
Stigmatization toward People with Anorexia Nervosa, Bulimia Nervosa, and Binge Eating Disorder: A Scoping Review

 , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Stigma and Mental Disorders
1.2. Stigma and Eating Disorders
1.3. Aims
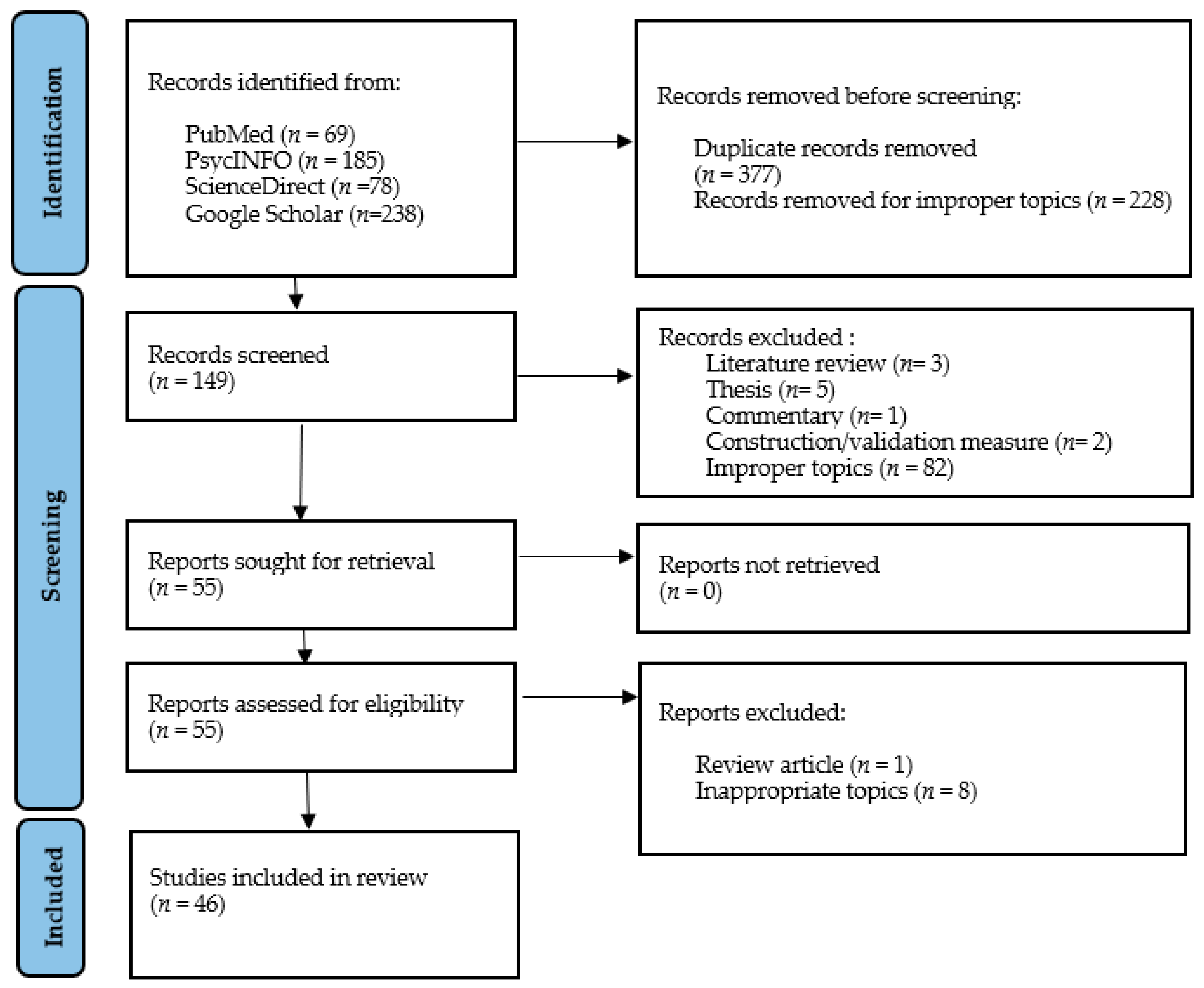
2. Methods
2.1. Eligibility Criteria
2.2. Information Sources, Search, and Study Selection
2.3. Data Extraction
2.4. Risk of Bias
3. Results
3.1. Characteristics of Included Studies
3.2. Content of Stigma
3.2.1. Stereotypes
3.2.2. Prejudice
3.2.3. Discrimination
3.3. Distribution of Stigma
3.3.1. Most Stigmatizing Individuals
3.3.2. Least Stigmatizing Individuals
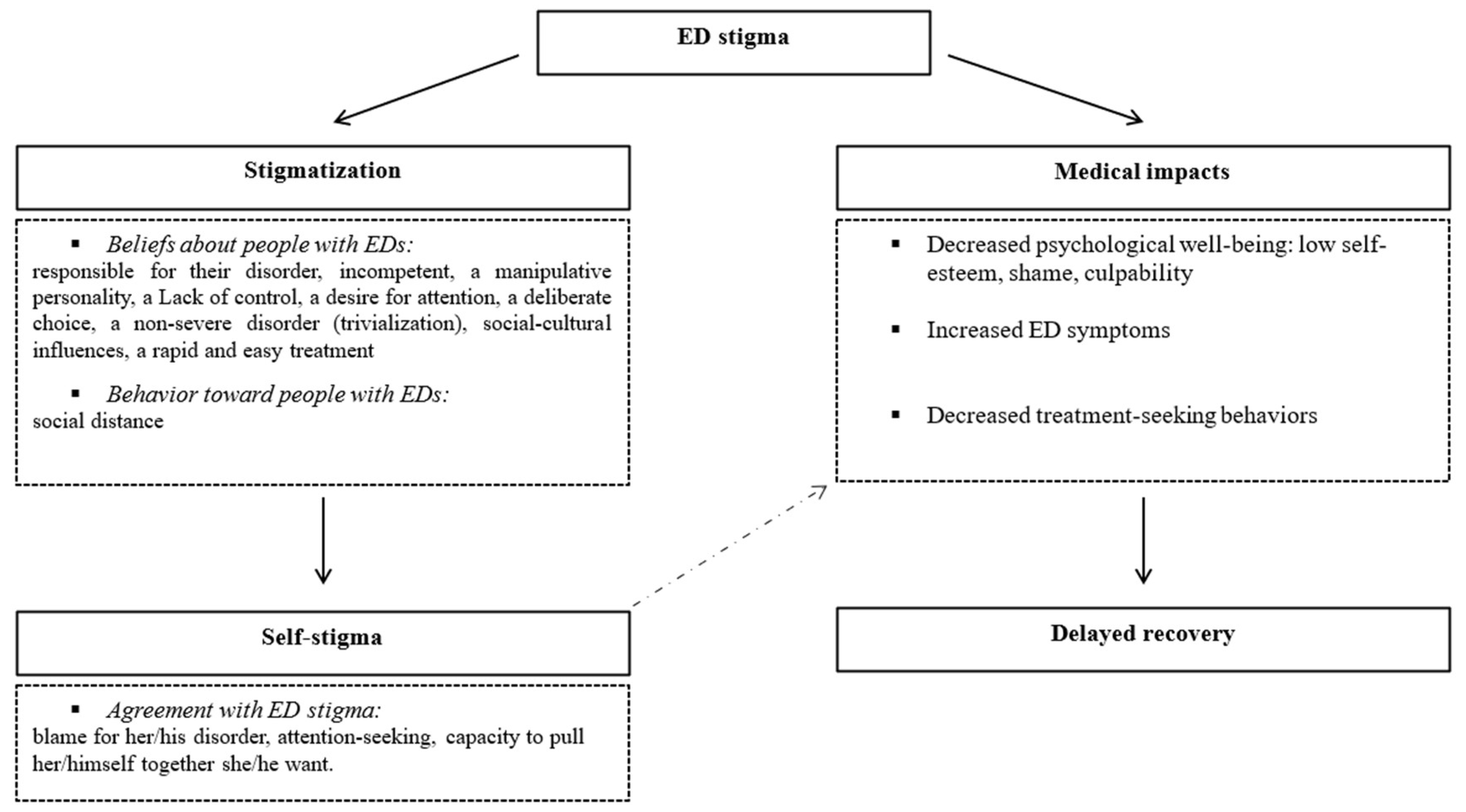
3.4. Consequences of Stigma
3.4.1. Stigma Perception
3.4.2. Self-Stigma
3.4.3. Impact on ED Symptoms and Severity
4. Discussion
4.1. Present Contributions and Future Research
4.2. Challenges and Opportunities in the Study of ED Stigma
4.3. Clinical Implications
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Reference | Tools |
|---|---|
| [29] | Vignette paradigm Twenty-item characteristics scale Level of interpersonal discomfort scale Opinion scale |
| [32] | Vignette paradigm Affective reaction scale Social distance scale Causal attribution |
| [28] | Vignette paradigm Items of: Biological attribution scale Vanity attitude scale Self-responsibility attribution scale Admiration reaction scale Sympathy reaction scale Anger reaction scale Coercion into treatment scale Imitation scale Social distance scale |
| [49] | Vignette paradigm Semantic differential scale |
| [50] | Vignette paradigm Items of the attributional model |
| [51] | Vignette paradigm Characteristics scale Affective reactions scale and social distance scale Blame attribution scale Balanced inventory of desirable responding Item for assumptions about weight status associated with BED |
| [52] | Vignette paradigm |
| [53] | Items created by authors |
| [1] | Vignette paradigm Universal stigma scale Marlowe–Crowne Social Desirability Scale |
| [54] | Vignette paradigm Twenty-item universal measure of bias Eleven-item universal stigma Sscale |
| [55] | Items based on DSM-5 diagnostic criteria Items based on Crisp et al., 2000; Currin, Waller, and Schmidt, 2009; Green, Johnston, Cabrini, Fornai, and Kendrick, 2008; Hay et al., 2007; Jones, Saeidi, and Morgan, 2012; NCCMH, 2004 |
| [2] | Vignette paradigm Universal stigma scale Item from Ebneter and Latner (2013) for lack of self-discipline German version (Angermeyer and Matschinger, 2005) of the seven-item scale developed by Link et al. (1987) for desire for social distance |
| [56] | Vignette paradigm Twelve-item illness perceptions questionnaire Item for social distance |
| [30] | Vignette paradigm Measures based on Jorm et al. (1999); Crisp et al. (2000); Corrigan et al. (2003); Mond et al. (2004a) Level of familiarity questionnaire SCOFF questionnaire (Sick-Control-One Stone-Fat-Food) |
| [57] | Vignette paradigm Items of: Opinions scale Characteristics scale Affective reaction scale Social distance scale Level of interpersonal discomfort scale Perception of community norms Measure of personal acquaintance |
| [58] | Vignette paradigm Measures created by Crisp et al. (2000), Mond et al. (2006); Roehrig and McLean (2010); Stewart et al. (2006) |
| [59] | Items of the opinions scale Items of the international research on personal stigma |
| [27] | Vignette paradigm Items of Dejong 1980; Heblet and Mannix, 2003 |
| [60] | Eating disorder examination questionnaire (EDE-Q) General psychological distress (K10) Medical outcome study short form (SF-12) Vignette paradigm Semi-structured interview |
| [61] | Vignette paradigm Semi-structured interview |
| [31] | Stigmatizing attitudes and beliefs about BN |
| [47] | Stigmatizing attitudes and beliefs about BN Level of familiarity questionnaire Eating disorder examination questionnaire (EDE-Q) |
| [25] | Stigmatizing attitudes and beliefs about BN Stigmatizing attitudes and beliefs about AN |
| [46] | Items adapted from Currin et al. 2009 Items derived from the illness perception questionnaire |
| [26] | Italian version of the McLean SAB-BN-ITA for BN and adapted for AN |
| [33] | Vignette paradigm Universal measure of bias Universal stigma scale Items for psychopathology perceived based on previous works. |
| [62] | Vignette paradigm Items based on perceptions of severity, Australian Bureau of Statistics, 2011; Mond and Arrighi 2011; Mond et al. 2004 |
| [3] | Vignette paradigm Illness perceptions questionnaire |
| [63] | Vignette paradigm Illness perceptions questionnaire Affective reaction and personality characteristics, adapted from Penn et al. (1994) |
| [7] | Causal attributions scale Opinions scale Eating disorder stigma scale Characteristics scale Affective reaction scale |
| [64] | Unknow |
| [65] | Vignette paradigm |
| [66] | Levels of contact report Vignette paradigm Attribute rating scale Eating attitude test |
| [67] | Interview Vignette paradigm |
| [68] | Vignette paradigm Depression stigma scale Opinion scale Just world scale Marlowe–Crowne Social Desirability Scale |
