
Spontaneous Spine Fracture in Patient with Ankylosing Spondylitis under Spinal Anesthesia: A Case Report and Review of the Literature


Abstract
:1. Introduction
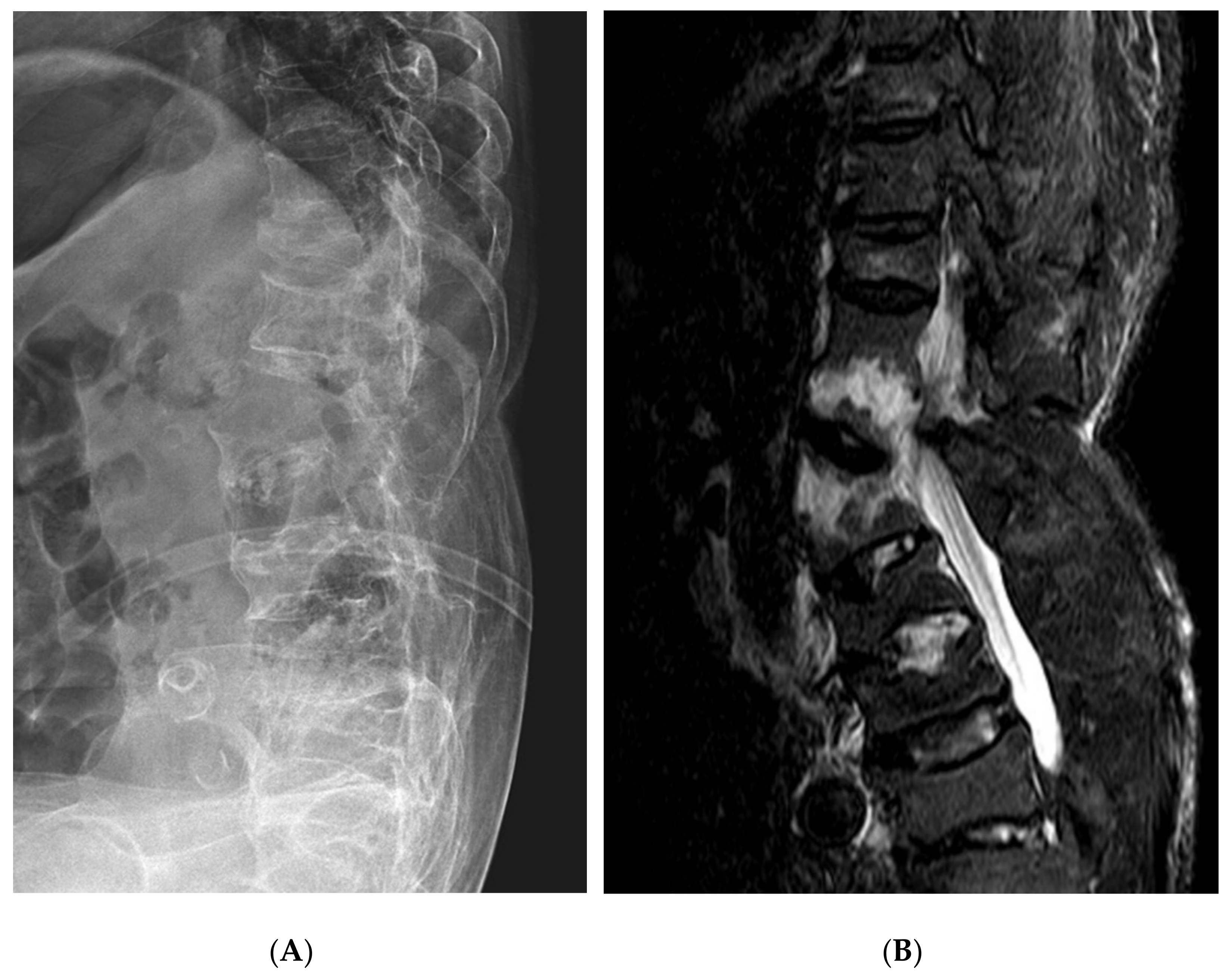
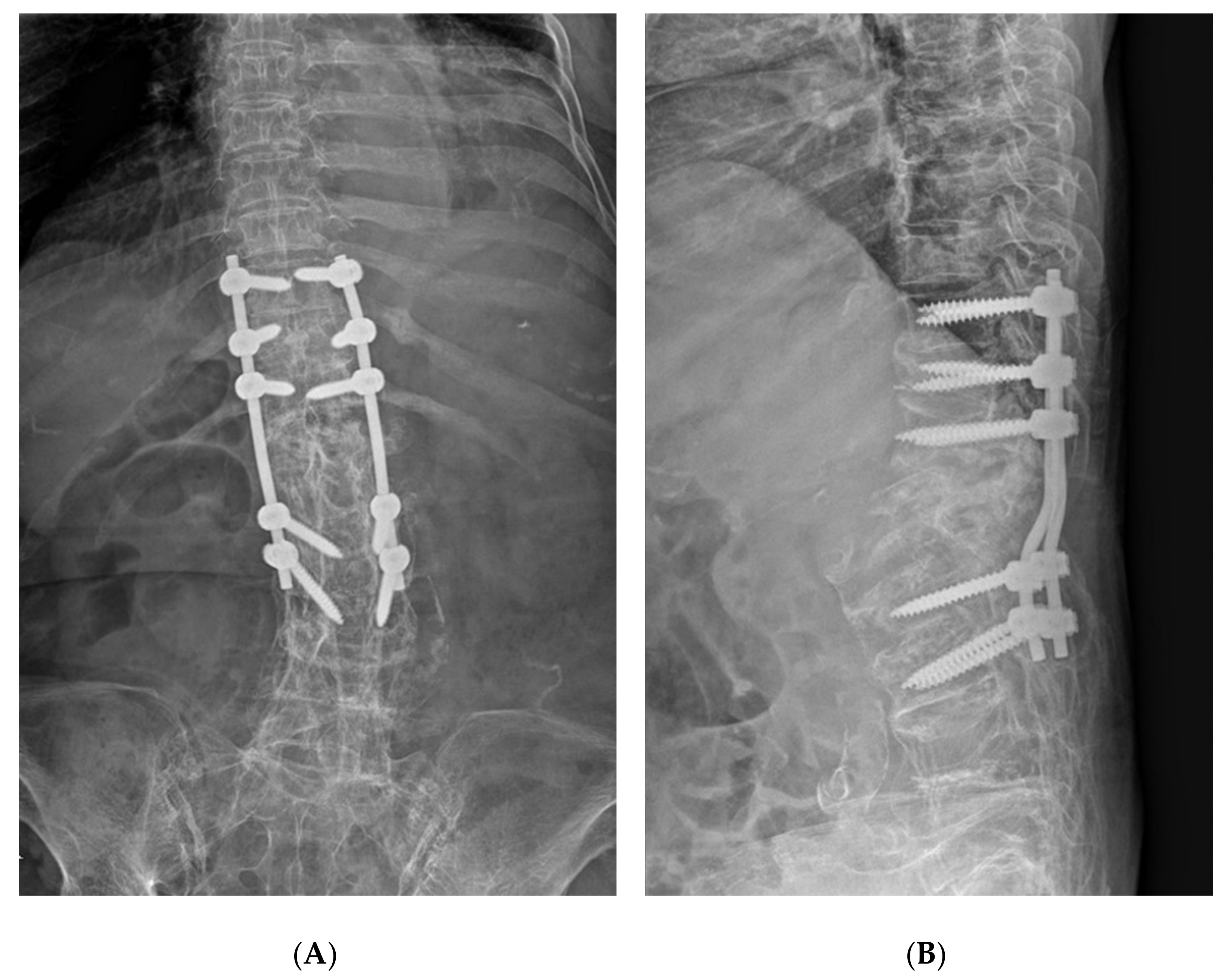
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Westerveld, L.A.; Verlaan, J.J.; Oner, F.C. Spinal fractures in patients with ankylosing spinal disorders: A systematic review of the literature on treatment, neurological status and complications. Eur. Spine J. 2008, 18, 145–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caron, T.; Bransford, R.; Nguyen, Q.; Agel, J.; Chapman, J.; Bellabarba, C. Spine Fractures in Patients with Ankylosing Spinal Disorders. Spine 2010, 35, E458–E464. [Google Scholar] [CrossRef] [PubMed]
- Ruf, M.; Rehm, S.; Poeckler-Schoeniger, C.; Merk, H.R.; Harms, J. Iatrogenic fractures in ankylosing spondylitis—A report of two cases. Eur. Spine J. 2005, 15, 100–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danish, S.F.; Wilden, J.A.; Schuster, J. Iatrogenic paraplegia in 2 morbidly obese patients with ankylosing spondylitis undergoing total hip arthroplasty. J. Neurosurg. Spine 2008, 8, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, M.; Okuyama, K.; Ninomiya, K.; Yato, Y.; Miyamoto, T.; Nakamura, M.; Matsumoto, M. Association of Continuous Vertebral Bone Bridges and Bone Mineral Density with the Fracture Risk in Patients with Diffuse Idiopathic Skeletal Hyperostosis. Asian Spine J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Trent, G.; Armstrong, G.W.D.; O’Neil, J. Thoracolumbar