
Non-Typhoidal Salmonella Infection in Children: Influence of Antibiotic Therapy on Postconvalescent Excretion and Clinical Course—A Systematic Review

Abstract
1. Introduction
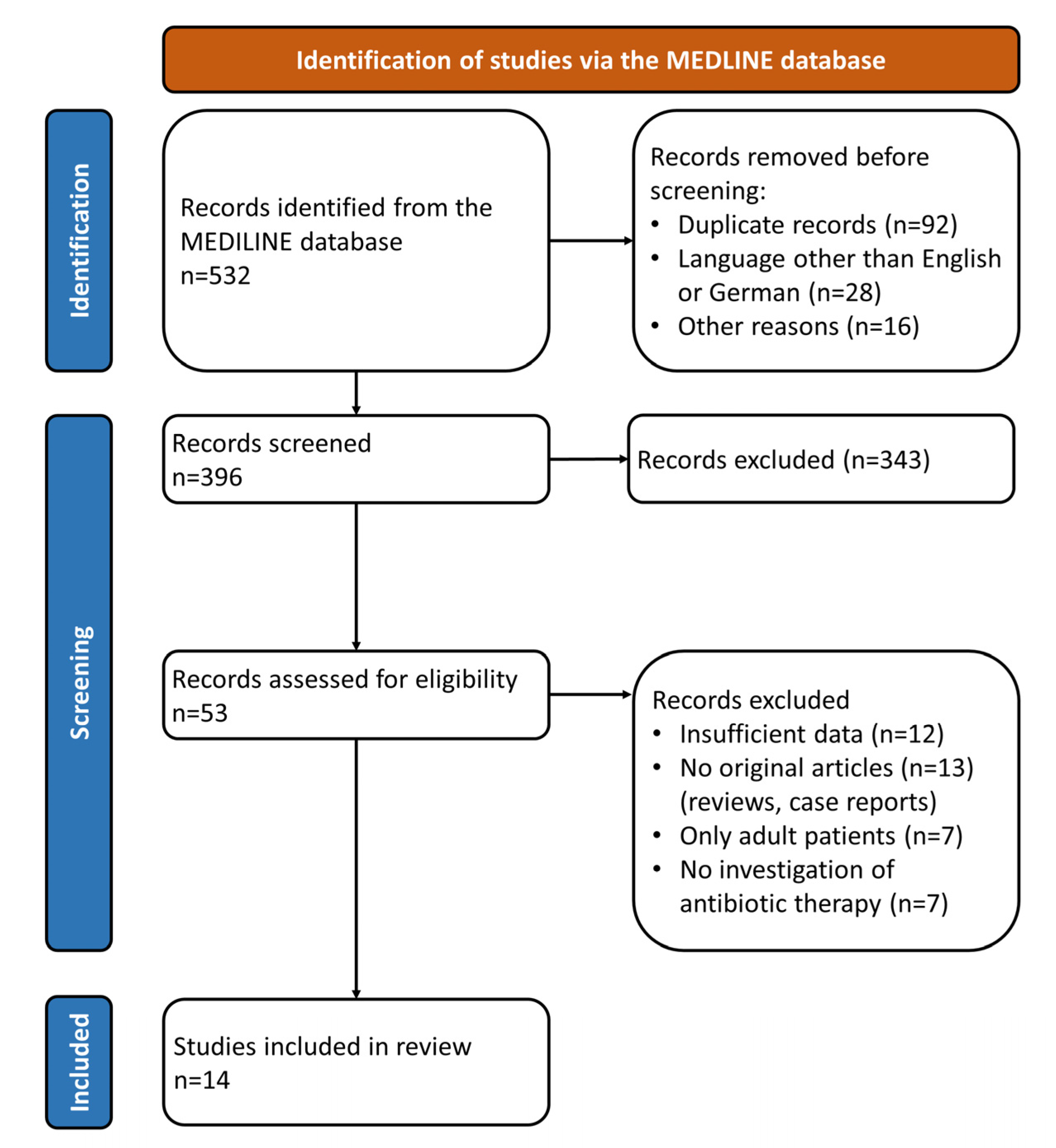
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Stanaway, J.D. The global burden of non-typhoidal salmonella invasive disease: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Infect. Dis. 2019, 19, 1312–1324. [Google Scholar] [CrossRef]
- Havelaar, A.H.; Kirk, M.D.; Torgerson, P.R.; Gibb, H.J.; Hald, T.; Lake, R.J.; Praet, N.; Bellinger, D.C.; de Silva, N.R.; Gargouri, N.; et al. World Health Organization Global Estimates and Regional Comparisons of the Burden of Foodborne Disease in 2010. PLoS Med. 2015, 12, e1001923. [Google Scholar] [CrossRef]
- Dewey-Mattia, D.; Manikonda, K.; Hall, A.J.; Wise, M.E.; Crowe, S.J. Surveillance for Foodborne Disease Outbreaks—United States, 2009–2015. MMWR Surveill. Summ. 2018, 67, 1–11. [Google Scholar] [CrossRef]
- Butler, A.J.; Thomas, M.K.; Pintar, K.D.M. Expert Elicitation as a Means to Attribute 28 Enteric Pathogens to Foodborne, Waterborne, Animal Contact, and Person-to-Person Transmission Routes in Canada. Foodborne Pathog. Dis. 2015, 12, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Christidis, T.; Hurst, M.; Rudnick, W.; Pintar, K.D.M.; Pollari, F. A comparative exposure assessment of foodborne, animal contact and waterborne transmission routes of Salmonella in Canada. Food Control 2020, 109, 106899. [Google Scholar] [CrossRef]
- Feasey, N.A.; Archer, B.N.; Heyderman, R.S.; Sooka, A.; Dennis, B.; Gordon, M.A.; Keddy, K.H. Typhoid fever and invasive nontyphoid salmonellosis, Malawi and South Africa. Emerg. Infect. Dis. 2010, 16, 1448–1451. [Google Scholar] [CrossRef] [PubMed]
- Kariuki, S.; Owusu-Dabo, E. Research on Invasive Nontyphoidal Salmonella Disease and Developments Towards Better Understanding of Epidemiology, Management, and Control Strategies. Clin. Infect. Dis. 2020, 71, S127–S129. [Google Scholar] [CrossRef] [PubMed]
- Scallan, E.; Hoekstra, R.M.; Angulo, F.J.; Tauxe, R.V.; Widdowson, M.A.; Roy, S.L.; Jones, J.L.; Griffin, P.M. Foodborne illness acquired in the United States—Major pathogens. Emerg. Infect. Dis. 2011, 17, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Crump, J.A.; Sjolund-Karlsson, M.; Gordon, M.A.; Parry, C.M. Epidemiology, Clinical Presentation, Laboratory Diagnosis, Antimicrobial Resistance, and Antimicrobial Management of Invasive Salmonella Infections. Clin. Microbiol. Rev. 2015, 28, 901–937. [Google Scholar] [CrossRef]
