Clinical Trials of Stem Cell Therapy for Cerebral Ischemic Stroke



1
Department of Neurosurgery, Hokkaido University Graduate School of Medicine, Sapporo 060-8638, Japan
2
Department of Neurosurgery, Toyama University, Toyama 930-0194, Japan
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2020, 21(19), 7380; https://doi.org/10.3390/ijms21197380
Submission received: 25 August 2020
/
Revised: 24 September 2020
/
Accepted: 2 October 2020
/
Published: 6 October 2020
(This article belongs to the Section Molecular Neurobiology)
Abstract
:Despite recent developments in innovative treatment strategies, stroke remains one of the leading causes of death and disability worldwide. Stem cell therapy is currently attracting much attention due to its potential for exerting significant therapeutic effects on stroke patients. Various types of cells, including bone marrow mononuclear cells, bone marrow/adipose-derived stem/stromal cells, umbilical cord blood cells, neural stem cells, and olfactory ensheathing cells have enhanced neurological outcomes in animal stroke models. These stem cells have also been tested via clinical trials involving stroke patients. In this article, the authors review potential molecular mechanisms underlying neural recovery associated with stem cell treatment, as well as recent advances in stem cell therapy, with particular reference to clinical trials and future prospects for such therapy in treating stroke.
1. Introduction
Besides the rapidly expanding use of thrombectomy as a remedy for acute ischemic stroke [1], few drugs that can effectively recover its sequelae have been developed. Lately, stem cell therapy has been recognized as a promising strategy that functionally enhances recovery from ischemic stroke. Thus, a variety of cells, including bone marrow mononuclear cells (BMMNCs) [2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21], bone marrow/adipose-derived stem/stromal cells (BMSCs/ADMSCs) [4,6,7,22,23,24,25,26,27,28,29,30,31], umbilical cord blood cells (UCBCs) and hematopoietic stem cells [32,33,34,35,36,37], neural stem cells (NSCs) [34,36,38,39,40,41,42,43], olfactory ensheathing cells (OECs) [38], and fetal porcine cells [44], have been explored as candidate donors. Animal studies have indicated that such cells may ameliorate the neurological deficits that follow cerebral stroke, and some have been tested in clinical trials with somewhat favorable results. However, many issues, such as the need to develop techniques that maximally enhance the effects of cell therapy on stroke, remain unresolved, and require clarification [45,46,47,48]. These issues relate to optimal cell types, cell doses, transplantation routes, and candidate patient types (Figure 1). In addition to the refinement of scientific aspects, cell therapy requires an assessment from a commercial point of view, to be successfully distributed as a new therapeutic method. Cell therapy requires the implementation of good manufacturing practice (GMP) grade production method at a reasonable cost for production, preservation, and transfer of the cells. Here, the authors review potential mechanisms underlying stem cell-associated neural recovery, the current status of clinical trials, and future prospects for utilizing cell therapy against ischemic stroke.
2. Pathophysiology of Ischemic Stroke and Therapeutic Targets
To coordinate bodily processes, the brain requires approximately 20% of the entire cardiac output of glucose and oxygen, which is equivalent to only 2% of total body weight [49,50]. As the brain stores little or no energy on its own, disruption of the energy supply, even for a short duration, may lead to catastrophic damage. Ischemic stroke is often caused by the occlusion of a single blood vessel, which subsequently affects its downstream branches via deprivation of glucose and oxygen. Although brain arteries possess a network of collateral vessels that compensate by ensuring the delivery of blood, it is often insufficient to rescue the whole ischemic area, as a result of which ischemic areas closer to the occluded vessel become more susceptible to receiving less blood. Theoretically, an affected brain may be divided into two different damaged areas, namely the ischemic core and the penumbra. Because the blood flow in the ischemic core is lower than the threshold required for cell survival, its cells are irreversibly damaged and die due to necrosis, for which there is no rescue. In contrast, blood flow at the penumbra is too low to support neurological functions but provides the minimal energy required for preventing cells from immediate death, allowing the brain cells to recover if blood flow is restored in time [51]. Therefore, current treatment strategies for stem cell transplantation involve rescuing the penumbra before it dies, or regaining a new neuronal network via cell transplantation [52]. The ischemic cascade in the penumbra progresses with time. Events including the depletion of adenosine triphosphate (ATP); disturbance of ionic concentrations of sodium, potassium, and calcium, increased lactate, acidosis, accumulation of oxygen free radicals, the release of excitotoxic glutamate, and intracellular accumulation of water, may be initiated within minutes to hours following the onset (acute phase) of stroke. This acute phase may be followed by events such as apoptosis of neuronal cells, infiltration, and activation of inflammatory cells (neutrophil, monocyte, and microglia), vasogenic edema, and increase in intracranial pressure, within hours to weeks (subacute phase) [53]. Although the condition of the brain appears to stabilize during the chronic phase (months to years), recent findings indicate that inflammation and blood–brain barrier leakage, which are detrimental to brain recovery, may continue [54,55,56,57].
Currently, standardized treatments, such as thrombectomy and recombinant tissue plasminogen activator (r-tPA) therapy, are applied during the acute phase (<4.5 h). These treatments aim to recanalize the occluded vessel and rescue the penumbra. However, it is often difficult to successfully apply these treatments during short time periods, and reportedly, only 5–10% of all stroke patients become eligible for such treatment [58]. Stem cell therapy, which is known to be effective in all three phases, namely acute, subacute, and chronic, reportedly exerts multiple effects on animal models, such as extending the penumbra period (acute phase), inhibiting unwarranted inflammation (subacute phase), and initiating neuro/angiogenesis (chronic phase) [59].
3. Potential Mechanisms of Stem Cell Therapy
Extensive efforts have been made to elucidate the mode of action underlying the treatment of ischemic stroke via stem cell transplantation, resulting in the publication of multiple descriptive reviews [60,61,62,63,64]. Briefly, transplanted cells are known to exert a variety of neuro- and vascular-protective effects during the various phases of an ischemic stroke. The transplanted cells not only reorganize the neuronal network but also reduce local and systemic inflammation, support axonal regeneration and synaptic sprouting, and reduce glial scars. These mechanisms can be sub-categorized into two distinct types: (i) cell differentiation (cell replacement); (ii) secretion of paracrine factors (Bystander effect).
3.1. Cell Differentiation
Cell replacement may be achieved via the differentiation of transplanted cells into neuronal or vascular cells, which compensates for lost functions, or via the direct settlement and development of neuronal progenitor cells [65,66]. Azizi et al. (1998) examined, ex vivo expanded bone marrow-derived stem cell settlement in the ischemic brain, and indicated that 20% of human BMSCs transplanted into a rat brain remained alive 72 d after infusion, and showed neuronal phenotypes [67]. Our group demonstrated that in vitro chemical induction of BMSCs reduced the expression of mesenchymal cell lineage genes and enhanced the expression of neural genes associated with the release of trophic factors [68,69]. An in vivo study revealed that approximately 50% of engrafted stem cells in the ischemic brain expressed a neuronal phenotype 2 months following cell transplantation [70,71,72]. The migration of stem cells to the damaged area is also reported [72]. Intracerebrally injected stem cells express the CXCR4 receptor, which can bind to stromal cell-derived factor-1 (SDF-1), a chemoattractant. SDF-1 is expressed from the damaged brain and the stem cell uses this CXCR4/SDF-1 axis to migrate to the damaged regions of the brain. However, whether these transplanted and phenotype-altered cells actually compensate for the lost neurological network remains unclear [35].
