
Oral Iron Absorption of Ferric Citrate Hydrate and Hepcidin-25 in Hemodialysis Patients: A Prospective, Multicenter, Observational Riona-Oral Iron Absorption Trial
 , ,
, ,
Abstract
:1. Introduction
2. Results
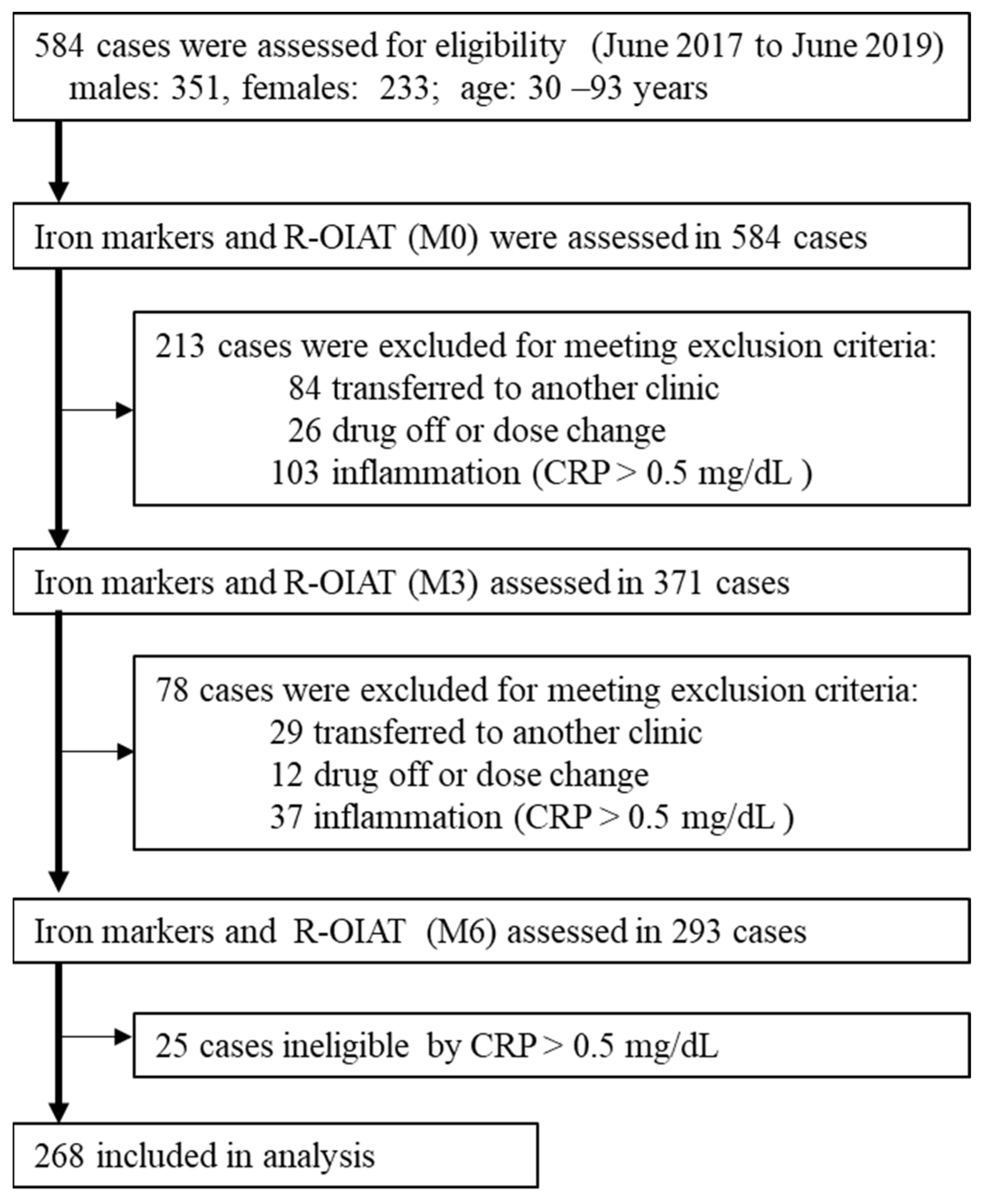
2.1. Baseline Characteristics of the Study Participants
2.2. Association of Changes in Clinical Indices at Different 3-Month Intervals
2.3. Association of ΔFe2h with Iron Variables
2.4. Association of Hepcidin-25 with Iron Variables
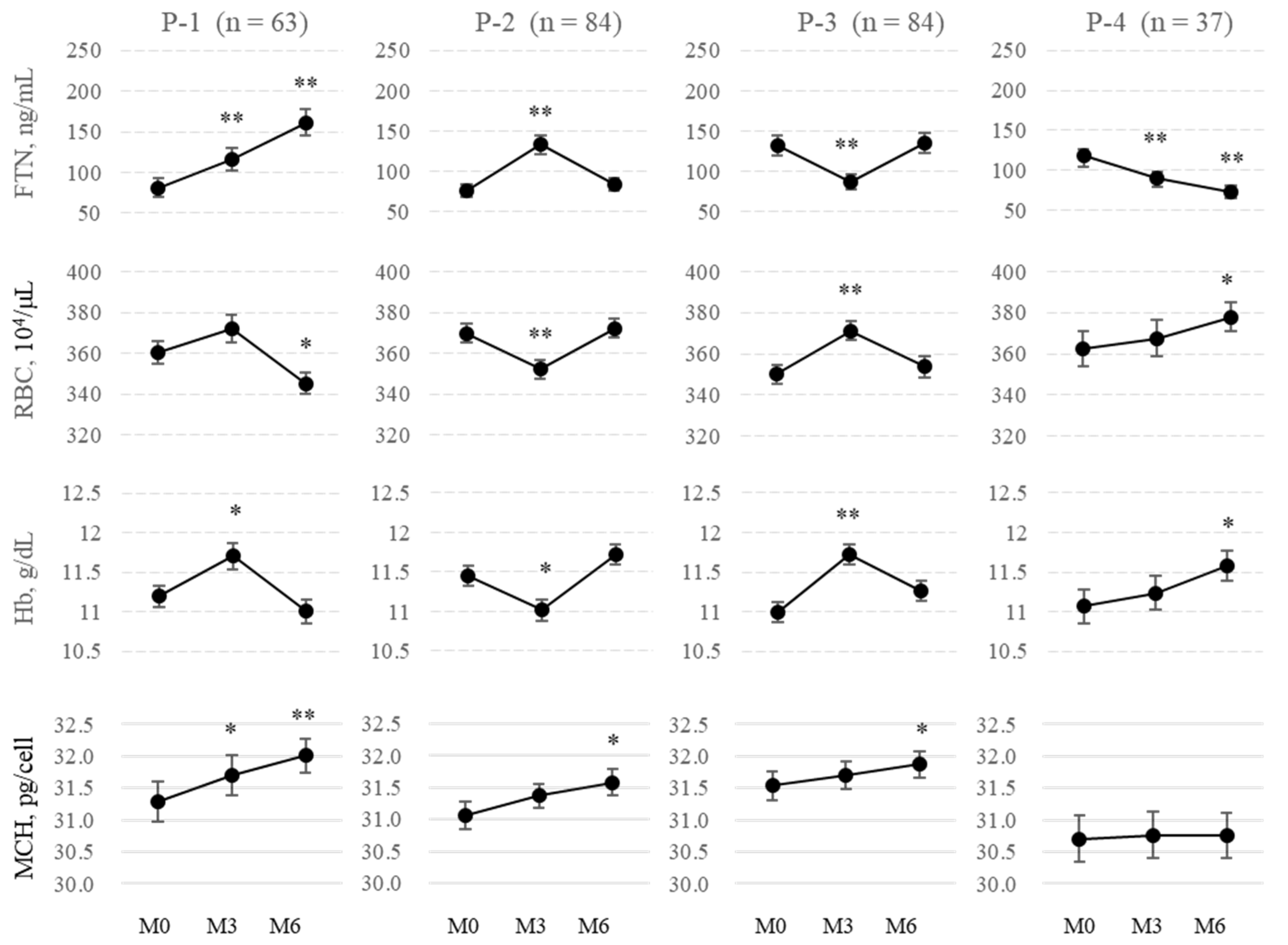
2.5. Patterns of FTN Fluctuations
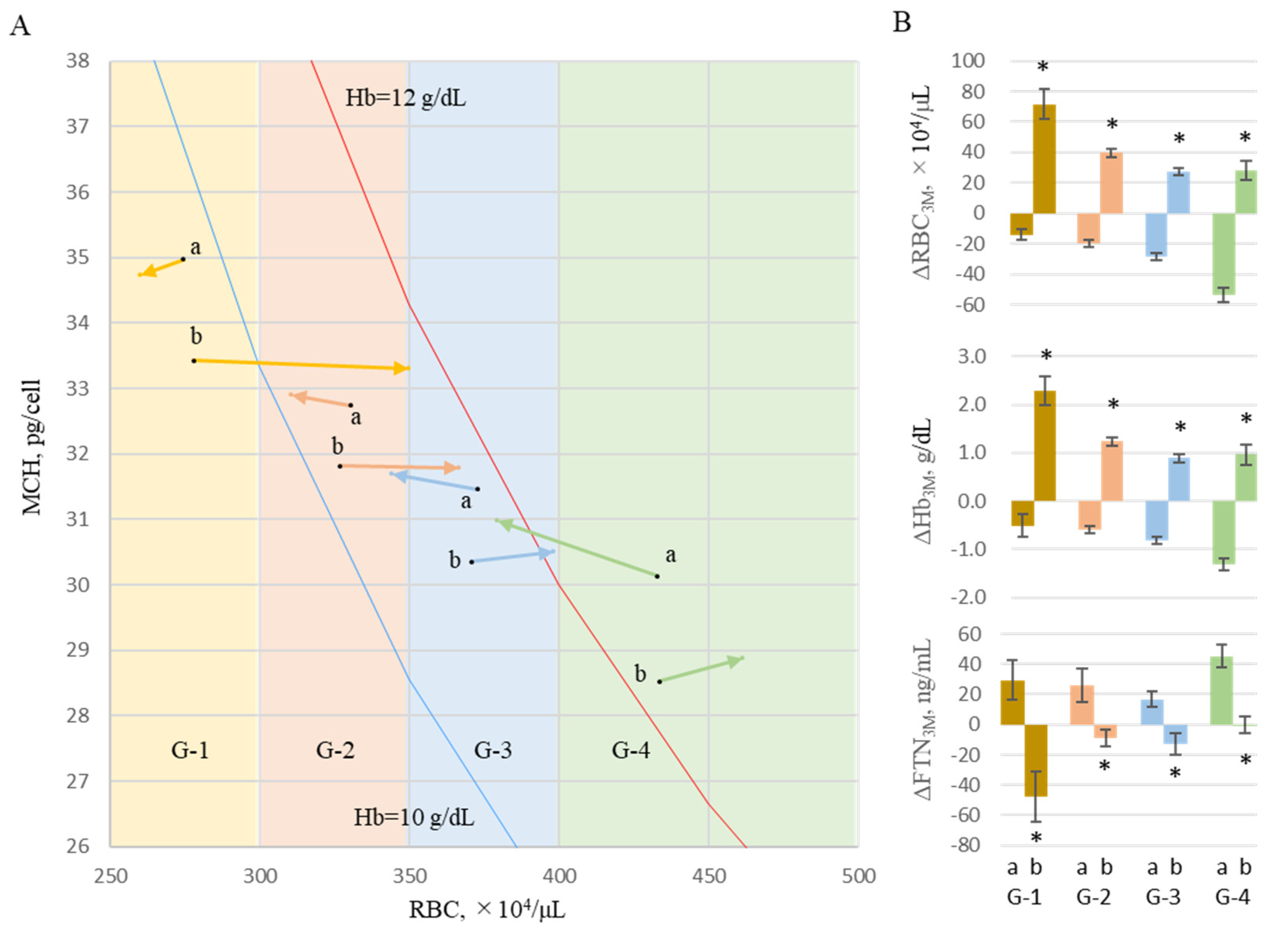
2.6. Background of Changes in FTN
3. Discussion
4. Materials and Methods
4.1. Study Design and Data Sources
4.2. Procedures
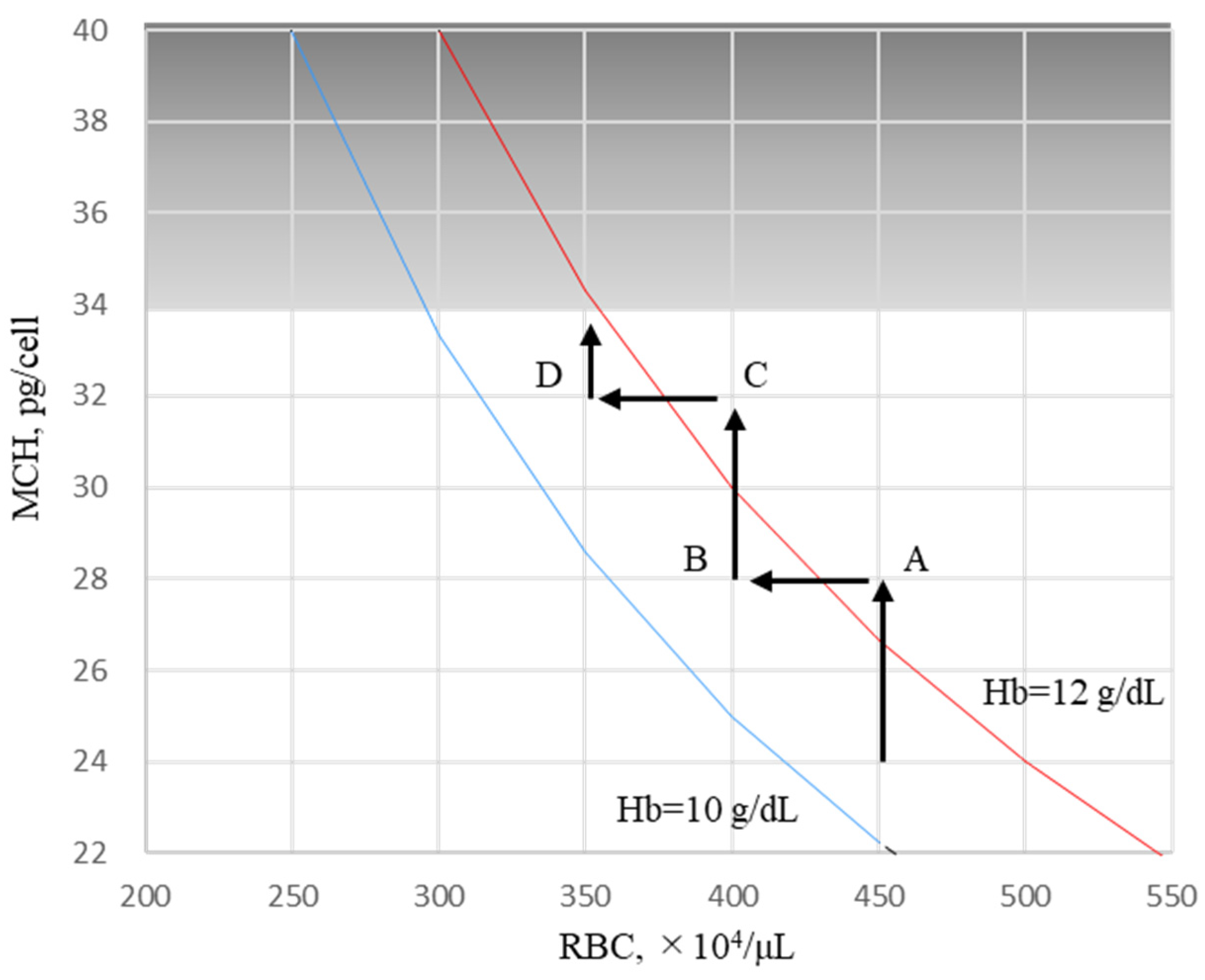
4.3. Estimating Iron Absorption
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fishbane, S.; Spinowitz, B. Update on anemia in ESRD and earlier stages of CKD: Core curriculum 2018. Am. J. Kidney Dis. 2018, 71, 423–435. [Google Scholar] [CrossRef]
- Besarab, A.; Coyne, D.W. Iron supplementation to treat anemia in patients with chronic kidney disease. Nat. Rev. Nephrol. 2010, 6, 699–710. [Google Scholar] [CrossRef]
- Pergola, P.E.; Fishbane, S.; Ganz, T. Novel oral iron therapies for iron deficiency anemia in chronic kidney disease. Adv. Chronic Kidney Dis. 2019, 26, 272–291. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, K.; Akiba, T.; Fukagawa, M.; Nakayama, M.; Sawada, K.; Kumagai, Y.; Chertow, G.M.; Hirakata, H. Long-term safety and efficacy of a novel iron-containing phosphate binder, JTT-751, in patients receiving hemodialysis. J. Ren. Nutr. 2014, 24, 261–267. [Google Scholar] [CrossRef]
- Lewis, J.B.; Sika, M.; Koury, M.J.; Chuang, P.; Schulman, G.; Smith, M.T.; Whittier, F.C.; Linfert, D.R.; Galphin, C.M.; Athreya, B.P.; et al. Ferric citrate controls phosphorus and delivers iron in patients on dialysis. J. Am. Soc. Nephrol. 2015, 26, 493–503. [Google Scholar] [CrossRef]
- Umanath, K.; Jalal, D.I.; Greco, B.A.; Umeukeje, E.M.; Reisin, E.; Manley, J.; Zeig, S.; Negoi, D.G.; Hiremath, A.N.; Blumenthal, S.S.; et al. Ferric citrate reduces intravenous iron and erythropoiesis-stimulating agent use in ESRD. J. Am. Soc. Nephrol. 2015, 26, 2578–2587. [Google Scholar] [CrossRef] [PubMed]
