
Do Intraoperative Platelet-Rich Plasma Injections Influence the Final Appearance of Vertical Scars after Breast Reduction? Spectrophotometric Analysis


Abstract
:1. Introduction
2. Materials and Methods
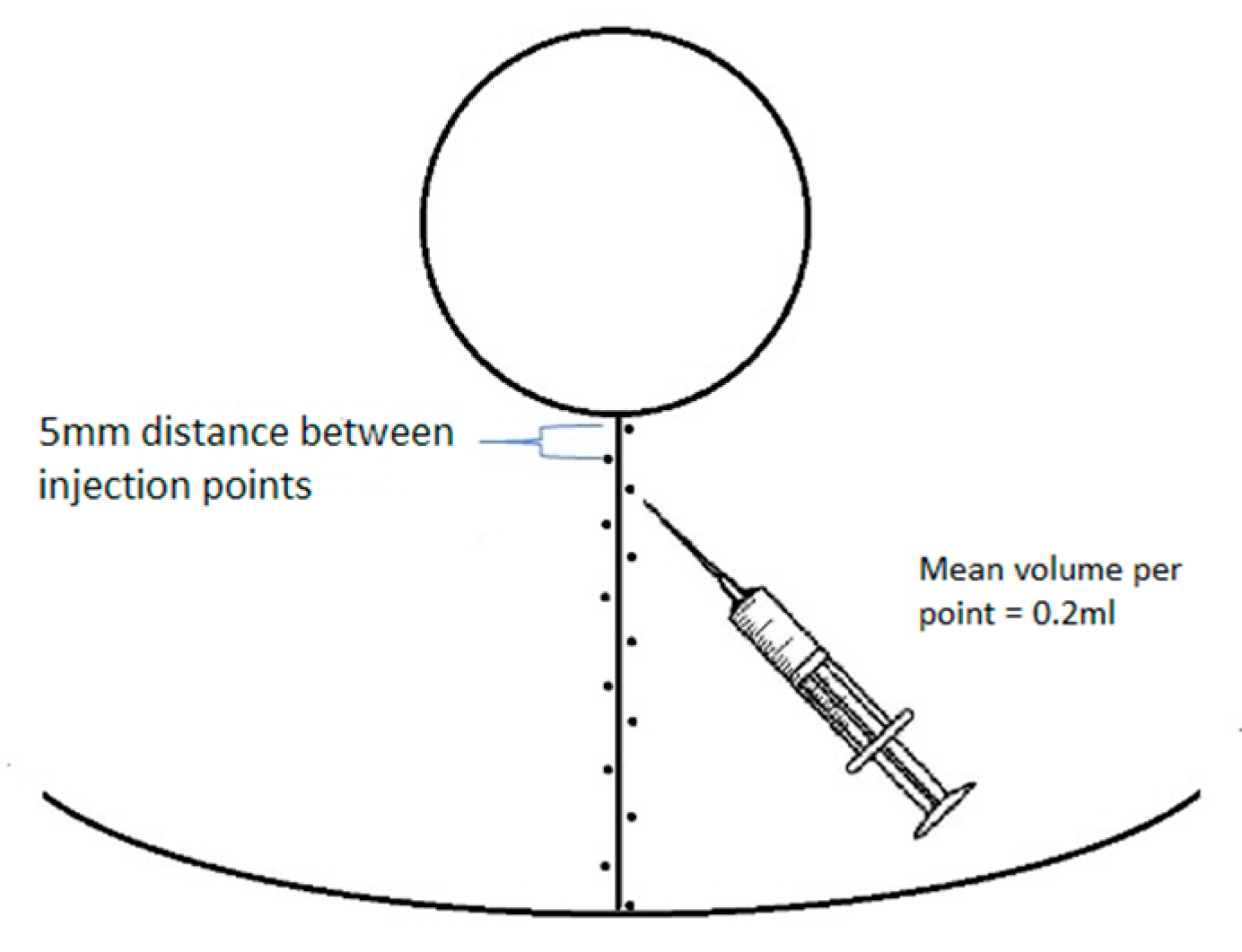
2.1. PRP Quantification
2.2. Statistical Analysis
3. Results
3.1. Spectrophotometric Parameters 3 Months versus 6 Months after Surgery, PRP vs. NaCl
