
Clinical and Cytogenetic Characterization of Early and Late Relapses in Patients Allografted for Myeloid Neoplasms with a Myelodysplastic Component

 , ,
, , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Cytogenetic and Fluorescence In Situ Hybridization (FISH) Analyses
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Patient, Disease and Transplant Characteristics
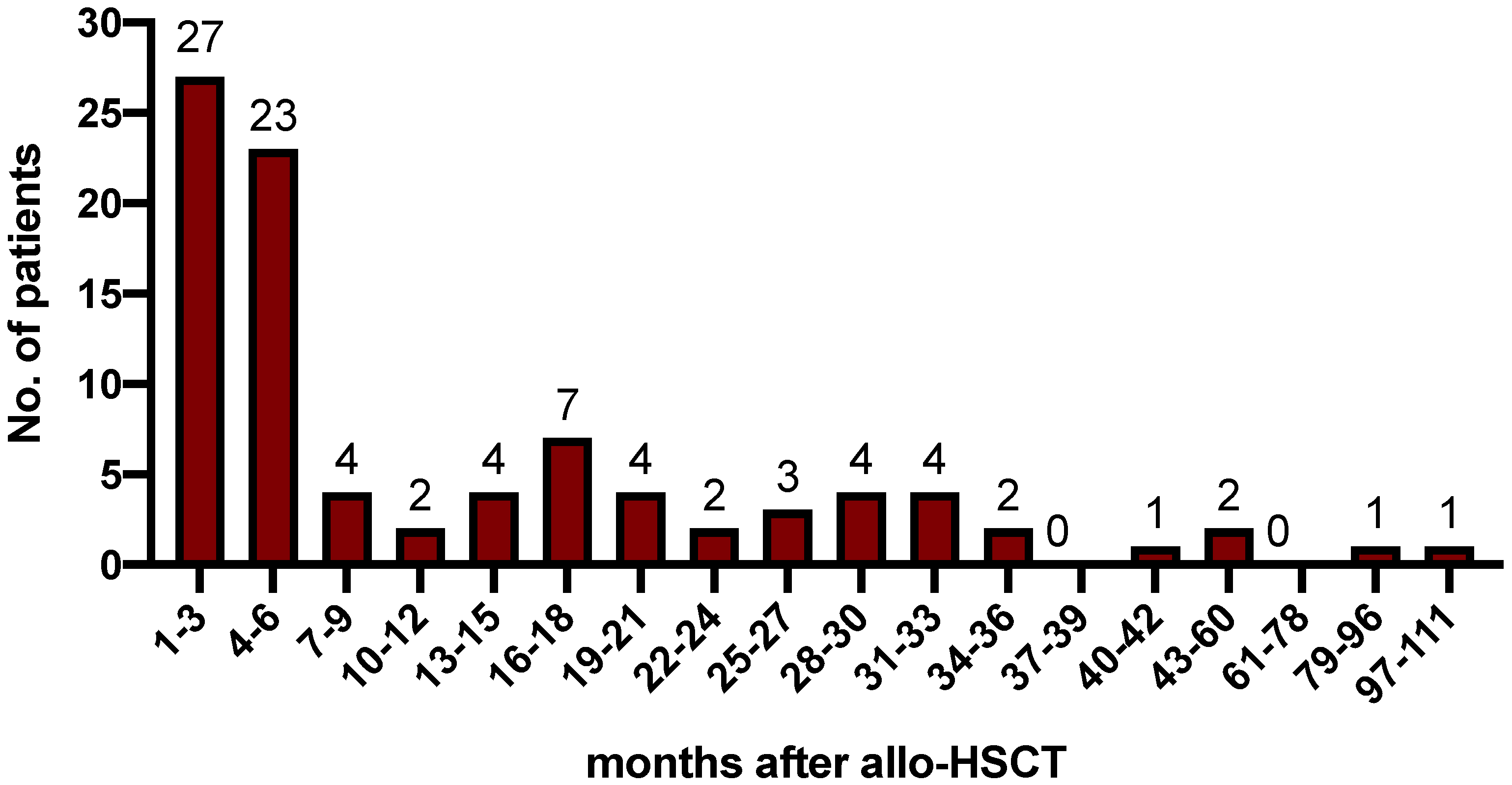
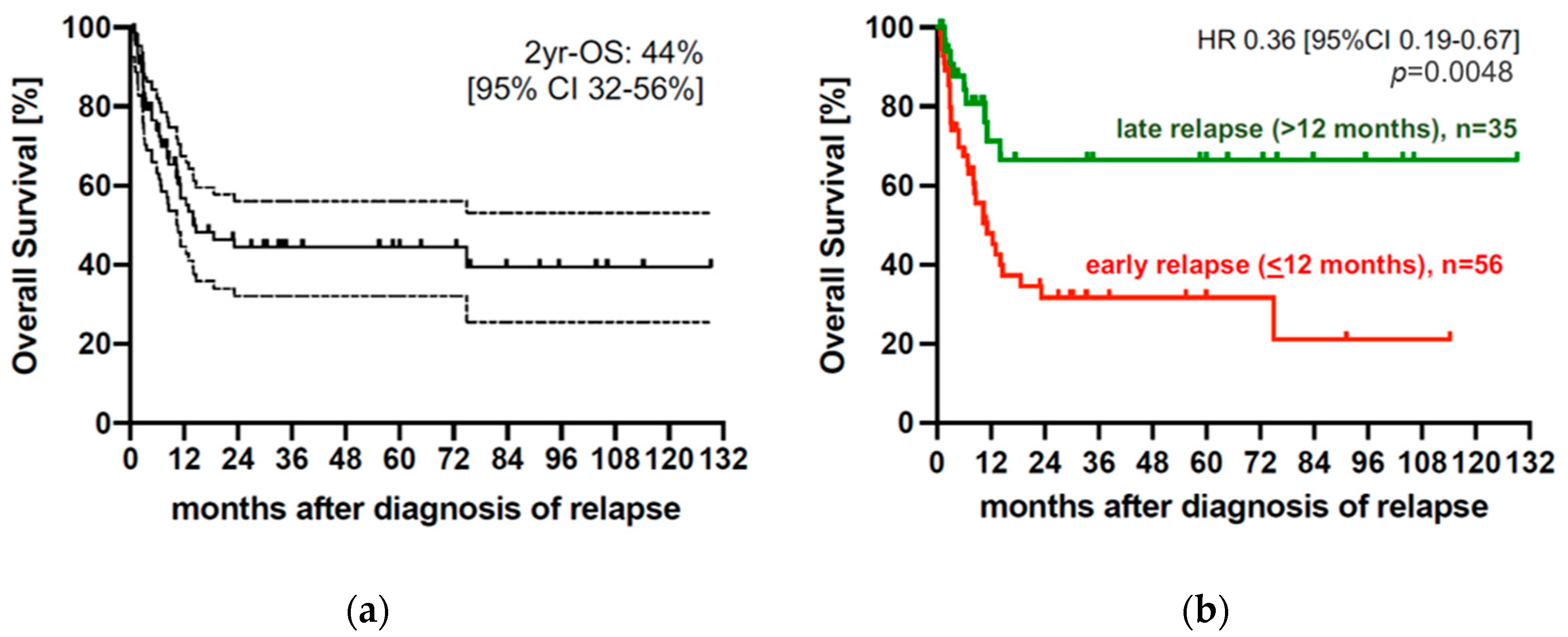
3.2. Relapse Characteristics and Outcomes
3.3. Comparison of Early and Late Relapses after Allo-SCT
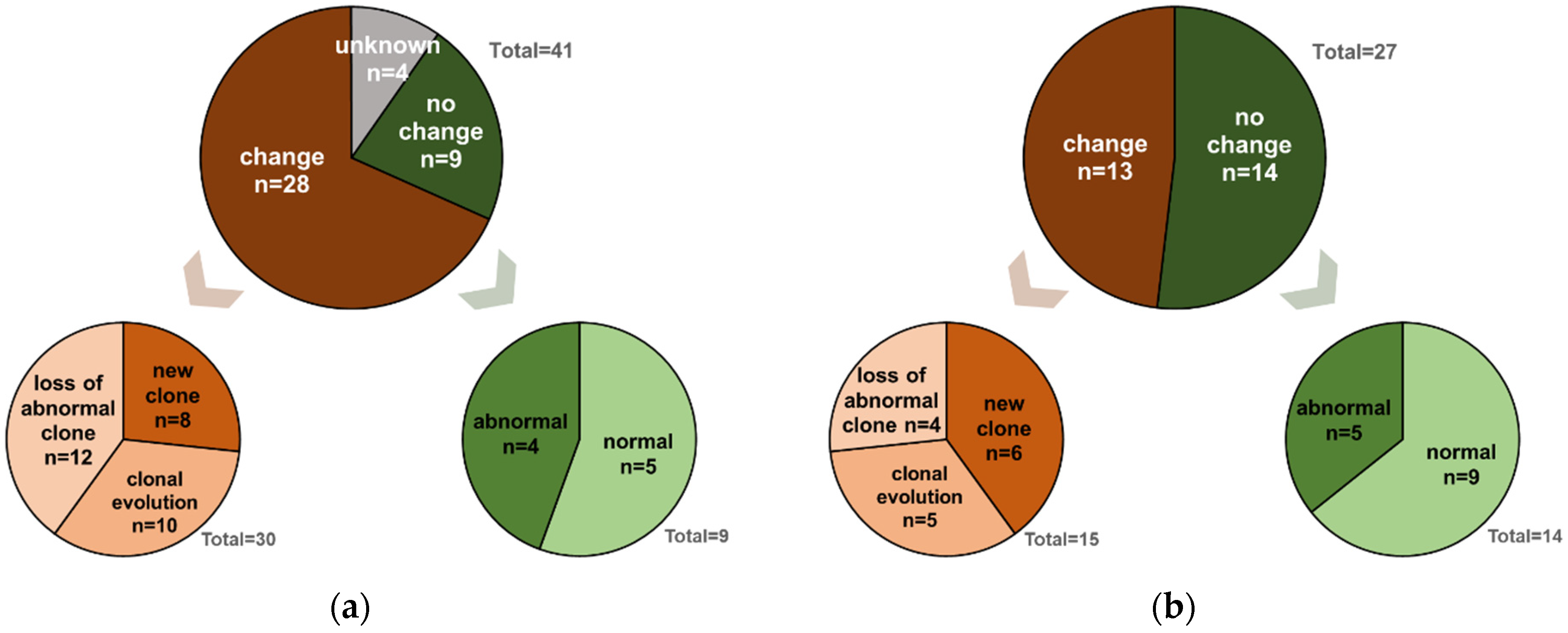
3.4. Comparative Karyotype Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Lima, M.; Porter, D.L.; Battiwalla, M.; Bishop, M.R.; Giralt, S.A.; Hardy, N.M.; Kröger, N.; Wayne, A.S.; Schmid, C. Proceedings from the National Cancer Institute’s Second International Workshop on the Biology, Prevention, and Treatment of Relapse after Hematopoietic Stem Cell Transplantation: Part III. Prevention and Treatment of Relapse after Allogeneic Transplantation. Biol. Blood Marrow Transplant. 2014, 20, 4–13. [Google Scholar] [PubMed]
- Schmid, C.; de Wreede, L.C.; van Biezen, A.; Finke, J.; Ehninger, G.; Ganser, A.; Volin, L.; Niederwieser, D.; Beelen, D.; Alessandrino, P.; et al. Outcome after relapse of myelodysplastic syndrome and secondary acute myeloid leukemia following allogeneic stem cell transplantation: A retrospective registry analysis on 698 patients by the Chronic Malignancies Working Party of the European Society of Blood and Marrow Transplantation. Haematologica 2018, 103, 237–245. [Google Scholar] [PubMed]
- Schuler, E.; Boughoufala, S.; Rautenberg, C.; Nachtkamp, K.; Dienst, A.; Fenk, R.; Haas, R.; Kondakci, M.; Germing, U.; Schroeder, T.; et al. Relapse patterns and treatment strategies in patients receiving allogeneic hematopoietic stem cell transplantation for myeloid malignancies. Ann. Hematol. 2019, 98, 1225–1235. [Google Scholar] [CrossRef]
