The Effects on Immune Function and Digestive Health of Consuming the Skin and Flesh of Zespri® SunGold Kiwifruit (Actinidia Chinensis var. Chinensis ‘Zesy002’) in Healthy and IBS-Constipated Individuals

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
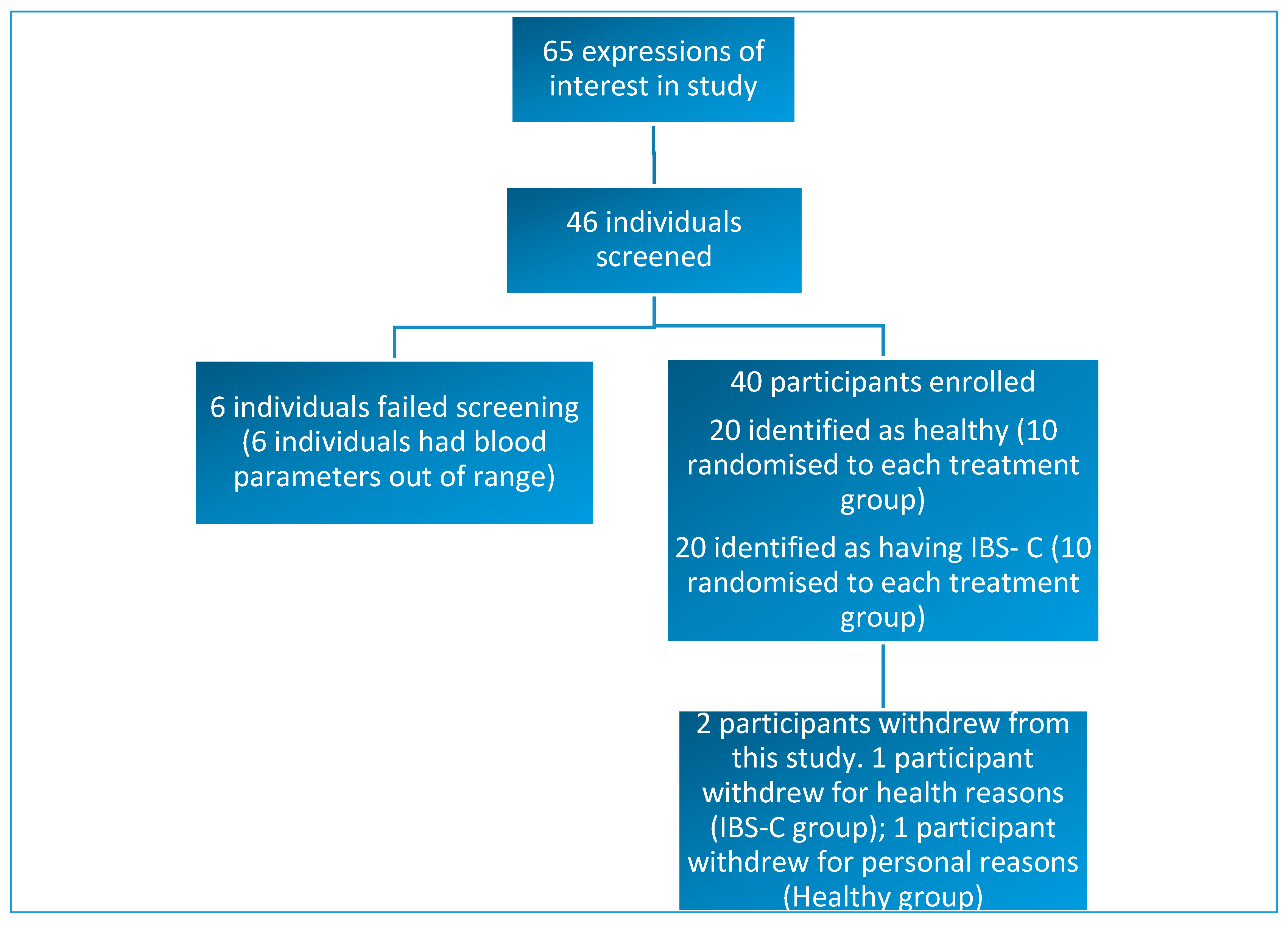
3.1. Participants
3.2. Primary Outcome
3.3. Secondary Outcomes
3.3.1. Stool Frequency and Consistency
3.3.2. Gastrointestinal Symptoms (GSRS)
3.3.3. Gastrointestinal Symptoms Birmingham IBS Questionnaire
3.3.4. Dietary Intake
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rush, E.C.; Patel, M.; Plank, L.D.; Ferguson, L.R. Kiwifruit promotes laxation in the elderly. Asia Pac. J. Clin. Nutr. 2002, 11, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Harvie, R.; Walmsley, R.; Schultz, M.; New Zealand Soc, G. “We are what our bacteria eat“: The role of bacteria in personalizing nutrition therapy in gastrointestinal conditions. J. Gastroenterol. Hepatol. 2017, 32, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Barbara, G.; Cremon, C.; Carini, G.; Bellacosa, L.; Zecchi, L.; De Giorgio, R.; Corinaldesi, R.; Stanghellini, V. The Immune System in Irritable Bowel Syndrome. J. Neurogastroenterol. Motil. 2011, 17, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Barbara, G.; De Giorgio, R.; Stanghellini, V.; Cremon, C.; Corinaldesi, R. A role for inflammation in irritable bowel syndrome? Gut 2002, 51, I41–I44. [Google Scholar] [CrossRef] [PubMed]
- Gonsalkorale, W.M.; Perrey, C.; Pravica, V.; Whorwell, P.J.; Hutchinson, I.V. Interleukin 10 genotypes in irritable bowel syndrome: Evidence for an inflammatory component? Gut 2003, 52, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Ohman, L.; Simren, M. Pathogenesis of IBs: Role of inflammation, immunity and neuroimmune interactions. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 163–173. [Google Scholar] [CrossRef]
- Seyedmirzaee, S.; Hayatbakhsh, M.M.; Ahmadi, B.; Baniasadi, N.; Bagheri Rafsanjani, A.M.; Nikpoor, A.R.; Mohammadi, M. Serum immune biomarkers in irritable bowel syndrome. Clin. Res. Hepatol. Gastroenterol. 2016, 40, 631–637. [Google Scholar] [CrossRef]
- Ford, A.C.; Talley, N.J. Mucosal inflammation as a potential etiological factor in irritable bowel syndrome: A systematic review. J. Gastroenterol. 2011, 46, 421–431. [Google Scholar] [CrossRef]