3.2. General Linear Model (GLM)—Variables Influencing Scars’ Scores
3.3. Multivariable Analysis
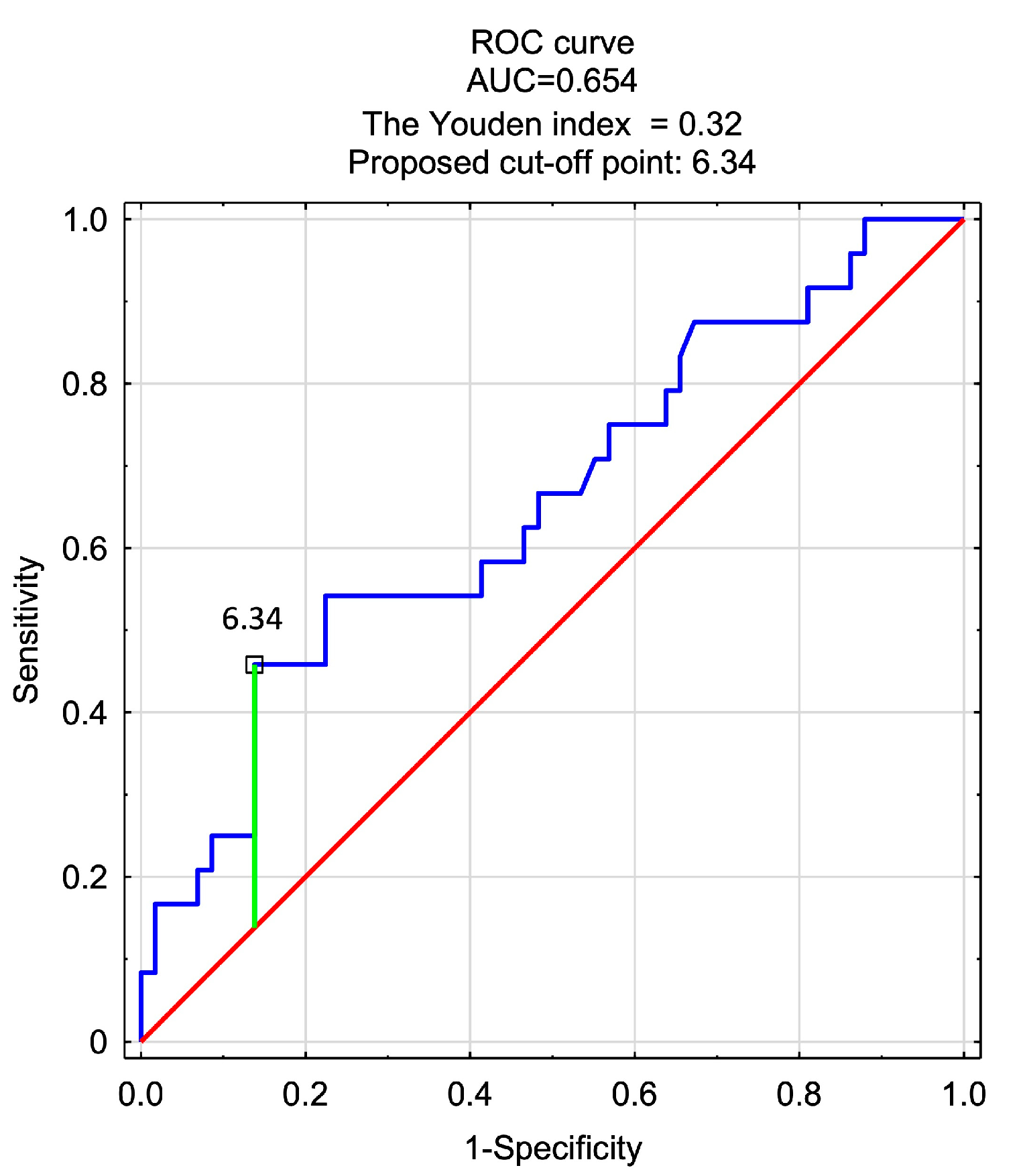
3.4. Logistic Regression Model—Predictors of a Very Good Score in Scar Assessment (>4.5)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ISAPS. Global Survey 2021: Full Report and Press Release in English. Available online: https://www.isaps.org/media/vdpdanke/isaps-global-survey_2021.pdf (accessed on 11 December 2023).
