
Endosonography-Guided Versus Percutaneous Gallbladder Drainage Versus Cholecystectomy in Fragile Patients with Acute Cholecystitis—A High-Volume Center Study

 ,
,  , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Outcomes Definitions
2.2. Procedures
2.3. Statistical Analysis
3. Results
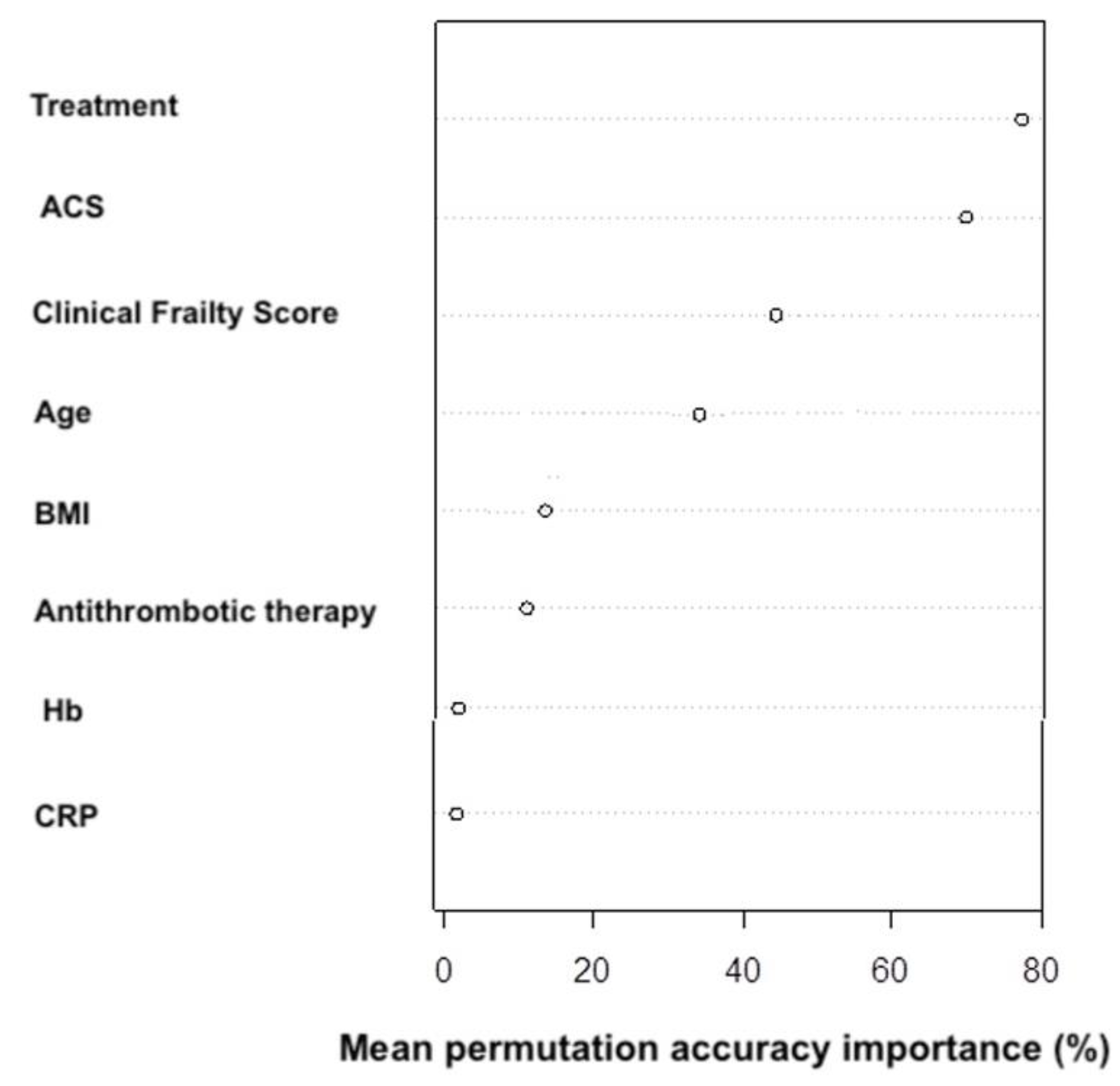
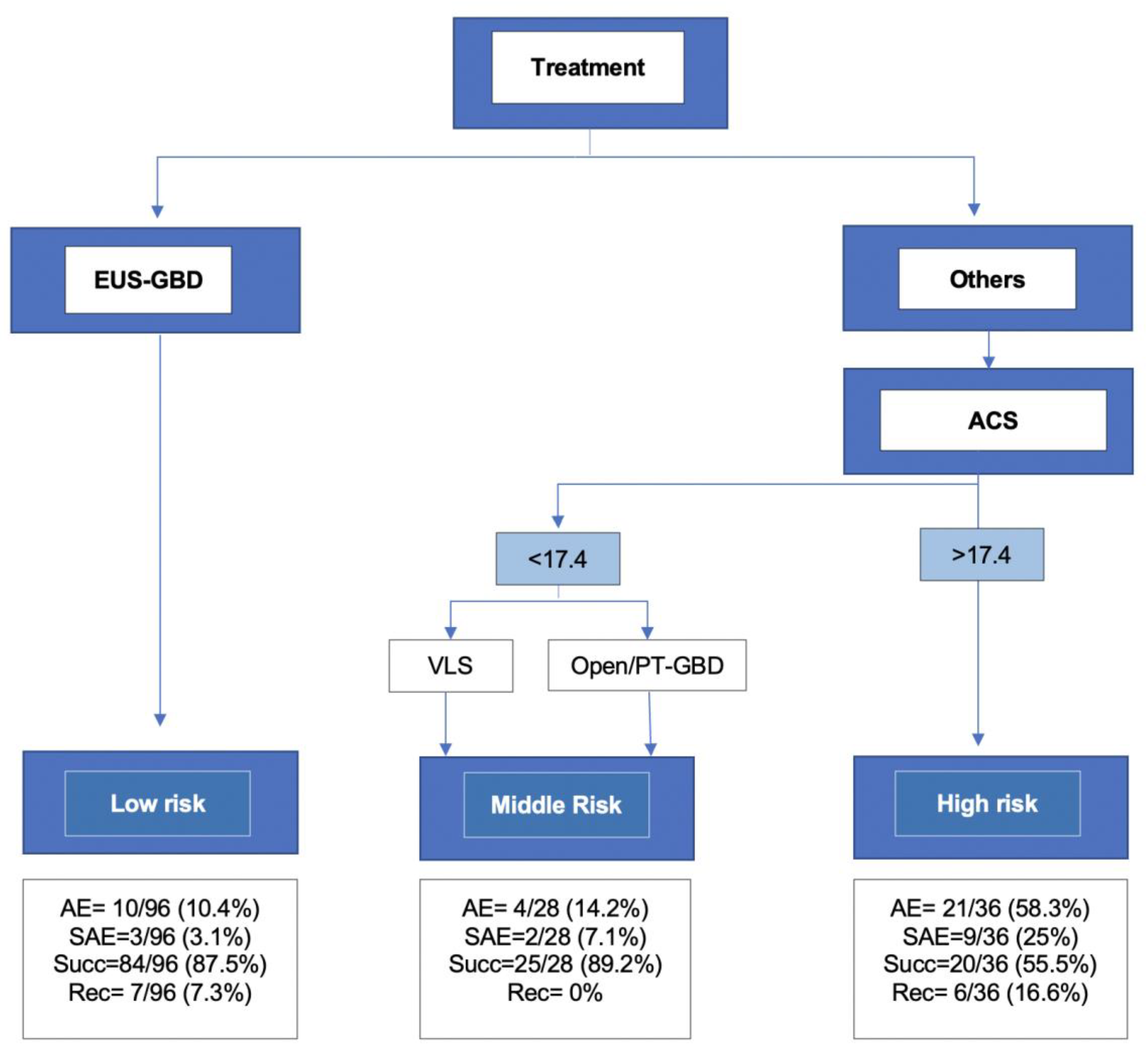
3.1. Recursive Partitioning Analysis
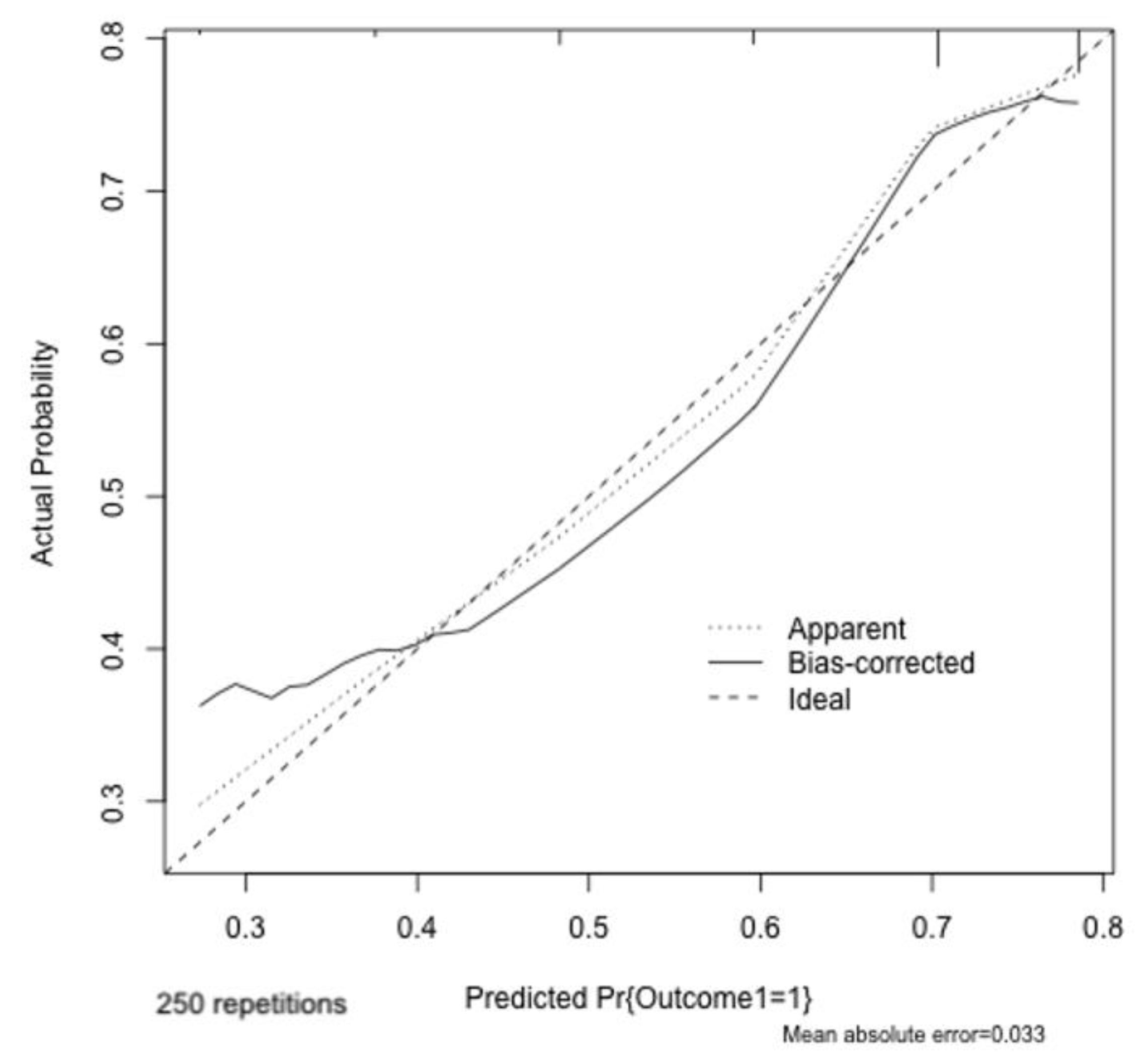
3.2. Performance of the Model and Validation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Miura, F.; Okamoto, K.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Pitt, H.A.; Gomi, H.; Solomkin, J.; Schlossberg, D.; Han, H.-S.; et al. Tokyo Guidelines 2018: Initial management of acute biliary infection and flowchart for acute cholangitis. J. Hepato-Biliary-Pancreat. Sci. 2017, 25, 31–40. [Google Scholar] [CrossRef]
- Yokoe, M.; Hata, J.; Takada, T.; Strasberg, S.M.; Bun, T.A.Y.; Wakabayashi, G.; Kozaka, K.; Endo, I.; DeZiel, D.J.; Miura, F.; et al. Tokyo Guidelines 2018: Diagnostic criteria and severity grading of acute cholecystitis (with videos). J. Hepato-Biliary-Pancreat. Sci. 2017, 25, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Pisano, M.; Ceresoli, M.; Cimbanassi, S.; Gurusamy, K.; Coccolini, F.; Borzellino, G.; Costa, G.; Allievi, N.; Amato, B.; Boerma, D.; et al. 2017 WSES and SICG guidelines on acute calcolous cholecystitis in elderly population. World J. Emerg. Surg. 2019, 14, 10. [Google Scholar] [CrossRef] [PubMed]
- Loozen, C.S.; van Santvoort, H.C.; van Duijvendijk, P.; Besselink, M.G.; Gouma, D.J.; Nieuwenhuijzen, G.A.; Kelder, C.J.; Donkervoort, S.C.; van Geloven, A.A.W.; Kruyt, P.M.; et al. Laparoscopic cholecystectomy versus percutaneous catheter drainage for acute cholecystitis in high risk patients (CHOCOLATE): Multicentre randomised clinical trial. BMJ 2018, 2018, 3965. [Google Scholar] [CrossRef] [PubMed]
