of probiotics to prevent respiratory infections in children and adolescents. Pediatr. Pulmonol. 2017, 52, 833–843. [Google Scholar] [CrossRef]
- Feng, J.R.; Wang, F.; Qiu, X.; McFarland, L.V.; Chen, P.F.; Zhou, R.; Liu, J.; Zhao, Q.; Li, J. Efficacy and safety of probiotic-supplemented triple therapy for eradication of Helicobacter pylori in children: A systematic review and network meta-analysis. Eur. J. Clin. Pharmacol. 2017, 73, 1199–1208. [Google Scholar] [CrossRef]
- Laursen, R.P.; Hojsak, I. Probiotics for respiratory tract infections in children attending day care centers-a systematic review. Eur. J. Pediatr. 2018, 177, 979–994. [Google Scholar] [CrossRef] [PubMed]
- Scott, A.M.; Clark, J.; Julien, B.; Islam, F.; Roos, K.; Grimwood, K.; Little, P.; Del Mar, C.B. Probiotics for preventing acute otitis media in children. Cochrane Database Syst. Rev. 2019, 6, CD012941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Didari, T.; Solki, S.; Mozaffari, S.; Nikfar, S.; Abdollahi, M. A systematic review of the safety of probiotics. Expert. Opin. Drug Saf. 2014, 13, 227–239. [Google Scholar] [CrossRef] [PubMed]
- Merenstein, D.; Murphy, M.; Fokar, A.; Hernandez, R.K.; Park, H.; Nsouli, H.; Sanders, M.E.; Davis, B.A.; Niborski, V.; Tondu, F.; et al. Use of a fermented dairy probiotic drink containing Lactobacillus casei (DN-114 001) to decrease the rate of illness in kids: The DRINK study. A patient-oriented, double-blind, cluster-randomized, placebo-controlled, clinical trial. Eur.J. Clin. Nutr. 2010, 64, 669–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, J.; Wittouck, S.; Salvetti, E.; Franz, C.; Harris, H.M.B.; Mattarelli, P.; O’Toole, P.W.; Pot, B.; Vandamme, P.; Walter, J.; et al. A taxonomic note on the genus Lactobacillus: Description of 23 novel genera, emended description of the genus Lactobacillus Beijerinck 1901, and union of Lactobacillaceae and Leuconostocaceae. Int. J. Syst. Evol. Microbiol. 2020, 70, 2782–2858. [Google Scholar] [CrossRef]
- Ingrassia, I.; Leplingard, A.; Darfeuille-Michaud, A. Lactobacillus casei DN-114 001 inhibits the ability of adherent-invasive Escherichia coli isolated from Crohn’s disease patients to adhere to and to invade intestinal epithelial cells. Appl. Environ. Microbiol. 2005, 71, 2880–2887. [Google Scholar] [CrossRef] [Green Version]
- Llopis, M.; Antolín, M.; Guarner, F.; Salas, A.; Malagelada, J.R. Mucosal colonisation with Lactobacillus casei mitigates barrier injury induced by exposure to trinitronbenzene sulphonic acid. Gut 2005, 54, 955–959. [Google Scholar] [CrossRef] [Green Version]
- Zakostelska, Z.; Kverka, M.; Klimesova, K.; Rossmann, P.; Mrazek, J.; Kopecny, J.; Hornova, M.; Srutkova, D.; Hudcovic, T.; Ridl, J.; et al. Lysate of probiotic Lactobacillus casei DN-114 001 ameliorates colitis by strengthening the gut barrier function and changing the gut microenvironment. PLoS ONE 2011, 6, e27961. [Google Scholar] [CrossRef]
- Cazorla, S.I.; Maldonado-Galdeano, C.; Wdeill, R.; De Paula, J.; Perdigón, G.D.V. Oral administration of probiotics increases Paneth cells and intestinal antimicrobial activity. Front. Microbiol. 2018, 9, 736. [Google Scholar] [CrossRef]
- Oozeer, R.; Goupil-Feuillerat, N.; Alpert, C.A.; van de Guchte, M.; Anba, J.; Mengaud, J.; Corthier, G. Lactobacillus casei is able to survive and initiate protein synthesis during its transit in the digestive tract of human flora-associated mice. Appl. Environ. Microbiol. 2002, 68, 3570–3574. [Google Scholar] [CrossRef] [Green Version]
- Oozeer, R.; Leplingard, A.; Mater, D.D.; Mogenet, A.; Michelin, R.; Seksek, I.; Marteau, P.; Doré, J.; Bresson, J.L.; Corthier, G. Survival of Lactobacillus casei in the human digestive tract after consumption of fermented milk. Appl. Environ. Microbiol. 2006, 72, 5615–5617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochet, V.; Rigottier-Gois, L.; Levenez, F.; Cadiou, J.; Marteau, P.; Bresson, J.L.; Goupil-Feillerat, N.; Doré, J. Modulation of Lactobacillus casei in ileal and fecal samples from healthy volunteers after consumption of a fermented milk containing Lactobacillus casei DN-114 001Rif. Can. J. Microbiol. 2008, 54, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Borruel, N.; Casellas, F.; Antolín, M.; Llopis, M.; Carol, M.; Espíin, E.; Naval, J.; Guarner, F.; Malagelada, J.R. Effects of nonpathogenic bacteria on cytokine secretion by human intestinal mucosa. Am. J. Gastroenterol. 2003, 98, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Plantinga, T.S.; van Maren, W.W.; van Bergenhenegouwen, J.; Hameetman, M.; Nierkens, S.; Jacobs, C.; de Jong, D.J.; Joosten, L.A.; van’t Land, B.; Garssen, J.; et al. Differential Toll-like receptor recognition and induction of cytokine profile by Bifidobacterium breve and Lactobacillus strains of probiotics. Clin. Vaccine Immunol. 2011, 18, 621–628. [Google Scholar] [CrossRef]
- Belkacem, N.; Serafini, N.; Wheeler, R.; Derrien, M.; Boucinha, L.; Couesnon, A.; Cerf-Bensussan, N.; Gomperts Boneca, I.; Di Santo, J.P.; Taha, M.K.; et al. Lactobacillus paracasei feeding improves immune control of influenza infection in mice. PLoS ONE 2017, 12, e0184976. [Google Scholar] [CrossRef]
- Pujol, P.; Huguet, J.; Drobnic, F.; Banquells, M.; Ruiz, O.; Galilea, P.; Segarra, N.; Aguilera, S.; Burnat, A.; Mateos, J.A.; et al. The effect of fermented milk containing Lactobacillus casei on the immune response to exercise. Sports Med. Train. Rehab. 2000, 9, 209–223. [Google Scholar] [CrossRef]