- Wise, R.J. A preliminary report on a method of planning the mammaplasty. Plast. Reconstr. Surg. 1956, 17, 367–375. [Google Scholar] [CrossRef]
- Lassus, C. A technique for breast reduction. Int. Surg. 1970, 53, 69–72. [Google Scholar]
- Lejour, M. Vertical mammaplasty and liposuction of the breast. Plast. Reconstr. Surg. 1994, 94, 100–114. [Google Scholar] [CrossRef] [PubMed]
- Hall-Findlay, E.J.; Shestak, K.C. Breast Reduction. Plast. Reconstr. Surg. 2015, 136, 531e–544e. [Google Scholar] [CrossRef] [PubMed]
- Hammond, D.C.; Loffredo, M. Breast reduction. Plast. Reconstr. Surg. 2012, 129, 829e–839e. [Google Scholar] [CrossRef] [PubMed]
- Lalonde, D.H.; Lalonde, J.; French, R. The no vertical scar breast reduction: A minor variation that allows to remove vertical scar portion of the inferior pedicle wise pattern T scar. Aesthetic Plast. Surg. 2003, 27, 335–344. [Google Scholar] [CrossRef]
- Surowiecka, A. Combined therapies in scar treatment-The role of autologous derived agents in scar remodeling: A series of cases. Dermatol. Ther. 2022, 35, e15877. [Google Scholar] [CrossRef]
- Juhasz, M.L.W.; Cohen, J.L. Microneedling for the Treatment of Scars: An Update for Clinicians. Clin. Cosmet. Investig. Dermatol. 2020, 13, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Khansa, I.; Harrison, B.; Janis, J.E. Evidence-Based Scar Management: How to Improve Results with Technique and Technology. Plast. Reconstr. Surg. 2016, 138, 165s–178s. [Google Scholar] [CrossRef]
- Zheng, W.; Zhao, D.L.; Zhao, Y.Q.; Li, Z.Y. Effectiveness of platelet rich plasma in burn wound healing: A systematic review and meta-analysis. J. Dermatolog. Treat. 2022, 33, 131–137. [Google Scholar] [CrossRef]
- Oneto, P.; Etulain, J. PRP in wound healing applications. Platelets 2021, 32, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.J.; Fylling, C.P.; Parnell, L.K. Use of platelet rich plasma gel on wound healing: A systematic review and meta-analysis. Eplasty 2011, 11, e38. [Google Scholar] [PubMed]
- Broughton, G., 2nd; Janis, J.E.; Attinger, C.E. Wound healing: An overview. Plast. Reconstr. Surg. 2006, 117, 1e-S–32e-S. [Google Scholar] [CrossRef] [PubMed]
- Etulain, J. Platelets in wound healing and regenerative medicine. Platelets 2018, 29, 556–568. [Google Scholar] [CrossRef]
- Oudelaar, B.W.; Peerbooms, J.C.; Huis In ‘t Veld, R.; Vochteloo, A.J.H. Concentrations of Blood Components in Commercial Platelet-Rich Plasma Separation Systems: A Review of the Literature. Am. J. Sports Med. 2019, 47, 479–487. [Google Scholar] [CrossRef]
