
Outpatient Telehealth Implementation in the United States during the COVID-19 Global Pandemic: A Systematic Review


Abstract
:1. Introduction
1.1. Rationale
1.2. Objectives
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search
2.4. Initial Study Selection
3. Results
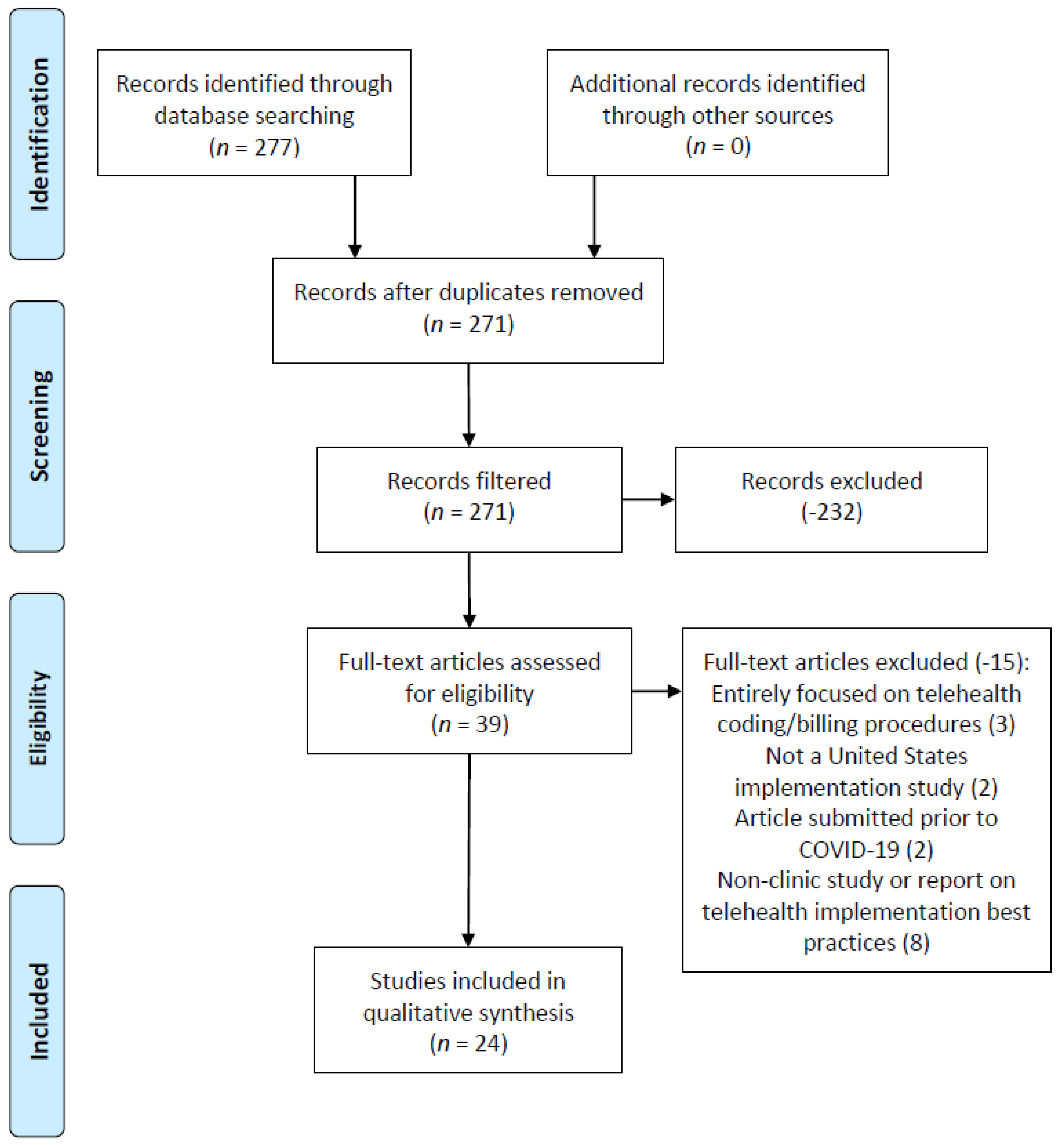
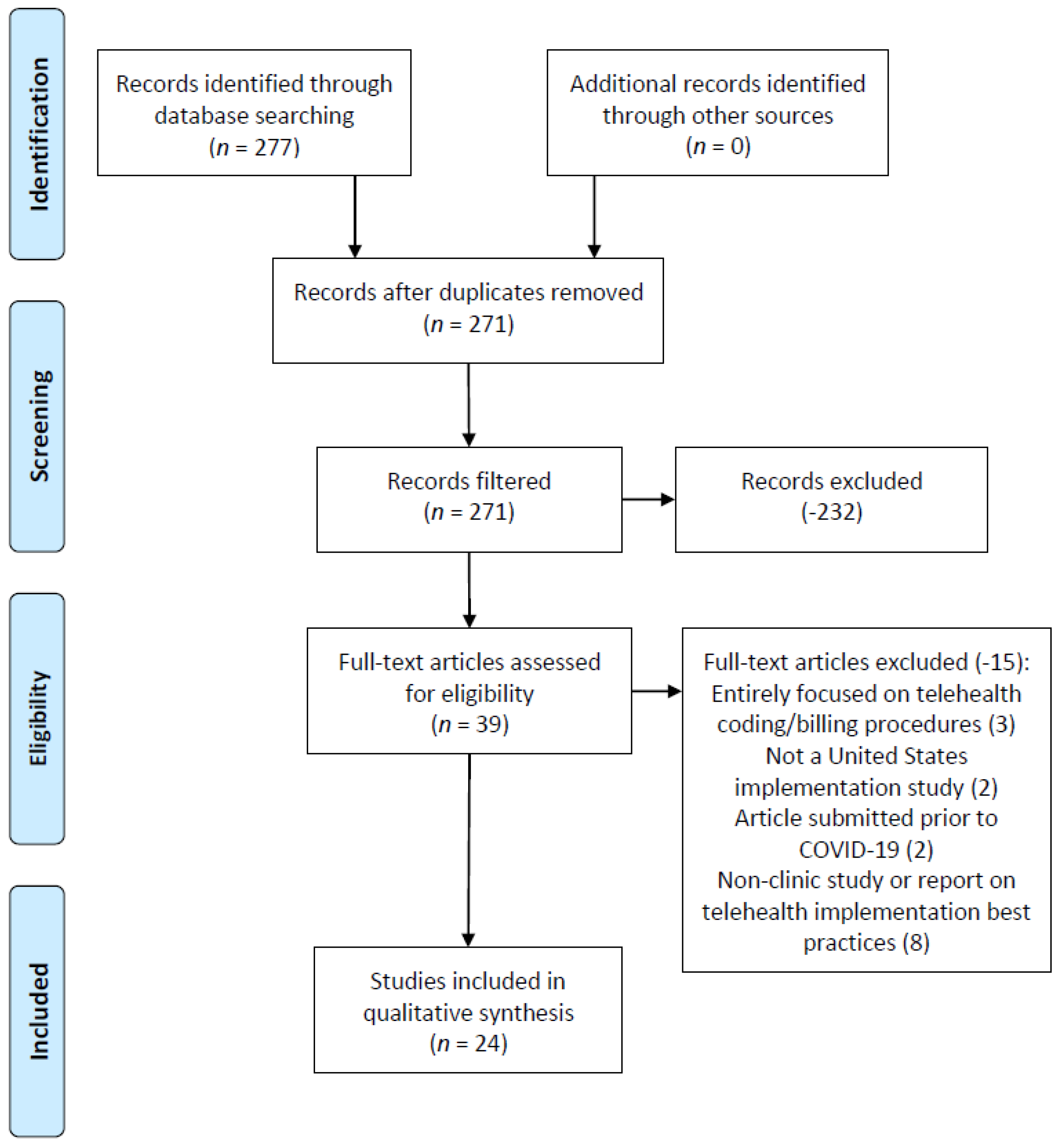
3.1. Study Selection/Exclusion
- (a)
- A primary focus of telehealth coding and billing processes/procedures (3 articles),
- (b)
- Ambulatory care organizations not located within the United States (2 articles),
- (c)
- Articles published during the review criteria publication date range but with research conducted prior to the pandemic (2 articles), and
- (d)
- A non-clinic or other non-health care organization-focused article (professional association and/or other non-health care delivery organization publication) (8 articles).
