
Salvage Therapy with Second-Generation Inhibitors for FLT3 Mutated Acute Myeloid Leukemia: A Real-World Study by the CETLAM and PETHEMA Groups

 , , , , , , , , ,
on behalf of the CETLAM and PETHEMA Groupsadd
Show full author list
, , , , , , , , ,
on behalf of the CETLAM and PETHEMA Groupsadd
Show full author list
Simple Summary
Abstract
1. Introduction
2. Methods
3. Results
3.1. Patients and Treatment
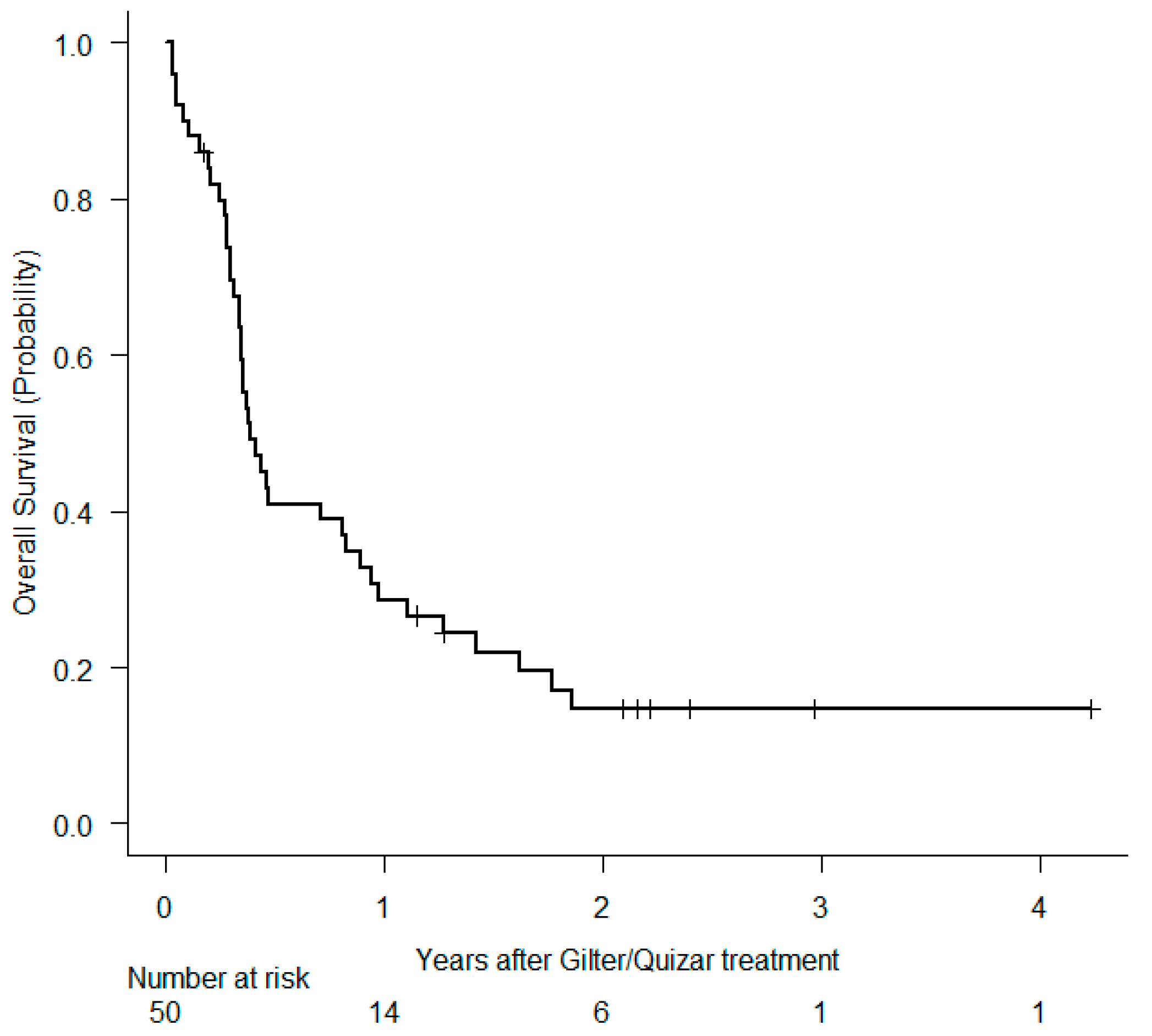
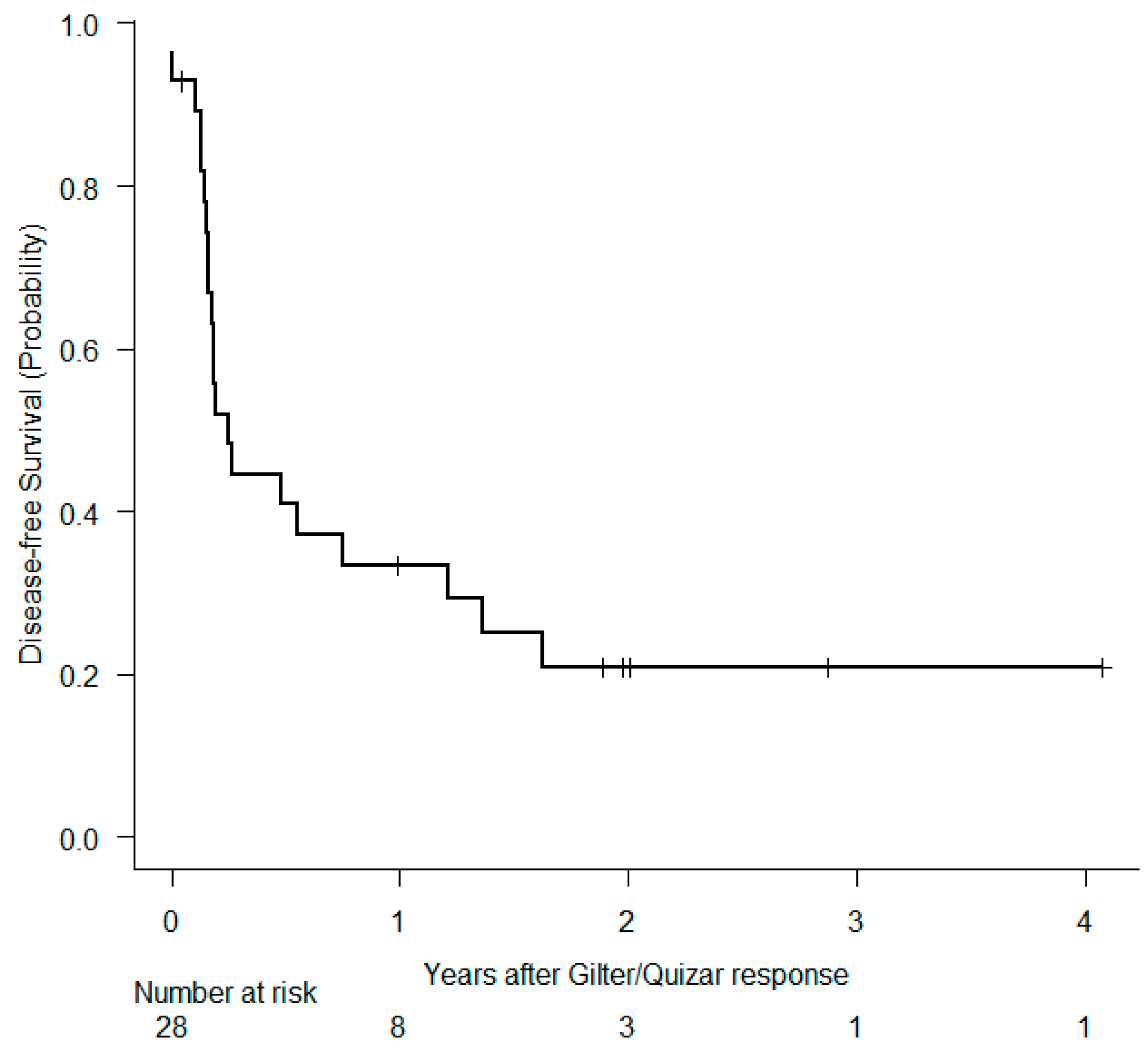
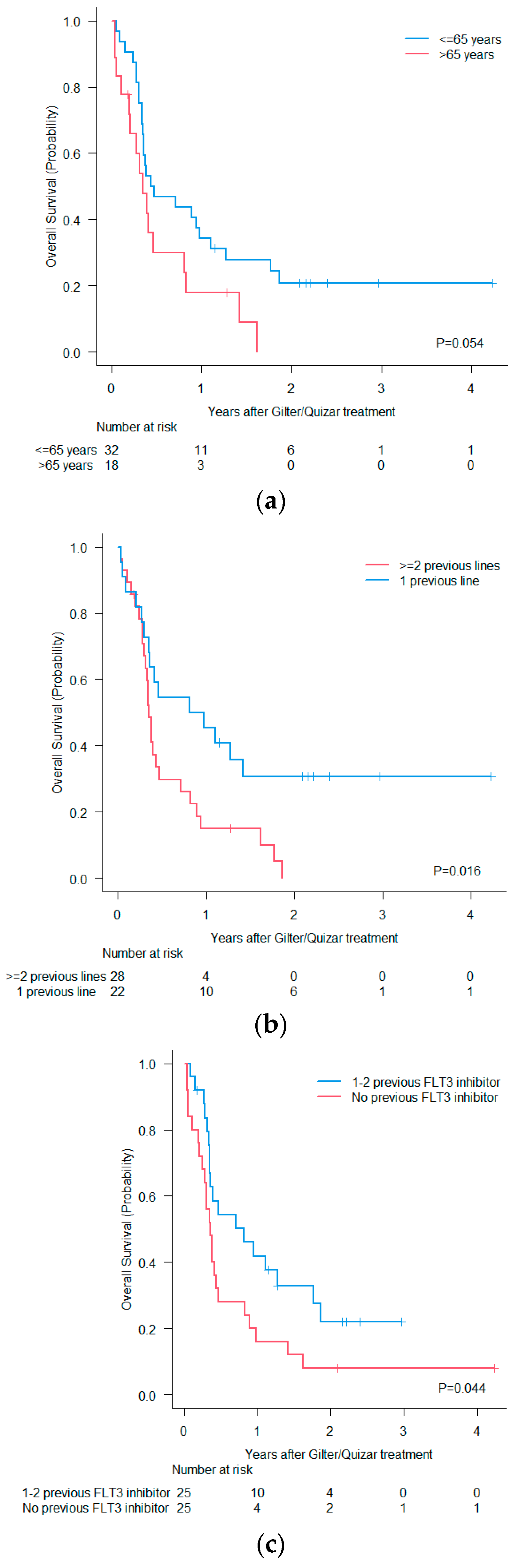
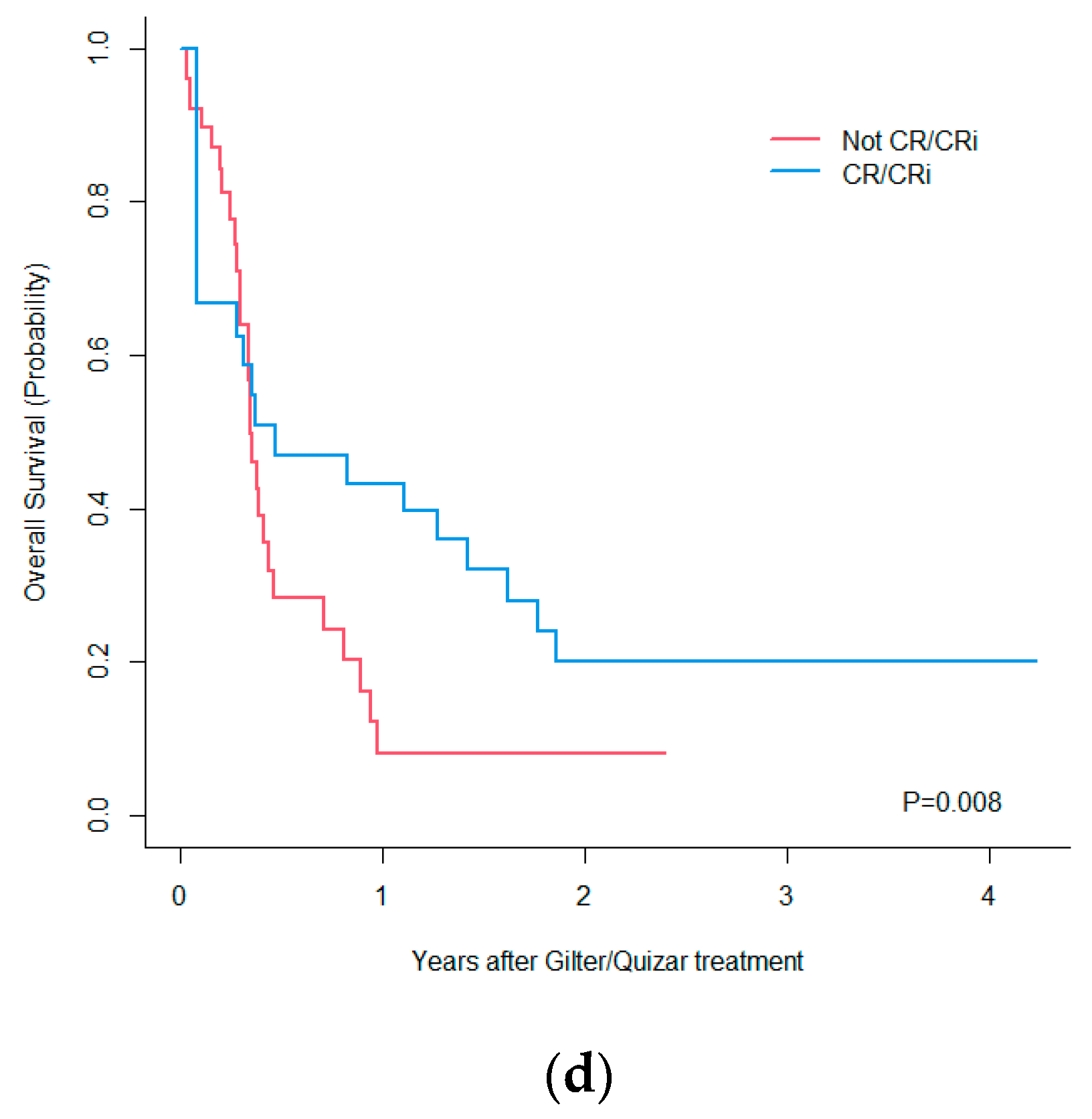
3.2. Outcomes
3.3. Toxicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ravandi, F.; Kantarjian, H.; Faderl, S.; Garcia-Manero, G.; O’Brien, S.; Koller, C.; Pierce, S.; Brandt, M.; Kennedy, D.; Cortes, J.; et al. Outcome of patients with FLT3-mutated acute myeloid leukemia in first relapse. Leuk. Res. 2010, 34, 752–756. [Google Scholar] [CrossRef]
- Cocciardi, S.; Dolnik, A.; Kapp-Schwoerer, S.; Rücker, F.G.; Lux, S.; Blätte, T.J.; Skambraks, S.; Krönke, J.; Heidel, F.H.; Schnöder, T.M.; et al. Clonal evolution patterns in acute myeloid leukemia with NPM1 mutation. Nat. Commun. 2019, 10, 2031. [Google Scholar] [CrossRef] [PubMed]
- Arber, D.A.; Orazi, A.; Hasserjian, R.P.; Borowitz, M.J.; Calvo, K.R.; Kvasnicka, H.M.; Wang, S.A.; Bagg, A.; Barbui, T.; Branford, S.; et al. International consensus classifications of myeloid neoplasms and acute leukemias: Integrating morphologic, clinical, and genomic data. Blood 2022, 140, 1200–1228. [Google Scholar] [CrossRef]