- Mazzucco, L.; Balbo, V.; Cattana, E.; Guaschino, R.; Borzini, P. Not every PRP-gel is born equal. Evaluation of growth factor availability for tissues through four PRP-gel preparations: Fibrinet, RegenPRP-Kit, Plateltex and one manual procedure. Vox Sang. 2009, 97, 110–118. [Google Scholar] [CrossRef]
- White, C.P.; Farhang Khoee, H.; Kattan, A.E.; Farrokhyar, F.; Hynes, N.M. Breast reduction scars: A prospective survey of patient preferences. Aesthet. Surg. J. 2013, 33, 817–821. [Google Scholar] [CrossRef]
- Sprole, A.M.; Adepoju, I.; Ascherman, J.; Gayle, L.B.; Grant, R.T.; Talmor, M. Horizontal or vertical? an evaluation of patient preferences for reduction mammaplasty scars. Aesthet. Surg. J. 2007, 27, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Celebiler, O.; Sönmez, A.; Erdim, M.; Yaman, M.; Numanoğlu, A. Patients’ and surgeons’ perspectives on the scar components after inferior pedicle breast reduction surgery. Plast. Reconstr. Surg. 2005, 116, 459–464; discussion 465–466. [Google Scholar] [CrossRef]
- Refahee, S.M.; Aboulhassan, M.A.; Abdel Aziz, O.; Emara, D.; Seif El Dein, H.M.; Moussa, B.G.; Abu Sneineh, M. Is PRP Effective in Reducing the Scar Width of Primary Cleft Lip Repair? A Randomized Controlled Clinical Study. Cleft Palate Craniofac. J. 2020, 57, 581–588. [Google Scholar] [CrossRef]
- Verhaegen, P.; van der Wal, M.B.A.; Middelkoop, E.; van Zuijlen, P.P.M. Objective scar assessment tools: A clinimetric appraisal. Plast. Reconstr. Surg. 2011, 127, 1561–1570. [Google Scholar] [CrossRef] [PubMed]
- Takiwaki, H. Measurement of skin color: Practical application and theoretical considerations. J. Med. Investig. 1998, 44, 121–126. [Google Scholar]
- van der Wal, M.; Bloemen, M.; Verhaegen, P.; Tuinebreijer, W.; de Vet, H.; van Zuijlen, P.; Middelkoop, E. Objective color measurements: Clinimetric performance of three devices on normal skin and scar tissue. J. Burn Care Res. 2013, 34, e187–e194. [Google Scholar] [CrossRef]
- Sitek, A.; Rosset, I.; Żądzińska, E.; Kasielska-Trojan, A.; Neskoromna-Jędrzejczak, A.; Antoszewski, B. Skin color parameters and Fitzpatrick phototypes in estimating the risk of skin cancer: A case-control study in the Polish population. J. Am. Acad. Dermatol. 2016, 74, 716–723. [Google Scholar] [CrossRef]
- Fijałkowska, M.; Koziej, M.; Antoszewski, B.; Sitek, A. Correlations between antimicrobial peptides and spectrophotometric skin color parameters in patients with basal cell carcinoma. J. Cancer Res. Clin. Oncol. 2022, 149, 5697–5704. [Google Scholar] [CrossRef]