- Takkinsatian, P.; Silpskulsuk, C.; Prommalikit, O. Clinical features and antibiotic susceptibility of Salmonella gastroenteritis in children: A ten-year review. Med. J. Malays. 2020, 75, 672–676. [Google Scholar]
- Lounis, Y.; Hugo, J.; Demarche, M.; Seghaye, M.C. Influence of age on clinical presentation, diagnosis delay and outcome in pre-school children with acute appendicitis. BMC Pediatr. 2020, 20, 151. [Google Scholar] [CrossRef]
- Park, S.E.; Pak, G.D.; Aaby, P.; Adu-Sarkodie, Y.; Ali, M.; Aseffa, A.; Biggs, H.M.; Bjerregaard-Andersen, M.; Breiman, R.F.; Crump, J.A.; et al. The Relationship Between Invasive Nontyphoidal Salmonella Disease, Other Bacterial Bloodstream Infections, and Malaria in Sub-Saharan Africa. Clin. Infect. Dis. 2016, 62 (Suppl. S1), S23–S31. [Google Scholar] [CrossRef]
- Tsai, M.H.; Huang, Y.C.; Lin, T.Y.; Huang, Y.L.; Kuo, C.C.; Chiu, C.H. Reappraisal of parenteral antimicrobial therapy for nontyphoidal Salmonella enteric infection in children. Clin. Microbiol. Infect. 2011, 17, 300–305. [Google Scholar] [CrossRef]
- Cohen, J.I.; Bartlett, J.A.; Corey, G.R. Extra-intestinal manifestations of salmonella infections. Medicine 1987, 66, 349–388. [Google Scholar] [CrossRef]
- Wang, J.H.; Liu, Y.C.; Yen, M.Y.; Wang, J.H.; Chen, Y.S.; Wann, S.R.; Cheng, D.L. Mycotic aneurysm due to non-typhi salmonella: Report of 16 cases. Clin. Infect. Dis. 1996, 23, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, E.; Bachur, R.; Harper, M. Non-typhi Salmonella bacteremia in children. Pediatr Infect. Dis. J. 1999, 18, 1073–1077. [Google Scholar] [CrossRef]
- Mohan, A.; Munusamy, C.; Tan, Y.C.; Muthuvelu, S.; Hashim, R.; Chien, S.L.; Wong, M.K.; Khairuddin, N.A.; Podin, Y.; Lau, P.S.; et al. Invasive Salmonella infections among children in Bintulu, Sarawak, Malaysian Borneo: A 6-year retrospective review. BMC Infect. Dis. 2019, 19, 330. [Google Scholar] [CrossRef] [PubMed]
- Uche, I.V.; MacLennan, C.A.; Saul, A. A Systematic Review of the Incidence, Risk Factors and Case Fatality Rates of Invasive Nontyphoidal Salmonella (iNTS) Disease in Africa (1966 to 2014). PLoS Negl. Trop. Dis. 2017, 11, e0005118. [Google Scholar] [CrossRef] [PubMed]
