Sirt1 Activity in PBMCs as a Biomarker of Different Heart Failure Phenotypes

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Echocardiography
2.3. Six-Minute Walking Test
2.4. Blood Sampling and SIRT1 Activity
2.5. Circulating Angiotensin-Converting Enzyme 2 (ACE2) Activity and TNF-Alpha Measurement
2.6. Statistical Analysis
3. Results
3.1. Study Population
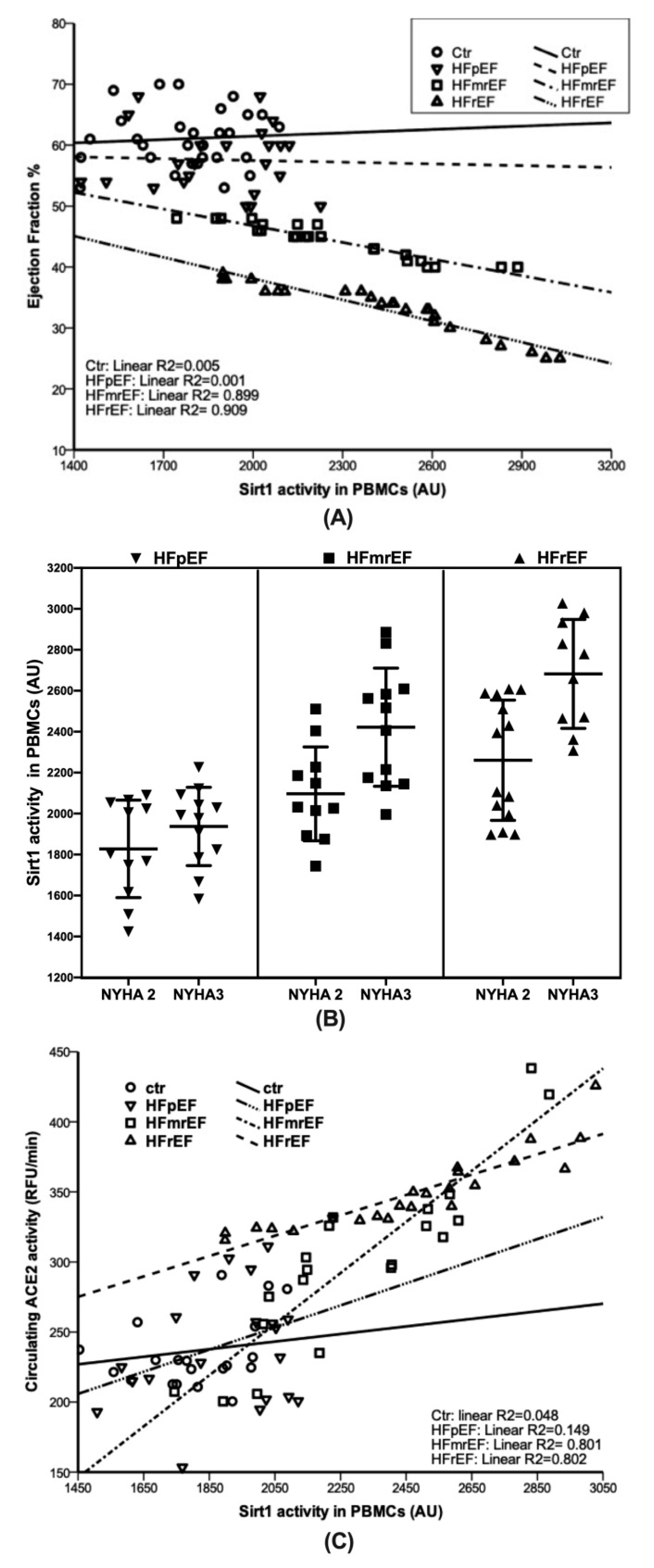
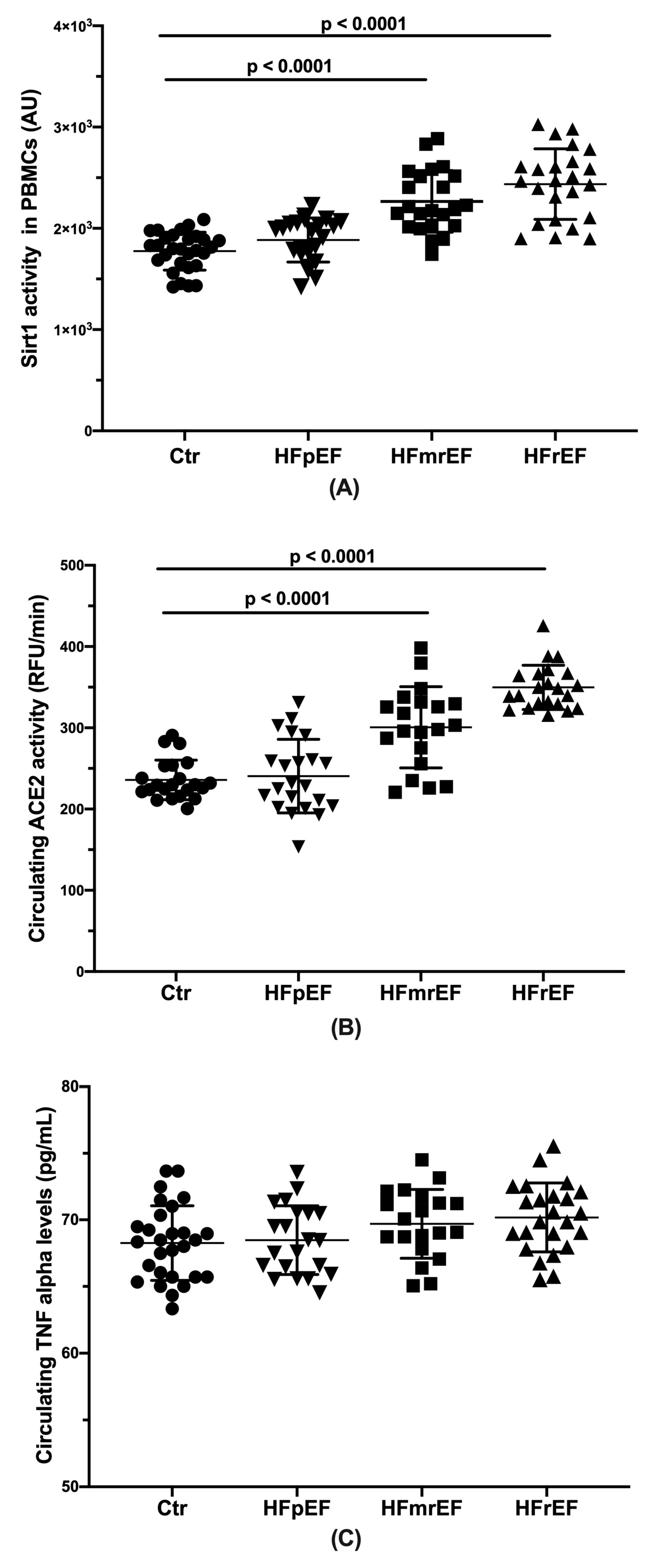
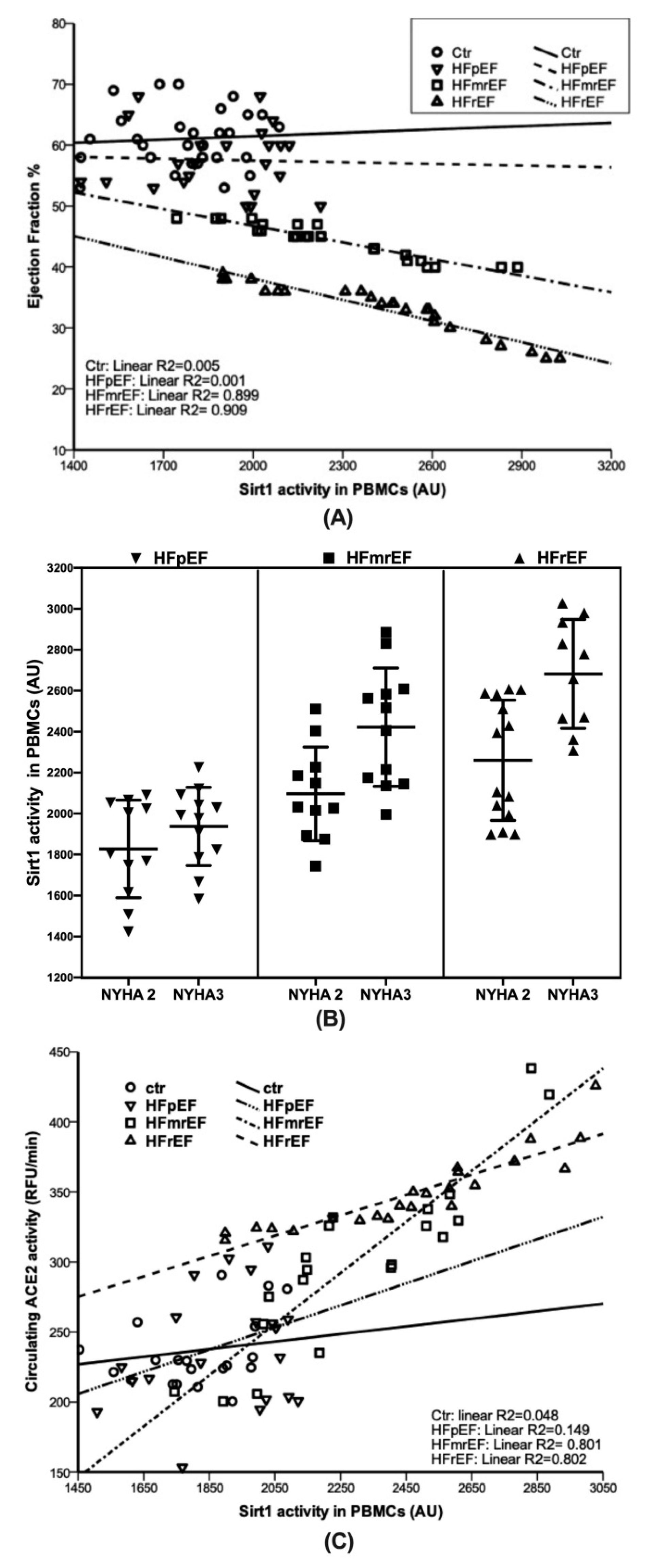
3.2. Sirt1 Activity
3.3. Circulating Angiotensin-Converting Enzyme 2 (ACE2) Activity
3.4. Circulating Tumor Necrosis Factor-Alpha (TNF-α) Levels
3.5. Circulating Brain Natriuretic Peptide (BNP) levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Tschöpe, C.; Birner, C.; Böhm, M.; Bruder, O.; Frantz, S.; Luchner, A.; Maier, L.; Störk, S.; Kherad, B.; Laufs, U. Heart failure with preserved ejection fraction: Current management and future strategies: Expert opinion on the behalf of the Nucleus of the “Heart Failure Working Group” of the German Society of Cardiology (DKG). Clin. Res. Cardiol. 2018, 107, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.J.; Ziaeian, B.; Fonarow, G.C. Heart Failure with Mid-Range (Borderline) Ejection Fraction: Clinical Implications and Future Directions. JACC Heart Fail. 2017, 5, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef]
- Lopatin, Y. Heart Failure with Mid-Range Ejection Fraction and How to Treat It. Card. Fail. Rev. 2018, 4, 9–13. [Google Scholar] [CrossRef]
- Tanno, M.; Kuno, A.; Horio, Y.; Miura, T. Emerging beneficial roles of sirtuins in heart failure. Basic Res. Cardiol. 2012, 107, 273. [Google Scholar] [CrossRef] [Green Version]
- Conti, V.; Forte, M.; Corbi, G.; Russomanno, G.; Formisano, L.; Landolfi, A.; Izzo, V.; Filippelli, A.; Vecchione, C.; Carrizzo, A. Sirtuins: Possible Clinical Implications in Cardio and Cerebrovascular Diseases. Curr. Drug Targets 2017, 18, 473–484. [Google Scholar] [CrossRef]