- Craddock, C.; Labopin, M.; Robin, M.; Finke, J.; Chevallier, P.; Yakoub-Agha, I.; Bourhis, J.H.; Sengelov, H.; Blaise, D.; Luft, T.; et al. Clinical activity of azacitidine in patients who relapse after allogeneic stem cell transplantation for acute myeloid leukemia. Haematologica 2016, 101, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Rautenberg, C.; Bergmann, A.; Germing, U.; Fischermanns, C.; Pechtel, S.; Kaivers, J.; Jäger, P.; Schuler, E.; Haas, R.; Kobbe, G.; et al. Prediction of Response and Survival Following Treatment with Azacitidine for Relapse of Acute Myeloid Leukemia and Myelodysplastic Syndromes after Allogeneic Hematopoietic Stem Cell Transplantation. Cancers 2020, 12, 2255. [Google Scholar] [CrossRef]
- Bejar, R.; Stevenson, K.E.; Caughey, B.; Lindsley, R.C.; Mar, B.G.; Stojanov, P.; Getz, G.; Steensma, D.P.; Ritz, J.; Soiffer, R.; et al. Somatic mutations predict poor outcome in patients with myelodysplastic syndrome after hematopoietic stem-cell transplantation. J. Clin. Oncol. 2014, 32, 2691–2698. [Google Scholar] [CrossRef] [PubMed]
- Heuser, M.; Gabdoulline, R.; Löffeld, P.; Dobbernack, V.; Kreimeyer, H.; Pankratz, M.; Flintrop, M.; Liebich, A.; Klesse, S.; Panagiota, V.; et al. Individual outcome prediction for myelodysplastic syndrome (MDS) and secondary acute myeloid leukemia from MDS after allogeneic hematopoietic cell transplantation. Ann. Hematol. 2017, 96, 1361–1372. [Google Scholar] [CrossRef]
- Rautenberg, C.; Germing, U.; Stepanow, S.; Lauseker, M.; Köhrer, K.; Jäger, P.S.; Geyh, S.; Fan, M.; Haas, R.; Kobbe, G.; et al. Influence of somatic mutations and pretransplant strategies in patients allografted for myelodysplastic syndrome or secondary acute myeloid leukemia. Am. J. Hematol. 2020, 96, ajh.26013. [Google Scholar] [CrossRef]