- Lehrnbecher, T.; Laws, H.J. Infectious complications in pediatric cancer patients. Klin. Padiatr. 2005, 217 (Suppl. S1), S3–S8. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Huang, I.F.; Kao, C.H.; Lee, W.Y.; Chang, M.F.; Chen, Y.S.; Wu, K.S.; Hu, H.H.; Hsieh, K.S.; Chiou, C.C. Clinical manifestations of nontyphoid salmonellosis in children younger than 2 years old—Experiences of a tertiary hospital in southern Taiwan. Pediatr. Neonatol. 2012, 53, 193–198. [Google Scholar] [CrossRef]
- Wu, H.M.; Huang, W.Y.; Lee, M.L.; Yang, A.D.; Chaou, K.P.; Hsieh, L.Y. Clinical features, acute complications, and outcome of Salmonella meningitis in children under one year of age in Taiwan. BMC Infect. Dis. 2011, 11, 30. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.S.; Puthucheary, S.D.; Parasakthi, N. Extra-intestinal non-typhoidal Salmonella infections in children. Ann. Trop. Paediatr. 2000, 20, 125–129. [Google Scholar] [CrossRef]
- Barbara, G.; Stanghellini, V.; Berti-Ceroni, C.; De Giorgio, R.; Salvioli, B.; Corradi, F.; Cremon, C.; Corinaldesi, R. Role of antibiotic therapy on long-term germ excretion in faeces and digestive symptoms after Salmonella infection. Aliment. Pharmacol. Ther. 2000, 14, 1127–1131. [Google Scholar] [CrossRef] [PubMed]
- Gal-Mor, O. Persistent Infection and Long-Term Carriage of Typhoidal and Nontyphoidal Salmonellae. Clin. Microbiol. Rev. 2019, 32. [Google Scholar] [CrossRef] [PubMed]
- Marzel, A.; Desai, P.T.; Goren, A.; Schorr, Y.I.; Nissan, I.; Porwollik, S.; Valinsky, L.; McClelland, M.; Rahav, G.; Gal-Mor, O. Persistent Infections by Nontyphoidal Salmonella in Humans: Epidemiology and Genetics. Clin. Infect. Dis. 2016, 62, 879–886. [Google Scholar] [CrossRef]
- Buchwald, D.S.; Blaser, M.J. A review of human salmonellosis: II. Duration of excretion following infection with nontyphi Salmonella. Rev. Infect. Dis. 1984, 6, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Devi, S.; Murray, C.J. Salmonella carriage rate amongst school children—A three year study. Southeast Asian J. Trop. Med. Public Health 1991, 22, 357–361. [Google Scholar] [PubMed]