| [8] | Masculine norms inventory 46 Conformity to feminine norms inventory 45 Vignette paradigm Items created by Crisp et al., 2000; Ebneter and Latner 2013; Griffiths et al. 2015; Roehrig and McLean 2010; Stewart et al. 2006 Modified version of the level of contact scale Twelve-item eating disorder examination questionnaire |
| [6] | Items of: Devaluation–discrimination scale The consumers’ experience of stigma questionnaire Opinions scale Revised illness perception questionnaire |
| [69] | Semi-structured interview |
| [42] | Eating disorder examination questionnaire (EDE-Q) Devaluation of consumer scale Devaluation of consumer families scale Internalized stigma of mental illness Rosenberg Self-Esteem Scale General self-efficacy scale Recovery assessment scale |
| [70] | Semi-structured interview |
| [71] | Semi-structured interview based on Darcy et al. 2010; Easter, 2012 |
| [72] | Eating attitude test (EAT-26) Self-stigma seeking help scale Attitude toward seeking professional psychological help—short gorm Disclosure expectations scale |
| [73] | Five-subscale internalized stigma of mental illness scale Eating disorder examination questionnaire (EDE-Q) Self-stigma of seeking help scale Twenty-one-item depression anxiety stress scale |
| [5] | Self-stigma of seeking help scale Twenty-one-item depression anxiety stress scale Ten-item self-esteem scale Eating disorder examination questionnaire (EDE-Q) |
| [74] | Self-stigma of seeking help scale Perceived discrimination and devaluation scale Eating disorder examination questionnaire (EDE-Q) |
| [75] | Eating disorder examination questionnaire (EDE-Q) Discrimination exposure subscale of the internalized stigma of mental illness scale Alienation subscale of the modified internalized stigma of mental illness scale (ISMI) Social withdrawal subscale of the modified ISMI |
Appendix B
| Anorexia Nervosa (AN) | Bulimia Nervosa (BN) | Binge Eating Disorder (BED) | |
|---|---|---|---|
| STEREOTYPES | |||
| Responsibility | Responsible for their disorder, to blame for their disorder | ||
| Character traits | Self-destructive, dangerous, incompetent, able to pull themselves together, difficult to talk to, attention-seeking | Self-destructive | Larger body, less desirable personality traits than non-BED individuals, |
| Gender attribution | Women | Inconclusive | Men (non-significant) |
| Disorder severity and control | Not a very severe disorder, low level of minimization, low perception of benefits | Little minimization, little perception of benefits, a severe disorder, difficult to treat | |
| Supposed causes Internal | Lack of self-discipline, desire for attention, vanity | Lacking self-discipline, having low self-esteem | Lacking self-discipline, self-control, and willpower |
| External | Lacking social support and parental support, sociocultural influences (media). | Lacking social support and parental support, sexual abuse, overweight/obesity during childhood/adolescence, sociocultural influences (media). | Lacking social support |
| PREJUDICE | |||
| Emotions involved | Desire to imitate, admiration, attractiveness, irritation, anger, little sympathy, discomfort in interaction | Desire to imitate, sympathy | Negative reactions, greater prejudice for BED than for non-BED individuals |
| DISCRIMINATION | |||
| Behaviors involved | Social distance, reluctance to offer work | Social Distance | Social distance (but not always observed) |
| COMPARISON BETWEEN EDs | |||
| More self-discipline than BN/BED, More distrustful than BED | More to blame for their disorder, more lack of discipline, more self-destructive, less admirable, and less desire for social distance than AN, More severe and more distrustful than BED | More responsible, lacking willpower/self-discipline/control, more negative reactions than AN/BN, but perceived as more attractive and associated with fewer negative character traits and less desire for social distance. No attribution to poor parental support | |
| COMPARISON WITH OTHER MENTAL DISORDERS | |||
| More responsible but less control, distrust, and desire for social distance than depression or MDE; a longer illness than depression; fewer positive reactions | |||
| More negative assessment; Less intelligent, more driven, more disciplined, more enthusiastic, and less lazy than depression, evoking more anger but also more admiration; Greater lack of social support, parental support, and self-discipline than schizophrenia, but perceived as less dangerous, more able to pull themselves together, their condition is less likely to be attributed to genetic and biological factors, and people feel less discomfort in interaction; More perceived as a psychopathology than ARFID and other eating problems | More friendly attitudes than depression | More negative assessment; More personal control and less reliable than depression; More perceived as a psychopathology than ARFID and other eating problems; More negative traits and more blame for obesity without BED than obesity with BED | |
