Sustainability and Kaizen: Business Model Trends in Healthcare



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
- (1)
- contribution to the preservation of nature by limiting the use of resources and other environmental pressures,
- (2)
- reduction of costs to the national economy, and
- (3)
- minimization of social burdens inside and outside the hospital.
2. Materials and Methods
- ▪
- There is a high probability of finding few results with our search criteria.
- ▪
- This first phase should inform the focusing on the best combination of keywords following our research objective.
- (1)
- Kaizen, Lean, hospital, sustainab *: 797 papers.
- (2)
- Kaizen, Lean, health, sustainab *: 895 papers
3. Results
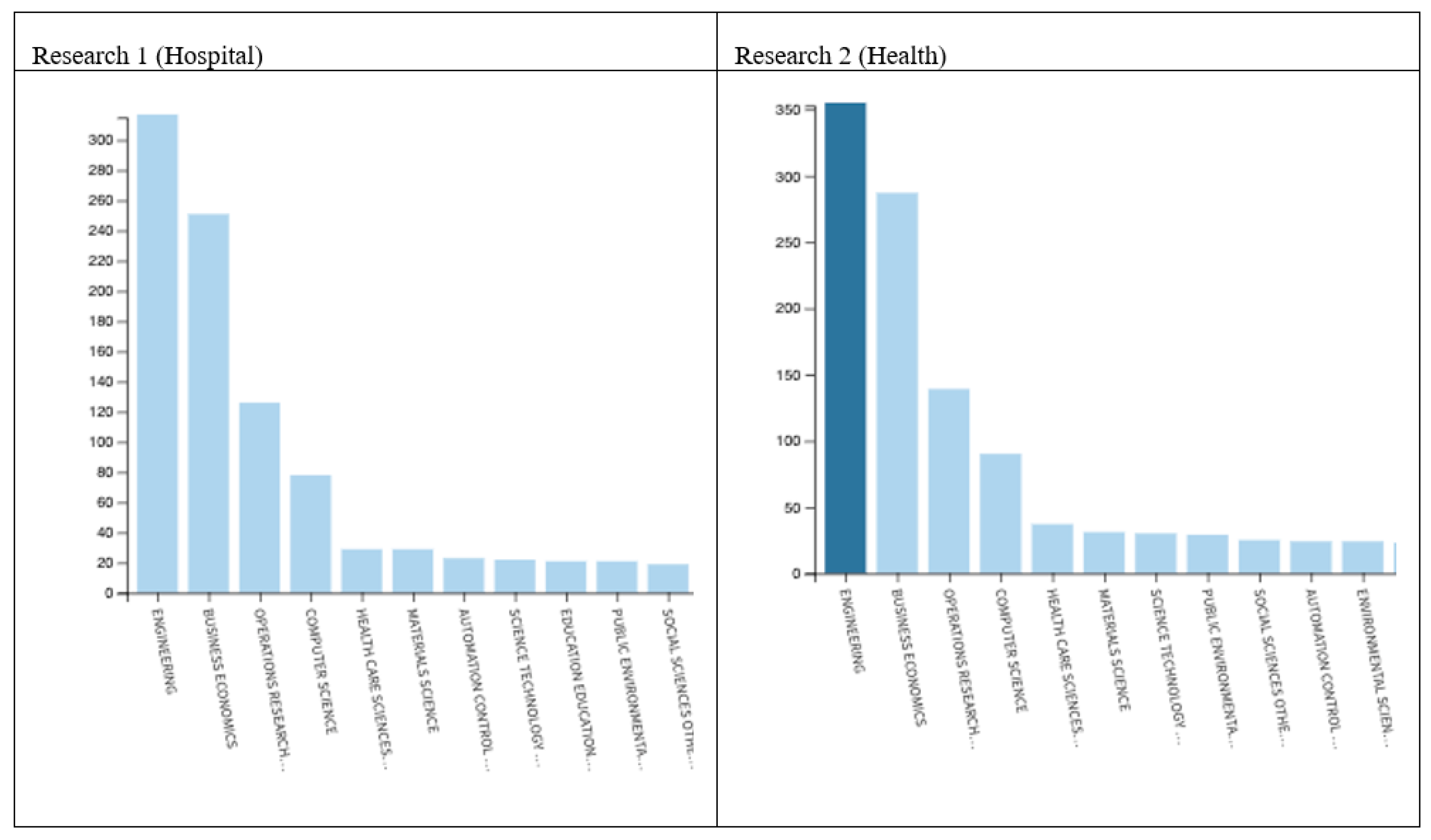
3.1. Web of Science Results
3.2. SCIMAT Results
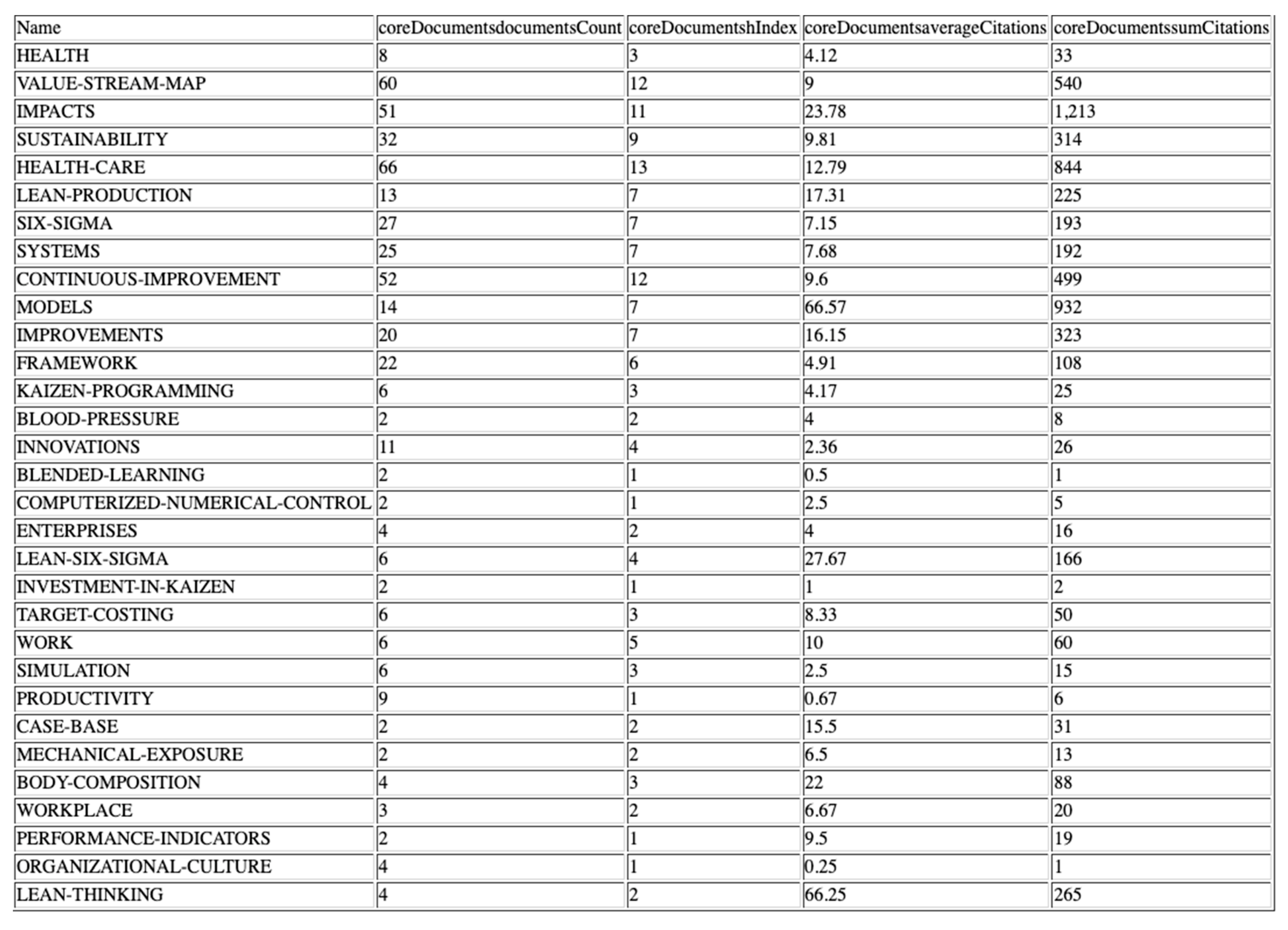
3.2.1. Keyword Analysis