- Gao, P.; Xu, T.T.; Lu, J.; Li, L.; Xu, J.; Hao, D.L.; Chen, H.Z.; Liu, D.P. Overexpression of SIRT1 in vascular smooth muscle cells attenuates angiotensin II-induced vascular remodeling and hypertension in mice. J. Mol. Med. (Berl.) 2014, 92, 347–357. [Google Scholar] [CrossRef]
- Niethammer, M.; Sieber, M.; von Haehling, S.; Anker, S.D.; Munzel, T.; Horstick, G.; Genth-Zotz, S. Inflammatory pathways in patients with heart failure and preserved ejection fraction. J. Cardiol. 2008, 129, 111–117. [Google Scholar] [CrossRef]
- Vahtola, E.; Louhelainen, M.; Merasto, S.; Martonen, E.; Penttinen, S.; Aahos, I.; Kytö, V.; Virtanen, I.; Mervaala, E. Forkhead class O transcription factor 3a activation and Sirtuin1 overexpression in the hypertrophied myocardium of the diabetic Goto-Kakizaki rat. J. Hypertens. 2008, 26, 334–344. [Google Scholar] [CrossRef]
- Li, L.; Zhao, L.; Yi-Ming, W.; Yu, Y.S.; Xia, C.Y.; Duan, J.L.; Su, D.F. Sirt1 hyperexpression in SHR heart related to left ventricular hypertrophy. Can. J. Physiol. Pharmacol. 2009, 87, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Conti, V.; Corbi, G.; Simeon, V.; Russomanno, G.; Manzo, V.; Ferrara, N.; Filippelli, A. Aging-related changes in oxidative stress response of human endothelial cells. Aging Clin. Exp. Res. 2015, 27, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Qin, J.; Chen, C.; Fu, Y.; Wang, W. Moderate calorie restriction attenuates age-associated alterations and improves cardiac function by increasing SIRT1 and SIRT3 expression. Mol. Med. Rep. 2018, 18, 4087–4094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcendor, R.R.; Gao, S.; Zhai, P.; Zablocki, D.; Holle, E.; Yu, X.; Tian, B.; Wagner, T.; Vatner, S.F.; Sadoshima, J. Sirt1 regulates aging and resistance to oxidative stress in the heart. Circ. Res. 2007, 100, 1512–1521. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Zhang, J.; Cole-Jeffrey, C.T.; Shenoy, V.; Espejo, A.; Hanna, M.; Song, C.; Pepine, C.J.; Katovich, M.J.; Raizada, M.K. Diminazene aceturate enhances angiotensin-converting enzyme 2 activity and attenuates ischemia-induced cardiac pathophysiology. Hypertension 2013, 62, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Kane, A.E.; Sinclair, D.A. Sirtuins and NAD+ in the Development and Treatment of Metabolic and Cardiovascular Diseases. Circ. Res. 2018, 123, 868–885. [Google Scholar] [CrossRef]
