
Psychological and Antibacterial Effects of Footbath Using the Lindera umbellata Essential Oil

 , , and
, , and
Abstract
:1. Introduction
2. Results
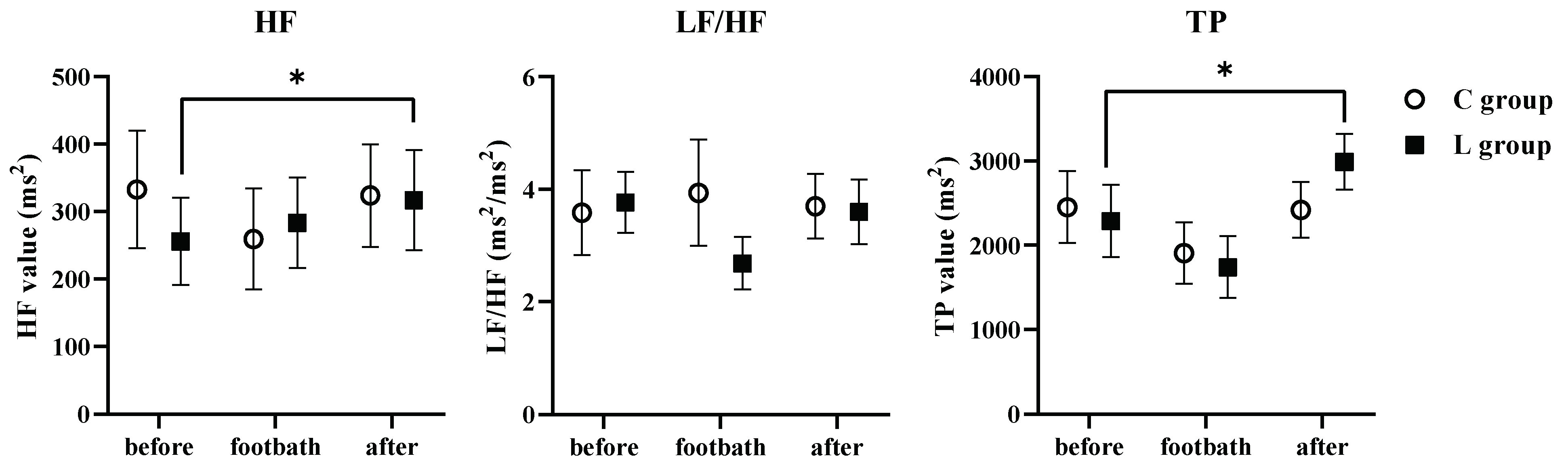
2.1. Changes of the Autonomic Nervous System Activity
2.2. Effect of the Psychological Index
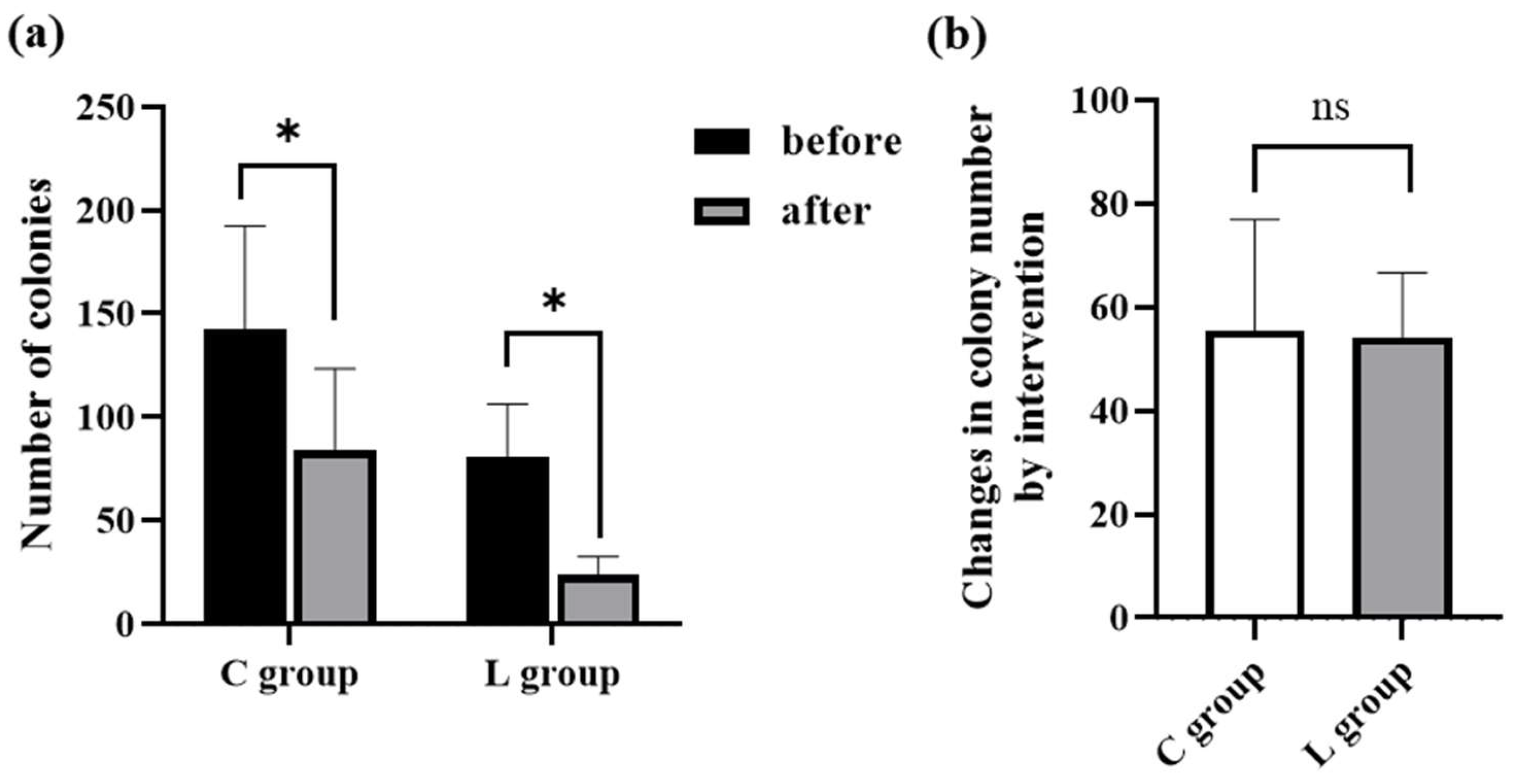
2.3. Aerobic Viable Count
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Setting
4.3. Evaluation Index
4.3.1. Questionnaire about the Psychological Assessment
4.3.2. Autonomic Nervous System Activity
4.3.3. Aerobic Viable Count
4.4. Protocol
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Edris, A.E. Pharmaceutical and therapeutic Potentials of essential oils and their individual volatile constituents: A review. Phytother. Res. 2007, 21, 308–323. [Google Scholar] [CrossRef]
- Ghiasi, A.; Bagheri, L.; Haseli, A. A systematic review on the anxiolytic effect of aromatherapy during the first stage of labor. J. Caring. Sci. 2019, 8, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchbauer, G.; Jirovetz, L.; Jager, W.; Plank, C.; Dietrich, H. Fragrance compounds and essential oil with sedative effects upon inhalation. J. Pharm. Sci. 1993, 82, 660–664. [Google Scholar] [CrossRef]
- Linck, V.M.; da Silva, A.L.; Figueiró, M.; Caramão, E.B.; Moreno, P.R.; Elisabetsky, E. Effects of inhaled Linalool in anxiety, social interaction and aggressive behavior in mice. Phytomedicine 2010, 17, 679–683. [Google Scholar] [CrossRef]
- Maeda, H.; Yamazaki, M.; Katagata, Y. Kuromoji (Lindera umbellata) essential oil inhibits LPS-induced inflammation in RAW 264.7 cells. Biosci. Biotechnol. Biochem. 2013, 77, 482–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeda, H.; Yamazaki, M.; Katagata, Y. Kuromoji (Lindera umbellata) essential oil-induced apoptosis and differentiation in human leukemia HL-60 cells. Exp. Ther. Med. 2012, 3, 49–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gnatta, J.R.; Kurebayashi, L.F.; Turrini, R.N.; Silva, M.J. Aromatherapy and nursing: Historical and theoretical conception. Rev. Esc. Enferm. USP 2016, 50, 130–136. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.L.; Chen, X.P.; Lee, K.C.; Fang, F.F.; Chao, Y.F. The effects of warm-water foot bath on relieving fatigue and insomnia of the gynecologic cancer patients on chemotherapy. Cancer Nurs. 2010, 33, 454–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, H.Y.; Lin, E.Y.; Chiu, H.T.; Chen, P.Y. A feasibility randomized controlled crossover trial of home-based warm footbath to improve sleep in the chronic phase of traumatic brain injury. J. Neurosci. Nurs. 2017, 49, 380–385. [Google Scholar] [CrossRef]
- Saeki, Y. The effect of foot-bath with or without the essential oil of lavender on the autonomic nervous system: A randomized trial. Compl. Ther. Med. 2000, 8, 2–7. [Google Scholar] [CrossRef]
- Lee, J.H.; Seo, E.K.; Shim, J.S.; Chung, S.P. The effects of aroma massage and foot bath on psychophysiological response in stroke patients. J. Phys. Ther. Sci. 2017, 29, 1292–1296. [Google Scholar] [CrossRef] [Green Version]
- Lv, X.N.; Liu, Z.J.; Zhang, H.J.; Tzeng, C.M. Aromatherapy and the central nerve system (CNS): Therapeutic mechanism and its associated genes. Curr. Drug. Targets 2013, 14, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Morishita, A.; Nakata, Y.; Tamura, Y.; Ishikawa, Y.; Bontje, P.; Takase, H.; Kubo, Y.; Tsuda, N. Effects of ‘foot bathing’ on psycho-somatic responses in healthy young adults. Bull. Health Sci. Kobe 2004, 19, 129–136. [Google Scholar]
- Shimizu, M.; Nagaya, S. Examination of the optimal depth of water in a foot-bath for adult women through physiological and psychological evaluation. J. Jpn. Acad. Nurs. Sci. 2015, 35, 18–27. [Google Scholar] [CrossRef] [Green Version]
- Rosa, P.B.; Orquiza, B.; Rocha, F.B.; Donadel, R.W.; Diniz, R.P.; Beloni, T.M.; Aniceto, J.T.; Fragoso, Y.D. Anger and stroke: A potential association that deserves serious consideration. Acta Neuropsychiatr. 2016, 28, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Chida, Y.; Steptoe, A. The association of anger and hostility with future coronary heart disease: A meta-analytic review of prospective evidence. J. Am. Coll. Cardiol. 2009, 53, 936–946. [Google Scholar] [CrossRef] [PubMed]