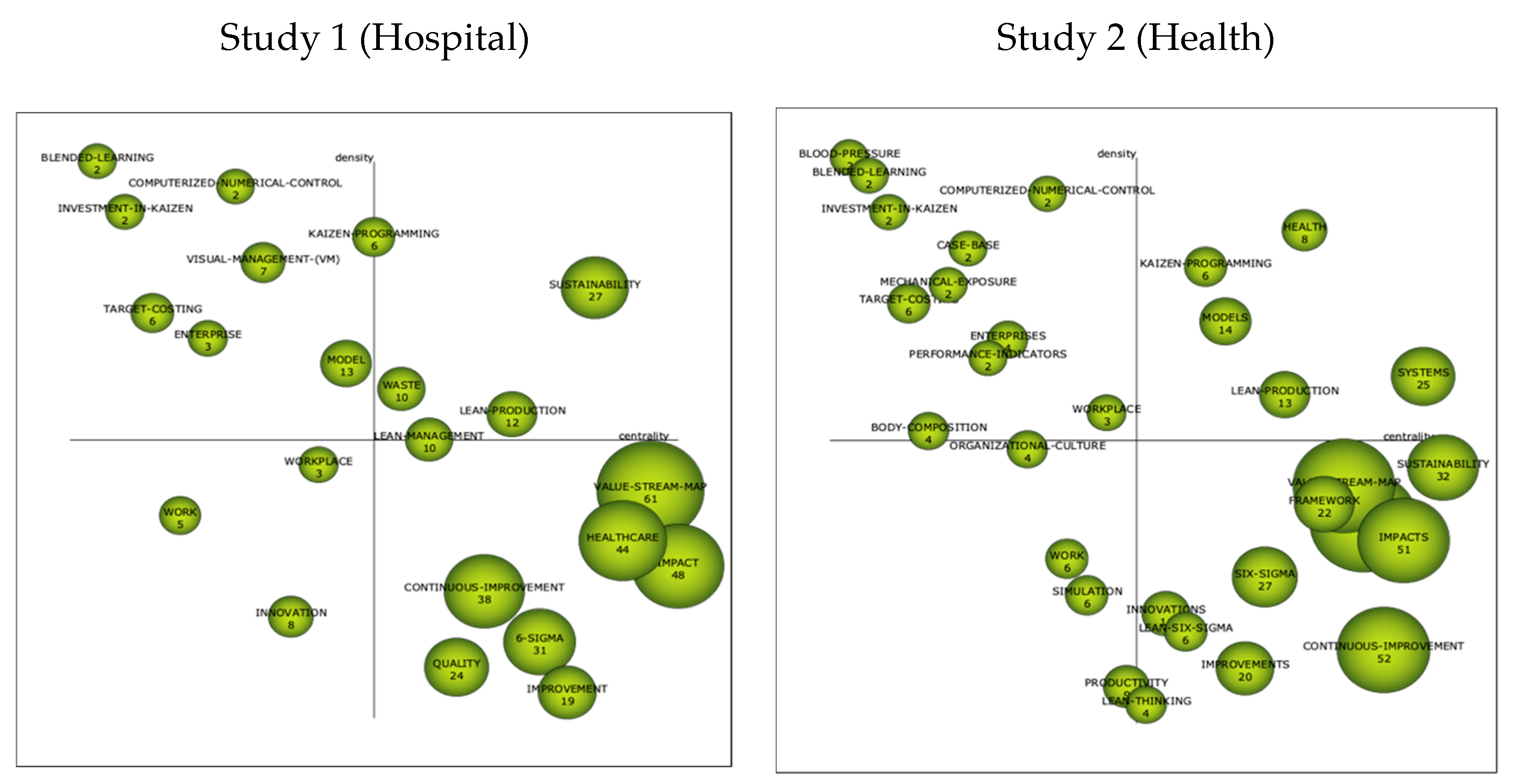
3.2.2. Strategics Diagrams
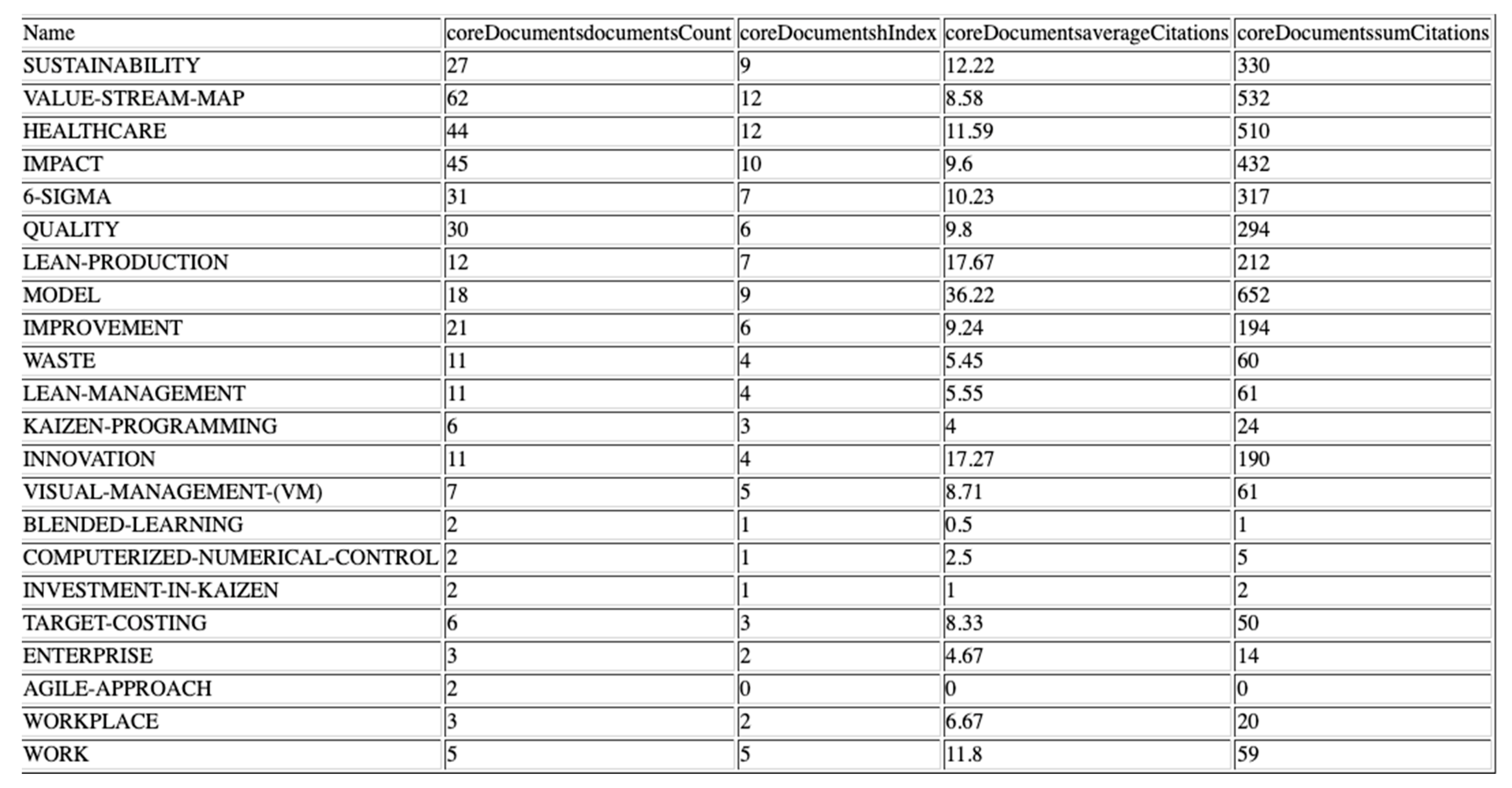
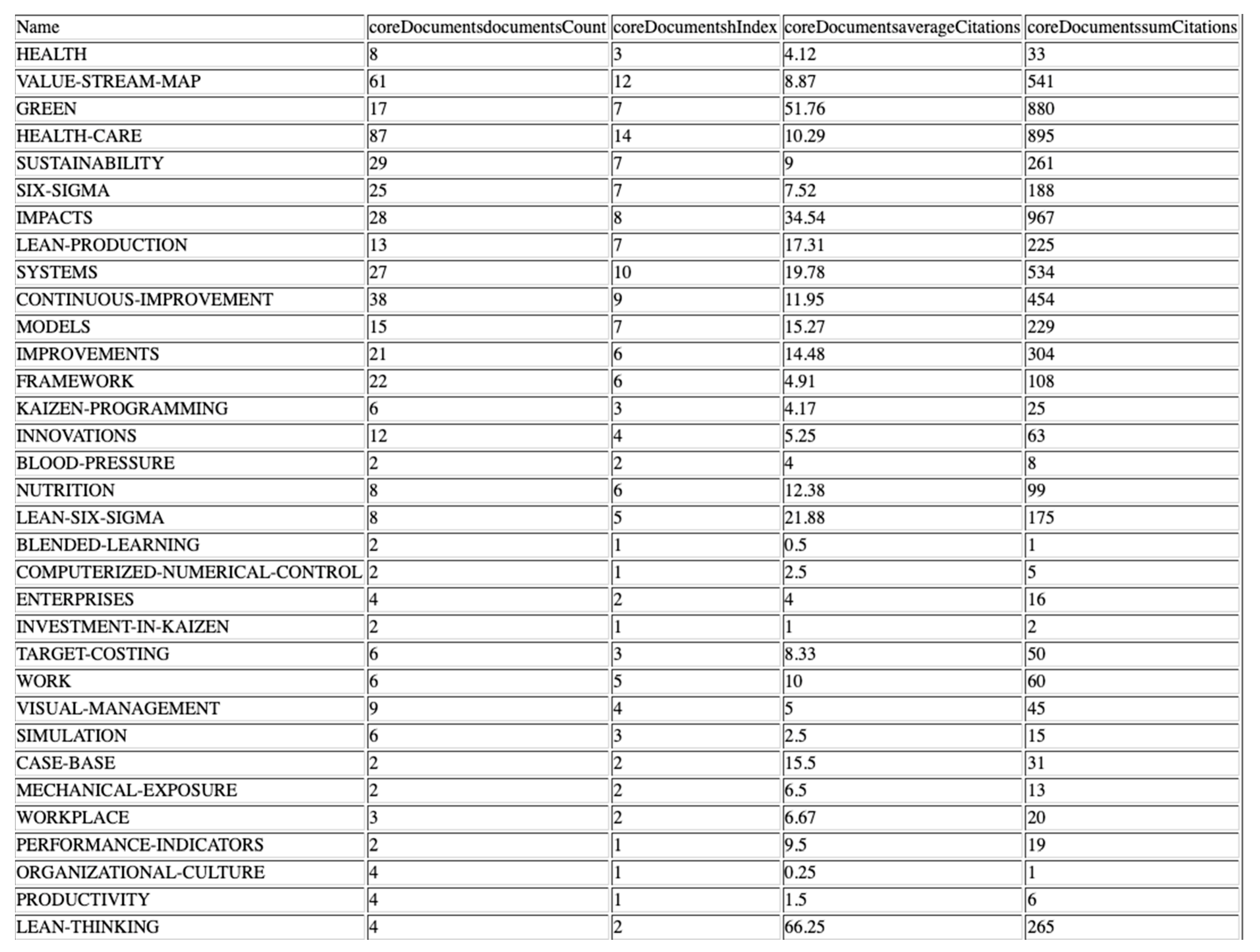
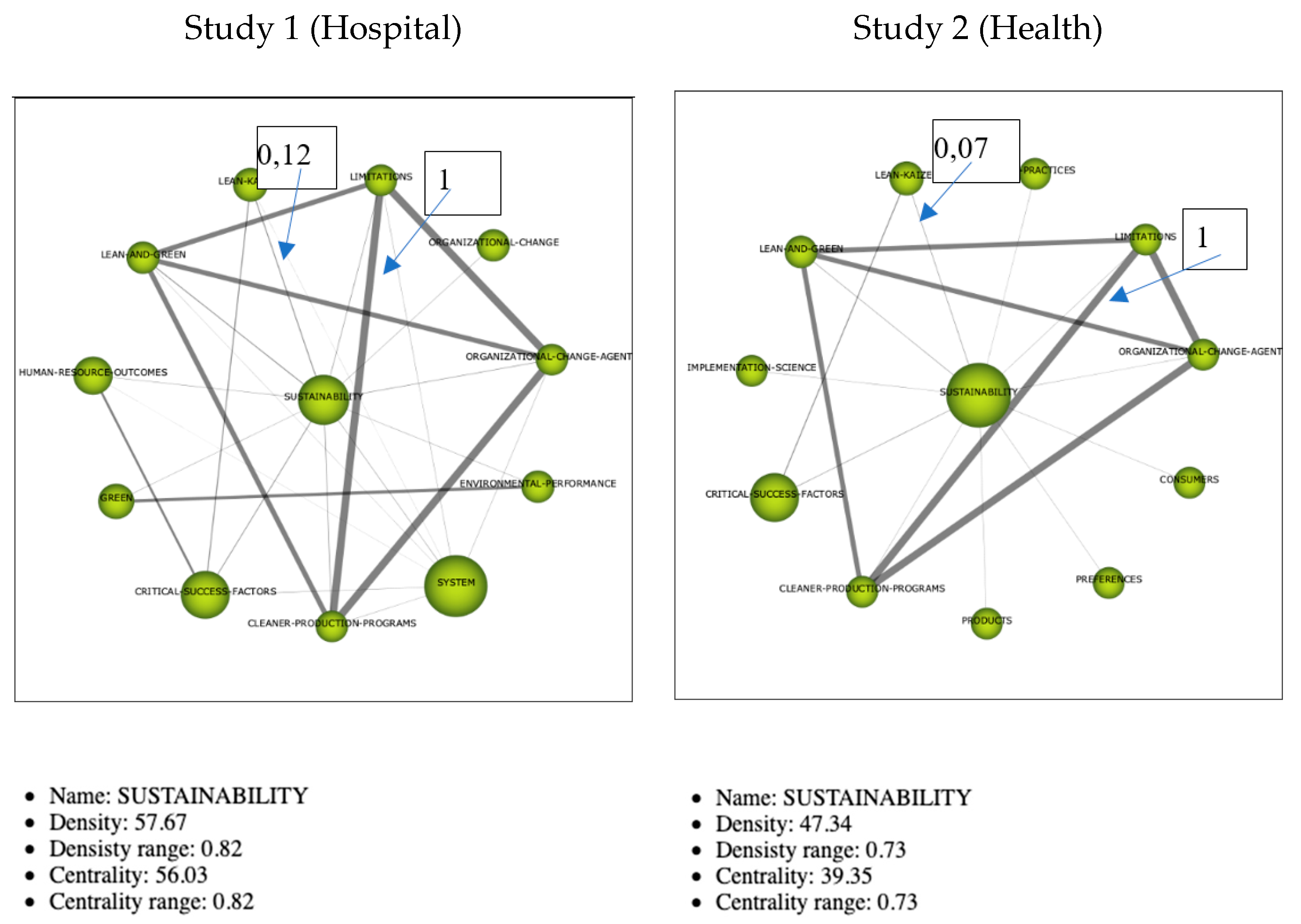
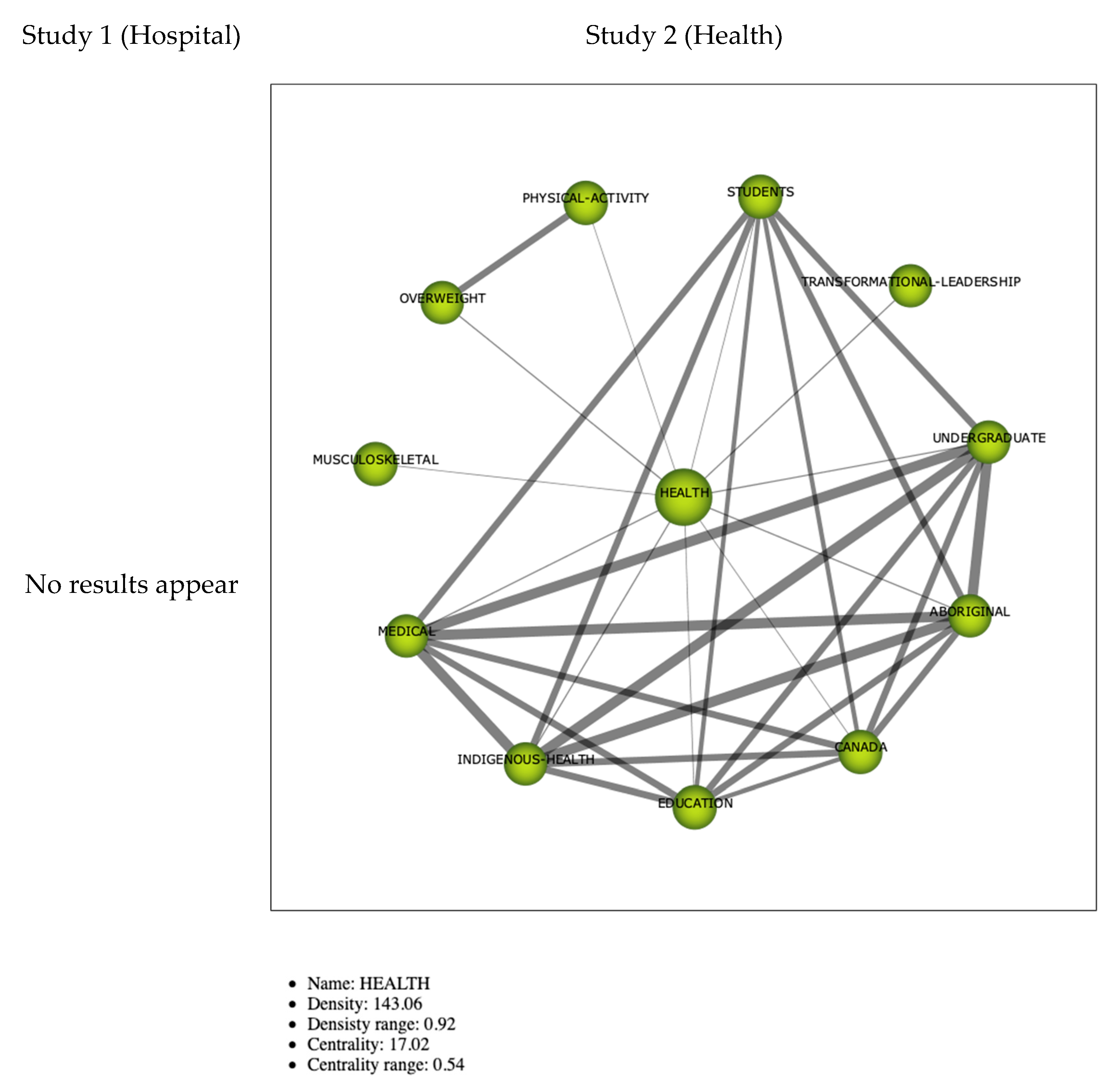
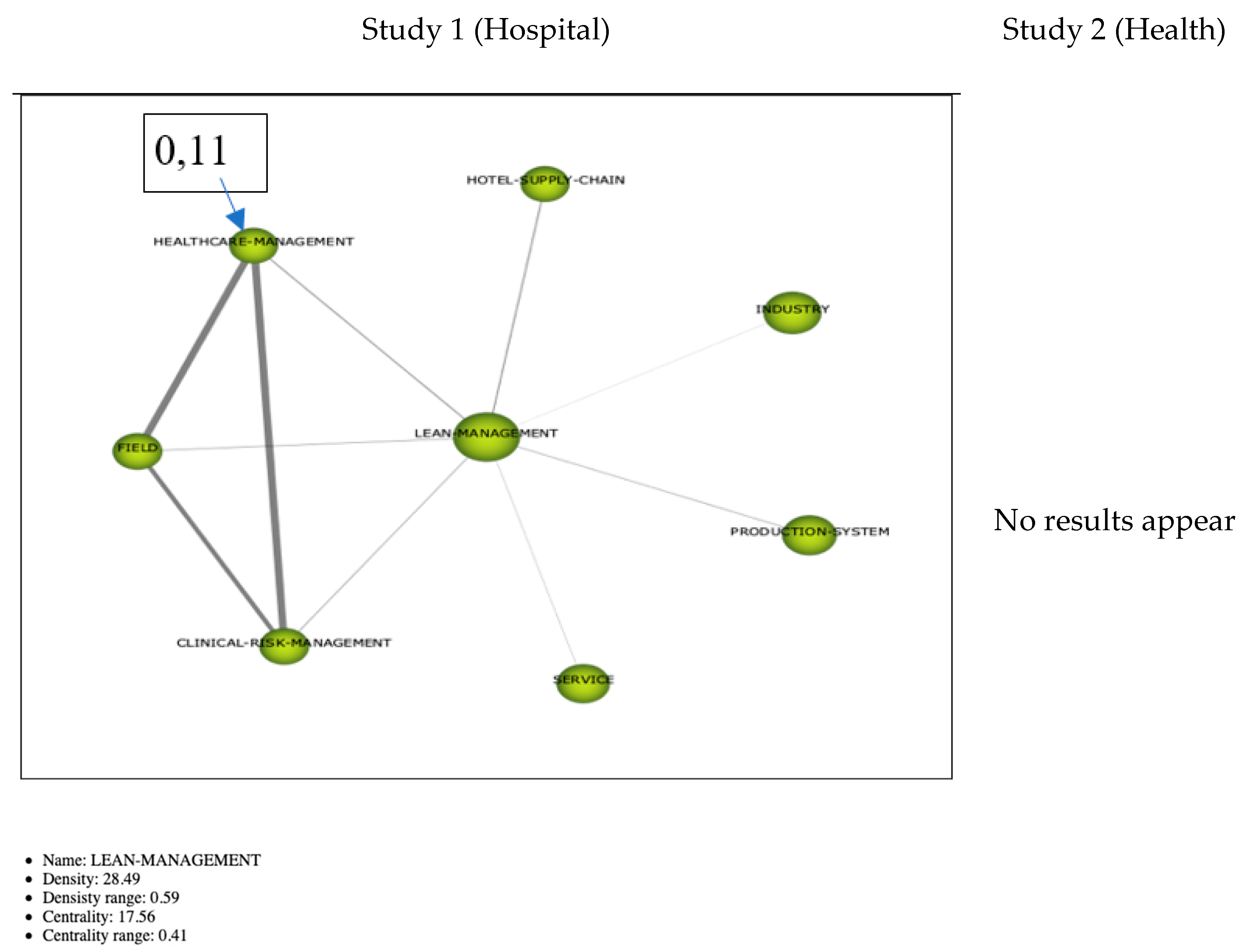
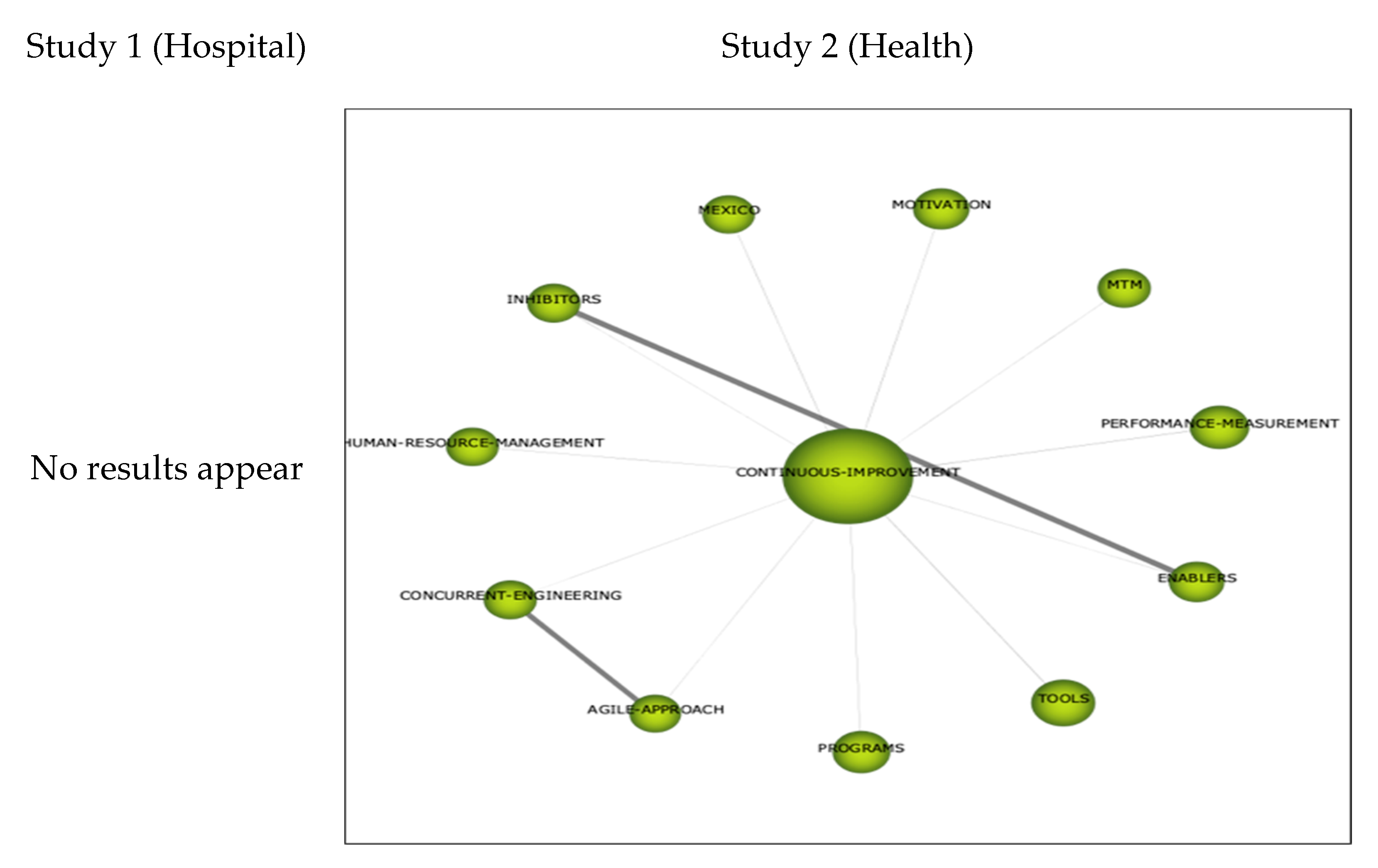