- Corbi, G.; Conti, V.; Scapagnini, G.; Filippelli, A.; Ferrara, N. Role of sirtuins, calorie restriction and physical activity in aging. Front. Biosci. Elite Ed. 2012, 4, 768–778. [Google Scholar] [CrossRef]
- Park, S.; Mori, R.; Shimokawa, I. Do sirtuins promote mammalian longevity? A critical review on its relevance to the longevity effect induced by calorie restriction. Mol. Cells 2013, 35, 474–480. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, N.; Rinaldi, B.; Corbi, G.; Conti, V.; Stiuso, P.; Boccuti, S.; Rengo, G.; Rossi, F.; Filippelli, A. Exercise training promotes SIRT1 activity in aged rats. Rejuvenation Res. 2008, 11, 139–150. [Google Scholar] [CrossRef]
- Bonkowski, M.S.; Sinclair, D.A. Slowing ageing by design: The rise of NAD+ and sirtuin-activating compounds. Nat. Rev. Mol. Cell Biol. 2016, 17, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Sen, P.; Kemppainen, E.; Orešič, M. Perspectives on Systems Modeling of Human Peripheral Blood Mononuclear Cells. Front. Mol. Biosci. 2018, 4, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bo, S.; Togliatto, G.; Gambino, R.; Ponzo, V.; Lombardo, G.; Rosato, R.; Cassader, M.; Brizzi, M.F. Impact of sirtuin-1 expression on H3K56 acetylation and oxidative stress: A double-blind randomized controlled trial with resveratrol supplementation. Acta Diabetol. 2018, 55, 331–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taka, C.; Hayashi, R.; Shimokawa, K.; Tokui, K.; Okazawa, S.; Kambara, K.; Inomata, M.; Yamada, T.; Matsui, S.; Tobe, K. SIRT1 and FOXO1 mRNA expression in PBMC correlates to physical activity in COPD patients. Int. J. Chronic Obstruct. Pulmon. Dis. 2017, 12, 3237–3244. [Google Scholar] [CrossRef] [Green Version]
