
Effects of Probiotic Supplementation on Immune and Inflammatory Markers in Athletes: A Meta-Analysis of Randomized Clinical Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Eligibility Criteria
2.3. Data Selection and Extraction
2.4. Outcomes
2.5. Assessment of Risk of Bias
2.6. Statistical Analysis
3. Results
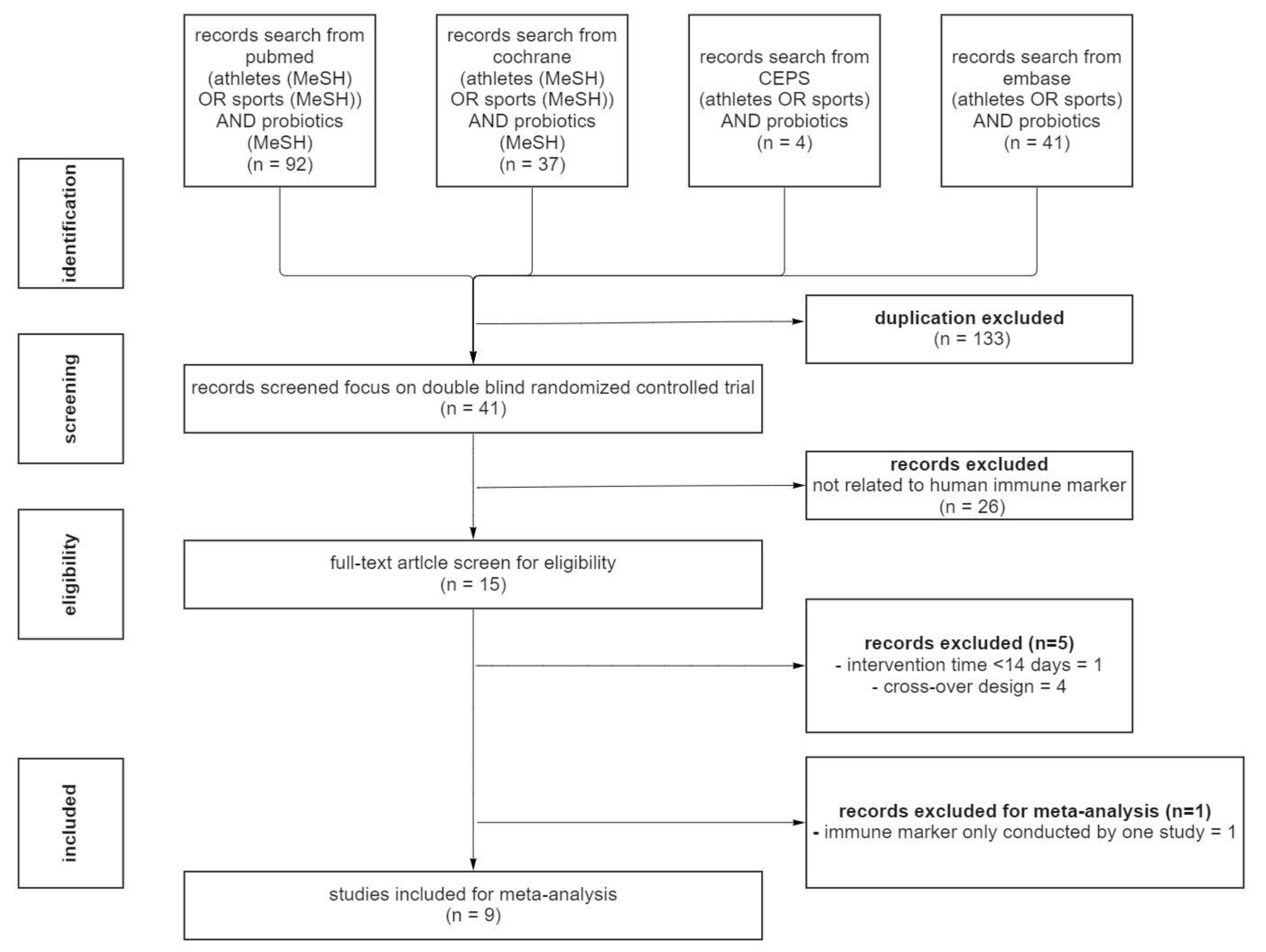
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Inflammatory-Related Markers
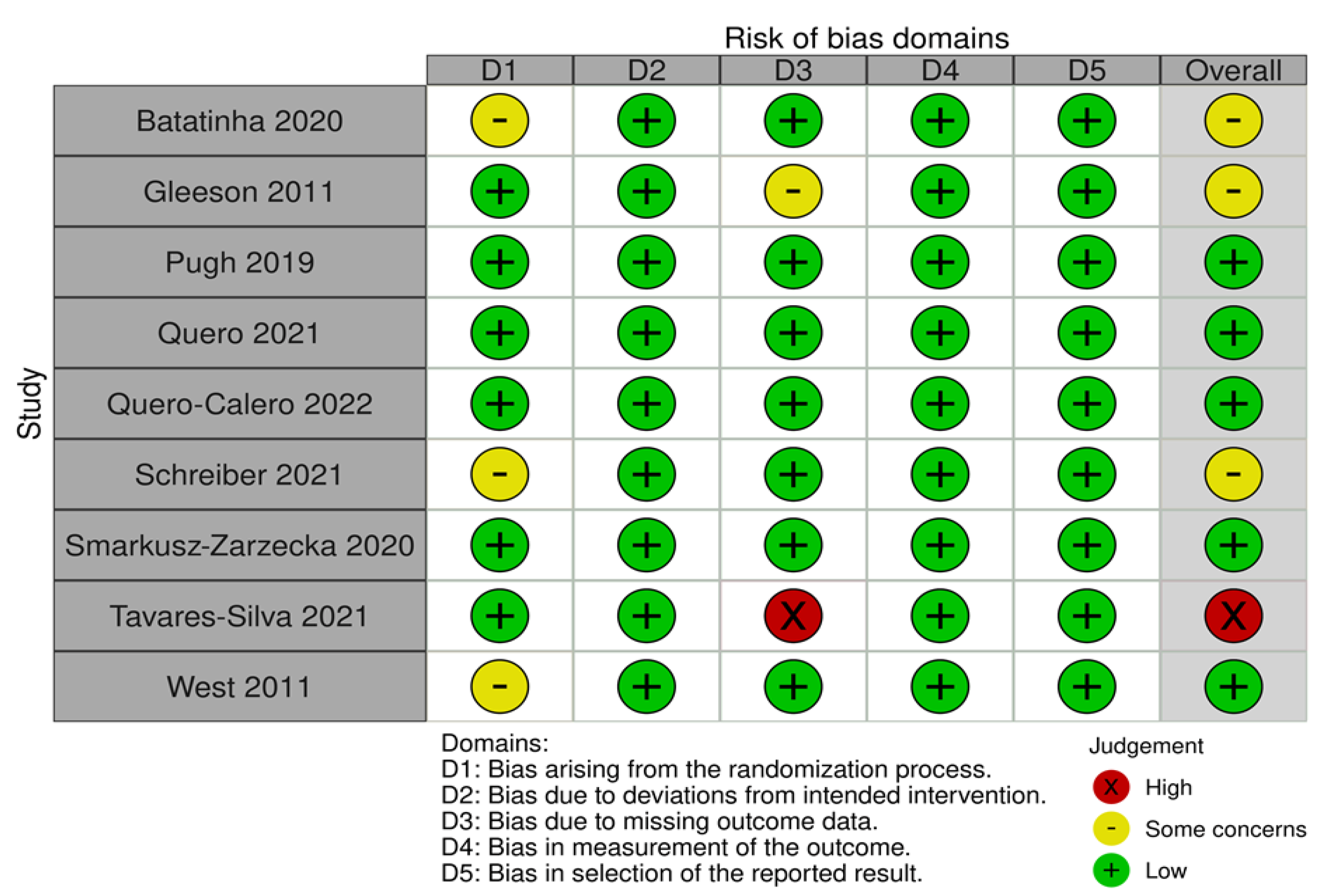
3.4. RoB 2.0 Assessment
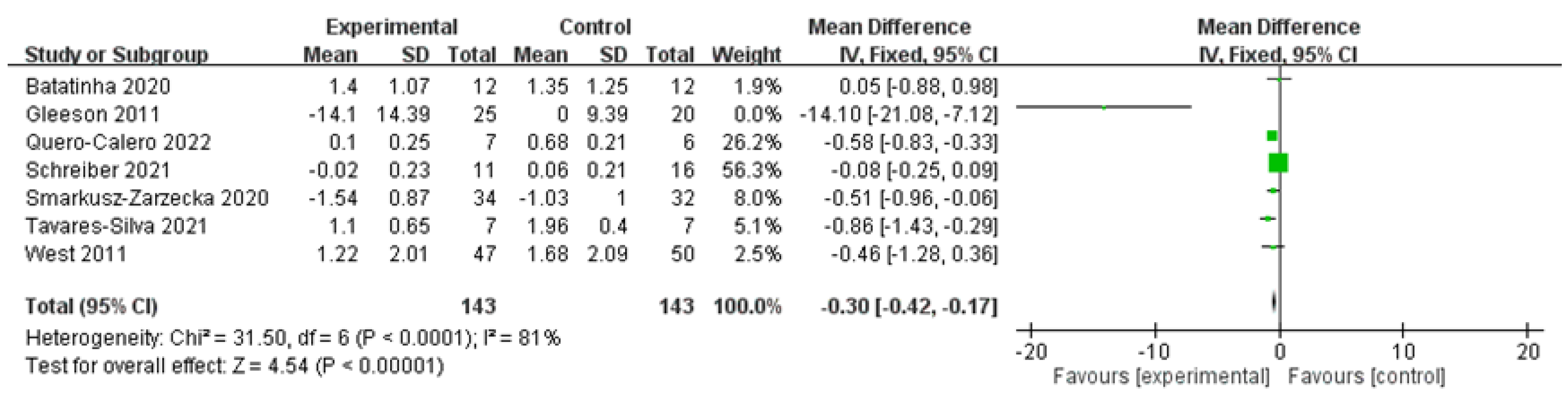
3.5. Overall Effects
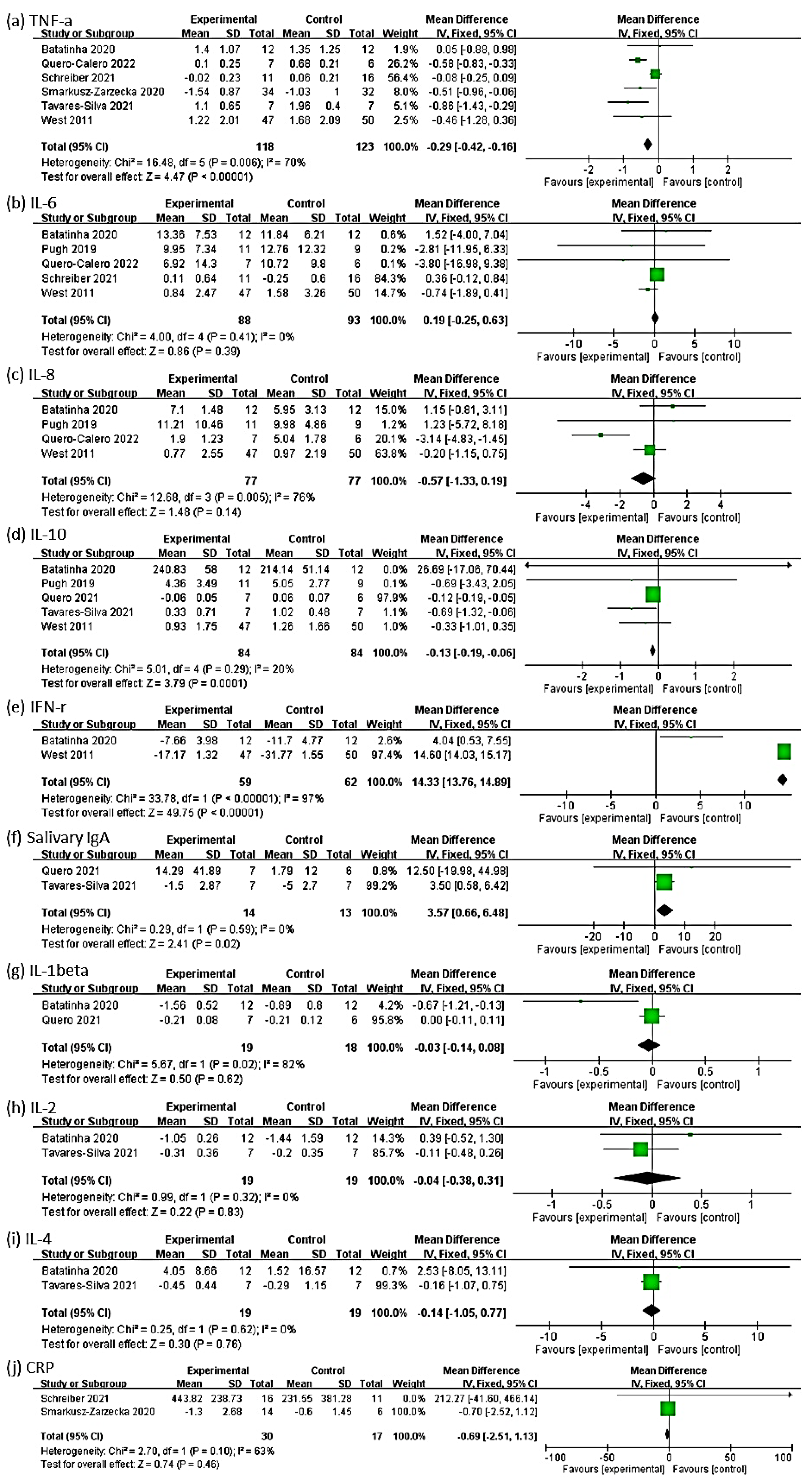
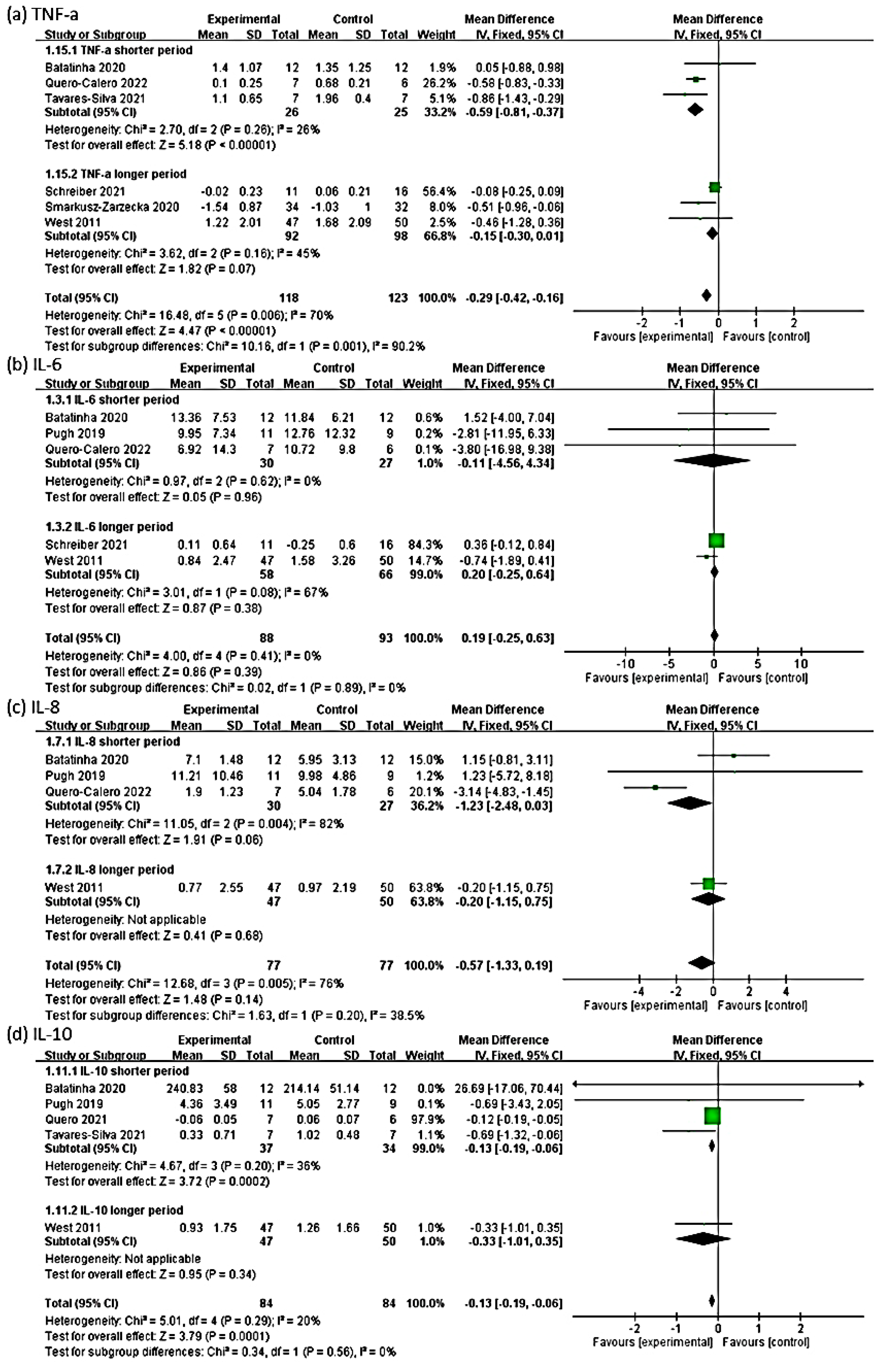
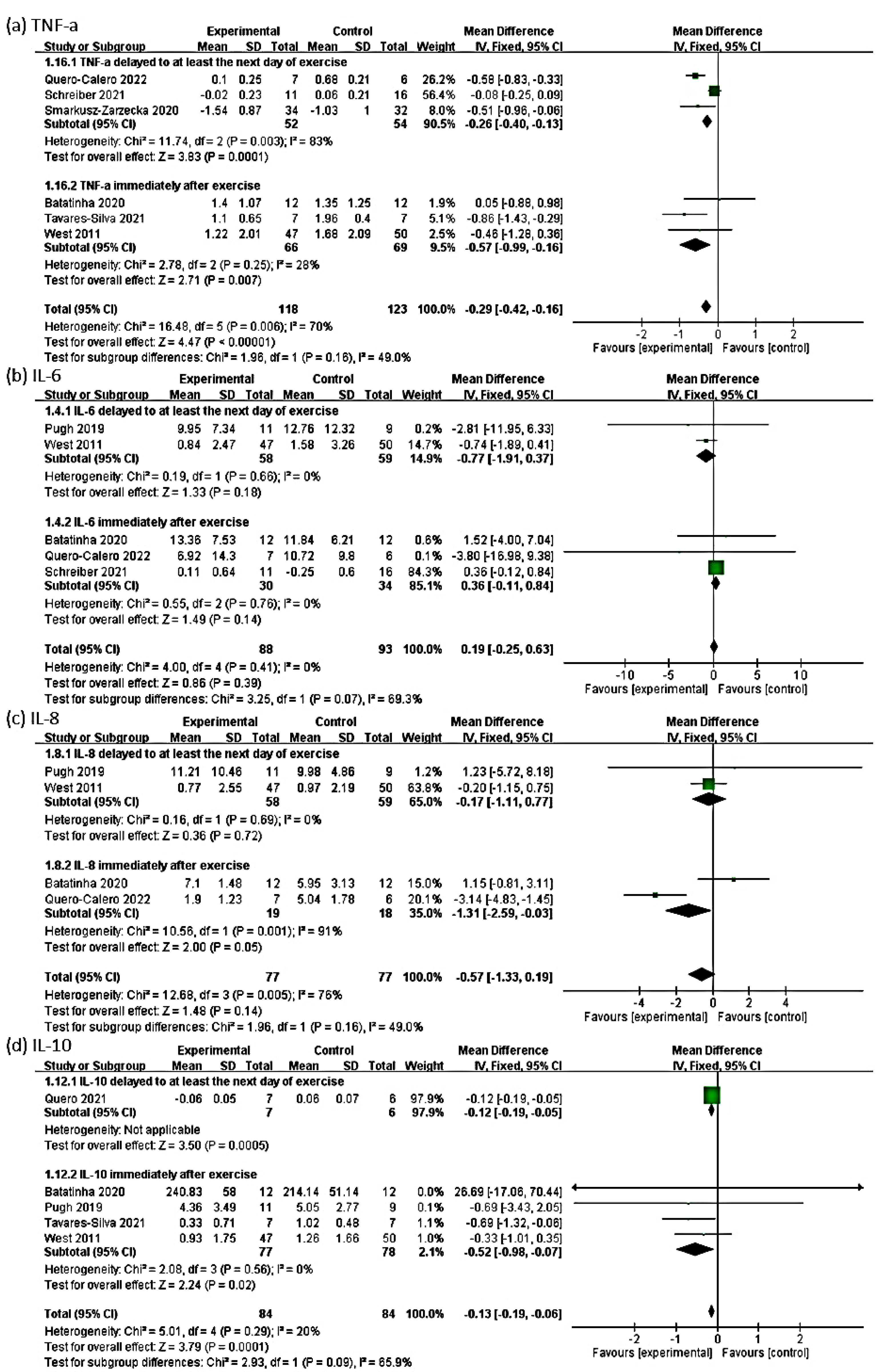
3.6. Outcome of TNF-α
3.7. Outcome of IL-6
3.8. Outcome of IL-8
3.9. Outcome of IL-10
3.10. Outcome of IFN-γ
3.11. Outcome of Salivary IgA
3.12. Outcome of IL-1β
3.13. Outcome of IL-2
3.14. Outcome of IL-4
3.15. Outcome of CRP
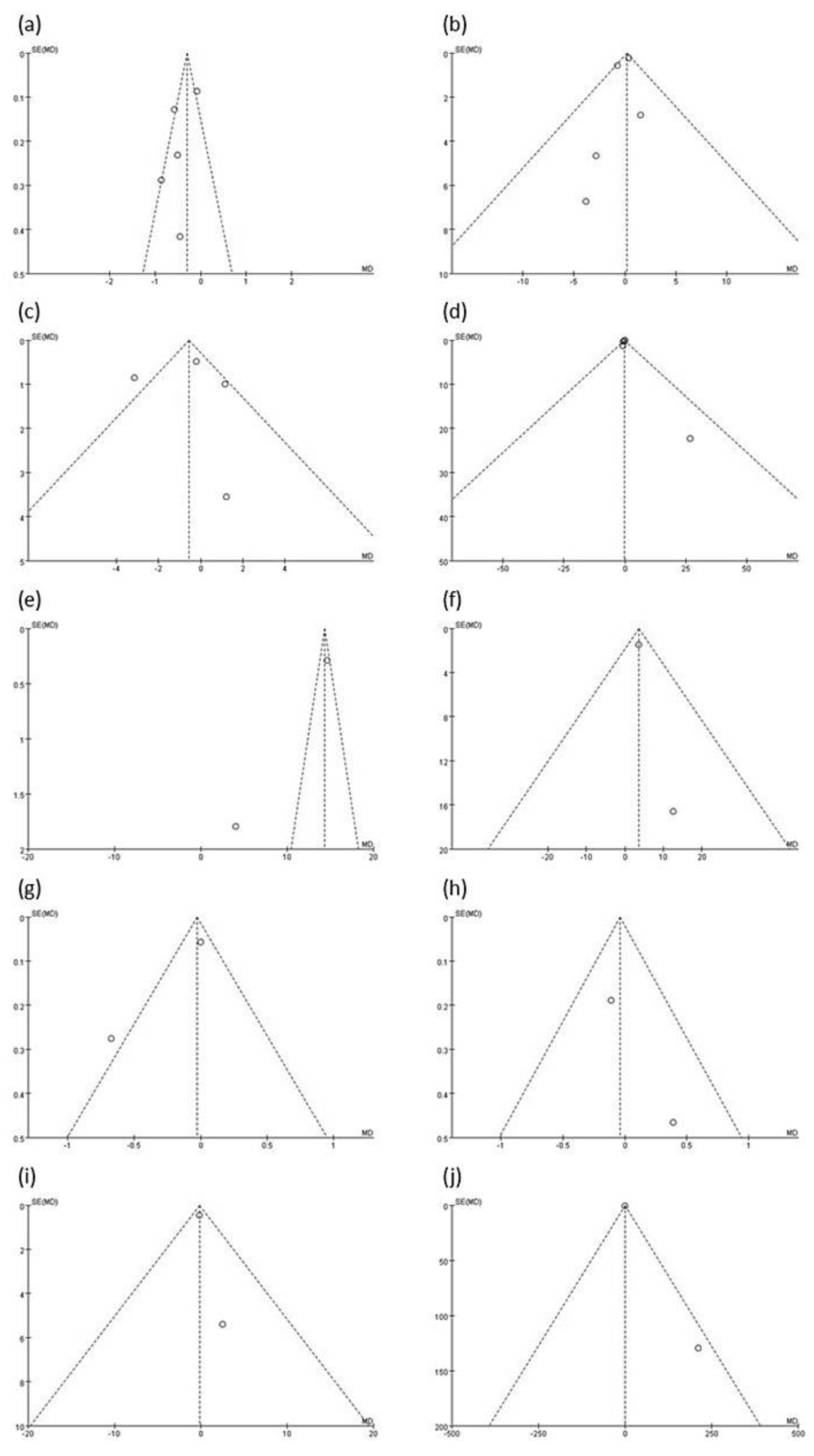
3.16. Publication Bias
4. Discussion
4.1. Overall Effect
4.2. Proinflammatory Markers: IL-1β, IL-2, IL-4, IL-6, IL-8, TNF-α, and CRP
4.3. Anti-Inflammatory Markers: IL-10 and IFN-γ
4.4. Salivary IgA
4.5. Heterogeneity
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Costa, R.J.S.; Snipe, R.M.J.; Kitic, C.M.; Gibson, P.R. Systematic review: Exercise-induced gastrointestinal syndrome-implications for health and intestinal disease. Aliment. Pharmacol. Ther. 2017, 46, 246–265. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M. Mucosal immunity and respiratory illness in elite athletes. Int. J. Sports Med. 2000, 21 (Suppl. 1), 33–43. [Google Scholar] [CrossRef] [PubMed]
- ter Steege, R.W.; Kolkman, J.J. Review article: The pathophysiology and management of gastrointestinal symptoms during physical exercise, and the role of splanchnic blood flow. Aliment. Pharmacol. Ther. 2012, 35, 516–528. [Google Scholar] [CrossRef] [PubMed]
- Lang, J.A.; Gisolfi, C.V.; Lambert, G.P. Effect of exercise intensity on active and passive glucose absorption. Int. J. Sport Nutr. Exerc. Metab. 2006, 16, 485–493. [Google Scholar] [CrossRef]
- Hong, S.; Mills, P.J. Effects of an exercise challenge on mobilization and surface marker expression of monocyte subsets in individuals with normal vs. elevated blood pressure. Brain Behav. Immun. 2008, 22, 590–599. [Google Scholar] [CrossRef]
- Simpson, R.J.; McFarlin, B.K.; McSporran, C.; Spielmann, G.; Hartaigh, B.O.; Guy, K. Toll-like receptor expression on classic and pro-inflammatory blood monocytes after acute exercise in humans. Brain Behav. Immun. 2009, 23, 232–239. [Google Scholar] [CrossRef]
- Shing, C.M.; Peake, J.M.; Lim, C.L.; Briskey, D.; Walsh, N.P.; Fortes, M.B.; Ahuja, K.D.; Vitetta, L. Effects of probiotics supplementation on gastrointestinal permeability, inflammation and exercise performance in the heat. Eur. J. Appl. Physiol. 2014, 114, 93–103. [Google Scholar] [CrossRef]