- Balasubramanian, R.; Im, J.; Lee, J.S.; Jeon, H.J.; Mogeni, O.D.; Kim, J.H.; Rakotozandrindrainy, R.; Baker, S.; Marks, F. The global burden and epidemiology of invasive non-typhoidal Salmonella infections. Hum. Vaccines Immunother. 2019, 15, 1421–1426. [Google Scholar] [CrossRef]
- Mughini-Gras, L.; Pijnacker, R.; Duijster, J.; Heck, M.; Wit, B.; Veldman, K.; Franz, E. Changing epidemiology of invasive non-typhoid Salmonella infection: A nationwide population-based registry study. Clin. Microbiol. Infect. 2020, 26, 941.e9–941.e14. [Google Scholar] [CrossRef]
- Marchello, C.S.; Fiorino, F.; Pettini, E.; Crump, J.A.; Vacc-i, N.T.S.C.C. Incidence of non-typhoidal Salmonella invasive disease: A systematic review and meta-analysis. J. Infect. 2021, in press. [Google Scholar] [CrossRef]
- Macdonald, W.B.; Friday, F.; Mc, E.M. The effect of chloramphenicol in Salmonella enteritis of infancy. Arch. Dis. Child. 1954, 29, 238–241. [Google Scholar] [CrossRef]
- Dixon, J.M. Effect of antibiotic treatment on duration of excretion of Salmonella typhimurium by children. Br. Med. J. 1965, 2, 1343–1345. [Google Scholar] [CrossRef][Green Version]
- Onwuezobe, I.A.; Oshun, P.O.; Odigwe, C.C. Antimicrobials for treating symptomatic non-typhoidal Salmonella infection. Cochrane Database Syst. Rev. 2012, 11, CD001167. [Google Scholar] [CrossRef]
- Huang, I.F.; Wagener, M.M.; Hsieh, K.S.; Liu, Y.C.; Wu, T.C.; Lee, W.Y.; Chiou, C.C. Nontyphoid salmonellosis in taiwan children: Clinical manifestations, outcome and antibiotic resistance. J. Pediatr. Gastroenterol. Nutr. 2004, 38, 518–523. [Google Scholar] [CrossRef]
- Duff, N.; Steele, A.D.; Garrett, D. Global Action for Local Impact: The 11th International Conference on Typhoid and Other Invasive Salmonelloses. Clin. Infect. Dis. 2020, 71, S59–S63. [Google Scholar] [CrossRef] [PubMed]
- Murase, T.; Yamada, M.; Muto, T.; Matsushima, A.; Yamai, S. Fecal excretion of Salmonella enterica serovar typhimurium following a food-borne outbreak. J. Clin. Microbiol. 2000, 38, 3495–3497. [Google Scholar] [CrossRef] [PubMed]
- Rosenstein, B.J. Salmonellosis in infants and children. J. Pediatr. 1967, 70, 1–7. [Google Scholar] [CrossRef]
- Wen, S.C.; Best, E.; Nourse, C. Non-typhoidal Salmonella infections in children: Review of literature and recommendations for management. J. Paediatr. Child. Health 2017, 53, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 31 August 2021).