- Conti, V.; Corbi, G.; Manzo, V.; Malangone, P.; Vitale, C.; Maglio, A.; Cotugno, R.; Capaccio, D.; Marino, L.; Selleri, C.; et al. SIRT1 Activity in Peripheral Blood Mononuclear Cells Correlates with Altered Lung Function in Patients with Chronic Obstructive Pulmonary Disease. Oxid. Med. Cell Longev. 2018, 2018, 9391261. [Google Scholar] [CrossRef]
- Santos-Bezerra, D.P.; Machado-Lima, A.; Monteiro, M.B.; Admoni, S.N.; Perez, R.V.; Machado, C.G.; Shimizu, M.H.; Cavaleiro, A.M.; Thieme, K.; Queiroz, M.S.; et al. Dietary advanced glycated end-products and medicines influence the expression of SIRT1 and DDOST in peripheral mononuclear cells from long-term type 1 diabetes patients. Diabetes Vasc. Dis. Res. 2018, 15, 81–89. [Google Scholar] [CrossRef]
- Russomanno, G.; Corbi, G.; Manzo, V.; Ferrara, N.; Rengo, G.; Puca, A.A.; Latte, S.; Carrizzo, A.; Calabrese, M.C.; Andriantsitohaina, R.; et al. The anti-ageing molecule sirt1 mediates beneficial effects of cardiac rehabilitation. Immun. Ageing 2017, 14, 7. [Google Scholar] [CrossRef]
- Sundaresan, N.R.; Pillai, V.B.; Gupta, M.P. Emerging roles of SIRT1 deacetylase in regulating cardiomyocyte survival and hypertrophy. J. Mol. Cell Cardiol. 2011, 51, 614–618. [Google Scholar] [CrossRef] [Green Version]
- Kawashima, T.; Inuzuka, Y.; Okuda, J.; Kato, T.; Niizuma, S.; Tamaki, Y.; Iwanaga, Y.; Kawamoto, A.; Narazaki, M.; Matsuda, T.; et al. Constitutive SIRT1 overexpression impairs mitochondria and reduces cardiac function in mice. J. Mol. Cell Cardiol. 2011, 51, 1026–1036. [Google Scholar] [CrossRef] [Green Version]
- Conti, V.; Russomanno, G.; Corbi, G.; Guerra, G.; Grasso, C.; Filippelli, W.; Paribello, V.; Ferrara, N.; Filippelli, A. Aerobic training workload affects human endothelial cells redox homeostasis. Med. Sci. Sports Exerc. 2013, 45, 644–653. [Google Scholar] [CrossRef] [Green Version]
