
Effects of Probiotics in Adults with Gastroenteritis: A Systematic Review and Meta-Analysis of Clinical Trials



Abstract
:1. Introduction
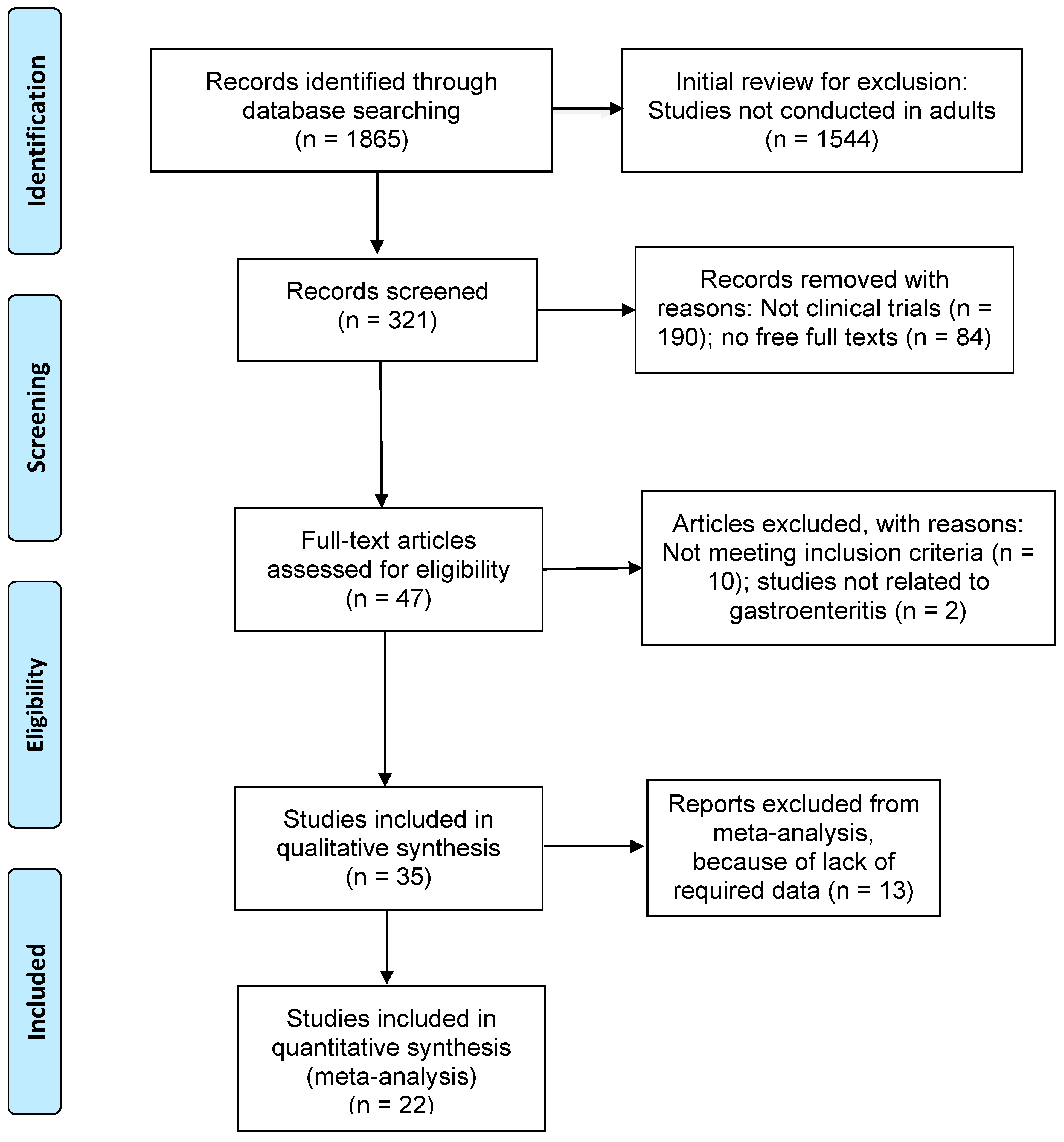
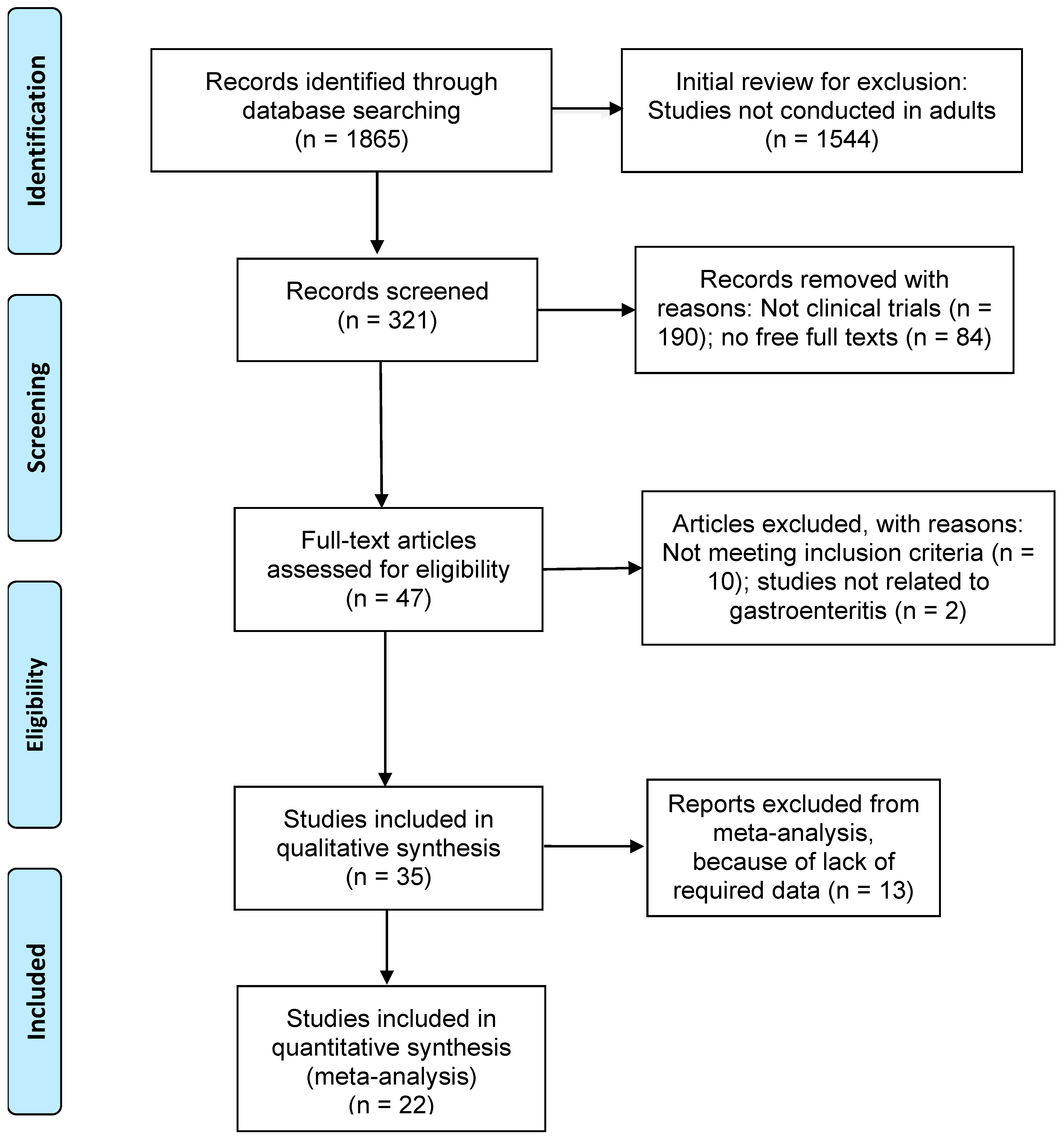
2. Materials and Methods
Quality Appraisal Methods
3. Results
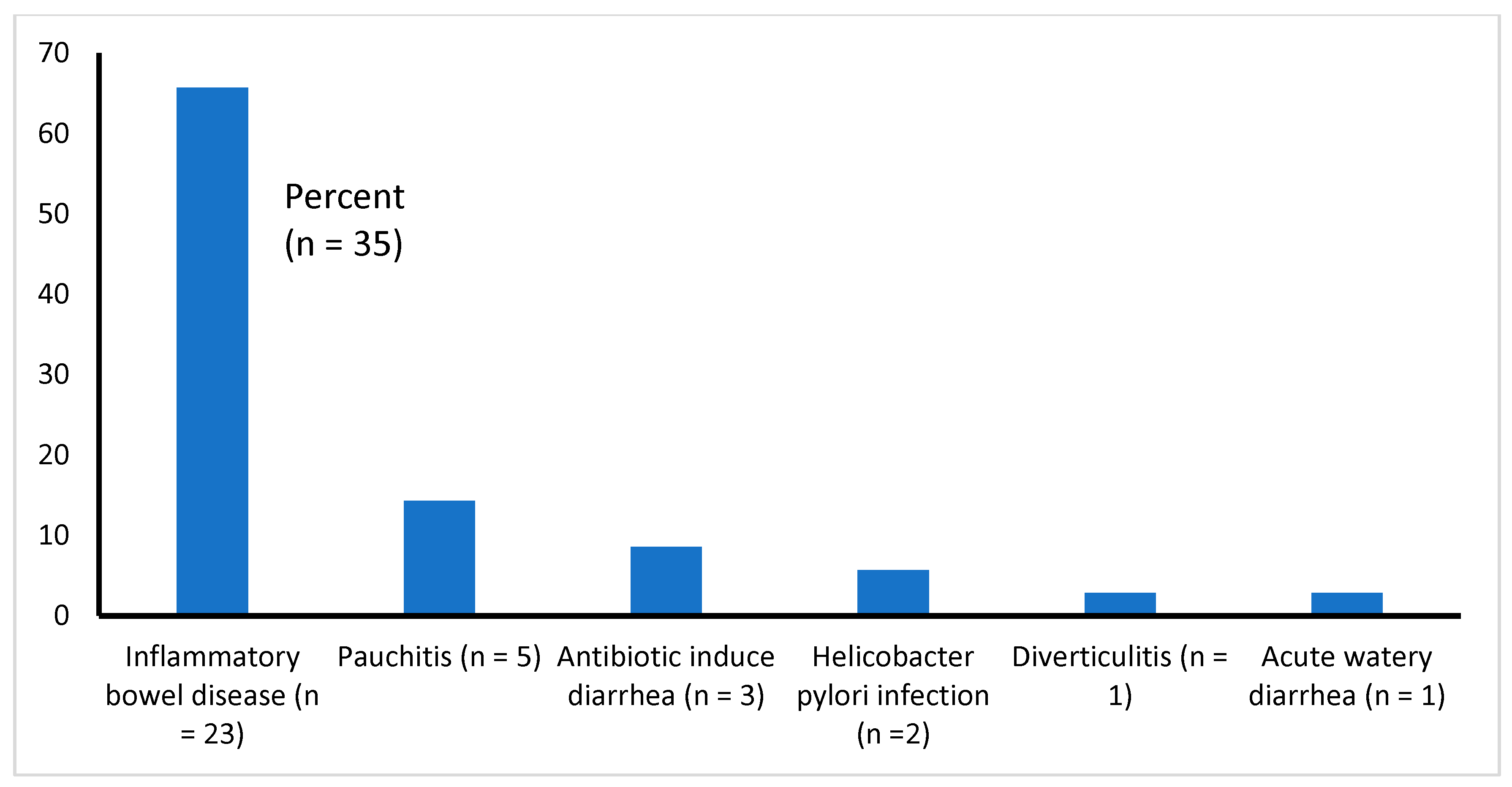
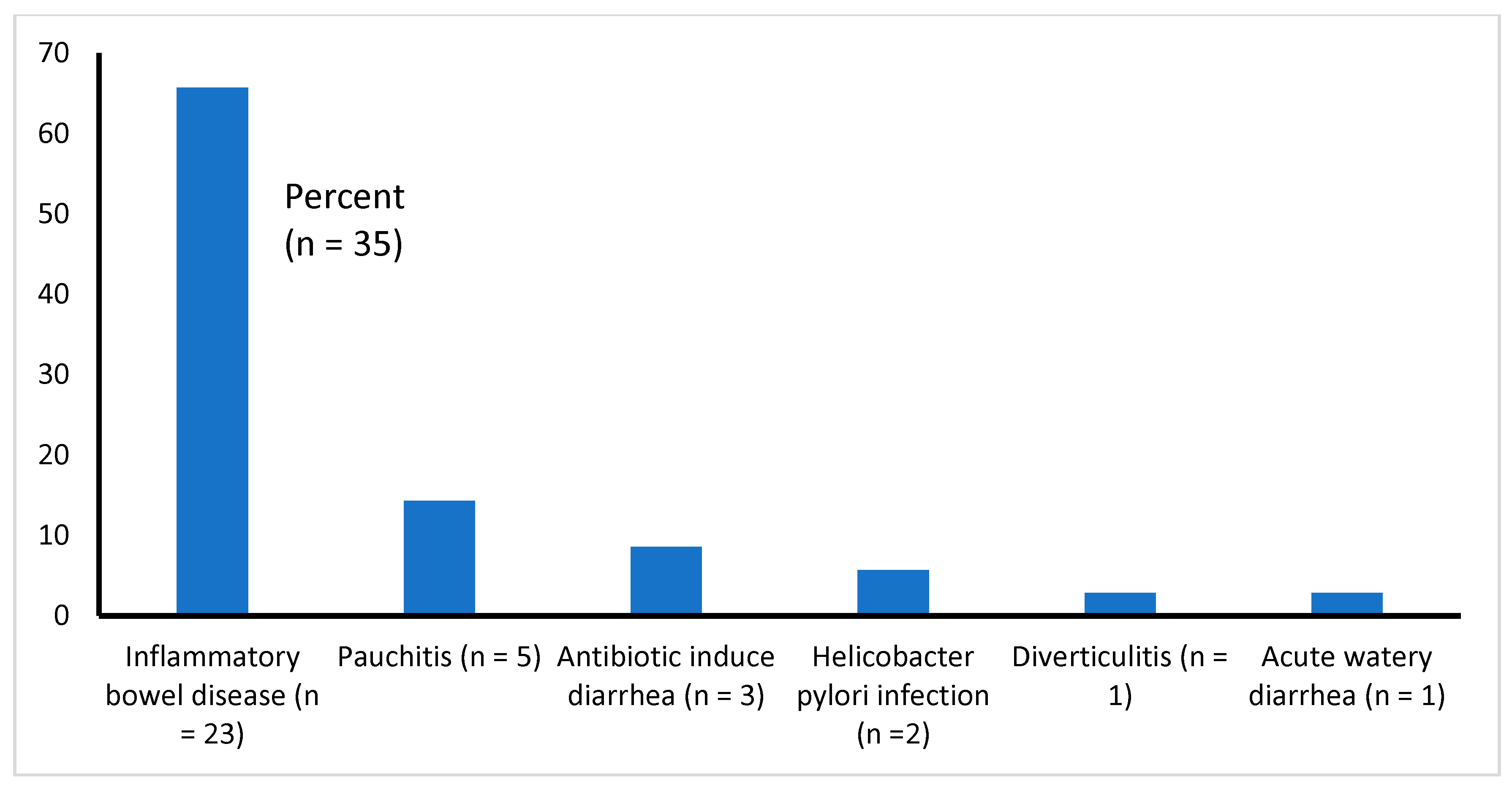
3.1. Type of Illnesses Associated with Diarrhea
3.2. Probiotic Strains Used and Follow-Up
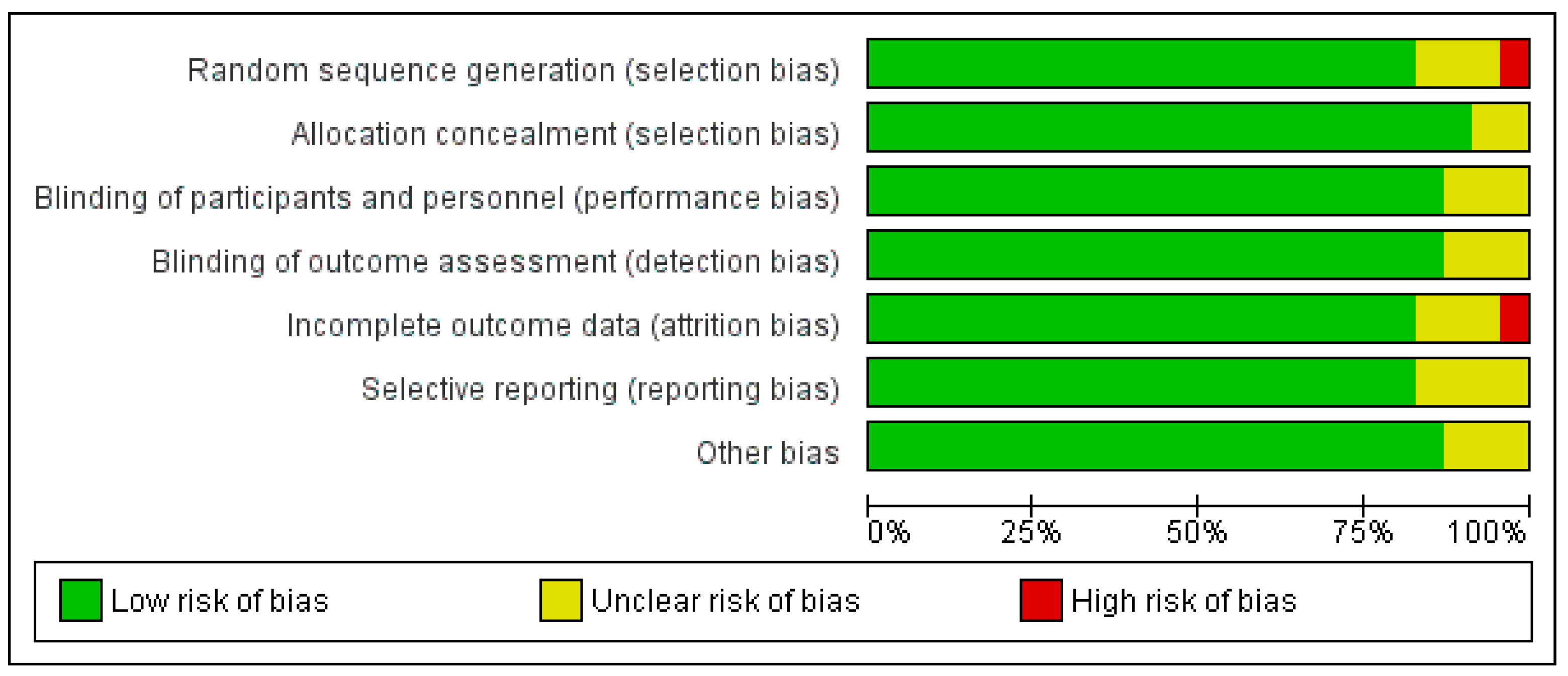
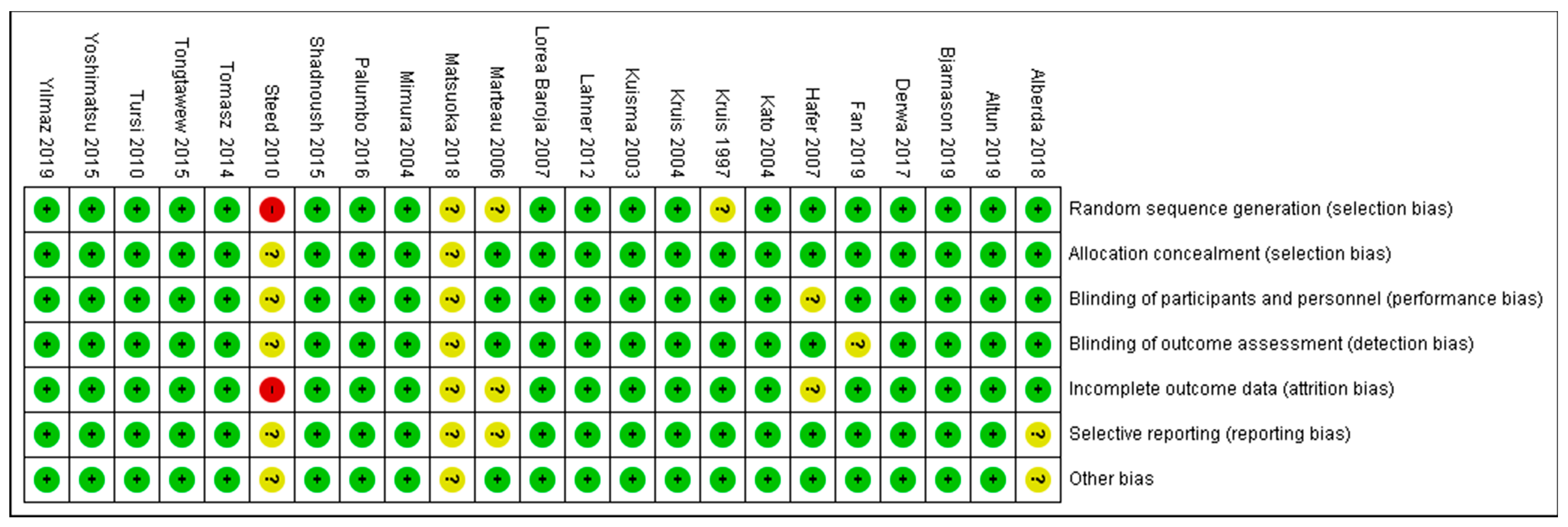
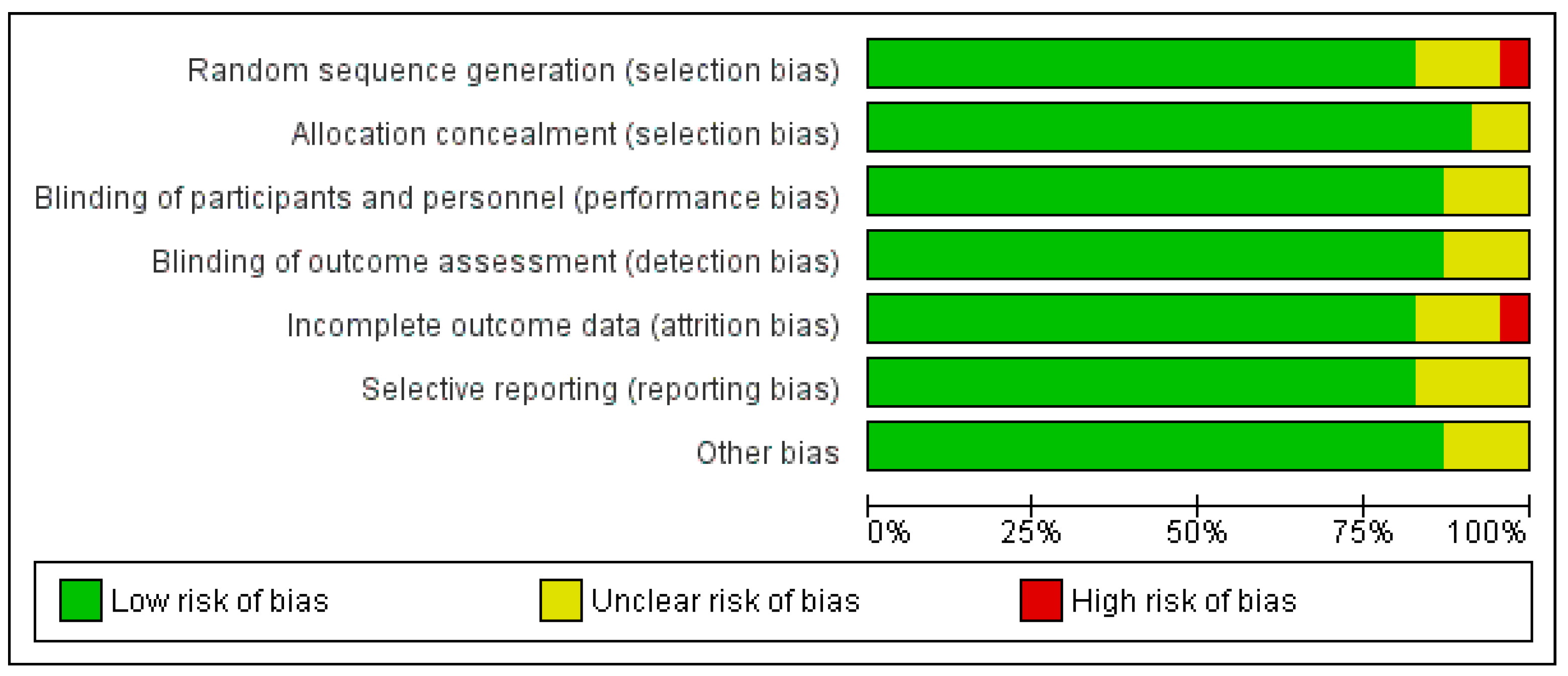
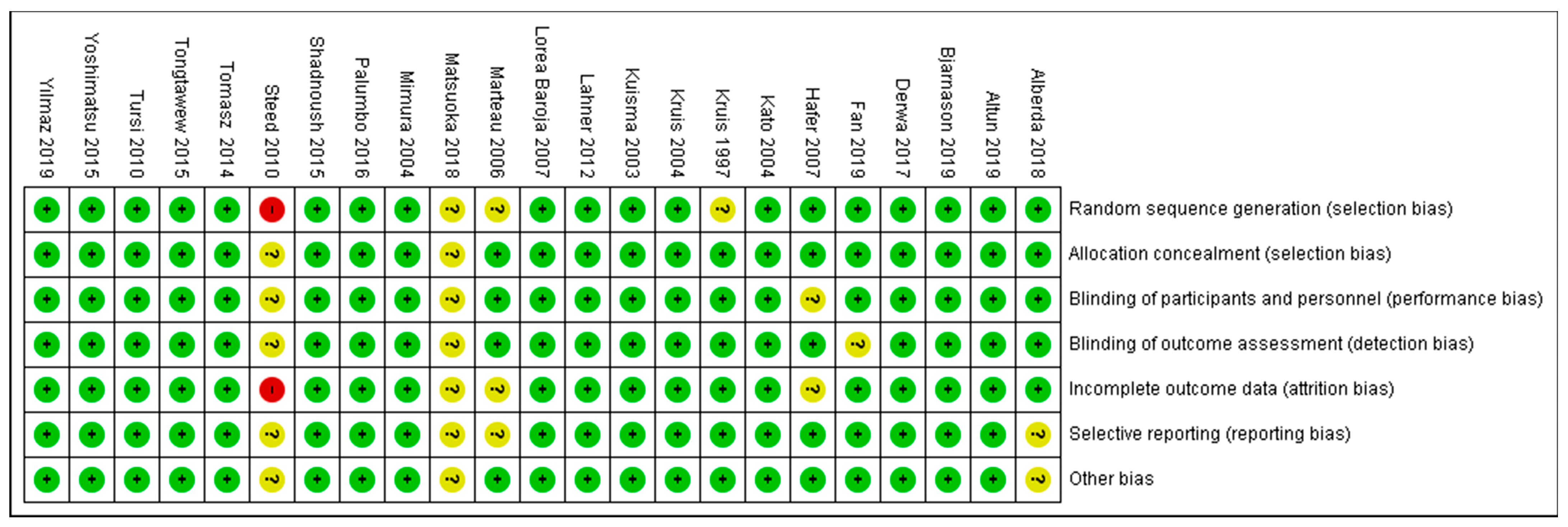
3.3. Quality Appraisal Findings
3.4. Efficacy and Safety of Probiotics
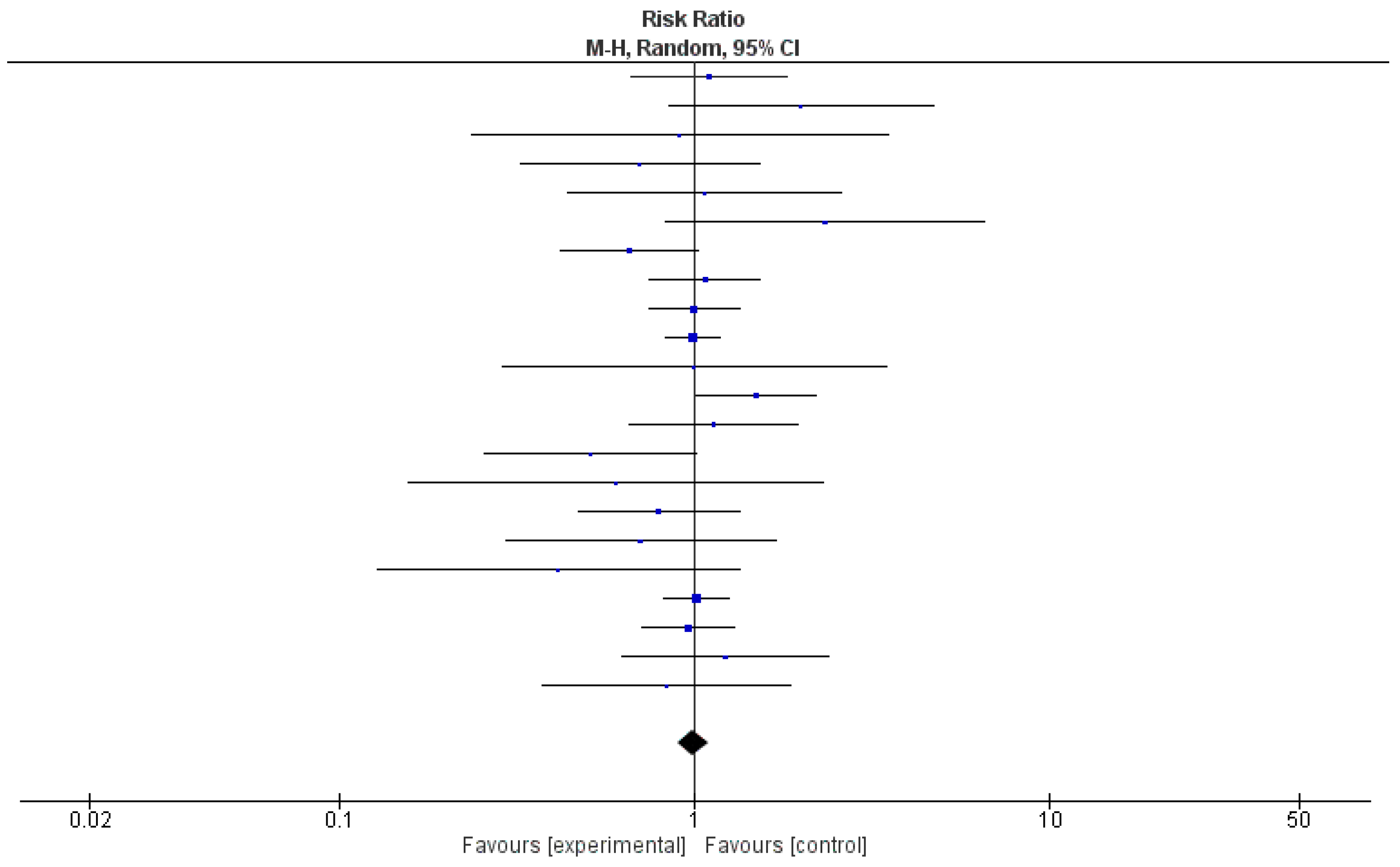
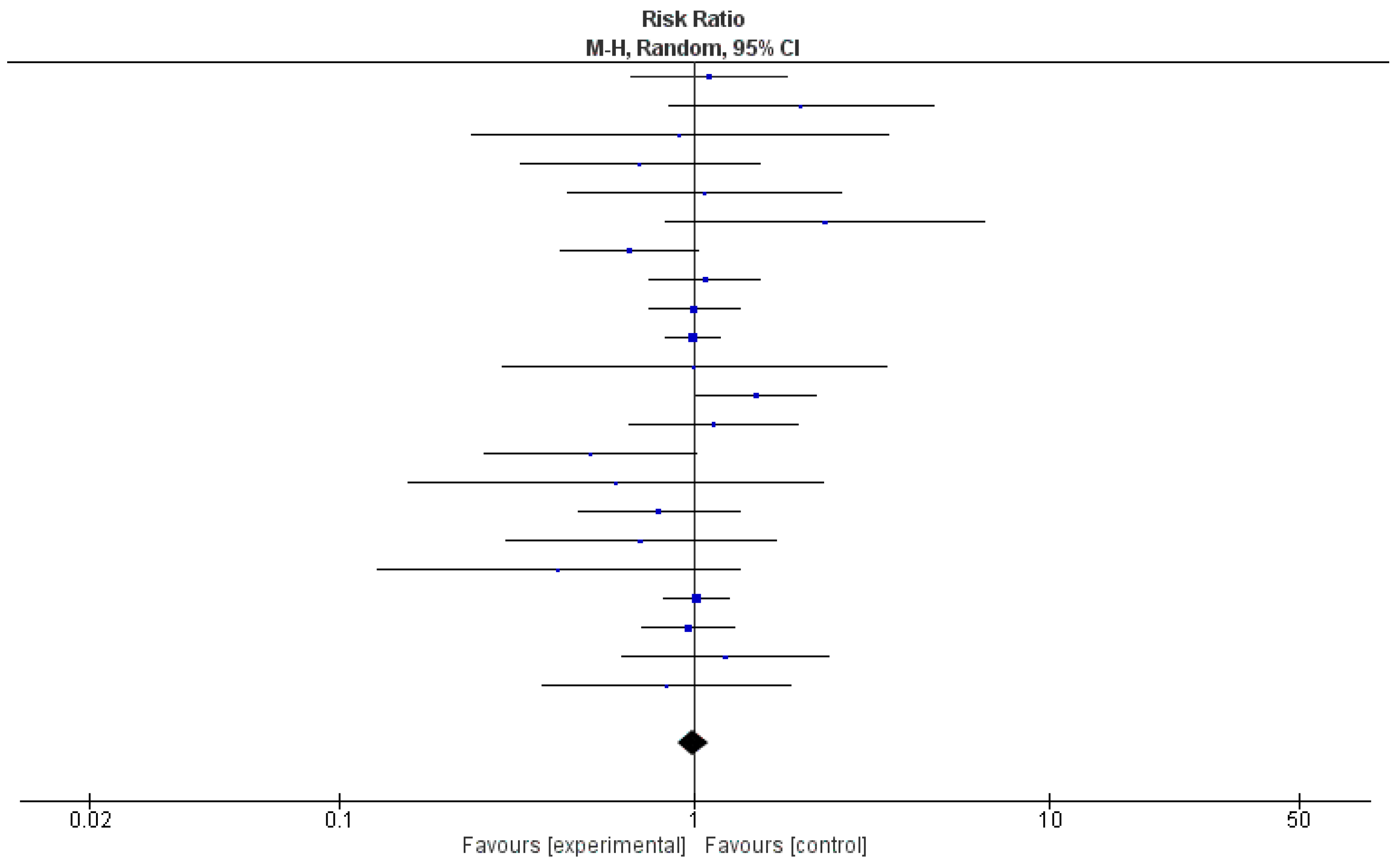
3.5. Effectiveness of Probiotics, as Evaluated through Meta-Analysis of 22 Clinical Trials
3.6. Overall Risk of Bias by Categories of Bias
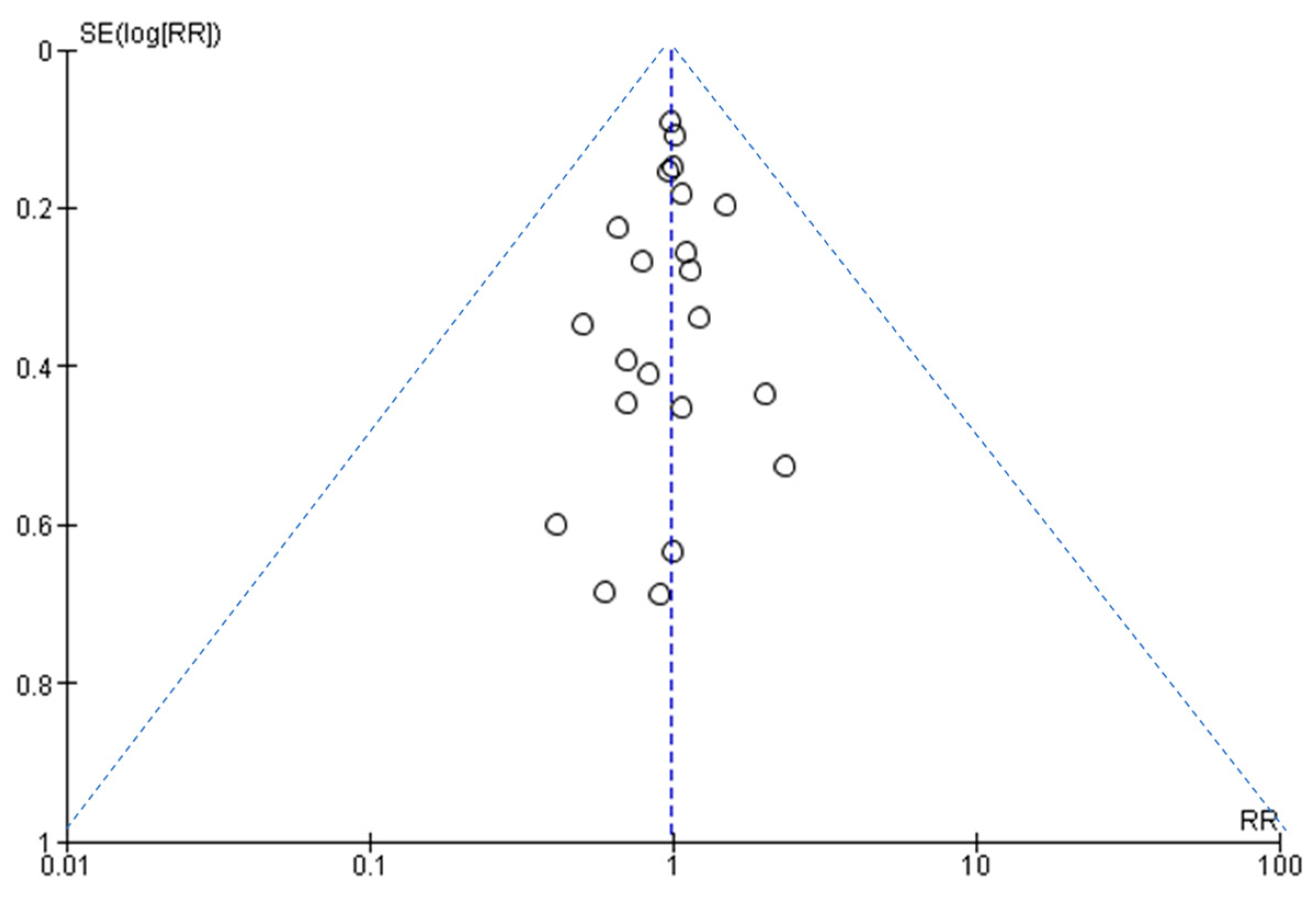
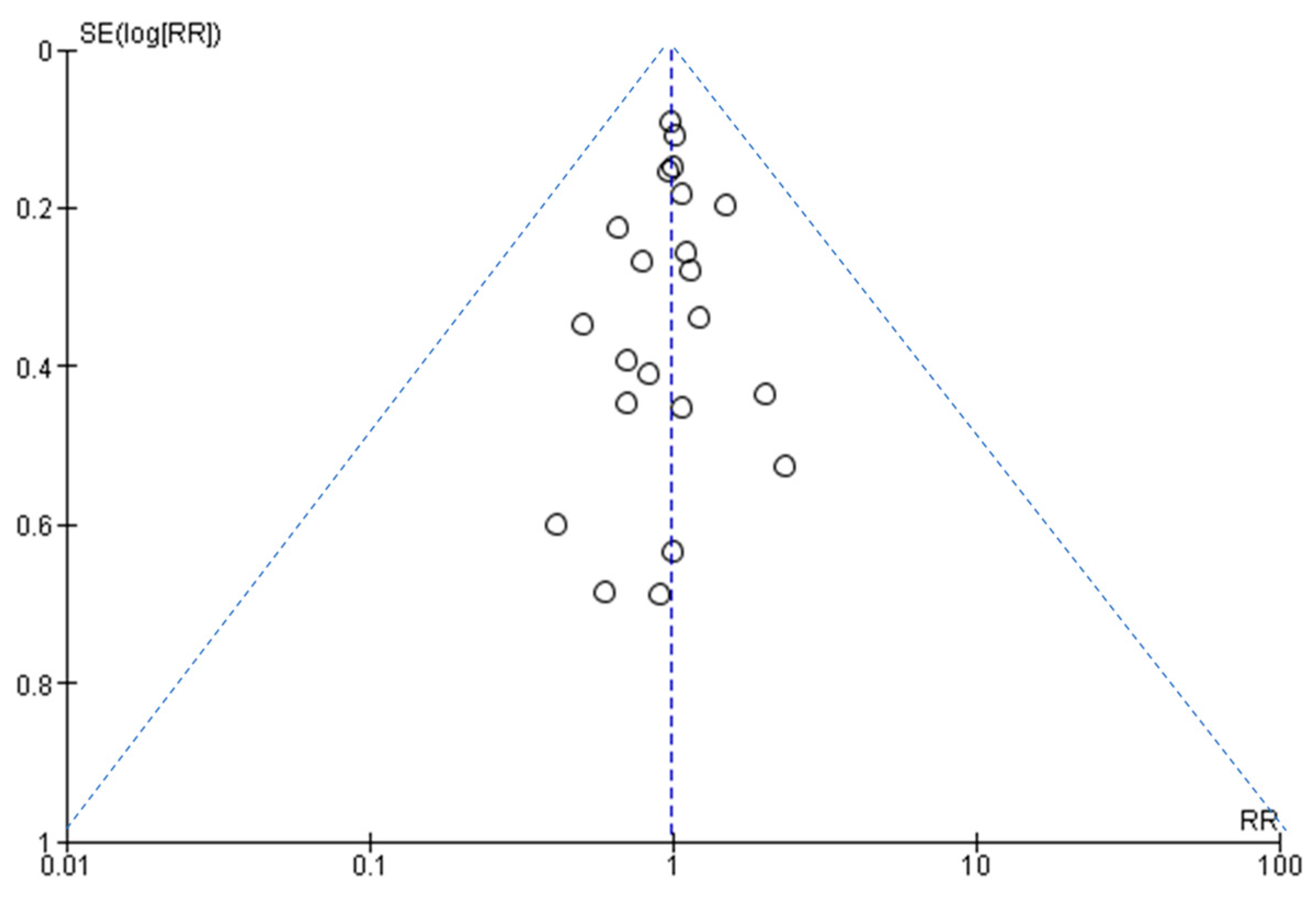
3.7. Assessment of Publication Bias
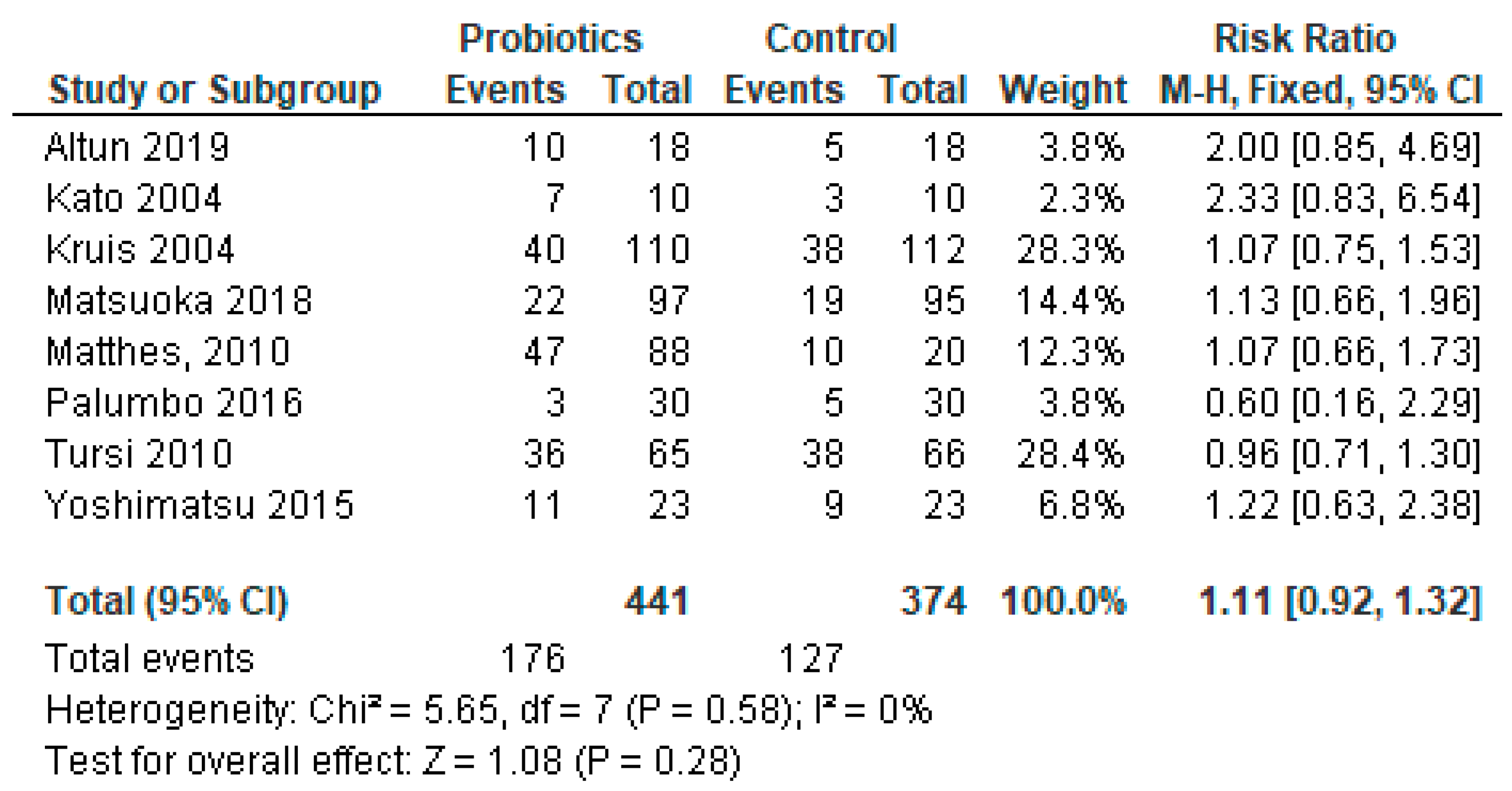