- Bashashati, M.; Rezaei, N.; Shafieyoun, A.; McKernan, D.P.; Chang, L.; Ohman, L. Cytokine imbalance in irritable bowel syndrome: A systematic review and meta-analysis. Neurogastroenterol. Motil. 2014, 26, 1036–1048. [Google Scholar] [CrossRef]
- Ringel, Y.; Maharshak, N. Intestinal microbiota and immune function in the pathogenesis of irritable bowel syndrome. Am. J. Physiol. Gastroint. Liver Physiol. 2013, 305, G529–G541. [Google Scholar] [CrossRef]
- Wilson, B.; Rossi, M.; Dimidi, E.; Whelan, K. Prebiotics in irritable bowel syndrome and other functional bowel disorders in adults: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2019, 109, 1098–1111. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.; Whelan, K. Prebiotic inulin-type fructans and galacto-oligosaccharides: Definition, specificity, function, and application in gastrointestinal disorders. J. Gastroenterol. Hepatol. 2017, 32, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Gearry, R.; Barbara, G.; Fukudo, S.; Ansell, J.; Eady, S.L.; Wallace, A.; Butts, C.A.; Dinnan, H.; Kuhn-Sherlock, B.; Drummond, L. The effect of ZespriTM green kiwifruit on constipation and abdominal discomfort: A controlled randomized cross-over intervention study. Gastroenterology 2017, 152, S917. [Google Scholar] [CrossRef]
- Eady, S.L.; Wallace, A.J.; Butts, C.A.; Hedderley, D.; Drummond, L.; Ansell, J.; Gearry, R.B. The effect of ‘Zesy002’ kiwifruit (Actinidia chinensis var. chinensis) on gut health function: A randomised cross-over clinical trial. J. Nutr. Sci. 2019, 8, 11. [Google Scholar] [CrossRef]
- Motohashi, N.; Shirataki, Y.; Kawase, M.; Tani, S.; Sakagami, H.; Satoh, K.; Kurihara, T.; Nakashima, H.; Wolfard, K.; Miskolci, C.; et al. Biological activity of kiwifruit peel extracts. Phytother. Res. 2001, 15, 337–343. [Google Scholar] [CrossRef]
- Pinelli, P.; Romani, A.; Fierini, E.; Remorini, D.; Agati, G. Characterisation of the polyphenol content in the kiwifruit (Actinidia deliciosa) exocarp for the calibration of a fruit-sorting optical sensor. Phytochem. Anal. 2013, 24, 460–466. [Google Scholar] [CrossRef]
- Rome, F. Guidelines—Rome III Diagnostic Criteria for Functional Gastrointestinal Disorders. J. Gastrointest. Liver Dis. JGLD 2006, 15, 307–312. [Google Scholar]
