
Perioperative Probiotics Application for Preventing Postoperative Complications in Patients with Colorectal Cancer: A Systematic Review and Meta-Analysis

Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Characteristics of Participants
2.3. Types of Interventions and Comparators
2.4. Types of Outcomes
2.5. Primary Outcomes
2.6. Secondary Outcomes
2.7. Assessment of Risk of Bias
2.8. Data Collection and Analysis
2.9. Summary of Findings Table
3. Results
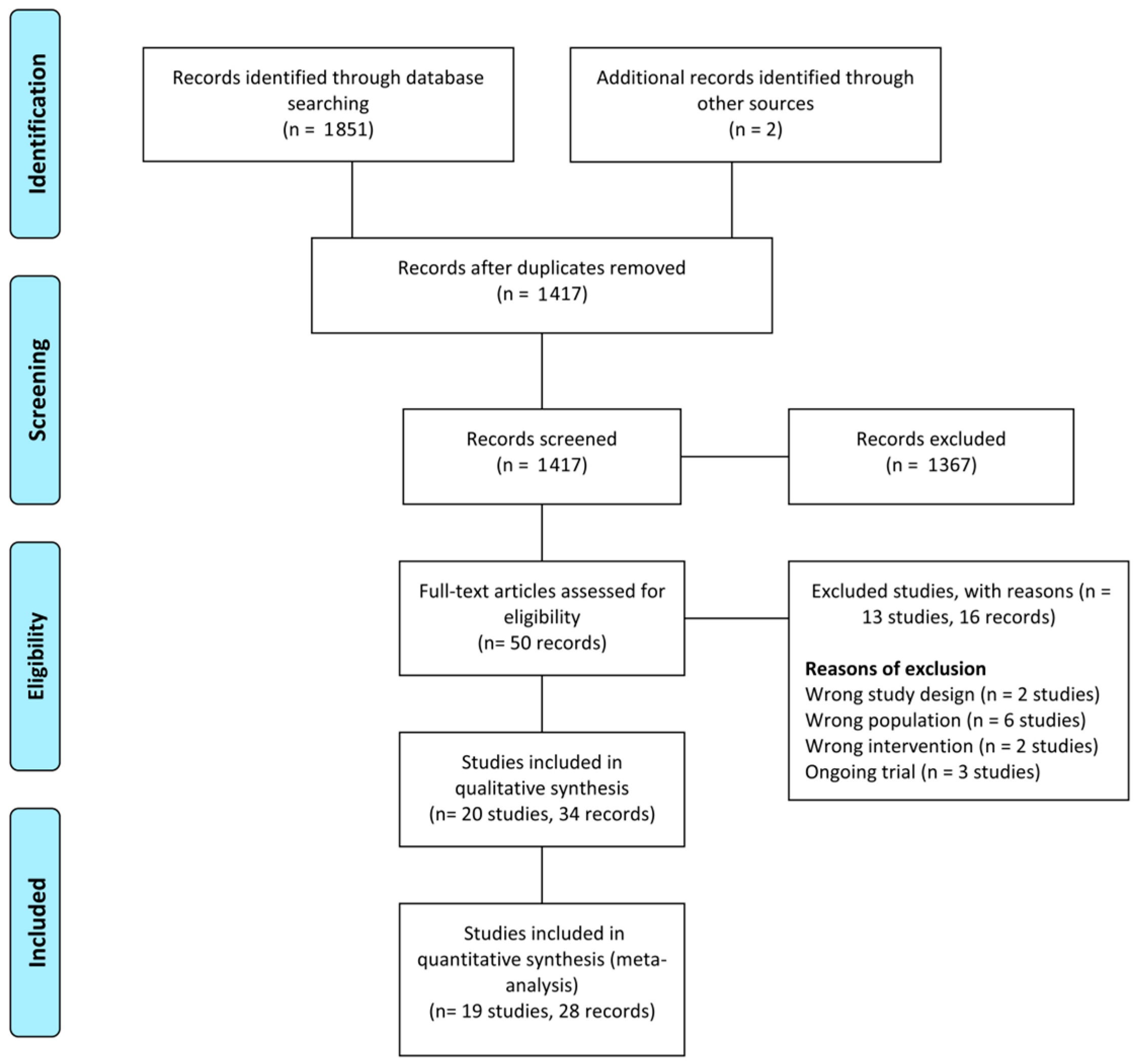
3.1. Search Results
3.2. Included Studies
3.3. Excluded Studies
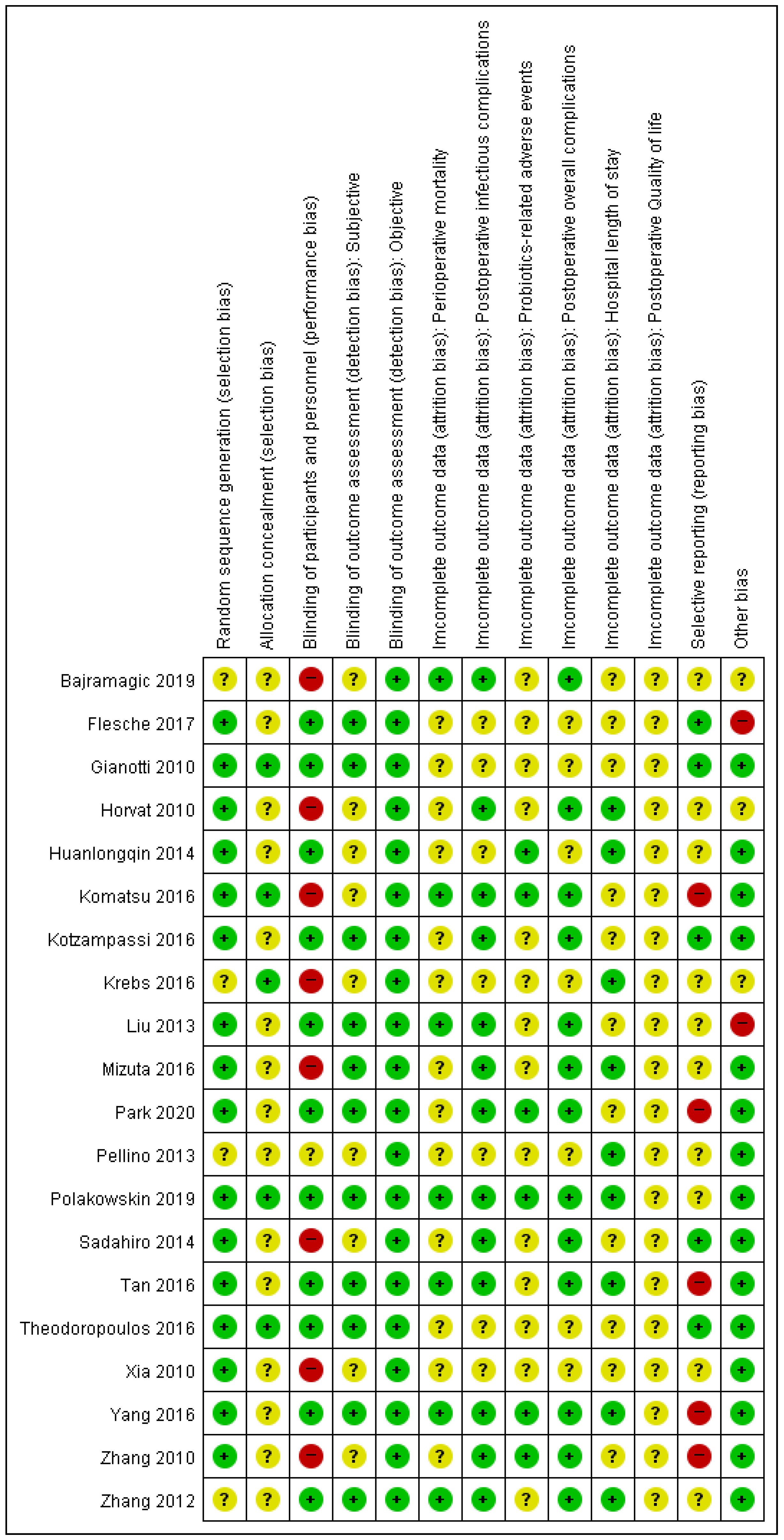
3.4. Risk of Bias of Included Studies
3.5. Effects of Interventions (Table 2)
3.5.1. Primary Outcomes (Table 2)
Perioperative Mortality

{kind=link}
{kind=link}
| Probiotics Compared to Placebo or No Treatment; Primary and Secondary Outcomes for Postoperative Outcome | |||||
|---|---|---|---|---|---|
| Patient: Colorectal Cancer Patients Who Underwent Curative Resection Setting: Inpatient Intervention: Probiotics Comparison: Placebo or Standard Care | |||||
| Outcomes | No of Participants (Studies) Follow-Up | Certainty of the Evidence (GRADE) | Relative Effect (95% CI) | Anticipated Absolute Effects | |
| Risk with Placebo or No Treatment; Primary Outcomes | Risk Difference with Probiotics | ||||
| Perioperative mortality follow-up: 30 days MCID: 2% absolute difference | 753 (8 RCTs) | ⨁⨁⨁◯ Moderate a,b | RR 0.17 (0.02 to 1.38) | 13 per 1000 | 11 fewer per 1000 (13 fewer to 5 more) |
| Overall postoperative infectious complication follow-up: 30 days MCID: 5% absolute difference | 651 (7 RCTs) | ⨁⨁◯◯ Low b,c | RR 0.45 (0.27 to 0.76) | 252 per 1000 | 138 fewer per 1000 (184 fewer to 60 fewer) |
| Probiotics related adverse events follow-up: 30 days MCID: 5% absolute difference | 692 (7 RCTs) | ⨁⨁◯◯ Low b,c | RR 0.73 (0.45 to 1.19) | 70 per 1000 | 19 fewer per 1000 (38 fewer to 13 more) |
| Overall postoperative complications follow-up: 30 days MCID: 5% absolute difference | 394 (6 RCTs) | ⨁⨁◯◯ Low b,c | RR 0.47 (0.30 to 0.74) | 359 per 1000 | 190 fewer per 1000 (251 fewer to 93 fewer) |
| Hospital length of stay follow-up: 30 days MCID: 2 days e | 411 (8 RCTs) | ⨁⨁◯◯ Low b,c | - | The mean hospital length of stay ranged from 4 to 23 days | MD 1.06 days lower (1.64 lower to 0.47 lower) |
| Quality of Life Scale from: 0 to 144 follow-up: 1 months MCID: 6.5 points f | 67 (1 RCT) | ⨁⨁◯◯ Low d | - | The mean quality of Life was 71.36 | MD 5.64 higher (0.98 higher to 10.3 higher) |
Overall Postoperative Infectious Complication
Probiotics-Related Adverse Events
3.5.2. Secondary Outcomes (Table 2)
Overall Postoperative Complications
Hospital LOS
Quality of Life (QOL)
3.6. Sensitivity Analysis: Double-Blinded Placebo-Controlled Studies Only
3.6.1. Perioperative Mortality
3.6.2. Overall Postoperative Infectious Complications
3.6.3. Probiotics-Related Adverse Events
4. Discussion
Advantage and Disadvantage
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Beck, C.; Weber, K.; Brunner, M.; Agaimy, A.; Semrau, S.; Grutzmann, R.; Schellerer, V.; Merkel, S. The influence of postoperative complications on long-term prognosis in patients with colorectal carcinoma. Int. J. Colorectal. Dis. 2020, 35, 1055–1066. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, S.; Hamada, K.; Sumida, Y.; Araki, M.; Wakata, K.; Kugiyama, T.; Shibuya, A.; Nishimuta, M.; Morino, S.; Baba, M.; et al. Postoperative complications predict long-term outcome after curative resection for perforated colorectal cancer. In Vivo 2021, 35, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Guarner, F.; Malagelada, J.-R. Gut flora in health and disease. Lancet 2003, 361, 512–519. [Google Scholar] [CrossRef]