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.H.; Laing Brown, G.; Latham Brown, D.; Emond, R.T.D.; Galpine, J.F.; Jamieson, S.R.; Lamb, S.G.; Lambert, H.P.; McKendrick, G.D.W.; Medlock, J.M.; et al. Effect of neomycin in non-invasive salmonella infections of the gastrointestinal tract. Joint Project by Members of the Association for the Study of Infectious Disease. Lancet 1970, 2, 1159–1161. [Google Scholar]
- Kazemi, M.; Gumpert, T.G.; Marks, M.I. A controlled trial comparing sulfametboxazole-trimethoprim, ampicillin, and no therapy in the treatment of salmonella gastroenteritis in children. J. Pediatr. 1973, 83, 646–650. [Google Scholar] [CrossRef]
- Nelson, J.D.; Kusmiesz, H.; Jackson, L.H.; Woodman, E. Treatment of Salmonella gastroenteritis with ampicillin, amoxicillin, or placebo. Pediatrics 1980, 65, 1125–1130. [Google Scholar]
- Stögmann, W.; Blümel, P. Salmonellosen im Kindersalter—Ein aktuelles Problem (Salmonella enteritis in childhood—A topical problem). Wien. Klin. Wochenschr. 1982, 94, 86–89. [Google Scholar] [PubMed]
- Chiu, C.H.; Lin, T.Y.; Ou, J.T. A clinical trial comparing oral azithromycin, cefixime and no antibiotics in the treatment of acute uncomplicated Salmonella enteritis in children. J. Paediatr. Child. Health 1999, 35, 372–374. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.Y.; Chiu, C.H.; Lin, P.Y.; Wang, M.H.; Su, L.H.; Lin, T.Y. Short-term ceftriaxone therapy for treatment of severe non-typhoidal Salmonella enterocolitis. Acta Paediatr. 2003, 92, 537–540. [Google Scholar] [CrossRef]
- Ho, P.Y.; Chen, W.L.; Cheng, M.F.; Shen, Y.T.; Hu, H.H.; Sheu, S.K.; Huang, I.F. Factors affecting fecal excretion time in pediatric nontyphoid Salmonella infection. Pediatr. Neonatol. 2021, 62, 387–393. [Google Scholar] [CrossRef]
- Chiu, C.H.; Lin, T.Y.; Ou, J.T. A pilot study of seven days of ceftriaxone therapy for children with Salmonella enterocolitis. Changgeng Yi Xue Za Zhi 1997, 20, 115–121. [Google Scholar]
- Kazemi, M.; Gumpert, G.; Marks, M.I. Clinical spectrum and carrier state of nontyphoidal salmonella infections in infants and children. Can. Med. Assoc. J. 1974, 110, 1253–1257. [Google Scholar]
- Ruiz, M.; Rodriguez, J.C.; Escribano, I.; Royo, G. Available options in the management of non-typhi Salmonella. Expert Opin. Pharmacother. 2004, 5, 1737–1743. [Google Scholar] [CrossRef]
- Robinson, J.L. Salmonella infections in Canadian children. Paediatr. Child. Health 2019, 24, 50–51. [Google Scholar] [CrossRef]
- Cohen, R.; Raymond, J.; Gendrel, D. Antimicrobial treatment of diarrhea/acute gastroenteritis in children. Arch. Pediatr. 2017, 24, S26–S29. [Google Scholar] [CrossRef]
- Büttcher, M.; Flieger, A.; Fruth, A.; Simon, S.; Huppertz, H.-I. Salmonellose. In Handbook of the German Society for Pediatric Infectious Diseases—DGPI, 7th ed.; Berner, R., Bialek, R., Forster, J., Eds.; Thieme: Stuttgart, Germany, 2018; pp. 719–723. [Google Scholar]
- AAP. Salmonella infections. In Red Book—Report of the Committee on Infectious Diseases, 32th ed.; Kimberlin, D.W., Barnett, E.D., Lynfield, R., Sawyer, M.H., Eds.; American Academy of Pediatrics: Elk Grove Village, IL, USA, 2021; pp. 655–662. [Google Scholar]
- Tack, B.; Vanaenrode, J.; Verbakel, J.Y.; Toelen, J.; Jacobs, J. Invasive non-typhoidal Salmonella infections in sub-Saharan Africa: A systematic review on antimicrobial resistance and treatment. BMC Med. 2020, 18, 212. [Google Scholar] [CrossRef] [PubMed]
- Aserkoff, B.; Bennett, J.V. Effect of antibiotic therapy in acute salmonellosis on the fecal excretion of salmonellae. N. Engl. J. Med. 1969, 281, 636–640. [Google Scholar] [CrossRef] [PubMed]