| COMPARISON WITH OTHER PHYSICAL DISORDERS | |||
| Less responsibility but more distrust and more desire for social distance than obesity; more negative assessment; fewer positive reactions | |||
| More able to pull themselves together than asthma; Greater lack of social support, parental support, and self-discipline than asthma and mononucleosis; Condition less likely to be attributed to genetic and biological factors than asthma, mononucleosis, obesity, and skin cancer; More social distance than obesity and skin cancer | More personal control than type 1 diabetes | ||
| HEALTHCARE PROFESSIONALS | |||
| Beliefs | Responsible for their condition, manipulative, disrespectful, deceitful, non-compliant with treatment; Fear, stress, anger, exasperation, displeasure, discomfort, frustration, preference to treat other patients, decreased motivation to treat | ||
| Unreliable | |||
| Emotions/behaviors | More reluctance to manage than type 1 diabetes | More negative reaction than cocaine users and healthy athletes | |
References
- Ebneter, D.S.; Latner, J.D. Stigmatizing attitudes differ across mental health disorders: A comparison of stigma across eating disorders, obesity, and major depressive disorder. J. Nerv. Ment. Dis. 2013, 201, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Thörel, N.; Thörel, E.; Tuschen-Caffier, B. Differential stigmatization in the context of eating disorders: Less blame might come at the price of greater social rejection. Stigma. Health 2021, 6, 100–112. [Google Scholar] [CrossRef]
- McNicholas, F.; O’Connor, C.; O’Hara, L.; McNamara, N. Stigma and treatment of eating disorders in Ireland: Healthcare professionals’ knowledge and attitudes. Ir. J. Psychol. Med. 2016, 33, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Foran, A.M.; O’Donnell, A.T.; Muldoon, O.T. Stigma of eating disorders and recovery-related outcomes: A systematic review. Eur. Eat. Disord. Rev. 2020, 28, 385–397. [Google Scholar] [CrossRef]
- Griffiths, S.; Mond, J.M.; Murray, S.B.; Touyz, S. The prevalence and adverse associations of stigmatization in people with eating disorders. Int. J. Eat. Disord. 2015, 48, 767–774. [Google Scholar] [CrossRef]
- Maier, A.; Ernst, J.P.; Müller, S.; Gross, D.; Zepf, F.D.; Herpertz-Dahlmann, B.; Hagenah, U. Self-perceived stigmatization in female patients with anorexia nervosa—Results from an explorative retrospective pilot study of adolescents. Psychopathology 2014, 47, 127–132. [Google Scholar] [CrossRef]
- Bannatyne, A.J.; Stapleton, P.B. Attitudes towards anorexia nervosa: Volitional stigma differences in a sample of pre-clinical medicine and psychology students. J. Ment. Health 2016, 26, 442–448. [Google Scholar] [CrossRef] [Green Version]
- Austen, E.; Griffiths, S. Why do men stigmatize individuals with eating disorders more than women? Experimental evidence that sex differences in conformity to gender norms, not biological sex, drive eating disorders’ stigmatization. Eat. Disord. J. Treat. Prev. 2019, 27, 267–290. [Google Scholar] [CrossRef]
- Bucchianeri, M.M.; Eisenberg, M.E.; Neumark-Sztainer, D. Weightism, Racism, Classism, and Sexism: Shared Forms of Harassment in Adolescents. J. Adolesc. Health 2013, 53, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Jones, K.P.; Sabat, I.E.; King, E.B.; Ahmad, A.; McCausland, T.C.; Chen, T. Isms and schisms: A meta-analysis of the prejudice-discrimination relationship across racism, sexism, and ageism. J. Organ. Behav. 2017, 38, 1076–1110. [Google Scholar] [CrossRef]
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Prentice, H., Ed.; Simon and Schuster: Englewood Cliffs, NJ, USA, 1963. [Google Scholar]
- Angermeyer, M.C.; Dietrich, S. Public beliefs about and attitudes towards people with mental illness: A review of population studies. Acta Psychiatr. Scand. 2006, 113, 163–179. [Google Scholar] [CrossRef] [PubMed]
- Crisp, A.H.; Gelder, M.G.; Rix, S.; Meltzer, H.I.; Rowlands, O.J. Stigmatisation of people with mental illnesses. Br. J. Psychiatry 2000, 177, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Kowert, R.; Griffiths, M.D.; Oldmeadow, J.A. Geek or Chic? Emerging Stereotypes of Online Gamers. Bull Sci. Technol. Soc. 2012, 32, 471–479. [Google Scholar] [CrossRef]
- Vartanian, L.R. Disgust and perceived control in attitudes toward obese people. Int. J. Obes. 2010, 34, 1302–1307. [Google Scholar] [CrossRef] [Green Version]
- Al Ramiah, A.; Hewstone, M.; Dovidio, J.F.; Penner, L.A. The social psychology of discrimination: Theory, measurement, and consequences. In Making Equality Count: Irish and International Approaches to Measuring Discrimination; Russell, H., Bond, L., McGinnity, F., Eds.; Liffey Press: Dublin, Ireland, 2010; pp. 84–112. [Google Scholar] [CrossRef]
- Bertrand, M.; Mullainathan, S. Are emily and greg more employable than lakisha and jamal? a field experiment on labor market discrimination. NBER Work. Pap. 2003, 9873, 167–169. [Google Scholar]
