
Advantage of First-Line Therapeutic Drug Monitoring-Driven Use of Infliximab for Treating Acute Intestinal and Liver GVHD in Children: A Prospective, Single-Center Study
 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Definitions and Endpoints
2.3. Infliximab Administration and TDM
2.4. Analysis of Cytokines and Chemokines
2.5. Statistical Analysis
3. Results
3.1. Patient and Disease Characteristics
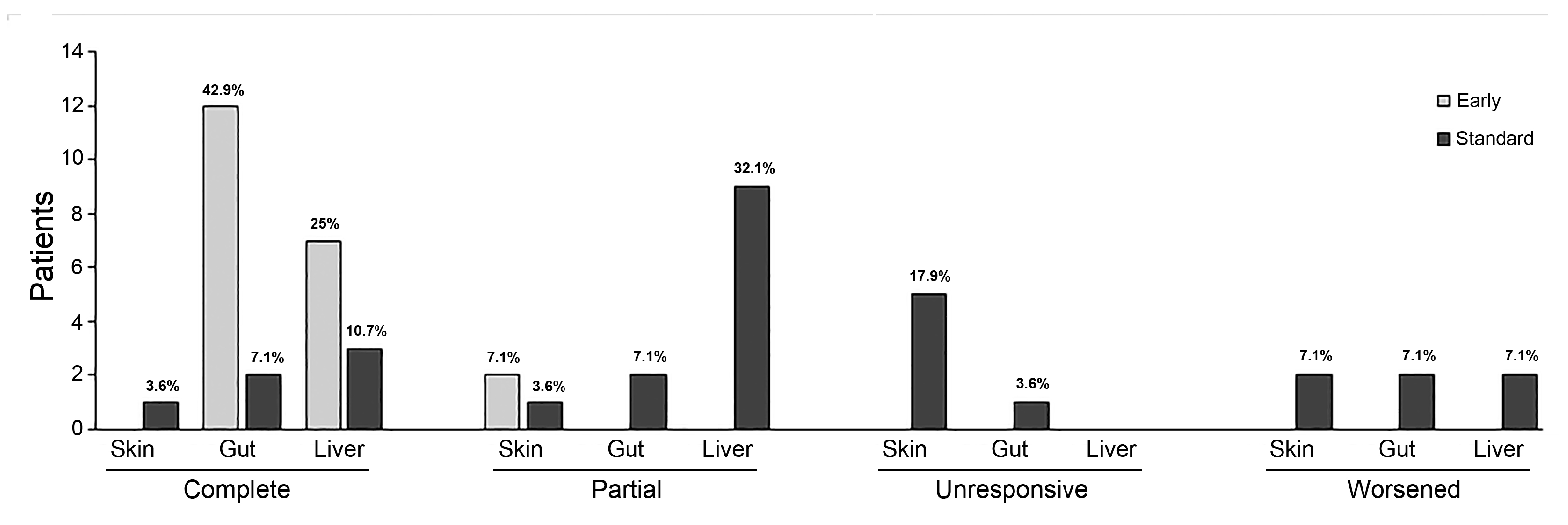
3.2. GVHD and Treatment Response
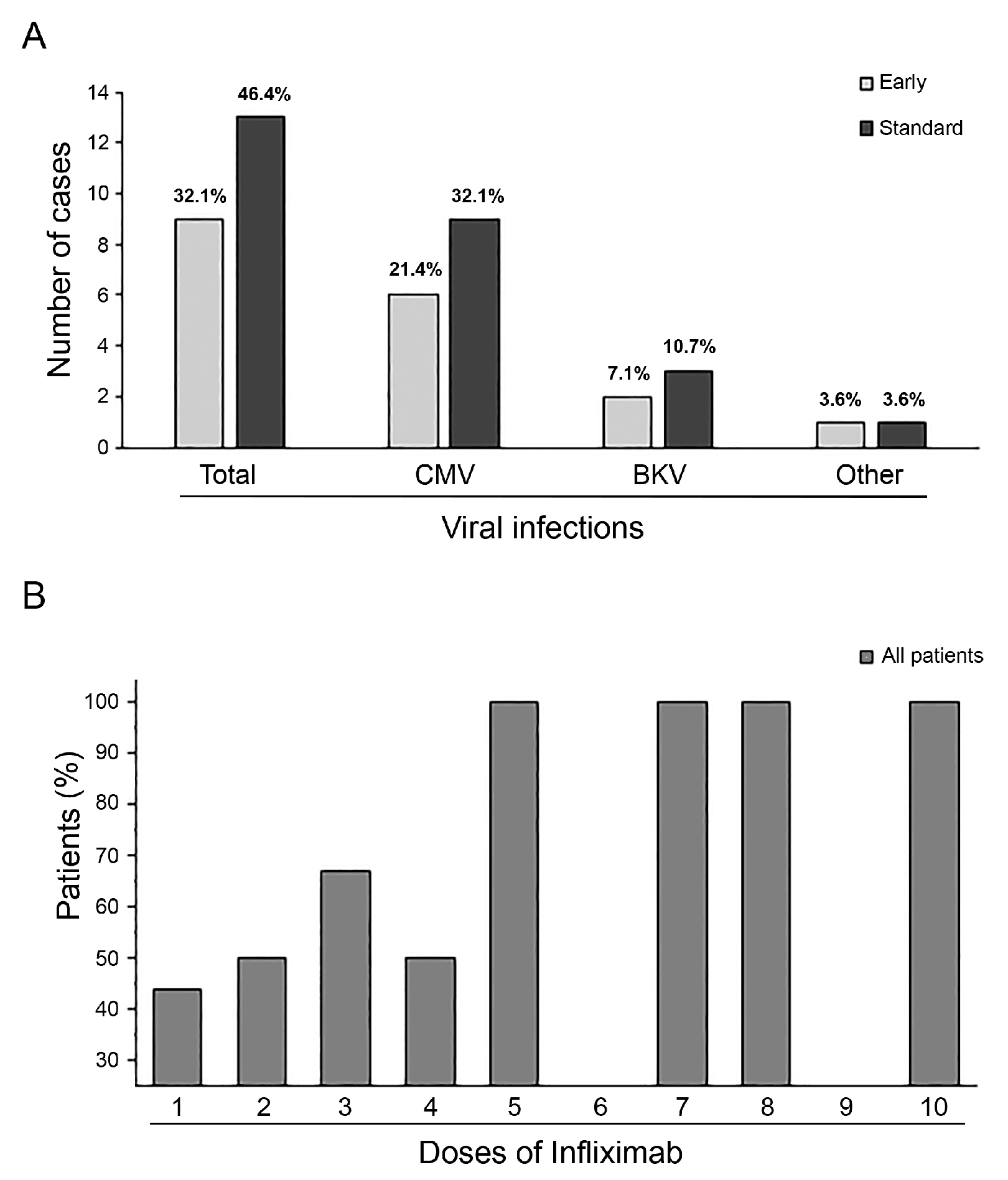
3.3. Adverse Effects and Infections
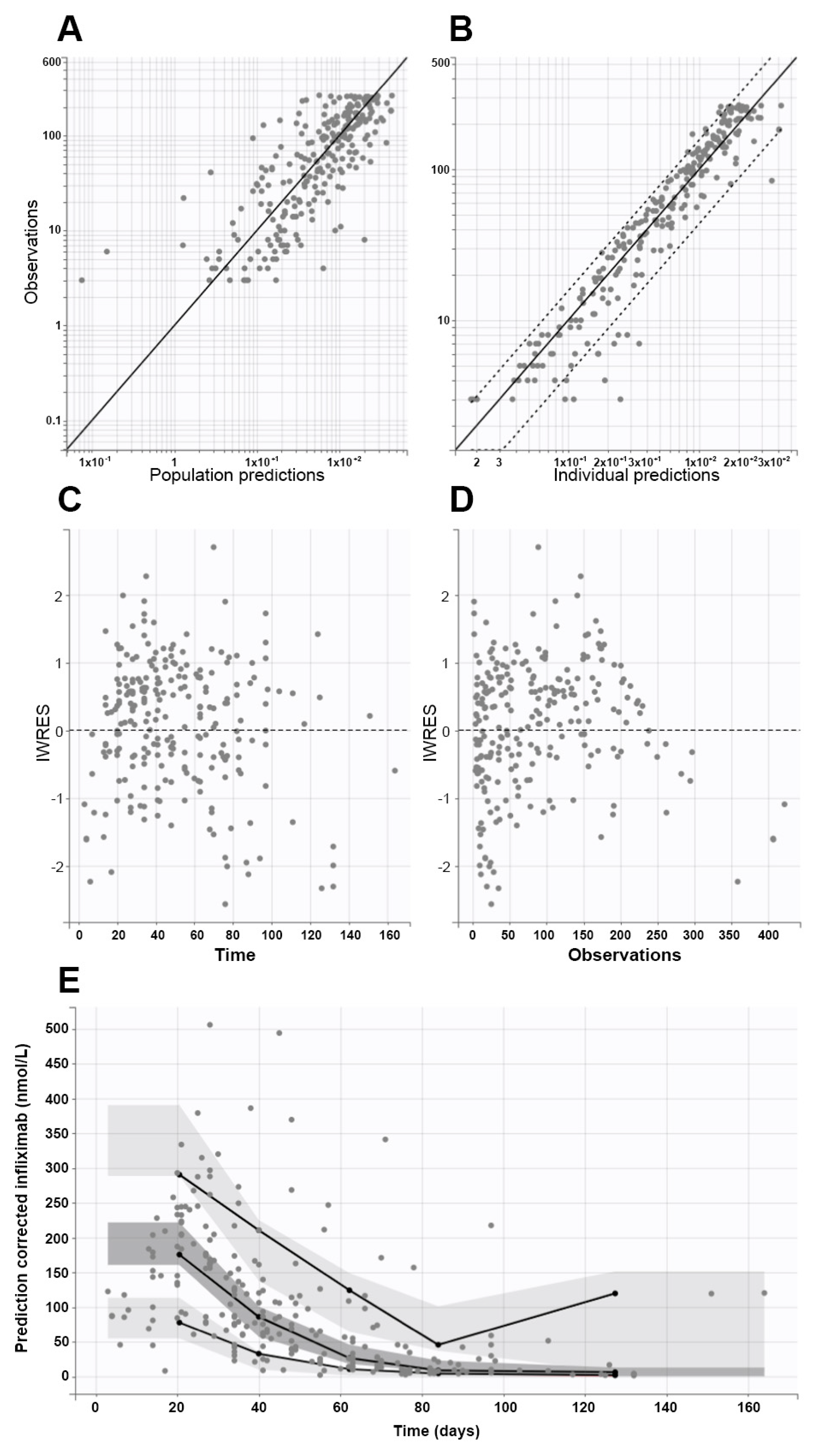
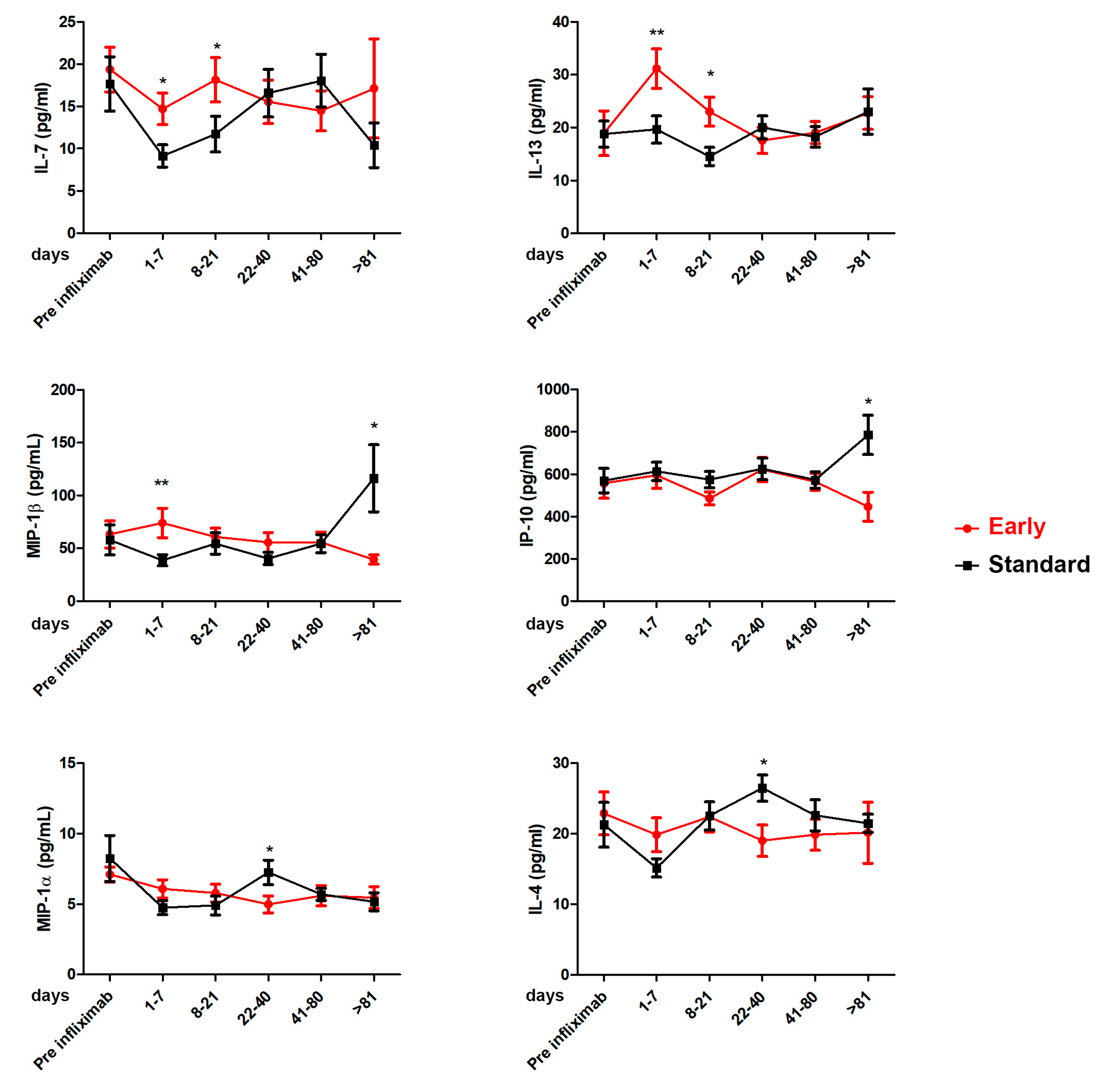
3.4. Infliximab Pharmacokinetic and Cytokines Evaluations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Greinix, H.T.; Eikema, D.J.; Koster, L.; Penack, O.; Yakoub-Agha, I.; Montoto, S.; Chabannon, C.; Styczynski, J.; Nagler, A.; Robin, M.; et al. Improved outcome of patients with graft-versus-host disease after allogeneic hematopoietic cell transplantation for hematologic malignancies over time: An EBMT mega-file study. Haematologica 2022, 107, 1054–1063. [Google Scholar] [CrossRef] [PubMed]
- Pasquini, M.; Wang, Z.; Horowitz, M.M.; Gale, R.P. 2013 report from the Center for International Blood and Marrow Transplant Research (CIBMTR): Current uses and outcomes of hematopoietic cell transplants for blood and bone marrow disorders. Clin. Transpl. 2013, 22, 187–197. [Google Scholar]
- Khoury, H.J.; Wang, T.; Hemmer, M.T.; Alousi, A.; Cutler, C.; Aljurf, M.; Antin, J.H.; Ayas, M.; Battiwalla, M.; Cahn, J.Y.; et al. Improved survival after acute graft-versus-host disease diagnosis in the modern era. Haematologica 2017, 102, 958–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gooptu, M.; Antin, J.H. GVHD Prophylaxis 2020. Front. Immunol. 2021, 12, 605726. [Google Scholar] [CrossRef]
- Garnett, C.; Apperley, J.F.; Pavlů, J. Treatment and management of graft-versus-host disease: Improving response and survival. Ther. Adv. Hematol. 2013, 4, 366–378. [Google Scholar] [CrossRef] [Green Version]
- Mo, X.D.; Hong, S.D.; Zhao, Y.L.; Jiang, E.L.; Chen, J.; Xu, Y.; Sun, Z.M.; Zhang, W.J.; Liu, Q.F.; Liu, D.H.; et al. Basiliximab for steroid-refractory acute graft-versus-host disease: A real-world analysis. Am. J. Hematol. 2022, 97, 458–469. [Google Scholar] [CrossRef]
