Vitamin D Daily versus Monthly Administration: Bone Turnover and Adipose Tissue Influences

 ,
,  ,
, 
Abstract
1. Introduction
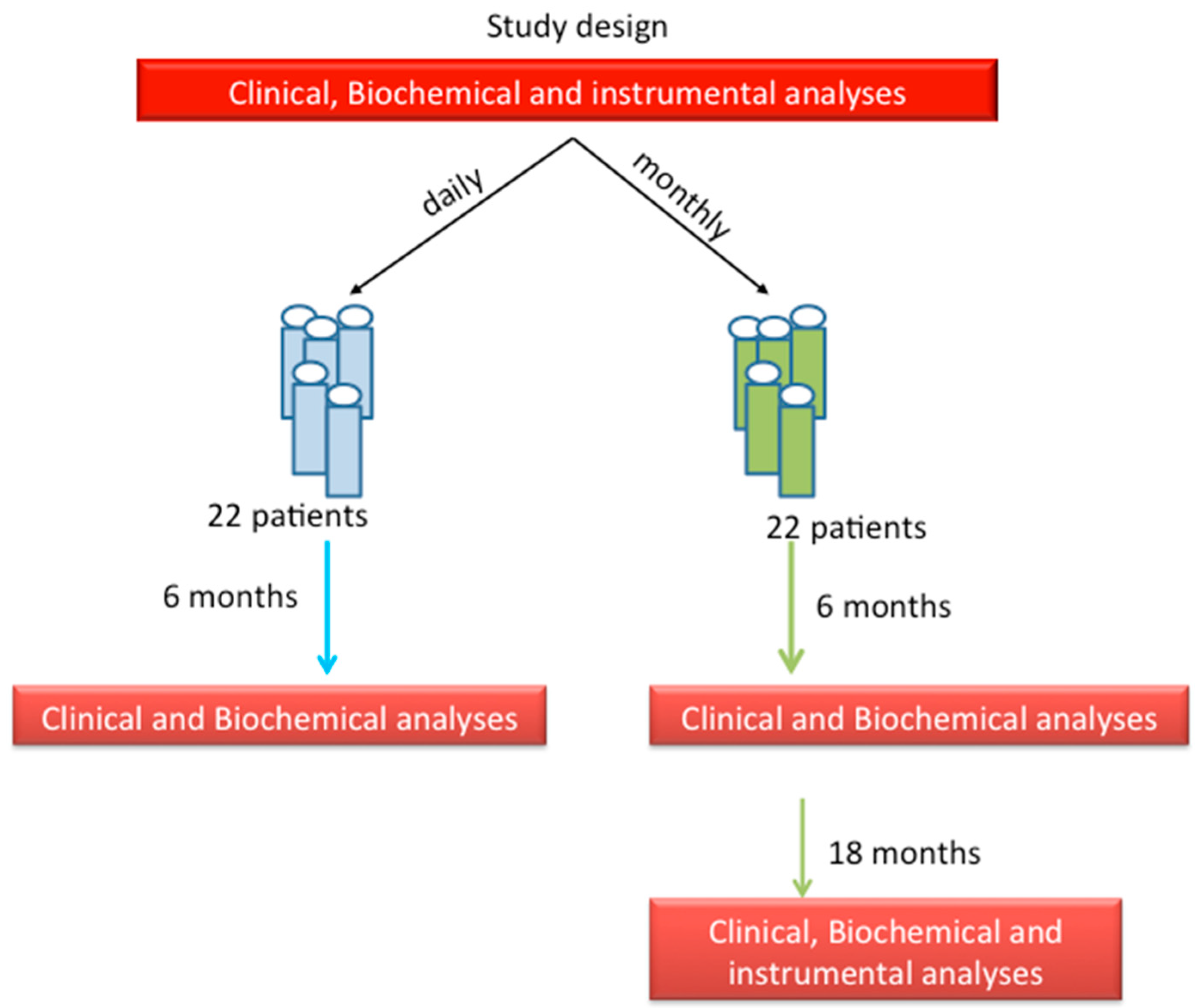
2. Patients and Methods
2.1. Biochemical Evaluations
2.2. Clinical Evaluations
2.3. Bone Densitometry
2.4. Statistical Analysis
3. Results
3.1. Groups of Treatment: Daily vs. Monthly
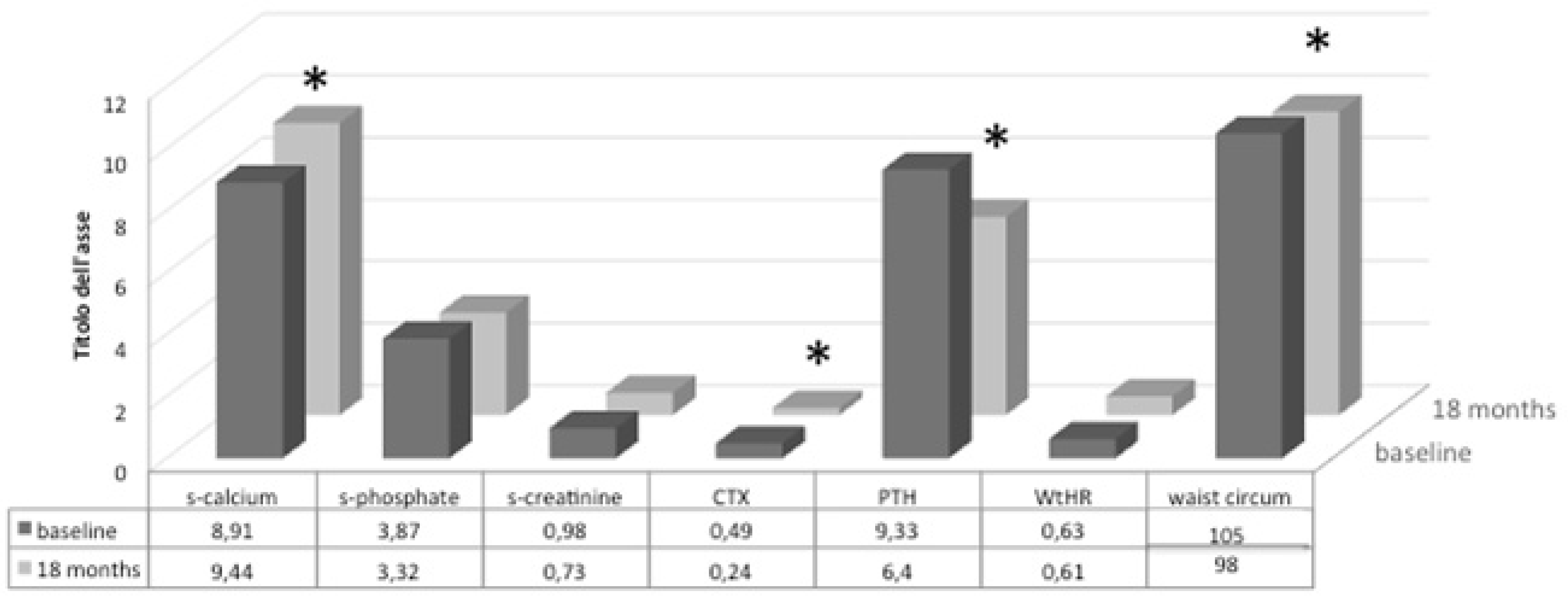
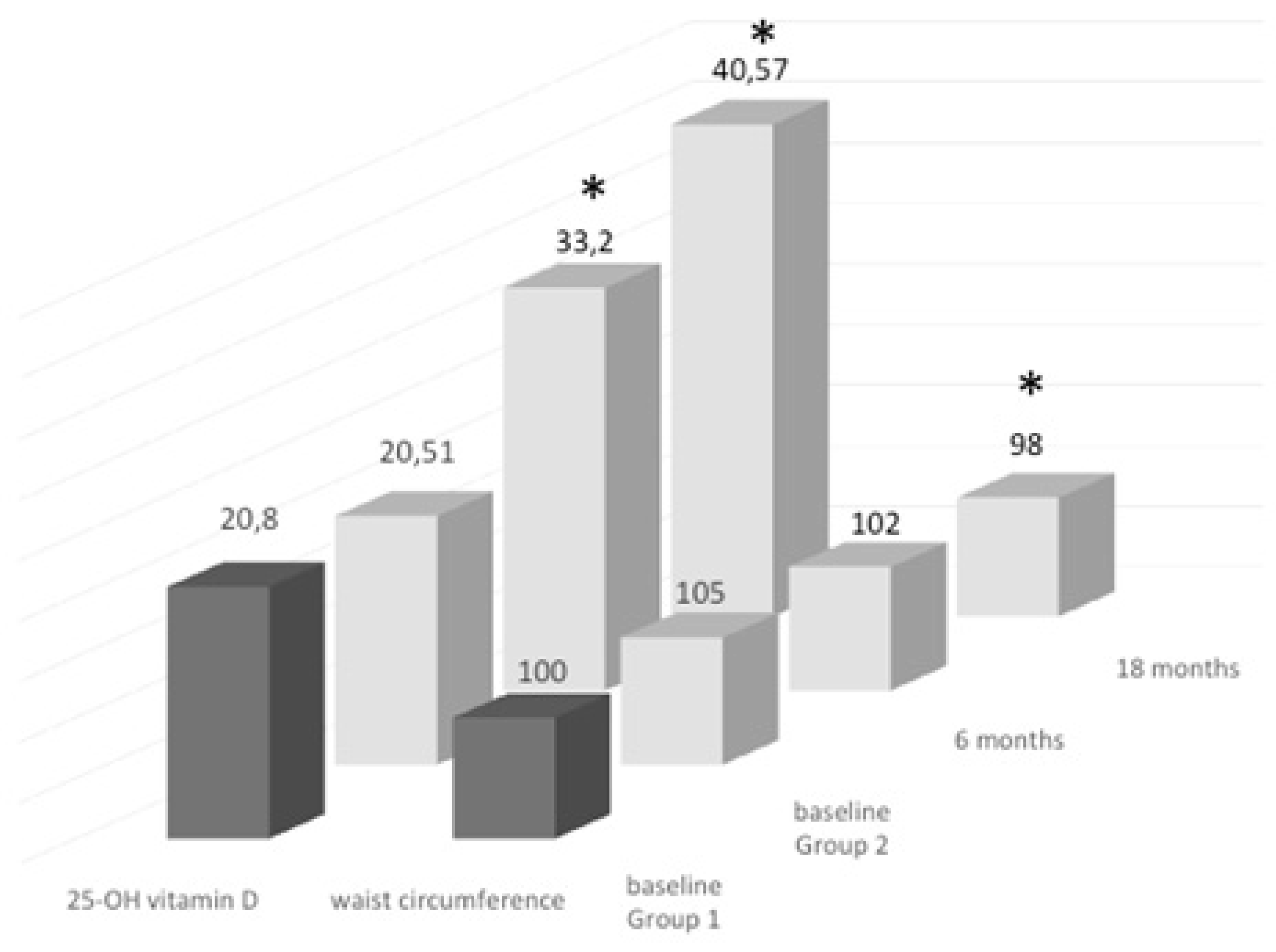
3.2. Follow-Up Study of Monthly Treatment
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Cashman, K.D. Vitamin D requirements for the future-lessons learned and charting a path forward. Nutrients 2018, 10, 533. [Google Scholar] [CrossRef]
- Dalle Carbonare, L.; Valenti, M.T.; del Forno, F.; Caneva, E.; Pietrobelli, A. Vitamin D: Daily vs. monthly use in children and elderly—What is going on? Nutrients 2017, 9, 652. [Google Scholar] [CrossRef] [PubMed]
- Ebeling, P.; Adler, R.; Jones, G.; Liberman, U.A.; Mazziotti, G.; Minisola, S.; Munns, C.; Napoli, N.; Pittas, A.; Giustina, A.; et al. Management of endocrine disease: Therapeutics of vitamin D. Eur. J. Endocrinol. 2018, 179, R239–R259. [Google Scholar] [CrossRef] [PubMed]
- Posa, F.; Di Benedetto, A.; Cavalcanti-Adam, E.A.; Colaianni, G.; Porro, C.; Trotta, T.; Brunetti, G.; Lo Muzio, L.; Grano, M.; Mori, G. Vitamin D promotes MSC osteogenic differentiation stimulating cell adhesion and alphavbeta3 expression. Stem Cells Int. 2018, 2018, 6958713. [Google Scholar] [CrossRef] [PubMed]
- Posa, F.; Di Benedetto, A.; Colaianni, G.; Cavalcanti-Adam, E.A.; Brunetti, G.; Porro, C.; Trotta, T.; Grano, M.; Mori, G. Vitamin D effects on osteoblastic differentiation of mesenchymal stem cells from dental tissues. Stem Cells Int. 2016, 2016, 9150819. [Google Scholar] [CrossRef]
- Liu, P.; Oyajobi, B.O.; Russell, R.G.; Scutt, A. Regulation of osteogenic differentiation of human bone marrow stromal cells: Interaction between transforming growth factor-beta and 1,25(OH)(2) vitamin D(3) in vitro. Calcified Tissue Int. 1999, 65, 173–180. [Google Scholar] [CrossRef]