- Olson, A.L.; Saliba, R.M.; Oran, B.; Chen, J.; Alousi, A.; Ahmed, S.; Bashir, Q.; Ciurea, S.O.; Hosing, C.; Im, J.S.; et al. Cytogenetics and Blast Count Determine Transplant Outcomes in Patients with Active Acute Myeloid Leukemia. Acta Haematol. 2021, 144, 74–81. [Google Scholar] [CrossRef]
- Yeung, C.C.S.; Gerds, A.T.; Fang, M.; Scott, B.L.; Flowers, M.E.D.; Gooley, T.; Deeg, H.J. Relapse after Allogeneic Hematopoietic Cell Transplantation for Myelodysplastic Syndromes: Analysis of Late Relapse Using Comparative Karyotype and Chromosome Genome Array Testing. Biol. Blood Marrow Transplant. 2015, 21, 1565–1575. [Google Scholar] [CrossRef]
- Courville, E.L.; Griffith, M.; Ustun, C.; Yohe, S.; Warlick, E. Impending relapse of myelodysplastic syndrome after allogeneic transplant is difficult to diagnose and requires a multi-modal approach. BMC Clin. Pathol. 2017, 17, 28. [Google Scholar] [CrossRef] [PubMed]
- Michallet, A.S.; Nicolini, F.; Fürst, S.; Le, Q.H.; Dubois, V.; Hayette, S.; Bourgeot, J.P.; Tremisi, J.P.; Thomas, X.; Gebuhrer, L.; et al. Outcome and long-term follow-up of alloreactive donor lymphocyte infusions given for relapse after myeloablative allogeneic hematopoietic stem cell transplantations (HSCT). Bone Marrow Transplant. 2005, 35, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Shaw, B.E.; Mufti, G.J.; Mackinnon, S.; Cavenagh, J.D.; Pearce, R.M.; Towlson, K.E.; Apperley, J.F.; Chakraverty, R.; Craddock, C.; Kazmi, M.A.; et al. Outcome of second allogeneic transplants using reduced-intensity conditioning following relapse of haematological malignancy after an initial allogeneic transplant. Bone Marrow Transplant. 2008, 42, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, P.L.; Tuechler, H.; Schanz, J.; Sanz, G.; Garcia-Manero, G.; Solé, F.; Bennett, J.M.; Bowen, D.; Fenaux, P.; Dreyfus, F.; et al. Revised International Prognostic Scoring System for Myelodysplastic Syndromes. Blood 2012, 120, 2454–2465. [Google Scholar] [CrossRef]