3.2. Study Characteristics
3.3. Risk of Bias
3.4. Additional Analysis
4. Discussion
4.1. Summary of Evidence
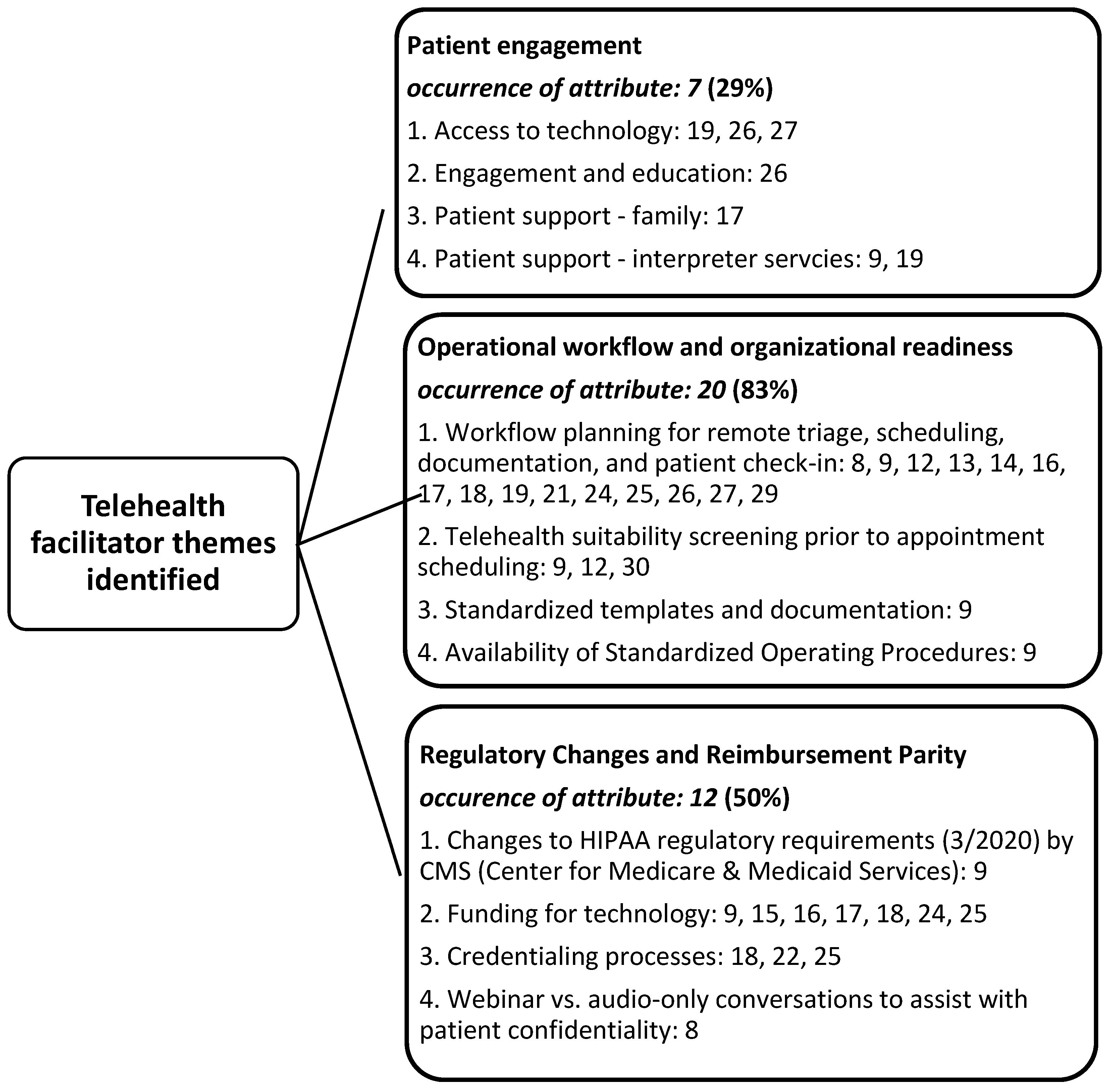
4.2. Facilitator of Telehealth Implementation: Patient Engagement
4.3. Facilitator of Telehealth Implementation: Operational Workflow and Organizational Readiness
4.4. Facilitator of Telehealth Implementation: Regulatory Changes and Reimbursement Parity
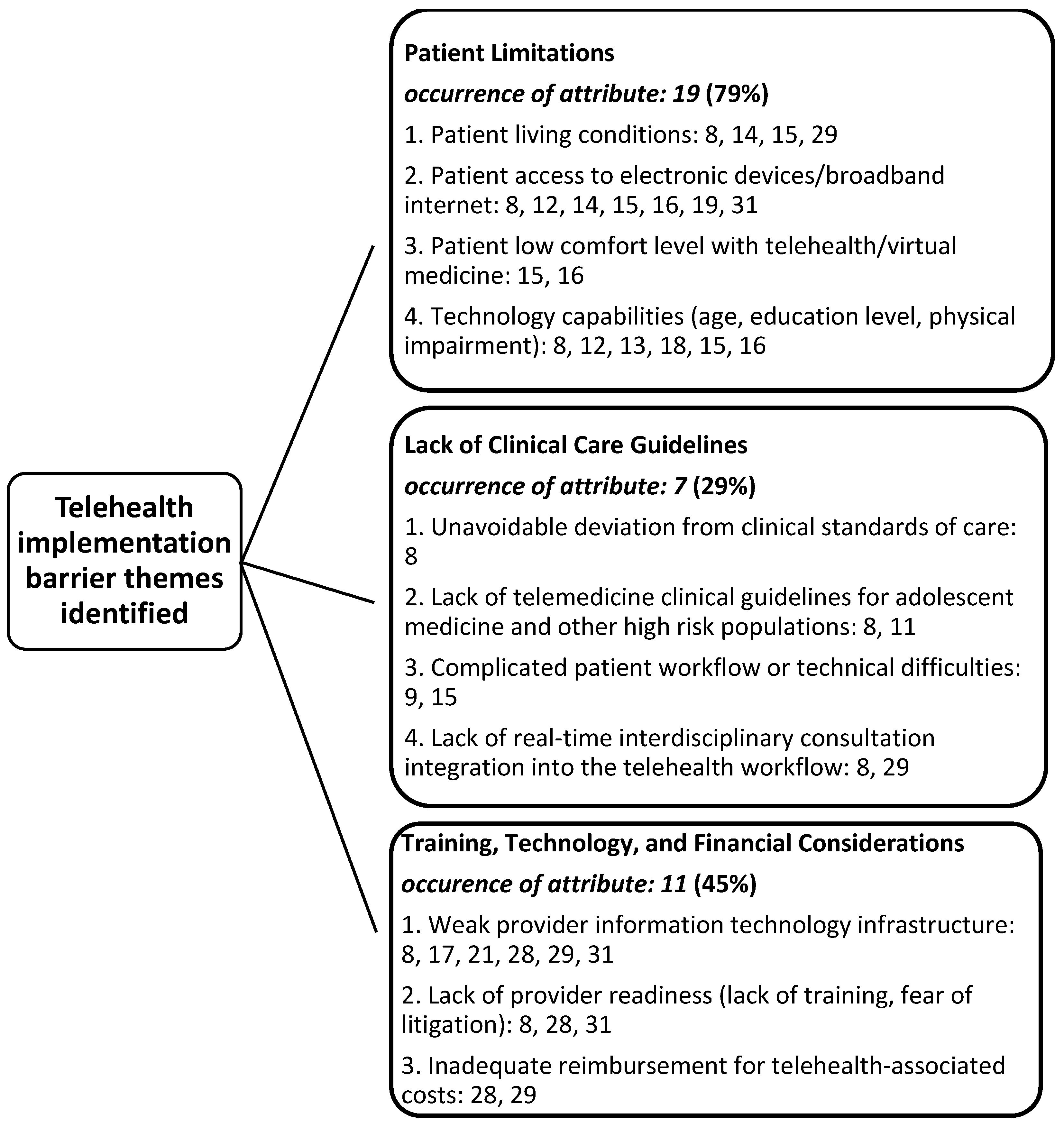
4.5. Barrier to Telehealth Implementation: Patient Limitations
4.6. Barrier to Telehealth Implementation: Lack of Clinical Care Guidelines
4.7. Barrier to Telehealth Implementation: Training, Technology, and Financial Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schub, T.B. COVID-19 Coronavirus. In CINAHL Nursing Guide; EBSSCO Publishing: Ipswich, MA, USA, 2020. [Google Scholar]
- Childs, A.W.; Unger, A.; Li, L. Rapid design and deployment of intensive outpatient, group-based psychiatric care using telehealth during coronavirus disease 2019 (COVID-19). J. Am. Med Inform. Assoc. JAMIA 2020, 27, 1420–1424. [Google Scholar] [CrossRef]
- Grossman, S.N.; Han, S.C.; Balcer, L.J.; Kurzweil, A.; Weinberg, H.; Galetta, S.L.; Busis, N.A. Rapid implementation of virtual neurology in response to the COVID-19 pandemic. Neurology 2020, 94, 1077–1087. [Google Scholar] [CrossRef]
- Mills, E.C.; Chiu, E.S.; Savage, E.; Lieder, J. Telemedicine and the COVID-19 Pandemic: Are We Ready to Go Live? Adv. Skin Wound Care 2020, 33, 410–417. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Telemedicine: Opportunities and Developments in Member States: Report on the Second Global Survey on eHealth; World Health Organization: Geneva, Switzerland, 2010; Available online: https://www.who.int/gho/goe/telehealth/en/ (accessed on 30 April 2021).