3.2. Bystander Effect of Stem Cells
The secretion of paracrine factors is an important aspect of the functional multipotency of stem cells, wherein these cells secrete various trophic factors such as cytokines, chemokines, and exosomes, which ameliorate neuronal damage or regenerate new neuronal circuits [73,74,75]. In addition to promoting anti-inflammatory and immunomodulatory effects, these factors induce anti-apoptotic effects and mobilize endogenous stem cells (NSC))/neural progenitor cells (NPCs) [76]. These factors are released into the surrounding environment via direct permeation or extracellular vesicles (EV), and directly ameliorate ischemic damage and down-regulate local as well as systemic inflammation via peripheral immune organs, such as the spleen and the thymus [77,78]. EVs are membrane structures of lipid bilayer nanoparticles that transport proteins, lipids, and nucleic acids through endocytosis. EVs are attracting attention due to their low immunogenicity and high blood-brain barrier (BBB) permeability, which reduces damage and facilitates recovery. These properties along with its versatility make EVs promising as vehicles for drug delivery [79]. Recent reports suggest that EVs can ameliorate ischemic damage through multiple mechanisms including upregulation of angiogenesis, neurogenesis, and modulation of autophagy after ischemic stroke [80,81]. Besides rescuing damaged brain cells, these factors accelerate the regeneration of in-house stem cells. Trophic factors fuel the proliferation of host neuronal progenitor cells, especially of those located around the subventricular zone (SVZ), which are normally inactive.
4. Key Aspects of Clinical Trials
4.1. Overview of Clinical Trial Results
A comprehensive search of the clincaltrials.gov database was performed using the search criteria “ischemic stroke” and “stem cell” on 23/04/2020. A total of 52 results were returned, and the status “completed” for the trial were then manually screened for its publication, following which PubMed articles linked to clincaltrials.gov were evaluated for additional information where appropriate. Further PubMed searches were performed using the terms “ischemic stroke*” and “stem cell” or “neural stem cell (or NSC),” “mesenchymal stem cell or mesenchymal stromal cell” (or “MSC”), “mononuclear cell or mononuclear precursor cell” (or “MNC”) and “Schwann cell” (or “SC”), “olfactory ensheathing or olfactory glia (or OEC)” or “oligodendrocyte precursor (or OPC).” Each article type was then restricted to “clinical trial” to identify any other published studies that had not been registered on clinicaltrials.gov. Additional searches were performed to identify case studies where appropriate. Cell type, cell source, dose, route, timing, patient number, assessment modality, and major outcome were extracted from the manuscript. Cell doses were re-calculated at 60 kg for each patient if the dose was only stated in terms of the number of cells per kilogram (cells/kg). A total of 43 published clinical trials were obtained (Table 1). The trials were categorized into acute (treatment within a week from stroke onset), sub-acute (treatment between 1 week and 6 months from onset), and chronic (treatment after 6 months from onset). Some trials contained multiple treatment time points and were divided by the actual timing of treatment listed in the manuscript.
The methodologies differed widely between trials as well as countries that the trials were executed in (Table 1). Autologous BMMNCs account for the largest portion of cells, followed by autologous bone marrow stem/stromal cells. Small amounts of other sources of cells, such as UCBCs and adipose-derived stem/stromal cells, or neuronal progenitor cells, are also used. Cell doses, which differed widely, ranged between 1 × 106 to 1 × 109, while transplantation routes consisted of intravenous (IV), intraarterial (IA), intrathecal or intracerebroventricular (IT), and intracerebral (IC) routes. Intravascular routes (IV and IA) appear to offer higher cell numbers (up to 109 cells) than those of IC transplantation (106-7) (Figure 2). This is because IC transplantation limits the amount of cells that can be transplanted to avoid a mass effect on the brain, whereas intravascular transplantation does not. IV transplantation appears to be preferable in the acute to sub-acute phase, while IC or IT transplantation is mostly performed during the chronic phase. A majority of these trials were of a preliminary nature and control groups were not set up, whereas some trials did set up control groups consisting of unblinded or blinded patients. All but one study reported no detrimental effects due to cell therapy, while the single study that did, used xenogeneic fetal porcine cells and reported that cell transplantation exerted a negative effect causing seizures and motor function aggravation, which led to the termination of the trial. Although assessment modalities also differed widely between trials, modified Rankin Scale (mRS), National Institute of Health Stroke Scale (NIHSS), and Barthel index were commonly applied.
4.1.1. The Acute Phase of Stroke
Cell transplantation within a week from the onset of a stroke is defined in this review as treatment during the acute phase. Because it is difficult to expand autologous mesenchymal stem cells under ex-vivo conditions within this time frame, BMMNCs or allogenic cells were selected [9,10,12,16,25,32,35,36]. The trials used IV or IA transplantation and did not use IC injections. Spontaneous recovery strongly influenced the final result within this time frame, and thus should be taken into consideration when assessing results. While the smaller, early phase studies that did not set up control groups reported good clinical recovery, two studies of IV and IA transplantation that used control patients reported an absence of statistical difference between functional recovery and control groups [12,25]. However, referring to their post-hoc analysis, one study declared that patients who received cells between 24 and 36 h (trial inclusion 24–48 h) showed a significant improvement in motor recovery one year following treatment [25]. This indicated that patients receiving their BMSCs early via IV injection benefited from the treatment. Currently, studies using these cells under new time course (24–36 h) conditions are ongoing in Japan [82].
4.1.2. The Sub-Acute Phase of Stroke
Cell transplantation after a week for up to 6 months is considered to be sub-acute treatment [2,3,5,8,11,13,14,15,17,20,22,24,26,27,28,34,36,42]. In addition to BMMNCs, autologous BMSCs are used for ex-vivo expansion within a time frame of approximately 1 month. IV or IA transplantation accounts for the majority of trials, while IT transplantation has also been reported. The results of these studies are mostly similar to the favorable results reported in the acute phase of trials using small samples, while larger randomized trials showed heterogeneous efficacy [8,11,14,17,22,24,27,28]. A large trial performed by Prasad et al. included 118 patients, half of which received approximately 3 × 107 autologous BMMNCs between 7 and 10 d following the insult [14]. This phase II multicenter, parallel-group, randomized accessor blinded trial revealed that, although IV infusion of BMMNCs was safe, it did not exert any beneficial effects (BI) on stroke outcome. Lee et al. reported that IV injection of 1 × 108 BMSCs resulted in better recovery and reduced mortality for up to 5 years from treatment initiation, compared with randomized controls [28], whereas Jaillard et al. did not report an overall benefit [27]. Differences in cell processing procedures, patient types, and timing make arriving at a specific conclusion much more difficult. The results of IA treatments also differed between trials. Bhatia reported a good trend (P = 0.06) of recovery via IA transplantation of autologous BMMNCs [8], while others did not report a difference [11,17]. A recent report by Savitz et al. discussed a new aspect regarding logistics [17]. Autologous stem cells are mainly processed at the transplantation site and do not require cell preservation while transferring. However, it is impossible to make these commercially available unless a cell preservation and logistics process is developed for wide commercial distribution. They reported that bone marrow extracted from the patient was transferred to a sorting facility, and shipped back to the hospital for transplantation. These procedures are considered very important for cell transplantation purposes especially when using autologous stem cells.
4.1.3. The Chronic Phase of Stroke
Initiating treatment 6 months after an ischemic stroke is considered as treatment during the chronic phase [4,5,6,7,18,19,23,29,30,31,33,36,37,38,39,40,41,42,43,44,66]. Currently, no effective treatments are available for this phase, and thus the establishment of an effective treatment process is highly anticipated. Interestingly, IC or IT injections account for most transplantation routes within this time frame. However, only one study investigating IC transplantation had used control patients, and this study reported that IC transplantation of CD34 positive hematopoietic cells initiated marked neurological recovery compared with that of the control [38]. Although the number of patients screened was small (N = 6 each), IT injection resulted in better recovery compared with that of the control [42]. The results of IV transplantation varied between trials, where some studies reported significant recovery compared with that of the control [5,7], while others did not [4,6,21]. Randomized clinical trials using larger patient samples are currently ongoing (NCT02448641, NCT02448641) and the results are expected soon.