- Teoh, A.Y.B.; Kitano, M.; Itoi, T.; Pérez-Miranda, M.; Ogura, T.; Chan, S.M.; Serna-Higuera, C.; Omoto, S.; Torres-Yuste, R.; Tsuichiya, T.; et al. Endosonography-guided gallbladder drainage versus percutaneous cholecystostomy in very high-risk surgical patients with acute cholecystitis: An international randomised multicentre controlled superiority trial (DRAC 1). Gut 2020, 69, 1085–1091. [Google Scholar] [CrossRef]
- Teoh, A.Y.B.; Leung, C.H.; Tam, P.T.H.; Yeung, K.K.Y.A.; Mok, R.C.Y.; Chan, D.L.; Chan, S.M.; Yip, H.C.; Chiu, P.W.Y.; Ng, E.K.W. EUS-guided gallbladder drainage versus laparoscopic cholecystectomy for acute cholecystitis: A propensity score analysis with 1-year follow-up data. Gastrointest. Endosc. 2020, 93, 577–583. [Google Scholar] [CrossRef]
- Pisano, M.; Allievi, N.; Gurusamy, K.; Borzellino, G.; Cimbanassi, S.; Boerna, D.; Coccolini, F.; Tufo, A.; Di Martino, M.; Leung, J.; et al. 2020 World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis. World J. Emerg. Surg. 2020, 15, 61. [Google Scholar] [CrossRef]
- Bilimoria, K.Y.; Liu, Y.; Paruch, J.L.; Zhou, L.; Kmiecik, T.E.; Ko, C.Y.; Cohen, M.E. Development and Evaluation of the Universal ACS NSQIP Surgical Risk Calculator: A Decision Aid and Informed Consent Tool for Patients and Surgeons. J. Am. Coll. Surg. 2013, 217, 833–842.e3. [Google Scholar] [CrossRef]
- Church, S.; Rogers, E.; Rockwood, K.; Theou, O. A scoping review of the Clinical Frailty Scale. BMC Geriatr. 2020, 20, 393. [Google Scholar] [CrossRef]
- Fugazza, A.; Colombo, M.; Repici, A.; Anderloni, A. Endoscopic Ultrasound-Guided Gallbladder Drainage: Current Perspectives. Clin. Exp. Gastroenterol. 2020, 13, 193–201. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of Surgical Complications: A New Proposal With Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Coccolini, F.; Catena, F.; Pisano, M.; Gheza, F.; Fagiuoli, S.; Di Saverio, S.; Leandro, G.; Montori, G.; Ceresoli, M.; Corbella, D.; et al. Open versus laparoscopic cholecystectomy in acute cholecystitis. Systematic review and meta-analysis. Int. J. Surg. 2015, 18, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Rerknimitr, R.; Pham, K.C. Practical Approaches for High-Risk Surgical Patients with Acute Cholecystitis: The Percutaneous Approach versus Endoscopic Alternatives. Clin. Endosc. 2020, 53, 678–685. [Google Scholar] [CrossRef]
- Fugazza, A.; Sethi, A.; Trindade, A.J.; Troncone, E.; Devlin, J.; Khashab, M.A.; Vleggaar, F.P.; Bogte, A.; Tarantino, I.; Deprez, P.H.; et al. International multicenter comprehensive analysis of adverse events associated with lumen-apposing metal stent placement for pancreatic fluid collection drainage. Gastrointest. Endosc. 2019, 91, 574–583. [Google Scholar] [CrossRef]
- Facciorusso, A.; Di Maso, M.; Antonino, M.; Del Prete, V.; Panella, C.; Barone, M.; Muscatiello, N. Polidocanol injection decreases the bleeding rate after colon polypectomy: A propensity score analysis. Gastrointest. Endosc. 2015, 82, 350–358.e2. [Google Scholar] [CrossRef] [PubMed]
- McCaffrey, D.F.; Griffin, B.A.; Almirall, D.; Slaughter, M.E.; Ramchand, R.; Burgette, L.F. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat. Med. 2013, 32, 3388–3414. [Google Scholar] [CrossRef]
- Austin, P.C. The performance of different propensity score methods for estimating marginal hazard ratios. Stat. Med. 2012, 32, 2837–2849. [Google Scholar] [CrossRef]