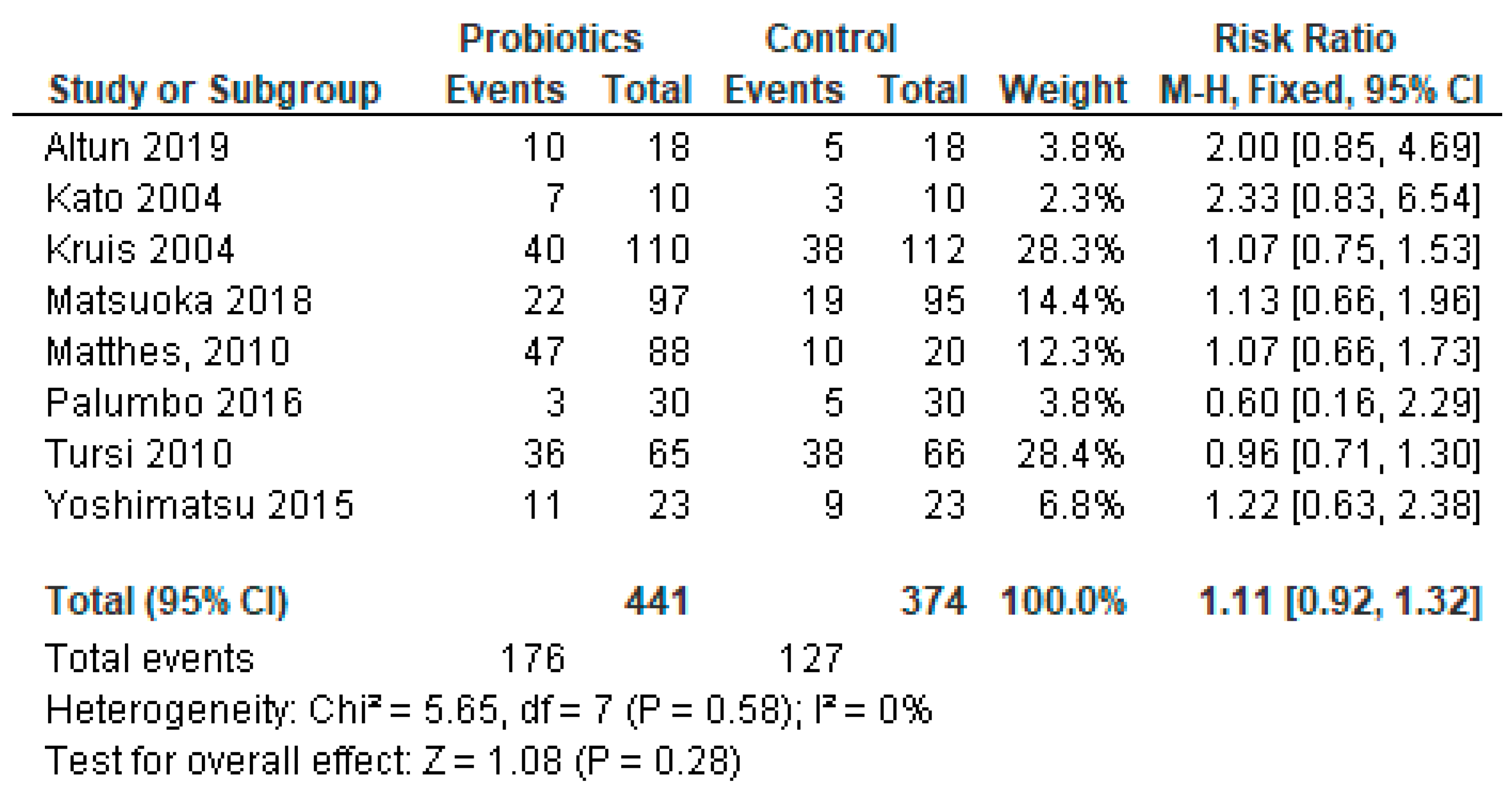
3.8. Sub-Group Meta-Analysis for Studies Reporting Ulcerative Colitis Only
4. Discussion
4.1. Effective Treatment with Probiotics
4.2. Ineffectiveness of Probiotics
4.3. Safety Issues
4.4. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bartsch, S.M.; Lopman, B.A.; Ozawa, S.; Hall, A.J.; Lee, B.Y. Global economic burden of norovirus gastroenteritis. PLoS ONE 2016, 11, e0151219. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.T.; Phan, K.; Teng, I.; Pu, J.; Watanabe, T. A systematic review and meta-analysis of the prevalence of norovirus in cases of gastroenteritis in developing countries. Medicine 2017, 96, e8139. [Google Scholar] [CrossRef] [PubMed]
- Graves, N.S. Acute gastroenteritis. Prim. Care Clin. Off. Pract. 2013, 40, 727–741. [Google Scholar] [CrossRef] [PubMed]
- Jagai, J.S.; Smith, G.S.; Schmid, J.E.; Wade, T.J. Trends in gastroenteritis-associated mortality in the United States, 1985–2005: Variations by ICD-9 and ICD-10 codes. BMC Gastroenterol. 2014, 14, 211. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.J.; Patel, M.M.; Lopman, B.A.; Armah, G.E. Part 2: Viral Diseases—Norovirus. In Hunter’s Tropical Medicine and Emerging Infectious Disease, 9th ed.; Magill, A.J., Ryan, E.T., Hill, D.R., Solomon, T., Eds.; Saunders Elsevier Inc.: Philadelphia, PA, USA, 2013; pp. 280–282. [Google Scholar]
- Centers for Disease Control and Prevention. Diarrhea: Common Illness, Global Killer. Available online: https://www.cdc.gov/healthywater/pdf/global/programs/globaldiarrhea508c.pdf (accessed on 29 September 2023).
- Lichtenstein, G.R.; Shahabi, A.; Seabury, S.A.; Lakdawalla, D.N.; Espinosa, O.D.; Green, S.; Brauer, M.; Baldassano, R.N. Increased lifetime risk of intestinal complications and extraintestinal manifestations in Crohn’s disease and ulcerative colitis. Gastroenterol. Hepatol. 2022, 18, 32–43. [Google Scholar]
- Williams, N.T. Probiotics. Am. J. Health Syst. Pharm. 2010, 67, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Tomasik, P.; Tomasik, P. Probiotics, non-dairy prebiotics and postbiotics in nutrition. Appl. Sci. 2020, 10, 1470. [Google Scholar] [CrossRef]