- Corrigan, P.W.; Rüsch, N. Mental Illness Stereotypes and Clinical Care: Do People Avoid Treatment Because of Stigma? Psychiatr. Rehabil. Ski. 2002, 6, 312–334. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Watson, A.C. The paradox of self-stigma and mental illness. Clin. Psychol. Sci. Pract. 2002, 9, 35–53. [Google Scholar] [CrossRef]
- Hipes, C.; Lucas, J.; Phelan, J.C.; White, R.C. The stigma of mental illness in the labor market. Soc. Sci. Res. 2016, 56, 16–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Puhl, R.; Suh, Y. Stigma and Eating and Weight Disorders. Curr. Psychiatry Rep. 2015, 17, 1–10. [Google Scholar] [CrossRef]
- Smith, K.E.; Ellison, J.M.; Crosby, R.D.; Engel, S.G.; Mitchell, J.E.; Crow, S.J.; Peterson, C.B.; Le Grange, D.; Wonderlich, S.A. The validity of DSM-5 severity specifiers for anorexia nervosa, bulimia nervosa, and binge-eating disorder. Int. J. Eat. 2017, 50, 1109–1113. [Google Scholar] [CrossRef] [Green Version]
- Ágh, T.; Kovács, G.; Supina, D.; Pawaskar, M.; Herman, B.K.; Vokó, Z.; Sheehan, D.V. A systematic review of the health-related quality of life and economic burdens of anorexia nervosa, bulimia nervosa, and binge eating disorder. Eat. Weight. Disord. 2016, 21, 353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caslini, M.; Crocamo, C.; Dakanalis, A.; Tremolada, M.; Clerici, M.; Carrà, G. Stigmatizing attitudes and beliefs about anorexia and bulimia nervosa among Italian undergraduates. J. Nerv. Ment. Dis. 2016, 204, 916–924. [Google Scholar] [CrossRef] [PubMed]
- Lupo, R.; Zaminga, M.; Carriero, M.C.; Santoro, P.; Artioli, G.; Calabrò, A.; Ilari, F.; Benedetto, A.; Caslini, M.; Clerici, M.; et al. “Eating disorders and related stigma”: Analysis among a population of Italian nursing students. Acta Biomed. 2020, 91, 1–12. [Google Scholar] [CrossRef]
- Varnado-Sullivan, P.J.; Parker, C.C.; Rohner, A. Stigmatization and knowledge of anorexia nervosa. Eat. Weight. Disord. 2020, 25, 601–608. [Google Scholar] [CrossRef]
- Geerling, D.M.; Saunders, S.M. College students’ perceptions of individuals with anorexia nervosa: Irritation and admiration. J. Ment. Health 2015, 24, 83–87. [Google Scholar] [CrossRef]
- Stewart, M.-C.; Keel, P.K.; Schiavo, R.S. Stigmatization of Anorexia Nervosa. Int. J. Eat. Disord. 2006, 39, 320–325. [Google Scholar] [CrossRef]
- Mond, J.M.; Robertson-Smith, G.; Vetere, A. Stigma and eating disorders: Is there evidence of negative attitudes towards anorexia nervosa among women in the community? J. Ment. Health 2006, 15, 519–532. [Google Scholar] [CrossRef]
- McLean, S.A.; Paxton, S.J.; Massey, R.; Hay, P.J.; Mond, J.M.; Rodgers, B. Stigmatizing attitudes and beliefs about bulimia nervosa: Gender, age, education and income variability in a community sample. Int. J. Eat. Disord. 2014, 47, 353–361. [Google Scholar] [CrossRef]
- Zwickert, K.; Rieger, E. Stigmatizing attitudes towards individuals with anorexia nervosa: An investigation of attribution theory. J. Eat. Disord. 2013, 1, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Ellis, J.M.; Essayli, J.H.; Zickgraf, H.F.; Rossi, J.; Hlavka, R.; Carels, R.A.; Whited, M.C. Comparing stigmatizing attitudes toward anorexia nervosa, binge-eating disorder, avoidant-restrictive food intake disorder, and subthreshold eating behaviors in college students. Eat. Behav. 2020, 39, 101443. [Google Scholar] [CrossRef]
- Thompson-Brenner, H.; Satir, D.A.; Franko, D.L.; Herzog, D.B. Clinician Reactions to Patients With Eating Disorders: A review of the Literature. Psychiatr. Serv. 2012, 63, 73–78. [Google Scholar] [CrossRef]
- Rome, E.S.; Ammerman, S. Medical complications of eating disorders: An update. J. Adolesc. Health 2003, 33, 418–426. [Google Scholar] [CrossRef]
- Hart, L.M.; Granillo, M.T.; Jorm, A.F.; Paxton, S.J. Unmet need for treatment in the eating disorders: A systematic review of eating disorder specific treatment seeking among community cases. Clin. Psychol. Rev. 2011, 31, 727–735. [Google Scholar] [CrossRef]
- Brewis, A.A. Social Science & Medicine Stigma and the perpetuation of obesity. Soc. Sci. Med. 2014, 118, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Brochu, P.M.; Esses, V.M. What’s in a Name? The Effects of the Labels “Fat” Versus “Overweight” on Weight Bias. J. Appl. Soc. Psychol. 2011, 41, 1981–2008. [Google Scholar] [CrossRef]
- Lewis, S.; Thomas, S.L.; Blood, R.W.; Castle, D.J.; Hyde, J.; Komesaroff, P.A. How do obese individuals perceive and respond to the different types of obesity stigma that they encounter in their daily lives? A qualitative study. Soc. Sci. Med. 2011, 73, 1349–1356. [Google Scholar] [CrossRef] [PubMed]
- Vartanian, L.R.; Shaprow, J.G. Effects of weight stigma on exercise motivation and behavior: A preliminary investigation among college-aged females. J. Health Psychol. 2008, 13, 131–138. [Google Scholar] [CrossRef]
- Vartanian, L.R.; Porter, A.M. Weight stigma and eating behavior: A review of the literature. Appetite 2016, 102, 3–14. [Google Scholar] [CrossRef]