- Roalfe, A.K.; Roberts, L.M.; Wilson, S. Evaluation of the Birmingham IBS symptom questionnaire. BMC Gastroenterol. 2008, 8, 30. [Google Scholar] [CrossRef]
- Svedlund, J.; Sjödin, I.; Dotevall, G. GSRS—A clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef]
- Mateo, T.; Naim Abu Nabah, Y.; Losada, M.; Estellés, R.; Company, C.; Bedrina, B.; Cerdá-Nicolás, J.M.; Poole, S.; Jose, P.J.; Cortijo, J.; et al. A critical role for TNFα in the selective attachment of mononuclear leukocytes to angiotensin-II-stimulated arterioles. Blood 2007, 110, 1895–1902. [Google Scholar] [CrossRef]
- Scrivo, R.; Vasile, M.; Bartosiewicz, I.; Valesini, G. Inflammation as “common soil” of the multifactorial diseases. Autoimmun. Rev. 2011, 10, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, A. Obesity, metalic syndrome, and type 2 diabetes: Inflammatory basis of glucose metabolic disorders. Nutr. Rev. 2007, 65, S152–S156. [Google Scholar] [CrossRef]
- Pickup, J.C. Inflammation and Activated Innate Immunity in the Pathogenesis of Type 2 Diabetes. Diabetes Care 2004, 27, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Shukla, R.; Ranjan, P.; Kumar, A. Interleukin-10: A Compelling Therapeutic Target in Patients with Irritable Bowel Syndrome. Clin. Ther. 2017, 39, 632–643. [Google Scholar] [CrossRef] [PubMed]
- Clarke, G.; Quigley, E.M.M.; Cryan, J.F.; Dinan, T.G. Irritable bowel syndrome: Towards biomarker identification. Trends Mol. Med. 2009, 15, 478–489. [Google Scholar] [CrossRef] [PubMed]
- Dinan, T.G.; Quigley, E.M.M.; Ahmed, S.M.M.; Scully, P.; O’Brien, S.; O’Mahony, L.; O’Mahony, S.; Shanahan, F.; Keeling, P.W.N. Hypothalamic-Pituitary-Gut Axis Dysregulation in Irritable Bowel Syndrome: Plasma Cytokines as a Potential Biomarker? Gastroenterology 2006, 130, 304–311. [Google Scholar] [CrossRef]
- Liebregts, T.; Adam, B.; Bredack, C.; Roth, A.; Heinzel, S.; Lester, S.; Downie-Doyle, S.; Smith, E.; Drew, P.; Talley, N.J.; et al. Immune activation in patients with irritable bowel syndrome. Gastroenterology 2007, 132, 913–920. [Google Scholar] [CrossRef]
- Skinner, M.A.; Bentley-Hewitt, K.; Rosendale, D.; Naoko, S.; Pernthaner, A. Effects of kiwifruit on innate and adaptive immunity and symptoms of upper respiratory tract infections. Adv. Food Nutr. Res. 2013, 68, 301–320. [Google Scholar]
