Dupilumab for the Treatment of Atopic Dermatitis in an Austrian Cohort-Real-Life Data Shows Rosacea-Like Folliculitis

 , , , and
, , , and
Abstract
1. Introduction
2. Experimental Section
2.1. Study Design and Patients Included
2.2. Data Collection and Outcome Measures
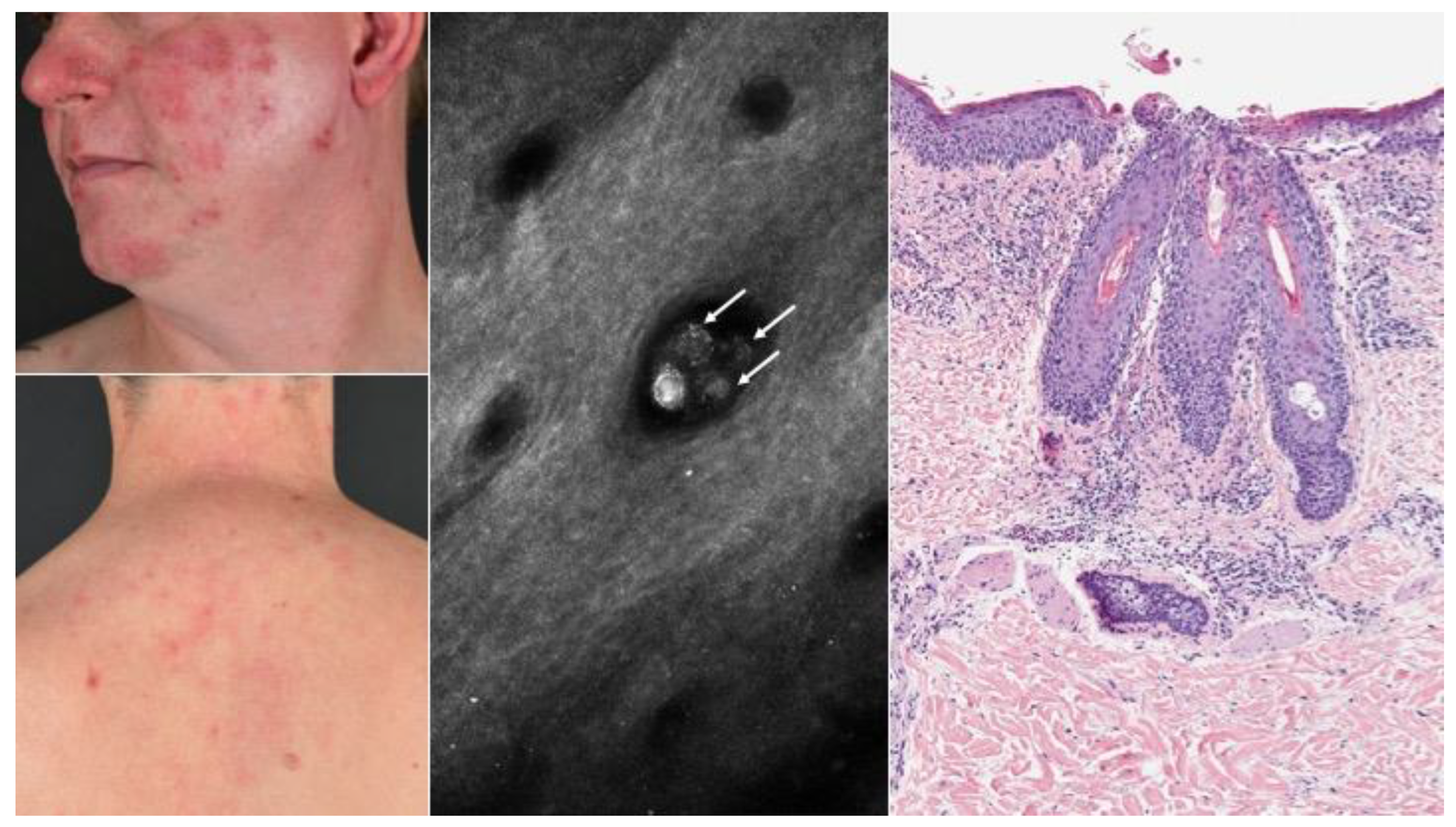
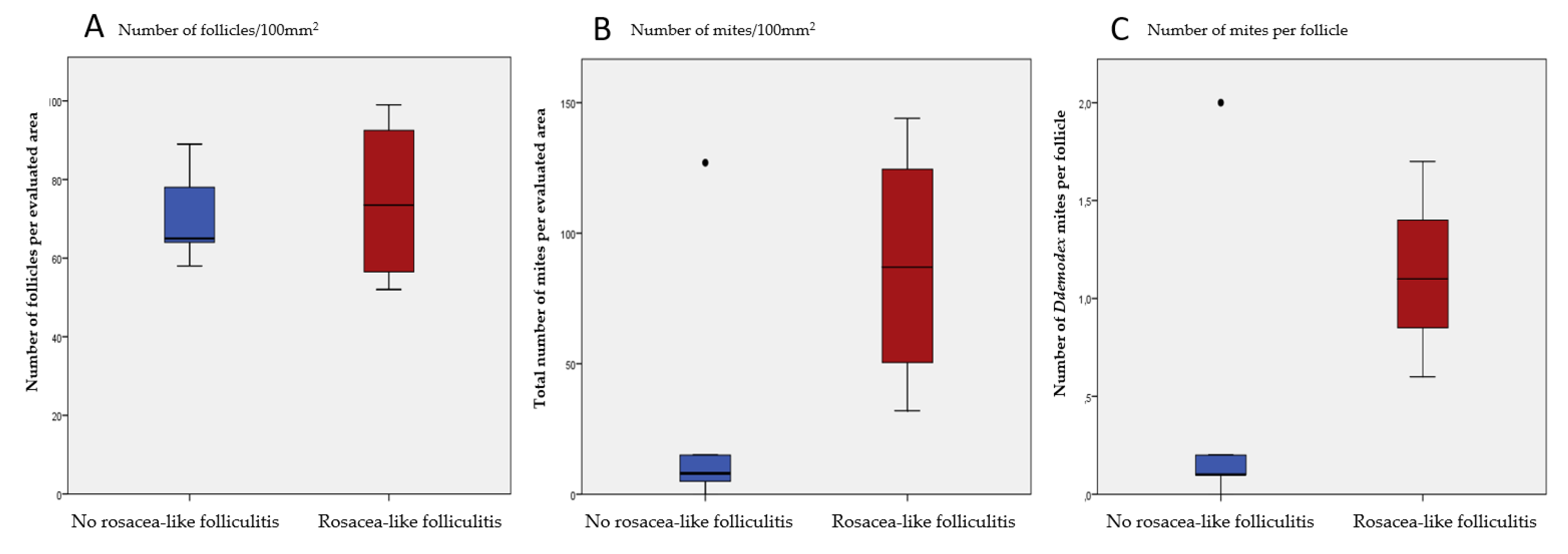
2.3. Diagnostic Procedures for Rosacea-Like Folliculitis
2.4. Statistical Analyses
3. Results
3.1. Baseline Population
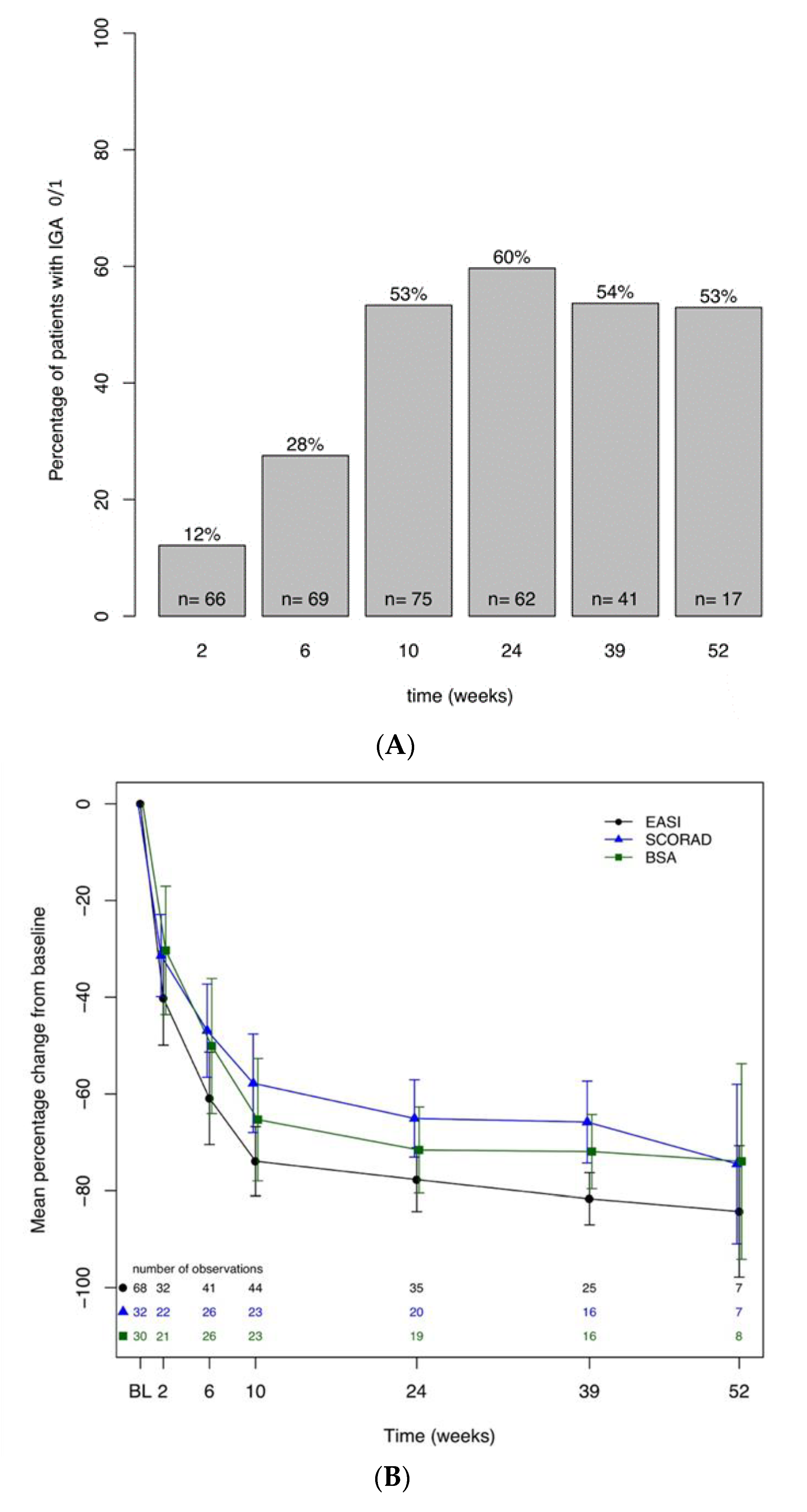
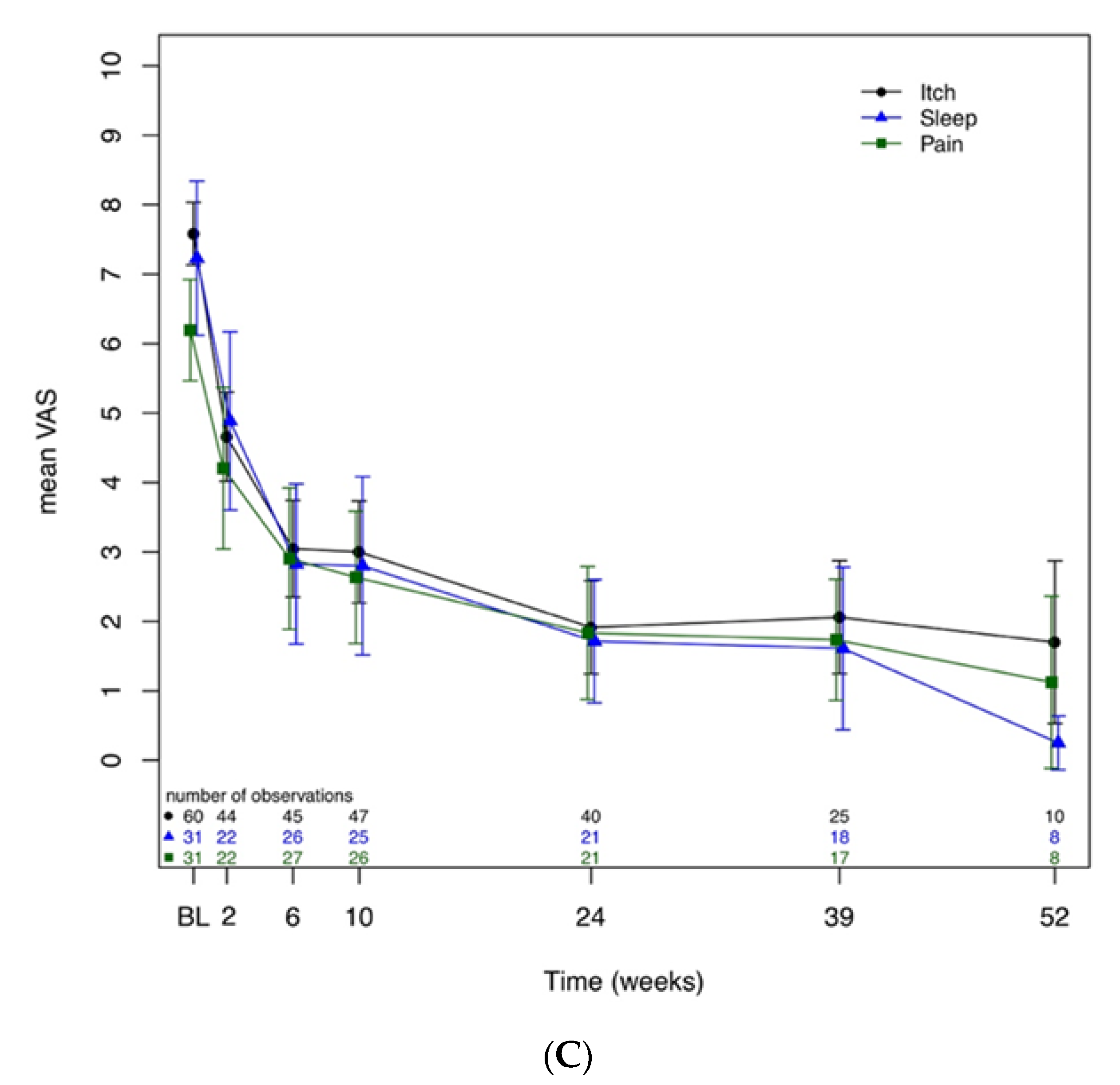
3.2. Clinical Effectiveness of Dupilumab
3.3. Safety
3.4. Discontinuation of Dupilumab
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Paternoster, L.; Savenije, O.E.; Heron, J.; Evans, D.M.; Vonk, J.M.; Brunekreef, B.; Wijga, A.H.; Henderson, A.J.; Koppelman, G.H.; Brown, S.J. Identification of atopic dermatitis subgroups in children from 2 longitudinal birth cohorts. J. Allergy Clin. Immunol. 2018, 141, 964–971. [Google Scholar] [CrossRef]
- Barbarot, S.; Auziere, S.; Gadkari, A.; Girolomoni, G.; Puig, L.; Simpson, E.L.; Margolis, D.J.; de Bruin-Weller, M.; Eckert, L. Epidemiology of atopic dermatitis in adults: Results from an international survey. Allergy 2018, 73, 1284–1293. [Google Scholar] [CrossRef] [PubMed]
- Weidinger, S.; Novak, N. Atopic dermatitis. Lancet 2016, 387, 1109–1122. [Google Scholar] [CrossRef]
- Beck, L.A.; Thaçi, D.; Hamilton, J.D.; Graham, N.M.; Bieber, T.; Rocklin, R.; Ming, J.E.; Ren, H.; Kao, R.; Simpson, E.; et al. Dupilumab treatment in adults with moderate-to-severe atopic dermatitis. N. Engl. J. Med. 2014, 371, 130–139. [Google Scholar] [CrossRef]