- Dimitropoulos, G.; Mccallum, L.; Colasanto, M.; Freeman, V.E.; Gadalla, T. The effects of stigma on recovery attitudes in people with anorexia nervosa in intensive treatment. J. Nerv. Ment. Dis. 2016, 204, 370–380. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larson, J.E.; Corrigan, P. The Stigma of Families with Mental Illness. Acad. Psychiatry 2008, 32, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Liegghio, M. ‘Not a good person’: Family stigma of mental illness from the perspectives of young siblings. Child. Fam. Soc. Work 2017, 22, 1237–1245. [Google Scholar] [CrossRef]
- Anderson, K.; Accurso, E.C.; Kinasz, K.R.; Le Grange, D. Residents’ and Fellows’ Knowledge and Attitudes about Eating Disorders at an Academic Medical Center. Acad. Psychiatry 2016, 41, 381–384. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, R.F.; Paxton, S.J.; McLean, S.A.; Massey, R.; Mond, J.M.; Hay, P.J.; Rodgers, B. Stigmatizing attitudes and beliefs toward bulimia nervosa: The importance of knowledge and eating disorder symptoms. J. Nerv. Ment. Dis. 2015, 203, 259–263. [Google Scholar] [CrossRef]
- Furnham, A. Belief in a just world: Research progress over the past decade. Pers. Individ. Dif. 2003, 34, 795–817. [Google Scholar] [CrossRef]
- Yu, J.; Hildebrandt, T.; Lanzieri, N. Healthcare professionals’ stigmatization of men with anabolic androgenic steroid use and eating disorders. Body Image. 2015, 15, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, A.A.; Lowe, J.D. With age comes responsibility: Changes in stigma for boys/men with bulimia nervosa. Eat. Weight Disord. 2020, 25, 1525–1532. [Google Scholar] [CrossRef]
- Hollett, K.B.; Carter, J.C. Separating Binge Eating Disorder Stigma and Weight Stigma: A Vignette Study. Int. J. Eat. Disord. 2021, 54, 755–763. [Google Scholar] [CrossRef]
- Roehrig, J.P.; McLean, C.P. A comparison of stigma toward eating disorders versus depression. Int. J. Eat. Disord. 2010, 43, 671–674. [Google Scholar] [CrossRef]
- Raveneau, G.; Feinstein, R.; Rosen, L.M.; Fisher, M. Attitudes and knowledge levels of nurses and residents caring for adolescents with an eating disorder. Int. J. Adolesc. Med. Health 2014, 26, 131–136. [Google Scholar] [CrossRef]
- Murakami, J.M.; Essayli, J.H.; Latner, J.D. The relative stigmatization of eating disorders and obesity in males and females. Appetite 2016, 102, 77–82. [Google Scholar] [CrossRef]
- Seah, X.Y.; Tham, X.C.; Kamaruzaman, N.R.; Yobas, P.K. Nurses’ perception of knowledge, attitudes and reported practice towards patients with eating disorders: A concurrent mixed-methods study. Arch. Psychiatr. Nurs. 2018, 32, 133–151. [Google Scholar] [CrossRef] [PubMed]
- Ogutlu, H.; McNicholas, F. Stigma and Treatment of Eating Disorders in School Counselors in Turkey (STED-SCIT). Psychiatry Behav. Sci. 2021, 11, 8. [Google Scholar] [CrossRef]
- Stewart, M.-C.; Schiavo, R.S.; Herzog, D.B.; Franko, D.L. Stereotypes, Prejudice and Discrimination of Women with Anorexia Nervosa. Eur. Eat. Disord. Rev. 2008, 16, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, S.; Mond, J.M.; Murray, S.B.; Touyz, S. Young peoples’ stigmatizing attitudes and beliefs about anorexia nervosa and muscle dysmorphia. Int. J. Eat. Disord. 2014, 47, 189–195. [Google Scholar] [CrossRef] [PubMed]
- McArdle, S.; Meade, M.M.; Burrows, E. Service providers’ attitudes toward athletes with eating disorders. Clin. J. Sport. Med. 2018, 28, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Mond, J.M.; Hay, P.J.; Rodgers, B.; Owen, C.; Beumont, P.J.V. Beliefs of women concerning the severity and prevalence of bulimia nervosa. Soc. Psychiatry Psychiatr. Epidemiol. 2004, 39, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Mond, J.M.; Hay, P.J.; Rodgers, B.; Owen, C.; Beumont, P.J.V. Beliefs of women concerning causes and risk factors for bulimia nervosa. Aust. N. Z. J Psychiatry 2004, 38, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.; Gratwick-Sarll, K.; Bentley, C.; Harrison, C.; Mond, J. Adolescents perception of the severity of binge eating disorder: A population-based study. J. Ment. Health 2015, 25, 16–22. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, C.; McNamara, N.; O’Hara, L.; McNicholas, F. Eating disorder literacy and stigmatising attitudes towards anorexia, bulimia and binge eating disorder among adolescents. Adv. Eat. Disord. Theory Res. Pract. 2016, 4, 125–140. [Google Scholar] [CrossRef] [Green Version]
- Crisp, A.H. Stigmatization of and discrimination against people with eating disorders including a report of two nationwide surverys. Eur. Eat. Disord. Rev. 2005, 13, 147–152. [Google Scholar] [CrossRef]
- Mond, J.M.; Arrighi, A. Gender differences in perceptions of the severity and prevalence of eating disorders. Early Interv. Psychiatry 2011, 5, 41–49. [Google Scholar] [CrossRef]
- Wingfield, N.; Kelly, N.; Serdar, K.; Shivy, V.A.; Mazzeo, S.E. College students’ perceptions of individuals with anorexia and bulimia nervosa. Int. J. Eat. Disord. 2011, 44, 369–375. [Google Scholar] [CrossRef] [Green Version]
- Makowski, A.C.; Mnich, E.E.; Angermeyer, M.C.; Löwe, B.; Von dem Knesebeck, O. Sex differences in attitudes towards females with eating disorders. Eat. Behav. 2015, 16, 78–83. [Google Scholar] [CrossRef]