Fractures in Ankylosing Spondylitis High-Risk Injuries. Clin. Orthop. Relat. Res. 1988, 227, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Maarouf, A.; McQuown, C.M.; Frey, J.A.; Ahmed, R.A.; Derrick, L. Iatrogenic Spinal Cord Injury in a Trauma Patient with Ankylosing Spondylitis. Prehospital Emerg. Care 2017, 21, 390–394. [Google Scholar] [CrossRef] [PubMed]
- Kremer, P.; Despaux, J.; Benmansour, A.; Wendling, D. Spontaneous fracture of the odontoid process in a patient with ankylosing spondylitis. Nonunion responsible for compression of the upper cervical cord. Rev. Rhum. 1995, 62, 455–458. [Google Scholar]
- Gartman, J.J., Jr.; Bullitt, E.; Baker, M.L. Axis fracture in ankylosing spondylitis: Case report. Neurosurgery 1991, 29, 590–594. [Google Scholar] [CrossRef] [PubMed]
- Rapp, G.F.; Kernek, C.B. Spontaneous Fracture of the Lumbar Spine with Correction of Deformity in Ankylosing Spondylitis. J. Bone Jt. Surg.-Am. Vol. 1974, 56, 1277–1278. [Google Scholar] [CrossRef]
- Oh, J.-S.; Doh, J.-W.; Shim, J.-J.; Lee, K.-S. Leading a Patient of Ankylosing Spondylitis to Death by Iatrogenic Spinal Fracture. Korean J. Spine 2016, 13, 80–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Number of Case | Level | Injury Mechanism | Symptom | Treatment | Remarks |
|---|---|---|---|---|---|---|---|
| Rapp GF et al. [10] | 1974 | 1 | L4 | Spontaneous | Back pain | Posterior fusion | During bed rest |
| Gartman JJ Jr et al. [9] | 1991 | 1 | C2 | Spontaneous | Radiating pain | Posterior decompression | Spontaneous neck spasm |