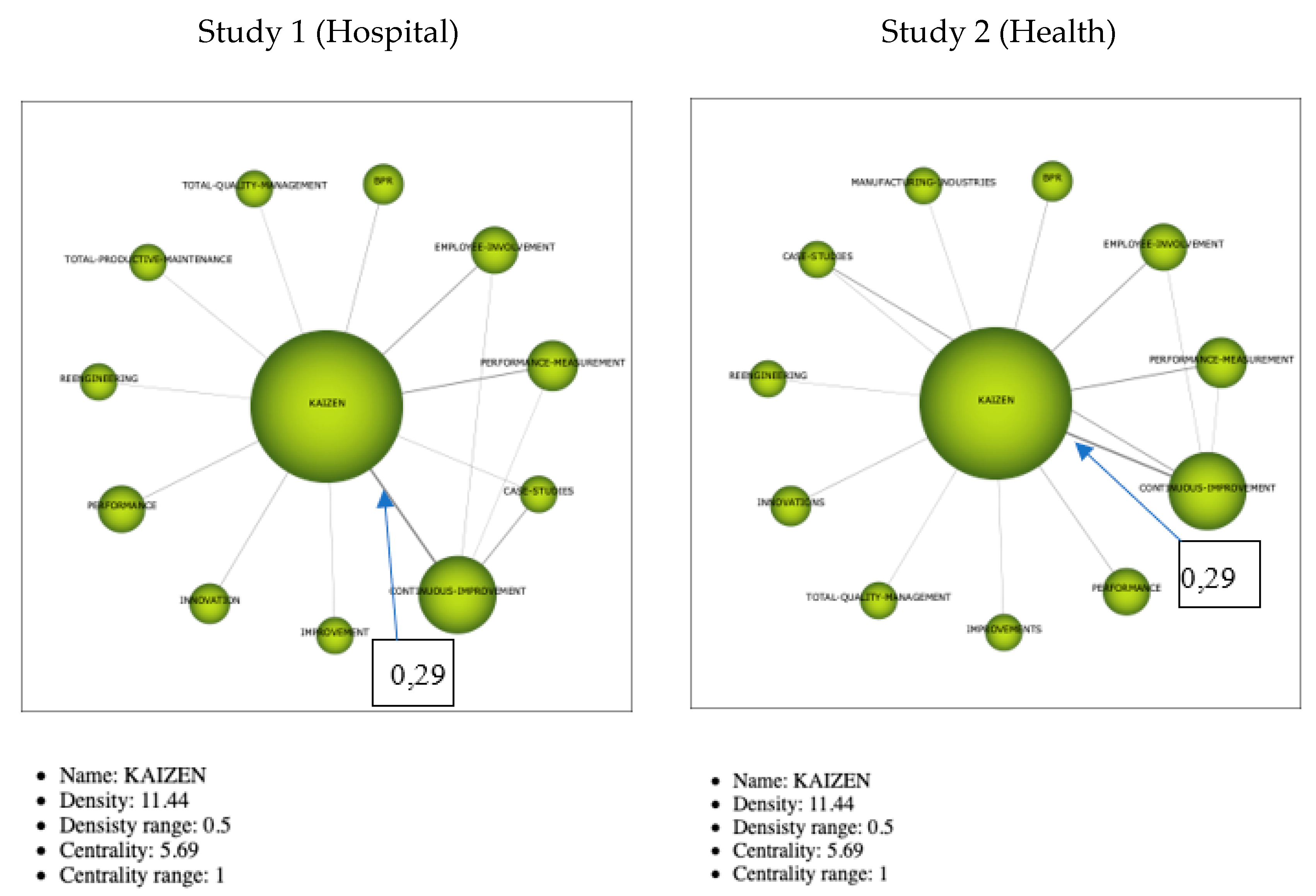
3.2.3. Thematic Networks
Cluster Sustainability
- -
- balance its books,
- -
- measure and manage its environmental impacts (e.g., air pollution, CO2 emissions), and
- -
- consider its social obligations (health and well-being of employees and clients).