- Bacigalupo, A.; Ballen, K.; Rizzo, D.; Giralt, S.; Lazarus, H.; Ho, V.; Apperley, J.; Slavin, S.; Pasquini, M.; Sandmaier, B.M.; et al. Defining the intensity of conditioning regimens: Working definitions. Biol. Blood Marrow Transplant. 2009, 15, 1628–1633. [Google Scholar] [CrossRef]
- Such, E.; Germing, U.; Malcovati, L.; Cervera, J.; Kuendgen, A.; Della Porta, M.G.; Nomdedeu, B.; Arenillas, L.; Luño, E.; Xicoy, B.; et al. Development and validation of a prognostic scoring system for patients with chronic myelomonocytic leukemia. Blood 2013, 121, 3005–3015. [Google Scholar] [CrossRef]
- Bejanyan, N.; Weisdorf, D.J.; Logan, B.R.; Wang, H.L.; Devine, S.M.; de Lima, M.; Bunjes, D.W.; Zhang, M.-J. Survival of patients with acute myeloid leukemia relapsing after allogeneic hematopoietic cell transplantation: A center for international blood and marrow transplant research study. Biol. Blood Marrow Transplant. 2015, 21, 454–459. [Google Scholar] [CrossRef]
- Sorror, M.L.; Sandmaier, B.M.; Storer, B.E.; Maris, M.B.; Baron, F.; Maloney, D.G.; Scott, B.L.; Deeg, H.J.; Appelbaum, F.R.; Storb, R. Comorbidity and Disease Status–Based Risk Stratification of Outcomes Among Patients With Acute Myeloid Leukemia or Myelodysplasia Receiving Allogeneic Hematopoietic Cell Transplantation. JCO 2007, 25, 4246–4254. [Google Scholar] [CrossRef]
- Schroeder, T.; Wegener, N.; Lauseker, M.; Rautenberg, C.; Nachtkamp, K.; Schuler, E.; Kondakci, M.; Haas, R.; Germing, U.; Kobbe, G. Comparison between Upfront Transplantation and different Pretransplant Cytoreductive Treatment Approaches in Patients with High-Risk Myelodysplastic Syndrome and Secondary Acute Myelogenous Leukemia. Biol. Blood Marrow Transplant. 2019, 25, 1550–1559. [Google Scholar] [CrossRef] [PubMed]