- Hennessey, D.B.; Burke, J.P.; Ni-Dhonochu, T.; Shields, C.; Winter, D.C.; Mealy, K. Risk factors for surgical site infection following colorectal resection: A multi-institutional study. Int. J. Colorectal. Dis. 2016, 31, 267–271. [Google Scholar] [CrossRef]
- Branch-Elliman, W.; O’Brien, W.; Strymish, J.; Itani, K.; Wyatt, C.; Gupta, K. Association of duration and type of surgical prophylaxis with antimicrobial-associated adverse events. JAMA Surg. 2019, 154, 590–598. [Google Scholar] [CrossRef]
- Pickard, J.M.; Zeng, M.Y.; Caruso, R.; Nunez, G. Gut microbiota: Role in pathogen colonization, immune responses, and inflammatory disease. Immunol. Rev. 2017, 279, 70–89. [Google Scholar] [CrossRef]
- Yu, L.C. Microbiota dysbiosis and barrier dysfunction in inflammatory bowel disease and colorectal cancers: Exploring a common ground hypothesis. J. Biomed. Sci. 2018, 25, 79. [Google Scholar] [CrossRef]
- Agnes, A.; Puccioni, C.; D’Ugo, D.; Gasbarrini, A.; Biondi, A.; Persiani, R. The gut microbiota and colorectal surgery outcomes: Facts or hype? A narrative review. BMC Surg. 2021, 21, 83. [Google Scholar] [CrossRef]
- Koliarakis, I.; Athanasakis, E.; Sgantzos, M.; Mariolis-Sapsakos, T.; Xynos, E.; Chrysos, E.; Souglakos, J.; Tsiaoussis, J. Intestinal microbiota in colorectal cancer surgery. Cancers 2020, 12, 3011. [Google Scholar] [CrossRef]
- Correia, M.I.; Liboredo, J.C.; Consoli, M.L. The role of probiotics in gastrointestinal surgery. Nutrition 2012, 28, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Grat, M.; Wronka, K.M.; Lewandowski, Z.; Grat, K.; Krasnodebski, M.; Stypulkowski, J.; Holowko, W.; Masior, L.; Kosinska, I.; Wasilewicz, M.; et al. Effects of continuous use of probiotics before liver transplantation: A randomized, double-blind, placebo-controlled trial. Clin. Nutr. 2017, 36, 1530–1539. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, Y.; Miyake, T.; Kokuryo, T.; Asahara, T.; Nomoto, K.; Nagino, M. Effect of perioperative synbiotic treatment on bacterial translocation and postoperative infectious complications after pancreatoduodenectomy. Dig. Surg. 2016, 33, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Polakowski, C.B.; Kato, M.; Preti, V.B.; Schieferdecker, M.E.M.; Ligocki Campos, A.C. 2019 polakowski; impact of the preoperative use of synbiotics in colorectal cancer patients: A prospective, randomized, double-blind, placebo-controlled study. Nutrition 2019, 58, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Xia, Y.; Chen, H.; Hong, L.; Feng, J.; Yang, J.; Yang, Z.; Shi, C.; Wu, W.; Gao, R.; et al. The effect of perioperative probiotics treatment for colorectal cancer: Short-term outcomes of a randomized controlled trial. Oncotarget 2016, 7, 8432–8440. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.K.; Said, S.; Rajandram, R.; Wang, Z.; Roslani, A.C.; Chin, K.F. Pre-surgical administration of microbial cell preparation in colorectal cancer patients: A randomized controlled trial. World J. Surg. 2016, 40, 1985–1992. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, S.; Sakamoto, E.; Norimizu, S.; Shingu, Y.; Asahara, T.; Nomoto, K.; Nagino, M. Efficacy of perioperative synbiotics treatment for the prevention of surgical site infection after laparoscopic colorectal surgery: A randomized controlled trial. Surg. Today 2016, 46, 479–490. [Google Scholar] [CrossRef]