- Nanashima, N.; Kitajima, M.; Takamagi, S.; Fujioka, M.; Tomisawa, T. Comparison of chemical composition between Kuromoji (Lindera umbellata) essential oil and hydrosol and determination of the deodorizing effect. Molecules 2020, 25, 4195. [Google Scholar] [CrossRef]
- Han, X.; Gibson, J.; Eggett, D.L.; Parker, T.L. Bergamot (citrus bergamia) essential oil inhalation improves positive feelings in the waiting room of a mental health treatment center: A pilot study. Phytother. Res. 2017, 31, 812–816. [Google Scholar] [CrossRef] [Green Version]
- Buchbauer, G.; Jirovetz, L.; Jager, W.; Dietrich, H.; Plank, C. Aromatherapy: Evidence for sedative effects of the essential oil of lavender after inhalation. J. Biosci. 1991, 46, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Białoń, M.; Krzyśko-Łupicka, T.; Nowakowska-Bogdan, E.; Wieczorek, P.P. Chemical composition of two different lavender essential oils and their effect on facial skin microbiota. Molecules 2019, 24, 3270. [Google Scholar] [CrossRef] [Green Version]
- Deans, S.G.; Ritchie, G. Antibacterial properties of plant essential oils. Int. J. Food Microbiol. 1987, 5, 165–180. [Google Scholar] [CrossRef]
- Bassett, I.B.; Pannowitz, D.L.; Barnetson, R.S. A comparative study of tea tree oil versus benzoylperoxide in the treatment of acne. Med. J. Aust. 1990, 153, 455–458. [Google Scholar] [CrossRef] [PubMed]
- Lis-Balchin, M. Aroma Science: The Chemistry and Bioactivity of Essential Oils; Amberwood Publishing Ltd.: Stittsville, ON, USA, 1995. [Google Scholar]
- Kelen, M.; Tepe, B. Chemical composition, antioxidant and antimicrobial properties of the essential oils of three Salvia species from Turkish flora. Bioresour. Technol. 2008, 99, 4096–4104. [Google Scholar] [CrossRef] [PubMed]
- Sonboli, A.; Eftekhar, F.; Yousefzadi, M.; Kanani, M.R. Antibacterial activity and chemical composition of the essential oil of Grammosciadium platycarpum Boiss. from Iran. Z. Naturforsch. 2005, 60, 30–34. [Google Scholar] [CrossRef]
- Mourey, A.; Canillac, N. Anti-Listeria monocytogenes activity of essential oils components of conifers. Food Control 2002, 13, 289–292. [Google Scholar] [CrossRef]
- Louis, M.; Kowalski, S.D. Use of aromatherapy with hospice patients to decrease pain, anxiety, and depression and to promote an increased sense of well-being. Am. J. Hosp. Palliat. Care 2002, 19, 381–386. [Google Scholar] [CrossRef]