- Wilkins, T.; Sequoia, J. Probiotics for gastrointestinal conditions: A summary of the evidence. Am. Fam. Physician 2017, 96, 170–178. [Google Scholar]
- Applegate, J.A.; Walker, C.L.F.; Ambikapathi, R.; Black, R.E. Systematic review of probiotics for the treatment of community-acquired acute diarrhea in children. BMC Public Health 2013, 13, S16. [Google Scholar] [CrossRef]
- Huang, R.; Xing, H.Y.; Liu, H.J.; Chen, Z.F.; Tang, B.B. Efficacy of probiotics in the treatment of acute diarrhea in children: A systematic review and meta-analysis of clinical trials. Transl. Pediatr. 2021, 10, 3248–3260. [Google Scholar] [CrossRef]
- Mahen, M.; Rizka, A. The efficacy of probiotic in adults with acute infectious diarrhea. J. Kedocteran Indones. 2017, 5, 57–63. [Google Scholar] [CrossRef]
- Mitra, A.K.; Rabbani, G.H. A double-blind controlled trial of Bioflorin (Streptococcus faecium SF68) in adults with diarrhoea due to Vibrio cholerae and enterotoxigenic Escherichia coli. Gastroenterology 1990, 99, 1149–1152. [Google Scholar] [CrossRef]
- Goodman, C.; Keating, G.; Georgousopoulou, E.; Hespe, C.; Levett, K. Probiotics for the prevention of antibiotic-associated diarrhoea: A systematic review and meta-analysis. BMJ Open 2021, 11, e043054. [Google Scholar] [CrossRef]
- Kumar, L.S.; Pugalenthi, L.S.; Ahmad, M.; Reddy, S.; Barkhane, Z.; Elmadi, J. Probiotics in irritable bowel syndrome: A review of their therapeutic role. Cureus 2022, 14, e24240. [Google Scholar] [CrossRef]
- Iheozor-Ejiofor, Z.; Kaur, L.; Gordon, M.; Baines, P.A.; Sinopoulou, V.; Akobeng, A.K. Probiotics for maintenance of remission in ulcerative colitis. Cochrane Database Syst. Rev. 2020, 3, CD007443. [Google Scholar] [CrossRef] [PubMed]
- Limketkai, B.N.; Akobeng, A.K.; Gordon, M.; Adepoju, A.A. Probiotics for induction of remission in Crohn’s disease. Cochrane Database Syst. Rev. 2020, 7, CD006634. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Joanna Briggs Institute. JBI Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 3 May 2023).