- Khoury, J.D.; Solary, E.; Abla, O.; Akkari, Y.; Alaggio, R.; Apperley, J.F.; Bejar, R.; Berti, E.; Busque, L.; Chan, J.K.C.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia 2022, 36, 1703–1719. [Google Scholar] [CrossRef] [PubMed]
- Döhner, H.; Wei, A.H.; Appelbaum, F.R.; Craddock, C.; DiNardo, C.D.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Godley, L.A.; Hasserjian, R.P.; et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood 2022, 140, 1345–1377. [Google Scholar] [CrossRef] [PubMed]
- Stone, R.M.; Mandrekar, S.J.; Sanford, B.L.; Laumann, K.; Geyer, S.; Bloomfield, C.D.; Thiede, C.; Prior, T.W.; Döhner, K.; Marcucci, G.; et al. Midostaurin plus Chemotherapy for Acute Myeloid Leukemia with a FLT3 Mutation. N. Engl. J. Med. 2017, 377, 454–464. [Google Scholar] [CrossRef]
- Larson, R.A.; Mandrekar, S.J.; Huebner, L.J.; Sanford, B.L.; Laumann, K.; Geyer, S.; Bloomfield, C.D.; Thiede, C.; Prior, T.W.; Döhner, K.; et al. Midostaurine reduces relapse in FLT3-mutant acute myeloid leukemia: The Alliance CALGB 10603/RATIFY trial. Leukemia 2021, 35, 2539–2551. [Google Scholar] [CrossRef]
- Erba, H.P.; Montesinos, P.; Kim, H.J.; Patkowska, E.; Vrhovac, R.; Žák, P.; Wang, P.N.; Mitov, T.; Hanyok, J.; Kamel, Y.M.; et al. Quizartinib plus chemotherapy in newly diagnosed patients with FLT3-internal-tandem-duplication-positive acute myeloid leukaemia (QuANTUM-First): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2023, 401, 1571–1583. [Google Scholar] [CrossRef]