| Kremer P et al. [8] | 1995 | 1 | C2 | Unknown | Tetraparesis | Unknown | Unknown |
| Ruf et al. [3] | 2008 | 2 | C6-7 C6-7 | Fracture & dislocation Hyperextension injury | Quadriplegia Unknown | Posterior decompression Posterior fusion | Unknown During AS * lumbar surgery |
| Danish et al. [4] | 2008 | 2 | T11-12 T11 | Hyperextension injury Hyperextension injury | Paraplegia Paraplegia | Posterior fusion Posterior decompression | During THA † in obese patients During THA † in obese patients |
| Oh JS et al. [11] | 2016 | 1 | T9-10 | Hyperextension injury | Paraplegia | Immobilization | During CT # evaluation |
| Maarouf et al. [7] | 2017 | 1 | T10-11 | Extension injury | Paraplegia | Spinal fusion | Rigid backboard immobilization |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeung, U.-O.; Joo, D.-C.; Kim, S.-K.; Im, C.-J. Spontaneous Spine Fracture in Patient with Ankylosing Spondylitis under Spinal Anesthesia: A Case Report and Review of the Literature. Medicina 2021, 57, 1051. https://doi.org/10.3390/medicina57101051
Jeung U-O, Joo D-C, Kim S-K, Im C-J. Spontaneous Spine Fracture in Patient with Ankylosing Spondylitis under Spinal Anesthesia: A Case Report and Review of the Literature. Medicina. 2021; 57(10):1051. https://doi.org/10.3390/medicina57101051
Chicago/Turabian StyleJeung, Ul-Oh, Dae-Chang Joo, Sung-Kyu Kim, and Chae-Jin Im. 2021. "Spontaneous Spine Fracture in Patient with Ankylosing Spondylitis under Spinal Anesthesia: A Case Report and Review of the Literature" Medicina 57, no. 10: 1051. https://doi.org/10.3390/medicina57101051