- Richardson, D.P.; Ansell, J.; Drummond, L.N. The nutritional and health attributes of kiwifruit: A review. Eur. J. Nutr. 2018, 57, 2659–2676. [Google Scholar] [CrossRef]
- Johanson, J.F.; Wald, A.; Tougas, G.; Chey, W.D.; Novick, J.S.; Lembo, A.J.; Fordham, F.; Guella, M.; Nault, B. Effect of Tegaserod in Chronic Constipation: A Randomized, Double-Blind, Controlled Trial. Clin. Gastroenterol. Hepatol. 2004, 2, 796–805. [Google Scholar] [CrossRef]
- Perveen, I.; Parvin, R.; Saha, M.; Bari, M.S.; Uddoula, M.S.; Ghosh, M.K. Bowel habit and perception about bowel habit pattern of medical students. J. Gastrointest. Dig. Syst. 2016, 6, 2. [Google Scholar] [CrossRef]
- Verspreet, J.; Damen, B.; Broekaert, W.F.; Verbeke, K.; Delcour, J.A.; Courtin, C.M. A Critical Look at Prebiotics within the Dietary Fiber Concept. In Annual Review of Food Science and Technology; Doyle, M.P., Klaenhammer, T.R., Eds.; Annual Reviews; Palo Alto: Santa Clara, CA, USA, 2016; Volume 7, pp. 167–190. [Google Scholar]
- National Health and Medical Research Council Australia; Ministry of Health New Zealand. Nutrient Reference Values for Australia and New Zealand Including Recommended Dietary Intakes; National Health and Medical Research Council: Canberra, Austrilia, 2006.
- El-Salhy, M.; Ystad, S.O.; Mazzawi, T.; Gundersen, D. Dietary fiber in irritable bowel syndrome. Int. J. Mol. Med. 2017, 40, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Dimidi, E.; Christodoulides, S.; Fragkos, K.C.; Scott, S.M.; Whelan, K. The effect of probiotics on functional constipation in adults: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2014, 100, 1075–1084. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Energy and Activity Guidelines for New Zealand Adults; Ministry of Health: Wellington, DC, USA, 2015.
- Thompson, F.E.; Subar, A.F.; Loria, C.M.; Reedy, J.L.; Baranowski, T. Need for Technological Innovation in Dietary Assessment. J. Am. Diet. Assoc. 2010, 110, 48–51. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Recurrent Abdominal Pain on Average at Least 1 Day/Week in the Last 3 Months, Associated with Two or More of the Following Criteria: |
|---|
| 1. Related to defecation |
| 2. Associated with a change in the frequency of stool |