- Rosen, C.J.; Ackert-Bicknell, C.; Rodriguez, J.P.; Pino, A.M. Marrow fat and the bone microenvironment: Developmental, functional, and pathological implications. Crit. Rev. Eukaryot Gene Expr. 2009, 19, 109–124. [Google Scholar] [CrossRef]
- Ge, C.; Cawthorn, W.P.; Li, Y.; Zhao, G.; Macdougald, O.A.; Franceschi, R.T. Reciprocal control of osteogenic and adipogenic differentiation by ERK/MAP kinase phosphorylation of Runx2 and PPARgamma transcription factors. J. Cell. Physiol. 2016, 231, 587–596. [Google Scholar] [CrossRef]
- Dalle Carbonare, L.; Manfredi, M.; Caviglia, G.; Conte, E.; Robotti, E.; Marengo, E.; Cheri, S.; Zamboni, F.; Gabbiani, D.; Deiana, M.; et al. Can half-marathon affect overall health? The yin-yang of sport. J. Proteomics 2018, 170, 80–87. [Google Scholar] [CrossRef]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific opinion on dietary reference values for vitamin A. EFSA J. 2016, 14, 4547. [Google Scholar] [CrossRef]
- Hollis, B.W.; Wagner, C.L. Clinical review: The role of the parent compound vitamin D with respect to metabolism and function: Why clinical dose intervals can affect clinical outcomes. J. Clin. Endocrinol. MeTable 2013, 98, 4619–4628. [Google Scholar] [CrossRef] [PubMed]
- Szlagatys-Sidorkiewicz, A.; Brzeziński, M.; Jankowska, A.; Metelska, P.; Słomińska-Frączek, M.; Socha, P. Long-term effects of vitamin D supplementation in vitamin D deficient obese children participating in an integrated weight-loss programme (a double-blind placebo-controlled study)—Rationale for the study design. BMC Pediatr. 2017, 17, 97. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Faith, M.S.; Wang, J.; Brambilla, P.; Chiumello, G.; Heymsfield, S.B. Association of lean tissue and fat mass with bone mineral content in children and adolescents. Obes. Res. 2002, 10, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Feizabad, E.; Hossein-Nezhad, A.; Maghbooli, Z.; Ramezani, M.; Hashemian, R.; Moattari, S. Impact of air pollution on vitamin D deficiency and bone health in adolescents. Arch Osteoporos. 2017, 12, 34. [Google Scholar] [CrossRef] [PubMed]
- Ogata, M.; Iwasaki, N.; Ide, R.; Takizawa, M.; Tanaka, M.; Tetsuo, T.; Sato, A.; Uchigata, Y. Role of vitamin D in energy and bone metabolism in postmenopausal women with type 2 diabetes mellitus: A 6-month follow-up evaluation. J. Diabetes Investig. 2018, 9, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Dix, C.F.; Bauer, J.D.; Martin, I.; Rochester, S.; Duarte Romero, B.; Prins, J.B.; Wright, O.R.L. Association of sun exposure, skin colour and body mass index with vitamin d status in individuals who are morbidly obese. Nutrients 2017, 9, 1094. [Google Scholar] [CrossRef] [PubMed]
- Carlberg, C.; Campbell, M.J. Vitamin D receptor signaling mechanisms: Integrated actions of a well-defined transcription factor. Steroids 2013, 78, 127–136. [Google Scholar] [CrossRef]
- Javaid, M.K. Maternal vitamin D status during pregnancy and childhood bone mass at age 9 years: A longitudinal study. Lancet 2006, 367, 36–44. [Google Scholar] [CrossRef]
- Hart, P.H.; Lucas, R.M.; Walsh, J.P. Vitamin D in fetal development: Findings from a birth cohort study. Pediatrics 2015, 135, e167–e173. [Google Scholar] [CrossRef]
- Hewison, M.; Adams, J.S. Vitamin insufficiency and skeletal development in utero. J Bone Miner. Res. 2010, 25, 11–13. [Google Scholar] [CrossRef]
- Eggemoen, A.R.; Jenum, A.K.; Mdala, I.; Knutsen, K.V.; Lagerlov, P.; Sletner, L. Vitamin D levels during pregnancy and association with birth weight and body composition of the newborn: A longitudinal multiethnic population-based study. BMJ 2017, 117, 985–993. [Google Scholar] [CrossRef] [PubMed]