- Strobl, C.; Malley, J.; Tutz, G. An introduction to recursive partitioning: Rationale, application, and characteristics of classification and regression trees, bagging, and random forests. Psychol. Methods 2009, 14, 323–348. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Harrell, F.E.; Borsboom, G.J.; Eijkemans, M.; Vergouwe, Y.; Habbema, J.F. Internal validation of predictive models: Efficiency of some procedures for logistic regression analysis. J. Clin. Epidemiol. 2001, 54, 774–781. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Hosmer, T.; Le Cessie, S.; Lemeshow, S. A comparison of goodness-of-fit tests for the logistic regression model. Stat. Med. 1997, 15, 965–980. [Google Scholar] [CrossRef]
- McKay, A.; Abulfaraj, M.; Lipschitz, J. Short- and long-term outcomes following percutaneous cholecystostomy for acute cholecystitis in high-risk patients. Surg. Endosc. 2011, 26, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Markopoulos, G.; Mulita, F.; Kehagias, D.; Tsochatzis, S.; Lampropoulos, C.; Kehagias, I. Outcomes of percutaneous cholecystostomy in elderly patients: A systematic review and meta-analysis. Gastroenterol. Rev. 2020, 15, 188–195. [Google Scholar] [CrossRef]
- Dimou, F.M.; Adhikari, D.; Mehta, H.B.; Riall, T.S. Outcomes in Older Patients with Grade III Cholecystitis and Cholecystostomy Tube Placement: A Propensity Score Analysis. J. Am. Coll. Surg. 2017, 224, 502–511e1. [Google Scholar] [CrossRef]
- Anderloni, A.; Buda, A.; Vieceli, F.; Khashab, M.A.; Hassan, C.; Repici, A. Endoscopic ultrasound-guided transmural stenting for gallbladder drainage in high-risk patients with acute cholecystitis: A systematic review and pooled analysis. Surg. Endosc. 2016, 30, 5200–5208. [Google Scholar] [CrossRef] [PubMed]
- Mussetto, A.; Anderloni, A. Through the LAMS towards the future: Current uses and outcomes of lumen-apposing metal stents. Ann. Gastroenterol. 2018, 31, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Luk, S.W.-Y.; Irani, S.; Krishnamoorthi, R.; Lau, J.Y.W.; Ng, E.K.W.; Teoh, A.Y.-B. Endoscopic ultrasound-guided gallbladder drainage versus percutaneous cholecystostomy for high risk surgical patients with acute cholecystitis: A systematic review and meta-analysis. Endoscopy 2019, 51, 722–732. [Google Scholar] [CrossRef]