- Zullo, A.; Simone, E.; Grimaldi, M.; Musto, V.; Mancini, F.P. Sirtuins as Mediator of the Anti-Ageing Effects of Calorie Restriction in Skeletal and Cardiac Muscle. Int. J. Mol. Sci. 2018, 19, 928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, D.; Bonné, K.; Alders, T.; Hermans, A.; Copermans, K.; Swinnen, H.; Maris, V.; Jansegers, T.; Mathijs, W.; Haenen, L.; et al. Exercise training intensity determination in cardiovascular rehabilitation: Should the guidelines be reconsidered? Eur. J. Prev. Cardiol. 2019, 26, 1921–1928. [Google Scholar] [CrossRef] [PubMed]
- Hartupee, J.; Mann, D.L. Neurohormonal activation in heart failure with reduced ejection fraction. Nat. Rev. Cardiol. 2017, 14, 30–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyazaki, R.; Ichiki, T.; Hashimoto, T.; Inanaga, K.; Imayama, I.; Sadoshima, J.; Sunagawa, K. SIRT1, a longevity gene, downregulates angiotensin II type 1 receptor expression in vascular smooth muscle cells. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 1263–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, P.A.; Pagnin, E.; Dal Maso, L.; Caielli, P.; Maiolino, G.; Fusaro, M.; Paolo Rossi, G.; Calò, L.A. SIRT1, heme oxygenase-1 and NO-mediated vasodilation in a human model of endogenous angiotensin II type 1 receptor antagonism: Implications for hypertension. Hypertens. Res. 2013, 36, 873–878. [Google Scholar] [CrossRef]
- Forte, M.; Conti, V.; Damato, A.; Ambrosio, M.; Puca, A.A.; Sciarretta, S.; Frati, G.; Vecchione, C.; Carrizzo, A. Targeting Nitric Oxide with Natural Derived Compounds as a Therapeutic Strategy in Vascular Diseases. Oxid. Med. Cell Longev. 2016, 7364138. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.C. Focused Treatment of Heart Failure with Reduced Ejection Fraction Using Sacubitril/Valsartan. Am. J. Cardiovasc. Drugs 2018, 18, 473–482. [Google Scholar] [CrossRef]
- Komajda, M.; Lam, C.S. Heart failure with preserved ejection fraction: A clinical dilemma. Eur. Heart J. 2014, 35, 1022–1032. [Google Scholar] [CrossRef] [Green Version]
- Úri, K.; Fagyas, M.; Kertész, A.; Borbély, A.; Jenei, C.; Bene, O.; Csanádi, Z.; Paulus, W.J.; Édes, I.; Papp, Z.; et al. Circulating ACE2 activity correlates with cardiovascular disease development. J. Renin-Angiotensin-Aldosterone Syst. 2016, 17. [Google Scholar] [CrossRef] [Green Version]