- Kotzampassi, K.; Stavrou, G.; Damoraki, G.; Georgitsi, M.; Basdanis, G.; Tsaousi, G.; Giamarellos-Bourboulis, E.J. A four-probiotics regimen reduces postoperative complications after colorectal surgery: A randomized, double-blind, placebo-controlled study. World J. Surg. 2015, 39, 2776–2783. [Google Scholar] [CrossRef]
- Zaharuddin, L.; Mokhtar, N.M.; Muhammad Nawawi, K.N.; Raja Ali, R.A. A randomized double-blind placebo-controlled trial of probiotics in post-surgical colorectal cancer. BMC Gastroenterol. 2019, 19, 131. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the cochrane handbook for systematic reviews of interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef]
- Julian Higgins, J.T.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021). Available online: www.training.cochrane.org/handbook (accessed on 10 March 2022).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.; Brożek, J.; Guyatt, G.; Oxman, A. Handbook for Grading the Quality of Evidence and the Strength of Recommendations Using the Grade Approach. Available online: https://gdt.gradepro.org/app/handbook/handbook.html#h.m9385o5z3li7%20(10%20March) (accessed on 10 March 2022).
- Park, I.J.; Lee, J.H.; Kye, B.H.; Oh, H.K.; Cho, Y.B.; Kim, Y.T.; Kim, J.Y.; Sung, N.Y.; Kang, S.B.; Seo, J.M.; et al. Effects of probiotics on the symptoms and surgical outcomes after anterior resection of colon cancer (postcare): A randomized, double-blind, placebo-controlled trial. J. Clin. Med. 2020, 9, 2181. [Google Scholar] [CrossRef] [PubMed]
- Bajramagic, S.; Hodzic, E.; Mulabdic, A.; Holjan, S.; Smajlovic, S.V.; Rovcanin, A. 2019 bajramagic; usage of probiotics and its clinical significance at surgically treated patients sufferig from colorectal carcinoma. Med. Arch. 2019, 73, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Flesch, A.T.; Tonial, S.T.; Contu, P.C.; Damin, D.C. Perioperative synbiotics administration decreases postoperative infections in patients with colorectal cancer: A randomized, double-blind clinical trial. Rev. Col. Bras. Cir. 2017, 44, 567–573. [Google Scholar] [CrossRef]
- Theodoropoulos, G.E.; Memos, N.A.; Peitsidou, K.; Karantanos, T.; Spyropoulos, B.G.; Zografos, G. Synbiotics and gastrointestinal function-related quality of life after elective colorectal cancer resection. Ann. Gastroenterol. 2016, 29, 56–62. [Google Scholar]
- Mizuta, M.; Endo, I.; Yamamoto, S.; Inokawa, H.; Kubo, M.; Udaka, T.; Sogabe, O.; Maeda, H.; Shirakawa, K.; Okazaki, E.; et al. Perioperative supplementation with bifidobacteria improves postoperative nutritional recovery, inflammatory response, and fecal microbiota in patients undergoing colorectal surgery: A prospective, randomized clinical trial. Biosci. Microbiota Food Health 2016, 35, 77–87. [Google Scholar] [CrossRef]
- Krebs, B. Prebiotic and synbiotic treatment before colorectal surgery-randomised double blind trial. Coll. Antropol. 2016, 40, 35–40. [Google Scholar]
- Sadahiro, S.; Suzuki, T.; Tanaka, A.; Okada, K.; Kamata, H.; Ozaki, T.; Koga, Y. Comparison between oral antibiotics and probiotics as bowel preparation for elective colon cancer surgery to prevent infection: Prospective randomized trial. Surgery 2014, 155, 493–503. [Google Scholar] [CrossRef]