- Wang, E.S.; Montesinos, P.; Minden, M.D.; Lee, J.H.; Heuser, M.; Naoe, T.; Chou, W.C.; Laribi, K.; Esteve, J.; Altman, J.K.; et al. Phase 3 trial of gilteritinib plus azacitidine vs azacitidine for newly diagnosed FLT3mut+ AML ineligible for intensive chemotherapy. Blood 2022, 140, 1845–1857. [Google Scholar] [CrossRef]
- Daver, N.; Perl, A.E.; Maly, J.; Levis, M.; Ritchie, E.; Litzow, M.; McCloskey, J.; Smith, C.C.; Schiller, G.; Bradley, T.; et al. Venetoclax Plus Gilteritinib for FLT3-Mutated Relapsed/Refractory Acute Myeloid Leukemia. J. Clin. Oncol. 2022, 40, 4048–4059. [Google Scholar] [CrossRef]
- Ma, J.; Zhao, S.; Qiao, X.; Knight, T.; Edwards, H.; Polin, L.; Kushner, J.; Dzinic, S.H.; White, K.; Wang, G.; et al. Inhibition of Bcl-2 Synergistically Enhances the Antileukemic Activity of Midostaurin and Gilteritinib in Preclinical Models of FLT3-Mutated Acute Myeloid Leukemia. Clin. Cancer Res. 2019, 25, 6815–6826. [Google Scholar] [CrossRef] [PubMed]
- Short, N.J.; Daver, N.; Dinardo, C.D.; Kadia, T.; Nasr, L.F.; Macaron, W.; Yilmaz, M.; Borthakur, G.; Montalban-Bravo, G.; Garcia-Manero, G.; et al. Azacitidine, Venetoclax, and Gilteritinib in Newly Diagnosed and Relapsed or Refractory FLT3-Mutated AML. J. Clin. Oncol. 2024, 42, 1499–1508. [Google Scholar] [CrossRef]