5. Unsolved Issues Associated with Optimal Treatment
5.1. Stem Cell Types
Many stem cell types, including mononuclear cells (MNCs), MSCs, OECs, and NSCs have been intensively examined as promising sources and tested via clinical trials, as previously mentioned. Some cells use gene-modification processes to enhance the release of trophic factors and survival [30,31]. Autologous cells (MNCs, MSCs, OECs) possess the advantage of being associated with a low risk for post-transplant rejection and allergies, whereas allogenic cells (MSCs, NSCs) are considered to be advantageous due to easier accessibility resulting from large-scale manufacturing and availability of standardized stocks. Clinical trials discussed here show a trend of moving from autologous to allogeneic cells, which aims for large-scale manufacturing for commercial purposes. Prior to distributing an available cell source for commercial purposes, several factors such as safety, efficiency, cost, and feasibility of manufacturing on a large scale, must be taken into consideration. Recent reports indicate that MSCs from the same bone marrow may express different functional and molecular phenotypes if produced using different facilities and methods [83]. This is indicative of the difficulties encountered in maintaining consistent quality during cell preparation. Several basic studies have compared the efficacy of different cell sources as treatments [84,85]. However, each stem cell type comes with its own benefits and drawbacks, and at present, which cell type represents the most beneficial treatment remains unclear.
5.1.1. MNCs
An advantage associated with MNCs is that these may be obtained from patients without resorting to ex-vivo expansion. Approximately, 1 × 108 MNCs can be obtained from 50 mL of bone marrow, and transplanted immediately following isolation [83]. Therefore, this cell type is widely used in the acute and subacute phases, that nearly half of the trials used bone marrow-derived mononuclear cells (Table 1). However, a disadvantage associated with using MNCs is that MNCs only contain very small amounts of MSCs (0.1–0.01% of MNCs), which, according to some researchers, casts doubts regarding its efficacy.
5.1.2. Hematopoietic Stem Cells (CD34 Positive)
Hematopoietic stem cells, expressing CD34, which are obtained from both bone marrow and peripheral blood are also frequently used. These cells, which have a long history of being harvested and used to treat hematological disorders under clinical conditions, are considered safe for clinical use. These cells show a strong capacity for angiogenesis, as witnessed in diseases such as myocardial infarction and limb ischemia [86,87,88], and show potential for reorganizing the vascular network in the brain [89]. An advantage of using these cells is that ex-vivo cell expansion, which requires time and effort, is not required. However, these cells show limited capacity for neuronal differentiation and are thus unable to complete the complex restoration process needed to repair ischemic stroke-related damage. These cells tend to accumulate during inflammation, and may not reach the brain when other organs, such as heart and lung, are inflamed [90].
5.1.3. MSCs
The nomenclature of MSCs (stromal or stem cells) is convoluted. The International Society for Cell & Gene Therapy (ISCT) Mesenchymal Stromal Cell Committee has established the minimal criteria that are required for a cell to qualify as a mesenchymal stromal cell: (i) plastic-adherence; (ii) CD73, CD90, and CD105 expression; 3) absence of expression of hematopoietic and endothelial markers CD11b, CD14, CD19, CD34, CD45, CD79a, and HLA-DR; (iv) capable of in vitro differentiation into adipocyte, chondrocyte, and osteoblast lineages [91,92]. However, it was later observed that some cell-surface markers displayed an ability to be reversibly upregulated or downregulated according to cell culture conditions [93,94,95]. The use of “stromal” and “stem” to describe MSCs is almost equivalently found in the literature, and the ISCT suggests that “mesenchymal stromal cell” should be used to describe bulk unfractionated populations, which include fibroblasts, myofibroblasts, and stem/progenitor cells, whereas “mesenchymal stem cell” should be used for purified stem/progenitor cells [96]. An abundance of preclinical evidence indicates that MSCs possess an ability to ameliorate tissue damage and facilitate functional recovery via multiple processes, including immunomodulation, pro-angiogenic signaling, neurotrophic factor secretion, and neural differentiation [70,71,97,98]. MSCs can be harvested from bone marrow, abdominal fat tissue, teeth, umbilical cord blood, and Wharton’s Jelly. MSCs have several advantages over other stem cells due to well-established harvesting methods, low risk for tumorigenicity, and the absence of ethical issues [64]. MSCs possess a unique immune tolerance, where even allogenic MSCs, which do not show immunological rejection responses, are approved for graft vs host disease (GvHD) treatment in many countries [99]. Gene modification of BMSCs has also been reported. SanBio developed SB623 cells through transient transfection of a plasmid containing the human Notch-1 intracellular domain [100]. This cell showed better neuroprotective properties, via higher trophic factor secretion, stronger anti-inflammatory effect, and neuro-/angiogenesis. They recently reported that SB623 was associated with a rate of recovery from chronic traumatic brain injury, which was statistically significant (unpublished data).
5.1.4. NSCs
NSCs are multipotent progenitor cells capable of integrating with the host brain by transforming into neural cells, oligodendrocytes, and astrocytes [101,102]. These cells survive in the host brain and exhibit neuroprotective effects through extending processes, expressing neurotransmitters, and forming functional synapses [103,104]. Although these cells are mostly found during the development of the fetal CNS, they are also present in a limited number of other regions of the adult brain, such as the subventricular zone next to the cerebral lateral ventricle [105]. Although NSCs appear to be ideal for refilling lost neuronal networks, the cells need to be harvested from the fetus, which poses ethical issues and there is the possibility of immune rejection by the host. Other potential concerns include whether NSCs can initiate angiogenesis, differentiate to vascular structures, since brain reconstruction requires other cell types including vascular cells, such as endothelial cells, and remain pluripotent after adulthood.
5.1.5. OECs
OECs surround olfactory neurons, and function as scavengers of pathogens and debris around the border between the CNS and the nasal mucosa. Additionally, they reportedly express neurotrophic factors that facilitate olfactory regeneration. OECs can be harvested from the nasal mucosa and the olfactory bulb. These cells secrete neurotrophic factors, such as the stromal cell-derived factor 1-a (SDF-1 a), and the brain-derived neurotrophic factor (BDNF), which promote neuronal regeneration [106,107]. These cells have been extensively examined in relation to spinal cord injury, but investigating its usefulness in treating ischemic stroke has just started [108,109,110,111]. Data indicating its potential or detrimental nature are scant.
5.1.6. Other Cell Types
Embryonic stem (ES) cells and induced pluripotent stem (iPS) cells have also been examined in preclinical studies [112,113,114]. Their pluripotency is an attractive characteristic in relation to its usefulness in treatment. However, data regarding clinical trials of these cells are currently unavailable due to factors associated with ethics and tumorigenicity.
5.2. Cell Dose and Route
IV transplantation has the advantage of showing the lowest invasiveness, thereby allowing multiple injections. The method also does not require special equipment for transplantation. However, despite its efficacy, small amounts of cells are often found in the damaged lesion, and most cells are trapped in the lungs [71]. The bystander effect exerted by neurotrophic factors resulting in the amelioration of apoptosis and inflammation are considered as the main therapeutic mechanisms underlying IV transplantation. This is useful in the acute phase of ischemic stroke, but may not be beneficial in the chronic phase during which cell damage and inflammation are mostly settled. The IA approach is considered superior to IV administering in delivering more cells to the lesion. However, recent reports have indicated that this method is not effective for cell engraftment in the brain [2,3,15]. Additional ischemic damage caused by cell clusters clogging the arteries is a drawback of this method [17]. IT application, which can deliver a large number of cells to the subarachnoid space, is less invasive relative to IC transplantation. However, the rate of cell engraftment is unclear, and complications, such as hydrocephalus and liquorrhea, may arise. The IC approach of directly administering cells achieves the highest level of cell engraftment but requires invasive surgery, and the risk of additional brain damage being caused by injection needles should not be underestimated [115].