- Lieneck, C.; Weaver, E.; Maryon, T. Pandemic Pause: Systematic Review of Cost Variables for Ambulatory Care Organizations Participating in Accountable Care Organizations. Healthcare 2021, 9, 198. [Google Scholar] [CrossRef] [PubMed]
- Lieneck, C.; Garvey, J.; Collins, C.; Graham, D.; Loving, C.; Pearson, R. Rapid Telehealth Implementation during the COVID-19 Global Pandemic: A Rapid Review. Healthcare 2020, 8, 517. [Google Scholar] [CrossRef] [PubMed]
- Barney, A.; Buckelew, S.; Mesheriakova, V.; Raymond-Flesch, M. The COVID-19 Pandemic and Rapid Implementation of Adolescent and Young Adult Telemedicine: Challenges and Opportunities for Innovation. J. Adolesc. Health 2020, 67, 164–171. [Google Scholar] [CrossRef]
- Bulman, J.C.; Moussa, M.; Lewis, T.K.; Berkowitz, S.; Sarwar, A.; Faintuch, S.; Ahmed, M. Transitioning the IR Clinic to Telehealth: A Single-Center Experience during the COVID-19 Pandemic. J. Vasc. Interv. Radiol. 2020, 31, 1315–1319.e4. [Google Scholar] [CrossRef]
- Chavis, A.; Bakken, H.; Ellenby, M.; Hasan, R. COVID-19 and Telehealth: Prevention of Exposure in a Medically Complex Patient with a Mild Presentation. J. Adolesc. Health 2020, 67, 456–458. [Google Scholar] [CrossRef]
- Compton, M.; Soper, M.; Reilly, B.; Gettle, L.; List, R.; Bailey, M.; Bruschwein, H.; Somerville, L.; Albon, D. A Feasibility Study of Urgent Implementation of Cystic Fibrosis Multidisciplinary Telemedicine Clinic in the Face of COVID-19 Pandemic: Single-Center Experience. Telemed. J. E-Health Off. J. Am. Telemed. Assoc. 2020, 26, 978–984. [Google Scholar] [CrossRef]