- Zeng, Y.S.; Wang, C.; Ward, K.E.; Hume, A.L. Complementary and alternativemedicine in hospice and palliative care: A systematic review. J. Pain Symptom Manag. 2018, 56, 781–794. [Google Scholar] [CrossRef] [Green Version]
- Dimitriou, V.; Mavridou, P.; Manataki, A.; Damigos, D. The use of aromatherapy for postoperative pain management: A systematic review of randomized controlled trials. J. Perianesth. Nurs. 2017, 32, 530–541. [Google Scholar] [CrossRef]
- Rezaie-Keikhaie, K.; Hastings-Tolsma, M.; Bouya, S.; Shad, F.S.; Sari, M.; Shoorvazi, M.; Barani, Z.Y.; Balouchi, A. Effect of aromatherapy on post-partum complications: A systematic review. Complement. Ther. Clin. Pract. 2019, 35, 290–295. [Google Scholar] [CrossRef]
- Knasko, S.C. Ambient odor’s effect on creativity, mood, and perceived health. Chem. Senses 1992, 17, 27–35. [Google Scholar] [CrossRef]
- McNair, D.M.; Lorr, M.; Droppleman, L.F. Profile of Mood States; Educational and Industrial Testing Service: San Diego, CA, USA, 1992. [Google Scholar]
- Yokoyama, K.; Araki, S.; Kawakami, N. Production of the Japanese edition of profile of Mood States (POMS): Assessment of reliability and validity. Jpn. J. Public Health 1990, 37, 913–918. [Google Scholar]
- Yokoyama, K. (Ed.) A Handbook of Short POMS; Kaneko Shobo: Tokyo, Japan, 2002. (In Japanese) [Google Scholar]
- Lan, T.T.; Kanitpong, K.; Tomiyama, K.; Kawamura, A.; Nakatsuji, T. Effectiveness of retro-reflective tape at the rear of heavy trucks to increase visibility and reduce rear-end collisions. IATSS Res. 2019, 43, 176–784. [Google Scholar] [CrossRef]
- Adachi, Y. Measurement of Time-Dependent Stress Levels by Wavelet Analysis. IEEE 2014. [Google Scholar] [CrossRef]
- Minakuchi, E.; Ohnishi, E.; Ohnishi, J.; Sakamoto, S.; Hori, M.; Motomura, M.; Hoshino, J.; Murakami, K.; Kawaguchi, T. Evaluation of mental stress by physiological indices derived from finger plethysmography. J. Physiol. Anthropol. 2013, 32, 17. [Google Scholar] [CrossRef] [Green Version]