- Choi, J.H.; Lee, S.; Choi, J.; Park, D.; Seo, D.W.; Lee, S.; Kim, M.H. Long-term outcomes after endoscopic ultrasonography-guided gallbladder drainage for acute cholecystitis. Endoscopy 2014, 30, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Fleming, C.A.; Ismail, M.; Kavanagh, R.G.; Heneghan, H.M.; Prichard, R.S.; Geoghegan, J.; Brophy, D.P.; McDermott, E.W. Clinical and Survival Outcomes Using Percutaneous Cholecystostomy Tube Alone or Subsequent Interval Cholecystectomy to Treat Acute Cholecystitis. J. Gastrointest. Surg. 2019, 24, 627–632. [Google Scholar] [CrossRef]
- Anderloni, A.; Attili, F.; Sferrazza, A.; Rimbaș, M.; Costamagna, G.; Repici, A.; Larghi, A. EUS-guided gallbladder drainage using a lumen-apposing self-expandable metal stent in patients with coagulopathy or anticoagulation therapy: A case series. Endosc. Int. Open 2017, 5, E1100–E1103. [Google Scholar] [CrossRef][Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 163) | PT-GBD (n = 33) | EUS-GBD (n = 21) | LC (n = 81) | OC (n = 25) | p Value |
|---|---|---|---|---|---|---|
| Age Median (IQR) | 77 (71–82) | 83 (75–87) | 84 (81–89) | 74 (70–79) | 74 (69–80) | <0.001 |
| Male No (%) | 90 (56%) | 12 (36%) | 10 (48%) | 51 (63%) | 17 (68%) | 0.03 |
| BMI Median (IQR) | 26.2 (24.2–29.1) | 26.7 (23.6–29.6) | 25.8 (21.6–28) | 25.8 (24.3–25.8) | 27.3 (25.2–31.2) | 0.24 |
| Clinical Fraility Scale Score (median [range]) | 3.00 [1.00, 8.00] | 6.00 [2.00, 8.00] | 4.00 [2.00, 8.00] | 3.00 [1.00, 8.00] | 3.00 [2.00, 7.00] | <0.001 |
| ACS score Median (IQR) | 6.45 (3.88–17.02) | 17.6 (16.4,23) | 6.1 (5.3–7.3) | 4 (2.8–6) | 17.5 (12.9–20.6) | <0.001 |
| Non operative management (NOM) failure | 36 (22.5) | 17 (51.5) | 4 (19.0) | 11 (13.6) | 4 (16.0) | <0.001 |