- Hanifin, J.M.; Reed, M.L. A population-based survey of eczema prevalence in the United States. Dermatitis 2007, 18, 82–91. [Google Scholar] [CrossRef]
- Vestergaard, C.; Deleuran, M. Advances in the diagnosis and therapeutic management of atopic dermatitis. Drugs 2014, 74, 757–769. [Google Scholar] [CrossRef]
- Torres, T.; Ferreira, E.O.; Goncalo, M.; Mendes-Bastos, P.; Selores, M.; Filipe, P. Update on Atopic Dermatitis. Acta Med. Port. 2019, 32, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Ariens, L.F.; Gadkari, A.; Van Os-Medendorp, H.; Ayyagari, R.; Terasawa, E.; Kuznik, A.; Chen, Z.; Bagousse, G.B.L.; Lu, Y.; Rizova, E.; et al. Dupilumab Versus Cyclosporine for the Treatment of Moderate-to-Severe Atopic Dermatitis in Adults: Indirect Comparison Using the Eczema Area and Severity Index. Acta Derm. Venereol 2019, 99, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Blauvelt, A.; de Bruin-Weller, M.; Gooderham, M.; Cather, J.C.; Weisman, J.; Pariser, D.; Simpson, E.L.; Papp, K.A.; Hong, H.C.H.; Rubel, D.; et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): A 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet 2017, 389, 2287–2303. [Google Scholar] [CrossRef]
- de Bruin-Weller, M.; Thaçi, D.; Smith, C.H.; Reich, K.; Cork, M.J.; Radin, A.; Zhang, Q.; Akinlade, B.; Gadkari, A.; Eckert, L.; et al. Dupilumab with concomitant topical corticosteroid treatment in adults with atopic dermatitis with an inadequate response or intolerance to ciclosporin A or when this treatment is medically inadvisable: A placebo-controlled, randomized phase III clinical trial (LIBERTY AD CAFE). Br. J. Dermatol. 2018, 178, 1083–1101. [Google Scholar] [PubMed]