- Chen, H.; Xia, Y.; Shi, C.; Liang, Y.; Yang, Y.; Qin, H. Effects of perioperative probiotics administration on patients with colorectal cancer. Chin. J. Clin. Nutr. 2014, 22, 74–80. [Google Scholar]
- Pellino, G.; Sciaudone, G.; Candilio, G.; Camerlingo, A.; Marcellinaro, R.; De Fatico, S.; Rocco, F.; Canonico, S.; Riegler, G.; Selvaggi, F. Early postoperative administration of probiotics versus placebo in elderly patients undergoing elective colorectal surgery: A double-blind randomized controlled trial. BMC Surg. 2013, 13 (Suppl. 2), S57. [Google Scholar] [CrossRef]
- Liu, Z.H.; Huang, M.J.; Zhang, X.W.; Wang, L.; Huang, N.Q.; Peng, H.; Lan, P.; Peng, J.S.; Yang, Z.; Xia, Y.; et al. The effects of perioperative probiotic treatment on serum zonulin concentration and subsequent postoperative infectious complications after colorectal cancer surgery: A double-center and double-blind randomized clinical trial. Am. J. Clin. Nutr. 2013, 97, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.W.; Du, P.; Gao, J.; Yang, B.R.; Fang, W.J.; Ying, C.M. Preoperative probiotics decrease postoperative infectious complications of colorectal cancer. Am. J. Med. Sci. 2012, 343, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.W.; Du, P.; Chen, D.W.; Cui, L.; Ying, C.M. Effect of viable bifidobacterium supplement on the immune status and inflammatory response in patients undergoing resection for colorectal cancer. Zhonghua Wei Chang Wai Ke Za Zhi = Chin. J. Gastrointest. Surg. 2010, 13, 40–43. [Google Scholar]
- Xia, Y.; Yang, Z.; Chen, H.Q.; Qin, H.L. Effect of bowel preparation with probiotics on intestinal barrier after surgery for colorectal cancer. Zhonghua Wei Chang Wai Ke Za Zhi = Chin. J. Gastrointest. Surg. 2010, 13, 528–531. [Google Scholar]
- Horvat, M.; Krebs, B.; Potrc, S.; Ivanecz, A.; Kompan, L. Preoperative synbiotic bowel conditioning for elective colorectal surgery. Wien. Klin. Wochenschr. 2010, 122 (Suppl. 2), 26–30. [Google Scholar] [CrossRef]
- Gianotti, L.; Morelli, L.; Galbiati, F.; Rocchetti, S.; Coppola, S.; Beneduce, A.; Gilardini, C.; Zonenschain, D.; Nespoli, A.; Braga, M. A randomized double-blind trial on perioperative administration of probiotics in colorectal cancer patients. World J. Gastroenterol. 2010, 16, 167–175. [Google Scholar] [CrossRef]
- de Oliveira, A.L. Nutritional status and systemic inflammatory activity of colorectal patients on symbiotic supplementation. Arq. Bras. Cir. Dig. 2012, 25, 147–153. [Google Scholar] [CrossRef][Green Version]
- Carlini, M.; Grieco, M.; Spoletini, D.; Menditto, R.; Napoleone, V.; Brachini, G.; Mingoli, A.; Marcellinaro, R. Implementation of the gut microbiota prevents anastomotic leaks in laparoscopic colorectal surgery for cancer:The results of the miracle study. Updates Surg. 2022, 74, 1253–1262. [Google Scholar] [CrossRef]
- Consoli, M.L.; da Silva, R.S.; Nicoli, J.R.; Bruna-Romero, O.; da Silva, R.G.; de Vasconcelos Generoso, S.; Correia, M.I. Randomized clinical trial: Impact of oral administration of saccharomyces boulardii on gene expression of intestinal cytokines in patients undergoing colon resection. J. Parenter. Enter. Nutr. 2016, 40, 1114–1121. [Google Scholar] [CrossRef]
- Mangell, P.; Thorlacius, H.; Syk, I.; Ahrne, S.; Molin, G.; Olsson, C.; Jeppsson, B. Lactobacillus plantarum 299v does not reduce enteric bacteria or bacterial translocation in patients undergoing colon resection. Dig. Dis. Sci. 2012, 57, 1915–1924. [Google Scholar] [CrossRef]