- Lancet, J.E.; Uy, G.L.; Cortes, J.E.; Newell, L.F.; Lin, T.L.; Ritchie, E.K.; Stuart, R.K.; Strickland, S.A.; Hogge, D.; Solomon, S.R.; et al. CPX-351 (cytarabine and daunorubicin) Liposome for Injection Versus Conventional Cytarabine Plus Daunorubicin in Older Patients with Newly Diagnosed Secondary Acute Myeloid Leukemia. J. Clin. Oncol. 2018, 36, 2684–2692. [Google Scholar] [CrossRef] [PubMed]
- Guolo, F.; Fianchi, L.; Minetto, P.; Clavio, M.; Gottardi, M.; Galimberti, S.; Rizzuto, G.; Rondoni, M.; Bertani, G.; Dargenio, M.; et al. CPX-351 treatment in secondary acute myeloblastic leukemia is effective and improves the feasibility of allogeneic stem cell transplantation: Results of the Italian compassionate use program. Blood Cancer J. 2020, 10, 96. [Google Scholar] [CrossRef] [PubMed]
- Chiche, E.; Rahmé, R.; Bertoli, S.; Dumas, P.Y.; Micol, J.B.; Hicheri, Y.; Pasquier, F.; Peterlin, P.; Chevallier, P.; Thomas, X.; et al. Real-life experience with CPX-351 and impact on the outcome of high-risk AML patients: A multicentric French cohort. Blood Adv. 2021, 5, 176–184. [Google Scholar] [CrossRef]
- Rautenberg, C.; Stölzel, F.; Röllig, C.; Stelljes, M.; Gaidzik, V.; Lauseker, M.; Kriege, O.; Verbeek, M.; Unglaub, J.M.; Thol, F.; et al. Real-world experience of CPX-351 as first-line treatment for patients with acute myeloid leukemia. Blood Cancer J. 2021, 11, 164. [Google Scholar] [CrossRef]
- Matthews, A.H.; Perl, A.E.; Luger, S.M.; Loren, A.W.; Gill, S.I.; Porter, D.L.; Babushok, D.V.; Maillard, I.P.; Carroll, M.P.; Frey, N.V.; et al. Real-world effectiveness of CPX-351 vs venetoclax and azacitidine in acute myeloid leukemia. Blood Adv. 2022, 6, 3997–4005. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | All | Early Relapse (≤12 Months) | Late Relapse (>12 Months) | p |
|---|---|---|---|---|
| No. of patients (%) | 91 | 56 (62) | 35 (38) | |
| Age at transplant, median (range), year | 57 (20–76) | 59 (20–71) | 57 (24–76) | ns |
| Gender | ||||