- Ebneter, D.S.; Latner, J.D.; O’Brien, K.S. Just world beliefs, causal beliefs, and acquaintance: Associations with stigma toward eating disorders and obesity. Pers. Individ. Dif. 2011, 51, 618–622. [Google Scholar] [CrossRef]
- Dimitropoulos, G.; Freeman, V.E.; Muskat, S.; Domingo, A.; McCallum, L. You dont have anorexia, you just want to look like a celebrity": Perceived stigma in individuals with anorexia nervosa. J. Ment. Health 2015, 25, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Pettersen, G.; Rosenvinge, J.H.; Ytterhus, B. The “double life” of Bulimia: Patients’ experiences in daily life interactions. Eat. Disord. J. Treat. Prev. 2008, 16, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Bannatyne, A.J.; Stapleton, P.B. Eating Disorder Patient Experiences of Volitional Stigma Within the Healthcare System and Views on Biogenetic Framing: A Qualitative Perspective. Aust. Psychol. 2016, 53, 325–338. [Google Scholar] [CrossRef]
- Hackler, A.H.; Vogel, D.L.; Wade, N.G. Attitudes Toward Seeking Professional Help for an Eating Disorder: The Role of stigma and anticipated outcomes. J. Couns. Dev. 2010, 88, 424–432. [Google Scholar] [CrossRef]
- Griffiths, S.; Mond, J.M.; Murray, S.B.; Thornton, C.; Touyz, S. Stigma resistance in eating disorders. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, S.; Mond, J.M.; Li, Z.; Gunatilake, S.; Murray, S.B.; Sheffield, J.; Touyz, S. Self-stigma of seeking treatment and being male predict an increased likelihood of having an undiagnosed eating disorder. Int. J. Eat. Disord. 2015, 48, 775–778. [Google Scholar] [CrossRef]
- Griffiths, S.; Mitchison, D.; Murray, S.B.; Mond, J.M.; Bastian, B.B. How might eating disorders stigmatization worsen eating disorders symptom severity? Evaluation of a stigma internalization model. Int. J. Eat. Disord. 2018, 51, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, P.W.; Watson, A.C.; Warpinski, A.C.; Gracia, G. Implications of Educating the Public on Mental Illness, Violence, and Stigma. Psychiatr. Serv. 2004, 55, 577–580. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, R.; Fialho, A.; Wijetunge, A.; Checinski, K.; Surgenor, T. The stigmatisation of psychiatric illness: The attitudes of medical students and doctors in a London teaching hospital. Psychiatr. Bull 2002, 26, 178–181. [Google Scholar] [CrossRef] [Green Version]
- Larose, J.G.; Gorin, A.A.; Clarke, M.M.; Wing, R.R. Beliefs about weight gain among young adults: Potential challenges to prevention. Obesity 2011, 19, 1901–1904. [Google Scholar] [CrossRef]
- Miller, E.; Halberstadt, J. Media consumption, body image and thin ideals in New Zealand men and women. N. Z. J Psychol. 2005, 34, 189–195. [Google Scholar]
- Foster, G.D.; Wadden, T.A.; Makris, A.P.; Davidson, D.; Sanderson, R.S.; Allison, D.B.; Kessler, A. Primary care physicians’ attitudes about obesity and its treatment. Obes. Res. 2003, 11, 1168–1177. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Schwartz, M.B.; Brownell, K.D. Impact of perceived consensus on stereotypes about obese people: A new approach for reducing bias. Health Psychol. 2005, 24, 517–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horsburgh-McLeod, G.; Latner, J.D.; O’Brien, K.S. Unprompted generation of obesity stereotypes. Eat. Weight. Disord. 2009, 14, 153–157. [Google Scholar] [CrossRef]
- Musher-Eizenman, D.R.; Holub, S.C.; Miller, A.B.; Goldstein, S.E.; Edwards-Leeper, L. Body size stigmatization in preschool children: The role of control attributions. J. Pediatr. Psychol. 2004, 29, 613–620. [Google Scholar] [CrossRef] [Green Version]
- Agerström, J.; Rooth, D.O. The Role of Automatic Obesity Stereotypes in Real Hiring Discrimination. J. Appl. Psychol. 2011, 96, 790–805. [Google Scholar] [CrossRef]
- Wott, C.B.; Carels, R.A. Overt weight stigma, psychological distress and weight loss treatment outcomes. J. Health. Psychol. 2010, 15, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Ashmore, J.A.; Friedman, K.E.; Reichmann, S.K.; Musante, G.J. Weight-based stigmatization, psychological distress, & binge eating behavior among obese treatment-seeking adults. Eat. Behav. 2008, 9, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Friedman, K.E.; Ashmore, J.A.; Applegate, K.L. Recent experiences of weight-based stigmatization in a weight loss surgery population: Psychological and behavioral correlates. Obesity 2008, 16, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Galbraith, K.; Elmquist, J.; White, M.A.; Grilo, C.M.; Lydecker, J.A. Weighty decisions: How symptom severity and weight impact perceptions of bulimia nervosa. Int. J. Eat. Disord. 2019, 52, 1035–10411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfoukha, M.M.; Hamdan-Mansour, A.M.; Banihani, M.A. Social and Psychological Factors Related to Risk of Eating Disorders Among High School Girls. J. Sch. Nurs. 2019, 35, 169–177. [Google Scholar] [CrossRef]
- National Institute of Mental Health. Eating Disorders Statistics Reports for the U.S. 2017. Available online: https://www.nimh.nih.gov/health/statistics/eating-disorders.shtml (accessed on 24 April 2020).