- Hensen, K.E.; Johnson, M.G. An update on vitamin D for clinicians. Curr. Opin. Endocrinol. Diabetes Obes. 2016, 23, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R. Comparative analysis of nutritional guidelines for vitamin D. Nat. Rev. 2017, 13, 466–479. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.J. Vitamin D and adipogenesis: New molecular insights. Nutr. Rev. 2008, 66, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Kamei, Y.; Kawada, T.; Kazuki, R.; Ono, T.; Kato, S.; Sugimoto, E. Vitamin D receptor gene expression is upregulated by 1,25-dihydroxyvitamin D3 in 3T3-L1 preadipocytes. Biochem. Biophys. Res. Commun. 1993, 193, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Marcotorchino, J.; Tourniaire, F.; Landrier, J.F. Vitamin D, adipose tissue, and obesity. Horm. Mol. Biol. Clin. Investig. 2013, 15, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Hyppönen, E.; Power, C. Vitamin D status and glucose homeostasis in the 1958 British birth cohort: The role of obesity. Diabetes Care 2006, 29, 2244–2246. [Google Scholar] [CrossRef]
- Chawla, A.; Nguyen, K.D.; Goh, Y.P. Macrophage-mediated inflammation in metabolic disease. Nat. Rev. Immunol. 2011, 11, 738–749. [Google Scholar] [CrossRef]
- Moreno-Navarrete, J.M.; Fernández-Real, J.M. Adipocyte differentiation. In Adipose Tissue Biology; Symonds, M., Ed.; Springer: New York, NY, USA, 2012; pp. 17–28. [Google Scholar]
- Felicidade, I.; Sartori, D.; Coort, S.L.M.; Semprebon, S.C.; Niwa, A.M.; D’Epiro, G.F.R.; Biazi, B.I.; Marques, L.A.; Evelo, C.T.; Mantovani, M.S.; et al. Role of 1α,25-Dihydroxyvitamin D3 in adipogenesis of SGBS cells: New insights into human preadipocyte proliferation. Cell. Physiol. Biochem. 2018, 48, 397–408. [Google Scholar] [CrossRef]
- Kong, J.; Li, Y.C. Molecular mechanism of 1,25-dihydroxyvitamin D3 inhibition of adipogenesis in 3T3-L1 cells. Am. J. Physiol. Endocrinol. MeTable 2006, 290, E916–E924. [Google Scholar] [CrossRef]