- Fijałkowska, M.; Koziej, M.; Żądzińska, E.; Antoszewski, B.; Sitek, A. Assessment of the Predictive Value of Spectrophotometric Skin Color Parameters and Environmental and Behavioral Factors in Estimating the Risk of Skin Cancer: A Case-Control Study. J. Clin. Med. 2022, 11, 2969. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Type of Injection | SD | Me | Q1–Q3 | W | p | |
|---|---|---|---|---|---|---|---|
| Age (years) | - | 37.8 | 7.5 | 38.0 | 33.0–43.0 | 0.976 | 0.534 |
| Height (m) | - | 1.66 | 0.06 | 1.65 | 1.63–1.70 | 0.970 | 0.331 |
| Body mass (kg) | - | 67.4 | 6.8 | 68.0 | 63.0–71.0 | 0.973 | 0.435 |
| BMI | - | 24.5 | 2.1 | 25.0 | 23.5–25.9 | 0.881 | 0.001 |
| Scar length (cm) | PRP/placebo | 6.7 | 0.3 | 6.5 | 6.5–7.0 | 0.732 | <0.001 |
| Density of injected agent (mL/cm) | PRP/placebo | 0.20 | 0.03 | 0.21 | 0.19–0.22 | 0.949 | 0.063 |
| Weight of resection (g) | PRP | 670.2 | 247.9 | 675.0 | 498.0–810.0 | 0.969 | 0.322 |
| placebo | 661.5 | 255.0 | 632.0 | 457.0–855.0 | 0.963 | 0.195 | |
| R after 3 m | PRP | 104 | 8 | 102 | 99–110 | 0.987 | 0.914 |
| placebo | 105 | 10 | 106 | 96–112 | 0.965 | 0.238 | |
| G after 3 m | PRP | 72 | 9 | 71 | 67–75 | 0.975 | 0.483 |
| placebo | 73 | 10 | 74 | 65–80 | 0.973 | 0.430 | |
| B after 3 m | PRP | 78 | 9.61 | 78 | 72–84 | 0.978 | 0.597 |
| placebo | 78 | 12 | 79 | 73–85 | 0.951 | 0.076 | |
| L after 3 m | PRP | 30.52 | 3.51 | 30.29 | 28.71–32.04 | 0.983 | 0.803 |
| placebo | 30.68 | 4.25 | 30.92 | 28.19–33.56 | 0.970 | 0.335 | |
| a after 3 m | PRP | 20.48 | 2.49 | 20.49 | 18.72–22.04 | 0.964 | 0.221 |
| placebo | 20.74 | 3.02 | 20.40 | 18.43–22.76 | 0.984 | 0.819 | |
| b after 3 m | PRP | 4.21 | 2.20 | 3.90 | 2.72–5.94 | 0.967 | 0.279 |
| placebo | 4.92 | 2.76 | 4.08 | 3.08–6.58 | 0.949 | 0.062 | |
| MI after 3 m | PRP | 39.16 | 3.64 | 38.98 | 36.72–41.09 | 0.986 | 0.888 |
| placebo | 38.79 | 4.20 | 38.92 | 35.73–42,42 | 0.970 | 0.353 | |
| EI after 3 m | PRP | 16.18 | 2.79 | 16.09 | 14.80–17.24 | 0.929 | 0.014 |
| placebo | 16.37 | 3.15 | 15.17 | 14.44–19.10 | 0.941 | 0.035 | |
| R after 6 m | PRP | 115 | 16 | 116 | 106–123 | 0.960 | 0.160 |
| placebo | 116 | 15 | 115 | 106–122 | 0.940 | 0.031 | |
| G after 6 m | PRP | 82 | 17 | 80 | 71–91 | 0.963 | 0.206 |
| placebo | 84 | 17 | 82 | 73–95 | 0.944 | 0.043 | |
| B after 6 m | PRP | 89 | 16 | 87 | 79–97 | 0.977 | 0.559 |
| placebo | 91 | 17 | 87 | 79–99 | 0.948 | 0.058 | |
| L after 6 m | PRP | 34.99 | 6.36 | 34.75 | 30.58–38.55 | 0.971 | 0.359 |
| placebo | 35.49 | 6.43 | 34.67 | 30.72–39.39 | 0.942 | 0.038 | |