Cluster Healthcare-Health
- -
- High-quality healthcare is diminishing as interventions become more expensive, patient expectations increase, and resources become more constrained [1]. Moreover, the sector is under increasing pressure to provide timely healthcare assistance to taxpayers that claim to be paying their taxes in exchange for a reasonable level of service [70].
- -
- -
- Healthcare systems need healthcare models which contribute to sustainability’s development. Inter-system collaborative networks are essential because there are multiple stakeholders involved, e.g., professionals (clinicians and non-clinical professions), managers, patients, providers of healthcare products, scientists, and governments/policy makers.
Cluster Kaizen
4. Discussion and Conclusions
- -
- The interest in continuous improvement tools/Kaizen/Lean in the health sector has grown in the last 6 or 7 years.
- -
- The majority of published work with regard to the implementation of this type of methodology in the health sector centers around the need to create a more agile and functional organization in the short term, such as making basic improvements in inventory reduction, cost reduction, and time reduction.
- -
- Although it cannot be said that no results have been obtained that improve sustainability, the current long-term maintenance of continuous improvements in different sectors does not constitute a reference of study.
- -
- On some occasions, the treatment required to reduce the morbidity and mortality of chronic diseases are unfavorable to environmental sustainability.
- -
- In many organizations, caring for the environment is a long-term challenge and means increasing resource costs, which makes it impossible to take care of the environment.
- -
- There is insufficient dissemination of sustainability programs.
- -
- Organizations experience difficulties in implementing new work methodologies that require training and involvement of the different hierarchy levels.
- -
- Improving an organization’s processes by eliminating critical points (those that do not add value) can improve the level of economic, social, and environmental sustainability.
- -
- Sustainability of results after the initial period of short-term gains is difficult to achieve.
- -
- There is limited understanding of the factors that influence the variation in results across different organizational environments
- -
- There is no doubt that Lean thinking achieves sustainability in the health care sector.
- -
- While managers are aware of the improvements that can be achieved, they lack the commitment to generate a business culture.
- -
- Few health care organizations have achieved sustainable, long-term implementation of Lean.
- -
- There should be organizational commitment to achieving corporate sustainability which should be included in their approach to social responsibility.
- -
- The lack of existing research in this area results in significant limitations in the ability to observe a direct relationship between adjusted health care practices and sustainability.
5. Future Lines of Research
- -
- To identify barriers and enablers in connection with the wider promotion and sustainability of continuous improvement among health personnel, i.e., not only promoted by process departments.
- -
- To develop models that promote sustainability in health, not only in its economic aspect, but also in its social and environmental contexts.
- -
- To identify and develop models that are adapted to the different types of services in the health sector: primary, secondary, and tertiary care.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Morton, S.; Pencheon, D.; Squires, N. Sustainable Development Goals (SDGs), and their implementation. A national global framework for health, development and equity needs a systems approach at every level. Br. Med. Bull. 2017, 124, 81–90. [Google Scholar]
- Sepetis, A. Sustainable Health Care Management in the Greek Health Care Sector. Open J. Soc. Sci. 2019, 7, 386–402. [Google Scholar] [CrossRef][Green Version]
- Alliance for Natural Health. Sustainable Healthcare—Working towards the Paradigm Shift. 2018. Available online: https://www.anhinternational.org/wp-content/uploads/old/files/100617SustainableHealthcare_White-Paper.pdf (accessed on 5 April 2020).
- Economic Planning Unit. Transforming Services Sector. 2015. Available online: http://www.epu.gov.my (accessed on 3 May 2020).
- Anuar, A.; Saad, R.; Yusoff, R.Z. Sustainability through lean healthcare and operational performance in the private hospitals: A proposed framework. Int. J. Supply Chain Manag. 2018, 7, 221–227. [Google Scholar]
- Sepetis, A. Environmental and Sustainable Management in Public Health; Papazisis Publications: Athens, Greece, 2009. [Google Scholar]
- Weisz, U.; Haas, W.; Pelikan, J.M.; Schmied, H. Sustainable hospitals: A socio-ecological approach. Gaia-Ecol. Perspect. Sci. Soc. 2011, 20, 191–198. [Google Scholar] [CrossRef]
- McGain, F.; Naylor, C. Environmental Sustainability in Hospitals—A Systematic Review and Research Agenda. J. Health Serv. Res. Policy 2014, 19, 245–252. [Google Scholar] [CrossRef] [PubMed]
- D’Andreamatteo, A.; Ianni, L.; Lega, F.; Sargiacomo, M. Lean in healthcare: A comprehensive review. Health Policy 2015, 119, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Norazlan, A.N.I.; Habidin, N.F.; Roslan, M.H.; Zainudin, M.Z. Investigation of kaizen blitz and sustainable performance for malaysian healthcare industry. Int. J. Qual. Innov. 2014, 2, 272–284. [Google Scholar] [CrossRef]
- Jamaludin, N.H.; Habidin, N.F.; Shazali, N.A.; Ali, N.; Khaidir, N.A. Exploring sustainable healthcare service and sustainable healthcare performance: Based on Malaysian healthcare industry. J. Sustain. Dev. Stud. 2013, 3, 14–26. [Google Scholar]
- Health Organization. Patient Safety in Developing and Transitional Countries 2012. Available online: www.who.int/patientsafety/research/emro_afro_report.pdf (accessed on 15 September 2020).