- Perl, A.E.; Larson, R.A.; Podoltsev, N.A.; Strickland, S.; Wang, E.S.; Atallah, E.; Schiller, G.J.; Martinelli, G.; Neubauer, A.; Sierra, J.; et al. Follow-up of patients with R/R FLT3-mutation-positive AML treated with gilteritinib in the phase 3 ADMIRAL trial. Blood 2022, 139, 3366–3375. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.E.; Khaled, S.; Martinelli, G.; Perl, A.E.; Ganguly, S.; Russell, N.; Krämer, A.; Dombret, H.; Hogge, D.; Jonas, B.A.; et al. Quizartinib versus salvage chemotherapy in relapsed or refractory FLT3-ITD acute myeloid leukaemia (QuANTUM-R): A multicentre, randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 984–997. [Google Scholar] [CrossRef] [PubMed]
- Mohebbi, A.; Shahriyary, F.; Farrokhi, V.; Bandar, B.; Saki, N. A systematic review of second-generation FLT3 inhibitors for treatment of patients with relapsed/refractory acute myeloid leukemia. Leuk. Res. 2024, 141, 107505. [Google Scholar] [CrossRef]
- Travaglini, S.; Gurnari, C.; Ottone, T.; Voso, M.T. Advances in the pathogenesis of FLT3 -mutated acute myeloid leukemia and targeted treatments. Curr. Opin. Oncol. 2024, 36, 569–576. [Google Scholar] [CrossRef]
- Daver, N.; Schlenk, R.F.; Russell, N.H.; Levis, M.J. Targeting FLT3 mutations in AML: Review of current knowledge and evidence. Leukemia 2019, 33, 299–312. [Google Scholar] [CrossRef]
- Larrosa-García, M.; Baer, M.R. FLT3 Inhibitors in Acute Myeloid Leukemia: Current Status and Future Directions. Mol. Cancer Ther. 2017, 16, 991–1001. [Google Scholar] [CrossRef]
- Loschi, M.; Sammut, R.; Chiche, E.; Cluzeau, T. FLT3 Tyrosine Kinase Inhibitors for the Treatment of Fit and Unfit Patients with FLT3-Mutated AML: A Systematic Review. Int. J. Mol. Sci. 2021, 22, 5873. [Google Scholar] [CrossRef]