| 3. Associated with a change in the form (appearance) of stool |
| Baseline Characteristics | Total Number |
|---|---|
| Number of study participants | 38 |
| Male | 11 |
| Female | 27 |
| Ethnicity | |
| New Zealand European | 32 |
| Māori | 1 |
| Israeli | 1 |
| South American | 2 |
| Russian | 2 |
| Age (years) 1 | 44 (22–65) |
| Weight (kg) 1 | 71 (52–109) |
| BMI 1 | 25 (19–34) |
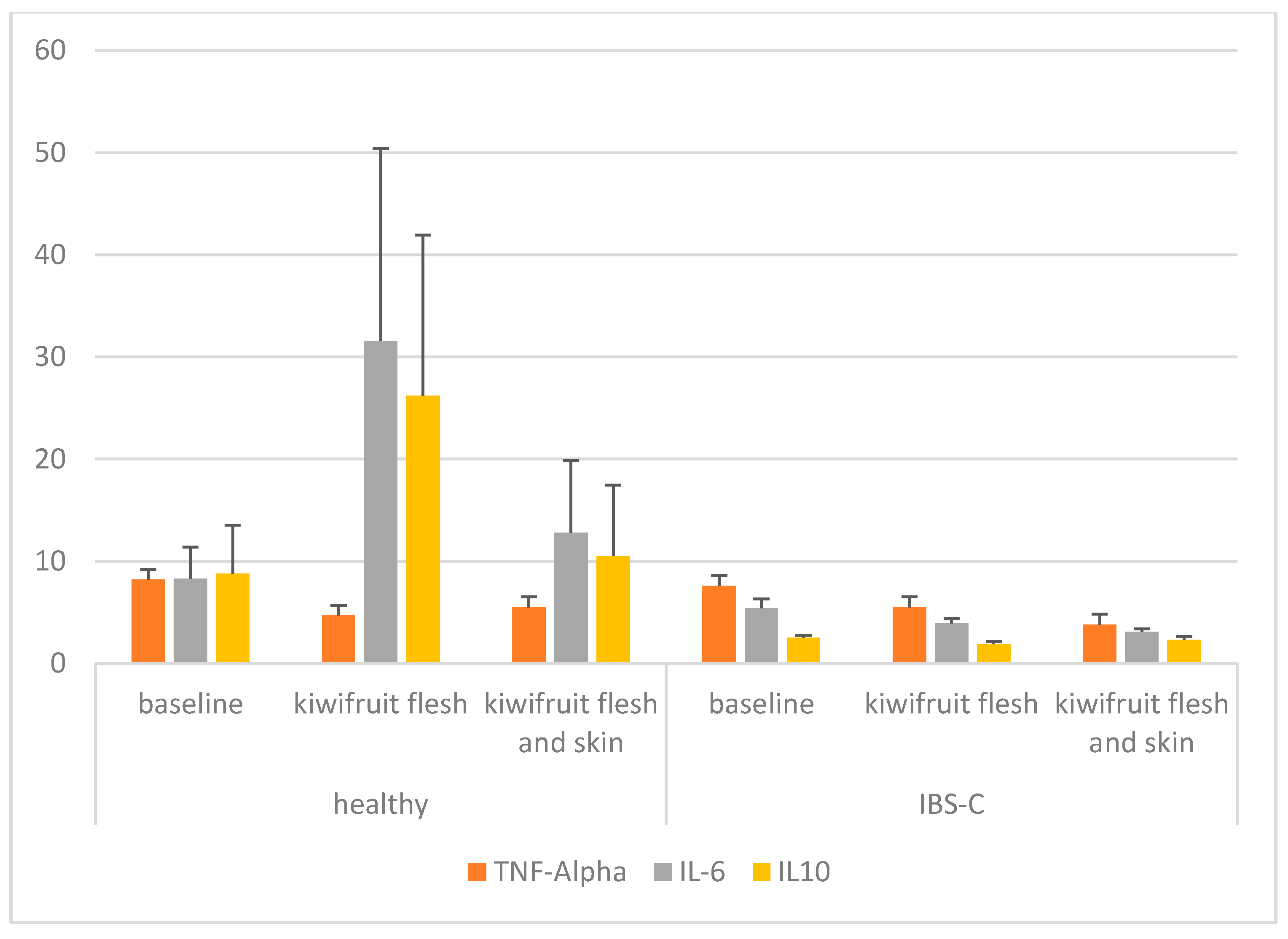
| Participant Group | Trial Phase | TNF-α | IL-6 | IL-10 |
|---|---|---|---|---|
| Healthy | Baseline | 8.2 (3.0) | 8.3 (13.4) | 8.8 (20.7) |
| Kiwifruit flesh | 4.7 * (1.6) | 31.6 (82.0) | 26.2 (68.5) | |
| Kiwifruit flesh and skin | 5.5 * (3.8) | 12.8 (30.8) | 10.5 (30.4) | |
| IBS-C | Baseline | 7.6 (2.9) | 5.4 (3.9) | 2.5 (1.1) |
| Kiwifruit flesh | 5.5 (4.0) | 3.9 (2.3) | 1.9 ^ (1.1) | |
| Kiwifruit flesh and skin | 3.8 * (1.5) | 3.1 (1.2) | 2.3 (1.5) | |
| p Values | ||||
| Treatment | <0.001 | 0.141 | 0.083 | |
| Group | 0.476 | 0.065 | 0.302 | |
| Treatment × Group | 0.083 | 0.003 | 0.370 |
| Participant Group | Trial Phase | No. of CSBMs Per Week | No. of BMs Per Week | No. of CBMs Per Week | No. of SBMs Per Week | No. of Strained BMs Per Week | Bristol Stool Scale |
|---|---|---|---|---|---|---|---|
| Healthy | Baseline | 7.6 (5.4) | 10.5 (5.2) | 9.7 (5.6) | 8.3 (5.2) | 1.1 (1.5) | 3.3 (0.7) |
| Kiwifruit flesh | 7.8 (5.1) | 10.1 (5.3) | 9.7 (5.6) | 8.1 (5.0) | 0.6 (1.0) | 4.0 * (1.0) | |
| Kiwifruit flesh and skin | 9.8 (5.7) | 11.4 (5.7) | 11.1 (6.0) | 10.1 (5.4) | 0.1 (0.3) | 3.9 * (0.7) | |
| IBS-C | Baseline | 6.7 (4.8) | 9.5 (5.6) | 6.7 (4.8) | 9.4 (5.6) | 2.8 (2.9) | 3.5 (1.0) |
| Kiwifruit flesh | 8.4 (7.0) | 11.0 (7.5) | 8.7 (6.9) | 10.7 (7.7) | 2.3 (2.7) | 3.9 (1.0) | |
| Kiwifruit flesh and skin | 9.2 * (5.8) | 11.4 (6.2) | 8.7 (6.9) | 11.3 (6.1) | 1.9 (2.5) | 3.8 (1.1) | |
| p Values | |||||||
| Treatment | <0.001 | 0.020 | <0.001 | 0.009 | 0.007 | <0.001 | |
| Group | 0.871 | 0.995 | 0.303 | 0.377 | 0.004 | 0.953 | |
| Treatment × Group | 0.405 | 0.174 | 0.151 | 0.422 | 0.972 | 0.390 |
| Participant Group | Trial Phase | Diarrhoea | Indigestion | Constipation | Abdominal Pain | Reflux |
|---|---|---|---|---|---|---|
| Healthy | Baseline | 1.10 (0.13) | 1.37 (0.34) | 1.29 (0.35) | 1.25 (0.24) | 1.13 (0.23) |