| a after 6 m | PRP | 20.72 | 3.52 | 21.06 | 17.57–22.93 | 0.971 | 0.357 |
| placebo | 19.91 | 3.26 | 19.61 | 17.69–22.16 | 0.985 | 0.852 | |
| b after 6 m | PRP | 4.89 | 2.95 | 4.06 | 2.21–6.97 | 0.940 | 0.032 |
| placebo | 5.36 | 3.43 | 5.05 | 2.89–7.99 | 0.958 | 0.133 | |
| MI after 6 m | PRP | 34.45 | 5.12 | 34.43 | 31.86–37.67 | 0.976 | 0.538 |
| placebo | 34.57 | 5.21 | 35.21 | 32.01–38.26 | 0.962 | 0.178 | |
| EI after 6 m | PRP | 15.22 | 3.95 | 14.94 | 12.31–17.69 | 0.961 | 0.175 |
| placebo | 14.53 | 3.48 | 14.66 | 11.76–16.59 | 0.984 | 0.814 | |
| Scar assessment | PRP | 4.0 | 0.7 | 4.0 | 4.0–4.5 | 0.844 | <0.001 |
| placebo | 4.0 | 0.7 | 4.0 | 4.0–4.5 | 0.886 | 0.001 |
| Score | PRP (n = 41) | Placebo (n = 41) | Z/p |
|---|---|---|---|
| 2 | 1 | 1 | −0.01/ 0.996 |
| 3 | 6 | 6 | |
| 3.5 | 1 | 3 | |
| 4 | 22 | 18 | |
| 4.5 | 2 | 4 | |
| 5 | 9 | 9 |
| Dependent Variables | Type of Injection (PRP vs. Placebo) | Time of Examination (3 m vs. 6 m) | Type of Injection × Time of Examination |
|---|---|---|---|
| R (B-C) | F = 0.32; p = 0.571 | F = 44.16; p < 0.001 | F = 0.01; p = 0.909 |
| G (B-C) | F = 0.36; p = 0.553 | F = 40.14; p < 0,001 | F = 0.20; p = 0.656 |
| B | F = 0.06; p = 0.808 | F = 46.80; p < 0.001 | F = 0.08; p = 0.777 |
| L (B-C) | F = 0.07; p = 0.790 | F = 49.18; p < 0.001 | F = 0.14; p = 0.714 |
| a | F = 0.22; p = 0.638 | F = 0.69; p = 0.409 | F = 2.20; p = 0.142 |
| b (B-C) | F = 0.78; p = 0.381 | F = 1.25; p = 0.266 | F = 0.32; p = 0.572 |
| MI | F = 0.02; p = 0.877 | F = 53.33; p < 0.001 | F = 0.16; p = 0.687 |
| EI (B-C) | F = 0.18; p = 0.674 | F = 13.65; p = 0.004 | F = 1.03; p = 0.314 |
| Variables | F | p |
|---|---|---|
| PRP/Placebo | 0.56 | 0.458 |
| Age | 0.20 | 0.660 |
| PRP/Placebo × Age | 0.58 | 0.449 |
| PRP/Placebo | 2.03 | 0.158 |
| BMI | 2.27 | 0.136 |
| PRP/Placebo × BMI | 2.04 | 0.157 |
| PRP/Placebo | 0.84 | 0.362 |
| Vertical scar length | 8.81 | 0.004 |
| PRP/Placebo × vertical scar length | 0.84 | 0.362 |
| PRP/Placebo | 1.32 | 0.253 |
| Density of injected PRP/Placebo | 3.12 | 0.081 |
| PRP/Placebo × Density of injected PRP/Placebo | 1.35 | 0.249 |
| PRP/Placebo | 0.50 | 0.482 |
| Weight of resected tissues | 7.54 | 0.008 |
| PRP/Placebo × Weight of resected tissue | 0.60 | 0.442 |
| PRP/Placebo | 0.10 | 0.753 |
| R after 3 m | 4.67 | 0.034 |
| PRP/Placebo × R after 3 m | 0.09 | 0.765 |
| PRP/Placebo | 0.71 | 0.402 |
| G after 3 m | 4.32 | 0.041 |
| PRP/Placebo × G after 3 m | 0.69 | 0.407 |
| PRP/Placebo | 0.07 | 0.786 |
| B after 3 m | 3.12 | 0.081 |