- Pitkäjärvi, T.; Kujanne, E.; Sillantaka, I.; Lumio, J. Norfloxacin and Salmonella excretion in acute gastroenteritis--a 6-month follow-up study. Scand. J. Infect. Dis. 1996, 28, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, C.; Garcia-Restoy, E.; Garau, J.; Bella, F.; Freixas, N.; Simo, M.; Lite, J.; Sanchez, P.; Espejo, E.; Cobo, E.; et al. Ciprofloxacin and trimethoprim-sulfamethoxazole versus placebo in acute uncomplicated Salmonella enteritis: A double-blind trial. J. Infect. Dis. 1993, 168, 1304–1307. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.R.; Badley, B.W. Treatment of Salmonella enteritis and its effect on the carrier state. Can. Med. Assoc. J. 1971, 104, 1004–1006. [Google Scholar] [PubMed]
- Shen, Y.; Huang, I.; Hu, H.; Chang, M.; Sheu, S. Whether Antimicrobial Therapy Affect Fecal Excretion Time In Paediatric Patients Of Nontyphoid Salmonellosis With Different Severity. Arch. Dis. Child. 2014, 99, A293. [Google Scholar] [CrossRef][Green Version]
- Yeung, C.Y.; Lee, H.C.; Chao, Y.N.; Chiu, N.C.; Huang, F.Y.; Hsieh, M.A. Effect of Antibiotic Therapy on Salmonella Fecal Excretion Time. J. Pediatr. Gastroenterol. Nutr. 2004, 39, 249–250. [Google Scholar] [CrossRef]
- Bula-Rudas, F.J.; Rathore, M.H.; Maraqa, N.F. Salmonella Infections in Childhood. Adv. Pediatr. 2015, 62, 29–58. [Google Scholar] [CrossRef]
- Carlstedt, G.; Dahl, P.; Niklasson, P.M.; Gullberg, K.; Banck, G.; Kahlmeter, G. Norfloxacin treatment of salmonellosis does not shorten the carrier stage. Scand. J. Infect. Dis. 1990, 22, 553–556. [Google Scholar] [CrossRef]
- Neill, M.A.; Opal, S.M.; Heelan, J.; Giusti, R.; Cassidy, J.E.; White, R.; Mayer, K.H. Failure of ciprofloxacin to eradicate convalescent fecal excretion after acute salmonellosis: Experience during an outbreak in health care workers. Ann. Int. Med. 1991, 114, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Kumta, N.; Roberts, J.A.; Lipman, J.; Wong, W.T.; Joynt, G.M.; Cotta, M.O. A Systematic Review of Studies Reporting Antibiotic Pharmacokinetic Data in the Cerebrospinal Fluid of Critically Ill Patients with Uninflamed Meninges. Antimicrob. Agents Chemother. 2020, 65, e01998-20. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, M.; Reynolds, J.; Karp, B.E.; Tate, H.; Fedorka-Cray, P.J.; Plumblee, J.R.; Hoekstra, R.M.; Whichard, J.M.; Mahon, B.E. Ceftriaxone-Resistant Nontyphoidal Salmonella from Humans, Retail Meats, and Food Animals in the United States, 1996–2013. Foodborne Pathog. Dis. 2017, 14, 74–83. [Google Scholar] [CrossRef]
- Su, L.H.; Chiu, C.H.; Chu, C.; Ou, J.T. Antimicrobial resistance in nontyphoid Salmonella serotypes: A global challenge. Clin. Infect. Dis. 2004, 39, 546–551. [Google Scholar] [CrossRef]
- Kariuki, S.; Gordon, M.A.; Feasey, N.; Parry, C.M. Antimicrobial resistance and management of invasive Salmonella disease. Vaccine 2015, 33 (Suppl. S3), C21–C29. [Google Scholar] [CrossRef]
- Sharland, M.; Pulcini, C.; Harbarth, S.; Zeng, M.; Gandra, S.; Mathur, S.; Magrini, N.; 21st WHO Expert Committee on Selection and Use of Essential Medicines. Classifying antibiotics in the WHO Essential Medicines List for optimal use-be AWaRe. Lancet Infect. Dis. 2018, 18, 18–20. [Google Scholar] [CrossRef]
- Baliban, S.M.; Lu, Y.J.; Malley, R. Overview of the Nontyphoidal and Paratyphoidal Salmonella Vaccine Pipeline: Current Status and Future Prospects. Clin. Infect. Dis. 2020, 71, S151–S154. [Google Scholar] [CrossRef]


{kind=link}
| First Author, Year of Publication | Country | Type of Study | Pathogen | Patients (Children) 1 | Antibiotics | Influence of Antibiotic Treatment on Excretion | Influence of Antibiotic Treatment on Clinical Course |
|---|---|---|---|---|---|---|---|
| Macdonald, 1954 [31] | Australia | RCS | S. typhimurium 2 | 51 (100%) | CHL | no influence | no influence |