- West, N.P.; Pyne, D.B.; Cripps, A.W.; Hopkins, W.G.; Eskesen, D.C.; Jairath, A.; Christophersen, C.T.; Conlon, M.A.; Fricker, P.A. Lactobacillus fermentum (PCC(R)) supplementation and gastrointestinal and respiratory-tract illness symptoms: A randomised control trial in athletes. Nutr. J. 2011, 10, 30. [Google Scholar] [CrossRef]
- Nieman, D.C.; Johanssen, L.M.; Lee, J.W.; Arabatzis, K. Infectious episodes in runners before and after the Los Angeles Marathon. J. Sports Med. Phys. Fit. 1990, 30, 316–328. [Google Scholar]
- Peters, E.M.; Goetzsche, J.M.; Grobbelaar, B.G.; Noakes, T.D. Vitamin C supplementation reduces the incidence of postrace symptoms of upper-respiratory-tract infection in ultramarathon runners. Am. J. Clin. Nutr. 1993, 57, 170–174. [Google Scholar] [CrossRef]
- Foster, C. Monitoring training in athletes with reference to overtraining syndrome. Med. Sci. Sports Exerc. 1998, 30, 1164–1168. [Google Scholar] [CrossRef]
- Mackinnon, L.T. Chronic exercise training effects on immune function. Med. Sci. Sports Exerc. 2000, 32, S369–S376. [Google Scholar] [CrossRef]
- Yasmin, A.; Butt, M.S.; Afzaal, M.; van Baak, M.; Nadeem, M.T.; Shahid, M.Z. Prebiotics, gut microbiota and metabolic risks: Unveiling the relationship. J. Funct. Foods 2015, 17, 189–201. [Google Scholar] [CrossRef]
- de Vrese, M.; Schrezenmeir, J. Probiotics, prebiotics, and synbiotics. Adv. Biochem. Eng. Biotechnol. 2008, 111, 1–66. [Google Scholar] [CrossRef]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef]
- Weichselbaum, E. Potential benefits of probiotics--main findings of an in-depth review. Br. J. Community Nurs. 2010, 15, 110–114. [Google Scholar] [CrossRef]
- Gibson, G.R.; Roberfroid, M.B. Dietary modulation of the human colonic microbiota: Introducing the concept of prebiotics. J. Nutr. 1995, 125, 1401–1412. [Google Scholar] [CrossRef]
- Ouwehand, A.C.; Kirjavainen, P.V.; Grönlund, M.M.; Isolauri, E.; Salminen, S.J. Adhesion of probiotic micro-organisms to intestinal mucus. Int. Dairy J. 1999, 9, 623–630. [Google Scholar] [CrossRef]
- Bernet, M.F.; Brassart, D.; Neeser, J.R.; Servin, A.L. Adhesion of human bifidobacterial strains to cultured human intestinal epithelial cells and inhibition of enteropathogen-cell interactions. Appl. Environ. Microbiol. 1993, 59, 4121–4128. [Google Scholar] [CrossRef]
- Schreiber, C.; Tamir, S.; Golan, R.; Weinstein, A.; Weinstein, Y. The effect of probiotic supplementation on performance, inflammatory markers and gastro-intestinal symptoms in elite road cyclists. J. Int. Soc. Sports Nutr. 2021, 18, 36. [Google Scholar] [CrossRef]
- Tavares-Silva, E.; Caris, A.V.; Santos, S.A.; Ravacci, G.R.; Thomatieli-Santos, R.V. Effect of Multi-Strain Probiotic Supplementation on URTI Symptoms and Cytokine Production by Monocytes after a Marathon Race: A Randomized, Double-Blind, Placebo Study. Nutrients 2021, 13, 1478. [Google Scholar] [CrossRef]
- Smarkusz-Zarzecka, J.; Ostrowska, L.; Leszczynska, J.; Orywal, K.; Cwalina, U.; Pogodzinski, D. Analysis of the Impact of a Multi-Strain Probiotic on Body Composition and Cardiorespiratory Fitness in Long-Distance Runners. Nutrients 2020, 12, 3758. [Google Scholar] [CrossRef]