| Male | 22 (48) | 37 (66) | 20 (57) | ns |
| Female | 24 (52) | 19 (34) | 15 (43) | |
| WHO 2016 diagnosis (15) | ||||
| AML-MRC | 29 (32) | 21 (38) | 8 (23) | ns a |
| MDS-SLD/-MLD | 8 (9) | 4 (7) | 4 (11) | ns b |
| MDS-RS-SLD/-MLD | 1 (1) | 0 (0) | 1 (3) | |
| MDS-EBI/-II | 42 (46) | 22 (39) | 20 (57) | ns c |
| MDS-u | 3 (3) | 3 (5) | 0 (0) | |
| CMML-0 | 1 (1) | 1 (2) | 0 (0) | ns d |
| CMML-I/-II | 7 (8) | 5 (9) | 2 (6) | |
| t-related myeloid neoplasm (MDS) | 12 (13) | 7 (13) | 5 (14) | |
| Karyotype at diagnosis | ||||
| Normal | 37 (41) | 20 (36) | 17 (49) | ns |
| Aberrant | 50 (55) | 32 (57) | 18 (41) | |
| Complex | 29 (36) | 25 (45) | 4 (11) | 0.0004 e |
| Missing | 4 (4) | 4 (7) | 0 | |
| ELN 2017//IPSS-R//CPSS at diagnosis (14,16,18) * | ||||
| favorable | 35 (38) | 15 (27) | 20 (57) | |
| intermediate | 20 (22) | 11 (20) | 9 (26) | 0.0008 f |
| unfavorable | 36 (40) | 30 (53) | 6 (17) | |
| HCT-CI (19) | ||||
| Low | 43 (47) | 25 (45) | 18 (51) | ns |
| Intermediate/high | 48 (53) | 31 (55) | 17 (49) | |
| Conditioning (17) | ||||
| Standard-dose | 27 (30) | 16 (29) | 11 (31) | ns |
| Dose-reduced | 64 (70) | 40 (71) | 24 (69) | |
| Donor Type (n = 90) | ||||
| related | 15 (17) | 12 (22) | 3 (9) | ns |
| unrelated | 75 (83) | 43 (78) | 32 (91) | |
| HLA-matching | ||||
| matched | 61 (67) | 37 (66) | 24 (69) | ns |
| mismatched | 30 (33) | 19 (34) | 11 (31) | |
| Type of Relapse | ||||
| molecular | 23 (25) | 15 (27) | 8 (23) | ns |
| hematolgic | 68 (75) | 41 (73) | 27 (77) | |
| Karyotype at relapse (n = 68 &) | ||||
| change | 41 (64) | 28 (76) | 13 (48) | 0.03 |
| no change | 23 36) | 9 (24) | 14 (52) | |
| Blast count at relapse | ||||
| normal | 36 (40) | 21 (38) | 15 (43) | ns |
| elevated | 55 (60) | 35 (62) | 20 (57) | |
| Pretreatment Strategy | ||||
| Upfront # or CR after CTX | 51 (56) | 26 (46) | 25 (71) | 0.02 |