- Kühn, L.C. Iron regulatory proteins and their role in controlling iron metabolism. Metallomics 2015, 7, 232–243. [Google Scholar] [CrossRef]
- Ramanathan, G.; Olynyk, J.K.; Ferrari, P. Diagnosing and preventing iron overload. Hemodial. Int. 2017, 21 (Suppl. S1), S58–S67. [Google Scholar] [CrossRef] [PubMed]
- Roe, M.A.; Collings, R.; Dainty, J.R.; Swinkels, D.W.; Fairweather-Tait, S.J. Plasma hepcidin concentrations significantly predict interindividual variation in iron absorption in healthy men. Am. J. Clin. Nutr. 2009, 89, 1088–1091. [Google Scholar] [CrossRef]
- Honda, H.; Kobayashi, Y.; Onuma, S.; Shibagaki, K.; Yuza, T.; Hirao, K.; Yamamoto, T.; Tomosugi, N.; Shibata, T. Associations among erythroferrone and biomarkers of erythropoiesis and iron metabolism, and treatment with long-term erythropoiesis-stimulating agents in patients on hemodialysis. PLoS ONE 2016, 11, e0151601. [Google Scholar] [CrossRef]
- Pak, M.; Lopez, M.A.; Gabayan, V.; Ganz, T.; Rivera, S. Suppression of hepcidin during anemia requires erythropoietic activity. Blood 2006, 108, 3730–3735. [Google Scholar] [CrossRef] [PubMed]
- Gulec, S.; Anderson, G.J.; Collins, J.F. Mechanistic and regulatory aspects of intestinal iron absorption. Am. J. Physiol. Gastrointest. Liver Physiol. 2014, 307, G397–G409. [Google Scholar] [CrossRef]
- Kautz, L.; Jung, G.; Valore, E.V.; Rivella, S.; Nemeth, E.; Ganz, T. Identification of erythroferrone as an erythroid regulator of iron metabolism. Nat. Genet. 2014, 46, 678–684. [Google Scholar] [CrossRef]
- Li, H.; Ginzburg, Y.Z. Crosstalk between iron metabolism and erythropoiesis. Adv. Hematol. 2010, 2010, 605435. [Google Scholar] [CrossRef]
- Verga Falzacappa, M.V.; Vujic Spasic, M.; Kessler, R.; Stolte, J.; Hentze, M.W.; Muckenthaler, M.U. STAT3 mediates hepatic hepcidin expression and its inflammatory stimulation. Blood 2007, 109, 353–358. [Google Scholar] [CrossRef]
- Chaston, T.; Chung, B.; Mascarenhas, M.; Marks, J.; Patel, B.; Srai, S.K.; Sharp, P. Evidence for differential effects of hepcidin in macrophages and intestinal epithelial cells. Gut 2008, 57, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Brasse-Lagnel, C.; Karim, Z.; Letteron, P.; Bekri, S.; Bado, A.; Beaumont, C. Intestinal DMT1 cotransporter is down-regulated by hepcidin via proteasome internalization and degradation. Gastroenterology 2011, 140, 1261–1271. [Google Scholar] [CrossRef]