- Weisdorf, D.; Haake, R.; Blazar, B.; Miller, W.; McGlave, P.; Ramsay, N.; Kersey, J.; Filipovich, A. Treatment of moderate/severe acute graft-versus-host disease after allogeneic bone marrow transplantation: An analysis of clinical risk features and outcome. Blood 1990, 75, 1024–1103. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, G.A.; Varelias, A.; Vuckovic, S.; Le Texier, L.; Gartlan, K.H.; Zhang, P.; Thomas, G.; Anderson, L.; Boyle, G.; Cloonan, N.; et al. Addition of interleukin-6 inhibition with tocilizumab to standard graft-versus-host disease prophylaxis after allogeneic stem-cell transplantation: A phase 1/2 trial. Lancet Oncol. 2014, 15, 1451–1459. [Google Scholar] [CrossRef]
- Holler, E.; Kolb, H.J.; Hintermeier-Knabe, R.; Mittermüller, J.; Thierfelder, S.; Kaul, M.; Wilmanns, W. Role of tumor necrosis factor-alpha in acute graft-versus-host disease and complications following allogeneic bone marrow transplantation. Transplant. Proc. 1993, 25, 1234–1236. [Google Scholar]
- Holler, E.; Kolb, H.J.; Moller, A.; Kempeni, J.; Liesenfeld, S.; Pechumer, H.; Lehmacher, W.; Ruckdeschel, G.; Gleixner, B.; Riedner, C. Increased serum levels of tumor necrosis factor-alpha precede major complications of bone marrow transplantation. Blood 1990, 75, 1011–1016. [Google Scholar] [CrossRef] [Green Version]
- Pidala, J.; Kim, J.; Field, T.; McBride, A.; Kharfan-Dabaja, M.; Perkins, J.; Fernandez, H.; Perez, L.; Ayala, E.; Anasetti, C. Infliximab for managing steroid-refractory acute graft-versus-host disease. Biol. Blood Marrow Transplant. 2009, 15, 1116–1121. [Google Scholar] [CrossRef] [Green Version]
- Nygaard, M.; Andersen, N.S.; Moser, C.E.; Olesen, G.; Schjødt, I.M.; Heilmann, C.; Sengeløv, H. Evaluation of infliximab as second-line treatment of acute graft versus host disease -validating response on day 7 and 28 as predictors of survival. Bone Marrow Transplant. 2018, 53, 844–851. [Google Scholar] [CrossRef]
- Carlone, G.; Torelli, L.; Maestro, A.; Zanon, D.; Barbi, E.; Maximova, N. Pentaglobin®Efficacy in Reducing the Incidence of Sepsis and Transplant-Related Mortality in Pediatric Patients Undergoing Hematopoietic Stem Cell Transplantation: A Retrospective Study. J. Clin. Med. 2020, 9, 1592. [Google Scholar] [CrossRef] [PubMed]
- Bacigalupo, A.; Ballen, K.; Rizzo, D.; Giralt, S.; Lazarus, H.; Ho, V.; Apperley, J.; Slavin, S.; Pasquini, M.; Sandmaier, B.M.; et al. Defining the intensity of conditioning regimens: Working definitions. Biol. Blood Marrow Transplant. 2009, 15, 1628–1633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maximova, N.; Schillani, G.; Simeone, R.; Maestro, A.; Zanon, D. Comparison of Efficacy and Safety of Caspofungin Versus Micafungin in Pediatric Allogeneic Stem Cell Transplant Recipients: A Retrospective Analysis. Adv. Ther. 2017, 34, 1184–1199. [Google Scholar] [CrossRef]