- Tarvirdizade, K.; Taheri, S.; Asvadi Kermani, T.; Shahrasbi, M.; Kakaei, F. Assessment of probiotic effects on colorectal surgery complications: A double blinded, randomized clinical trial. Biomed. Res. Ther. 2019, 6, 3067–3072. [Google Scholar] [CrossRef]
- Worthley, D.L.; Le Leu, R.K.; Whitehall, V.L.; Conlon, M.; Christophersen, C.; Belobrajdic, D.; Mallitt, K.A.; Hu, Y.; Irahara, N.; Ogino, S.; et al. A human, double-blind, placebo-controlled, crossover trial of prebiotic, probiotic, and synbiotic supplementation: Effects on luminal, inflammatory, epigenetic, and epithelial biomarkers of colorectal cancer. Am. J. Clin. Nutr. 2009, 90, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Golkhalkhali, B.; Rajandram, R.; Paliany, A.S.; Ho, G.F.; Wan Ishak, W.Z.; Johari, C.S.; Chin, K.F. Strain-specific probiotic (microbial cell preparation) and omega-3 fatty acid in modulating quality of life and inflammatory markers in colorectal cancer patients: A randomized controlled trial. Asia Pac. J. Clin. Oncol. 2018, 14, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Li, C.; Huang, M.; Tong, C.; Zhang, X.; Wang, L.; Peng, H.; Lan, P.; Zhang, P.; Huang, N.; et al. Positive regulatory effects of perioperative probiotic treatment on postoperative liver complications after colorectal liver metastases surgery: A double-center and double-blind randomized clinical trial. BMC Gastroenterol. 2015, 15, 34. [Google Scholar] [CrossRef]
- Xu, Q.; Xu, P.; Cen, Y.; Li, W. Effects of preoperative oral administration of glucose solution combined with postoperative probiotics on inflammation and intestinal barrier function in patients after colorectal cancer surgery. Oncol. Lett. 2019, 18, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.Y.; Lee, K.T.; Lee, H.H.; Uen, Y.H.; Na, H.L.; Chao, F.T.; Chiu, C.C. The minimal clinically important difference in the gastrointestinal quality-of-life index after cholecystectomy. Surg. Endosc. 2009, 23, 2708–2712. [Google Scholar] [CrossRef]
- Chen, Y.; Qi, A.; Teng, D.; Li, S.; Yan, Y.; Hu, S.; Du, X. Probiotics and synbiotics for preventing postoperative infectious complications in colorectal cancer patients: A systematic review and meta-analysis. Tech. Coloproctol. 2022, 26, 425–436. [Google Scholar] [CrossRef]
- Ouyang, X.; Li, Q.; Shi, M.; Niu, D.; Song, W.; Nian, Q.; Li, X.; Ding, Z.; Ai, X.; Wang, J. Probiotics for preventing postoperative infection in colorectal cancer patients: A systematic review and meta-analysis. Int. J. Colorectal. Dis. 2019, 34, 459–469. [Google Scholar] [CrossRef]
- Chen, C.; Wen, T.; Zhao, Q. Probiotics used for postoperative infections in patients undergoing colorectal cancer surgery. Biomed. Res. Int. 2020, 2020, 5734718. [Google Scholar] [CrossRef]
- Shogan, B.D.; Belogortseva, N.; Luong, P.M.; Zaborin, A.; Lax, S.; Bethel, C.; Ward, M.; Muldoon, J.P.; Singer, M.; An, G.; et al. Collagen degradation and mmp9 activation by enterococcus faecalis contribute to intestinal anastomotic leak. Sci. Transl. Med. 2015, 7, 286ra268. [Google Scholar] [CrossRef]
- Okada, M.; Bothin, C.; Kanazawa, K.; Midtvedt, T. Experimental study of the influence of intestinal flora on the healing of intestinal anastomoses. Br. J. Surg. 1999, 86, 961–965. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Hart, A.L.; Kamm, M.A.; Stagg, A.J.; Knight, S.C. Mechanisms of action of probiotics: Recent advances. Inflamm. Bowel Dis. 2009, 15, 300–310. [Google Scholar] [CrossRef] [PubMed]