As previously mentioned, IV and IA transplantations, using a large number of cells ranging up to 10e9 cells, are preferred in the acute and sub-acute phases, whereas, in the chronic phase, IC transplantation with a smaller cell dose of 107 cells is preferred. Interestingly, most IV/IA transplanted stem cells are not found in the brain but the other organs, such as lungs, spleen, and bladder [2,3,9,15]. Rosado-de-Castro et al. transplanted technetium-99m labeled BMMNCs intravenously and intra-arterially into sub-acute stroke patients, and found that only 0.6–0.9 % of cells were present in the brain 2–24 h after transplantation [15]. They reported that the IA transplantation group had higher radioactive counts in the liver (2 h: 40% and 24 h: 47%) and spleen (2 h: 6% and 24 h: 7%), and low counts in the lungs (2 h: 7% and 24 h: 4%), compared to IV transplantation (liver 14% and 19%, spleen 2% and 3%, and lung 21% and 7%, respectively). According to this result, intravenously and intra-arterially transplanted cells are distributed differently soon after transplantation, following which intravenously transplanted cells are found in the lung, while intra-arterially transplanted cells are in the liver. This result is similar to other reports that intra-arterially transplanted technetium-99m labeled BMMNCs, which were found in the brain 2 h after ischemia with the main uptake occurring in the liver, lungs, spleen, kidneys, and bladder. After 24 h, the cells were hardly distinguishable in the brain, while uptake was still observed in the other organs [2]. These results indicate that cells that are transplanted intravenously or intra-arterially are unable to stay in the brain for a long time. We have recently revealed that intracerebrally injected iron labeled BMSCs can migrate, settle in the ischemic area, and survive for more than 2 years (unpublished data) [116].
5.3. Patient Characteristics and Outcome Measure
It is difficult to estimate which pathological aspect (timing, stroke type, comorbidity disease) of a patient will most benefit from stem cell treatment, via the use of animal models. Clinical trials involving a large number of patients or real-world data are required to resolve this issue. Outcome evaluation needs to be adequately refined to accurately monitor the results of clinical trials. mRS, NIHSS, and BI are often used in clinical trials, but mRS is too broad-based to detect small differences, while NIHSS is mostly intended for acute assessment of patients.
6. Future Directions
While the results of the clinical trials are promising, there are other factors such as regulatory approval and the overall cost to be considered for the widespread use of stem cells in the treatment of ischemic stroke. The key is to achieve a balance between the quality of cells produced and the costs involved, two apparently conflicting parameters.
6.1. Producing Good Cells (GMP Grade)
Most of the clinical trials, especially those using autologous cells, were performed completely within a single hospital, where cell preparation was also done on-site. Some clinical trials mentioned about the GMP grade cell production, while the others did not. GMP is a system for ensuring quality controlled drug production to minimize the risks. It covers all aspects of production such as the handling and checking of materials, producing drugs according to the standard operating procedures (SOP), appropriate packing of drugs, and delivery management. Following GMP is time-consuming and costly, however, the cells will not qualify for drug use in many countries unless GMP is followed. The problem with this is that each country possesses its own GMP requirement. Pharmaceutical companies need to fulfill the requirement of the country where drug production will be carried out. Many regulatory agencies are working together to develop a set of common rules for drug approval, and this policy can help achieve faster drug development and approval in the future.
6.2. Producing Cells at Low Cost
Many clinical trials are executed as an investigator-oriented trial, where government or public funds are used for cell production. Cell preparation can be very expensive and to normalize stem cells as a standard treatment method, the cost needs to be minimized. Current cell expanding procedures requires the expertise of experienced technicians. Allogeneic stem cells are suitable for bulk production using automated cell producing machines; however, there is a need for innovative technology when it comes to autologous stem cells, which are made-to-order and are difficult to be adapted for automated production. Cell logistics are another key issue. Stem cells differ from ordinary low-molecular drug compounds in that stem cell efficacy is dependent on viability, which means that adequate cell preservation is mandatory. Cryopreservation and shipping of stem cells are often adopted in the clinical trials, but the reagent for cryopreservation contains DMSO, a possible toxic reagent, and shipping under extremely low temperature (using liquid nitrogen) is costly. Therefore, the production and transfer of stem cells at an affordable cost require further optimization.
7. Conclusions
Stem cell therapy is expected to ameliorate the sequelae of those ischemic stroke patients who have reached the acute phase, a stage at which no proven treatment is currently available. The results of clinical trials are promising, in the sense that most methods used for stem cell transplantation appear to be safe. It seems that intravenous or intra-arterial transplantation is preferred in the acute phase, where the aim is to ameliorate systemic and local inflammation and cell engraftment is not required. Alternatively, intracerebral transplantation is preferred in the chronic phase, where cell engraftment is considered the objective of cell therapy. However, optimal parameters including the choice of cell type, cell dose, and patient characteristics remain elusive and further research is needed for maximizing the effects of the proposed methods. To achieve this, it is expected that the integration of pre-clinical and clinical research will take place in the near future.
Author Contributions