- Lerner, K.; Kao, G.F.; Storb, R.; Buckner, C.D.; Clift, R.A.; Thomas, E.D. Histopathology of graft-vs-host reaction (GvHR) in human recipients of marrow from HLA-matched sibling donors. Transplant. Proc. 1974, 6, 367–371. [Google Scholar] [PubMed]
- Przepiorka, D.; Weisdorf, D.; Martin, P.; Klingemann, H.G.; Beatty, P.; Hows, J.; Thomas, E.D. 1994 Consensus conference on acute GVHD grading. Bone Marrow Transplant. 1995, 15, 825–828. [Google Scholar] [PubMed]
- Rowlings, P.A.; Przepiorka, D.; Klein, J.P.; Gale, R.P.; Passweg, J.R.; Henslee-Downey, P.J.; Cahn, J.Y.; Calderwood, S.; Gratwohl, A.; Socié, G.; et al. IBMTR Severity Index for grading acute graft-versus-host disease: Retrospective comparison with Glucksberg grade. Br. J. Haematol. 1997, 97, 855–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawitschka, A.; Lucchini, G.; Strahm, B.; Dalle, J.H.; Balduzzi, A.; Gibson, B.; Diaz De Heredia, C.; Wachowiak, J.; Dalissier, A.; Vettenranta, K.; et al. Pediatric acute graft-versus-host disease prophylaxis and treatment: Surveyed real-life approach reveals dissimilarities compared to published recommendations. Transpl. Int. 2020, 33, 762–772. [Google Scholar] [CrossRef] [Green Version]
- Verbeek, A.B.; Jansen, S.A.; von Asmuth, E.G.J.; Ippoliti, C.; de Lima, M.; Hosing, C.; Khouri, I.; Andersson, B.; Gajewski, J.; Donato, M.; et al. Clinical Features, Treatment, and Outcome of Pediatric Steroid Refractory Acute Graft-Versus-Host Disease: A Multicenter Study. Transplant. Cell Ther. 2022, 28, 600.e1–600.e9. [Google Scholar] [CrossRef]
- Couriel, D.; Saliba, R.; Hicks, K.; Ippoliti, C.; de Lima, M.; Hosing, C.; Khouri, I.; Andersson, B.; Gajewski, J.; Donato, M.; et al. Tumor necrosis factor-alpha blockade for the treatment of acute GVHD. Blood 2004, 104, 649–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobbe, G.; Schneider, P.; Rohr, U.; Fenk, R.; Neumann, F.; Aivado, M.; Dietze, L.; Kronenwett, R.; Hünerlitürkoglu, A.; Haas, R. Treatment of severe steroid refractory acute graft-versus-host disease with infliximab, a chimeric human/mouse antiTNFalpha antibody. Bone Marrow Transplant. 2001, 28, 47–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patriarca, F.; Sperotto, A.; Damiani, D.; Morreale, G.; Bonifazi, F.; Olivieri, A.; Ciceri, F.; Milone, G.; Cesaro, S.; Bandini, G.; et al. Infliximab treatment for steroid-refractory acute graft-versus-host disease. Haematologica 2004, 89, 1352–1359. [Google Scholar] [PubMed]