- Marcos, A.; Wärnberg, J.; Nova, E.; Gómez, S.; Alvarez, A.; Alvarez, R.; Mateos, J.A.; Cobo, J.M. The effect of milk fermented by yogurt cultures plus Lactobacillus casei DN-114001 on the immune response of subjects under academic examination stress. Eur. J. Nutr. 2004, 43, 381–389. [Google Scholar] [CrossRef]
- Ortiz-Andrellucchi, A.; Sánchez-Villegas, A.; Rodríguez-Gallego, C.; Lemes, A.; Molero, T.; Soria, A.; Peña-Quintana, L.; Santana, M.; Ramírez, O.; García, J.; et al. Immunomodulatory effects of the intake of fermented milk with Lactobacillus casei DN114001 in lactating mothers and their children. Br. J. Nutr. 2008, 100, 834–845. [Google Scholar] [CrossRef] [Green Version]
- Guillemard, E.; Tanguy, J.; Flavigny, A.; de la Motte, S.; Schrezenmeir, J. Effects of consumption of a fermented dairy product containing the probiotic Lactobacillus casei DN-114 001 on common respiratory and gastrointestinal infections in shift workers in a randomized controlled trial. J. Am. Coll. Nutr. 2010, 29, 455–468. [Google Scholar] [CrossRef]
- Boge, T.; Rémigy, M.; Vaudaine, S.; Tanguy, J.; Bourdet-Sicard, R.; van der Werf, S. A probiotic fermented dairy drink improves antibody response to influenza vaccination in the elderly in two randomised controlled trials. Vaccine 2009, 27, 5677–5684. [Google Scholar] [CrossRef]
- Turchet, P.; Laurenzano, M.; Auboiron, S.; Antoine, J.M. Effect of fermented milk containing the probiotic Lactobacillus casei DN-114001 on winter infections in free-living elderly subjects: A randomised, controlled pilot study. J. Nutr. Health Aging 2003, 7, 75–77. [Google Scholar] [PubMed]
- Guillemard, E.; Tondu, F.; Lacoin, F.; Schrezenmeir, J. Consumption of a fermented dairy product containing the probiotic Lactobacillus casei DN-114001 reduces the duration of respiratory infections in the elderly in a randomised controlled trial. Br. J. Nutr. 2010, 103, 58–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NHLBI. Study Quality Assessment Tools. National Institutes of Health (NIH), National Heart, Lung, and Blood Institute (NHLBI): Bethesda, MD, USA. 2020. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 10 February 2020).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Pereg, D.; Kimhi, O.; Tirosh, A.; Orr, N.; Kayouf, R.; Lishner, M. The effect of fermented yogurt on the prevention of diarrhea in a healthy adult population. Am. J. Infect. Control 2005, 33, 122–125. [Google Scholar] [CrossRef]
- Tiollier, E.; Chennaoui, M.; Gomez-Merino, D.; Drogou, C.; Filaire, E.; Guezennec, C.Y. Effect of a probiotics supplementation on respiratory infections and immune and hormonal parameters during intense military training. Mil. Med. 2007, 172, 1006–1011. [Google Scholar] [CrossRef] [Green Version]
- Cai, J.; Zhao, C.; Du, Y.; Zhang, Y.; Zhao, M.; Zhao, Q. Comparative efficacy and tolerability of probiotics for antibiotic-associated diarrhea: Systematic review with network meta-analysis. United Eur. Gastroenterol. J. 2018, 6, 169–180. [Google Scholar] [CrossRef]
- McFarland, L.V.; Evans, C.T.; Goldstein, E.J.C. Strain-specificity and disease-specificity of probiotic efficacy: A systematic review and meta-analysis. Front. Med. 2018, 5, 124. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, E.J.; Tyrrell, K.L.; Citron, D.M. Lactobacillus species: Taxonomic complexity and controversial susceptibilities. Clin. Infect. Dis. 2015, 60 (Suppl. 2), S98–S107. [Google Scholar] [CrossRef] [Green Version]
- Liévin-Le Moal, V.; Servin, A.L. Anti-infective activities of Lactobacillus strains in the human intestinal microbiota: From probiotics to gastrointestinal anti-infectious biotherapeutic agents. Clin. Microbiol. Rev. 2014, 27, 167–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budden, K.F.; Gellatly, S.L.; Wood, D.L.; Cooper, M.A.; Morrison, M.; Hugenholtz, P.; Hansbro, P.M. Emerging pathogenic links between microbiota and the gut-lung axis. Nat. Rev. Microbiol. 2017, 15, 55–63. [Google Scholar] [CrossRef] [PubMed]
- McAleer, J.P.; Kolls, J.K. Contributions of the intestinal microbiome in lung immunity. Eur. J. Immunol. 2018, 48, 39–49. [Google Scholar] [CrossRef]
- Enaud, R.; Prevel, R.; Ciarlo, E.; Beaufils, F.; Wieërs, G.; Guery, B.; Delhaes, L. The gut-lung axis in health and respiratory diseases: A place for inter-organ and inter-kingdom crosstalks. Front. Cell Infect. Microbiol. 2020, 10, 9. [Google Scholar] [CrossRef] [Green Version]
- Fagundes, C.T.; Amaral, F.A.; Vieira, A.T.; Soares, A.C.; Pinho, V.; Nicoli, J.R.; Vieira, L.Q.; Teixeira, M.M.; Souza, D.G. Transient TLR activation restores inflammatory response and ability to control pulmonary bacterial infection in germfree mice. J. Immunol. 2012, 188, 1411–1420. [Google Scholar] [CrossRef] [Green Version]
- Clarke, T.B. Early innate immunity to bacterial infection in the lung is regulated systemically by the commensal microbiota via nod-like receptor ligands. Infec.t Immun. 2014, 82, 4596–4606. [Google Scholar] [CrossRef] [Green Version]
- Okumura, R.; Takeda, K. Roles of intestinal epithelial cells in the maintenance of gut homeostasis. Exp. Mol. Med. 2017, 49, e338. [Google Scholar] [CrossRef] [Green Version]
- Peterson, L.W.; Artis, D. Intestinal epithelial cells: Regulators of barrier function and immune homeostasis. Nat. Rev. Immunol. 2014, 14, 141–153. [Google Scholar] [CrossRef]