- Alberda, C.; Marcushamer, S.; Hewer, T.; Journault, N.; Kutsogiannis, D. Feasibility of a Lactobacillus casei drink in the intensive care unit for prevention of antibiotic associated diarrhea and Clostridium difficile. Nutrients 2018, 10, 539. [Google Scholar] [CrossRef]
- Altun, H.K.; Yildiz, E.A.; Akin, M. Effects of synbiotic therapy in mild-to-moderately active ulcerative colitis: A randomized placebo-controlled study. Turk. J. Gastroenterol. 2019, 30, 313–320. [Google Scholar] [CrossRef]
- Bjarnason, I.; Sission, G.; Hayee, B. A randomised, double-blind, placebo-controlled trial of a multi-strain probiotic in patients with asymptomatic ulcerative colitis and Crohn’s disease. Inflammopharmacology 2019, 27, 465–473. [Google Scholar] [CrossRef]
- Derwa, Y.; Gracie, D.J.; Hamlin, P.J.; Ford, A.C. Systematic review with meta-analysis: The efficacy of probiotics in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2017, 46, 389–400. [Google Scholar] [CrossRef]
- Fan, H.; Du, J.; Liu, X.; Zheng, W.-W.; Zhuang, Z.-H.; Wang, C.-D.; Gao, R. Effects of pentasa-combined probiotics on the microflora structure and prognosis of patients with inflammatory bowel disease. Turk. J. Gastroenterol. 2019, 30, 680–685. [Google Scholar] [CrossRef]
- Groeger, D.; O’mahony, L.; Murphy, E.F.; Bourke, J.F.; Dinan, T.G.; Kiely, B.; Shanahan, F.; Quigley, E.M. Bifidobacterium infantis 35624 modulates host inflammatory processes beyond the gut. Gut Microbes 2013, 4, 325–339. [Google Scholar] [CrossRef] [PubMed]
- Hafer, A.; Krämer, S.; Duncker, S.; Krüger, M.; Manns, M.P.; Bischoff, S.C. Effect of oral lactulose on clinical and immunohistochemical parameters in patients with inflammatory bowel disease: A pilot study. BMC Gastroenterol. 2007, 7, 36. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Mizuno, S.; Umesaki, Y.; Ishii, Y.; Sugitani, M.; Imaoka, A.; Otsuka, M.; Hasunuma, O.; Kurihara, R.; Iwasaki, A.; et al. Randomized placebo-controlled trial assessing the effect of bifidobacteria-fermented milk on active ulcerative colitis. Aliment. Pharmacol. Ther. 2004, 20, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Krag, A.; Israelsen, H.; von Ryberg, B.; Andersen, K.K.; Bendtsen, F. Safety and efficacy of Profermin® to induce remission in ulcerative colitis. World J. Gastroenterol. 2012, 18, 1773–1780. [Google Scholar] [CrossRef] [PubMed]
- Kruis, W.; Schütz, E.; Fric, P.; Fixa, B.; Judmaier, G.; Stolte, M. Double-blind comparison of an oral Escherichia coli preparation and mesalazine in maintaining remission of ulcerative colitis. Aliment. Pharmacol. Ther. 1997, 11, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Kruis, W.; Frič, P.; Pokrotnieks, J.; Lukáš, M.; Fixa, B.; Kaščák, M.; Kamm, M.A.; Weismueller, J.; Beglinger, C.; Stolte, M.; et al. Maintaining remission of ulcerative colitis with the probiotic Escherichia coli Nissle 1917 is as effective as with standard mesalazine. Gut 2004, 53, 1617–1623. [Google Scholar] [CrossRef] [PubMed]
- Kuhbacher, T.; Ott, S.J.; Helwig, U.; Mimura, T.; Rizzello, F.; Kleessen, B.; Gionchetti, P.; Blaut, M.; Campieri, M.; Fölsch, U.R.; et al. Bacterial and fungal microbiota in relation to probiotic therapy (VSL# 3) in pouchitis. Gut 2006, 55, 833–841. [Google Scholar]
- Kuisma, J.; Mentula, S.; Jarvinen, H.; Kahri, A.; Saxelin, M.; Farkkila, M. Effect of Lactobacillus rhamnosus GG on ileal pouch inflammation and microbial flora. Aliment. Pharmacol. Ther. 2003, 17, 509–515. [Google Scholar] [CrossRef]
- Lahner, E.; Esposito, G.; Zullo, A.; Hassan, C.; Cannaviello, C.; Di Paolo, M.C.; Pallotta, L.; Garbagna, N.; Grossi, E.; Annibale, B. High-fibre diet and Lactobacillus paracasei B21060 in symptomatic uncomplicated diverticular disease. World J. Gastroenterol. 2012, 18, 5918–5924. [Google Scholar] [CrossRef] [PubMed]
- Lorea Baroja, M.; Kirjavainen, P.V.; Hekmat, S.; Reid, G. Anti-inflammatory effects of probiotic yogurt in inflammatory bowel disease patients. Clin. Exp. Immunol. 2007, 149, 470–479. [Google Scholar] [CrossRef] [PubMed]
- Marteau, P.; Lémann, M.; Seksik, P.; Laharie, D.; Colombel, J.F.; Bouhnik, Y. Ineffectiveness of Lactobacillus johnsonii LA1 for prophylaxis of postoperative recurrence in Crohn’s disease: A randomised, double blind, placebo controlled GETAID trial. Gut 2006, 55, 842–847. [Google Scholar] [CrossRef]
- Matsuoka, K.; Uemura, Y.; Kanai, T.; Kunisaki, R.; Suzuki, Y.; Yokoyama, K.; Yoshimura, N.; Hibi, T. Efficacy of Bifidobacterium breve fermented milk in maintaining remission of ulcerative colitis. Dig. Dis. Sci. 2018, 63, 1910–1919. [Google Scholar] [CrossRef]
- Matthes, H.; Krummenerl, T.; Giensch, M.; Wolff, C.; Schulze, J. Clinical trial: Probiotic treatment of acute distal ulcerative colitis with rectally administered Escherichia coli Nissle 1917 (EcN). BMC Complement. Altern. Med. 2010, 10, 13. [Google Scholar] [CrossRef]
- Mimura, T.; Rizzello, F.; Helwig, U.; Poggioli, G.; Schreiber, S.; Talbot, I.C.; Nicholls, R.J.; Gionchetti, P.; Campieri, M.; Kamm, M.A. Once daily high dose probiotic therapy (VSL# 3) for maintaining remission in recurrent or refractory pouchitis. Gut 2004, 53, 108–114. [Google Scholar] [PubMed]
- Montalto, M.; Gallo, A.; Curigliano, V.; D’Onofrio, F.; Santoro, L.; Covino, M.; Dalvai, S.; Gasbarrini, A.; Gasbarrini, G. Clinical trial: The effects of a probiotic mixture on non-steroidal anti-inflammatory drug enteropathy–a randomized, double-blind, cross-over, placebo-controlled study. Aliment. Pharmacol. Ther. 2010, 32, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, V.D.; Romeo, M.; Gammazza, A.M.; Carini, F.; Damiani, P.; Damiano, G.; Buscemi, S.; Monte, A.I.L.; Gerges-Geagea, A.; Jurjus, A.; et al. The long-term effects of probiotics in the therapy of ulcerative colitis: A clinical study. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2016, 160, 372–377. [Google Scholar] [CrossRef]
- Persborn, M.; Gerritsen, J.; Wallon, C.; Carlsson, A.; Akkermans, L.M.A.; Söderholm, J.D. The effects of probiotics on barrier function and mucosal pouch microbiota during maintenance treatment for severe pouchitis in patients with ulcerative colitis. Aliment. Pharmacol. Ther. 2013, 38, 772–783. [Google Scholar] [CrossRef]
- Shadnoush, M.; Hosseini, R.S.; Khalilnezhad, A.; Navai, L.; Goudarzi, H.; Vaezjalali, M. Effects of probiotics on gut microbiota in patients with inflammatory bowel disease: A double-blind, placebo-controlled clinical trial. Korean J. Gastroenterol. 2015, 65, 215–221. [Google Scholar] [CrossRef]
- Shen, B.; Brzezinski, A.; Fazio, V.W.; Remzi, F.H.; Achkar, J.-P.; Bennett, A.E.; Sherman, K.; Lashner, B.A. Maintenance therapy with a probiotic in antibiotic-dependent pouchitis: Experience in clinical practice. Aliment. Pharmacol. Ther. 2005, 22, 721–728. [Google Scholar] [CrossRef]
- Steed, H.; Macfarlane, G.T.; Blackett, K.L.; Bahrami, B.; Reynolds, N.; Walsh, S.V.; Cummings, J.H.; Macfarlane, S. Clinical trial: The microbiological and immunological effects of symbiotic consumption–a randomized double-blind placebo-controlled study in active Crohn’s disease. Aliment. Pharmacol. Ther. 2010, 32, 872–883. [Google Scholar] [CrossRef]
- Tomasz, B.; Zoran, S.; Jarosław, W.; Ryszard, M.; Marcin, G.; Robert, B.; Piotr, K.; Lukasz, K.; Jacek, P.; Piotr, G.; et al. Long-term use of probiotics Lactobacillus and Bifidobacterium has a prophylactic effect on the occurrence and severity of pouchitis: A randomized prospective study. Biomed Res. Int. 2014, 2014, 208064. [Google Scholar] [CrossRef]
- Tongtawee, T.; Dechsukhum, C.; Leeanansaksiri, W.; Kaewpitoon, S.; Kaewpitoon, N.; Loyd, R.A.; Matrakool, L.; Panpimanmas, S. Effect of pretreatment with Lactobacillus delbrueckii and Streptococcus thermophillus on tailored triple therapy for Helicobacter pylori eradication: A prospective randomized controlled clinical trial. Asian Pac. J. Cancer Prev. 2015, 16, 4885–4890. [Google Scholar] [CrossRef] [PubMed]
- Tursi, A.; Brandimarte, G.; Papa, A.; Giglio, A.; Elisei, W.; Giorgetti, G.M.; Forti, G.; Morini, S.; Hassan, C.; Pistoia, M.A.; et al. Treatment of relapsing mild-to-moderate ulcerative colitis with the probiotic VSL# 3 as adjunctive to a standard pharmaceutical treatment: A double-blind, randomized, placebo-controlled study. Am. J. Gastroenterol. 2010, 105, 2218–2227. [Google Scholar] [PubMed]
- Venturi, A.; Gionchetti, P.; Rizzello, F.; Johansson, R.; Zucconi, E.; Brigidi, P.; Matteuzzi, D.; Campieri, M. Impact on the composition of the faecal flora by a new probiotic preparation: Preliminary data on maintenance treatment of patients with ulcerative colitis. Aliment. Pharmacol. Ther. 1999, 13, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, İ.; Dolar, M.E.; Özpınar, H. Effect of administering kefir on the changes in fecal microbiota and symptoms of inflammatory bowel disease: A randomized controlled trial. Turk. J. Gastroenterol. 2019, 30, 242–253. [Google Scholar] [CrossRef]
- Yoshimatsu, Y.; Yamada, A.; Furukawa, R.; Sono, K.; Osamura, A.; Nakamura, K.; Aoki, H.; Tsuda, Y.; Hosoe, N.; Takada, N.; et al. Effectiveness of probiotic therapy for the prevention of relapse in patients with inactive ulcerative colitis. World J. Gastroenterol. 2015, 21, 5985–5994. [Google Scholar] [CrossRef]
- Ziemniak, W. Efficacy of Helicobacter pylori eradication taking into account its resistance to antibiotics. J. Physiol. Pharmacol. 2006, 57, 123–141. [Google Scholar]
- Zocco, M.A.; dal Verme, L.Z.; Cremonini, F.; Piscaglia, A.C.; Nista, E.C.; Candelli, M.; Novi, M.; Rigante, D.; Cazzato, I.A.; Ojetti, V.; et al. Efficacy of Lactobacillus GG in maintaining remission of ulcerative colitis. Aliment. Pharmacol. Ther. 2006, 23, 1567–1574. [Google Scholar] [CrossRef]