Conceptualization, M.K.; methodology, M.K.; investigation, M.K.; data curation, M.K.; writing—original draft preparation, M.K.; writing—review and editing, M.K, H.S., S.K., and K.H.; funding acquisition, K.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by AMED under Grant Number JP17bk0104045h0003.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.; Mitchell, P.J.; Demchuk, A.M.; Davalos, A.; Majoie, C.B.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Barbosa da Fonseca, L.M.; Gutfilen, B.; Rosado de Castro, P.H.; Battistella, V.; Goldenberg, R.C.; Kasai-Brunswick, T.; Chagas, C.L.; Wajnberg, E.; Maiolino, A.; Salles Xavier, S.; et al. Migration and homing of bone-marrow mononuclear cells in chronic ischemic stroke after intra-arterial injection. Exp. Neurol. 2010, 221, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Battistella, V.; de Freitas, G.R.; da Fonseca, L.M.; Mercante, D.; Gutfilen, B.; Goldenberg, R.C.; Dias, J.V.; Kasai-Brunswick, T.H.; Wajnberg, E.; Rosado-de-Castro, P.H.; et al. Safety of autologous bone marrow mononuclear cell transplantation in patients with nonacute ischemic stroke. Regen. Med. 2011, 6, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Bhasin, A.; Kumaran, S.S.; Bhatia, R.; Mohanty, S.; Srivastava, M.V.P. Safety and Feasibility of Autologous Mesenchymal Stem Cell Transplantation in Chronic Stroke in Indian patients. A four-year follow up. J. Stem Cells Regen. Med. 2017, 13, 14–19. [Google Scholar]
- Bhasin, A.; Srivastava, M.; Bhatia, R.; Mohanty, S.; Kumaran, S.; Bose, S. Autologous intravenous mononuclear stem cell therapy in chronic ischemic stroke. J. Stem Cells Regen. Med. 2012, 8, 181–189. [Google Scholar]
- Bhasin, A.; Srivastava, M.V.; Kumaran, S.S.; Mohanty, S.; Bhatia, R.; Bose, S.; Gaikwad, S.; Garg, A.; Airan, B. Autologous mesenchymal stem cells in chronic stroke. Cerebrovasc. Dis. Extra 2011, 1, 93–104. [Google Scholar] [CrossRef]
- Bhasin, A.; Srivastava, M.V.; Mohanty, S.; Bhatia, R.; Kumaran, S.S.; Bose, S. Stem cell therapy: A clinical trial of stroke. Clin. Neurol. Neurosurg. 2013, 115, 1003–1008. [Google Scholar] [CrossRef]
- Bhatia, V.; Gupta, V.; Khurana, D.; Sharma, R.R.; Khandelwal, N. Randomized Assessment of the Safety and Efficacy of Intra-Arterial Infusion of Autologous Stem Cells in Subacute Ischemic Stroke. AJNR Am. J. Neuroradiol. 2018, 39, 899–904. [Google Scholar] [CrossRef] [Green Version]
- Correa, P.L.; Mesquita, C.T.; Felix, R.M.; Azevedo, J.C.; Barbirato, G.B.; Falcao, C.H.; Gonzalez, C.; Mendonca, M.L.; Manfrim, A.; de Freitas, G.; et al. Assessment of intra-arterial injected autologous bone marrow mononuclear cell distribution by radioactive labeling in acute ischemic stroke. Clin. Nucl. Med. 2007, 32, 839–841. [Google Scholar] [CrossRef]
- Friedrich, M.A.; Martins, M.P.; Araujo, M.D.; Klamt, C.; Vedolin, L.; Garicochea, B.; Raupp, E.F.; Sartori El Ammar, J.; Machado, D.C.; Costa, J.C.; et al. Intra-arterial infusion of autologous bone marrow mononuclear cells in patients with moderate to severe middle cerebral artery acute ischemic stroke. Cell Transplant. 2012, 21, S13–S21. [Google Scholar] [CrossRef]
- Ghali, A.A.; Yousef, M.K.; Ragab, O.A.; ElZamarany, E.A. Intra-arterial Infusion of Autologous Bone Marrow Mononuclear Stem Cells in Subacute Ischemic Stroke Patients. Front. Neurol. 2016, 7, 228. [Google Scholar] [CrossRef] [PubMed]
- Moniche, F.; Gonzalez, A.; Gonzalez-Marcos, J.R.; Carmona, M.; Pinero, P.; Espigado, I.; Garcia-Solis, D.; Cayuela, A.; Montaner, J.; Boada, C.; et al. Intra-arterial bone marrow mononuclear cells in ischemic stroke: A pilot clinical trial. Stroke 2012, 43, 2242–2244. [Google Scholar] [CrossRef] [PubMed]
- Prasad, K.; Mohanty, S.; Bhatia, R.; Srivastava, M.V.; Garg, A.; Srivastava, A.; Goyal, V.; Tripathi, M.; Kumar, A.; Bal, C.; et al. Autologous intravenous bone marrow mononuclear cell therapy for patients with subacute ischaemic stroke: A pilot study. Indian J. Med. Res. 2012, 136, 221–228. [Google Scholar] [PubMed]
- Prasad, K.; Sharma, A.; Garg, A.; Mohanty, S.; Bhatnagar, S.; Johri, S.; Singh, K.K.; Nair, V.; Sarkar, R.S.; Gorthi, S.P.; et al. Intravenous autologous bone marrow mononuclear stem cell therapy for ischemic stroke: A multicentric, randomized trial. Stroke 2014, 45, 3618–3624. [Google Scholar] [CrossRef] [Green Version]
- Rosado-de-Castro, P.H.; Schmidt Fda, R.; Battistella, V.; Lopes de Souza, S.A.; Gutfilen, B.; Goldenberg, R.C.; Kasai-Brunswick, T.H.; Vairo, L.; Silva, R.M.; Wajnberg, E.; et al. Biodistribution of bone marrow mononuclear cells after intra-arterial or intravenous transplantation in subacute stroke patients. Regen. Med. 2013, 8, 145–155. [Google Scholar] [CrossRef] [Green Version]
- Savitz, S.I.; Misra, V.; Kasam, M.; Juneja, H.; Cox, C.S., Jr.; Alderman, S.; Aisiku, I.; Kar, S.; Gee, A.; Grotta, J.C. Intravenous autologous bone marrow mononuclear cells for ischemic stroke. Ann. Neurol. 2011, 70, 59–69. [Google Scholar] [CrossRef]
- Savitz, S.I.; Yavagal, D.; Rappard, G.; Likosky, W.; Rutledge, N.; Graffagnino, C.; Alderazi, Y.; Elder, J.A.; Chen, P.R.; Budzik, R.F., Jr.; et al. A Phase 2 Randomized, Sham-Controlled Trial of Internal Carotid Artery Infusion of Autologous Bone Marrow-Derived ALD-401 Cells in Patients With Recent Stable Ischemic Stroke (RECOVER-Stroke). Circulation 2019, 139, 192–205. [Google Scholar] [CrossRef]
- Sharma, A.; Sane, H.; Gokulchandran, N.; Khopkar, D.; Paranjape, A.; Sundaram, J.; Gandhi, S.; Badhe, P. Autologous bone marrow mononuclear cells intrathecal transplantation in chronic stroke. Stroke Res. Treat. 2014, 2014, 234095. [Google Scholar] [CrossRef] [Green Version]
- Suarez-Monteagudo, C.; Hernandez-Ramirez, P.; Alvarez-Gonzalez, L.; Garcia-Maeso, I.; de la Cuetara-Bernal, K.; Castillo-Diaz, L.; Bringas-Vega, M.L.; Martinez-Aching, G.; Morales-Chacon, L.M.; Baez-Martin, M.M.; et al. Autologous bone marrow stem cell neurotransplantation in stroke patients. An open study. Restor. Neurol. Neurosci. 2009, 27, 151–161. [Google Scholar] [CrossRef]
- Taguchi, A.; Sakai, C.; Soma, T.; Kasahara, Y.; Stern, D.M.; Kajimoto, K.; Ihara, M.; Daimon, T.; Yamahara, K.; Doi, K.; et al. Intravenous Autologous Bone Marrow Mononuclear Cell Transplantation for Stroke: Phase1/2a Clinical Trial in a Homogeneous Group of Stroke Patients. Stem Cells Dev. 2015, 24, 2207–2218. [Google Scholar] [CrossRef] [Green Version]
- Bhasin, A.; Srivastava, M.V.P.; Mohanty, S.; Vivekanandhan, S.; Sharma, S.; Kumaran, S.; Bhatia, R. Paracrine Mechanisms of Intravenous Bone Marrow-Derived Mononuclear Stem Cells in Chronic Ischemic Stroke. Cerebrovasc. Dis. Extra 2016, 6, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Bang, O.Y.; Lee, J.S.; Lee, P.H.; Lee, G. Autologous mesenchymal stem cell transplantation in stroke patients. Ann. Neurol. 2005, 57, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Duma, C.; Kopyov, O.; Kopyov, A.; Berman, M.; Lander, E.; Elam, M.; Arata, M.; Weiland, D.; Cannell, R.; Caraway, C.; et al. Human intracerebroventricular (ICV) injection of autologous, non-engineered, adipose-derived stromal vascular fraction (ADSVF) for neurodegenerative disorders: Results of a 3-year phase 1 study of 113 injections in 31 patients. Mol. Biol. Rep. 2019, 46, 5257–5272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, J.; Guo, Y.; Tan, S.; Li, Z.; Xie, H.; Chen, P.; Wang, K.; He, Z.; He, P.; Ke, Y.; et al. Autologous Endothelial Progenitor Cells Transplantation for Acute Ischemic Stroke: A 4-Year Follow-Up Study. Stem Cells Transl. Med. 2019, 8, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Hess, D.C.; Wechsler, L.R.; Clark, W.M.; Savitz, S.I.; Ford, G.A.; Chiu, D.; Yavagal, D.R.; Uchino, K.; Liebeskind, D.S.; Auchus, A.P.; et al. Safety and efficacy of multipotent adult progenitor cells in acute ischaemic stroke (MASTERS): A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Neurol. 2017, 16, 360–368. [Google Scholar] [CrossRef]