- Numan, Y.; Abdel Rahman, Z.; Grenet, J.; Boisclair, S.; Bewersdorf, J.P.; Collins, C.; Barth, D.; Fraga, M.; Bixby, D.L.; Zeidan, A.M.; et al. Gilteritinib clinical activity in relapsed/refractory FLT3 mutated acute myeloid leukemia previously treated with FLT3 inhibitors. Am. J. Hematol. 2022, 97, 322–328. [Google Scholar] [CrossRef]
- Dumas, P.Y.; Bertoli, S.; Bérard, E.; Largeaud, L.; Bidet, A.; Delabesse, E.; Leguay, T.; Leroy, H.; Gadaud, N.; Rieu, J.B.; et al. Real-World Outcomes of Patients with Refractory or Relapsed FLT3-ITD Acute Myeloid Leukemia: A Toulouse-Bordeaux DATAML Registry Study. Cancers 2020, 12, 2044. [Google Scholar] [CrossRef] [PubMed]
- Shimony, S.; Canaani, J.; Kugler, E.; Nachmias, B.; Ram, R.; Henig, I.; Frisch, A.; Ganzel, C.; Vainstein, V.; Moshe, Y.; et al. Gilteritinib monotherapy for relapsed/refractory FLT3 mutated acute myeloid leukemia: A real-world, multi-center, matched analysis. Ann. Hematol. 2022, 101, 2001–2010. [Google Scholar] [CrossRef] [PubMed]
- Dogu, M.H.; Tekgunduz, A.I.E.; Deveci, B.; Korkmaz, G.; Comert, M.; Sevindik, O.G.; Yokus, O.; Serin, I. Gilteritinib (XOSPATA®) in Turkey: Early Access Program Results. Mediterr. J. Hematol. Infect. Dis. 2023, 15, e2023031. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef]
- Common Terminology Criteria for Advers Events (CTACAE). Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 1 January 2021).