- Pugh, J.N.; Sparks, A.S.; Doran, D.A.; Fleming, S.C.; Langan-Evans, C.; Kirk, B.; Fearn, R.; Morton, J.P.; Close, G.L. Four weeks of probiotic supplementation reduces GI symptoms during a marathon race. Eur. J. Appl. Physiol. 2019, 119, 1491–1501. [Google Scholar] [CrossRef]
- Quero, C.D.; Manonelles, P.; Fernandez, M.; Abellan-Aynes, O.; Lopez-Plaza, D.; Andreu-Caravaca, L.; Hinchado, M.D.; Galvez, I.; Ortega, E. Differential Health Effects on Inflammatory, Immunological and Stress Parameters in Professional Soccer Players and Sedentary Individuals after Consuming a Synbiotic. A Triple-Blinded, Randomized, Placebo-Controlled Pilot Study. Nutrients 2021, 13, 1321. [Google Scholar] [CrossRef]
- Quero-Calero, C.D.; Abellan-Aynes, O.; Manonelles, P.; Ortega, E. The Consumption of a Synbiotic Does Not Affect the Immune, Inflammatory, and Sympathovagal Parameters in Athletes and Sedentary Individuals: A Triple-Blinded, Randomized, Place-bo-Controlled Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 3421. [Google Scholar] [CrossRef]
- Batatinha, H.; Tavares-Silva, E.; Leite, G.S.F.; Resende, A.S.; Albuquerque, J.A.T.; Arslanian, C.; Fock, R.A.; Lancha, A.H., Jr.; Lira, F.S.; Kruger, K.; et al. Probiotic supplementation in marathonists and its impact on lymphocyte population and function after a marathon: A randomized placebo-controlled double-blind study. Sci. Rep. 2020, 10, 18777. [Google Scholar] [CrossRef]
- Gleeson, M.; Bishop, N.C.; Oliveira, M.; Tauler, P. Daily probiotic’s (Lactobacillus casei Shirota) reduction of infection incidence in athletes. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 55–64. [Google Scholar] [CrossRef]
- Petersen, A.M.; Pedersen, B.K. The anti-inflammatory effect of exercise. J. Appl. Physiol. 2005, 98, 1154–1162. [Google Scholar] [CrossRef] [PubMed]
- Akira, S.; Kishimoto, T. IL-6 and NF-IL6 in acute-phase response and viral infection. Immunol. Rev. 1992, 127, 25–50. [Google Scholar] [CrossRef] [PubMed]
- Akira, S.; Taga, T.; Kishimoto, T. Interleukin-6 in biology and medicine. Adv. Immunol. 1993, 54, 1–78. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, J.; O’Mahony, L.; O’Callaghan, L.; Sheil, B.; Vaughan, E.E.; Fitzsimons, N.; Fitzgibbon, J.; O’Sullivan, G.C.; Kiely, B.; Collins, J.K.; et al. Double blind, placebo controlled trial of two probiotic strains in interleukin 10 knockout mice and mechanistic link with cytokine balance. Gut 2003, 52, 975–980. [Google Scholar] [CrossRef]
- Li, A.; Wang, Y.; Li, Z.; Qamar, H.; Mehmood, K.; Zhang, L.; Liu, J.; Zhang, H.; Li, J. Probiotics isolated from yaks improves the growth performance, antioxidant activity, and cytokines related to immunity and inflammation in mice. Microb. Cell Fact. 2019, 18, 112. [Google Scholar] [CrossRef]
- Hajifaraji, M.; Jahanjou, F.; Abbasalizadeh, F.; Aghamohammadzadeh, N.; Abbasi, M.M.; Dolatkhah, N. Effect of probiotic supplements in women with gestational diabetes mellitus on inflammation and oxidative stress biomarkers: A randomized clinical trial. Asia Pac. J. Clin. Nutr. 2018, 27, 581–591. [Google Scholar] [CrossRef]