- Nogueira, M.C.; Azevedo, A.M.; Pereira, S.C.; Ferreira, J.L.; Lerner, D.; Lobo, A.M.; Tavares, R.C.; Tabak, D.G.; Lorenzi, N.; Renault, I.Z.; et al. Anti-tumor necrosis factor-a for the treatment of steroid-refractory acute graft-versus-host disease. Braz. J. Med. Biol. Res. 2007, 40, 1623–1629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yalniz, F.F.; Hefazi, M.; McCullough, K.; Litzow, M.R.; Hogan, W.J.; Wolf, R.; Alkhateeb, H.; Kansagra, A.; Damlaj, M.; Patnaik, M.M. Safety and Efficacy of Infliximab Therapy in the Setting of Steroid-Refractory Acute Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2017, 23, 1478–1484. [Google Scholar] [CrossRef] [Green Version]
- Alousi, A.M.; Weisdorf, D.J.; Logan, B.R.; Bolaños-Meade, J.; Carter, S.; Difronzo, N.; Pasquini, M.; Goldstein, S.C.; Ho, V.T.; Hayes-Lattin, B.; et al. Etanercept, mycophenolate, denileukin, or pentostatin plus corticosteroids for acute graft-versus-host disease: A randomized phase 2 trial from the Blood and Marrow Transplant Clinical Trials Network. Blood 2009, 114, 511–517. [Google Scholar] [CrossRef] [Green Version]
- Uberti, J.P.; Ayash, L.; Ratanatharathorn, V.; Silver, S.; Reynolds, C.; Becker, M.; Reddy, P.; Cooke, K.R.; Yanik, G.; Whitfield, J.; et al. Pilot trial on the use of etanercept and methylprednisolone as primary treatment for acute graft-versus-host disease. Biol. Blood Marrow Transplant. 2005, 11, 680–687. [Google Scholar] [CrossRef] [Green Version]
- Levine, J.E.; Paczesny, S.; Mineishi, S.; Braun, T.; Choi, S.W.; Hutchinson, R.J.; Jones, D.; Khaled, Y.; Kitko, C.L.; Bickley, D.; et al. Etanercept plus methylprednisolone as initial therapy for acute graft-versus-host disease. Blood 2008, 111, 2470–2475. [Google Scholar] [CrossRef]
- Couriel, D.R.; Saliba, R.; de Lima, M.; Giralt, S.; Andersson, B.; Khouri, I.; Hosing, C.; Ippoliti, C.; Shpall, E.J.; Champlin, R.; et al. A phase III study of infliximab and corticosteroids for the initial treatment of acute graft-versus-host disease. Biol. Blood Marrow Transplant. 2009, 15, 1555–1562. [Google Scholar] [CrossRef] [Green Version]
- Gatza, E.; Braun, T.; Levine, J.E.; Ferrara, J.L.; Zhao, S.; Wang, T.; Chang, L.; Harris, A.; Pawarode, A.; Kitko, C.; et al. Etanercept plus topical corticosteroids as initial therapy for grade one acute graft-versus-host disease after allogeneic hematopoietic cell transplantation. Biol. Blood Marrow Transplant. 2014, 20, 1426–1434. [Google Scholar] [CrossRef] [Green Version]
