Clinical Characteristics of Diagnosis for Internet Gaming Disorder: Comparison of DSM-5 IGD and ICD-11 GD Diagnosis

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
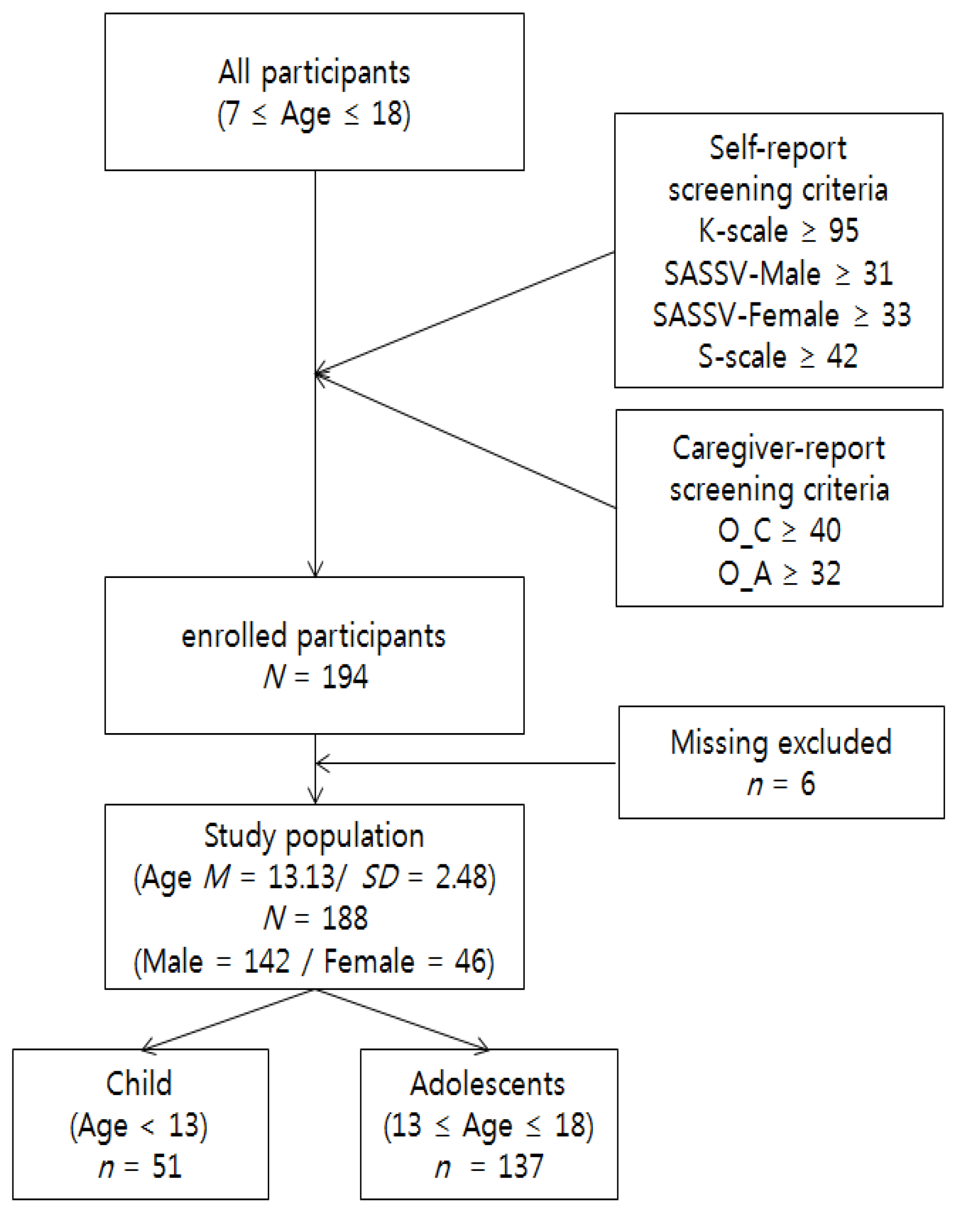
2.1. Participants and Procedure
2.2. Measures
2.2.1. Diagnostic Interview for Internet, Game, SNS, etc. Addiction (DIA)
2.2.2. Diagnostic Interview for Comorbid Psychiatric Disorders
2.3. Data Management and Analysis
2.4. Ethical Approval
3. Results
3.1. Comparison of DSM-5 IGD Diagnosis and ICD-11 GD Diagnosis
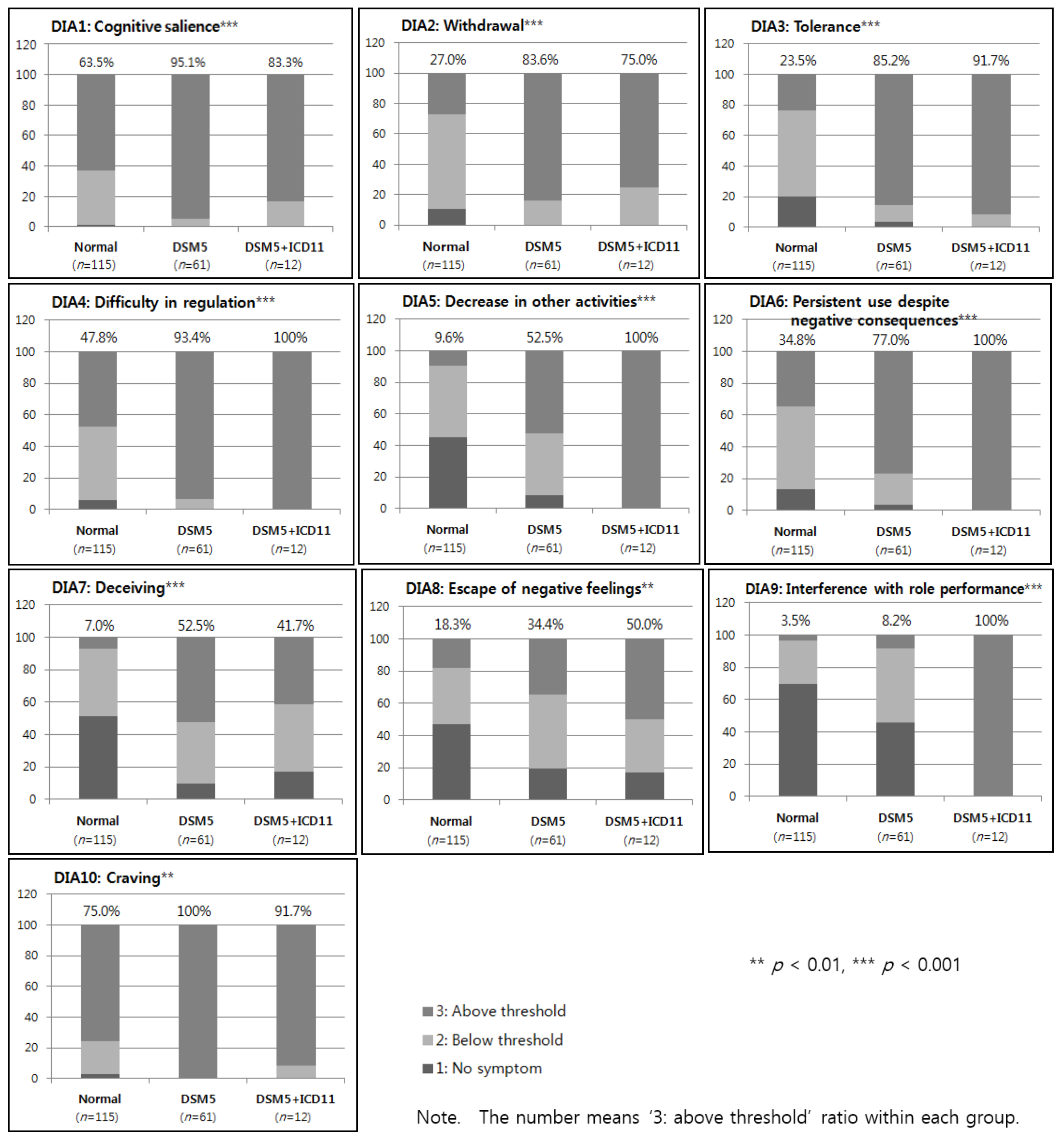
3.2. Clinical Characteristics of IGD Diagnosis Groups
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Korean Ministry of Science and ICT. The Survey Internet/Smartphone Overdependence in 2018; Korean National Information Society Agency: Seoul, Korea, 2019.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- World Health Organization. Public Health Implications of Excessive Use of the Internet, Computers, Smartphones and Similar Electronic Devices Meeting Report; World Health Organization: Tokyo, Japan, 2014. [Google Scholar]
- World Health Organization. Print Versions for the ICD-11 Beta Draft (Mortality and Morbidity Statistics); World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. The ICD-11 Classification of Mental and Behavioral Disorders: Diagnostic Criteria for Research; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Korean Addiction Form. Public Health Response to Health Problems Related to Excessive Use of Game; Korean Association Medical Law: Seoul, Korea, 2019. [Google Scholar]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems (ICD-11): New Release; World Health Assembly: Geneva, Switzerland, 2019; Available online: https://www.who.int/news-room/detail/25-05-2019-world-health-assembly-update (accessed on 26 May 2019).
- Kuss, D.J.; Griffiths, M.D.; Pontes, H.M. Chaos and confusion in DSM-5 diagnosis of internet gaming disorder: Issues, concerns, and recommendations for clarity in the field. J. Behav. Addict. 2017, 6, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Kuss, D.J.; Griffiths, M.D.; Pontes, H.M. DSM-5 diagnosis of internet gaming disorder: Some ways forward in overcoming issues and concerns in the gaming studies field. J. Behav. Addict. 