- Soret, P.; Vandenborght, L.E.; Francis, F.; Coron, N.; Enaud, R.; Avalos, M.; Schaeverbeke, T.; Berger, P.; Fayon, M.; Thiebaut, R.; et al. Respiratory mycobiome and suggestion of inter-kingdom network during acute pulmonary exacerbation in cystic fibrosis. Sci. Rep. 2020, 10, 3589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandenborght, L.-E.; Enaud, R.; Coron, N.; Denning, D.W.; Delhaes, L. From culturomics to metagenomics: The mycobiome in chronic respiratory diseases. In The Lung Microbiome; European Respiratory Society: Norwich, UK, 2019; pp. 88–118. [Google Scholar] [CrossRef]
- Lawley, T.D.; Walker, A.W. Intestinal colonization resistance. Immunology 2013, 138, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ducarmon, Q.R.; Zwittink, R.D.; Hornung, B.V.H.; van Schaik, W.; Young, V.B.; Kuijper, E.J. Gut microbiota and colonization resistance against bacterial enteric infection. Microbiol. Mol. Biol. Rev. 2019, 83. [Google Scholar] [CrossRef]
- Djouzi, Z.; Andrieux, C.; Degivry, M.C.; Bouley, C.; Szylit, O. The association of yogurt starters with Lactobacillus casei DN 114.001 in fermented milk alters the composition and metabolism of intestinal microflora in germ-free rats and in human flora-associated rats. J. Nutr. 1997, 127, 2260–2266. [Google Scholar] [CrossRef] [PubMed]
- Klewicka, E.; Cukrowska, B.; Libudzisz, Z.; Slizewska, K.; Motyl, I. Changes in gut microbiota in children with atopic dermatitis administered the bacteria Lactobacillus casei DN--114001. Pol. J. Microbiol. 2011, 60, 329–333. [Google Scholar] [CrossRef]
- Rochet, V.; Rigottier-Gois, L.; Sutren, M.; Krementscki, M.N.; Andrieux, C.; Furet, J.P.; Tailliez, P.; Levenez, F.; Mogenet, A.; Bresson, J.L.; et al. Effects of orally administered Lactobacillus casei DN-114 001 on the composition or activities of the dominant faecal microbiota in healthy humans. Br. J. Nutr. 2006, 95, 421–429. [Google Scholar] [CrossRef] [Green Version]
- Fayol-Messaoudi, D.; Berger, C.N.; Coconnier-Polter, M.H.; Liévin-Le Moal, V.; Servin, A.L. pH-, Lactic acid-, and non-lactic acid-dependent activities of probiotic Lactobacilli against Salmonella enterica Serovar Typhimurium. Appl. Environ. Microbiol. 2005, 71, 6008–6013. [Google Scholar] [CrossRef] [Green Version]
- Parassol, N.; Freitas, M.; Thoreux, K.; Dalmasso, G.; Bourdet-Sicard, R.; Rampal, P. Lactobacillus casei DN-114 001 inhibits the increase in paracellular permeability of enteropathogenic Escherichia coli-infected T84 cells. Res. Microbiol. 2005, 156, 256–262. [Google Scholar] [CrossRef]
- Varyukhina, S.; Freitas, M.; Bardin, S.; Robillard, E.; Tavan, E.; Sapin, C.; Grill, J.P.; Trugnan, G. Glycan-modifying bacteria-derived soluble factors from Bacteroides thetaiotaomicron and Lactobacillus casei inhibit rotavirus infection in human intestinal cells. Microbes. Infect. 2012, 14, 273–278. [Google Scholar] [CrossRef]
- Thoreux, K.; Senegas-Balas, F.; Bernard-Perrone, F.; Giannarelli, S.; Denariaz, G.; Bouley, C.; Balas, D. Modulation of proliferation, second messenger levels, and morphotype expression of the rat intestinal epithelial cell line IEC-6 by fermented milk. J. Dairy Sci. 1996, 79, 33–43. [Google Scholar] [CrossRef]
- Thoreux, K.; Balas, D.; Bouley, C.; Senegas-Balas, F. Diet supplemented with yoghurt or milk fermented by Lactobacillus casei DN-114 001 stimulates growth and brush-border enzyme activities in mouse small intestine. Digestion 1998, 59, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Maldonado Galdeano, C.M.; de Leblanc Ade, M.; Carmuega, E.; Weill, R.; Perdigón, G. Mechanisms involved in the immunostimulation by probiotic fermented milk. J. Dairy Res. 2009, 76, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Baba, N.; Samson, S.; Bourdet-Sicard, R.; Rubio, M.; Sarfati, M. Commensal bacteria trigger a full dendritic cell maturation program that promotes the expansion of non-Tr1 suppressor T cells. J. Leukoc. Biol. 2008, 84, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Baba, N.; Samson, S.; Bourdet-Sicard, R.; Rubio, M.; Sarfati, M. Selected commensal-related bacteria and Toll-like receptor 3 agonist combinatorial codes synergistically induce interleukin-12 production by dendritic cells to trigger a T helper type 1 polarizing programme. Immunology 2009, 128, e523–e531. [Google Scholar] [CrossRef]
- De Moreno de LeBlanc, A.; Chaves, S.; Carmuega, E.; Weill, R.; Antóine, J.; Perdigón, G. Effect of long-term continuous consumption of fermented milk containing probiotic bacteria on mucosal immunity and the activity of peritoneal macrophages. Immunobiology 2008, 213, 97–108. [Google Scholar] [CrossRef]
- Vinderola, G.; Matar, C.; Perdigon, G. Role of intestinal epithelial cells in immune effects mediated by gram-positive probiotic bacteria: Involvement of Toll-like receptors. Clin. Diagn. Lab. Immunol. 2005, 12, 1075–1084. [Google Scholar] [CrossRef] [Green Version]
- Maldonado Galdeano, C.; Novotny Nuñez, I.; Carmuega, E.; de Moreno de LeBlanc, A.; Perdigón, G. Role of probiotics and functional foods in health: Gut immune stimulation by two probiotic strains and a potential probiotic yoghurt. Endocr. Metab. Immune Disord. Drug Targets 2015, 15, 37–45. [Google Scholar] [CrossRef]
- WHO. Influenza (Seasonal); Fact Sheet; World Health Organization (WHO): Geneva, Switzerland, 2018; Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (accessed on 21 March 2020).