- Simpson, E.L.; Bieber, T.; Guttman-Yassky, E.; Beck, L.A.; Blauvelt, A.; Cork, M.J.; Silverberg, J.I.; Deleuran, M.; Kataoka, Y.; Lacour, J.P.; et al. Two Phase 3 Trials of Dupilumab versus Placebo in Atopic Dermatitis. N. Engl. J. Med. 2016, 375, 2335–2348. [Google Scholar] [CrossRef] [PubMed]
- Mareschal, A.; Puzenat, E.; Aubin, F. Dupilumab Efficacy and Safety in Adolescents with Moderate-to-Severe Atopic Dermatitis: A Case Series. Acta Derm. Venereol. 2020, 100, adv00014. [Google Scholar] [CrossRef] [PubMed]
- Hanifin, J.M.; Cooper, K.D.; Ho, V.C.; Kang, S.; Krafchik, B.R. Guidelines of care for atopic dermatitis, developed in accordance with the American Academy of Dermatology (AAD)/American Academy of Dermatology Association "Administrative Regulations for Evidence-Based Clinical Practice Guidelines". J. Am. Acad. Dermatol. 2004, 50, 391–404. [Google Scholar] [CrossRef]
- Czarnowicki, T.; He, H.; Krueger, J.G.; Guttman-Yassky, E. Atopic dermatitis endotypes and implications for targeted therapeutics. J. Allergy Clin. Immunol. 2019, 143, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Rajadhyaksha, M.; Grossman, M.; Esterowitz, D.; Webb, R.H.; Anderson, R.R. In vivo confocal scanning laser microscopy of human skin: Melanin provides strong contrast. J. Investig. Dermatol. 1995, 104, 946–952. [Google Scholar] [CrossRef] [PubMed]
- Sattler, E.C.; Hoffmann, V.S.; Ruzicka, T.; Braunmuhl, T.V.; Berking, C. Reflectance confocal microscopy for monitoring the density of Demodex mites in patients with rosacea before and after treatment. Br. J. Dermatol. 2015, 173, 69–75. [Google Scholar] [CrossRef]
- Kenward, M.G.; Roger, J.H. Small sample inference for fixed effects from restricted maximum likelihood. Biometrics 1997, 53, 983–997. [Google Scholar] [CrossRef]