2017, 6, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Aarseth, E.; Bean, A.M.; Boonen, H.; Colder Carras, M.; Coulson, M.; Das, D.; Deleuze, J.; Dunkels, E.; Edman, J.; Ferguson, C.J.; et al. Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal. J. Behav. Addict. 2017, 6, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Van den Brink, W. ICD-11 Gaming Disorder: Needed and just in time or dangerous and much too early? J. Behav. Addict. 2017, 6, 290–292. [Google Scholar] [CrossRef] [PubMed]
- Rumpf, H.J.; Achab, S.; Billieux, J.; Bowden-Jones, H.; Carragher, N.; Demetrovics, Z.; Higuchi, S.; King, D.L.; Mann, K.; Potenza, M.; et al. Including gaming disorder in the ICD-11: The need to do so from a clinical and public health perspective. J. Behav. Addict. 2018, 7, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Han, D.H.; Lyoo, I.K.; Renshaw, P.F. Differential regional gray matter volumes in patients with on-line game addiction and professional gamers. J. Psychiatr. Res. 2012, 46, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Han, D.H.; Yoo, M.; Renshaw, P.F.; Petry, N.M. A cohort study of patients seeking internet gaming disorder treatment. J. Behav. Addict. 2018, 7, 930–938. [Google Scholar] [CrossRef]
- Yuan, K.; Qin, W.; Wang, G.; Zeng, F.; Zhao, L.; Yang, X.; Liu, P.; Liu, J.; Sun, J.; Gong, Q.; et al. Microstructure abnormalities in adolescents with internet addiction disorder. PLoS ONE 2011, 6, e20708. [Google Scholar] [CrossRef]
- Pickard, H. Denial in addiction. Mind Lang. 2016, 31, 277–299. [Google Scholar] [CrossRef]
- Jeong, H.; Yim, H.W.; Lee, S.Y.; Lee, H.K.; Potenza, M.N.; Kwon, J.H.; Koo, H.J.; Kweon, Y.S.; Bhang, S.Y.; Choi, J.S. Discordance between self-report and clinical diagnosis of internet gaming disorder in adolescents. Sci. Rep. 2018, 8, 10084. [Google Scholar] [CrossRef]
- Jeong, H.; Yim, H.W.; Lee, S.Y.; Lee, H.K.; Bhang, S.Y.; Jo, S.J.; Kwon, Y.S.; Choi, J.S. Comparison of the proposed DSM-5 IGD diagnostic criteria and clinical interview by psychiatrist in adolescents. J. Korean Acad. Addict. Psychiatry 2018, 22, 42–47. [Google Scholar]