- Maes, M.L.; Fixen, D.R.; Linnebur, S.A. Adverse effects of proton-pump inhibitor use in older adults: A review of the evidence. Ther. Adv. Drug Saf. 2017, 8, 273–297. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Element | Description |
|---|---|
| Population | Generally healthy children and adults aged 2 years and older |
| Intervention | FDD, defined as a fermented dairy drink containing Lacticaseibacillus paracasei subsp. paracasei CNCM I-1518 and the standard yogurt cultures (i.e., Lactobacillus bulgaricus and Streptococcus thermophilus) |
| Comparator | No placebo Placebo (e.g., non-fermented dairy product) |
| Outcome | Incidence, duration, or severity of common infectious diseases, including upper respiratory tract infections (e.g., rhinosinusitis, pharyngitis, laryngitis, acute otitis media), lower respiratory tract infections (e.g., acute bronchitis, bronchiolitis, pneumonia, tracheitis), and gastrointestinal tract infections (e.g., diarrhea) |
| Study design | Randomized, controlled trial |
| Reference | Study Design | Study Population | Interventions | Study Quality a | |||
|---|---|---|---|---|---|---|---|
| Sample Size Country of Conduct | Health Status at Baseline | Active | Control | Pattern of Consumption | |||
| Children (n = 2 Studies) | |||||||
| Merenstein et al. [24] | R, DB, PC, P Run-in: NR Intervention: 13 wk Follow-up: NR | ni = 638 (329 M, 309 F) nf = 636 (gender distribution NR) ITT = 638 PP = 564 b Mean age = 4.9 y U.S. | Healthy children, aged 3–6 y; vaccination status NR | 200 mL/day FDD (1 × 108 CFU/g Lacticaseibacillus paracasei subsp. paracasei CNCM I-1518; >1 × 107 CFU/g yogurt culturesc) | 200 mL/day non-fermented, acidified diary drink (assumed without standard yogurt cultures) | 200 mL once per day (time of day NR) | Poor |
| Prodeus et al. [2] | R, DB, PC, P Run-in: NR Intervention: 12 wk Follow-up: 4 wk | ni = 600 (325 M, 274 F, 1 NR) nf = 584 (gender distribution NR) ITT = 599 d PP = 578 e Mean age = 4 y Russia | Healthy children aged 3–6 y; 32% of subjects were vaccinated against influenza during the previous year | 200 g/day FDD (≥1 × 108 CFU/g L. paracasei subsp. paracasei CNCM I-1518; ≥1 × 107 CFU/g yogurt culturesc) | 200 g/day non-fermented, acidified dairy drink without Lactobacilli and Streptococcus thermophilus | 100 g twice per day (morning, afternoon) | Good |
| Adults (n = 3 Studies) | |||||||