- Zwolinska-Wcislo, M.; Brzozowski, T.; Budak, A.; Kwiecien, S.; Sliwowski, Z.; Drozdowicz, D.; Trojanowska, D.; Rudnicka-Sosin, L.; Mach, T.; Konturek, S.J.; et al. Effect of Candida colonization on human ulcerative colitis and the healing of inflammatory changes of the colon in the experimental model of colitis ulcerosa. J. Physiol. Pharmacol. 2009, 60, 107–118. [Google Scholar] [PubMed]
- Ansari, F.; Pashazadeh, F.; Nourollahi, E.; Hajebrahimi, S.; Munn, Z.; Pourjafar, H. A systematic review and meta-analysis: The effectiveness of probiotics for viral gastroenteritis. Curr. Pharm. Biotechnol. 2020, 21, 1042–1051. [Google Scholar] [CrossRef] [PubMed]
- Vakadaris, G.; Stefanis, C.; Giorgi, E.; Brouvalis, M.; Voidarou, C.; Kourkoutas, Y.; Tsigalou, C.; Bezirtzoglou, E. The role of probiotics in inducing and maintaining remission in Crohn’s disease and ulcerative colitis: A systematic review of the literature. Biomedicines 2023, 11, 494. [Google Scholar] [CrossRef] [PubMed]
- Lorentz, A.; Müller, L. Probiotics in the treatment of inflammatory bowel diseases in adulthood: A systematic review. J. Gastrointest. Liver Dis. 2022, 31, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Fagnant, H.S.; Isidean, S.D.; Wilson, L.; Bukhari, A.S.; Allen, J.T.; Agans, R.T.; Lee, D.M.; Hatch-McChesney, A.; Whitney, C.C.; Sullo, E.; et al. Orraly ingested probiotic, prebiotic, and symbiotic interventions as countermeasures for gastrointestinal tract infections in nonelderly adults: A systematic review and meta-analysis. Adv. Nutr. 2023, 14, 539–554. [Google Scholar] [CrossRef]
- Jones, E.A.K.; Mitra, A.K.; Bisht, A.; Edet, P.P.; Iseguede, F.; Okoye, E. Probiotics in gastroenteritis in children: A systematic review. IMC J. Med. Sci. 2023, 17, 010. [Google Scholar] [CrossRef]
- Cameron, D.; Hock, Q.S.; Kadim, M.; Mohan, N.; Ryoo, E.; Sandhu, B.; Yamashiro, Y.; Jie, C.; Hoekstra, H.; Guarino, A. Probiotics for gastrointestinal disorders: Proposed recommendations for children of the Asia-Pacific region. World J. Gastroenterol. 2017, 23, 7952–7964. [Google Scholar] [CrossRef]
- Dore, M.P.; Bibbò, S.; Fresi, G.; Bassotti, G.; Pes, G.M. Side effects associated with probiotic Use in adult patients with inflammatory bowel disease: A systematic review and meta-analysis of randomized controlled trials. Nutrients 2019, 11, 2913. [Google Scholar] [CrossRef]
- Doron, S.; Snydman, D.R. Risk and safety of probiotics. Clin. Infect. Dis. 2015, 60, S129–S134. [Google Scholar] [CrossRef]
- Ciernikova, S.; Mego, M.; Semanova, M.; Wachsmannova, L.; Adamcikova, Z.; Stevurkova, V.; Drgona, L.; Zajac, V. Probiotic survey in cancer patients treated in the outpatient department in a comprehensive cancer center. Integr. Cancer Ther. 2017, 16, 188–195. [Google Scholar] [CrossRef]
- van den Nieuwboer, M.; Brummer, R.J.; Guarner, F.; Morelli, L.; Cabana, M.; Claassen, E. The administration of probiotics and synbiotics in immune compromised adults: Is it safe? Benef. Microbes 2015, 6, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Merenstein, D.; Pot, B.; Leyer, G.; Ouwehand, A.C.; Preidis, G.A.; Elkins, C.A.; Hill, C.; Lewis, Z.T.; Shane, A.L.; Zmora, N.; et al. Emerging issues in probiotic safety: 2023 perspectives. Gut Microbes 2023, 15, 2185034. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors, Year [Ref.] | Disease Conditions 1 and Sample Size | Type of Probiotics Used | Prevention/Treatment | Effective | Quality Appraisal and Scoring 6 | Major Findings/Conclusions | Country |
|---|---|---|---|---|---|---|---|
| Alberda et al., 2018 [21] | Antibiotic-associated diarrhea (AAD) and Clostridium difficile-induced diarrhea; sample size = 32 | Lactobacillus casei | Prevention | Yes | Score 3 out of 4 (Moderate) | Probiotic drinks can prevent AAD and Clostridium difficile infections. | Canada |
| Altun, et al., 2019 [22] | Inflammatory bowel disease (IBD) 2: ulcerative colitis (UC); sample size = 40 | Enterococcus faecium, Lactobacillus plantarum, Streptococcus thermophilus, Bifidobacterium lactis, Lactobacillus acidophilus, Bifidobacterium longum)-and fructooligosaccharide | Treatment | No | Score 4 out of 4 (High) | The use of synbiotic therapy3 had no statistically significant effect in the improvement of clinical and endoscopic parameters compared with controls. | Turkey |
| Bjarnason, et al., 2019 [23] | IBDs: UC (n = 81) and Crohn’s disease (CD) (n = 61); total samples more than 500. | Symprove contains multiple strains of probiotics such as Lactobacillus plantarum, Lactobacillus rhamnosus, Lactobacillus plantarum, Lactobacillus acidophilus, and E. faecium | Treatment | Yes | Score 4 out of 4 (High) | Multi-strain probiotics decreased intestinal inflammation in patients with UC, but not in patients with CD. | United Kingdom |
| Derwa, et al., 2017 [24] | IBDs 2; sample size = 777 | Probiotics vs. 5-aminosalicylates (5-ASAs) (in one RCT); probiotics vs. placebo (in 7 RCTs). | Treatment | No | Score 4 out of 4 (High) | There was no benefit of probiotics over 5-ASAs 4 or placebo in inducing remission in active inflammatory bowel diseases. For UC, relative risk of failure to achieve remission = 0.86; 95% CI = 0.68–1.08. | Multiple countries |
| Fan, et al., 2019 [25] | IBDs 2; sample size = 40 | Bifico contains probiotic bacteria Bacillus Coagulans GBI-30, 6086. Bifico was given as an adjuvant treatment with Pentasa, which is an anti-inflammatory agent. | Treatment | Yes | Score 4 out of 4 (High) | A combination of probiotics and pentasa can improve microflora composition in patients with IBD and reduce the level of inflammatory cytokines. | China |
| Groeger, et al., 2013 [26] | IBDs 2; chronic fatigue syndrome (CFS); Psoriasis. Sample sizes: UC = 22, CFS = 48, psoriasis = 26. | Bifidobacterium infantis 35624 | Treatment | Yes | Score 4 out of 4 (High) | Microbiota in humans have immuno-modulatory effects on both the mucosal and systemic immune systems. | Ireland |
| Hafer, et al., 2007 [27] | IBDs 2; sample sizes: UC = 14, Crohn’s disease = 17. | Standard treatment vs. standard treatment with oral lactulose. | Treatment | No | Score 3 out of 4 (Moderate) | Oral lactulose has no beneficial no clinical and immunological effects on IBD patients. | Germany |
| Kato, et al., 2004 [28] | IBD: UC; sample size = 20 | Bifidobacteria-fermented milk (BFM) | Treatment | Yes | Score 3 out of 4 (Moderate) | Supplementation with BFM has beneficial effects in managing active ulcerative colitis and is more effective than the conventional treatment alone. | Japan |
| Krag, et al., 2012 [29] | IBD: UC; sample size = 39 | Profermin, consisting of fermented oats, Lactobacillus plantarum 299v, barley malt, lecithin, and water | Treatment | Yes | Score 4 out of 4 (High) | Profermin is safe and may be effective in inducing remission of active ulcerative colitis. | Denmark |
| Kruis, et al., 1997 [30] | IBD: UC; sample size = 120 | Escherichia coli Nissle (Serotype 06: K5: H1), as an adjuvant treatment with mesalazine (also known as 5-aminosalicylic acid (5-ASA) 5 | Treatment | Yes | Score 4 out of 4 (High) | E. coli (Serotype 06: K5: H1) effectively prevents remission of ulcerative colitis as a standard treatment with 5-ASA 4. | Germany, Czech Republic, and Austria |
| Kruis, et al., 2004 [31] | IBD: UC; sample size = 327 | Escherichia coli Nissle 1917 | Maintaining remission and prevention of relapses | Yes | Score 4 out of 4 (High) | Probiotic EcN has therapeutic effects and is safe for remission in UC. EcN can be used as an alternative to 5-ASA 4. | Germany |
| Kuehbache, et al., 2006 [32] | Pouchitis 4; sample size = 15 | VSL #3 consists of Lactobacillus casei, L. plantarum, L. acidophilus, L. bulgaricus, Bifidobacterium longuum, B. breve, B. infantis, and Streptococcus salivarius sub-spp. Thermophillus | Treatment | Yes | Score 3 out of 4 (Moderate) | Probiotic therapy with VSL #3 increases the diversity, richness and total number of intestinal bacteria and bacterial microbiota. | Germany |
| Kuisma, et al., 2003 [33] | Pouchitis 4; sample size = 20 | Lactobacillus rhamnosus GG | Treatment | No | Score 3 out of 4 (Moderate) | Lactobacillus GG can alter the microbial flora in ileo-anal pouches but was inefficient for clinically improving pouch inflammation. | Finland |
| Lahner, et al., 2012 [34] | Symptomatic uncomplicated diverticular disease; sample size = 45 | Lactobacillus paracasei B21060 (symbiotic sachet Flortec©) plus high fiber diet (Treatment Group) vs high fiber diet only (Controls) | Treatment | Yes | Score 3 out of 4 (Moderate) | The treatment group having symbiotic sachet Flortec© plus a high fiber diet improved of clinical symptoms (abdominal pain, bloating) significantly more than the control group. | Italy |
| Lorea Baroja, et al., 2007 [35] | IBD: Crohn’s disease (n = 15) and UC (n = 5), control, (n = 20); total sample size = 40 | Lactobacillus rhamnosus GR-1 and L. reuteri RC-14- supplemented yogurt vs. placebo | Prevention | Yes | Score 4 out of 4 (High) | Short-term probiotic yogurt consumption with Lactobacillus rhamnosus GR-1 and RC-14 has beneficial immune modulatory effects. | Canada |
| Marteau, et al., 2006 [36] | IBD: Crohn’s disease; sample size = 98 | Lactobacillus johnsonii LA1 | Prevention of relapses | No | Score 4 out of 4 (High) | Lactobacillus johnsonii LA1 had no sufficient effect to prevent the recurrence of Crohn’s disease. | France |
| Matsuoka, et al., 2018 [37] | IBD: UC; sample size = 195 | Bifidobacterium breve fermented milk (BFM) | Prevention | No | Score 4 out of 4 (High) | BFM had no effect on the time to relapse in UC patients, compared with placebo. | Japan |
| Matthes, et al., 2010 [38] | IBD: UC; sample size = 90 (70 with UC and 20 controls) | Escherichia coli Nissle 1917 (EcN) | Treatment | Yes | Score 3 out of 4 (Moderate) | Escherichia coli Nissle 1917 (EcN) may be an alternative treatment for moderate distal UC. | Germany |