- Thiboutot, D.; Anderson, R.; Cook-Bolden, F.; Draelos, Z.; Gallo, R.; Granstein, R.; Kang, S.; Macsai, M.; Gold, L.S.; Tan, J. Standard Management Options for Rosacea: The 2019 Update by the National Rosacea Society Expert Committee. J. Am. Acad. Dermatol. 2020. Epub ahead of print. [Google Scholar] [CrossRef]
- Maier, T.; Sattler, E.; Braun-Falco, M.; Ruzicka, T.; Berking, C. High-definition optical coherence tomography for the in vivo detection of demodex mites. Dermatology 2012, 225, 271–276. [Google Scholar] [CrossRef]
- Turgut Erdemir, A.; Gurel, M.S.; Koku Aksu, A.E.; Bilgin Karahalli, F.; Incel, P.; Kutlu Haytoğlu, N.S.; Falay, T. Reflectance confocal microscopy vs. standardized skin surface biopsy for measuring the density of Demodex mites. Skin Res. Technol. 2014, 20, 435–439. [Google Scholar] [CrossRef]
- Faiz, S.; Giovannelli, J.; Podevin, C.; Jachiet, M.; Bouaziz, J.D.; Reguiai, Z.; Nosbaum, A.; Lasek, A.; Le Bouedec, M.C.F.; Du Thanh, A.; et al. Effectiveness and safety of dupilumab for the treatment of atopic dermatitis in a real-life French multicenter adult cohort. J. Am. Acad Dermatol. 2019, 81, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Olesen, C.M.; Holm, J.G.; Norreslet, L.B.; Serup, J.V.; Thomsen, S.F.; Agner, T. Treatment of atopic dermatitis with dupilumab: Experience from a tertiary referral centre. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1562–1568. [Google Scholar] [CrossRef] [PubMed]