| Guillemard et al. [39] | R, DB, PC, P Run-in: 2 wk Intervention: 12 wk Follow-up: 4 wk | ni = 1000 (435 M, 565 F) nf = 962 (gender distribution NR) ITT = 1000 PP = 900 f Mean age = 32.2 y Germany | Healthy adults; 6.2% of subjects were vaccinated against influenza at study inclusion | 200 g/day FDD (≥1 × 108 CFU/g L. paracasei subsp. paracasei CNCM I-1518; ≥1 × 107 CFU/g yogurt culturesc) | 200 g/day non-fermented, acidified dairy drink (assumed without standard yogurt cultures) | 100 g twice per day (breakfast, dinner) | Good |
| Pereg et al. [49] | R, SB, PC, P Run-in: NR Intervention: 8 wk (6 days/wk) Follow-up: NR | ni = 541 M nf = 502 M ITT = NA PP = 502 Mean age = 18.5 y Israel | Healthy adults residing in military camp; vaccination status NR | 100 mL/day FDD (1 × 108 CFU/mL L. paracasei subsp. paracasei CNCM I-1518; yogurt cultures and dose NR) | 100 mL/day non-probiotic yogurt without live bacteria | 100 mL once per day (time of day NR) | Poor |
| Tiollier et al. [50] | R, DB, PC, P Run-in: 3 wk Intervention: 4 wkg Follow-up: 1 wk | ni = nf = 47 M h ITT = PP = 47 h Mean age = 21 ± 0.4 y France | Adults in good mental and physical condition undergoing army training; vaccination status NR | 300 mL/day FDD (L. paracasei subsp. paracasei CNCM I-1518 dose NR; yogurt cultures and dose NR) | 300 mL/day non-fermented milk (assumed without standard yogurt cultures) | 100 mL three times per day (time of day NR) | Poor |
| Elderly (n = 4 Studies) | |||||||
| Boge et al. ([40], pilot and confirmatory studies) pilot study | R, DB, PC, P Run-in: 1 to 4 wk Intervention: 7 wk Follow-up: 18.5 wk | ni = 86 (30 M, 56 F) nf = 75 (gender distribution NR) ITT = 86 PP = NA Mean age = 83.6 y France | Healthy elderly aged ≥70 y residing in nursing homes; all subjects were vaccinated against influenza 4 wk after product consumption | 200 g/day FDD (L. paracasei subsp. paracasei CNCM I-1518 dose NR; yogurt culture dose NR c) | 200 g/day non-fermented acidified dairy drink (milk) | 100 g twice per day (time of day NR) | Fair |
| Boge et al. ([40], pilot and confirmatory studies) confirmatory study | R, DB, PC, P Run-in: 1 to 4 wk Intervention: 13 wk Follow-up: 12.5 wk | ni = 241 (74 M, 148 F, 19 NR) nf = 195 (gender distribution NR) ITT = 222 i PP = NA Mean age = 84.6 y France | Healthy elderly aged ≥70 y residing in nursing homes; all subjects were vaccinated against influenza 4 wk after product consumption | 200 g/day FDD (L. paracasei subsp. paracasei CNCM I-1518 dose NR; yogurt culture dose NR c) | 200 g/day non-fermented acidified dairy drink (milk) | 100 g twice per day (time of day NR) | Poor |