- Honmou, O.; Houkin, K.; Matsunaga, T.; Niitsu, Y.; Ishiai, S.; Onodera, R.; Waxman, S.G.; Kocsis, J.D. Intravenous administration of auto serum-expanded autologous mesenchymal stem cells in stroke. Brain 2011, 134, 1790–1807. [Google Scholar] [CrossRef] [Green Version]
- Jaillard, A.; Hommel, M.; Moisan, A.; Zeffiro, T.A.; Favre-Wiki, I.M.; Barbieux-Guillot, M.; Vadot, W.; Marcel, S.; Lamalle, L.; Grand, S.; et al. Autologous Mesenchymal Stem Cells Improve Motor Recovery in Subacute Ischemic Stroke: A Randomized Clinical Trial. Transl. Stroke Res. 2020. [Google Scholar] [CrossRef]
- Lee, J.S.; Hong, J.M.; Moon, G.J.; Lee, P.H.; Ahn, Y.H.; Bang, O.Y. A long-term follow-up study of intravenous autologous mesenchymal stem cell transplantation in patients with ischemic stroke. Stem Cells 2010, 28, 1099–1106. [Google Scholar] [CrossRef]
- Levy, M.L.; Crawford, J.R.; Dib, N.; Verkh, L.; Tankovich, N.; Cramer, S.C. Phase I/II Study of Safety and Preliminary Efficacy of Intravenous Allogeneic Mesenchymal Stem Cells in Chronic Stroke. Stroke 2019, 50, 2835–2841. [Google Scholar] [CrossRef]
- Steinberg, G.K.; Kondziolka, D.; Wechsler, L.R.; Lunsford, L.D.; Coburn, M.L.; Billigen, J.B.; Kim, A.S.; Johnson, J.N.; Bates, D.; King, B.; et al. Clinical Outcomes of Transplanted Modified Bone Marrow-Derived Mesenchymal Stem Cells in Stroke: A Phase 1/2a Study. Stroke 2016, 47, 1817–1824. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, G.K.; Kondziolka, D.; Wechsler, L.R.; Lunsford, L.D.; Kim, A.S.; Johnson, J.N.; Bates, D.; Poggio, G.; Case, C.; McGrogan, M.; et al. Two-year safety and clinical outcomes in chronic ischemic stroke patients after implantation of modified bone marrow-derived mesenchymal stem cells (SB623): A phase 1/2a study. J. Neurosurg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Bentley, P.; Hamady, M.; Marley, S.; Davis, J.; Shlebak, A.; Nicholls, J.; Williamson, D.A.; Jensen, S.L.; Gordon, M.; et al. Intra-Arterial Immunoselected CD34+ Stem Cells for Acute Ischemic Stroke. Stem Cells Transl. Med. 2014, 3, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.C.; Lin, S.Z.; Fan, J.R.; Lin, C.H.; Lee, W.; Lin, C.C.; Liu, Y.J.; Tsai, C.H.; Chen, J.C.; Cho, D.Y.; et al. Intracerebral implantation of autologous peripheral blood stem cells in stroke patients: A randomized phase II study. Cell Transplant. 2014, 23, 1599–1612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.; Zhu, W.; Zhu, J.; Wu, L.; Xu, G.; Liu, X. Feasibility of delivering mesenchymal stem cells via catheter to the proximal end of the lesion artery in patients with stroke in the territory of the middle cerebral artery. Cell Transplant. 2013, 22, 2291–2298. [Google Scholar] [CrossRef] [PubMed]
- Laskowitz, D.T.; Bennett, E.R.; Durham, R.J.; Volpi, J.J.; Wiese, J.R.; Frankel, M.; Shpall, E.; Wilson, J.M.; Troy, J.; Kurtzberg, J. Allogeneic Umbilical Cord Blood Infusion for Adults with Ischemic Stroke: Clinical Outcomes from a Phase I Safety Study. Stem Cells Transl. Med. 2018, 7, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Qiao, L.Y.; Huang, F.J.; Zhao, M.; Xie, J.H.; Shi, J.; Wang, J.; Lin, X.Z.; Zuo, H.; Wang, Y.L.; Geng, T.C. A two-year follow-up study of cotransplantation with neural stem/progenitor cells and mesenchymal stromal cells in ischemic stroke patients. Cell Transplant. 2014, 23, S65–S72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Ji, H.; Li, M.; Zhou, J.; Bai, W.; Zhong, Z.; Li, N.; Zhu, D.; Zhang, Z.; Liu, Y.; et al. Intrathecal Administration of Autologous CD34 Positive Cells in Patients with Past Cerebral Infarction: A Safety Study. ISRN Neurol. 2013, 2013, 128591. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Xi, H.; Huang, H.; Zhang, F.; Liu, Y.; Chen, D.; Xiao, J. Multiple cell transplantation based on an intraparenchymal approach for patients with chronic phase stroke. Cell Transplant. 2013, 22, S83–S91. [Google Scholar] [CrossRef]
- Kalladka, D.; Sinden, J.; Pollock, K.; Haig, C.; McLean, J.; Smith, W.; McConnachie, A.; Santosh, C.; Bath, P.M.; Dunn, L.; et al. Human neural stem cells in patients with chronic ischaemic stroke (PISCES): A phase 1, first-in-man study. Lancet 2016, 388, 787–796. [Google Scholar] [CrossRef] [Green Version]
- Kondziolka, D.; Steinberg, G.K.; Wechsler, L.; Meltzer, C.C.; Elder, E.; Gebel, J.; Decesare, S.; Jovin, T.; Zafonte, R.; Lebowitz, J.; et al. Neurotransplantation for patients with subcortical motor stroke: A phase 2 randomized trial. J. Neurosurg. 2005, 103, 38–45. [Google Scholar] [CrossRef]
- Kondziolka, D.; Wechsler, L.; Goldstein, S.; Meltzer, C.; Thulborn, K.R.; Gebel, J.; Jannetta, P.; DeCesare, S.; Elder, E.M.; McGrogan, M.; et al. Transplantation of cultured human neuronal cells for patients with stroke. Neurology 2000, 55, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Rabinovich, S.S.; Seledtsov, V.I.; Banul, N.V.; Poveshchenko, O.V.; Senyukov, V.V.; Astrakov, S.V.; Samarin, D.M.; Taraban, V.Y. Cell therapy of brain stroke. Bull. Exp. Biol. Med. 2005, 139, 126–128. [Google Scholar] [CrossRef] [PubMed]
- Muir, K.W.; Bulters, D.; Willmot, M.; Sprigg, N.; Dixit, A.; Ward, N.; Tyrrell, P.; Majid, A.; Dunn, L.; Bath, P.; et al. Intracerebral implantation of human neural stem cells and motor recovery after stroke: Multicentre prospective single-arm study (PISCES-2). J. Neurol. Neurosurg. Psychiatry 2020, 91, 396–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savitz, S.I.; Dinsmore, J.; Wu, J.; Henderson, G.V.; Stieg, P.; Caplan, L.R. Neurotransplantation of fetal porcine cells in patients with basal ganglia infarcts: A preliminary safety and feasibility study. Cerebrovasc. Dis. 2005, 20, 101–107. [Google Scholar] [CrossRef]
- Boltze, J.; Modo, M.M.; Mays, R.W.; Taguchi, A.; Jolkkonen, J.; Savitz, S.I.; Consortium, S. Stem Cells as an Emerging Paradigm in Stroke 4: Advancing and Accelerating Preclinical Research. Stroke 2019, 50, 3299–3306. [Google Scholar] [CrossRef]
- Savitz, S.I.; Chopp, M.; Deans, R.; Carmichael, T.; Phinney, D.; Wechsler, L.; Participants, S. Stem Cell Therapy as an Emerging Paradigm for Stroke (STEPS) II. Stroke 2011, 42, 825–829. [Google Scholar] [CrossRef] [Green Version]
- Savitz, S.I.; Cramer, S.C.; Wechsler, L.; Consortium, S. Stem cells as an emerging paradigm in stroke 3: Enhancing the development of clinical trials. Stroke 2014, 45, 634–639. [Google Scholar] [CrossRef] [Green Version]