- Dos Reis, S.A.; da Conceicao, L.L.; Siqueira, N.P.; Rosa, D.D.; da Silva, L.L.; Peluzio, M.D. Review of the mechanisms of probiotic actions in the prevention of colorectal cancer. Nutr. Res. 2017, 37, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Amitay, E.L.; Carr, P.R.; Gies, A.; Laetsch, D.C.; Brenner, H. Probiotic/synbiotic treatment and postoperative complications in colorectal cancer patients: Systematic review and meta-analysis of randomized controlled trials. Clin. Transl. Gastroenterol. 2020, 11, e00268. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.D.; Xu, W.; Liu, M.M.; Hu, K.J.; Sun, Y.Y.; Yang, X.F.; Zhu, G.Q.; Wang, Z.W.; Huang, W. Efficacy of prophylactic probiotics in combination with antibiotics versus antibiotics alone for colorectal surgery: A meta-analysis of randomized controlled trials. J. Surg. Oncol. 2018, 117, 1394–1404. [Google Scholar] [CrossRef] [PubMed]
- He, D.; Wang, H.Y.; Feng, J.Y.; Zhang, M.M.; Zhou, Y.; Wu, X.T. Use of pro-/synbiotics as prophylaxis in patients undergoing colorectal resection for cancer: A meta-analysis of randomized controlled trials. Clin. Res. Hepatol. Gastroenterol. 2013, 37, 406–415. [Google Scholar] [CrossRef]
- Collinson, S.; Deans, A.; Padua-Zamora, A.; Gregorio, G.V.; Li, C.; Dans, L.F.; Allen, S.J. Probiotics for treating acute infectious diarrhoea. Cochrane Database Syst. Rev. 2020, 12, CD003048. [Google Scholar] [CrossRef]
- Liu, G.; Cao, S.; Liu, X.; Li, Z.; Tian, Y.; Zhang, X.; Zhong, H.; Zhou, Y. Effect of perioperative probiotic supplements on postoperative short-term outcomes in gastric cancer patients receiving neoadjuvant chemotherapy: A double-blind, randomized controlled trial. Nutrition 2022, 96, 111574. [Google Scholar] [CrossRef]
- Sommacal, H.M.; Bersch, V.P.; Vitola, S.P.; Osvaldt, A.B. Perioperative synbiotics decrease postoperative complications in periampullary neoplasms: A randomized, double-blind clinical trial. Nutr. Cancer 2015, 67, 457–462. [Google Scholar] [CrossRef]
- Chowdhury, A.H.; Adiamah, A.; Kushairi, A.; Varadhan, K.K.; Krznaric, Z.; Kulkarni, A.D.; Neal, K.R.; Lobo, D.N. Perioperative probiotics or synbiotics in adults undergoing elective abdominal surgery: A systematic review and meta-analysis of randomized controlled trials. Ann. Surg. 2020, 271, 1036–1047. [Google Scholar] [CrossRef]


| Study | Study Design/Setting | Trial Period (Year to Year) | Country /Language | Type of Surgery | Stage | Total Number of Analyzed Participant | Age (Mean ± Standard Deviation) | Treatment | Route | Duration of Administration | Duration of Follow-Up (Months) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | Intervention | Control | |||||||||
| Park 2020 [24] | RCT/multicenter | 2016 to 2018 | Korea/ English | sigmoid colon cancer resection (anterior resection) | I~III | 29 | 31 | 60.1 ± 10.37 | 61.03 ± 7.02 | probiotics (Bifidobacterium animalis, lactis, Lactobacillus casei, and Lactobacillus plantarum) | placebo | oral | 1 week before surgery to 21 days after surgery | 1 month |
| Polakowski 2019 [14] | RCT/single center | Brazil/ English | colorectal cancer resection | I~III | 36 | 37 | 60.9 ± 6.7 | 58.9 ± 6.3 | synbiotics (Lactobacillus acidophilus NCFM, L. rhamnosus HN001, L. casei LPC-37, and Bifidobacterium lactis HN019 + fructooligosaccharide) | placebo | oral | 8 days before surgery to the day before surgery | 1 month | |