| Guillemard et al. [42] | R, DB, PC, P Run-in: 2 wk Intervention: 12 wk Follow-up: 4 wk | ni = 1072 (400 M, 672 F) nf = 1026 (gender distribution NR) ITT = 1072 PP = 864 j Median age = 76.0 y France | Healthy, free-living elderly aged ≥70 y; all subjects were vaccinated against influenza ≥14 days before study inclusion | 200 g/day FDD (≥1 × 108 CFU/g L. paracasei subsp. paracasei CNCM I-1518; ≥1 × 107 CFU/g yogurt cultures c) | 200 g/day non-fermented, acidified dairy drink (assumed without standard yogurt cultures) | 100 g twice per day (breakfast, dinner) | Good |
| Turchet et al. [41] | R, OL, C, P Run-in: NR Intervention: 3 wk Follow-up: NR | ni = 360 (119 M, 241 F) nf = 358 (gender distribution NR) ITT = 360 PP = NA Mean age = 68.2 y Italy | Healthy, free-living elderly aged >60 years; 82% of subjects were vaccinated against influenza 3 months before study | 200 mL/day FDD (1 × 108 CFU/mL L. paracasei subsp. paracasei CNCM I-1518; yogurt cultures and dose NR) | No product | 100 mL twice per day (time of day NR) | Poor |
| Additional Potential Confounders Considered in Scoring Criteria #6, #10, and #11 of the NIH Quality Appraisal Tool | Children | Adults | Elderly | Accounted For | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Merenstein et al. [24] | Prodeus et al. [2] | Guillemard et al. [39] | Pereg et al. [49] | Tiollier et al. [50] | Boge et al. ([40], Pilot and Confirmatory Studies) Pilot Study | Boge et al. ([40], Pilot and Confirmatory Studies) Confirmatory Study | Guillemard et al. [42] | Turchet et al. [41] | ||
| 6. Were the groups similar at baseline on important characteristics that could affect outcomes (e.g., demographics, risk factors, and co-morbid conditions)? a | Partially | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ | Partially b | 5/9 |
| (1) Presence of CIDs at baseline | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ | ✓ | 7/9 |
| (2) Influenza or rotavirus vaccination status at baseline | NR | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ | ✓ | 6/9 |
| (3) Medication/supplement use at baseline (e.g., proton pump inhibitors) | ✓ | ✓ | ✓ | NR | NR | ✓ | ✓ | ✓ | ✓ | 7/9 |
| 10. Were other interventions avoided or similar in the groups (e.g., similar background treatments)? c | ✓ | ✓ | ✓ | NR | Partially | Partially | Partially | ✓ | NR/No | 4/9 |
| (1) Use of rescue medications/supplements during study (e.g., for colds, flu, or diarrhea) | ✓ | ✓ | ✓ | NR | NR | NR | NR | ✓ | NR | 4/9 |
| (2) Consumption of other probiotics during study | ✓ | ✓ | ✓ | NR | ✓ | ✓ | ✓ | ✓ | No | 7/9 |
| 11. Were outcomes assessed using valid and reliable measures, implemented consistently across all study participants? d | Partially | ✓ | Partially | Partially | Partially | NR | NR | ✓ | Partially | 2/9 |
| (A) Incidence of CIDs | Partially | ✓ | ✓ | Partially | Partially | NR | NR | ✓ | ✓ | 4/9 |