- Dewar, S.; Lee, P.G.; Suh, T.T.; Min, L. Uptake of Virtual Visits in A Geriatric Primary Care Clinic During the COVID-19 Pandemic. J. Am. Geriatr. Soc. 2020, 68, 1392–1394. [Google Scholar] [CrossRef]
- Eberly, L.A.; Khatana, S.A.M.; Nathan, A.S.; Snider, C.; Julien, H.M.; Deleener, M.E.; Adusumalli, S. Telemedicine Outpatient Cardiovascular Care During the COVID-19 Pandemic: Bridging or Opening the Digital Divide? Circulation 2020, 142, 510–512. [Google Scholar] [CrossRef]
- Lau, J.; Knudsen, J.; Jackson, H.; Silvestri, D.M.; Wallach, A.B.; Bouton, M.; Chokshi, D.A.; Natsui, S.; Philippou, C.; Karim, E.; et al. Staying connected in the COVID-19 pandemic: Telehealth at the largest safety-net system in the United States. Health Aff. 2020, 39, 1437–1442. [Google Scholar] [CrossRef]
- Knopf, A. How one large outpatient practice moved to home-based telemedicine services. Brown Univ. Child Adolesc. Psychopharmacol. Update 2020, 22, 1–5. [Google Scholar] [CrossRef]
- Loeb, A.E.; Rao, S.S.; Ficke, J.R.; Morris, C.D.; Riley, L.H., III; Levin, A.S. Departmental Experience and Lessons Learned with Accelerated Introduction of Telemedicine During the COVID-19 Crisis. J. Am. Acad. Orthop. Surg. 2020, 28, E469–E476. [Google Scholar] [CrossRef]
- Madden, N.; Emeruwa, U.N.; Friedman, A.M.; Aubey, J.J.; Aziz, A.; Baptiste, C.D.; Coletta, J.M.; D’Alton, M.E.; Fuchs, K.M.; Goffman, D.; et al. Telehealth Uptake into Prenatal Care and Provider Attitudes during the COVID-19 Pandemic in New York City: A Quantitative and Qualitative Analysis. Am. J. Perinatol. 2020, 37, 1005–1014. [Google Scholar] [CrossRef]
- Mann, D.M.; Chen, J.; Chunara, R.; Testa, P.A.; Nov, O. COVID-19 transforms health care through telemedicine: Evidence from the field. J. Am. Med Inform. Assoc. JAMIA 2020, 27, 1132–1135. [Google Scholar] [CrossRef]