| Dixon, 1965 [32] | England/Wales | RCS | S. typhimurium | 127 (100%) | NEO, STR, AMP, TET, CHL | prolongation | NA |
| Rosenstein, 1967 [37] | USA | RCS | NTS | 70 (100%) | AMP, NEO, CHL | prolongation | NA |
| Joint Group, 1970 [41] | England | RCT | NTS | 168 (64%) 4 | NEO | prolongation | no difference in duration of symptoms |
| Kazemi, 1973 [42] | Canada | RCT | NTS | 36 (100%) | SXT, AMP | no influence | no difference in clinical features or duration of symptoms |
| Kazemi, 1974 [49] | Canada | RCS | NTS | 117 (100%) | AMP, PEN, CHL, SXT | prolongation | slight increase in morbidity |
| Nelson, 1980 [43] | USA | RCT | NTS 3 | 44 (100%) | AMP, AMX | no influence, but more frequent bacteriologic relapse | no influence on symptoms |
| Stögmann, 1982 [44] | Austria | RCS | NTS | 148 (100%) | SXT and/or AMP | no influence | NA |
| Chiu, 1997 [48] | Taiwan | PCT | NTS | 30 (100%) | CRO | shortening | no difference in duration of symptoms |
| Chiu, 1999 [45] | Taiwan | RCT | NTS | 42 (100%) | AZM, CFM | no influence | no difference in duration of symptoms |
| Barbara, 2000 [23] | Italy | PCS | NTS | 1543 (95.1%) | PENs, SXT, CEFs | no influence | higher frequency of persistent symptoms after antibiotic treatment |
| Lin, 2003 [46] | Taiwan | PCT | NTS | 73 (100%) | CRO | no influence | longer duration of fever but rapid defervescence after antibiotic treatment |
| Tsai, 2011 [13] | Taiwan | RCS | NTS | 683 (100%) | AMP, CHL, SXT, CIP, CRO, FLO, CMF, IPM | NA | shorter hospitalization and duration of fever after treatment with CIP or CRO |
| Ho, 2021 [47] | Taiwan | PCS | NTS | 141 (100%) | CRO, SXT, AMP | no influence after appropriate treatment | worse clinical outcome in children with inappropriate antibiotics 5 |
| Findings | Conclusions | |
|---|---|---|
| Influence of antibiotic treatment on NTS excretion | Prolongation in four studies (all published before 1975) | Most recent studies did not observe a prolongation of NTS excretion. |
| Prolongation only after inappropriate antibiotic treatment in one study | ||
| Shortening in one study | ||
| No influence in six studies | ||
| Influence of antibiotic treatment on the clinical course of NTS infection | Higher frequency of persistent symptoms in one study | Variable results. Most recent studies did not observe a negative influence of antibiotic treatment on the clinical course. |
| Worse clinical outcome only after inappropriate antibiotic treatment in one study | ||
| Positive effects in two studies | ||
| No influence in six studies |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leinert, J.L.; Weichert, S.; Jordan, A.J.; Adam, R. Non-Typhoidal Salmonella Infection in Children: Influence of Antibiotic Therapy on Postconvalescent Excretion and Clinical Course—A Systematic Review. Antibiotics 2021, 10, 1187. https://doi.org/10.3390/antibiotics10101187
Leinert JL, Weichert S, Jordan AJ, Adam R. Non-Typhoidal Salmonella Infection in Children: Influence of Antibiotic Therapy on Postconvalescent Excretion and Clinical Course—A Systematic Review. Antibiotics. 2021; 10(10):1187. https://doi.org/10.3390/antibiotics10101187
Chicago/Turabian StyleLeinert, Johanna L., Stefan Weichert, Alexander J. Jordan, and Rüdiger Adam. 2021. "Non-Typhoidal Salmonella Infection in Children: Influence of Antibiotic Therapy on Postconvalescent Excretion and Clinical Course—A Systematic Review" Antibiotics 10, no. 10: 1187. https://doi.org/10.3390/antibiotics10101187
APA StyleLeinert, J. L., Weichert, S., Jordan, A. J., & Adam, R. (2021). Non-Typhoidal Salmonella Infection in Children: Influence of Antibiotic Therapy on Postconvalescent Excretion and Clinical Course—A Systematic Review. Antibiotics, 10(10), 1187. https://doi.org/10.3390/antibiotics10101187