- Epelman, S.; Shrestha, K.; Troughton, R.W.; Francis, G.S.; Sen, S.; Klein, A.L.; Tang, W. Soluble Angiotensin Converting Enzyme 2 in Human Heart Failure: Relation with Myocardial Function and Clinical Outcomes. J. Card. Fail. 2009, 15, 565–571. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Ctr (n = 29) | HFpEF (n = 23) | HFmrEF (n = 23) | HFrEF (n = 24) | p | |
|---|---|---|---|---|---|
| Age, years | 60.52 ± 8.91 | 63.87 ± 10.25 | 63.00 ± 9.16 | 63.50 ± 9.57 | 0.558 |
| Sex, (M/F) n (%) | 19/10 (65.5/34.5) | 13/10 (56.5/43.5) | 15/8 (65.2/34.8) | 16/8 (66.7/33.3) | 0.157 |
| BMI, kg/m2 | 27.00 ± 3.14 | 27.89 ± 2.80 | 28.40 ± 3.80 | 28.07 ± 4.73 | 0.545 |
| SBP, mmHg | 126 ± 8 a | 123 ± 7 b | 121 ± 6 c | 106 ± 12 | <0.0001 |
| DBP, mmHg | 81 ± 5 a | 80 ± 4 d | 79 ± 7 e | 72 ± 8 | <0.0001 |
| EF, % | 61.07 ± 4.75 f,g | 57.61 ± 5.39 h | 44.35 ± 2.93 i | 33.03 ± 4.24 | <0.0001 |
| BNP, pg/mL | 31.33 ± 14.00 f | 105.00 ± 64.42 b,j | 408.08 ± 55.5 i | 814.50 ± 193.83 | <0.0001 |
| LVESV, mL | 32.56 ± 4.82 f | 44.30 ± 17.48 b,k | 72.63 ± 21.69 i | 122.17 ± 33.56 | <0.0001 |
| LVEDV, mL | 84.83 ± 10.22 a | 103.17 ± 34.06 k | 131.68 ± 39.51 l | 171.25 ± 44.74 | <0.0001 |
| Cardiac Index, L/min/m2 | 2.94 ± 0.35 | 2.82 ± 0.47 | 2.74 ± 0.43 | 2.64 ± 0.36 | 0.059 |
| SPAP, mmHg | 28.41 ± 3.57 m,n | 40.00 ± 17.15 | 32.16 ± 5.83 | 36.33 ± 11.48 | 0.002 |
| E/e’ ratio | 6.72 ± 1.56 a,o | 12.85 ± 6.75 | 10.87 ± 2.61 p | 16.54 ± 8.03 | <0.0001 |
| Walking distance at 6′, m | 522.69 ± 26.63 q | 387.30 ± 56.14 | 406.65 ± 49.14 | 408.54 ± 73.69 | <0.0001 |
| Walking distance at 6′ ≥ 350 m, n (%) | 29 (100.0) | 19 (82.6) | 18 (78.3) | 18 (75.0) | 0.049 |
| CKD, (yes) n (%) | 0 (0) | 5 (22.2) | 6 (26.7) | 8 (35) | 0.116 |
| Hypertension, (yes) n (%) | 10 (34.5) | 16 (69.6) | 14 (60.9) | 14 (58.3) | 0.063 |
| Dyslipidaemia, (yes) n (%) | 7 (24.1) | 12 (52.2) | 12 (52.2) | 14 (58.3) | 0.051 |