- Hanudel, M.R.; Czaya, B.; Wong, S.; Rappaport, M.; Namjoshi, S.; Chua, K.; Jung, G.; Gabayan, V.; Qiao, B.; Nemeth, E.; et al. Enteral ferric citrate absorption is dependent on the iron transport protein ferroportin. Kidney Int. 2022, 101, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, E.; Ganz, T. Hepcidin-Ferroportin Interaction Controls Systemic Iron Homeostasis. Int. J. Mol. Sci. 2021, 22, 6493. [Google Scholar] [CrossRef]
- Wintrobe, M.M. Chapter 2: The erythrocyte. In Clinical Hematology, 6th ed.; Wintrobe, M.M., Ed.; Lea & Febiger: Philadelphia, PA, USA, 1967; pp. 63–103. [Google Scholar]
- Vajpayee, N.; Graham, S.S.; Bem, S. Chapter 30: Basic examination of blood and bone marrow. In Henry’s Clinical Diagnosis and Management by Laboratory Methods, 22nd ed.; McPherson, R.A., Pincus, M.R., Eds.; WB Saunders: Philadelphia, PA, USA, 2011; pp. 509–535. [Google Scholar]
- Kawabata, H. Transferrin and transferrin receptors update. Free Radic. Biol. Med. 2019, 133, 46–54. [Google Scholar] [CrossRef]
- Eschbach, J.W.; Cook, J.D.; Scribner, B.H.; Finch, C.A. Iron balance in hemodialysis patients. Ann. Intern. Med. 1977, 87, 710–713. [Google Scholar] [CrossRef]
- Camaschella, C.; Nai, A.; Silvestri, L. Iron metabolism and iron disorders revisited in the hepcidin era. Haematologica 2020, 105, 260–272. [Google Scholar] [CrossRef]
- Egrie, J.C.; Strickland, T.W.; Lane, J.; Aoki, K.; Cohen, A.M.; Smalling, R.; Trail, G.; Lin, F.K.; Browne, J.K.; Hines, D.K. Characterization and biological effects of recombinant human erythropoietin. Immunobiology 1986, 172, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Kawabata, H.; Fleming, R.E.; Gui, D.; Moon, S.Y.; Saitoh, T.; O’Kelly, J.; Umehara, Y.; Wano, Y.; Said, J.W.; Koeffler, H.P. Expression of hepcidin is down-regulated in TfR2 mutant mice manifesting a phenotype of hereditary hemochromatosis. Blood 2005, 105, 376–381. [Google Scholar] [CrossRef]
- Daru, J.; Colman, K.; Stanworth, S.J.; De La Salle, B.; Wood, E.M.; Pasricha, S.R. Serum ferritin as an indicator of iron status: What do we need to know? Am. J. Clin. Nutr. 2017, 106, 1634S–1639S. [Google Scholar] [CrossRef] [PubMed]