| Previous AC No (%) | 41 (26%) | 12 (38%) | 8 (38%) | 17 (21%) | 4 (16%) | 0.10 |
| Previous ERCP No (%) | 17 (11%) | 3 (9%) | 6 (29%) | 7 (9%) | 1 (4%) | 0.12 |
| Anticoagulant therapy No (%) | 47 (29%) | 10 (30%) | 12 (57%) | 18 (22%) | 7 (28%) | 0.02 |
| WBC No (×1000) | 12 (8.5–16.5) | 6.9 (0.7–16.1) | 14.7 (7.5–17.1) | 12.6 (10.4–17) | 11.7 (10.7–14.4) | 0.02 |
| Hb [g/dl] Median (IQR) | 12.9 (10.3–13.4) | NR | NR | 13.1 (10.3–14.2) | 12.4 (11–14.3) | 0.11 |
| CRP [mg/dl] Median (IQR) | 11.5 (4–22.7) | 15 (11.2–24) | 6.15 (1.87–25) | 8.32 (2.4–19.1) | 13.5 (7.16–24.8) | 0.04 |
| Total Bilirubin [mg/dl] Median (IQR) | 1.2 (0.73–2) | 1.2 (0.7–2.4) | 1.1 (0.62–1.53) | 1.32 (0.88–2.08) | 0.9 (0.68–1.87) | 0.43 |
| INR Median (IQR) | 1.21 (1.1–1.37) | 1.32 (1.21–1.69) | 1.23 (1.1–1.36) | 1.15 (1.07–1.31) | 1.2 (1.13–1.29) | 0.008 |
| Total (163 pts) | PT- GBD (n = 33) | EUS-GBD (n = 21) | LC (n= 81) | OC (n = 25) | ||
|---|---|---|---|---|---|---|
| Technical Success (TS) No (%) | 162 (99) | 33 (100) | 20 (95) | 81 (100) | 25 (100) | 0.084 |
| Clinical success (CS) No (%) | 124 (78) | 21 (64) | 18 (85) | 69 (85) | 16 (64) | 0.02 |
| Recurrence Rate (RR) No (%) | 11 (9) | 7 (24) | 3 (14) | 0 | 1 (4) | <0.001 |
| Adverse event rate No (%) | 41 (26) | 13 (9) | 2 (10) | 13 (16) | 13 (52) | <0.001 |
| Severe Adverse Event rate No (%) | 17 (11) | 9 (27) | 0 | 2 (2) | 4 (16) | 0.001 |
| Type of adverse event | ||||||
| Drainage Displacement No (%) | 6 (12) | 5 (18) | 0 | - | - | NC |
| Sepsis/Septic Shock No (%) | 8 (19) | 4 (12) | 1 (5) | 2 (2) | 2 (8) | NC |
| Cystic duct obstruction No (%) | 1 (2) | 1 (3) | - | NC | ||
| .cBiliary leak No (%) | 6 (15) | 1 * (3) | - | - | 5 * (20) | NC |
| Cholangitis No (%) | 1 (2) | - | - | - | 1 (4) | NC |
| Medical complications (cardiological, respiratory, renal failure) No (%) | 17 (41) | 1 (3) | 1 (5) | 6 (7) | 4 (16) | NC |