| PRP/Placebo × B after 3 m | 0.07 | 0.785 |
| PRP/Placebo | 0.50 | 0.481 |
| L after 3 m | 4.05 | 0.048 |
| PRP/Placebo × L after 3 m | 0.50 | 0.481 |
| PRP/Placebo | 1.70 | 0.196 |
| a after 3 m | 0.44 | 0.510 |
| PRP/Placebo × a after 3 m | 1.72 | 0.194 |
| PRP/Placebo | 0.00 | 0.968 |
| b after 3 m | 5.81 | 0.018 |
| PRP/Placebo × b po 3 m | 0.05 | 0.816 |
| PRP/Placebo | 0.63 | 0.431 |
| MI after 3 m | 3.06 | 0.084 |
| PRP/Placebo × MI after 3 m | 0.65 | 0.424 |
| PRP/Placebo | 2.28 | 0.135 |
| EI after 3 m | 1.46 | 0.230 |
| PRP/Placebo × EI after 3 m | 2.33 | 0.131 |
| Independent Variable | R2 = 0.2848, Corrected R2 = 0.1088; F (16.65) = 1.62 p < 0.089; Estimation Error: 0.67 | |||
|---|---|---|---|---|
| b | SEb | t | p | |
| PRP/Placebo | 0.0436 | 0.1096 | 0.40 | 0.692 |
| Age | −0.0094 | 0.1185 | −0.08 | 0.937 |
| Weight of resected tissues | 0.0143 | 0.1756 | 0.08 | 0.935 |
| Scar length | −0.1860 | 0.1757 | −1.06 | 0.294 |
| Density of injected PRP/Placebo | 0.1717 | 0.1236 | 1.39 | 0.17 |
| Body height | 4.9669 | 1.8749 | 2.65 | 0.01 |
| Body weight | −6.9170 | 2.6440 | −2.62 | 0.011 |
| BMI | 5.9491 | 2.2878 | 2.60 | 0.012 |
| R after 3 m (B-C) | 0.1838 | 0.8551 | 0.21 | 0.83 |
| G after 3 m (B-C) | 0.5648 | 0.8150 | 0.69 | 0.491 |
| B after 3 m | 0.0133 | 0.4978 | 0.03 | 0.979 |
| L after 3 m (B-C) | 0.0200 | 0.5463 | 0.04 | 0.971 |
| a after 3 m | −0.4391 | 0.6729 | −0.65 | 0.516 |
| b after 3 m (B-C) | 0.2065 | 0.2559 | 0.81 | 0.423 |
| MI after 3 m | 0.2858 | 0.3263 | 0.88 | 0.384 |
| EI after 3 m (B-C) | 0.6677 | 0.7220 | 0.92 | 0.358 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zawadzki, T.; Sitek, A.; Antoszewski, B.; Kasielska-Trojan, A. Do Intraoperative Platelet-Rich Plasma Injections Influence the Final Appearance of Vertical Scars after Breast Reduction? Spectrophotometric Analysis. J. Clin. Med. 2024, 13, 691. https://doi.org/10.3390/jcm13030691
Zawadzki T, Sitek A, Antoszewski B, Kasielska-Trojan A. Do Intraoperative Platelet-Rich Plasma Injections Influence the Final Appearance of Vertical Scars after Breast Reduction? Spectrophotometric Analysis. Journal of Clinical Medicine. 2024; 13(3):691. https://doi.org/10.3390/jcm13030691
Chicago/Turabian StyleZawadzki, Tomasz, Aneta Sitek, Bogusław Antoszewski, and Anna Kasielska-Trojan. 2024. "Do Intraoperative Platelet-Rich Plasma Injections Influence the Final Appearance of Vertical Scars after Breast Reduction? Spectrophotometric Analysis" Journal of Clinical Medicine 13, no. 3: 691. https://doi.org/10.3390/jcm13030691