- Babitt, J.L.; Eisenga, M.F.; Haase, V.H.; Kshirsagar, A.V.; Levin, A.; Locatelli, F.; Małyszko, J.; Swinkels, D.W.; Tarng, D.C.; Cheung, M.; et al. Controversies in optimal anemia management: Conclusions from a kidney disease: Improving Global Outcomes (KDIGO) Conference. Kidney Int. 2021, 99, 1280–1295. [Google Scholar] [CrossRef] [PubMed]
- Tsubakihara, Y.; Nishi, S.; Akiba, T.; Hirakata, H.; Iseki, K.; Kubota, M.; Kuriyama, S.; Komatsu, Y.; Suzuki, M.; Nakai, S.; et al. 2008 Japanese Society for Dialysis Therapy: Guidelines for renal anemia in chronic kidney disease. Ther. Apher. Dial. 2010, 14, 240–275. [Google Scholar] [CrossRef]
- Soe-Lin, S.; Apte, S.S.; Andriopoulos, B., Jr.; Andrews, M.C.; Schranzhofer, M.; Kahawita, T.; Garcia-Santos, D.; Ponka, P. Nramp1 promotes efficient macrophage recycling of iron following erythrophagocytosis in vivo. Proc. Natl. Acad. Sci. USA 2009, 106, 5960–5965. [Google Scholar] [CrossRef]
- Zhang, D.L.; Ghosh, M.C.; Ollivierre, H.; Li, Y.; Rouault, T.A. Ferroportin deficiency in erythroid cells causes serum iron deficiency and promotes hemolysis due to oxidative stress. Blood 2018, 132, 2078–2087. [Google Scholar] [CrossRef]
- Coffey, R.; Ganz, T. Iron homeostasis: An anthropocentric perspective. J. Biol. Chem. 2017, 292, 12727–12734. [Google Scholar] [CrossRef]
- Santini, V.; Girelli, D.; Sanna, A.; Martinelli, N.; Duca, L.; Campostrini, N.; Cortelezzi, A.; Corbella, M.; Bosi, A.; Reda, G.; et al. Hepcidin levels and their determinants in different types of myelodysplastic syndromes. PLoS ONE 2011, 6, e23109. [Google Scholar] [CrossRef] [PubMed]
- Tantiworawit, A.; Khemakapasiddhi, S.; Rattanathammethee, T.; Hantrakool, S.; Chai-Adisaksopha, C.; Rattarittamrong, E.; Norasetthada, L.; Charoenkwan, P.; Srichairatanakool, S.; Fanhchaksai, K. Correlation of hepcidin and serum ferritin levels in thalassemia patients at Chiang Mai University Hospital. Biosci. Rep. 2021, 41, BSR20203352. [Google Scholar] [CrossRef]
- Daimon, S. Efficacy for anaemia and changes in serum ferritin levels by long-term oral iron administration in haemodialysis patients. Ther. Apher. Dial. 2019, 23, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Rausa, M.; Pagani, A.; Nai, A.; Campanella, A.; Gilberti, M.E.; Apostoli, P.; Camaschella, C.; Silvestri, L. Bmp6 expression in murine liver non parenchymal cells: A mechanism to control their high iron exporter activity and protect hepatocytes from iron overload? PLoS ONE 2015, 10, e0122696. [Google Scholar] [CrossRef]