- Cytokines in the balance. Nat. Immunol. 2019, 20, 1557. [CrossRef]
- Ostrowski, K.; Rohde, T.; Asp, S.; Schjerling, P.; Pedersen, B.K. Pro- and anti-inflammatory cytokine balance in strenuous exercise in humans. J. Physiol. 1999, 515, 287–291. [Google Scholar] [CrossRef]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef]
- Bernecker, C.; Scherr, J.; Schinner, S.; Braun, S.; Scherbaum, W.A.; Halle, M. Evidence for an exercise induced increase of TNF-alpha and IL-6 in marathon runners. Scand. J. Med. Sci. Sports 2013, 23, 207–214. [Google Scholar] [CrossRef]
- Cerqueira, E.; Marinho, D.A.; Neiva, H.P.; Lourenco, O. Inflammatory Effects of High and Moderate Intensity Exercise-A Systematic Review. Front. Physiol. 2019, 10, 1550. [Google Scholar] [CrossRef]
- Malek, T.R. The main function of IL-2 is to promote the development of T regulatory cells. J. Leukoc. Biol. 2003, 74, 961–965. [Google Scholar] [CrossRef]
- Bao, K.; Reinhardt, R.L. The differential expression of IL-4 and IL-13 and its impact on type-2 immunity. Cytokine 2015, 75, 25–37. [Google Scholar] [CrossRef]
- Alves, M.D.J.; Silva, D.D.S.; Pereira, E.V.M.; Pereira, D.D.; de Sousa Fernandes, M.S.; Santos, D.F.C.; Oliveira, D.P.M.; Vieira-Souza, L.M.; Aidar, F.J.; de Souza, R.F. Changes in Cytokines Concentration Following Long-Distance Running: A Systematic Review and Meta-Analysis. Front. Physiol. 2022, 13, 838069. [Google Scholar] [CrossRef]
- Smyth, M.J.; Johnstone, R.W. Role of TNF in lymphocyte-mediated cytotoxicity. Microsc. Res. Tech. 2000, 50, 196–208. [Google Scholar] [CrossRef]
- Neville, V.; Gleeson, M.; Folland, J.P. Salivary IgA as a risk factor for upper respiratory infections in elite professional athletes. Med. Sci. Sports Exerc. 2008, 40, 1228–1236. [Google Scholar] [CrossRef] [PubMed]
- Harbige, L.S.; Pinto, E.; Allgrove, J.; Thomas, L.V. Immune Response of Healthy Adults to the Ingested Probiotic Lactobacillus casei Shirota. Scand. J. Immunol. 2016, 84, 353–364. [Google Scholar] [CrossRef]
- Gill, S.K.; Allerton, D.M.; Ansley-Robson, P.; Hemmings, K.; Cox, M.; Costa, R.J. Does Short-Term High Dose Probiotic Supplementation Containing Lactobacillus casei Attenuate Exertional-Heat Stress Induced Endotoxaemia and Cytokinaemia? Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 268–275. [Google Scholar] [CrossRef]
- Rohatgi, A. Webplotdigitizer, Version 4.4. 2020. Available online: https://automeris.io/WebPlotDigitizer (accessed on 3 November 2020).
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Song, F.; Khan, K.S.; Dinnes, J.; Sutton, A.J. Asymmetric funnel plots and publication bias in meta-analyses of diagnostic accuracy. Int. J. Epidemiol. 2002, 31, 88–95. [Google Scholar] [CrossRef]
- Cuijpers, P. 3.16—Systematic Reviews and Meta-Analytic Methods in Clinical Psychology. In Comprehensive Clinical Psychology, 2nd ed.; Asmundson, G.J.G., Ed.; Elsevier: Oxford, UK, 2022; pp. 224–237. [Google Scholar] [CrossRef]