| Lenght of stay (day) (median [range]) | 6.00 [1.00, 167.69] | 15.26 [5.00, 57.53] | 5.00 [1.00, 167.69] | 4.61 [1.12, 70.90] | 8.12 [3.00, 53.82] | <0.001 |
| 90-Day mortality No (%) | 5 (4) | 3 (27) | - | 2 (2) | 0 (0) | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurihara, H.; Bunino, F.M.; Fugazza, A.; Marrano, E.; Mauri, G.; Ceolin, M.; Lanza, E.; Colombo, M.; Facciorusso, A.; Repici, A.; et al. Endosonography-Guided Versus Percutaneous Gallbladder Drainage Versus Cholecystectomy in Fragile Patients with Acute Cholecystitis—A High-Volume Center Study. Medicina 2022, 58, 1647. https://doi.org/10.3390/medicina58111647
Kurihara H, Bunino FM, Fugazza A, Marrano E, Mauri G, Ceolin M, Lanza E, Colombo M, Facciorusso A, Repici A, et al. Endosonography-Guided Versus Percutaneous Gallbladder Drainage Versus Cholecystectomy in Fragile Patients with Acute Cholecystitis—A High-Volume Center Study. Medicina. 2022; 58(11):1647. https://doi.org/10.3390/medicina58111647
Chicago/Turabian StyleKurihara, Hayato, Francesca M. Bunino, Alessandro Fugazza, Enrico Marrano, Giulia Mauri, Martina Ceolin, Ezio Lanza, Matteo Colombo, Antonio Facciorusso, Alessandro Repici, and et al. 2022. "Endosonography-Guided Versus Percutaneous Gallbladder Drainage Versus Cholecystectomy in Fragile Patients with Acute Cholecystitis—A High-Volume Center Study" Medicina 58, no. 11: 1647. https://doi.org/10.3390/medicina58111647
APA StyleKurihara, H., Bunino, F. M., Fugazza, A., Marrano, E., Mauri, G., Ceolin, M., Lanza, E., Colombo, M., Facciorusso, A., Repici, A., & Anderloni, A. (2022). Endosonography-Guided Versus Percutaneous Gallbladder Drainage Versus Cholecystectomy in Fragile Patients with Acute Cholecystitis—A High-Volume Center Study. Medicina, 58(11), 1647. https://doi.org/10.3390/medicina58111647