- Kawabata, H.; Usuki, K.; Shindo-Ueda, M.; Kanda, J.; Tohyama, K.; Matsuda, A.; Araseki, K.; Hata, T.; Suzuki, T.; Kayano, H.; et al. Serum ferritin levels at diagnosis predict prognosis in patients with low blast count myelodysplastic syndromes. Int. J. Hematol. 2019, 110, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Murao, N.; Ishigai, M.; Yasuno, H.; Shimonaka, Y.; Aso, Y. Simple and sensitive quantification of bioactive peptides in biological matrices using liquid chromatography/selected reaction monitoring mass spectrometry coupled with trichloroacetic acid clean-up. Rapid Commun. Mass Spectrom. 2007, 21, 4033–4038. [Google Scholar] [CrossRef] [PubMed]
- Aljama, P.; Bommer, J.; Canaud, B.; Carrera, F.; Eckardt, K.U.; Hörl, W.H.; Krediet, R.T.; Locatelli, F.; Macdougall, I.C.; Wikström, B. Practical guidelines for the use of NESP in treating renal anaemia. Nephrol. Dial. Transplant. 2001, 16 (Suppl. S3), 22–28. [Google Scholar] [CrossRef]
- Carrera, F.; Lok, C.E.; de Francisco, A.; Locatelli, F.; Mann, J.F.; Canaud, B.; Kerr, P.G.; Macdougall, I.C.; Besarab, A.; Villa, G.; et al. Maintenance treatment of renal anaemia in haemodialysis patients with methoxy polyethylene glycolepoetin beta versus darbepoetin alfa administered monthly: A randomized comparative trial. Nephrol. Dial. Transplant. 2010, 25, 4009–4017. [Google Scholar] [CrossRef]
- Conway, R.E.; Geissler, C.A.; Hider, R.C.; Thompson, R.P.; Powell, J.J. Serum iron curves can be used to estimate dietary iron bioavailability in humans. J. Nutr. 2006, 136, 1910–1914. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Baseline (n = 268) |
|---|---|
| Age (years) | 63.0 (11.6) |
| Males, age, n (%) | 63.8 (11.3), 153 (57%) |
| Females, age, n (%) | 62.0 (12.0), 115 (43%) |
| Riona | |
| 3 tablets (750 mg of FCH) | 149 (55.6%) |
| 6 tablets (1500 mg of FCH) | 101 (37.7%) |
| 9 tablets (2250 mg of FCH) | 18 (6.7%) |
| ESA | |
| epoetin alfa/beta, n (%) | 40 (14.9%) |
| darbepoetin alfa, n (%) | 133 (49.6%) |
| epoetin beta pegol, n (%) | 65 (24.3%) |
| No ESA, n (%) | 30 (11.2%) |
| Baseline | 3 Months | 6 Months | |||||
|---|---|---|---|---|---|---|---|
| M0 (n = 268) | M3 (n = 268) | M6 (n = 268) | |||||
| Mean | (SD) | Mean | (SD) | Mean | (SD) | p | |