- Huang, W.C.; Wei, C.C.; Huang, C.C.; Chen, W.L.; Huang, H.Y. The Beneficial Effects of Lactobacillus plantarum PS128 on High-Intensity, Exercise-Induced Oxidative Stress, Inflammation, and Performance in Triathletes. Nutrients 2019, 11, 353. [Google Scholar] [CrossRef]
- Moreira, A.; Delgado, L.; Moreira, P.; Haahtela, T. Does exercise increase the risk of upper respiratory tract infections? Br. Med. Bull. 2009, 90, 111–131. [Google Scholar] [CrossRef]
- Lopez-Castejon, G.; Brough, D. Understanding the mechanism of IL-1beta secretion. Cytokine Growth Factor Rev. 2011, 22, 189–195. [Google Scholar] [CrossRef]
- Ren, K.; Torres, R. Role of interleukin-1beta during pain and inflammation. Brain Res. Rev. 2009, 60, 57–64. [Google Scholar] [CrossRef]
- Dembic, Z. Chapter 6—Cytokines of the Immune System: Interleukins. In The Cytokines of the Immune System; Dembic, Z., Ed.; Academic Press: Amsterdam, The Netherlands, 2015; pp. 143–239. [Google Scholar] [CrossRef]
- Suzuki, K.; Yamada, M.; Kurakake, S.; Okamura, N.; Yamaya, K.; Liu, Q.; Kudoh, S.; Kowatari, K.; Nakaji, S.; Sugawara, K. Circulating cytokines and hormones with immunosuppressive but neutrophil-priming potentials rise after endurance exercise in humans. Eur. J. Appl. Physiol. 2000, 81, 281–287. [Google Scholar] [CrossRef]
- Ma, Q. Polarization of Immune Cells in the Pathologic Response to Inhaled Particulates. Front. Immunol. 2020, 11, 1060. [Google Scholar] [CrossRef]
- Zhang, C.; Wu, Z.; Li, J.W.; Zhao, H.; Wang, G.Q. Cytokine release syndrome in severe COVID-19: Interleukin-6 receptor antagonist tocilizumab may be the key to reduce mortality. Int. J. Antimicrob. Agents 2020, 55, 105954. [Google Scholar] [CrossRef]
- Hunter, C.A.; Jones, S.A. IL-6 as a keystone cytokine in health and disease. Nat. Immunol. 2015, 16, 448–457. [Google Scholar] [CrossRef]
- Bickel, M. The role of interleukin-8 in inflammation and mechanisms of regulation. J. Periodontol. 1993, 64, 456–460. [Google Scholar]
- Heidemann, J.; Ogawa, H.; Dwinell, M.B.; Rafiee, P.; Maaser, C.; Gockel, H.R.; Otterson, M.F.; Ota, D.M.; Lugering, N.; Domschke, W.; et al. Angiogenic effects of interleukin 8 (CXCL8) in human intestinal microvascular endothelial cells are mediated by CXCR2. J. Biol. Chem. 2003, 278, 8508–8515. [Google Scholar] [CrossRef]
- Idriss, H.T.; Naismith, J.H. TNF alpha and the TNF receptor superfamily: Structure-function relationship(s). Microsc. Res. Tech. 2000, 50, 184–195. [Google Scholar] [CrossRef]
- Nehring, S.M.; Goyal, A.; Patel, B.C. C Reactive Protein; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Kazemi, A.; Soltani, S.; Ghorabi, S.; Keshtkar, A.; Daneshzad, E.; Nasri, F.; Mazloomi, S.M. Effect of probiotic and synbiotic supplementation on inflammatory markers in health and disease status: A systematic review and meta-analysis of clinical trials. Clin. Nutr. 2020, 39, 789–819. [Google Scholar] [CrossRef]
- Su, G.L.; Ko, C.W.; Bercik, P.; Falck-Ytter, Y.; Sultan, S.; Weizman, A.V.; Morgan, R.L. AGA Clinical Practice Guidelines on the Role of Probiotics in the Management of Gastrointestinal Disorders. Gastroenterology 2020, 159, 697–705. [Google Scholar] [CrossRef]