- Lee, S.Y.; Lee, H.K.; Jeong, H.; Yim, H.W.; Bhang, S.Y.; Jo, S.J.; Baek, K.Y.; Kim, E.; Kim, M.S.; Choi, J.S. The hierarchical implications of internet gaming disorder criteria: Which indicate more severe pathology? Psychiatry Investig. 2017, 14, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Korean National Information Society Agency. A Validation Study of K-Scale as a Diagnostic Tool; Korean National Information Society Agency: Seoul, Korea, 2013. [Google Scholar]
- Kwon, M.; Kim, D.-J.; Cho, H.; Yang, S. The smartphone addiction scale: Development and validation of a short version for adolescents. PLoS ONE 2013, 8, e83558. [Google Scholar] [CrossRef]
- Kim, D.I.; Chung, Y.J.; Lee, Y.H.; Kim, B.K.; Jeon, H.J. Development and Validation of Youth Smartphone Addiction Self-report Scale. Korean J. Couns. 2016, 17, 319–335. [Google Scholar]
- Kim, D.I.; Chung, Y.J.; Lee, Y.H.; Kim, B.K.; Jeon, H.J.; Lee, Y.H. Development and Validation of Child Smartphone Addiction Observer Scale. Korean J. Couns. 2015, 16, 369–383. [Google Scholar]
- Korean National Information Society Agency. Third Standardization of Korean Internet Addiction Proneness Scale; NIA IV-RER-11050; Korean National Information Society Agency: Seoul, Korea, 2011. [Google Scholar]
- Ryu, H.; Lee, J.Y.; Choi, A.R.; Chung, S.J.; Park, M.K.; Bhang, S.Y.; Kwon, J.G.; Kweon, Y.S.; Choi, J.S. Application of diagnostic interview for internet addiction (DIA) in clinical practice for Korean adolescents. J. Clin. Med. 2019, 8, 202. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Cheon, K.A.; Kim, B.N.; Chang, S.A.; Yoo, H.J.; Kim, J.W.; Cho, S.C.; Seo, D.H.; Bae, M.O.; So, Y.K.; et al. The reliability and validity of kiddie schedule for affective disorders and schizophrenia present and lifetime version-korean version (K-SADS-PL-K). Yonsei Med. J. 2004, 45, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Qi, X.; Yang, Y.; Du, G.; Gao, P.; Zhang, Y.; Qin, W.; Li, X.; Zhang, Q. Altered structural correlates of impulsivity in adolescents with internet gaming disorder. Front. Hum. Neurosci. 2016, 10, 4. [Google Scholar] [CrossRef]
- Ko, C.-H.; Hsieh, T.-J.; Wang, P.-W.; Lin, W.-C.; Yen, C.-F.; Chen, C.-S.; Yen, J.-Y. Altered gray matter density and disrupted functional connectivity of the amygdala in adults with internet gaming disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2015, 57, 185–192. [Google Scholar] [CrossRef]