- Elmontsri, A.; Almashrafi, A.; Banarsee, R.; Majeed, A. Status of patient safety culture in Arab countries: A systematic review. BMJ Open 2017, 7, e013487. [Google Scholar] [CrossRef]
- Garcia-Sabater, J.J.; Maheut, J.Y.; Vidal-Carreras, P.I. Utilización del mapa de la cadena de valor en un entorno sanitario: Un caso de estudio. In Proceedings of the 8th International Conference on Industrial Engineering and Industrial Management, XX International Conference on Industrial Engineering and Operations Management, International IIE Conference, Malaga, Spain, 23–25 July 2014. [Google Scholar]
- Morell-Santandreu, O.Y.; Santandreu-Mascarell, C. Nuevas herramientas de gestión: Lean sector servicios. In Proceedings of the XXXIII Annual Meeting of the Acdemy (AEDEM), Sevilla, España, 5–7 June 2019. [Google Scholar]
- Morell-Santandreu, O.; Santandre-Mascarell, C.Y.; Canós-Darós, L. Lean en la gestión hospitalaria: Resultados tangibles e intangibles. In Proceedings of the XXXII Annual Meeting of the Acdemy (AEDEM), Gandia, España, 6–8 June 2018. [Google Scholar]
- Morell-Santandreu, O.; García-Sabater, J.; Santandre-Mascarell, C. Mejora de procesos en un centro público de atención primaria: Un caso de estudio. In Proceedings of the XXXI Annual Meeting of the Acdemy (AEDEM), Madrid, España, 7–9 June 2017. [Google Scholar]
- Imai, M. Gemba Kaizen: A Commonsense Approach to a Continuous Improvement Strategy; McGraw Hill: New York, NY, USA, 2012. [Google Scholar]
- Spear, S.; Bowen, H.K. Decoding the DNA of the Toyota Production System. Harv. Bus. Rev. 1999, 97, 96–106. [Google Scholar]
- Brunet, A.P.; New, S. Kaizen in Japan: An Empirical Study. Int. J. Oper. Prod. Manag. 2003, 23, 1426–1446. [Google Scholar] [CrossRef]
- Glover, W.J. Critical success factors for sustaining Kaizen Event outcomes. Ph.D. Thesis, Virginia Tech, Blacksburg, VA, USA, 2010. [Google Scholar]
- Ferreira, D.M.C.; Saurin, T.A. A complexity theory perspective of kaizen: A study in healthcare. Prod. Plan. Control 2019, 30, 1337–1353. [Google Scholar] [CrossRef]
- Chahal, H.F. An exploratory study on kaizen muda and organisational sustainability: Patients’ perspective. Int. J. Lean Enterp. Res. 2016, 2, 81–94. [Google Scholar] [CrossRef]
- Ishijima, H.; Nishikido, K.; Teshima, M.; Nishikawa, S.; Gawad, E.A. Introducing the “5S-KAIZEN-TQM approach into public hospitals in Egypt. Int. J. Health Care Qual. Assur. 2019, 33, 89–109. [Google Scholar] [CrossRef]
- Mazzocato, P.; Stenfors-Hayes, T.; von Thiele Schwarz, U.; Hasson, H.; Nyström, M.E. Kaizen practice in healthcare: A qualitative analysis of hospital employees’ suggestions for improvement. BMJ Open 2016, 6, e012256. [Google Scholar] [CrossRef]
- Anuar, A.; Saad, R.; Yusoff, R.Z. Operational performance as a mediator on the relationship between lean healthcare and sustainability among private hospitals in malaysia using pls-sem. J. Inf. 2017, 2, 84–104. [Google Scholar]
- Gowen, C.R., III; McFadden, K.L.; Settaluri, S. Contrasting continuous quality improvement, Six Sigma, and lean management for enhanced outcomes in US hospitals. Am. J. Bus. 2014, 27, 133–153. [Google Scholar] [CrossRef]
- Grove, A.L.; Meredith, J.O.; MacIntyre, M.; Angelis, J.; Neailey, K. UK health visiting: Challenges faced during lean implementation. Leadersh. Health Serv. 2010, 23, 204–218. [Google Scholar] [CrossRef]
- Elshennawy, A.K.; Bahaitham, H.; Furterer, S. Assessing Sustainability of Lean Implementation in Healthcare: A Case Study Using the Lean Sustainability Assessment Framework (LSAF). J. Manag. Eng. Integr. 2012, 5, 29. [Google Scholar]
- Ho, S.K.M. Integrated lean TQM model for sustainable development. TQM J. 2010, 22, 143–158. [Google Scholar] [CrossRef]
- DelliFraine, J.L.; Langabeer, J.R.; Nembhard, I.M. Assessing the evidence of Six Sigma and Lean in the health care industry. Qual. Manag. Healthc. 2010, 19, 211–225. [Google Scholar] [CrossRef]
- Souza, J.P.E.; Alves, J.M. Lean-integrated management system: A model for sustainability improvement. J. Clean. Prod. 2018, 172, 2667–2682. [Google Scholar] [CrossRef]
- Braithwaite, J.; Mannion, R.; Matsuyama, Y.; Shekelle, P.; Whittaker, S.; Al-Adawi, S. (Eds.) Health Systems Improvement across the Globe: Success Stories from 60 Countries; CRC Press: Boca Raton, FL, USA, 2017. [Google Scholar]
- Braithwaite, J.; Mannion, R.; Matsuyama, Y.; Shekelle, P.G.; Whittaker, S.; Al-Adawi, S. (Eds.) Healthcare Systems: Future Predictions for Global Care; CRC Press: Boca Raton, FL, USA, 2018. [Google Scholar]
- Costa, L.B.M.; Godinho Filho, M. Lean healthcare: Review, classification and analysis of literature. Prod. Plan. Control 2016, 27, 823–836. [Google Scholar] [CrossRef]
- Costa, D.G.D.; Pasin, S.S.; Magalhães, A.M.M.D.; Moura, G.M.S.S.D.; Rosso, C.B.; Saurin, T.A. Analysis of the preparation and administration of medications in the hospital context based on Lean thinking. Esc. Anna Nery 2018, 22. [Google Scholar] [CrossRef]
- Van Aken, J.; Chandrasekaran, A.; Halman, J. Conducting and publishing design science research: Inaugural essay of the design science department of the Journal of Operations Management. J. Oper. Manag. 2016, 47, 1–8. [Google Scholar] [CrossRef]
- Glover, W.J.; Farris, J.A.; Van Aken, E.M.; Doolen, T.L. Critical success factors for the sustainability of Kaizen event human resource outcomes: An empirical study. Int. J. Prod. Econ. 2011, 132, 197–213. [Google Scholar] [CrossRef]
- Glover, W.J.; Liu, W.H.; Farris, J.A.; Van Aken, E.M. Characteristics of established kaizen event programs: An empirical study. Int. J. Oper. Prod. Manag. 2013, 33, 1166–1201. [Google Scholar] [CrossRef]
- Aij, K.H.; Rapsaniotis, S. Leadership requirements for Lean versus servant leadership in health care: A systematic review of the literature. J. Healthc. Leadersh. 2017, 9, 1. [Google Scholar]
- Graban, M. Lean Hospitals: Improving Quality, Patient Safety, and Employee Engagement; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Graban, M.; Swartz, J.E. Healthcare kaizen: Engaging Front-Line Staff in Sustainable Continuous Improvements; CRC Press: Boca Raton, FL, USA, 2018. [Google Scholar]
- Garcia, S.; Cintra, Y.; Rita de Cássia, S.R.; Lima, F.G. Corporate sustainability management: A proposed multi-criteria model to support balanced decisionmaking. J. Clean. Prod. 2014, 136, 181–196. [Google Scholar] [CrossRef]
- RobecoSAM, A.G. The Sustainability Yearbook 2014. Available online: https://www.p-plus.nl/resources/articlefiles/SustainabilityYearbook2014.pdf (accessed on 25 January 2020).
- Rebelo, M.F.; Santos, G.; Silva, R. Integration of management systems: Towards a sustained success and development of organizations. J. Clean. Prod. 2015, 127, 96–111. [Google Scholar] [CrossRef]
- World Health Organization. Health Workforce Requirements for Universal Health Coverage and the Sustainable Development Goals 2016; (Human Resources for Health Observer, 17); World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Cobo, M.J.; López-Herrera, A.G.; Herrera-Viedma, E.; Herrera, F. An approach for detecting, quantifying, and visualizing the evolution of a research field: A practical application to the fuzzy sets theory field. J. Informetr. 2011, 5, 146–166. [Google Scholar] [CrossRef]
- Cobo, M.J.; López-Herrera, A.G.; Herrera-Viedma, E.; Herrera, F. SciMAT: A new science mapping analysis software tool. J. Am. Soc. Inf. Sci. Technol. 2012, 63, 1609–1630. [Google Scholar] [CrossRef]
- Martínez-Jurado, P.J.; Moyano-Fuentes, J. Lean Management, Supply Chain Management and Sustainability: A Literature Review. J. Clean. Prod. 2014, 85, 134–150. [Google Scholar] [CrossRef]
- López-Robles, J.R.; Guallar, J.; Otegi-Olaso, J.R.; Gamboa-Rosales, N.K. El profesional de la información (EPI): Bibliometric and thematic analysis (2006–2017). Prof. Inf. 2019, 28, e280417. [Google Scholar] [CrossRef]
- FEYCT. WOS Database Available from the Spanish Foundation for Science and Technology. Available online: https://www.recursoscientificos.fecyt.es/ (accessed on 13 April 2020).