| (1) Diagnosed by a physician/health professional | No | ✓ | ✓ | No | No | NR | NR | ✓ | ✓ | 4/9 |
| (2) If not diagnosed, type of symptoms listed (e.g., sneezing or runny nose) | ✓ | NA | NA | ✓ | ✓ | NR | NR | NA | NA | 3/5 |
| (3) If not diagnosed, number and duration of symptoms used to define a CID episode (e.g., must have at least two symptoms within two consecutive days) | NR | NA | NA | NR | ✓ | NR | NR | NA | NA | 1/5 |
| (B) Duration of CIDs: how duration was determined (e.g., first to the last day of symptoms) | Not assessed | ✓ | NR | NR | NR | NR | NR | ✓ | NR | 2/8 |
| (C) Severity of CIDs: how severity was determined (e.g., scoring system: mild, moderate, or severe) | Not assessed | ✓ | ✓ | Not assessed | ✓ | NR | NR | ✓ | NR | 4/7 |
| Outcome/Metric Assessed | Children | Adults | Elderly | Number of Studies in which Metric was Assessed | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Merenstein et al. [24] | Prodeus et al. [2] | Guillemard et al. [39] | Pereg et al. [49] | Tiollier et al. [50] | Boge et al. ([40], Pilot and Confirmatory Studies) Pilot Study | Boge et al. ([40], Pilot and Confirmatory Studies) Confirmatory Study | Guillemard et al. [42] | Turchet et al. [41] | ||
| Incidence | ||||||||||
| Relative risk | ✓ | ✓ | ✓ | ✓ | 4 a | |||||
| Mean CIDs per subject | ✓ | ✓ b | 2 a | |||||||
| Subjects with ≥1 CID | ✓ | ✓ | ✓ c | 3 a | ||||||
| Subjects with diarrhea | ✓ | 1 | ||||||||
| Subjects who vomited amongst subjects with diarrhea | ✓ | 1 | ||||||||
| Subjects with abdominal pain amongst subjects with diarrhea | ✓ | 1 | ||||||||
| "Mean maximal number of watery stools/day" | ✓ | 1 | ||||||||
| Duration | ||||||||||
| Mean cumulative days of CIDs amongst subjects with CIDs | ✓ | ✓ | ✓ d | 3 a | ||||||
| Mean cumulative days of CIDs amongst all subjects | ✓ | 1 | ||||||||
| Mean days per CID episode amongst subjects with CIDs | ✓ | ✓ | ✓ | 3 a | ||||||
| “Mean duration of diarrhea (days)” | ✓ | 1 | ||||||||
| Severity | ||||||||||
| Cumulative number of CIDs categorized as “mild” | ✓ | 1 | ||||||||
| Cumulative number of CIDs categorized as “moderate” | ✓ | 1 | ||||||||
| “Severity of CID” | ✓ e | 1 | ||||||||
| Cumulative number of CIDs categorized as “severe” amongst subjects with CIDs | ✓ | ✓ | 2 a | |||||||
| "Severity of symptoms (mild, moderate, severe)" | ✓ e | 1 | ||||||||
| "Severity of CID or influenza illnesses" | ✓e | ✓ e | 2 | |||||||
| "Intensity" | ✓e | 1 | ||||||||
| Analysis | Metric | Studies | Study Quality | Meta-Analysis Results | Heterogeneity | Publication Bias | ||
|---|---|---|---|---|---|---|---|---|
| Combined Effect (95% CI) | P-Value | I2 | p-Value | |||||