- Sleight, B.S.; Chan, K.W.; Braun, T.M.; Serrano, A.; Gilman, A.L. Infliximab for GVHD therapy in children. Bone Marrow Transpl. 2007, 40, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Cheuk, D.K.L.; Ha, S.Y.; Chiang, A.K.; Lee, T.L.; Ho, M.H.; Chan, G.C. Infliximab for steroid refractory or dependent gastrointestinal acute graft-versus-host disease in children after allogeneic hematopoietic stem cell transplantation. Pediatr. Transpl. 2012, 16, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.R.; Hsu, F.C.; Simkin, P.A.; Wener, M.H. Effect of tumour necrosis factor alpha antagonists on serum transaminases and viraemia in patients with rheumatoid arthritis and chronic hepatitis C infection. Ann. Rheum. Dis. 2003, 62, 1078–1082. [Google Scholar] [CrossRef] [PubMed]
- Bjornsson, E.S. Hepatotoxicity by drugs: The most common implicated agents. Int. J. Mol. Sci. 2016, 17, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.; Ziring, D.; Desai, S.; Kim, S.; Wong, M.; Korin, Y.; Braun, J.; Reed, E.; Gjertson, D.; Singh, R.R. TNFalpha blockade in human diseases: An overview of efficacy and safety. Clin. Immunol. 2008, 126, 13–30. [Google Scholar] [CrossRef] [Green Version]
- Salvana, E.M.; Salata, R.A. Infectious complications associated with monoclonal antibodies and related small molecules. Clin. Microbiol. Rev. 2009, 22, 274–290. [Google Scholar] [CrossRef] [Green Version]
- Kourbeti, I.S.; Ziakas, P.D.; Mylonakis, E. Biologic therapies in rheumatoid arthritis and the risk of opportunistic infections: A meta-analysis. Clin. Infect. Dis. 2014, 58, 1649–1657. [Google Scholar] [CrossRef]
- Wirk, B.; Wingard, J.R. Current approaches in antifungal prophylaxis in high risk hematologic malignancy and hematopoietic stem cell transplant patients. Mycopathologia 2009, 168, 299–311. [Google Scholar] [CrossRef]
- Post, M.J.; Lass-Floerl, C.; Gastl, G.; Nachbaur, D. Invasive fungal infections in allogeneic and autologous stem cell transplant recipients: A single-center study of 166 transplanted patients. Transpl. Infect. Dis. 2007, 9, 189–195. [Google Scholar] [CrossRef]
- Koldehoff, M.; Zakrzewski, J.L. Modern management of respiratory failure due to pulmonary mycoses following allogeneic hematopoietic stem-cell transplantation. Am. J. Hematol. 2005, 79, 158–163. [Google Scholar] [CrossRef]
- Marty, F.M.; Lee, S.J.; Fahey, M.M.; Alyea, E.P.; Soiffer, R.J.; Antin, J.H.; Baden, L.R. Infliximab use in patients with severe graft-versus-host disease and other emerging risk factors of non-Candida invasive fungal infections in allogeneic hematopoietic stem cell transplant recipients: A cohort study. Blood 2003, 102, 2768–2776. [Google Scholar] [CrossRef] [Green Version]
- Lai, H.Y.; Chou, T.Y.; Tzeng, C.H.; Lee, O.K. Cytokine profiles in various graft-versus-host disease target organs following hematopoietic stem cell transplantation. Cell Transplant. 2012, 21, 2033–2045. [Google Scholar] [CrossRef] [PubMed]