- Yen, J.Y.; Liu, T.L.; Wang, P.W.; Chen, C.S.; Yen, C.F.; Ko, C.H. Association between internet gaming disorder and adult attention deficit and hyperactivity disorder and their correlates: Impulsivity and hostility. Addict. Behav. 2017, 64, 308–313. [Google Scholar] [CrossRef]
- Liu, L.; Yao, Y.W.; Li, C.R.; Zhang, J.T.; Xia, C.C.; Lan, J.; Ma, S.S.; Zhou, N.; Fang, X.Y. The comorbidity between internet gaming disorder and depression: Interrelationship and neural mechanisms. Front Psychiatry 2018, 23, 154. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.R.; Cho, H.; Kim, D.J. Prevalence and correlates of comorbid depression in a nonclinical online sample with DSM-5 internet gaming disorder. J. Affect. Disord. 2018, 226, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Han, D.H.; Lee, Y.S.; Na, C.; Ahn, J.Y.; Chung, U.S.; Daniels, M.A.; Hawse, C.A.; Renshaw, P.F. The effect of methylphenidate on internet video game play in children with attention-deficit/hyperactivity disorder. Compr. Psychiatry 2009, 50, 251–256. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Item | Standardized Representative Questions |
|---|---|
| 1. Cognitive salience | “Even if you are not using the Internet/game/social network service (SNS), do you spend a lot of time thinking about the Internet/game/SNS or planning what to do next?” |
| 2. Withdrawal | “Do you experience restlessness, irritability, depression, anxiety, sadness, etc. when you reduce, stop, or do not allow Internet/game/SNS?” |
| 3. Tolerance | “Do you want to spend more Internet/game/SNS time, find more interesting things, or use better equipment such as cell phones or computers to make it feel as fun as before?” |
| 4. Difficulty in regulating use | “Do you feel you should reduce Internet/game/SNS use, but cannot reduce the time you spend doing Internet/game/SNS?” |
| 5. Decrease in other activities | “Because of the Internet/game/SNS, are you less interested in participating in other leisure activities such as hobbies or meeting friends?” |
| 6. Persistent use despite negative consequences | “Despite negative consequences, such as lack of sleep time, being late to school or work, spending too much money, debating with other people, or neglecting important things, do you continue the Internet/game/SNS use?” |