- O’Hara, S.K.; Smith, K.C. Presentation of eating disorders in the news media: What are the implications for patient diagnosis and treatment? Patient Educ. Couns. 2007, 68, 43–51. [Google Scholar] [CrossRef]
- Rao, H.; Mahadevappa, H.; Pillay, P.; Sessay, M.; Abraham, A.; Luty, J. A study of stigmatized attitudes towards people with mental health problems among health professionals. J. Psychiatr. Ment. Health Nurs. 2009, 16, 279–284. [Google Scholar] [CrossRef]
- Chambliss, H.O.; Finley, C.E.; Blair, S.N. Attitudes toward Obese Individuals among Exercise Science Students. Med. Sci. Sports Exerc. 2004, 36, 468–474. [Google Scholar] [CrossRef]
- Schwartz, M.B.; Chambliss, H.O.N.; Brownell, K.D.; Blair, S.N.; Billington, C. Weight Bias among Health Professionals Specializing in Obesity. Obes. Res. 2003, 11, 1033–1039. [Google Scholar] [CrossRef]
- Smink, F.R.E.; Van Hoeken, D.; Hoek, H.W. Epidemiology of eating disorders: Incidence, prevalence and mortality rates. Curr. Psychiatry Rep. 2012, 14, 406–414. [Google Scholar] [CrossRef] [Green Version]
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S. Mortality rates in patients with anorexia nervosa and other eating disorders: A meta-analysis of 36 studies. Arch. Gen. Psychiatry 2011, 68, 724–731. [Google Scholar] [CrossRef] [Green Version]
- Chesney, E.; Goodwin, G.M.; Fazel, S. Risks of all-cause and suicide mortality in mental disorders: A meta-review. World Psychiatry 2014, 13, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Allport, G.W. Nature of Prejudice; Addison-Wesley: Reading, MA, USA, 1954. [Google Scholar]
- Evans-Lacko, S.; Brohan, E.; Mojtabai, R.; Thornicroft, G. Association between public views of mental illness and self-stigma among individuals with mental illness in 14 European countries. Psychol. Med. 2012, 42, 1741–1752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, T.B.; Mozdzierz, P.; Wang, S.; Smith, K.E. Discrimination and Eating Disorder Psychopathology: A Meta-Analysis. Behav. Ther. 2021, 52, 406–417. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, P.W.; Rao, D. On the self-stigma of mental illness: Stages, disclosure, and strategies for change. Can. J. Psychiatry 2012, 57, 464–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rüsch, N.; Angermeyer, M.C.; Corrigan, P.W. Mental illness stigma: Concepts, consequences, and initiatives to reduce stigma. Eur. Psychiatry 2005, 20, 529–539. [Google Scholar] [CrossRef]
- Crowne, D.P.; Marlowe, D. A new scale of social desirability independent of psychopathology. J. Consult. Psychol. 1960, 24, 349–354. [Google Scholar] [CrossRef] [Green Version]
- Peris, T.S.; Teachman, B.A.; Nosek, B.A. Implicit and explicit stigma of mental illness: Links to clinical care. J. Nerv. Ment. Dis. 2008, 196, 752–760. [Google Scholar] [CrossRef] [Green Version]
- Dabby, L.; Tranulis, C.; Kirmayer, L.J. Explicit and implicit attitudes of canadian psychiatrists toward people with mental illness. Can. J. Psychiatry 2015, 60, 451–459. [Google Scholar] [CrossRef] [Green Version]
- Teachman, B.A.; Wilson, J.G.; Komarovskaya, I. Implicit and explicit stigma of mental illness in diagnosed and healthy samples. J. Soc. Clin. Psychol. 2006, 25, 75–95. [Google Scholar] [CrossRef] [Green Version]
- Kopera, M.; Suszek, H.; Bonar, E.; Myszka, M.; Gmaj, B.; Ilgen, M.; Wojnar, M. Evaluating Explicit and Implicit Stigma of Mental Illness in Mental Health Professionals and Medical Students. Commun. Ment. Health J. 2015, 51, 628–634. [Google Scholar] [CrossRef] [Green Version]
- Cheon, B.K.; Chiao, J.Y. Cultural Variation in Implicit Mental Illness Stigma Bobby. J. Cross. Cult. Psychol. 2012, 43, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, A.; Hilbert, A. A novel measure to assess self-discrimination in binge-eating disorder and obesity. Int. J. Obes. 2015, 39, 368–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalky, H.F. Mental Illness Stigma Reduction Interventions: Review of Intervention Trials. West. J. Nurs. Res. 2012, 34, 520–547. [Google Scholar] [CrossRef] [PubMed]
- Thornicroft, G.; Mehta, N.; Clement, S.; Evans-Lacko, S.; Doherty, M.; Rose, D.; Koschorke, M.; Shidhaye, R.; O’Reilly, C.; Henderson, C. Evidence for effective interventions to reduce mental-health-related stigma and discrimination. Lancet 2016, 387, 1123–1132. [Google Scholar] [CrossRef]
- Spagnolo, A.B.; Murphy, A.A.; Librera, L.A. Reducing stigma by meeting and learning from people with mental illness. attitudes towards me. Psycnet. Apa. Org. 2008, 31, 186–193. [Google Scholar]
- Crisafulli, M.A.; Thompson-Brenner, H.; Franko, D.L.; Eddy, K.T.; Herzog, D.B. Stigmatization of anorexia nervosa: Characteristics and response to intervention. J. Soc. Clin. Psychol. 2010, 29, 756–770. [Google Scholar] [CrossRef]
- Crisafulli, M.A.; Von Holle, A.; Bulik, C.M. Attitudes towards anorexia nervosa: The impact of framing on blame and stigma. Int. J. Eat. Disord. 2008, 41, 333–339. [Google Scholar] [CrossRef]
- Iles, I.A.; Seate, A.A.; Waks, L. Eating disorder public service announcements: Analyzing effects from an intergroup affect and stereotype perspective. Health Educ. 2016, 116, 476–488. [Google Scholar] [CrossRef]
- Iles, I.A.; Atwell Seate, A.; Waks, L. Stigmatizing the other: An exploratory study of unintended consequences of eating disorder public service announcements. J. Health Psychol. 2017, 22, 120–131. [Google Scholar] [CrossRef] [PubMed]
- Christofi, M.; Michael-Grigoriou, D. Virtual reality for inducing empathy and reducing prejudice towards stigmatized groups: A survey. In Proceedings of the 2017 23rd International Conference on Virtual System & Multimedia (VSMM), Dublin, Ireland, 31 October–2 November 2017; IEEE: Piscataway, NJ, USA, 2017. [Google Scholar] [CrossRef]
- Lucksted, A.; Drapalski, A.; Calmes, C.; Forbes, C.; DeForge, B.; Boyd, J. Ending self-stigma: Pilot evaluation of a new intervention to reduce internalized stigma among people with mental illnesses. Psychiatr. Rehabil. J. 2011, 35, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Rüsch, N.; Xu, Z. Strategies to Reduce Mental illness Stigma. In The Stigma of Mental Illness-End of the Story; Springer: Cham, Switzerland, 2017; pp. 451–467. [Google Scholar] [CrossRef]
- Strahan, E.J.; Stillar, A.; Files, N.; Nash, P.; Scarborough, J.; Connors, L.; Gusella, J.; Henderson, K.; Mayman, S.; Marchand, P.; et al. Increasing parental self-efficacy with emotion-focused family therapy for eating disorders: A process model. Pers. Exp. Psychother. 2017, 16, 256–269. [Google Scholar] [CrossRef]
| Reference | Location | Final Sample | Study Design | ED Concerned | ED Stigma |
|---|---|---|---|---|---|
| [29] | USA | 91 Volunteers | Vignette paradigm and questionnaire completion | AN | Content |
| [32] | Australia | 135 College students (only women) | Vignette paradigm and questionnaire completion | AN | Content |