| Smoking, (yes) n (%) | 8 (27.6) | 5 (21.7) | 9 (39.1) | 6 (25.0) | 0.582 |
| Diabetes Mellitus, (yes) n (%) | 2 (6.9) | 8 (34.8) | 6 (26.1) | 9 (37.5) | 0.042 |
| COPD, (yes) n (%) | 3 (10.3) | 5 (21.7) | 4 (17.4) | 6 (25.0) | 0.541 |
| Prior MI, (yes) n (%) | 0 (0) | 4 (26.7) | 8 (44.4) | 12 (50.0) | 0.415 |
| HF etiology, (yes) n (%) | |||||
| Ischemic cardiomyopathy | 0 (0) | 5 (21.7) | 11 (47.8) | 19 (79.2) | 0.004 |
| Valvular cardiomyopathy | 0 (0) | 6 (26.1) | 5 (21.7) | 2 (8.3) | 0.083 |
| Hypertensive cardiomyopathy | 0 (0) | 5 (21.7) | 4 (17.4) | 1 (4.2) | 0.329 |
| Primary cardiomyopathy | 0 (0) | 7 (30.4) | 3 (13) | 2 (8.3) | 0.195 |
| Diuretics, (yes) n (%) | 1 (3.4) | 8 (34.8) | 27 (73.9) | 20 (83.3) | <0.0001 |
| Beta-blockers, (yes) n (%) | 3 (10.3) | 22 (95.7) | 21 (91.3) | 22 (91.7) | <0.0001 |
| ACE-inhibitors, (yes) n (%) | 4 (13.8) | 14 (60.9) | 15 (65.2) | 15 (62.5) | <0.0001 |
| ARBs, (yes) n (%) | 3 (10.3) | 7 (30.4) | 7 (30.4) | 3 (12.5) | 0.132 |
| Statins, (yes) n (%) | 8 (27.6) | 15 (65.2) | 16 (69.6) | 16 (66.7) | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conti, V.; Corbi, G.; Polito, M.V.; Ciccarelli, M.; Manzo, V.; Torsiello, M.; De Bellis, E.; D’Auria, F.; Vitulano, G.; Piscione, F.; et al. Sirt1 Activity in PBMCs as a Biomarker of Different Heart Failure Phenotypes. Biomolecules 2020, 10, 1590. https://doi.org/10.3390/biom10111590
Conti V, Corbi G, Polito MV, Ciccarelli M, Manzo V, Torsiello M, De Bellis E, D’Auria F, Vitulano G, Piscione F, et al. Sirt1 Activity in PBMCs as a Biomarker of Different Heart Failure Phenotypes. Biomolecules. 2020; 10(11):1590. https://doi.org/10.3390/biom10111590
Chicago/Turabian StyleConti, Valeria, Graziamaria Corbi, Maria Vincenza Polito, Michele Ciccarelli, Valentina Manzo, Martina Torsiello, Emanuela De Bellis, Federica D’Auria, Gennaro Vitulano, Federico Piscione, and et al. 2020. "Sirt1 Activity in PBMCs as a Biomarker of Different Heart Failure Phenotypes" Biomolecules 10, no. 11: 1590. https://doi.org/10.3390/biom10111590