- Yi, T.; Chen, Y.; Wang, L.; Du, G.; Huang, D.; Zhao, D.; Johnston, H.; Young, J.; Todorov, I.; Umetsu, D.T.; et al. Reciprocal differentiation and tissue-specific pathogenesis of Th1, Th2, and Th17 cells in graft-versus-host disease. Blood 2009, 114, 3101–3112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serody, J.S.; Burkett, S.E.; Panoskaltsis-Mortari, A.; Ng-Cashin, J.; McMahon, E.; Matsushima, G.K.; Lira, S.A.; Cook, D.N.; Blazar, B.R. T-lymphocyte production of macrophage inflammatory protein-1alpha is critical to the recruitment of CD8(+) T cells to the liver, lung, and spleen during graft-versus-host disease. Blood 2000, 96, 2973–2980. [Google Scholar] [CrossRef] [PubMed]
- New, J.Y.; Li, B.; Koh, W.P.; Ng, H.K.; Tan, S.Y.; Yap, E.H.; Chan, S.H.; Hu, H.Z. T cell infiltration and chemokine expression: Relevance to the disease localization in murine graft-versus-host disease. Bone Marrow Transplant. 2002, 29, 979–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamarthée, B.; Malard, F.; Gamonet, C.; Bossard, C.; Couturier, M.; Renauld, J.C.; Mohty, M.; Saas, P.; Gaugler, B. Donor interleukin-22 and host type I interferon signaling pathway participate in intestinal graft-versus-host disease via STAT1 activation and CXCL10. Mucosal Immunol. 2016, 9, 309–321. [Google Scholar] [CrossRef] [Green Version]
- Piper, K.P.; Horlock, C.; Curnow, S.J.; Arrazi, J.; Nicholls, S.; Mahendra, P.; Craddock, C.; Moss, P.A. CXCL10-CXCR3 interactions play an important role in the pathogenesis of acute graft-versus-host disease in the skin following allogeneic stem-cell transplantation. Blood 2007, 110, 3827–3832. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.; Ahrens, R.; Osterfeld, H.; Noah, T.K.; Groschwitz, K.; Foster, P.S.; Steinbrecher, K.A.; Rothenberg, M.E.; Shroyer, N.F.; Matthaei, K.I.; et al. Interleukin-13 (IL-13)/IL-13 receptor alpha1 (IL-13Ralpha1) signaling regulates intestinal epithelial cystic fibrosis transmembrane conductance regulator channel-dependent Cl- secretion. J. Biol. Chem. 2011, 286, 13357–13369. [Google Scholar] [CrossRef] [Green Version]
- Thiant, S.; Yakoub-Agha, I.; Magro, L.; Trauet, J.; Coiteux, V.; Jouet, J.P.; Dessaint, J.P.; Labalette, M. Plasma levels of IL-7 and IL-15 in the first month after myeloablative BMT are predictive biomarkers of both acute GVHD and relapse. Bone Marrow Transplant. 2010, 45, 1546–1552. [Google Scholar] [CrossRef] [Green Version]
- Serody, J.S.; Cook, D.N.; Kirby, S.L.; Reap, E.; Shea, T.C.; Frelinger, J.A. Murine T lymphocytes incapable of producing macrophage inhibitory protein-1 are impaired in causing graft-versus-host disease across a class I but not class II major histocompatibility complex barrier. Blood 1999, 93, 43–50. [Google Scholar] [CrossRef]