| 7. Deceiving | “Do you lie or hide how much time you spend on the Internet/game/SNS to your family or friends?” |
| 8. Escape of negative feelings | “Do you use the Internet/game/SNS to avoid/relieve negative feelings?” “Do you use the game to forget unpleasant moods (e.g., helplessness, depression, guilt, anxiety, etc.)?” |
| 9. Interference with role performance | “Have you ever been troubled or fallen out due to the use of Internet/game/SNS in your important interpersonal, career, and academic settings?” |
| 10. Craving | “Do you have a strong desire to engage in activities such as using the Internet/game/SNS?” “If you want to play on Internet/game/SNS, is this desire difficult to tolerate?” |
| n (%) | ICD-11 Game Disorder (GD) Diagnosis Criteria | All | ||
|---|---|---|---|---|
| Normal | GD | |||
| DSM-5 IGD Diagnosis Criteria | Normal | 115 (61.2) | 0 | 115 (61.2) |
| IGD | 61 (32.4) | 12 (6.4) | 73 (38.8) | |
| All | 176 (93.6) | 12 (6.4) | 188 (100) | |
| n (%) | Normal (n = 115) | DSM5 (n = 61) | DSM5 + ICD11 (n = 12) | All (n = 188) | x2 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Internet content (percentage in all group) | 4.19 | |||||||||
| 1. Game | 26 (13.8) | 15 (8.0) | 2 (1.1) | 43 (22.9) | ||||||
| 2. SNS | 9 (4.8) | 2 (1.1) | 0 | 11 (5.9) | ||||||
| 3. Other (YouTube, Africa TV) | 9 (4.8) | 5 (2.7) | 0 | 14 (7.4) | ||||||
| 4. Combined | 1. | 71 (37.8) | 51/11 | 39 (20.7) | 23/7 | 10 (5.3) | 8/2 | 120 (63.8) | 82/20 | |
| 2. | 8/14 | 6/2 | 0/1 | 14/17 | ||||||
| 3. | 12/46 | 10/30 | 2/7 | 24/83 | ||||||
| Internet device (percentage in all group) | 8.359 | |||||||||
| PC | 10 (5.3) | 10 (5.3) | 2 (1.1) | 22 (11.7) | ||||||
| Smartphone | 55 (29.3) | 18 (9.6) | 4 (2.1) | 77 (41.0) | ||||||
| Other (tablet PC) | 2 (1.0) | 0 | 0 | 2 (1.0) | ||||||
| Combination | 48 (25.5) | 33 (17.6) | 6 (3.2) | 87 (46.3) | ||||||
| n (%) | Normal (n = 115) | DSM5 (n = 61) | DSM5 + ICD11 (n = 12) | All (n = 188) | x2 |
|---|---|---|---|---|---|
| Psychiatric disorder (percentage within each group) | |||||
| Depressive dis. | 12 (10.4) | 12 (19.7) | 4 (33.3) | 28 (15.0) | 6.229 * |
| ADHD | 37 (32.2) | 25 (41.0) | 7 (58.3) | 69 (36.7) | 4.056 |