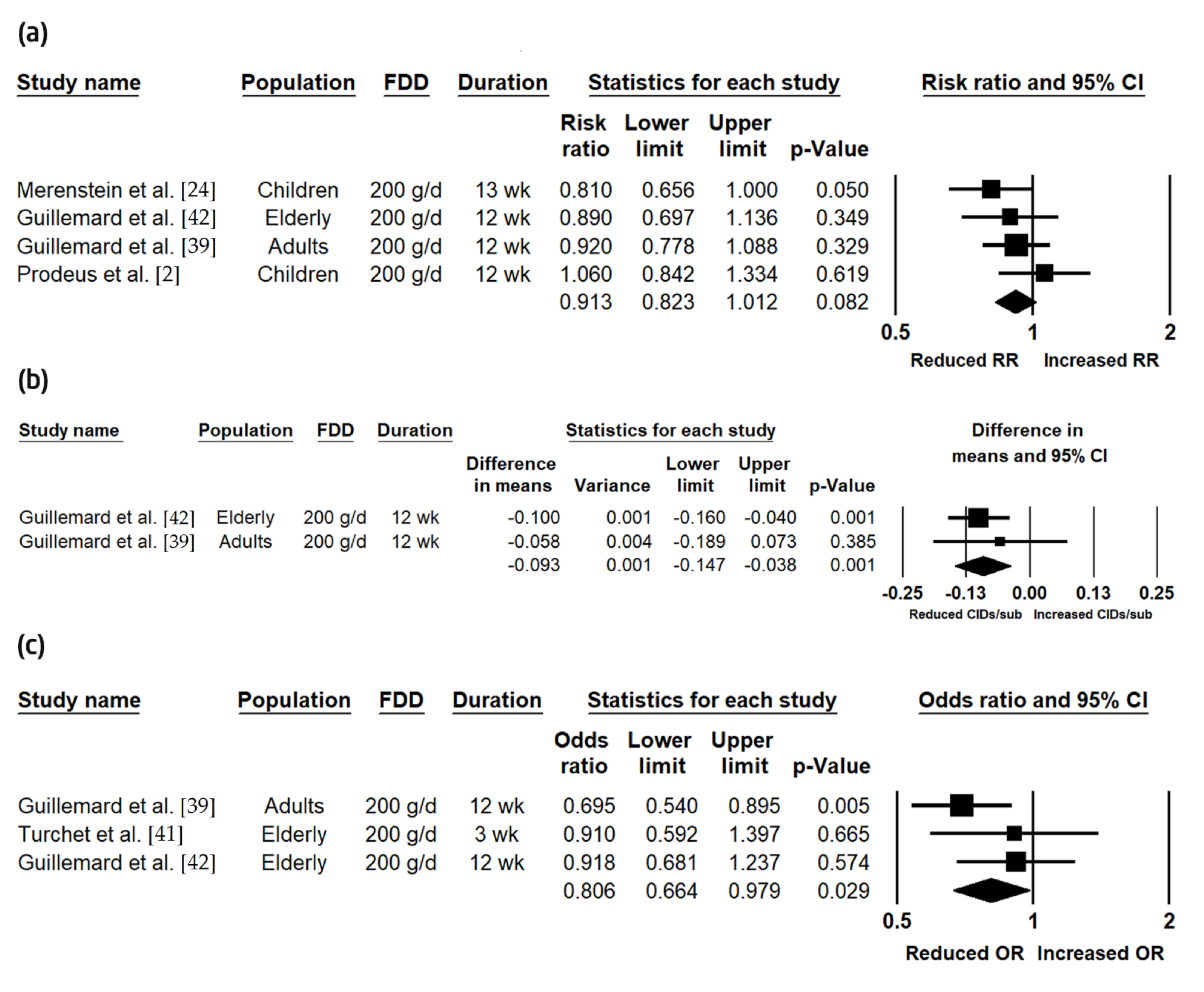
| Incidence | RR | n = 4 (n = 2 children; n = 1 adults; n = 1 elderly) | n = 3 good n = 1 poor | RR = 0.91 (0.82, 1.01) | 0.082 | 0.00 | 0.405 | No |
| Mean number of CIDs per subject | n = 2 (n = 1 adults; n = 1 elderly) | n = 2 good | −0.09 (−0.15, −0.04) | 0.001 | 0.00 | 0.567 | Insufficient data | |
| Subjects with ≥1 CID | n = 3 (n = 1 adults; n = 2 elderly) | n = 2 good n = 1 poor | OR = 0.81 (0.66, 0.98) | 0.029 | 14.84 | 0.309 | No | |
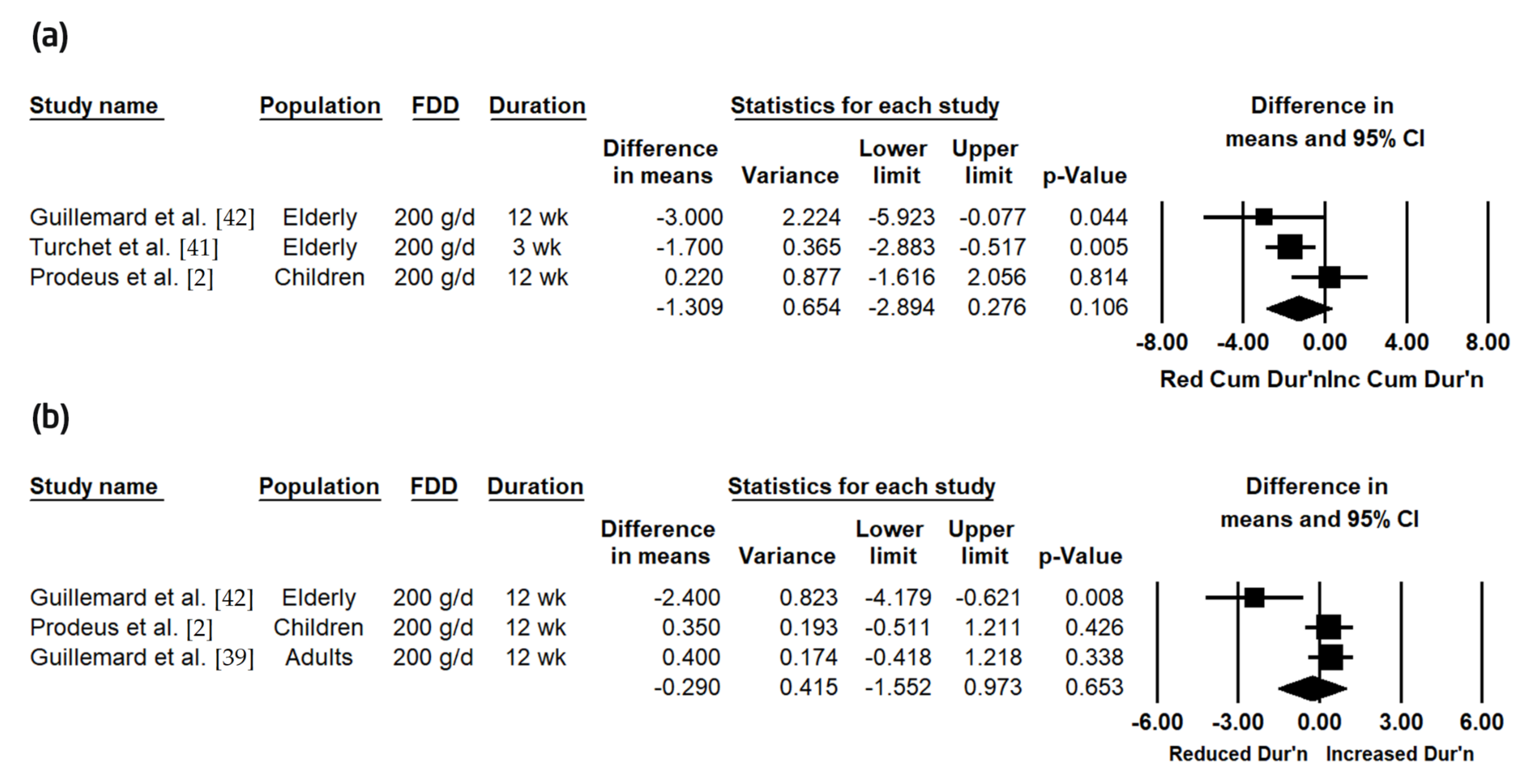
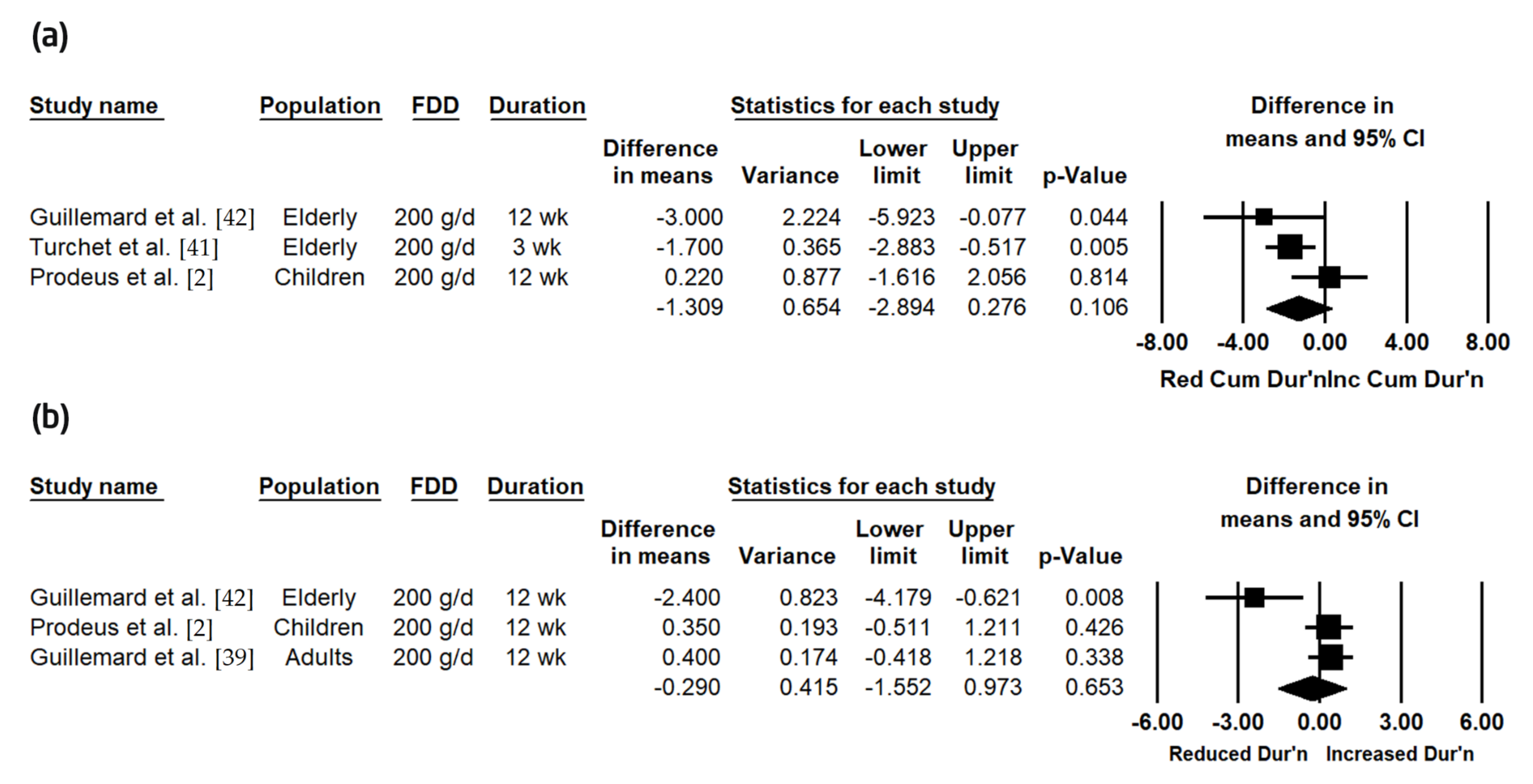
| Duration | Mean cumulative days of CIDs amongst subjects with CIDs | n = 3 (n = 1 children; n = 2 elderly) | n = 2 good n = 1 poor | −1.31 (−2.89, 0.28) | 0.106 | 55.85 | 0.079 | Yes a |
| Mean days per CID episode amongst subjects with CIDs | n = 3 (n = 1 children; n = 1 adults; n = 1 elderly) | n = 3 good | −0.29 (−1.55, 0.97) | 0.653 | 76.28 | 0.015 | No | |
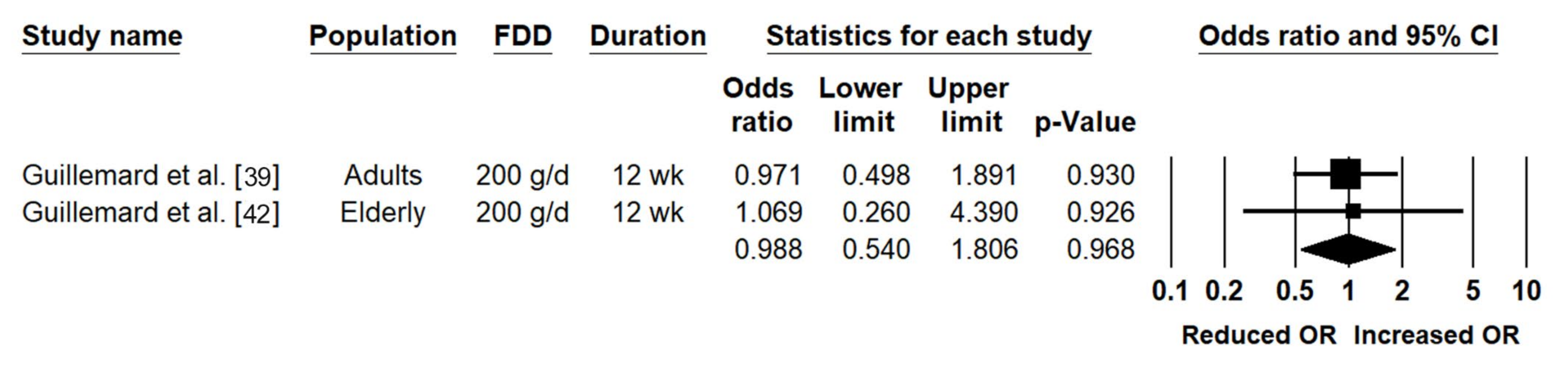
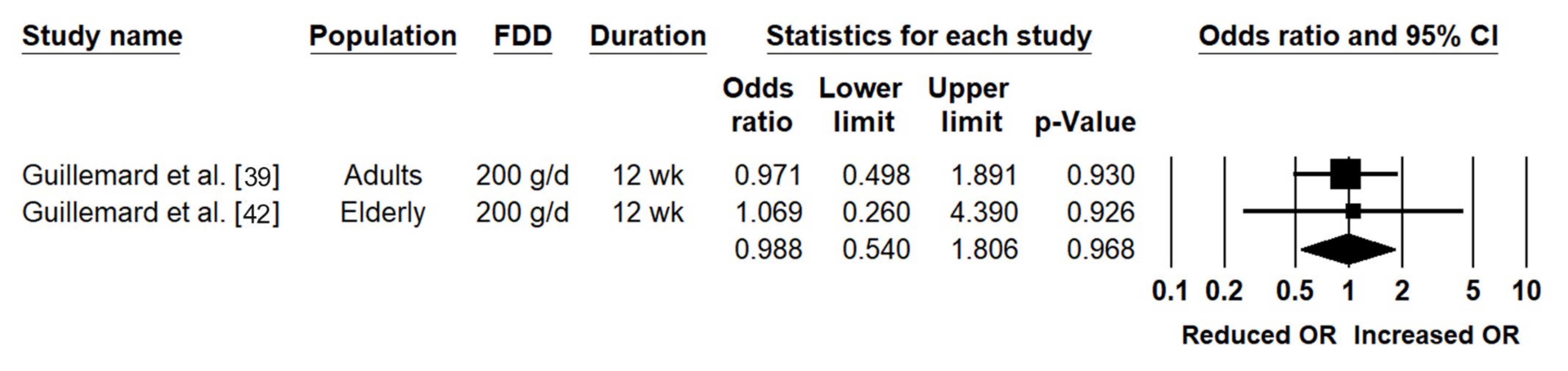
| Severity | Cumulative number of CIDs categorized as “severe” amongst subjects with CIDs | n = 2 (n = 1 adults; n = 1 elderly) | n = 2 good | OR = 0.99 (0.54, 1.81) | 0.968 | 0.00 | 0.903 | Insufficient data |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poon, T.; Juana, J.; Noori, D.; Jeansen, S.; Pierucci-Lagha, A.; Musa-Veloso, K. Effects of a Fermented Dairy Drink Containing Lacticaseibacillus paracasei subsp. paracasei CNCM I-1518 (Lactobacillus casei CNCM I-1518) and the Standard Yogurt Cultures on the Incidence, Duration, and Severity of Common Infectious Diseases: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2020, 12, 3443. https://doi.org/10.3390/nu12113443
Poon T, Juana J, Noori D, Jeansen S, Pierucci-Lagha A, Musa-Veloso K. Effects of a Fermented Dairy Drink Containing Lacticaseibacillus paracasei subsp. paracasei CNCM I-1518 (Lactobacillus casei CNCM I-1518) and the Standard Yogurt Cultures on the Incidence, Duration, and Severity of Common Infectious Diseases: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2020; 12(11):3443. https://doi.org/10.3390/nu12113443
Chicago/Turabian StylePoon, Theresa, Justine Juana, Daniel Noori, Stephanie Jeansen, Amira Pierucci-Lagha, and Kathy Musa-Veloso. 2020. "Effects of a Fermented Dairy Drink Containing Lacticaseibacillus paracasei subsp. paracasei CNCM I-1518 (Lactobacillus casei CNCM I-1518) and the Standard Yogurt Cultures on the Incidence, Duration, and Severity of Common Infectious Diseases: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Nutrients 12, no. 11: 3443. https://doi.org/10.3390/nu12113443