- Fundación Española para la Ciencia y la Tecnología (FECYT). Available online: www.fecyt.es (accessed on 15 January 2020).
- Marín-García, J.A.; García-Sabater, J.; Miralles, C. Manufacturing perfomance: Impact of kaizen-blitz implementation in several automotive components first tier suppliers. Dir. Organ. 2008, 35, 37–44. [Google Scholar]
- Womack, J.P.; Jones, D.X.; Roos, D. The Machine that Changed the World; Free Press: New York, NY, USA, 1990. [Google Scholar]
- Womack, J.P.; Jones, D.T. Lean Thinking; Simon and Schuster: New York, NY, USA, 1996. [Google Scholar]
- Womack, J.P.; Jones, D.T.; Roos, D. The Machine that Changed the World: The Story of Lean Production—Toyota’s Secret Weapon in the Global Car Wars that is Now Revolutionizing World Industry; Simon and Schuster: New York, NY, USA, 2007. [Google Scholar]
- Jiménez-García, M.; Ruiz-Chico, J.; Peña-Sánchez, A.R.; López-Sánchez, J.A. A Bibliometric Analysis of Sports Tourism and Sustainability (2002–2019). Sustainability 2020, 12, 2840. [Google Scholar] [CrossRef]
- Furstenau, L.B.; Sott, M.K.; Homrich, A.J.O.; Kipper, L.M.; Al Abri, A.A.; Cardoso, T.F.; López-Robles, J.R.; Cobo, M.J. 20 Years of Scientific Evolution of Cyber Security: A Science Mapping. In Proceedings of the International Conference on Industrial Engineering and Operations Management, Dubai, UAE, 10–12 March 2020. [Google Scholar]
- Imai, M. Kaizen: The Key to Japan’s Competitive Success; McGraw Hill: New York, NY, USA, 1986. [Google Scholar]
- Chiarini, A.; Baccarani, C.; Mascherpa, V. Lean production, Toyota production system and kaizen philosophy. TQM J. 2018, 30, 425–438. [Google Scholar] [CrossRef]
- Marin-Garcia, J.A.; Garcia-Sabater, J.J.; Bonavia, T. The impact of Kaizen Events on improving the performance of automotive components’ first-tier suppliers. Int. J. Automot. Technol. Manag. 2009, 9, 362–376. [Google Scholar] [CrossRef]
- Bukhari, A.; Aqdas Rana, R.; Bhatti, U. Factors influencing consumer’s green product purchase decision by mediation of green brand image. Int. J. Res. 2017, 4, 1620–1632. [Google Scholar]
- Schwerdtle, P.N.; Maxwell, J.; Horton, G.; Bonnamy, J. 12 tips for teaching environmental sustainability to health professionals. Med. Teach. 2020, 42, 150–155. [Google Scholar] [CrossRef]
- Vergunst, F.; Berry, H.L.; Rugkåsa, J.; Burns, T.; Molodynski, A.; Maughan, D.L. Applying the triple bottom line of sustainability to healthcare research—A feasibility study. Int. J. Qual. Health Care 2020, 32, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Haanaes, K.; Reeves, M.; Von Streng Velken, I.; Audretsch, M.; Kiron, D.; Kruschwitz, N. Sustainability Reaches a Tipping Point; MIT Sloan Management Review Research Reports; Massachusetts Institute of Technology (MIT): Cambridge, MA, USA; Sloan Management Review and Boston Consulting Group (BCG): North Hollywood, CA, USA, 2012. [Google Scholar]
- Aznar Mínguet, P.; Barrón Ruiz, Á. El desarrollo humano sostenible: Un compromiso educativo. Teor. Educ. 2017, 29, 25–53. [Google Scholar] [CrossRef]
- WCED, S.W.S. World commission on environment and development. In Our Common Future; Oxford University Press: Oxford, UK, 1987; Volume 17, pp. 1–91. [Google Scholar]
- Herrera, J.; de las Heras-Rosas, C. Corporate social responsibility and human resource management: Towards sustainable business organizations. Sustainability 2020, 12, 841. [Google Scholar] [CrossRef]
- Ling, T.; Pedersen, J.S.; Drabble, S.; Celia, C.; Brereton, L.; Tiefensee, C. Sustainable development in the National Health Service (NHS): The views and values of NHS leaders. Rand Health Q. 2012, 2, 12. [Google Scholar] [PubMed]
- Leite, H.; Bateman, N.; Radnor, Z. Beyond the ostensible: An exploration of barriers to lean implementation and sustainability in healthcare. Prod. Plan. Control 2020, 31, 1–18. [Google Scholar] [CrossRef]
- Nerminathan, V.; Adlan, W.N.A.B.W.F.; Nerminathan, A.A. Hospital at home: Sustainable healthcare in developing countries through reducing average length of stay in hospitals. Int. J. Manag. Sustain. 2014, 3, 51–61. [Google Scholar]
- Maghsoudi, T.; Cascón-Pereira, R.; Beatriz Hernández Lara, A. The Role of Collaborative Healthcare in Improving Social Sustainability: A Conceptual Framework. Sustainability 2020, 12, 3195. [Google Scholar] [CrossRef]
- Stelson, P.; Hille, J.; Eseonu, C.; Doolen, T. What drives continuous improvement project success in healthcare? Int. J. Health Care Qual. Assur. 2017, 30, 43–57. [Google Scholar] [CrossRef]
- Ramírez, K.A.; Álvaro, V.P. Prácticas de mejora continua, con enfoque Kaizen, en empresas del Distrito Metropolitano de Quito: Un estudio exploratorio. Intang. Cap. 2017, 13, 479–497. [Google Scholar] [CrossRef]
- Ten Have, H.; Gordijn, B. Medicine, Health care and Philosophy. Sustainability 2020, 23, 153–154. [Google Scholar]
- Daly, H.E. Toward some operational principles of sustainable development. Ecol. Econ. 1990, 2, 1–6. [Google Scholar] [CrossRef]































Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morell-Santandreu, O.; Santandreu-Mascarell, C.; García-Sabater, J. Sustainability and Kaizen: Business Model Trends in Healthcare. Sustainability 2020, 12, 10622. https://doi.org/10.3390/su122410622
Morell-Santandreu O, Santandreu-Mascarell C, García-Sabater J. Sustainability and Kaizen: Business Model Trends in Healthcare. Sustainability. 2020; 12(24):10622. https://doi.org/10.3390/su122410622
Chicago/Turabian StyleMorell-Santandreu, Oscar, Cristina Santandreu-Mascarell, and Julio García-Sabater. 2020. "Sustainability and Kaizen: Business Model Trends in Healthcare" Sustainability 12, no. 24: 10622. https://doi.org/10.3390/su122410622
APA StyleMorell-Santandreu, O., Santandreu-Mascarell, C., & García-Sabater, J. (2020). Sustainability and Kaizen: Business Model Trends in Healthcare. Sustainability, 12(24), 10622. https://doi.org/10.3390/su122410622