- The STEPS Participants. Stem Cell Therapies as an Emerging Paradigm in Stroke (STEPS): Bridging basic and clinical science for cellular and neurogenic factor therapy in treating stroke. Stroke 2009, 40, 510–515. [Google Scholar] [CrossRef] [Green Version]
- Xing, C.Y.; Tarumi, T.; Liu, J.; Zhang, Y.; Turner, M.; Riley, J.; Tinajero, C.D.; Yuan, L.J.; Zhang, R. Distribution of cardiac output to the brain across the adult lifespan. J. Cereb. Blood Flow Metab. 2017, 37, 2848–2856. [Google Scholar] [CrossRef]
- Markus, H.S. Cerebral perfusion and stroke. J. Neurol. Neurosurg. Psychiatry 2004, 75, 353–361. [Google Scholar] [CrossRef]
- Powers, W.J.; Grubb, R.L., Jr.; Raichle, M.E. Physiological responses to focal cerebral ischemia in humans. Ann. Neurol. 1984, 16, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Stonesifer, C.; Corey, S.; Ghanekar, S.; Diamandis, Z.; Acosta, S.A.; Borlongan, C.V. Stem cell therapy for abrogating stroke-induced neuroinflammation and relevant secondary cell death mechanisms. Prog. Neurobiol. 2017, 158, 94–131. [Google Scholar] [CrossRef] [PubMed]
- Kawabori, M.; Yenari, M.A. Inflammatory responses in brain ischemia. Curr. Med. Chem. 2015, 22, 1258–1277. [Google Scholar] [CrossRef] [Green Version]
- Kawabori, M.; Yenari, M.A. The role of the microglia in acute CNS injury. Metab. Brain Dis. 2015, 30, 381–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Z.; Lee, J.E.; Yenari, M.A. Stroke: Molecular mechanisms and potential targets for treatment. Curr. Mol. Med. 2003, 3, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Kawabori, M.; Hokari, M.; Zheng, Z.; Kim, J.Y.; Calosing, C.; Hsieh, C.L.; Nakamura, M.C.; Yenari, M.A. Triggering Receptor Expressed on Myeloid Cells-2 Correlates to Hypothermic Neuroprotection in Ischemic Stroke. Ther. Hypothermia Temp. Manag. 2013, 3, 189–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawabori, M.; Kacimi, R.; Kauppinen, T.; Calosing, C.; Kim, J.Y.; Hsieh, C.L.; Nakamura, M.C.; Yenari, M.A. Triggering receptor expressed on myeloid cells 2 (TREM2) deficiency attenuates phagocytic activities of microglia and exacerbates ischemic damage in experimental stroke. J. Neurosci. 2015, 35, 3384–3396. [Google Scholar] [CrossRef] [PubMed]
- Henninger, N.; Fisher, M. Extending the Time Window for Endovascular and Pharmacological Reperfusion. Transl. Stroke Res. 2016, 7, 284–293. [Google Scholar] [CrossRef]
- Kwak, K.A.; Kwon, H.B.; Lee, J.W.; Park, Y.S. Current Perspectives Regarding Stem Cell-based Therapy for Ischemic Stroke. Curr. Pharm. Des. 2018, 24, 3332–3340. [Google Scholar] [CrossRef]
- Barker, R.A.; Gotz, M.; Parmar, M. New approaches for brain repair-from rescue to reprogramming. Nature 2018, 557, 329–334. [Google Scholar] [CrossRef]
- Misra, V.; Ritchie, M.M.; Stone, L.L.; Low, W.C.; Janardhan, V. Stem cell therapy in ischemic stroke: Role of IV and intra-arterial therapy. Neurology 2012, 79, S207–S212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Zhang, Q.; Wang, W.; Lin, F.; Wang, S.; Zhao, J. Mesenchymal stem cell therapy for ischemic stroke: A look into treatment mechanism and therapeutic potential. J. Neurol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, S.; Shichinohe, H.; Houkin, K.; Iwasaki, Y. Autologous bone marrow stromal cell transplantation for central nervous system disorders—Recent progress and perspective for clinical application. J. Stem Cells Regen. Med. 2011, 7, 2–13. [Google Scholar] [PubMed]
- Cui, L.L.; Golubczyk, D.; Tolppanen, A.M.; Boltze, J.; Jolkkonen, J. Cell therapy for ischemic stroke: Are differences in preclinical and clinical study design responsible for the translational loss of efficacy? Ann. Neurol. 2019, 86, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Ceci, M.; Mariano, V.; Romano, N. Zebrafish as a translational regeneration model to study the activation of neural stem cells and role of their environment. Rev. Neurosci. 2018, 30, 45–66. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Qiu, R.; Li, L.; He, D.; Lv, H.; Wu, X.; Gu, N. The role of exogenous neural stem cells transplantation in cerebral ischemic stroke. J. Biomed. Nanotechnol. 2014, 10, 3219–3230. [Google Scholar] [CrossRef] [PubMed]
- Azizi, S.A.; Stokes, D.; Augelli, B.J.; DiGirolamo, C.; Prockop, D.J. Engraftment and migration of human bone marrow stromal cells implanted in the brains of albino rats--similarities to astrocyte grafts. Proc. Natl. Acad. Sci. USA 1998, 95, 3908–3913. [Google Scholar] [CrossRef] [Green Version]
- Hokari, M.; Kuroda, S.; Chiba, Y.; Maruichi, K.; Iwasaki, Y. Synergistic effects of granulocyte-colony stimulating factor on bone marrow stromal cell transplantation for mice cerebral infarct. Cytokine 2009, 46, 260–266. [Google Scholar] [CrossRef]
- Hokari, M.; Kuroda, S.; Shichinohe, H.; Yano, S.; Hida, K.; Iwasaki, Y. Bone marrow stromal cells protect and repair damaged neurons through multiple mechanisms. J. Neurosci. Res. 2008, 86, 1024–1035. [Google Scholar] [CrossRef]
- Kawabori, M.; Kuroda, S.; Ito, M.; Shichinohe, H.; Houkin, K.; Kuge, Y.; Tamaki, N. Timing and cell dose determine therapeutic effects of bone marrow stromal cell transplantation in rat model of cerebral infarct. Neuropathology 2013, 33, 140–148. [Google Scholar] [CrossRef]
- Kawabori, M.; Kuroda, S.; Sugiyama, T.; Ito, M.; Shichinohe, H.; Houkin, K.; Kuge, Y.; Tamaki, N. Intracerebral, but not intravenous, transplantation of bone marrow stromal cells enhances functional recovery in rat cerebral infarct: An optical imaging study. Neuropathology 2012, 32, 217–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shichinohe, H.; Kuroda, S.; Yano, S.; Hida, K.; Iwasaki, Y. Role of SDF-1/CXCR4 system in survival and migration of bone marrow stromal cells after transplantation into mice cerebral infarct. Brain Res. 2007, 1183, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, M.; Kuroda, S.; Zhao, S.; Magota, K.; Shichinohe, H.; Houkin, K.; Kuge, Y.; Tamaki, N. Bone marrow stromal cell transplantation enhances recovery of local glucose metabolism after cerebral infarction in rats: A serial 18F-FDG PET study. J. Nucl. Med. 2013, 54, 145–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shichinohe, H.; Ishihara, T.; Takahashi, K.; Tanaka, Y.; Miyamoto, M.; Yamauchi, T.; Saito, H.; Takemoto, H.; Houkin, K.; Kuroda, S. Bone marrow stromal cells rescue ischemic brain by trophic effects and phenotypic change toward neural cells. Neurorehabil. Neural Repair. 2015, 29, 80–89. [Google Scholar] [CrossRef]
- Chen, J.; Li, Y.; Katakowski, M.; Chen, X.; Wang, L.; Lu, D.; Lu, M.; Gautam, S.C.; Chopp, M. Intravenous bone marrow stromal cell therapy reduces apoptosis and promotes endogenous cell proliferation after stroke in female rat. J. Neurosci. Res. 2003, 73, 778–786. [Google Scholar] [CrossRef]