- Sivamaruthi, B.S.; Kesika, P.; Chaiyasut, C. Effect of Probiotics Supplementations on Health Status of Athletes. Int. J. Environ. Res. Public Health 2019, 16, 4469. [Google Scholar] [CrossRef]
- Leite, G.S.F.; Resende Master Student, A.S.; West, N.P.; Lancha, A.H., Jr. Probiotics and sports: A new magic bullet? Nutrition 2019, 60, 152–160. [Google Scholar] [CrossRef]
- Sabat, R.; Grutz, G.; Warszawska, K.; Kirsch, S.; Witte, E.; Wolk, K.; Geginat, J. Biology of interleukin-10. Cytokine Growth Factor Rev. 2010, 21, 331–344. [Google Scholar] [CrossRef]
- Ostrowski, K.; Schjerling, P.; Pedersen, B.K. Physical activity and plasma interleukin-6 in humans--effect of intensity of exercise. Eur. J. Appl. Physiol. 2000, 83, 512–515. [Google Scholar] [CrossRef]
- Schroder, K.; Hertzog, P.J.; Ravasi, T.; Hume, D.A. Interferon-gamma: An overview of signals, mechanisms and functions. J. Leukoc. Biol. 2004, 75, 163–189. [Google Scholar] [CrossRef]
- Flaishon, L.; Topilski, I.; Shoseyov, D.; Hershkoviz, R.; Fireman, E.; Levo, Y.; Marmor, S.; Shachar, I. Cutting edge: Anti-inflammatory properties of low levels of IFN-gamma. J. Immunol. 2002, 168, 3707–3711. [Google Scholar] [CrossRef]
- Cabral-Santos, C.; de Lima Junior, E.A.; Fernandes, I.; Pinto, R.Z.; Rosa-Neto, J.C.; Bishop, N.C.; Lira, F.S. Interleukin-10 responses from acute exercise in healthy subjects: A systematic review. J. Cell. Physiol. 2019, 234, 9956–9965. [Google Scholar] [CrossRef]
- Moldoveanu, A.I.; Shephard, R.J.; Shek, P.N. The cytokine response to physical activity and training. Sports Med. 2001, 31, 115–144. [Google Scholar] [CrossRef]
- Miletic, I.D.; Schiffman, S.S.; Miletic, V.D.; Sattely-Miller, E.A. Salivary IgA secretion rate in young and elderly persons. Physiol. Behav. 1996, 60, 243–248. [Google Scholar] [CrossRef]
- Baralic, I.; Andjelkovic, M.; Djordjevic, B.; Dikic, N.; Radivojevic, N.; Suzin-Zivkovic, V.; Radojevic-Skodric, S.; Pejic, S. Effect of Astaxanthin Supplementation on Salivary IgA, Oxidative Stress, and Inflammation in Young Soccer Players. Evid Based Complement. Altern. Med. 2015, 2015, 783761. [Google Scholar] [CrossRef]
- Aase, A.; Sommerfelt, H.; Petersen, L.B.; Bolstad, M.; Cox, R.J.; Langeland, N.; Guttormsen, A.B.; Steinsland, H.; Skrede, S.; Brandtzaeg, P. Salivary IgA from the sublingual compartment as a novel noninvasive proxy for intestinal immune induction. Mucosal Immunol. 2016, 9, 884–893. [Google Scholar] [CrossRef] [PubMed]
- Castilho, T.; da Silva Guimarães, L.; Póvoa, H.C.C.; Antunes, L.S.; Antunes, L.A.A. Influence of physical exercises on salivary immunoglobulin A (sIgA) concentration in athletes: A systematic review with meta-analysis. Sport Sci. Health 2021. [Google Scholar] [CrossRef]
- Clancy, R.L.; Gleeson, M.; Cox, A.; Callister, R.; Dorrington, M.; D′Este, C.; Pang, G.; Pyne, D.; Fricker, P.; Henriksson, A. Reversal in fatigued athletes of a defect in interferon gamma secretion after administration of Lactobacillus acidophilus. Br. J. Sports Med. 2006, 40, 351–354. [Google Scholar] [CrossRef]