- Pagani, M.; Lombardi, F.; Guzzetti, S.; Rimoldi, O.; Furlan, R.; Pizzinelli, P.; Sandrone, G.; Malfatto, G.; Dell’Orto, S.; Piccaluga, E.; et al. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ. Res. 1986, 59, 178–193. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| POMS Subscale | C Group | L Group | ||||
|---|---|---|---|---|---|---|
| Before Intervention | After Intervention | p Value | Before Intervention | After Intervention | p Value | |
| Tension–anxiety | 40.40 ± 4.68 | 36.25 ± 4.68 | 0.001 ** | 42.25 ± 6.99 | 35.80 ± 2.59 | 0.000 ** |
| Depression–dejection | 41.50 ± 2.93 | 40.00 ± 2.93 | 0.017 * | 43.05 ± 8.69 | 40.05 ± 2.35 | 0.001 ** |
| Anger–hostility | 38.60 ± 1.31 | 38.10 ± 1.31 | 0.102 | 40.10 ± 5.04 | 38.20 ± 0.89 | 0.010 * |
| Vigor | 42.90 ± 10.90 | 43.70 ± 10.90 | 0.959 | 42.65 ± 10.15 | 44.55 ± 10.90 | 0.315 |
| Fatigue | 39.30 ± 4.55 | 35.20 ± 4.55 | 0.002 ** | 41.15 ± 7.21 | 35.40 ± 1.96 | 0.000 ** |
| Confusion | 46.00 ± 6.93 | 43.25 ± 6.93 | 0.028 * | 47.10 ± 8.48 | 43.10 ± 4.30 | 0.000 ** |
| TMD | 162.90 ± 15.71 | 149.10 ± 15.71 | 0.000 ** | 171.00 ± 30.45 | 148.00 ± 12.97 | 0.000 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitajima, M.; Miura, M.; Nanashima, N.; Tomisawa, T.; Takamagi, S.; Fujioka, M.; In, N.; Osanai, T. Psychological and Antibacterial Effects of Footbath Using the Lindera umbellata Essential Oil. Molecules 2021, 26, 5128. https://doi.org/10.3390/molecules26175128
Kitajima M, Miura M, Nanashima N, Tomisawa T, Takamagi S, Fujioka M, In N, Osanai T. Psychological and Antibacterial Effects of Footbath Using the Lindera umbellata Essential Oil. Molecules. 2021; 26(17):5128. https://doi.org/10.3390/molecules26175128
Chicago/Turabian StyleKitajima, Maiko, Marika Miura, Naoki Nanashima, Toshiko Tomisawa, Shizuka Takamagi, Miyuki Fujioka, Naoya In, and Tomohiro Osanai. 2021. "Psychological and Antibacterial Effects of Footbath Using the Lindera umbellata Essential Oil" Molecules 26, no. 17: 5128. https://doi.org/10.3390/molecules26175128
APA StyleKitajima, M., Miura, M., Nanashima, N., Tomisawa, T., Takamagi, S., Fujioka, M., In, N., & Osanai, T. (2021). Psychological and Antibacterial Effects of Footbath Using the Lindera umbellata Essential Oil. Molecules, 26(17), 5128. https://doi.org/10.3390/molecules26175128