- De Wijs, L.E.M.; Bosma, A.L.; Erler, N.S.; Hollestein, L.M.; Gerbens, L.A.A.; Middelkamp-Hup, M.A.; Kunkeler, A.C.M.; Nijsten, T.E.C.; Spuls, P.I.; Hijnen, D.J. Effectiveness of dupilumab treatment in 95 patients with atopic dermatitis: Daily practice data. Br. J. Dermatol. 2019, 182, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Thijs, J.; Krastev, T.; Weidinger, S.; Buckens, C.F.; de Bruin-Weller, M.; Bruijnzeel-Koomen, C.; Flohr, C.; Hijnen, D. Biomarkers for atopic dermatitis: A systematic review and meta-analysis. Curr. Opin. Allergy Clin. Immunol. 2015, 15, 453–460. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Bissonnette, R.; Ungar, B.; Suárez-Fariñas, M.; Ardeleanu, M.; Esaki, H.; Suprun, M.; Estrada, Y.; Xu, H.; Peng, X.; et al. Dupilumab progressively improves systemic and cutaneous abnormalities in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2019, 143, 155–172. [Google Scholar] [CrossRef]
- Punnonen, J.; Yssel, H.; de Vries, J.E. The relative contribution of IL-4 and IL-13 to human IgE synthesis induced by activated CD4+ or CD8+ T cells. J. Allergy Clin. Immunol. 1997, 100, 792–801. [Google Scholar] [CrossRef]
- Bachert, C.; Hellings, P.W.; Mullol, J.; Hamilos, D.L.; Gevaert, P.; Naclerio, R.M.; Joish, V.N.; Chao, J.; Mannent, L.P.; Amin, N.; et al. Dupilumab improves health-related quality of life in patients with chronic rhinosinusitis with nasal polyposis. Allergy 2019, 75, 148–157. [Google Scholar] [CrossRef]
- Jonstam, K.; Swanson, B.N.; Mannent, L.P.; Cardell, L.O.; Tian, N.; Wang, Y.; Zhang, D.; Fan, C.; Holtappels, G.; Hamilton, J.D.; et al. Dupilumab reduces local type 2 pro-inflammatory biomarkers in chronic rhinosinusitis with nasal polyposis. Allergy 2019, 74, 743–752. [Google Scholar] [CrossRef]