- O’Hara, V.M.; Johnston, S.V.; Browne, N.T. The paediatric weight management office visit via telemedicine: Pre- to post-COVID-19 pandemic. Pediatric Obes. 2020, 15, e12694. [Google Scholar] [CrossRef] [PubMed]
- Panzirer, D. Role of Non-Profit Organizations during COVID-19 for Diabetes Care: Health Care Inequities and Role of Virtual Specialty Clinic. Diabetes Technol. Ther. 2020, 22, 440–443. [Google Scholar] [CrossRef]
- Peahl, A.F.; Smith, R.D.; Moniz, M.H. Prenatal care redesign: Creating flexible maternity care models through virtual care. Am. J. Obstet. Gynecol. 2020, 223, 389.e1–389.e10. [Google Scholar] [CrossRef] [PubMed]
- Segal, E.M.; Alwan, L.; Pitney, C.; Taketa, C.; Indorf, A.; Held, L.; Lee, K.S.; Son, M.; Chi, M.; Diamantides, E.; et al. Establishing clinical pharmacist telehealth services during the COVID-19 pandemic. Am. J. Health-Syst. Pharm. 2020, 77, 1403–1408. [Google Scholar] [CrossRef]
- Smith, W.R.; Atala, A.J.; Terlecki, R.P.; Kelly, E.E.; Matthews, C.A. Implementation Guide for Rapid Integration of an Outpatient Telemedicine Program During the COVID-19 Pandemic. J. Am. Coll. Surg. 2020, 231, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.J.; Oh, L.S.; Martin, S.D.; Berkson, E.M. Telemedicine in the Era of COVID-19: The Virtual Orthopaedic Examination. J. Bone Jt. Surg. Am. Vol. 2020, 102, e57. [Google Scholar] [CrossRef] [PubMed]
- Varma, N.; Marrouche, N.F.; Aguinaga, L.; Albert, C.M.; Arbelo, E.; Choi, J.; Chung, M.K.; Conte, G.; Dagher, L.; Epstein, L.M.; et al. HRS/EHRA/APHRS/LAHRS/ACC/AHA worldwide practice update for telehealth and arrhythmia monitoring during and after a pandemic. J. Arrhythmia 2020, 36, 813–826. [Google Scholar] [CrossRef]