| ESA, IU/week | 3679.3 | (3406.8) | 3256.1 | (3205.9) | 3147.7 | (3026.6) | 0.000 |
| RBCs, 104/μL | 360.3 | (44.5) | 364.9 | (48.4) | 360.9 | (45.5) | 0.301 |
| Hb, g/dL | 11.2 | (1.2) | 11.4 | (1.3) | 11.4 | (1.2) | 0.019 |
| Ht, % | 34.6 | (3.8) | 35.1 | (4.0) | 34.9 | (3.6) | 0.162 |
| MCV | 95.8 | (8.8) | 96.6 | (5.5) | 96.6 | (7.5) | 0.301 |
| MCH, pg/cell | 31.2 | (2.2) | 31.5 | (2.1) | 31.7 | (2.0) | 0.000 |
| Plat, 104/μL | 19.2 | (5.9) | 20.1 | (14.8) | 18.8 | (6.1) | 0.018 |
| S-Fe, μg/dL | 65.7 | (26.2) | 70.3 | (28.4) | 69.8 | (27.8) | 0.013 |
| FTN, ng/mL | 100.7 | (93.2) | 108.9 | (99.6) | 116.7 | (102.7) | 0.000 |
| TSAT, % | 27.4 | (11.6) | 28.9 | (12.0) | 29.5 | (12.5) | 0.009 |
| Hepcidin-25, ng/mL | 42.9 | (38.7) | 50.5 | (41.6) | 45.6 | (35.6) | 0.000 |
| ΔFe2h, μg/dL | 26.6 | (37.2) | 24.7 | (35.8) | 22.9 | (32.3) | 0.062 |
| P, mg/dL | 5.5 | (1.3) | 5.5 | (1.3) | 5.5 | (1.3) | 0.982 |
| Albumin, g/dL | 3.9 | (3.4) | 4.1 | (4.1) | 3.9 | (3.5) | 0.127 |
| AST, IU/L | 13.5 | (6.7) | 13.8 | (6.3) | 13.9 | (7.8) | 0.663 |
| ALT, IU/L | 11.4 | (5.4) | 11.9 | (7.6) | 12.2 | (9.4) | 0.898 |
| Al-P, IU/mL | 239.5 | (110.5) | 241.7 | (110.2) | 238 | (111.6) | 0.134 |
| γ-GTP, IU/L | 21.3 | (21.0) | 20.7 | (17.0) | 22.2 | (25.0) | 0.455 |
| Time Course | F | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Iron Variable | FCH (mg) | M0 | M3 | M6 | FCH | Time | Interaction | |||
| Amounts | Course | Effects | ||||||||
| ΔFe2h, μg/dL | 750 | 23.0 | (37.5) | 18.5 | (36.6) | 17.2 | (28.0) | 7.58 * | 2.42 | 0.35 |
| 1500 | 29.9 | (37.1) | 29.6 | (35.3) | 29.1 | (36.2) | ||||
| 2250 | 25.6 | (44.9) | 27.8 | (50.2) | 21.2 | (46.5) | ||||
| FTN, ng/mL | 750 | 72.8 | (72.0) | 81.3 | (70.4) | 84.5 | (78.0) | 22.02 ** | 7.92 * | 0.168 |
| 1500 | 136.7 | (103.8) | 147.9 | (120.8) | 160.3 | (114.4) | ||||
| 2250 | 129.4 | (112.3) | 118.6 | (105.2) | 139.2 | (121.8) | ||||
| Hepcidin-25, ng/mL | 750 | 33.9 | (32.2) | 41.1 | (32.8) | 36.6 | (24.5) | 8.23 ** | 5.66 * | 0.78 |
| 1500 | 53.8 | (43.1) | 63.0 | (49.6) | 54.7 | (41.9) | ||||
| 2250 | 56.4 | (44.7) | 58.9 | (39.5) | 68.8 | (51.2) | ||||
| TSAT, % | 750 | 26.5 | (11.5) | 29.1 | (12.5) | 28.7 | (11.2) | 0.52 | 5.13 * | 0.60 |
| 1500 | 28.4 | (11.7) | 28.4 | (11.2) | 29.9 | (13.6) | ||||