| Anxiety dis. | 3 (2.6) | 1 (1.6) | 0 | 4 (2.1) | 0.447 |
| OCD | 2 (1.1) | 1 (1.6) | 0 | 3 (1.6) | 0.20 |
| ODD + CD | 2 (1.7) | 1 (1.6) | 4 (33.3) | 7 (3.7) | 31.160 *** |
| Tic dis. | 4 (3.5) | 0 | 0 | 4 (2.1) | 2.559 |
| PTSD | 1 (0.9) | 1 (1.6) | 0 | 2 (1.1) | 0.375 |
| n = 188 | a. Normal (n = 115) M(SD) [95%CI] | b. DSM5 (n = 61) M(SD) [95%CI] | c. DSM5 + ICD11 (n = 12) M(SD) [95%CI] | F |
|---|---|---|---|---|
| Age when first used the Internet | 7.47 (1.864) [7.13–7.82] | 7.57 (2.384) [6.96–8.18] | 7.42 (2.539) [5.80–9.03] | 0.056 |
| Age when first started internet games | 8.06 (2.429) [7.61–8.51] | 8.28 (2.138) [7.73–8.83] | 8.42 (2.109) [7.08–9.76] | 0.256 |
| Age when first used smartphones | 8.62 (2.130) [8.23–9.02] | 8.87 (1.928) [8.38–9.36] | 7.67 (1.875) [6.48–8.86] | 1.734 |
| Amount of time spent during weekdays (min/day) | 248.78 (137.962) [223.30–274.27] | 254.92 (146.579) [217.38–292.46] | 290.00 (257.858) [126.16–453.84] | 0.412 |
| Amount of time spent during weekend (min/day) | 361.57 (172.787) [329.65–393.48] | 400.82 (186.148) [353.15–448.49] | 477.50 (273.899) [303.47–651.53] | 2.626 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jo, Y.S.; Bhang, S.Y.; Choi, J.S.; Lee, H.K.; Lee, S.Y.; Kweon, Y.-S. Clinical Characteristics of Diagnosis for Internet Gaming Disorder: Comparison of DSM-5 IGD and ICD-11 GD Diagnosis. J. Clin. Med. 2019, 8, 945. https://doi.org/10.3390/jcm8070945
Jo YS, Bhang SY, Choi JS, Lee HK, Lee SY, Kweon Y-S. Clinical Characteristics of Diagnosis for Internet Gaming Disorder: Comparison of DSM-5 IGD and ICD-11 GD Diagnosis. Journal of Clinical Medicine. 2019; 8(7):945. https://doi.org/10.3390/jcm8070945
Chicago/Turabian StyleJo, Yeong Seon, Soo Young Bhang, Jung Seok Choi, Hae Kook Lee, Seung Yup Lee, and Yong-Sil Kweon. 2019. "Clinical Characteristics of Diagnosis for Internet Gaming Disorder: Comparison of DSM-5 IGD and ICD-11 GD Diagnosis" Journal of Clinical Medicine 8, no. 7: 945. https://doi.org/10.3390/jcm8070945
APA StyleJo, Y. S., Bhang, S. Y., Choi, J. S., Lee, H. K., Lee, S. Y., & Kweon, Y.-S. (2019). Clinical Characteristics of Diagnosis for Internet Gaming Disorder: Comparison of DSM-5 IGD and ICD-11 GD Diagnosis. Journal of Clinical Medicine, 8(7), 945. https://doi.org/10.3390/jcm8070945