- Duque, G.; Daly, R.M.; Sanders, K.; Kiel, D.P. Review article: Vitamin D, bones, and muscle: Myth versus reality. Australas. J. Aging 2017, 36, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.J.; Abrams, S.A.; Aloia, S.J.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; Kovacs, C.S.; et al. IOM Committee members respond to Endocrine Society vitamin D guideline. J. Clin. Endocrinol. MeTable 2012, 97, 1146–1152. [Google Scholar] [CrossRef] [PubMed]
- Pironi, L.; Arends, J.; Bozzetti, F.; Cuerda, C.; Gillanders, L.; Jeppesen, P.B.; Joly, F.; Kelly, D.; Lal, S.; Staun, M.; et al. ESPEN guidelines on chronic intestinal failure in adults. Clin. Nutr. 2016, 35, 247–307. [Google Scholar] [CrossRef]
- Gallagher, J.C.; Yalamanchili, V.; Smith, L.M. The effect of vitamin D supplementation on serum 25OHD in thin and obese women. J. Steroid Biochem. Mol. Biol. 2013, 136, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Ekwaru, J.P.; Zwicker, J.D.; Holick, M.F.; Giovannucci, E.; Veugelers, P.J. The importance of body weight for the dose response relationship of oral vitamin D supplementation and serum 25-hydroxyvitamin D in healthy volunteers. PLoS ONE 2014, 9, e111265. [Google Scholar] [CrossRef] [PubMed]
- Rockwell, M.; Kraak, V.; Hulver, M.; Epling, J. Clinical management of low Vitamin D: A scoping review of physicians’ practices. Nutrients 2018, 10, 493. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.C.; Wu, C.C.; Liao, M.T.; Shyu, J.F.; Hung, C.F.; Yen, T.H.; Lu, C.L.; Lu, K.C. Role of nutritional vitamin D in osteoporosis treatment. Clin. Chim. Acta 2018, 484, 179–191. [Google Scholar] [CrossRef]
- Apostolakis, M.; Armeni, E.; Bakas, P.; Lambrinoudaki, I. Vitamin D and cardiovascular disease. Maturitas 2018, 115, 1–22. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Group 1 (Daily) | Group 2 (Montly) | P |
|---|---|---|---|
| Number of subjects | 22 | 22 | NS |
| Sex (M/F) | 10/12 | 9/13 | NS |