| Kiwifruit flesh | 1.04 (0.11) | 1.36 (0.41) | 1.21 (0.37) | 1.11 (0.19) | 1.13 (0.23) | |
| Kiwifruit flesh and skin | 1.21 (0.47) | 1.43 (0.49) | 1.05 (0.12) | 1.28 (0.39) | 1.16 (0.34) | |
| IBS-C | Baseline | 1.94 ^ (1.09) | 2.48 ^ (1.11) | 2.67 ^ (1.11) | 2.05 ^ (0.89) | 1.55 (0.91) |
| Kiwifruit flesh | 2.09 ^ (1.55) | 2.10 (1.26) | 1.73 * (0.95) | 1.67 (0.95) | 1.34 (0.57) | |
| Kiwifruit flesh and skin | 2.15 ^ (1.59) | 2.44 ^ (1.28) | 2.04 * ^ (1.15) | 2.02 ^ (1.12) | 1.56 (0.91) | |
| p Values | ||||||
| Treatment | 0.342 | 0.149 | 0.004 | 0.036 | 0.584 | |
| Group | <0.001 | 0.001 | <0.001 | 0.002 | 0.023 | |
| Treatment × Group | 0.788 | 0.241 | 0.018 | 0.528 | 0.623 |
| Participant Group | Trial Phase | Constipation | Diarrhoea | Pain |
|---|---|---|---|---|
| Healthy | Baseline | 0.44 (0.40) | 0.19 (0.20) | 0.37 (0.32) |
| Kiwifruit flesh | 0.35 (0.46) | 0.22 (0.33) | 0.30 (0.41) | |
| Kiwifruit flesh and skin | 0.22 (0.34) | 0.23 (0.27) | 0.22 (0.30) | |
| IBS-C | Baseline | 1.82 ^ (1.37) | 0.84 ^ (0.73) | 0.89 (0.81) |
| Kiwifruit flesh | 1.62 ^ (0.99) | 0.61 (0.53) | 0.63 (0.64) | |
| Kiwifruit flesh and skin | 1.22 ^ (1.16) | 0.51 (0.47) | 0.42 * (0.54) | |
| p Values | ||||
| Treatment | 0.014 | 0.376 | 0.004 | |
| Group | <0.001 | 0.001 | 0.030 | |
| Treatment × Group | 0.626 | 0.105 | 0.361 |
| Question | Response | N 1 (%) |
|---|---|---|
| How would you describe your appetite? | Good Fair Poor | 35 (92) 2 (5.5) 1 (2.6) |
| How diverse is your diet? | Different every day Different only sometimes during the week Different only during weekend days Very monotonous | 16 (42) 13 (34.2) 3 (7.9) 6 (15.8) |
| Nutrient | Baseline | Kiwifruit Flesh Only | Kiwifruit and Skin | p Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Healthy | IBS | Healthy | IBS | Healthy | IBS | Treatment | Group | Treatment × Group | |
| Total energy (kJ) | 8083 (2693) | 7258 (1858) | 7159 (2541) | 7877 (2885) | 6963 (2211) | 6829 (2255) | 0.078 | 0.911 | 0.105 |
| Protein (g) | 92 (50) | 72 (25) | 82 (30) | 75 (29) | 80 (19) | 65 (25) | 0.333 | 0.090 | 0.530 |
| Total fat (g) | 81 (35) | 73 (23) | 70 (29) | 71 (32) | 67 (24) | 69 (35) | 0.062 | 0.853 | 0.396 |
| Saturated fatty acids (g) | 32 (12) | 25 (10) | 27 (10) | 28 (12) | 24 * (11) | 28 (15) | 0.362 | 0.819 | 0.007 |