- Ramalingam, S.; Siamakpour-Reihani, S.; Bohannan, L.; Ren, Y.; Sibley, A.; Sheng, J.; Ma, L.; Nixon, A.B.; Lyu, J.; Parker, D.C.; et al. A phase 2 trial of the somatostatin analog pasireotide to prevent GI toxicity and acute GVHD in allogeneic hematopoietic stem cell transplant. PLoS ONE 2021, 16, e0252995. [Google Scholar] [CrossRef] [PubMed]
- Kleiner, G.; Marcuzzi, A.; Zanin, V.; Monasta, L.; Zauli, G. Cytokine levels in the serum of healthy subjects. Mediators Inflamm. 2013, 2013, 434010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vande Casteele, N.; Oyamada, J.; Shimizu, C.; Best, B.M.; Capparelli, E.V.; Tremoulet, A.H.; Burns, J.C. Infliximab pharmacokinetics are influenced by intravenous immunoglobulin administration in patients with Kawasaki disease. Clin. Pharmacokinet. 2018, 57, 1593–1601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauman, L.E.; Xiong, Y.; Mizuno, T.; Minar, P.; Fukuda, T.; Dong, M.; Rosen, M.J.; Vinks, A.A. Improved population pharmacokinetic model for predicting optimized infliximab exposure in pediatric inflammatory bowel disease. Inflamm. Bowel Dis. 2020, 26, 429–439. [Google Scholar] [CrossRef]
- Dotan, I.; Ron, Y.; Yanai, H.; Becker, S.; Fishman, S.; Yahav, L.; Ben Yehoyada, M.; Mould, D.R. Patient factors that increase infliximab clearance and shorten half-life in inflammatory bowel disease: A population pharmacokinetic study. Inflamm. Bowel Dis. 2014, 20, 2247–2259. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CHARACTERISTICS | Early Infliximab Group | Standard Infliximab Group | p-Value |
|---|---|---|---|
| Infliximab-concomitant therapy, number (%): | |||
| Tacrolimus | 13 (93) | 14 (100) | 0.847 |
| MMF | 1 (7) | 2 (14) | 0.540 |
| Steroids | 10 (71) | 11 (78) | 0.827 |
| Ruxolitinib | 3 (21) | 0 | <0.001 * |
| Patients, number (%) | 14 (50) | 14 (50) | 1.000 |
| Sex (male/female), number (%) | 8 (57)/6 (43) | 8 (57)/6 (43) | 1.000 |
| Age at treatment, years, median (range) | 6.5 (0.6–17) | 8 (1.1–17) | 0.984 |
| Body mass index, kg/m2, median (range) | 17.36 (13.43–26.46) | 17.03 (13.24–27.97) | 0.222 |
| Primary disease, number (%): | |||
| Acute lymphoblastic leukemia | 3 (21) | 8 (57) | 0.091 |
| Acute myeloid leukemia | 4 (29) | 1 (7) | 0.094 |
| Myelodysplastic syndromes | 4 (29) | 2 (14) | 0.386 |
| Non-malignant | 3 (21) | 3 (22) | 1.000 |
| Transplant type, number (%): | |||
| HLA-identical sibling | 4 (29) | 1 (7) | 0.094 |
| Related haploidentical | 4 (29) | 3 (21) | 0.703 |
| Matched unrelated | 6 (42) | 10 (72) | 0.302 |