- Busse, W.W.; Maspero, J.F.; Rabe, K.F.; Papi, A.; Wenzel, S.E.; Ford, L.B.; Pavord, I.D.; Zhang, B.; Staudinger, H.; Pirozzi, G.; et al. Liberty Asthma QUEST: Phase 3 Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Study to Evaluate Dupilumab Efficacy/Safety in Patients with Uncontrolled, Moderate-to-Severe Asthma. Adv. Ther. 2018, 35, 737–748. [Google Scholar] [CrossRef]
- Rabe, K.F.; Nair, P.; Brusselle, G.; Maspero, J.F.; Castro, M.; Sher, L.; Zhu, H.; Hamilton, J.D.; Swanson, B.N.; Khan, A.; et al. Efficacy and Safety of Dupilumab in Glucocorticoid-Dependent Severe Asthma. N. Engl. J. Med. 2018, 378, 2475–2485. [Google Scholar] [CrossRef]
- Wang, F.P.; Tang, X.J.; Wei, C.Q.; Xu, L.R.; Mao, H.; Luo, F.M. Dupilumab treatment in moderate-to-severe atopic dermatitis: A systematic review and meta-analysis. J. Dermatol. Sci. 2018, 90, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Wohlrab, J.; Werfel, T.; Wollenberg, A. Pathomechanism of dupilumab-associated inflammatory eye symptoms. J. Eur. Acad. Dermatol. Venereol. 2019, 33, e435–e436. [Google Scholar] [CrossRef] [PubMed]
- Buhl, T.; Sulk, M.; Nowak, P.; Buddenkotte, J.; McDonald, I.; Aubert, J.; Carlavan, I.; Déret, S.; Reiniche, P.; Rivier, M.; et al. Molecular and Morphological Characterization of Inflammatory Infiltrate in Rosacea Reveals Activation of Th1/Th17 Pathways. J. Investig. Dermatol. 2015, 135, 2198–2208. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.T.; Lee, S.H.; Chun, Y.S.; Kim, J.C. Tear cytokines and chemokines in patients with Demodex blepharitis. Cytokine 2011, 53, 94–99. [Google Scholar] [CrossRef]
- Thyssen, J.P. Could conjunctivitis in patients with atopic dermatitis treated with dupilumab be caused by colonization with Demodex and increased interleukin-17 levels? Br. J. Dermatol. 2018, 178, 1220. [Google Scholar] [CrossRef]