| Bajramagic 2019 [25] | RCT/single center | 2017 to 2017 | Bosnia/ English | colorectal cancer resection | III | 39 | 39 | probiotics (Lactobacillus acidophilus, Lactobacillus casei, Lactobacillus plantarum, Lactobacillus rhamnosus, Bifidobacterium lactis, Bifidobacterium bifidum, Bifidobacterium breve, and Streptococcus thermophilus) | standard care | oral | 3 days after surgery to 30 days after surgery | 12 months | ||
| Flesche 2017 [26] | RCT/single center | 2013 to 2015 | Brazil/ English | colorectal cancer resection | I~IV | 49 | 42 | 64.5 a | 61.6 a | synbiotics (Lactobacillus acidophilus NCFM, L. rhamnosus HN001, L. paracasei LPC-37, and Bifidobacterium lactis HN019 + oligosaccharide) | placebo | oral | 5 days before surgery to 14 days after surgery | 1 month |
| Yang 2016 [15] | RCT/single center | 2011 to 2012 | China/ English | colorectal cancer resection | I~III | 30 | 30 | 63.90 ± 12.25 | 62.17 ± 11.06 | probiotics (Bifidobacterium longum, Lactobacillus acidophilus, and Enterococcus faecalis) | placebo | oral | 5 days before surgery to 7 days after surgery | 1 month |
| Theodoropoulos 2016 [27] | RCT/single center | 2008 to 2012 | Greece/ English | colorectal cancer resection | 0~IV | 34 | 33 | 66.8 ± 2.17 | 69 ± 1.37 | synbiotics (Pediococcus pentosaceus, Leuconostoc mesenteroides, Lactobacillus paracasei spp. paracasei, and Lactobacillus plantarum, and 2.5 g of each of the four fermentable fibers (prebiotics)) | placebo | oral | 15 days from 2 days after surgery | 6 months |
| Tan 2016 [16] | RCT/single center | 2012 to 2015 | Malaysia/ English | colorectal cancer resection | I~III | 20 | 20 | 64.3 ± 14.5 | 68 ± 11.9 | probiotics (Lactobacillus acidophilus, Lactobacillus casei, Lactobacillus lactis, Bifidobacterium bifidum, Bifidobacterium longum, and Bifidobacterium infantis) | placebo | oral | 8 days before surgery to the day before surgery | 1 month |
| Mizuta 2016 [28] | RCT/single center | 2008 to 2012 | Japan/ English | colorectal cancer resection | 31 | 29 | 68.9 ± 10.4 | 71.2 ± 9.5 | probiotics (Bifidobacterium longum) | standard care | oral | 7–14 days before surgery to 14 days after surgery | 2 weeks | |
| Krebs 2016 [29] | RCT/single center | 2009 to 2012 | Slovenia/ English | colorectal cancer resection | 18 | 16 | 62 (43~87) a | 67 (52~78) a | synbiotics (Pediacoccus pentosaceus, Leuconostoc mesenteroides, Lactobacillus paracasei, and Lactobacillus plantarum) | standard care | oral | 3 days before the surgery | 1 month | |
| Komatsu 2016 [17] | RCT/single center | 2008 to 2013 | Japan/ English | laparoscopic colorectal cancer resection | 0~IV | 168 | 194 | 66.7 ± 11.6 | 67.7 ± 10.7 | synbiotics (Lactobacillus casei, Bifidobacterium breve + galactooligosaccharides) | standard care | oral | 7–11 days before surgery to 2–7 days after surgery | 1 month |
| Kotzampassi 2016 [18] | RCT/single center | 2013 to 2014 | Greece/ English | colorectal cancer resection | 84 | 80 | 65.9 ± 11.5 | 66.4 ± 11.9 | probiotics (Lactobacillus acidophilus, Lactobacillus plantarum, Bifidobacterium lactis, and Saccharomyces boulardii)+K14 | placebo | oral | the day of surgery to 14 days after surgery | 1 month | |
| Sadahiro 2014 [30] | RCT/single center | 2008 to 2011 | Japan/ English | colon cancer resection | I~III | 100 | 95 | 67 ± 9 | 66 ± 12 | probiotics (Bifidobacteria) | standard care | oral | 7 days before surgery to 5–10 days after surgery | 1 month |