| Mimura, et al., 2004 [39] | Recurrent or refractory pouchitis 3; sample size = 36 | VSL #3 contains Lactobacillus casei, L. plantarum, L. acidophilus, L. bulgaricus, Bifidobacterium. longuum, B. breve, B. infantis Streptococcus salivarius subsp. Thermophillus | Treatment of remission | Yes | Score 3 out of 4 (Moderate) | VSL#3 probiotic therapy is highly effective in maintaining treatment of recurrent pouchitis 3 and improving quality of life. | United Kingdom and Italy |
| Mitra & Rabbani, 1990 [14] | Acute watery diarrhea due to Vibrio cholerae and E. coli infection; sample size = 183 | Bioflorin (Streptococcus faecium SF68), given orally along with intravenous rehydration, and followed by oral rehydration solution | Treatment | No | Score 4 out of 4 (High) | Bioflorin was not effective in treating acute diarrhea due to V. cholerae and enterotoxigenic E. coli infections. | Bangladesh |
| Montalto, et al., 2010 [40] | Non-steroidal anti-inflammatory drug-induced enteropathy; sample size = 20 | VSL #3 contains Lactobacillus casei, L. plantarum, L. acidophilus, L. bulgaricus, Bifidobacterium. longuum, B. breve, B. infantis Streptococcus salivarius subsp. Thermophillus | Treatment | Yes | Score 2 out of 4 (Poor) | Probiotics mixture could be useful in decreasing indomethacin-induced intestinal inflammation. | Italy |
| Palumbo, et al., 2016 [41] | IBD: UC; sample size = 60 | A probiotic blend, which consists of Lactobacillus salivarius, Lactobacillus acidophilus and Bifidobacterium bifidus strain BGN4, given as an adjuvant therapy with Mesalazine | Treatment | Yes | Score 3 out of 4 (Moderate) | Long-term treatment modality of anti-inflammatory drugs and probiotics is viable and could be an alternative treatment for mild-to moderate UC. | Italy |
| Persborn, et al., 2013 [42] | Pouchitis 4; sample size = 16 patients with pouchitis and 13 controls with a healthy ileoanal pouch | Bifidobacterium bifidum (W23), B. lactis (W51), B. lactis (W52), Lactobacillus acidophilus (W22), L. casei (W56), L. paracasei (W20), L. plantarum (W62), L. salivarius (W24), L. lactis (W19) | Treatment | Yes | Score 3 out of 4 (Moderate) | Probiotics restored the mucosal barrier to E. coli in patients with pouchitis 3. This can prevent recurrence during maintenance therapy. | Sweden |
| Shadnoush, et al., 2015 [43] | IBDs 2; sample size = 305, of which 105 IBD patients received probiotic yogurt, 105 IBD patients received placebo, and 95 healthy controls received probiotic yogurt | Probiotic yogurt containing Lactobacillus acidophilus La-5 and Bifidobacterium BB-12 | Treatment | Inconclusive | Score 3 out of 4 (Moderate) | Fiber and energy intake in the treatment group did not increase when compared with those of controls. However, consumption of probiotic yogurt by patients with IBD may help to increase the number of probiotic bacteria in the intestine, thus improving intestinal function. | Iran |
| Shen, et al., 2005 [44] | Antibiotic-dependent pouchitis 4; sample size = 31 | VSL #3 contains four strains of Lactobacillus, three Bifidobacterium species, Streptococcus salivarius subsp. thermophillus | Treatment | Yes | Score 3 out of 4 (Moderate) | The use of probiotics is useful, and the authors suggested it in routine clinical care. | United States |
| Steed, et al., 2010 [45] | IBD: Crohn’s disease; sample size = 35 | Bifidobacterium longum and Synergy 1 which contains Orafti, Tienen, Belgium | Treatment | Yes | Score 4 out of 4 (High) | Effective in improving clinical symptoms in patients with active Crohn’s disease. | Scotland |
| Tomasz, et al., 2014 [46] | Pouchitis 4; sample size = 43 | Lactobacillus acidophillus, L. delbrueckii subsp. bulgaricus, and Bifidobacterium bifidus | Prevention | Yes | Score 4 out of 4 (High) | Long-term use of probiotics is safe and can be an effective method of preventing pouchitis 3. | Poland |
| Tongtawee, et al., 2015 [47] | Helicobacter pylori; sample size = 200 | Lactobacillus delbrueckii subsp. bulgaricus and Streptococcus thermophillus | Treatment | Yes | Score 4 out of 4 (High) | Pretreatment with probiotic containing yogurt can potentiate the effects of triple therapy for Helicobacter pylori. | Italy |
| Tursi, et al., 2010 [48] | IBD: UC; sample size = 144 | VSL #3 consists of Lactobacillus casei, L. plantarum, L. acidophilus, L. bulgaricus, Bifidobacterium longuum, B. breve, B. infantis, and Streptococcus salivarius sub-spp. Thermophillus | Treatment | Yes | Score 4 out of 4 (High) | High potency probiotic mixture supplementation is safe and improves rectal bleeding and reduce remission in relapsing UC patients after 8 weeks of treatment. | Thailand |
| Venturi, et al., 1999 [49] | IBD: UC; sample size = 20 | VSL #3 consists of Lactobacillus casei, L. plantarum, L. acidophilus, L. bulgaricus, Bifidobacterium longuum, B. breve, B. infantis, and Streptococcus salivarius sub-spp. Thermophillus | Treatment | Yes | Score 3 out of 4 (Moderate) | Intake of VSL #3 preparation enhances the concentrations of some strains of protective bacteria in the intestinal microflora. | Italy |
| Yilmaz, et al., 2019 [50] | IBDs 2; sample size = 45 | Kefir, a cultured, fermented beverage, which contains Lactobacillus bacteria | Treatment | Yes | Score 3 out of 4 (Moderate) | Consumptions of kefir has short term effects on improving the quality of life of patients. | Turkey |
| Yoshimatsu, et al., 2015 [51] | IBD: UC; sample size = 46 | Streptococcus faecalis (lactomin), Clostridium butyricum, and Bacillusmesentericus | Prevention of relapse | Yes | Score 3 out of 4 (Moderate) | Probiotics may be effective for maintaining clinical remission in patients with quiescent UC. | Japan |
| Ziemniak, 2006 [52] | Chronic gastritis, or duodenal ulcer caused by Helicobacter pylori; sample size = 641 | Lacidofil containing Lactobacillus acidophilus and Lactobacillus rhamnosus, as an adjuvant therapy with antibiotics and proton pump inhibitor (PPI) | Treatment | Yes | Score 4 out of 4 (High) | Lacidofil increases the efficacy of clarithromycin and amoxicillin and also reduces complications of antibiotic therapy. | Poland |
| Zocco, et al., 2006 [53] | IBD: UC; sample size = 187 | Lactobacillus GG | Treatment and prevention of remissions | Yes | Score 4 out of 4 (High) | Lactobacillus GG is effective and safe for maintaining ulcerative colitis remission and could be a good therapeutic alternative. | Italy |
| Zwolinsk, et al., 2009 [54] | IBD: UC; sample size = 101, of which 56 had active phase of UC, 33 non-active phase of UC, and 12 IBS controls | Lacidofil, containing two well-characterized strains of Lactobacillus: L. helveticus R-52 and L. rhamnosus R-11. | Treatment | Yes | Score 4 out of 4 (High) | Probiotic therapy is beneficial in counteracting the effects of delayed healing of trinitrobenzene sulfonic acid induced colitis caused by Candida. | Poland |
| Probiotics | Control Group | Risk Ratio | ||||
|---|---|---|---|---|---|---|
| Study | Events | Total | Events | Total | Weight (%) | M-H, Random, 95% CI |
| Alberda et al., 2018 [21] | 11 | 16 | 10 | 16 | 3.7 | 1.10 [0.67, 1.82] |
| Altun et al., 2019 [22] | 10 | 18 | 5 | 18 | 1.3 | 2.00 [0.85, 4.69] |
| Bjarnason et al. 2019 [23] | 4 | 77 | 4 | 70 | 0.5 | 0.91 [0.24, 3.50] |
| Fan et al., 2019 [25] | 7 | 21 | 9 | 19 | 1.6 | 0.70 [0.33, 1.52] |
| Hafer et al., 2007 [27] | 6 | 15 | 6 | 16 | 1.2 | 1.07 [0.44, 2.59] |
| Kato et al., 2004 [28] | 7 | 10 | 3 | 10 | 0.9 | 2.33 [0.83, 6.54] |
| Kruis et al., 1997 [30] | 18 | 50 | 29 | 53 | 4.7 | 0.66 [0.42, 1.03] |
| Kruis et al., 2004 [31] | 40 | 110 | 38 | 112 | 7.0 | 1.07 [0.75, 1.53] |
| Kuisma et al., 2003 [33] | 9 | 10 | 9 | 10 | 10.0 | 1.00 [0.75, 1.34] |
| Lahner et al., 2012 [34] | 27 | 30 | 20 | 22 | 21.8 | 0.99 [0.83, 1.18] |
| Lorea Baroja et al., 2007 [35] | 4 | 20 | 4 | 20 | 0.6 | 1.00 [0.29, 3.45] |
| Marteau et al., 2006 [36] | 30 | 47 | 21 | 49 | 6.0 | 1.49 [1.01, 2.20] |
| Matsuoka et al., 2018 [37] | 22 | 97 | 19 | 95 | 3.2 | 1.13 [0.66, 1.96] |
| Miruma et al., 2004 [39] | 7 | 20 | 11 | 16 | 2.1 | 0.51 [0.26, 1.01] |
| Palumbo et al., 2016 [41] | 3 | 30 | 5 | 30 | 0.5 | 0.60 [0.16, 2.29] |
| Shadnoush et al., 2015 [43] | 30 | 176 | 18 | 84 | 3.4 | 0.80 [0.47, 1.34] |
| Steed et al., 2010 [45] | 5 | 13 | 6 | 11 | 1.3 | 0.71 [0.29, 1.69] |
| Tomasz et al., 2014 [46] | 3 | 19 | 8 | 21 | 0.7 | 0.41 [0.13, 1.34] |
| Tongtawee et al., 2015 [47] | 62 | 98 | 60 | 96 | 16.3 | 1.01 [0.82, 1.26] |
| Tursi et al., 2010 [48] | 36 | 65 | 38 | 66 | 9.5 | 0.96 [0.71, 1.30] |
| Yilmaz et al., 2019 [50] | 11 | 23 | 9 | 23 | 2.2 | 1.22 [0.63, 2.38] |
| Yoshimatsu et al., 2015 [51] | 5 | 10 | 6 | 10 | 1.5 | 0.83 [0.37, 1.85] |
| Total (95% CI) | 975 | 867 | 100% | 0.99 [0.90, 1.09] | ||
| Total events | 357 | 338 | ||||
| Heterogeneity: Tau2 = 0.00; Chi2 = 22.43, df = 21 (p = 0.37); I2 = 6% | ||||||
| Test of overall effect Z = 0.18 (p = 0.85) | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitra, A.K.; Asala, A.F.; Malone, S.; Mridha, M.K. Effects of Probiotics in Adults with Gastroenteritis: A Systematic Review and Meta-Analysis of Clinical Trials. Diseases 2023, 11, 138. https://doi.org/10.3390/diseases11040138
Mitra AK, Asala AF, Malone S, Mridha MK. Effects of Probiotics in Adults with Gastroenteritis: A Systematic Review and Meta-Analysis of Clinical Trials. Diseases. 2023; 11(4):138. https://doi.org/10.3390/diseases11040138
Chicago/Turabian StyleMitra, Amal K., Adetoun F. Asala, Shelia Malone, and Malay Kanti Mridha. 2023. "Effects of Probiotics in Adults with Gastroenteritis: A Systematic Review and Meta-Analysis of Clinical Trials" Diseases 11, no. 4: 138. https://doi.org/10.3390/diseases11040138
APA StyleMitra, A. K., Asala, A. F., Malone, S., & Mridha, M. K. (2023). Effects of Probiotics in Adults with Gastroenteritis: A Systematic Review and Meta-Analysis of Clinical Trials. Diseases, 11(4), 138. https://doi.org/10.3390/diseases11040138