- Wood, S.M.; White, K.; Peebles, R.; Pickel, J.; Alausa, M.; Mehringer, J.; Dowshen, N. Outcomes of a Rapid Adolescent Telehealth Scale-Up During the COVID-19 Pandemic. J. Adolesc. Health 2020, 67, 172–178. [Google Scholar] [CrossRef]
- Wosik, J.; Fudim, M.; Cameron, B.; Gellad, Z.F.; Cho, A.; Phinney, D.; Curtis, S.; Roman, M.; Poon, E.G.; Ferranti, J.; et al. Telehealth transformation: COVID-19 and the rise of virtual care. J. Am. Med Inform. Assoc. 2020, 27, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Yellowlees, P.; Nakagawa, K.; Pakyurek, M.; Hanson, A.; Elder, J.; Kales, H.C. Rapid conversion of an outpatient psychiatric clinic to a 100% virtual telepsychiatry clinic in response to COVID-19. Psychiatr. Serv. 2020, 71, 749–752. [Google Scholar] [CrossRef] [PubMed]
- Centers for Medicare & Medicaid Services. COVID-19 Emergency Declaration Blanket Waivers for Health Care Providers. 2021. Available online: https://www.cms.gov/files/document/summary-covid-19-emergency-declaration-waivers.pdf (accessed on 30 April 2021).
- Centers for Medicare & Medicaid Services. Medicare Telemedicine Health Care Provider Fact Sheet. 2020. Available online: https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet (accessed on 30 April 2021).
- BlueCross BlueShield of Texas. Telemedicine and Telehealth Services. 2021. Available online: https://www.bcbstx.com/provider/clinical/tele_services.html (accessed on 30 April 2021).
- Landi, H. (2020). Fierce Healthcare: Payers have Lowered Barriers to Telehealth. Will Those Changes stick? Here’s what Experts have to Say. Available online: https://www.fiercehealthcare.com/practices/trump-administration-has-lowered-barriers-to-telehealth-will-those-changes-stick-here-s (accessed on 30 April 2021).