| 2250 | 28.3 | (12.1) | 30.1 | (12.2) | 32.8 | (15.4) | ||||
| RBCs, 104/μL | 750 | 360.3 | (42.5) | 361.2 | (47.6) | 358.2 | (44.9) | 5.29 * | 0.38 | 0.71 |
| 1500 | 365.3 | (44.9) | 372.5 | (48.7) | 368.7 | (42.5) | ||||
| 2250 | 332.3 | (50.3) | 353.8 | (50.9) | 339.8 | (58.8) | ||||
| Hb, g/dL | 750 | 11.2 | (1.1) | 11.3 | (1.2) | 11.3 | (1.2) | 4.63 * | 5.87 * | 0.73 |
| 1500 | 11.4 | (1.2) | 11.6 | (1.4) | 11.6 | (1.1) | ||||
| 2250 | 10.6 | (1.5) | 11.3 | (1.4) | 11.1 | (1.5) | ||||
| MCH, pg/cell | 750 | 31.1 | (2.3) | 31.5 | (2.2) | 31.6 | (2.2) | 1.31 | 9.85 * | 0.91 |
| 1500 | 31.2 | (2.0) | 31.4 | (1.8) | 31.6 | (1.8) | ||||
| 2250 | 32.1 | (2.0) | 32.2 | (2.5) | 32.3 | (2.0) | ||||
| ESA, IU/week | 750 | 3701 | (3318) | 3231 | (3367) | 3015 | (3031) | 1.36 | 0.77 | 3.20 |
| 1500 | 3606 | (3477) | 3092 | (2738) | 3096 | (2773) | ||||
| 2250 | 3902 | (3901) | 4375 | (4134) | 4527 | (4052) | ||||
| Parameter Estimates | |||||
|---|---|---|---|---|---|
| Variables | Log ΔFe2h, μg/dL | 95% CI | p Value | ||
| B | SE | Lower | Upper | ||
| hepcidn-25, ng/mL | −0.459 | 0.094 | −0.643 | −0.276 | 0.000 |
| RBCs, 104/μL | 0.989 | 0.719 | −0.421 | 2.398 | 0.169 |
| MCH, pg/cell | −1.220 | 1.582 | −4.321 | 1.882 | 0.441 |
| TSAT, % | −0.648 | 0.230 | −1.099 | −0.197 | 0.005 |
| FTN, ng/mL | 0.099 | 0.133 | −0.161 | 0.359 | 0.457 |
| ESA, IU/week | −0.188 | 0.121 | −0.426 | 0.049 | 0.120 |
| FCH, 750 mg | 0.005 | 0.218 | −0.431 | 0.422 | 0.983 |
| FCH, 1500 mg | 0.376 | 0.213 | −0.041 | 0.794 | 0.077 |
| FCH, 2250 mg | 0 a | ||||
| age | 0.005 | 0.004 | −0.002 | 0.013 | 0.155 |
| sex, female | 0.041 | 0.088 | −0.131 | 0.214 | 0.637 |
| sex, male | 0 a | ||||
| Parameter Estimates | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Log Hepcidin-25, ng/mL | 95% CI | p Value | Log Ferritin, ng/mL | 95% CI | p Value | |||||
| Variables | B | SE | Lower | Upper | B | SE | Lower | Upper | ||
| hepcidin-25, ng/mL | 0.297 | 0.030 | 0.239 | 0.355 | 0.000 | |||||
| FTN, ng/mL | 0.754 | 0.060 | 0.637 | 0.871 | 0.000 | |||||
| RBC, 104/μL | 0.790 | 0.312 | 0.178 | 1.401 | 0.011 | −1.392 | 0.182 | −1.749 | −1.035 | 0.000 |
| MCH, pg/cell | 1.667 | 0.789 | 0.121 | 3.213 | 0.035 | 0.858 | 0.514 | −0.150 | 1.866 | 0.095 |
| TSAT, % | 0.372 | 0.116 | 0.144 | 0.600 | 0.001 | 0.233 | 0.068 | 0.099 | 0.367 | 0.001 |