- Plaza-Diaz, J.; Ruiz-Ojeda, F.J.; Vilchez-Padial, L.M.; Gil, A. Evidence of the Anti-Inflammatory Effects of Probiotics and Synbiotics in Intestinal Chronic Diseases. Nutrients 2017, 9, 555. [Google Scholar] [CrossRef] [PubMed]
- Hao, Q.; Dong, B.R.; Wu, T. Probiotics for preventing acute upper respiratory tract infections. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | Publication Date | Country | Sport Type | Species | Assessed Inflammatory Markers | Probiotic Type | Control (Placebo) Type | Male Female Total | Probiotic Control | Probiotic Control | Probiotics | Baseline Assessment Time | Dose (16 CFU) | Frequency | Intervention Time | Post-Intervention Assessment Time |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| West, 2011 | 2011 April | Australia | Cycling | L. fermentum | IL-6, IL-8, IL-10, IFN-γ, TNF-α | Capsule | Capsule | M: 62 F: 35 T: 97 | P: 47 C: 50 T: 97 | P: 35.2 ± 10.3 C: 36.4 ± 8.9 | P: 77.9 ± 8.4 C: 76.9 ± 8.2 | Prior to supplement period | 1 billion CFU | 1 capsule QD | 11 weeks | Immediately after a race |
| Tavares-Silva, 2021 | 2021 April | Brazil | Running | B. bifidum, B. lactis, L. acidophilus, L. lactis, L. paracasei | IL-2, IL-4, IL-10, TNF-α, salivary IgA | Capsule | Capsule | M: 14 F: 0 T: 14 | P: 7 C: 7 T: 14 | P: 41.57 ± 3.20 C: 38.28 ± 3.09 | P: 71.24 ± 3.55 C: 78.43 ± 8.40 | 1st day | 5 billion CFU | 2 g 20 QN | 30 days | Immediately after a race |
| Smarkusz-Zarzecka, 2020 | 2020 December | Poland | Running | B. bifidum, B. animalis subsp. lactis, L. acidophilus, L. brevis W63, L. casei, L. lactis, L. salivarius | CRP, TNF-α | Capsule | Capsule | M: 46 F: 20 T: 66 | P: 34 C: 32 T: 66 | P: 39.35 ± 8.23 C: 37.62 ± 8.82 | P: 72.46 ± 4.62 C: 78.26 ± 6.74 | Prior to supplement period | 2.5 billion CFU | 2 capsules BID | 90 days | After the supplement period; physical activity was avoided for at least 24 h before the test |
| Schreiber, 2021 | 2021 May | Israel | Cycling | B. subtilis, B. lactis, B. longum ES1, E. faecium W54, L. helveticus | IL-6, 10 CRP, TNF-α | Capsule | Capsule | M: 27 F: 0 T: 27 | P: 11 C: 16 T: 27 | P: 25.9 ± 4.6 C: 29.5 ± 6.2 | P: 71.3 ± 8.9 C: 72.0 ± 6.2 | 1st day | 15 billion CFU | 1 capsule QD | 90 days | 90th day; strenuous activity was avoided for at least 24 h |
| Quero-Calero, 2022 | 2022 March | Spain | Soccer | B. lactis, B. longum ES1, L. rhamnosus GG | IL-6, IL-8, TNF-α | Powder stick | Powder stick | M: 13 F: 0 T: 13 | P: 7 C: 6 T: 13 | P: 20.6 ± 1.39 C: 21.9 ± 2.77 | P: 70.57 ± 6.75 C: 73.95 ± 6.42 | 1st day | 1 billion CFU | 1 #QD | 30 days | 30th day at 8 a.m. |
| Quero, 2021 | 2021 April | Spain | Soccer | B. lactis, B. longum ES1, L. rhamnosus GG | IL-1β, IL-10, salivary IgA | Powder stick | Powder stick | M: 13 F: 0 T: 13 | P: 7 C: 6 T: 13 | P: 20.66 ± 1.39 C: 21.9 ± 2.77 | P: 70.57 ± 6.75 C: 73.95 ± 6.42 | 1st day | 1 billion CFU | 1 #QD | 30 days | 30th day at 8 a.m. |