| Age (yrs) | 77 ± 9 | 78 ± 8 | NS |
| Weight (kg) | 76 ± 18.6 | 77 ± 11.2 | NS |
| BMI (kg/m2) | 27.7 ± 6.5 | 27.3 ± 4 | NS |
| Waist circumference (cm) | 99.5 ± 13 | 105 ± 9 | NS |
| WtHR | 0.60 ± 0.78 | 0.63 ± 0.07 | NS |
| 25(OH) vitamin D (ng/mL) | 20.81 ± 6.98 | 20.51 ± 5.61 | NS |
| s-Calcium (mg/dL) | 8.99 ± 0.45 | 8.91 ± 0.29 | NS |
| s-Phoshate (mg/dL) | 2.52 ± 0.67 | 3.87 ± 0.56 | NS |
| s-Creatinine (mg/dL) | 0.96 ± 0.23 | 0.98 ± 0.25 | NS |
| CTX (ng/mL) | 0.50 ± 0.37 | 0.49 ± 0.31 | NS |
| PTH (pmol/L) | 8.39 ± 3.31 | 9.33 ± 6.76 | NS |
| ALP (U/L) | 85.25 ± 31.18 | 100.5 ± 74.24 | NS |
| Total Hip BMD (g/cm2) | 0.821 ± 0.105 | 0.873 ± 0.101 | NS |
| Total Hip T-score (SD) | −1.0 ± 0.9 | −0.3 ± 0.7 | NS |
| Femoral Neck BMD (g/cm2) | 0.656 ± 0.137 | 0.798 ± 0.201 | NS |
| Femoral Neck T-score (SD) | −1.7 ± 0.3 | −0.7 ± 0.7 | NS |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalle Carbonare, L.; Valenti, M.T.; Del Forno, F.; Piacentini, G.; Pietrobelli, A. Vitamin D Daily versus Monthly Administration: Bone Turnover and Adipose Tissue Influences. Nutrients 2018, 10, 1934. https://doi.org/10.3390/nu10121934
Dalle Carbonare L, Valenti MT, Del Forno F, Piacentini G, Pietrobelli A. Vitamin D Daily versus Monthly Administration: Bone Turnover and Adipose Tissue Influences. Nutrients. 2018; 10(12):1934. https://doi.org/10.3390/nu10121934
Chicago/Turabian StyleDalle Carbonare, Luca, Maria Teresa Valenti, Francesco Del Forno, Giorgio Piacentini, and Angelo Pietrobelli. 2018. "Vitamin D Daily versus Monthly Administration: Bone Turnover and Adipose Tissue Influences" Nutrients 10, no. 12: 1934. https://doi.org/10.3390/nu10121934
APA StyleDalle Carbonare, L., Valenti, M. T., Del Forno, F., Piacentini, G., & Pietrobelli, A. (2018). Vitamin D Daily versus Monthly Administration: Bone Turnover and Adipose Tissue Influences. Nutrients, 10(12), 1934. https://doi.org/10.3390/nu10121934