Malnutrition-Inflammation Score VS Phase Angle in the Era of GLIM Criteria: A Cross-Sectional Study among Hemodialysis Patients in UAE



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Malnutrition-Inflammation Score (MIS)
2.3. Malnutrition Using the Global Leadership Initiative on Malnutrition (GLIM) Criteria
2.4. Phase Angle (PhA)
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Concordance of GLIM with MIS and PhA
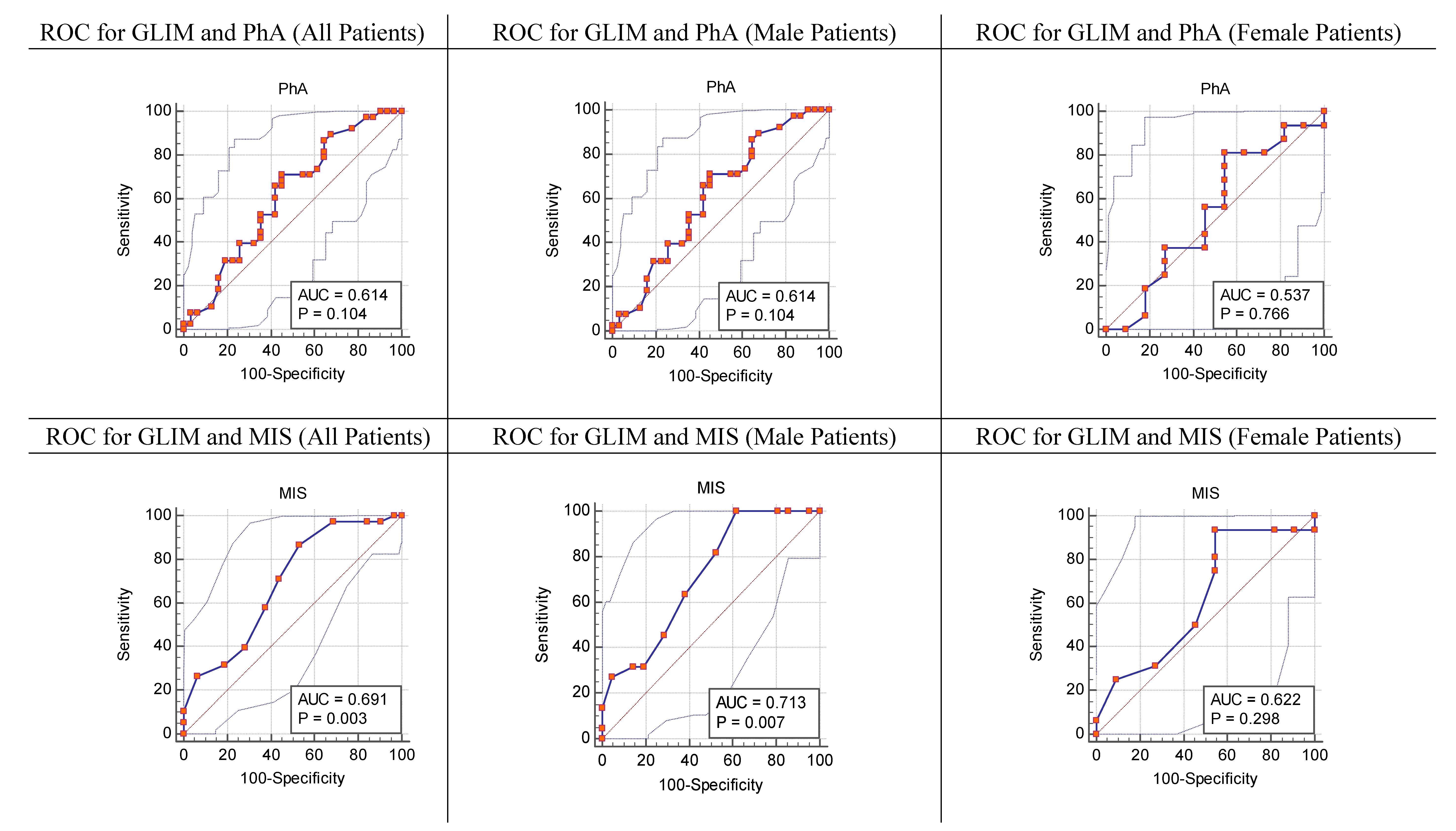
3.3. Strength of Agreement between the GLIM Criteria vs. the MIS, and the GLIM Criteria vs. PhA
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kalantar-Zadeh, K.; Kopple, J.D.; Humphreys, M.H.; Block, G. Comparing outcome predictability of markers of malnutrition-inflammation complex syndrome in haemodialysis patients. Nephrol. Dial. Transplant. 2004, 19, 1507–1519. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, A.; Regolisti, G.; Karupaiah, T.; Sahathevan, S.; Singh, B.K.S.; Khor, B.H.; Salhab, N.; Karavetian, M.; Cupisti, A.; Fiaccadori, E. Protein-energy wasting and nutritional supplementation in patients with end-stage renal disease on hemodialysis. Clin. Nutr. 2017, 36, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A.; Cano, N.J.; Franch, H.; Fouque, D.; Himmelfarb, J.; Kalantar-Zadeh, K.; Kuhlmann, M.K.; Stenvinkel, P.; TerWee, P.; Teta, D.; et al. Prevention and treatment of protein energy wasting in chronic kidney disease patients: A consensus statement by the International Society of Renal Nutrition and Metabolism. Kidney Int. 2013, 84, 1096–1107. [Google Scholar] [CrossRef] [PubMed]
- Poulia, K.A.; Klek, S.; Doundoulakis, I.; Bouras, E.; Karayiannis, D.; Baschali, A.; Passakiotou, M.; Chourdakis, M. The two most popular malnutrition screening tools in the light of the new ESPEN consensus definition of the diagnostic criteria for malnutrition. Clin. Nutr. 2017, 36, 1130–1135. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Rogowski, L.; Kusztal, M.; Golebiowski, T.; Bulinska, K.; Zembron-Lacny, A.; Wyka, J.; Klinger, M.; Wozniewski, M.; Dziubek, W. Nutritional assessment of patients with end-stage renal disease using the MNA scale. Adv. Clin. Exp. Med. 2018, 27, 1117–1123. [Google Scholar] [CrossRef]
- Da Silva, A.T.; Hauschild, D.B.; Moreno, Y.M.F.; Bastos, J.L.D.; Wazlawik, E. Diagnostic Accuracy of Bioelectrical Impedance Analysis Parameters for the Evaluation of Malnutrition in Patients Receiving Hemodialysis. Nutr. Clin. Pract. 2018, 33, 831–842. [Google Scholar] [CrossRef]
- Garcia, M.F.; Wazlawik, E.; Moreno, Y.M.F.; Fhur, L.M.; Gonzalez-Chica, D.A. Diagnostic accuracy of handgrip strength in the assessment of malnutrition in hemodialyzed patients. e-SPEN J. 2013, 8, e181–e186. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Kopple, J.D.; Block, G.; Humphreys, M.H. A malnutrition-inflammation score is correlated with morbidity and mortality in maintenance hemodialysis patients. Am. J. Kidney Dis. 2001, 38, 1251–1263. [Google Scholar] [CrossRef]
- Pisetkul, C.; Chanchairujira, K.; Chotipanvittayakul, N.; Ong-Ajyooth, L.; Chanchairujira, T. Malnutrition-inflammation score associated with atherosclerosis, inflammation and short-term outcome in hemodialysis patients. J. Med. Assoc. Thail. 2010, 93 (Suppl. 1), S147–S156. [Google Scholar]