| Polyunsaturated fatty acids (g) | 12 (11) | 13 (6) | 10 (8) | 13 (7) | 10 (6) | 9 (6) | 0.013 | 0.662 | 0.122 |
| Monounsaturated fatty acids (g) | 28 (13) | 28 (11) | 23 (11) | 28 (14) | 25 (9) | 24 (15) | 0.091 | 0.806 | 0.187 |
| Available carbohydrate (g) | 188 (59) | 172 (56) | 170 (67) | 193 (106) | 169 (78) | 161 (65) | 0.269 | 0.979 | 0.192 |
| Sugar (g) | 76 (33) | 77 (23) | 67 (44) | 75 (32) | 63 (38) | 70 (29) | 0.080 | 0.622 | 0.667 |
| Dietary fibre (g) | 23 (16) | 23 (5) | 20 (13) | 24 (9) | 17 (7) | 19 (7) | 0.004 | 0.486 | 0.427 |
| Vitamin C (mg) | 67 (79) | 80 (28) | 63 (51) | 74 (41) | 97 (79) | 73 (47) | 0.474 | 0.991 | 0.329 |
| Sodium (mg) | 2596 (1076) | 2163 (1020) | 2249 (962) | 2038 (878) | 2029 (1117) | 1933 (689) | 0.139 | 0.327 | 0.674 |
| Potassium (mg) | 3032 (1300) | 3159 (632) | 2373 (977) | 3074 (768) | 2546 (744) | 2642 (918) | 0.005 | 0.235 | 0.096 |
| Magnesium (mg) | 332 (160) | 328 (106) | 247 * (123) | 349 (140) | 256 * (95) | 292 (144) | 0.002 | 0.277 | 0.004 |
| Iron (mg) | 12 (6) | 12 (4) | 10 (4) | 12 (5) | 11 (4) | 10 (4) | 0.188 | 0.744 | 0.157 |
| Calcium (mg) | 752 (352) | 798 (382) | 700 (298) | 781 (326) | 651 (291) | 701 (365) | 0.202 | 0.534 | 0.939 |
| Nutrient | Baseline | Kiwifruit Flesh Only | Kiwifruit and Skin | p Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Healthy | IBS | Healthy | IBS | Healthy | IBS | Treatment | Group | Treatment × Group | |
| Total energy (kJ) | 8083 (2693) | 7258 (1858) | 7758 (2551) | 8444 (2873) | 7543 (2229) | 7432 (2256) | 0.237 | 0.907 | 0.116 |
| Protein (g) | 92 (50) | 72 (25) | 84 (31) | 78 (29) | 83 (19) | 68 (25) | 0.505 | 0.090 | 0.539 |
| Total fat (g) | 81 (35) | 73 (23) | 71 (29) | 78 (29) | 68 (24) | 70 (35) | 0.073 | 0.975 | 0.132 |
| Saturated fatty acids (g) | 32 (12) | 25 (10) | 27 (10) | 28 (12) | 24 * (11) | 28 (15) | 0.405 | 0.822 | 0.007 |
| Polyunsaturated fatty acids (g) | 12 (11) | 13 (6) | 10 (8) | 13 (7) | 10 (6) | 10 (6) | 0.026 | 0.670 | 0.124 |
| Monounsaturated fatty acids (g) | 28 (13) | 28 (11) | 23 (11) | 28 (14) | 25 (9) | 24 (14) | 0.098 | 0.807 | 0.180 |
| Available carbohydrate (g) | 188 (59) | 172 (56) | 200 (67) | 221 * (106) | 198 (78) | 190 (65) | 0.036 | 0.969 | 0.233 |
| Sugar (g) | 76 (33) | 77 (23) | 96 * (44) | 103 * (31) | 91 (40) | 99 * (29) | <0.001 | 0.650 | 0.715 |