- Voorberg, A.N.; den Dunnen, W.F.A.; Wijdh, R.H.J.; de Bruin-Weller, M.S.; Schuttelaar, M.L.A. Recurrence of conjunctival goblet cells after discontinuation of dupilumab in a patient with dupilumab-related conjunctivitis. J. Eur. Acad. Dermatol. Venereol. 2019. [Google Scholar] [CrossRef]
- Ivert, L.U.; Wahlgren, C.F.; Ivert, L.; Lundqvist, M.; Bradley, M. Eye Complications During Dupilumab Treatment for Severe Atopic Dermatitis. Acta Derm. Venereol. 2019, 99, 375–378. [Google Scholar] [CrossRef]
- Heibel, H.D.; Hendricks, A.J.; Foshee, J.P.; Shi, V.Y. Rosacea associated with dupilumab therapy. J. Dermatol. Treat. 2019, 2019, 1–3. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | 18–87 y | |
| Sex | Male | Female |
| n (%) | 59 (63%) | 35 (37%) |
| Atopic dermatitis (AD); n (%) | ||
| AD Intrinsic (IgE levels < 150 klU/L) | 11 (11.7%) | |
| AD Extrinsic (IgE levels > 150 klU/L) | 84 (89.4%) | |
| Scores at Baseline | ||
| Investigator Initiated Scores | ||
| IGA a (0–4) | 3.9 ± 0.7 | |
| EASI a (0–72) | 26.5 ± 12.5 | |
| SCORAD a (0–103) | 69.2 ± 11.6 | |
| BSA a (0–100%) | 60.2 ± 19 | |
| Patient-Oriented Scores | ||
| DLQI a (0–30) | 17.3 ± 6.5 | |
| Itch a (0–10) | 7.6 ± 1.7 | |
| Sleep a (0–10) | 7.2 ± 3 | |
| Pain a (0–10) | 6.2 ± 2 | |
| Biomarkers at Baseline | Value (first quartile, third quartile); sample size (n) | |
| Total IgE b klU/L | 3715 (557.5, 5000); n = 66 | |
| ECP b μg/L | 34.4 (24.15, 61,825); n = 30 | |
| LDH b U/L | 245.5 (205, 303.75); n = 64 | |
| Allergic Asthma; n (%) | 26 (27.6%) | |
| Asthma Control Test (ACT) a (0–25) | 18.4 ± 4.9 | |
| Previous Treatments; n (%) | ||
| Topical Treatments (Calcineurin Inhibitors, Corticosteroids) | 94 (100%) | |