- Rambod, M.; Bross, R.; Zitterkoph, J.; Benner, D.; Pithia, J.; Colman, S.; Kovesdy, C.P.; Kopple, J.D.; Kalantar-Zadeh, K. Association of Malnutrition-Inflammation Score with quality of life and mortality in hemodialysis patients: A 5-year prospective cohort study. Am. J. Kidney Dis. 2009, 53, 298–309. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, W.A. Moving the issue of renal dietitian staffing forward. J. Ren. Nutr. 2012, 22, 515–520. [Google Scholar] [CrossRef] [PubMed]
- The American Dietetic Association (ADA). Chronic Kidney Disease. In Evidence-Based Nutrition Practice Guideline; The American Dietetic Association (ADA): Chicago, IL, USA, 2010. [Google Scholar]
- Baumgartner, R.N.; Chumlea, W.C.; Roche, A.F. Bioelectric impedance phase angle and body composition. Am. J. Clin. Nutr. 1988, 48, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Barbosa-Silva, M.C.; Barros, A.J. Bioelectrical impedance analysis in clinical practice: A new perspective on its use beyond body composition equations. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Soundar, E.P.; Genton, L.; Pichard, C. Can phase angle determined by bioelectrical impedance analysis assess nutritional risk? A comparison between healthy and hospitalized subjects. Clin. Nutr. 2012, 31, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Wiech, P.; Bazalinski, D.; Salacinska, I.; Binkowska-Bury, M.; Korczowski, B.; Mazur, A.; Kozka, M.; Dabrowski, M. Decreased Bioelectrical Impedance Phase Angle in Hospitalized Children and Adolescents with Newly Diagnosed Type 1 Diabetes: A Case-Control Study. J. Clin. Med. 2018, 7, 516. [Google Scholar] [CrossRef] [PubMed]
- Salhab, N.; Karavetian, M.; Kooman, J.; Fiaccadori, E. Intradialytic Aerobic Exercise in the United Arab Emirates: A Descriptive Study. Arab J. Nutr. Exerc. 2018, 3, 18–34. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Liu, P.; Ma, F.; Lou, H.; Liu, Y. The utility of fat mass index vs. body mass index and percentage of body fat in the screening of metabolic syndrome. BMC Public Health 2013, 13, 629. [Google Scholar] [CrossRef] [PubMed]
- Peltz, G.; Aguirre, M.T.; Sanderson, M.; Fadden, M.K. The role of fat mass index in determining obesity. Am. J. Hum. Biol. 2010, 22, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, D.J.; Erskine, R.M.; Morse, C.I.; Onambele, G.L. Body Fat Percentage, Body Mass Index, Fat Mass Index and the Ageing Bone: Their Singular and Combined Roles Linked to Physical Activity and Diet. Nutrients 2019, 11, 195. [Google Scholar] [CrossRef] [PubMed]
- Graf, C.E.; Herrmann, F.R.; Genton, L. Relation of Disease with Standardized Phase Angle among Older Patients. J. Nutr. Health Aging 2018, 22, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.C.; Barbosa-Silva, T.G.; Bielemann, R.M.; Gallagher, D.; Heymsfield, S.B. Phase angle and its determinants in healthy subjects: Influence of body composition. Am. J. Clin. Nutr. 2016, 103, 712–716. [Google Scholar] [CrossRef]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gomez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis-part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Grunau, G.; Linn, S. Commentary: Sensitivity, Specificity, and Predictive Values: Foundations, Pliabilities, and Pitfalls in Research and Practice. Front. Public Health 2018, 6, 256. [Google Scholar] [CrossRef]