| no CR after CTX | 40 (44) | 30 (54) | 10 (29) |
| Variable | Odds Ratio ” | 95% CI | p |
|---|---|---|---|
| Treatment prior to allo-SCT Upfront #/CR vs. No CR | 3.402 | 1.140–10.155 | 0.028 |
| ELN 2017//IPSS-R//CPSS at diagnosis (14,16,18) * Favorable/intermediate Unfavorable | 2.777 | 0.755–10.213 | 0.124 |
| Karyotype Not complex vs. Complex | 3.038 | 0.695–13.278 | 0.140 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Platte, V.; Bergmann, A.; Hildebrandt, B.; Wieczorek, D.; Schuler, E.; Germing, U.; Kaivers, J.; Haas, R.; Kobbe, G.; Schroeder, T.; et al. Clinical and Cytogenetic Characterization of Early and Late Relapses in Patients Allografted for Myeloid Neoplasms with a Myelodysplastic Component. Cancers 2022, 14, 6244. https://doi.org/10.3390/cancers14246244
Platte V, Bergmann A, Hildebrandt B, Wieczorek D, Schuler E, Germing U, Kaivers J, Haas R, Kobbe G, Schroeder T, et al. Clinical and Cytogenetic Characterization of Early and Late Relapses in Patients Allografted for Myeloid Neoplasms with a Myelodysplastic Component. Cancers. 2022; 14(24):6244. https://doi.org/10.3390/cancers14246244
Chicago/Turabian StylePlatte, Victoria, Anika Bergmann, Barbara Hildebrandt, Dagmar Wieczorek, Esther Schuler, Ulrich Germing, Jennifer Kaivers, Rainer Haas, Guido Kobbe, Thomas Schroeder, and et al. 2022. "Clinical and Cytogenetic Characterization of Early and Late Relapses in Patients Allografted for Myeloid Neoplasms with a Myelodysplastic Component" Cancers 14, no. 24: 6244. https://doi.org/10.3390/cancers14246244
APA StylePlatte, V., Bergmann, A., Hildebrandt, B., Wieczorek, D., Schuler, E., Germing, U., Kaivers, J., Haas, R., Kobbe, G., Schroeder, T., & Rautenberg, C. (2022). Clinical and Cytogenetic Characterization of Early and Late Relapses in Patients Allografted for Myeloid Neoplasms with a Myelodysplastic Component. Cancers, 14(24), 6244. https://doi.org/10.3390/cancers14246244