- Perrone, S.; Ottone, T.; Zhdanovskaya, N.; Molica, M. How acute myeloid leukemia (AML) escapes from FMS-related tyrosine kinase 3 (FLT3) inhibitors? Still an overrated complication? Cancer Drug Resist. 2023, 6, 223–238. [Google Scholar] [CrossRef]
- Perl, A.E.; Hosono, N.; Montesinos, P.; Podoltsev, N.; Martinelli, G.; Panoskaltsis, N.; Recher, C.; Smith, C.C.; Levis, M.J.; Strickland, S.; et al. Clinical outcomes in patients with relapsed/refractory FLT3-mutated acute myeloid leukemia treated with gilteritinib who received prior midostaurin or sorafenib. Blood Cancer J. 2022, 12, 84. [Google Scholar] [CrossRef]
- Perl, A.E.; Altman, J.K.; Cortes, J.; Smith, C.; Litzow, M.; Baer, M.R.; Claxton, D.; Erba, H.P.; Gill, S.; Goldberg, S.; et al. Selective inhibition of FLT3 by gilteritinib in relapsed or refractory acute myeloid leukaemia: A multicentre, first-in-human, open-label, phase 1–2 study. Lancet Oncol. 2017, 18, 1061–1075. [Google Scholar] [CrossRef]
- Dumas, P.Y.; Raffoux, E.; Bérard, E.; Bertoli, S.; Hospital, M.A.; Heiblig, M.; Desbrosses, Y.; Bonmati, C.; Pautas, C.; Lambert, J.; et al. Gilteritinib activity in refractory or relapsed FLT3-mutated acute myeloid leukemia patients previously treated by intensive chemotherapy and midostaurin: A study from the French AML Intergroup ALFA/FILO. Leukemia 2023, 37, 91–101. [Google Scholar] [CrossRef]
- Yilmaz, M.; Alfayez, M.; DiNardo, C.D.; Borthakur, G.; Kadia, T.M.; Konopleva, M.Y.; Loghavi, S.; Kanagal-Shamanna, R.; Patel, K.P.; Jabbour, E.J.; et al. Outcomes with sequential FLT3-inhibitor-based therapies in patients with AML. J. Hematol. Oncol. 2020, 13, 132. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Newly Diagnosis n = 50 | R/R Status n = 50 | ||
|---|---|---|---|
| Age | Median [range] | 61.5 [22–81] | 62.5 [25–81] |
| Age | ≤65 years | 34 (68%) | 32 (64%) |
| >65 years | 16 (32%) | 18 (36%) | |
| Sex | Male | 24 (48%) 26 (52%) | |
| Female | |||
| ECOG PS | 0 | 22/48 (46%) | 17/48 (35%) |
| 1 | 21/48 (44%) | 20/48 (42%) | |
| 2 | 4/48 (8%) | 10/48 (21%) | |
| 3 | 1/48 (2%) | 1/48 (2%) | |
| WBC, ×109/L | Median [range] | 21.7 [0.4–343.7] | 5.1 [0.1–140] |
| ELN 2017 classification | Wild-type NPM1 and FLT3-ITDhigh | 13/47 (28%) | 10/38 (31%) |
| Mutated NPM1 without FLT3-ITD or with FLT3-ITDlow | 11/47 (23%) | 5/38 (18%) | |
| Mutated NPM1 and FLT3-ITDhigh | 10/47 (21%) | 12/38 (25%) | |
| Wild-type NPM1 without FLT3-ITD or with FLT3-ITDlow | 9/47 (19%) | 7/38 (13%) | |
| Mutated RUNX1 | 1/47 (2%) | 1/38 (3%) | |
| t(6;9)(p23;q34.1); DEK-NUP214 | 1/47 (2%) | 1/38 (3%) | |
| t(8;21)(q22;q22.1); RUNX1-RUNX1T1 | 1/47 (2%) | 1/38 (3%) | |
| inv(3)(q21.3q26.2) or t(3;3)(q21.3;q26.2);GATA2,MECOM (EVI1) | 1/47 (2%) | 1/38 (3%) | |
| ELN 2017 risk stratification | Favorable | 10 (20%) | 4/44 (9%) |
| Intermediate | 21 (42%) | 21/44 (48%) | |
| Adverse | 19 (38%) | 19/44 (43%) | |
| FLT3-ITD | Negative | 14 (28%) | 9/45 (20%) |
| Positive | 36 (72%) | 36/45 (80%) | |
| Allelic Ratio FLT3-ITD | <0.5 | 11/36 (31%) | 12/34 (35%) |
| ≥0.5 | 25/36 (69%) | 22/34 (65%) | |
| NPM1 | Negative | 29 (58%) | 23/41 (56%) |