{kind=link}
{kind=link}
{kind=link}
| Author(s) | Participant(s) | * JHNEBP Study Design | Facilitators Leading to an Increased Utilization of Telehealth in Ambulatory care Organizations during COVID-19 | Barriers Leading to an Increased Utilization of Telehealth in Ambulatory Care Organizations during COVID-19 |
|---|---|---|---|---|
| Barney et al. [8] | Adolescent and Young Adult Medicine Clinic at the University of California San Francisco | 4 |
|
|
| Bulman et al. [9] | Interventional radiology clinic | 4 |
|
|
| Chavis et al. [10] | Academic general pediatrics clinic | 4 |
|
|
| Childs et al. [11] | Intensive outpatient, group-based psychiatric (IOP) care clinic | 4 |
|
|
| Compton et al. [12] | Cystic Fibrosis Multidisciplinary Telemedicine Clinic | 4 |
|
|
| Dewar et al. [13] | Geriatrics primary care clinic | 4 |
|
|
| Eberly et al. [14] | Academic health system outpatient cardiovascular clinic | 2 | n/a |
|
| Grossman et al. [15] | Neurology outpatient clinic | 4 |
|
|
| Knudsen et al. [16] | NYC Health + Hospitals | 5 |
|
|
| Knopf [17] | University of Washington, the Seattle Children’s Research Institute, and Seattle Children’s Hospital psychiatry clinics | 5 |
|
|
| Loeb et al. [18] | Orthopedic surgery department | 5 |
|
|
| Madden et al. [19] | Prenatal medical practices | 3 |
|
|
| Mann et al. [20] | Large academic health care system with an existing telehealth infrastructure | 4 |
| n/a |
| Savage et al. [21] | Wound care clinic | 4 |
|
|
| O’Hara et al. [22] | Pediatric weight management clinic | 4 |
|
|
| Panzirer [23] | Virtual specialty diabetes clinic | 4 |
|
|
| Peahl et al. [24] | Obstetrical clinic providing prenatal care | 4 |
|
|
| Segal et al. [25] | Clinical pharmacy within an integrated health care system | 4 |
|
|
| Smith et al. [26] | Multispecialty physician groups | 4 |
|
|
| Tanaka et al. [27] | Orthopedic medical practice | 4 |
|
|
| Varma et al. [28] | Cardiovascular medical practice | 4 |
| n/a |
| Wood et al. [29] | Hospital-based specialty clinical program provides nonprimary care management of gender-affirming care, eating disorders, HIV, adolescent gynecology and contraception, general AM, and substance abuse disorders | 3 |
|
|
| Wosik et al. [30] | Multiple health care delivery settings/organizations | 3 |
|
|
| Yellowlees et al. [31] | Outpatient psychiatric clinic | 4 |
|
|
| Strength of Evidence | Frequency |
|---|---|
| II (Quasi-experimental) | 1 (4%) |
| III (Non-experimental, qualitative) | 3 (13%) |
| IV (Opinion of nationally recognized experts based on research evidence/consensus panels) | 17 (70%) |
| V (Opinions of industry experts not based on research evidence) | 3 (13%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lieneck, C.; Weaver, E.; Maryon, T. Outpatient Telehealth Implementation in the United States during the COVID-19 Global Pandemic: A Systematic Review. Medicina 2021, 57, 462. https://doi.org/10.3390/medicina57050462
Lieneck C, Weaver E, Maryon T. Outpatient Telehealth Implementation in the United States during the COVID-19 Global Pandemic: A Systematic Review. Medicina. 2021; 57(5):462. https://doi.org/10.3390/medicina57050462
Chicago/Turabian StyleLieneck, Cristian, Eric Weaver, and Thomas Maryon. 2021. "Outpatient Telehealth Implementation in the United States during the COVID-19 Global Pandemic: A Systematic Review" Medicina 57, no. 5: 462. https://doi.org/10.3390/medicina57050462
APA StyleLieneck, C., Weaver, E., & Maryon, T. (2021). Outpatient Telehealth Implementation in the United States during the COVID-19 Global Pandemic: A Systematic Review. Medicina, 57(5), 462. https://doi.org/10.3390/medicina57050462