| [28] | USA | 102 Psychology students (only women) | Vignette paradigm and questionnaire completion | AN | Content |
| [49] | USA | 148 Healthcare professionals | Vignette paradigm and questionnaire completion | BN | Content |
| [50] | USA | 360 Psychology students | Vignette paradigm and questionnaire completion | BN | Content |
| [51] | Canada | 421 Adult volunteers | Vignette paradigm and questionnaire completion | BED | Content |
| [52] | USA | 118 Psychology students | Vignette paradigm | AN + BN | Content |
| [53] | USA | 82 Pediatric residents and nurses | Questionnaire completion | AN + BN | Content |
| [1] | USA | 447 Psychology students | Vignette paradigm and questionnaire completion | All EDs | Content |
| [54] | USA | 318 College students | Vignette paradigm and questionnaire completion | All EDs | Content |
| [55] | Singapore | 19 Nurses | Questionnaire completion | All EDs | Content |
| [2] | Germany | 729: 267 college students and 523 nonstudents | Vignette paradigm and questionnaire completion | All EDs | Content |
| [56] | Turkey | 49 school counselor volunteers | Vignette paradigm and questionnaire completion | All EDs | Content |
| [30] | UK | 125 College students (only women) | Vignette paradigm and questionnaire completion | AN | Content Distribution |
| [57] | USA | 80 College students (only women) | Vignette paradigm and questionnaire completion | AN | Content Distribution |
| [58] | Australia | 343 Psychology students | Vignette paradigm and questionnaire completion | AN | Content Distribution |
| [59] | Ireland, UK | 152 Sport-based professionals | Questionnaire completion | AN | Content Distribution |
| [27] | USA | 86 Psychology students | Vignette paradigm and questionnaire completion | AN | Content Distribution |
| [60] | Australia | 208 Australian voters | Vignette paradigm, semi-structured interview, and questionnaire completion | BN | Content Distribution |
| [61] | Australia | 208 Australian voters | Vignette paradigm, semi-structured interview, and questionnaire completion | BN | Content Distribution |
| [31] | Australia | 1828 Australian voters | Questionnaire completion | BN | Content Distribution |
| [47] | Australia | 1828 Australian voters | Questionnaire completion | BN | Content Distribution |
| [25] | Italia | 2109 College students (<30 years) | Questionnaire completion | AN + BN | Content Distribution |
| [46] | USA | 80 Physicians | Questionnaire completion | AN + BN | Content Distribution |
| [26] | Italia | 517 Nursing students | Questionnaire completion | AN + BN | Content Distribution |
| [33] | USA | 1447 Psychology students | Vignette paradigm and questionnaire completion | AN + BED | Content Distribution |
| [62] | Australia | 1135 Adolescent volunteers | Vignette paradigm and questionnaire completion | BN + BED | Content Distribution |
| [3] | Ireland | 171 Healthcare professionals | Vignette paradigm and questionnaire completion | All EDs | Content Distribution |
| [63] | Ireland | 283 Adolescent volunteers | Vignette paradigm and questionnaire completion | All EDs | Content Distribution |
| [7] | Australia | 126 Psychology and physician students | Questionnaire completion | AN | Distribution |
| [64] | UK | ~3500 adult volunteers | Unknown | AN + BN | Distribution |
| [65] | Australia | 402 College students | Vignette paradigm | AN + BN | Distribution |
| [66] | USA | 235 Psychology students | Vignette paradigm and questionnaire completion | AN + BN | Distribution |
| [67] | Germany | 2014 Adult volunteers | Interview and vignette paradigm | AN + BN | Distribution |
| [68] | USA | 447 Psychology students | Vignette paradigm and questionnaire completion | All EDs | Distribution |
| [8] | Australia | 545 Psychology students | Vignette paradigm and questionnaire completion | All EDs | Distribution |
| [6] | Germany | 36 Adolescent patients with EDs (only women) | Questionnaire completion | AN | Consequences |
| [69] | Canada | 19 Patients with EDs (only women) | Semi-structured interview | AN | Consequences |
| [42] | Canada | 36 Patients with EDs (only women) | Questionnaire completion | AN | consequences |
| [70] | Norway | 38 patients with EDs (only women) | Semi-structured interview | BN | Consequences |
| [71] | Australia | 35 Adult volunteers with EDs (only women) | Semi-structured interview | AN + BN | Consequences |
| [72] | USA | 145 Psychology students with EDs | Questionnaire completion | All EDs | Consequences |
| [73] | Australia | 452 Adult volunteers with EDS | Questionnaire completion | All EDs | Consequences |
| [5] | Australia, USA, UK | 317 Adult volunteers with EDs | Questionnaire completion | All EDs | Consequences |
| [74] | Australia, USA, UK | 485 Adult volunteers with EDs (diagnosed and undiagnosed) | Questionnaire completion | All EDs | Consequences |
| [75] | Australia, USA, UK | 260 Adult volunteers with EDs | Questionnaire completion | All EDs | Consequences |
| Variable | Total Number of Studies | Target(s) | Main Results | Reference | |
|---|---|---|---|---|---|
| Most Stigmatizing Group | Least Stigmatizing Group | ||||
| Gender | 14 | EDs/AN/BN/BED | Men | Women | [7,8,25,26,27,31,33,47,58,59,62,65,66,67] |
| Familiarity with EDs | 8 | EDs/AN/BN | Unfamiliar people | Familiar people | [25,26,27,32,46,47,60,61] |
| Age | 4 | AN/BN | Young adults | Old adults | [25,31,61,64] |
| Education | 4 | AN/BN | People with low education | People with high education | [31,60,61,64] |
| Symptoms of EDs | 2 | AN | People with a low level of symptoms | People with a high level of symptoms | [30,66] |
| Degree program | 2 | EDs/AN | Medicine, sociology, education, science, economics, law, and statistics students | Psychology students | [7,25] |
| Income | 2 | AN/BN | People with low income | People with high income | [31,64] |
| Weight category | 1 | AN/BN | Normal-weight and overweight people | Underweight people | [25] |
| Ethnicity | 1 | EDs | African Americans | Caucasian Americans | [66] |
| Information/knowledge about EDs | 1 | EDs | Uninformed people | Informed people | [47] |
| Just world belief | 1 | EDs | Believers | Non-believers | [68] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brelet, L.; Flaudias, V.; Désert, M.; Guillaume, S.; Llorca, P.-M.; Boirie, Y. Stigmatization toward People with Anorexia Nervosa, Bulimia Nervosa, and Binge Eating Disorder: A Scoping Review. Nutrients 2021, 13, 2834. https://doi.org/10.3390/nu13082834
Brelet L, Flaudias V, Désert M, Guillaume S, Llorca P-M, Boirie Y. Stigmatization toward People with Anorexia Nervosa, Bulimia Nervosa, and Binge Eating Disorder: A Scoping Review. Nutrients. 2021; 13(8):2834. https://doi.org/10.3390/nu13082834
Chicago/Turabian StyleBrelet, Lisa, Valentin Flaudias, Michel Désert, Sébastien Guillaume, Pierre-Michel Llorca, and Yves Boirie. 2021. "Stigmatization toward People with Anorexia Nervosa, Bulimia Nervosa, and Binge Eating Disorder: A Scoping Review" Nutrients 13, no. 8: 2834. https://doi.org/10.3390/nu13082834