| Positive | 21 (42%) | 18/41 (44%) | |
| FLT3-TKD | Negative | 37/46 (80%) | 31/39 (79%) |
| Positive | 9/46 (20%) | 8/39 (21%) | |
| Bilirubin, mg/dL | Median [range] | 0.58 [0.25–3] | 0.44 [0.17–6] |
| Creatinine, mg/dL | Median [range] | 0.88 [0.46–2.99] | 0.76 [0.42–1.36] |
| LDH, U/L | Median [range] | 528 [155–3795] | 285 [98–10,840] |
| Urates, mg/dL | Median [range] | 4.8 [1.2–25] | 3.9 [1–10] |
| Clonal evolution | Yes | NA | 8/37 (22%) |
| No | NA | 29/37 (78%) | |
| Univariate Analisys | ||||
|---|---|---|---|---|
| Variable | n |
OS, HR (95% CI) | p | |
| Age R/R | Continuous | 50 | 1.021 (0.996–1.047) | 0.096 |
| ≤65 years | 32 | Reference | 0.058 | |
| >65 years | 18 | 1.863 (0.979–3.547) | ||
| Sex | Female | 26 | Reference | 0.581 |
| Male | 24 | 1.189 (0.644–2.195) | ||
| ECOG PS R/R | 0–1 | 37 | Reference | 0.447 |
| ≥2 | 11 | 1.324 (0.642–2.728) | ||
| WBC count R/R | Continuous | 48 | 1.015 (1.006–1.024) | 0.001 |
| <10 × 109/L | 32 | Reference | 0.001 | |
| ≥10 × 109/L | 16 | 3.241 (1.622–6.479) | ||
| Type of R/R | Relapse | 27 | Reference | 0.331 |
| Refractory | 23 | 1.358 (0.733–2.514) | ||
| ELN 17 risk stratification | Favorable/Intermediate | 25 | Reference | 0.157 |
| Adverse | 19 | 1.612 (0.832–3.121) | ||
| FLT3-ITDmut | Negative | 9 | Reference | 0.797 |
| Positive | 36 | 1.115 (0.489–2.541) | ||
| Allelic ratio FLT3-ITD | Continuous | 32 | 1.149 (0.872–1.515) | 0.323 |
| <0.5 | 12 | Reference | 0.873 | |
| ≥0.5 | 22 | 0.939 (0.434–2.031) | ||
| FLT3-TKDmut | Negative | 31 | Reference | 0.426 |
| Positive | 8 | 1.412 (0.604–3.300) | ||
| NPM1 | Positive | 18 | Reference | 0.367 |
| Negative | 23 | 1.391 (0.679–2.848) | ||
| Previous FLT3i exposure | Yes | 25 | Reference | 0.048 |
| No | 25 | 1.872 (1.005–3.487) | ||
| Number of prior therapies | 1 | 22 | Reference | 0.019 |
| ≥2 | 28 | 2.185 (1.138–4.196) | ||
| Previous Allo-SCT | No | 38 | Reference | 0.612 |
| Yes | 12 | 1.203 (0.589–2.456) | ||
| Subsequent Allo-SCT | No | 40 | 2.028 (0.758–5.422) | 0.159 |
| Yes | 10 | Reference | ||
| CR/CRi after Gilter/Quizar | No | 30 | 3.727 (1.497–9.276) | 0.008 |
| Yes | 20 | Reference | ||
| ORR post Gilter/Quizar | No | 22 | 1.568 (0.774–3.176) | 0.212 |
| Yes | 28 | Reference | ||
| Time from newly diagnosed AML to Gilter/Quizar | Continuous | 50 | 1.015 (0.987–1.043) | 0.310 |
| ≥12 months | 22 | Reference | 0.971 | |
| <12 months | 28 | 1.012 (0.544–1.880) | ||
| Multivariable Analisys | ||||
| Factor | n | OS, HR (95% CI) | p | |
| Age at R/R (increase risk per year) | 48 | 1.035 (1.008–1.063) | 0.011 | |
| WBC count at R/R (increase risk per 1 × 109/L) | 48 | 1.013 (1.004–1.022) | 0.006 | |
| Number of prior therapies (>1 line) | 48 | 2.225 (1.124–4.404) | 0.022 | |
| No CR/CRi after Gilter/Quizar | 48 | 5.170 (1.999–13.638) | 0.001 | |
| Any Grade | Grade ≥ 3 | FLT3i Discontinuation | Dose Reduction | |
|---|---|---|---|---|
| Febrile neutropenia | 21/49 (43%) | 15/15 | 8/21 | 4/21 |
| Liver toxicity | 10/49 (20%) | 3/6 | 2/10 | 1/10 |
| QTc interval prolongation | 7/49 (14%) | 2/7 | 2/7 | 4/7 |
| Myelotocicity | 3/49 (6%) | 3 | 1/3 | 1/3 |