- Bansal, N.; Zelnick, L.R.; Himmelfarb, J.; Chertow, G.M. Bioelectrical Impedance Analysis Measures and Clinical Outcomes in CKD. Am. J. Kidney Dis. 2018, 72, 662–672. [Google Scholar] [CrossRef]
- Barbosa-Silva, M.C. Subjective and objective nutritional assessment methods: What do they really assess? Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 248–254. [Google Scholar] [CrossRef]
- Rinaldi, S.; Gilliland, J.; O’Connor, C.; Chesworth, B.; Madill, J. Is phase angle an appropriate indicator of malnutrition in different disease states? A systematic review. Clin. Nutr. ESPEN 2019, 29, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Johansen, K.L.; Lee, C. Body composition in chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2015, 24, 268–275. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total n = 70 | |
| Mean (SD) | |
| Age (years) | 54.61 (12.79) |
| BMI (kg/m2) | 27.22 (6.48) |
| PhA (°) | 4.66 (1.21) |
| MIS | 9.40 (3.07) |
| FMI (kg/m2) | 10.15 (5.00) |
| SMM (kg) | 19.67 (6.44) |
| Fat (kg) | 26.70 (12.57) |
| Median (IQR) | |
| FFMI (kg/m2) | 17.09 (3.33) |
| FFM (kg) | 42.92 (15.14) |
| TBW (L) | 32.15 (11.4) |
| ECW (L) | 15.20 (4.7) |
| N (%) | |
| Gender: Male | 43 (61.4) |
| Comorbidities * Diabetes Hypertension Cardiovascular Diseases Others | 46 (65.71) 62 (88.57) 28 (40.00) 37 (52.86) |
| Dialysis Vintage <1 year 1–4 years >4 years | 5 (7.14) 35 (50.00) 30 (42.86) |
| Malnourished as per GLIM Criteria | 38 (54.29) |
| Stage 1: Moderate Malnutrition | 12 (31.58) |
| Stage 2: Severe Malnutrition | 26 (68.42) |
| Malnourished as per the MIS (>10) | 34 (48.57) |
| Criterion | MIS > 10 | PhA ≤ 5.7° |
|---|---|---|
| Sensitivity (%) | 39.47 | 86.84 |
| Specificity (%) | 71.87 | 35.48 |
| Positive predictive value (%) | 50.0 | 62.63 |
| Negative predictive value (%) | 62.5 | 68.68 |
| Positive likelihood ratio (LR+) | 1.40 | 1.35 |
| Negative likelihood ratio (LR−) | 0.84 | 0.37 |
| K value (p) | 0.202 (0.089) | 0.234 (0.029) |
| Area under the curve (AUC) | 0.691 | 0.614 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karavetian, M.; Salhab, N.; Rizk, R.; Poulia, K.A. Malnutrition-Inflammation Score VS Phase Angle in the Era of GLIM Criteria: A Cross-Sectional Study among Hemodialysis Patients in UAE. Nutrients 2019, 11, 2771. https://doi.org/10.3390/nu11112771
Karavetian M, Salhab N, Rizk R, Poulia KA. Malnutrition-Inflammation Score VS Phase Angle in the Era of GLIM Criteria: A Cross-Sectional Study among Hemodialysis Patients in UAE. Nutrients. 2019; 11(11):2771. https://doi.org/10.3390/nu11112771
Chicago/Turabian StyleKaravetian, Mirey, Nada Salhab, Rana Rizk, and Kalliopi Anna Poulia. 2019. "Malnutrition-Inflammation Score VS Phase Angle in the Era of GLIM Criteria: A Cross-Sectional Study among Hemodialysis Patients in UAE" Nutrients 11, no. 11: 2771. https://doi.org/10.3390/nu11112771
APA StyleKaravetian, M., Salhab, N., Rizk, R., & Poulia, K. A. (2019). Malnutrition-Inflammation Score VS Phase Angle in the Era of GLIM Criteria: A Cross-Sectional Study among Hemodialysis Patients in UAE. Nutrients, 11(11), 2771. https://doi.org/10.3390/nu11112771