| Pugh, 2019 | 2019 July | UK | Running | B. bifidum, B. animalis subsp. lactis, L. acidophilus | IL-6, IL-8, IL-10 | Capsule | Capsule | M: 20 F: 4 T: 24 | P: 11 C: 9 T: 20 | P: 34.8 ± 6.9 C: 36.1 ± 7.5 | P: 76.5 ± 9.4 C: 73.5 ± 11.3 | 4 weeks before the marathon and prior to the supplement period | 25 billion CFU | 1# 19 QDAMPC, 1# on the morning of the race, 1# 2 h before the start | 28 days | Immediately after a race |
| Gleeson, 2011 | 2011 February | UK | Endurance-based activities | L. casei Shirota | IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, IFN-γ, TNF-α, 9 salivary IgA | Fermented drink | Identical in color and taste | M: 54 F: 30 T: 84 | P: 32 C: 26 T: 58 | P: 32 ± 14 C: 25 ± 9 | P: 71.2 ± 9.9 C: 71.6 ± 10.7 | 1st day | 6.5 billion CFU | 1# 18 BID | 8 weeks | After 8 weeks and 16 weeks; strenuous activity was avoided for at least 24 h |
| Batatinha, 2020 | 2020 November | Brazil | Runners | B. animalis subsp. Lactis L. acidophilus | 1 IL-1β, 2 IL-2, 3 IL-4, 4 IL-6, 5 IL-8, 6 IL-10, 7 IFN-γ, 8 TNF-α | Sachets | Sachets | 11 M: 27 12 F: 0 13 T: 27 | 14 P: 14 15 C: 13 T: 27 | P: 35.96 ± 5.81 C: 40.46 ± 7.79 | P: 79.30 ± 10.99 C: 72.67 ± 10.20 | 1st day | 20 billion CFU | 1# 17 QD | 30 days | 1 h after a race |
| Period of Probiotic Intervention | Timing of Postassessment Blood Sampling | ||||
|---|---|---|---|---|---|
| Inflammation-Related Marker | Overall Effect | Shorter Period | Longer Period | Delayed to at Least the Next Day of Exercise | Immediate Assessment after Exercise |
| TNF-α | −0.29 | −0.59 | −0.15 | −0.26 | −0.57 |
| (−0.42, −0.16) | (−0.81, −0.37) | (−0.30, 0.01) | (−0.40, −0.13) | (−0.99, −0.16) | |
| IL-6 | 0.19 | −0.11 | 0.20 | −0.77 | 0.36 |
| (−0.25, 0.63) | (−4.56, 4.34) | (−0.25, 0.64) | (−1.91, 0.37) | (−0.11, 0.84) | |
| IL-8 | −0.57 | −1.23 | −0.20 | −0.17 | −1.31 |
| (−1.33, 0.19) | (−2.48, 0.03) | (−1.15, 0.75) | (−1.11, 0.77) | (−2.59, −0.04) | |
| IL-10 | −0.1 | −0.13 | −0.33 | −0.12 | −0.52 |
| (−0.19, −0.06) | (−0.19, −0.06) | (−1.01, 0.35) | (−0.19, −0.05) | (−0.98, −0.07) | |
| IFN-γ | 14.33 | ||||
| (13.76, 14.89) | |||||
| IgA | 3.57 | ||||
| (0.66, 6.48) | |||||
| IL-β | −0.03 | ||||
| (−0.14, 0.08) | |||||
| IL-2 | −0.04 | ||||
| (−0.38, 0.31) | |||||
| IL-4 | −0.14 | ||||
| (−1.05, 0.77) | |||||
| CRP | −0.69 | ||||
| (−2.51, 1.13) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Y.-T.; Peng, Y.-C.; Yen, H.-Y.; Wu, J.-C.; Hou, W.-H. Effects of Probiotic Supplementation on Immune and Inflammatory Markers in Athletes: A Meta-Analysis of Randomized Clinical Trials. Medicina 2022, 58, 1188. https://doi.org/10.3390/medicina58091188
Guo Y-T, Peng Y-C, Yen H-Y, Wu J-C, Hou W-H. Effects of Probiotic Supplementation on Immune and Inflammatory Markers in Athletes: A Meta-Analysis of Randomized Clinical Trials. Medicina. 2022; 58(9):1188. https://doi.org/10.3390/medicina58091188
Chicago/Turabian StyleGuo, Yi-Ting, Yu-Ching Peng, Hsin-Yen Yen, Jeng-Cheng Wu, and Wen-Hsuan Hou. 2022. "Effects of Probiotic Supplementation on Immune and Inflammatory Markers in Athletes: A Meta-Analysis of Randomized Clinical Trials" Medicina 58, no. 9: 1188. https://doi.org/10.3390/medicina58091188