| Systemic Treatments | 94 (100%) | |
| Phototherapy (NB UVB/PUVA) | 61 (64.9%) | |
| Cyclosporine A | 34 (36.2%) | |
| Methothrexate | 15 (15.9%) | |
| Azathrioprine | 8 (8.5%) | |
| Other (IVIG c, Omalizumab, Rituximab) | 26 (27.6%) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quint, T.; Brunner, P.M.; Sinz, C.; Steiner, I.; Ristl, R.; Vigl, K.; Kimeswenger, S.; Neubauer, K.; Pirkhammer, D.; Zikeli, M.; et al. Dupilumab for the Treatment of Atopic Dermatitis in an Austrian Cohort-Real-Life Data Shows Rosacea-Like Folliculitis. J. Clin. Med. 2020, 9, 1241. https://doi.org/10.3390/jcm9041241
Quint T, Brunner PM, Sinz C, Steiner I, Ristl R, Vigl K, Kimeswenger S, Neubauer K, Pirkhammer D, Zikeli M, et al. Dupilumab for the Treatment of Atopic Dermatitis in an Austrian Cohort-Real-Life Data Shows Rosacea-Like Folliculitis. Journal of Clinical Medicine. 2020; 9(4):1241. https://doi.org/10.3390/jcm9041241
Chicago/Turabian StyleQuint, Tamara, Patrick M. Brunner, Christoph Sinz, Irene Steiner, Robin Ristl, Kornelia Vigl, Susanne Kimeswenger, Katharina Neubauer, Detlev Pirkhammer, Martin Zikeli, and et al. 2020. "Dupilumab for the Treatment of Atopic Dermatitis in an Austrian Cohort-Real-Life Data Shows Rosacea-Like Folliculitis" Journal of Clinical Medicine 9, no. 4: 1241. https://doi.org/10.3390/jcm9041241
APA StyleQuint, T., Brunner, P. M., Sinz, C., Steiner, I., Ristl, R., Vigl, K., Kimeswenger, S., Neubauer, K., Pirkhammer, D., Zikeli, M., Hoetzenecker, W., Reider, N., & Bangert, C. (2020). Dupilumab for the Treatment of Atopic Dermatitis in an Austrian Cohort-Real-Life Data Shows Rosacea-Like Folliculitis. Journal of Clinical Medicine, 9(4), 1241. https://doi.org/10.3390/jcm9041241