| ESA, IU/week | −0.353 | 0.055 | −0.462 | −0.245 | 0.000 | −0.084 | 0.045 | −0.172 | 0.005 | 0.064 |
| FCH, 750 mg | −0.141 | 0.056 | −0.252 | 0.031 | 0.012 | −0.101 | 0.068 | −0.234 | 0.031 | 0.135 |
| FCH, 1500 mg | −0.144 | 0.061 | −0.263 | −0.026 | 0.017 | 0.131 | 0.072 | −0.009 | 0.270 | 0.067 |
| FCH, 2250 mg | 0 a | 0 a | ||||||||
| age | 0.000 | 0.001 | −0.002 | 0.003 | 0.773 | 0.000 | 0.0015 | −0.003 | 0.003 | 0.798 |
| sex, female | 0.130 | 0.036 | 0.060 | 0.200 | 0 | −0.037 | 0.033 | −0.101 | 0.028 | 0.263 |
| sex, male | 0 a | 0 a | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomosugi, N.; Koshino, Y.; Ogawa, C.; Maeda, K.; Shimada, N.; Tomita, K.; Daimon, S.; Shikano, T.; Ryu, K.; Takatani, T.; et al. Oral Iron Absorption of Ferric Citrate Hydrate and Hepcidin-25 in Hemodialysis Patients: A Prospective, Multicenter, Observational Riona-Oral Iron Absorption Trial. Int. J. Mol. Sci. 2023, 24, 13779. https://doi.org/10.3390/ijms241813779
Tomosugi N, Koshino Y, Ogawa C, Maeda K, Shimada N, Tomita K, Daimon S, Shikano T, Ryu K, Takatani T, et al. Oral Iron Absorption of Ferric Citrate Hydrate and Hepcidin-25 in Hemodialysis Patients: A Prospective, Multicenter, Observational Riona-Oral Iron Absorption Trial. International Journal of Molecular Sciences. 2023; 24(18):13779. https://doi.org/10.3390/ijms241813779
Chicago/Turabian StyleTomosugi, Naohisa, Yoshitaka Koshino, Chie Ogawa, Kunimi Maeda, Noriaki Shimada, Kimio Tomita, Shoichiro Daimon, Tsutomu Shikano, Kazuyuki Ryu, Toru Takatani, and et al. 2023. "Oral Iron Absorption of Ferric Citrate Hydrate and Hepcidin-25 in Hemodialysis Patients: A Prospective, Multicenter, Observational Riona-Oral Iron Absorption Trial" International Journal of Molecular Sciences 24, no. 18: 13779. https://doi.org/10.3390/ijms241813779
APA StyleTomosugi, N., Koshino, Y., Ogawa, C., Maeda, K., Shimada, N., Tomita, K., Daimon, S., Shikano, T., Ryu, K., Takatani, T., Sakamoto, K., Ueyama, S., Nagasaku, D., Nakamura, M., Ra, S., Nishimura, M., Takagi, C., Ishii, Y., Kudo, N., ... Shirai, S. (2023). Oral Iron Absorption of Ferric Citrate Hydrate and Hepcidin-25 in Hemodialysis Patients: A Prospective, Multicenter, Observational Riona-Oral Iron Absorption Trial. International Journal of Molecular Sciences, 24(18), 13779. https://doi.org/10.3390/ijms241813779