| Rash | 2/49 (0.4%) | 0 | 0 | 0 |
| Sweet and Differentiation syndrome | 1/49 (0.2%) | 0 | 0 | 0 |
| Pulmonary edema | 1/49 (0.2%) | 1/1 | 0 | 0 |
| Syncope | 1/49 (0.2%) | 1/1 | 1/1 | 0 |
| Diarrhea | 1/49 (0.2%) | 1/1 | 0 | 0 |
| VVZ infection | 1/49 (0.2%) | 0 | 0 | 0 |
| Real-World Data | n | Age, Years (Range) | Prior FLT3i Exposure (%) | Number of Prior Therapies | Duration of Gilteritinib | CR (%) | Median OS (Months) | SAE | Mortality at 30 and 60 Days (%) | Prognostic Factors OS |
|---|---|---|---|---|---|---|---|---|---|---|
| Numan Y et al. Am. J Hematol. 2022 [20] | 113 * | 58.3 (18–92) | 100 | NA | 4.6 months (0–25) | 22.1 | 7 (SD ± 7) | NA | NA | Achieve CR Underwent SCT |
| Dumas PY et al. Leukemia. 2023 [21] ** | 140 | 65.2 (23.1–86.1) | 50 | 29.3% (≥2) | NA | 16.9 | 6.4 (IQR, 3.2–14.7) | Thrombocytopenia (51.4%), neutropenia (48.9%), anemia (40.3%). | 5.0 and 12.9 | Female gender Adverse cytogenetic risk Underwent SCT |
| Shimony S et al. Ann Hematol. 2022 [22] | 25 | 61 (IQR1–3, 47–73) | 40 | 2 (1–3) | 2 cycles (1–34) | 48 | 8 (0–16.2) | Thrombocytopenia (20%), hepatic (24%) | 8.0 and 28.0 | Achieve CR Prior IC |
| Dogu MH et al. Mediterr J Hematol Infect Dis. 2023 [23] | 17 | 55 (27–73) | 41.1 | 1 (1–5) | 8.5 months (1–21) | 64.7 | 355.5 days (21–905) | Hypocalemia (41.2%), anemia (41.2%) | 5.9 and 11.8 | Febrile neutropenia Peripheral edema |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vives, S.; Quintela, D.; Morgades, M.; Cano-Ferri, I.; Serrano, A.; Acuña-Cruz, E.; Cervera, M.; Díaz-Beyá, M.; Vidriales, B.; Raposo-Puglia, J.Á.; et al. Salvage Therapy with Second-Generation Inhibitors for FLT3 Mutated Acute Myeloid Leukemia: A Real-World Study by the CETLAM and PETHEMA Groups. Cancers 2024, 16, 4028. https://doi.org/10.3390/cancers16234028
Vives S, Quintela D, Morgades M, Cano-Ferri I, Serrano A, Acuña-Cruz E, Cervera M, Díaz-Beyá M, Vidriales B, Raposo-Puglia JÁ, et al. Salvage Therapy with Second-Generation Inhibitors for FLT3 Mutated Acute Myeloid Leukemia: A Real-World Study by the CETLAM and PETHEMA Groups. Cancers. 2024; 16(23):4028. https://doi.org/10.3390/cancers16234028
Chicago/Turabian StyleVives, Susana, David Quintela, Mireia Morgades, Isabel Cano-Ferri, Alfons Serrano, Evelyn Acuña-Cruz, Marta Cervera, Marina Díaz-Beyá, Belén Vidriales, José Ángel Raposo-Puglia, and et al. 2024. "Salvage Therapy with Second-Generation Inhibitors for FLT3 Mutated Acute Myeloid Leukemia: A Real-World Study by the CETLAM and PETHEMA Groups" Cancers 16, no. 23: 4028. https://doi.org/10.3390/cancers16234028
APA StyleVives, S., Quintela, D., Morgades, M., Cano-Ferri, I., Serrano, A., Acuña-Cruz, E., Cervera, M., Díaz-Beyá, M., Vidriales, B., Raposo-Puglia, J. Á., Arnan, M., Garrido, A., Balerdi, A., Cabello, A. I., Herrera-Puente, P., Serrano, J., Coll, R., Tormo, M., López-Marín, J., ... Montesinos, P., on behalf of the CETLAM and PETHEMA Groups. (2024). Salvage Therapy with Second-Generation Inhibitors for FLT3 Mutated Acute Myeloid Leukemia: A Real-World Study by the CETLAM and PETHEMA Groups. Cancers, 16(23), 4028. https://doi.org/10.3390/cancers16234028