| Graft type, number (%): | |||
| Bone marrow | 8 (57) | 1 (7) | <0.001 * |
| Peripheral blood | 6 (43) | 13 (93) | 0.084 |
| Follow-up in survivors, months, median (range) | 3.75 (2.1–59) | 17.7 (7–35.8) | 0.004 * |
| Interval HSCT to aGVHD onset: | |||
| Median (range), days | 22.5 (9–93) | 15 (9–220) | 0.984 |
| >day + 100, number | 0 | 1 | <0.001 * |
| Maximum aGVHD grade, number (%): | |||
| 1 | 2 (14) | 0 | <0.001 * |
| 2 | 10 (72) | 4 (28) | 0.076 |
| 3 or 4 | 2 (14) | 10 (72) | 0.002 * |
| Total number of organs involved, number (%): | |||
| 1 | 8 (58) | 2 (14) | 0.018 * |
| 2 | 5 (35) | 8 (58) | 0.392 |
| 3 | 1 (7) | 4 (28) | 0.094 |
| Skin stage, number (%): | |||
| 0–1 | 1 (50) | 0 | <0.001 * |
| 2 | 1 (50) | 6 (67) | 0.007 * |
| 3–4 | 0 | 3 (33) | <0.001 * |
| Liver stage, number (%): | |||
| 0–1 | 2 (29) | 0 | <0.001 * |
| 2 | 5 (71) | 6 (43) | 0.762 |
| 3–4 | 0 | 8 (57) | <0.001 * |
| GI tract, number (%): | |||
| 0–1 | 2 (17) | 0 | <0.001 * |
| 2 | 8 (66) | 3 (43) | 0.091 |
| 3–4 | 2 (17) | 4 (57) | 0.386 |
| Other | 3 (21) | 6 (43) | 0.289 |
| Value | SE | RSE (%) | |
|---|---|---|---|
| Fixed effects | |||
| Vpop (L) | 3.433 | 0.336 | 9.79 |
| CLpop (L/day) | 0.146 | 0.014 | 9.26 |
| Standard deviation of the random effects | |||
| IIVV | 0.375 | 0.073 | 19.4 |
| IIVCL | 0.363 | 0.090 | 24.6 |
| IOVCL | 0.278 | 0.050 | 17.9 |
| Residual variability | |||
| Residual proportional error | 0.316 | 0.018 | 5.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maximova, N.; Nisticò, D.; Riccio, G.; Maestro, A.; Barbi, E.; Faganel Kotnik, B.; Marcuzzi, A.; Rimondi, E.; Di Paolo, A. Advantage of First-Line Therapeutic Drug Monitoring-Driven Use of Infliximab for Treating Acute Intestinal and Liver GVHD in Children: A Prospective, Single-Center Study. Cancers 2023, 15, 3605. https://doi.org/10.3390/cancers15143605
Maximova N, Nisticò D, Riccio G, Maestro A, Barbi E, Faganel Kotnik B, Marcuzzi A, Rimondi E, Di Paolo A. Advantage of First-Line Therapeutic Drug Monitoring-Driven Use of Infliximab for Treating Acute Intestinal and Liver GVHD in Children: A Prospective, Single-Center Study. Cancers. 2023; 15(14):3605. https://doi.org/10.3390/cancers15143605
Chicago/Turabian StyleMaximova, Natalia, Daniela Nisticò, Guglielmo Riccio, Alessandra Maestro, Egidio Barbi, Barbara Faganel Kotnik, Annalisa Marcuzzi, Erika Rimondi, and Antonello Di Paolo. 2023. "Advantage of First-Line Therapeutic Drug Monitoring-Driven Use of Infliximab for Treating Acute Intestinal and Liver GVHD in Children: A Prospective, Single-Center Study" Cancers 15, no. 14: 3605. https://doi.org/10.3390/cancers15143605