| Dietary fibre (g) | 23 (16) | 23 (5) | 24 (13) | 28 (9) | 21 (7) | 23 (7) | 0.042 | 0.484 | 0.458 |
| Vitamin C (mg) | 67 (79) | 80 (28) | 446 * (61) | 429 * (92) | 471 * (104) | 454 * (54) | <0.001 | 0.643 | 0.604 |
| Sodium (mg) | 2596 (1076) | 2163 (1020) | 2260 (960) | 2089 (878) | 2035 (1116) | 1940 (689) | 0.148 | 0.324 | 0.677 |
| Potassium (mg) | 3032 (1300) | 3159 (632) | 3117 (989) | 3787 (778) | 3276 (755) | 3402 (916) | 0.079 | 0.237 | 0.140 |
| Magnesium (mg) | 332 (160) | 328 (106) | 277 (123) | 377 (140) | 285 (95) | 322 (144) | 0.181 | 0.278 | 0.005 |
| Iron (mg) | 12 (6) | 12 (4) | 10 (4) | 13 (5) | 11 (4) | 11 (4) | 0.447 | 0.739 | 0.164 |
| Calcium (mg) | 752 (352) | 798 (382) | 741 (299) | 822 (327) | 691 (293) | 743 (365) | 0.454 | 0.532 | 0.945 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eady, S.L.; Wallace, A.J.; Hedderley, D.I.; Bentley-Hewitt, K.L.; Butts, C.A. The Effects on Immune Function and Digestive Health of Consuming the Skin and Flesh of Zespri® SunGold Kiwifruit (Actinidia Chinensis var. Chinensis ‘Zesy002’) in Healthy and IBS-Constipated Individuals. Nutrients 2020, 12, 1453. https://doi.org/10.3390/nu12051453
Eady SL, Wallace AJ, Hedderley DI, Bentley-Hewitt KL, Butts CA. The Effects on Immune Function and Digestive Health of Consuming the Skin and Flesh of Zespri® SunGold Kiwifruit (Actinidia Chinensis var. Chinensis ‘Zesy002’) in Healthy and IBS-Constipated Individuals. Nutrients. 2020; 12(5):1453. https://doi.org/10.3390/nu12051453
Chicago/Turabian StyleEady, Sarah L., Alison J. Wallace, Duncan I. Hedderley, Kerry L. Bentley-Hewitt, and Christine A. Butts. 2020. "The Effects on Immune Function and Digestive Health of Consuming the Skin and Flesh of Zespri® SunGold Kiwifruit (Actinidia Chinensis var. Chinensis ‘Zesy002’) in Healthy and IBS-Constipated Individuals" Nutrients 12, no. 5: 1453. https://doi.org/10.3390/nu12051453
APA StyleEady, S. L., Wallace, A. J., Hedderley, D. I., Bentley-Hewitt, K. L., & Butts, C. A. (2020). The Effects on Immune Function and Digestive Health of Consuming the Skin and Flesh of Zespri® SunGold Kiwifruit (Actinidia Chinensis var. Chinensis ‘Zesy002’) in Healthy and IBS-Constipated Individuals. Nutrients, 12(5), 1453. https://doi.org/10.3390/nu12051453