| Huanlongqin 2014 [31] | RCT/single center | 2011 to 2011 | China/ Chinese | colorectal cancer resection | I~III | 30 | 30 | 59.8 ± 18.7 | 60.3 ± 17.2 | probiotics (lactic acid bacteria) | placebo | oral | 5 days before surgery to 7 days after surgery | 1 month |
| Pellino 2013 [32] | RCT/single center | 2005 to 2012 | Italy/ English | laparoscopic colon cancer resection | 10 | 8 | 71.5 ± 2.1 | 72.9 ± 1.6 | probiotics (Streptococcus thermophilus, Bifidobacteria, Lactobacillus acidophilus, L. plantarum, L. paracasei, and L. delbrueckii subsp. Bulgaricus) | placebo | oral | 1 day after discontinuation of antibiotics to 4 weeks | 1 month | |
| Liu 2013 [33] | RCT/multicenter | 2007 to 2011 | China/ English | colorectal cancer resection | I~III | 75 | 75 | 62.28 ± 12.41 | 66.06 ± 11.02 | probiotics (Lactobacillus plantarum, Lactobacillus acidophilus, and Bifidobacterium longum) | placebo | oral | 6 days before surgery to 10 days after surgery | 1 month |
| Zhang 2012 [34] | RCT/single center | 2006 to 2007 | China/ English | colorectal cancer resection | I~III | 30 | 30 | 67.5 (45.0~87.0) a | 61.5 (46.0~82.0) a | probiotics (B. longum, L. acidophilus and Enterococcus faecalis) | placebo | oral | 5 days before surgery to 3 days before surgery | 1 month |
| Horvat 2010 [37] | RCT/single center | Slovenia/ English | colon cancer resection | 20 | 20 | 62 (42~86) a | 65 (52~78) a | synbiotics (Pediococcus pentosaceus, Leuconostoc mesenteroides, Lactobacillus paracasei subsp. Paracasei, and Lactobacillus plantarum) | standard care | oral | 3 days before the surgery | 1 month | ||
| Xia Yang 2010 [36] | RCT/single center | 2008 to 2008 | China/ Chinese | colorectal cancer resection | 30 | 30 | probiotics (sour milk, lactic acid bacteria) | standard care | oral | more than 5 days until the day before surgery | 1 month | |||
| Zhang 2010 [35] | RCT/single center | 2006 to 2007 | China/ Chinese | colorectal cancer resection | 30 | 30 | 66.7 (41~83) a | 63.0 (39~81) a | probiotics (Bifidobacterium) | standard care | oral | for 5 days before the surgery | 1 month | |
| Gianotti 2010 [38] | RCT/muti center (two) | 2006 to 2007 | Italy/ English | colorectal cancer resection | 21 | 10 | 63.3 ± 102 | 62.7 ± 7.8 | Probiotics (Lactobacillus johnsonii, Bifidobacterium longum) | placebo | oral | 3 days before the surgery | 1 month | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
An, S.; Kim, K.; Kim, M.H.; Jung, J.H.; Kim, Y. Perioperative Probiotics Application for Preventing Postoperative Complications in Patients with Colorectal Cancer: A Systematic Review and Meta-Analysis. Medicina 2022, 58, 1644. https://doi.org/10.3390/medicina58111644
An S, Kim K, Kim MH, Jung JH, Kim Y. Perioperative Probiotics Application for Preventing Postoperative Complications in Patients with Colorectal Cancer: A Systematic Review and Meta-Analysis. Medicina. 2022; 58(11):1644. https://doi.org/10.3390/medicina58111644
Chicago/Turabian StyleAn, Sanghyun, Kwangmin Kim, Myung Ha Kim, Jae Hung Jung, and Youngwan Kim. 2022. "Perioperative Probiotics Application for Preventing Postoperative Complications in Patients with Colorectal Cancer: A Systematic Review and Meta-Analysis" Medicina 58, no. 11: 1644. https://doi.org/10.3390/medicina58111644
APA StyleAn, S., Kim, K., Kim, M. H., Jung, J. H., & Kim, Y. (2022). Perioperative Probiotics Application for Preventing Postoperative Complications in Patients with Colorectal Cancer: A Systematic Review and Meta-Analysis. Medicina, 58(11), 1644. https://doi.org/10.3390/medicina58111644