- Ito, M.; Kuroda, S.; Sugiyama, T.; Maruichi, K.; Kawabori, M.; Nakayama, N.; Houkin, K.; Iwasaki, Y. Transplanted bone marrow stromal cells protect neurovascular units and ameliorate brain damage in stroke-prone spontaneously hypertensive rats. Neuropathology 2012, 32, 522–533. [Google Scholar] [CrossRef]
- Wang, Z.; He, D.; Zeng, Y.Y.; Zhu, L.; Yang, C.; Lu, Y.J.; Huang, J.Q.; Cheng, X.Y.; Huang, X.H.; Tan, X.J. The spleen may be an important target of stem cell therapy for stroke. J. Neuroinflamm. 2019, 16, 20. [Google Scholar] [CrossRef]
- Tan, C.; Zhao, S.; Higashikawa, K.; Wang, Z.; Kawabori, M.; Abumiya, T.; Nakayama, N.; Kazumata, K.; Ukon, N.; Yasui, H.; et al. [(18)F]DPA-714 PET imaging shows immunomodulatory effect of intravenous administration of bone marrow stromal cells after transient focal ischemia. EJNMMI Res. 2018, 8, 35. [Google Scholar] [CrossRef]
- Phinney, D.G.; Pittenger, M.F. Concise Review: MSC-Derived Exosomes for Cell-Free Therapy. Stem Cells 2017, 35, 851–858. [Google Scholar] [CrossRef] [Green Version]
- Doeppner, T.R.; Herz, J.; Gorgens, A.; Schlechter, J.; Ludwig, A.K.; Radtke, S.; de Miroschedji, K.; Horn, P.A.; Giebel, B.; Hermann, D.M. Extracellular Vesicles Improve Post-Stroke Neuroregeneration and Prevent Postischemic Immunosuppression. Stem Cells Transl. Med. 2015, 4, 1131–1143. [Google Scholar] [CrossRef] [Green Version]
- Xia, Y.; Ling, X.; Hu, G.; Zhu, Q.; Zhang, J.; Li, Q.; Zhao, B.; Wang, Y.; Deng, Z. Small extracellular vesicles secreted by human iPSC-derived MSC enhance angiogenesis through inhibiting STAT3-dependent autophagy in ischemic stroke. Stem Cell Res. Ther. 2020, 11, 313. [Google Scholar] [CrossRef] [PubMed]
- Osanai, T.; Houkin, K.; Uchiyama, S.; Minematsu, K.; Taguchi, A.; Terasaka, S. Treatment evaluation of acute stroke for using in regenerative cell elements (TREASURE) trial: Rationale and design. Int. J. Stroke 2018, 13, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Stroncek, D.F.; Jin, P.; McKenna, D.H.; Takanashi, M.; Fontaine, M.J.; Pati, S.; Schafer, R.; Peterson, E.; Benedetti, E.; Reems, J.A. Human Mesenchymal Stromal Cell (MSC) Characteristics Vary Among Laboratories When Manufactured From the Same Source Material: A Report by the Cellular Therapy Team of the Biomedical Excellence for Safer Transfusion (BEST) Collaborative. Front. Cell Dev. Biol. 2020, 8, 458. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Fernandez, M.; Rodriguez-Frutos, B.; Ramos-Cejudo, J.; Teresa Vallejo-Cremades, M.; Fuentes, B.; Cerdan, S.; Diez-Tejedor, E. Effects of intravenous administration of allogenic bone marrow- and adipose tissue-derived mesenchymal stem cells on functional recovery and brain repair markers in experimental ischemic stroke. Stem Cell Res. Ther. 2013, 4, 11. [Google Scholar] [CrossRef] [Green Version]
- Shichinohe, H.; Kuroda, S.; Maruichi, K.; Osanai, T.; Sugiyama, T.; Chiba, Y.; Yamaguchi, A.; Iwasaki, Y. Bone marrow stromal cells and bone marrow-derived mononuclear cells: Which are suitable as cell source of transplantation for mice infarct brain? Neuropathology 2010, 30, 113–122. [Google Scholar] [CrossRef]
- Kolvenbach, R.; Kreissig, C.; Ludwig, E.; Cagiannos, C. Stem cell use in critical limb ischemia. J. Cardiovasc. Surg. 2007, 48, 39–44. [Google Scholar]
- Strauer, B.E.; Brehm, M.; Zeus, T.; Kostering, M.; Hernandez, A.; Sorg, R.V.; Kogler, G.; Wernet, P. Repair of infarcted myocardium by autologous intracoronary mononuclear bone marrow cell transplantation in humans. Circulation 2002, 106, 1913–1918. [Google Scholar] [CrossRef] [Green Version]
- Tateishi-Yuyama, E.; Matsubara, H.; Murohara, T.; Ikeda, U.; Shintani, S.; Masaki, H.; Amano, K.; Kishimoto, Y.; Yoshimoto, K.; Akashi, H.; et al. Therapeutic angiogenesis for patients with limb ischaemia by autologous transplantation of bone-marrow cells: A pilot study and a randomised controlled trial. Lancet 2002, 360, 427–435. [Google Scholar] [CrossRef]
- Uemura, M.; Kasahara, Y.; Nagatsuka, K.; Taguchi, A. Cell-based therapy to promote angiogenesis in the brain following ischemic damage. Curr. Vasc. Pharmacol. 2012, 10, 285–288. [Google Scholar] [CrossRef]
- Inoue, T.; Croce, K.; Morooka, T.; Sakuma, M.; Node, K.; Simon, D.I. Vascular inflammation and repair: Implications for re-endothelialization, restenosis, and stent thrombosis. JACC Cardiovasc. Interv. 2011, 4, 1057–1066. [Google Scholar] [CrossRef] [Green Version]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, E.M.; Le Blanc, K.; Dominici, M.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.C.; Deans, R.J.; Krause, D.S.; Keating, A.; International Society for Cellular, T. Clarification of the nomenclature for MSC: The International Society for Cellular Therapy position statement. Cytotherapy 2005, 7, 393–395. [Google Scholar] [CrossRef] [PubMed]
- Bellagamba, B.C.; Grudzinski, P.B.; Ely, P.B.; Nader, P.J.H.; Nardi, N.B.; da Silva Meirelles, L. Induction of Expression of CD271 and CD34 in Mesenchymal Stromal Cells Cultured as Spheroids. Stem Cells Int. 2018, 2018, 7357213. [Google Scholar] [CrossRef] [PubMed]
- Romieu-Mourez, R.; Francois, M.; Boivin, M.N.; Stagg, J.; Galipeau, J. Regulation of MHC class II expression and antigen processing in murine and human mesenchymal stromal cells by IFN-gamma, TGF-beta, and cell density. J. Immunol. 2007, 179, 1549–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stagg, J.; Pommey, S.; Eliopoulos, N.; Galipeau, J. Interferon-gamma-stimulated marrow stromal cells: A new type of nonhematopoietic antigen-presenting cell. Blood 2006, 107, 2570–2577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viswanathan, S.; Shi, Y.; Galipeau, J.; Krampera, M.; Leblanc, K.; Martin, I.; Nolta, J.; Phinney, D.G.; Sensebe, L. Mesenchymal stem versus stromal cells: International Society for Cell & Gene Therapy (ISCT(R)) Mesenchymal Stromal Cell committee position statement on nomenclature. Cytotherapy 2019, 21, 1019–1024. [Google Scholar] [CrossRef]
- Kopen, G.C.; Prockop, D.J.; Phinney, D.G. Marrow stromal cells migrate throughout forebrain and cerebellum, and they differentiate into astrocytes after injection into neonatal mouse brains. Proc. Natl. Acad. Sci. USA 1999, 96, 10711–10716. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Ramos, J.; Song, S.; Cardozo-Pelaez, F.; Hazzi, C.; Stedeford, T.; Willing, A.; Freeman, T.B.; Saporta, S.; Janssen, W.; Patel, N.; et al. Adult bone marrow stromal cells differentiate into neural cells in vitro. Exp. Neurol. 2000, 164, 247–256. [Google Scholar] [CrossRef] [Green Version]
- Porada, C.D.; Zanjani, E.D.; Almeida-Porad, G. Adult mesenchymal stem cells: A pluripotent population with multiple applications. Curr. Stem Cell Res. Ther. 2006, 1, 365–369. [Google Scholar] [CrossRef]
- Tate, C.C.; Fonck, C.; McGrogan, M.; Case, C.C. Human mesenchymal stromal cells and their derivative, SB623 cells, rescue neural cells via trophic support following in vitro ischemia. Cell Transplant. 2010, 19, 973–984. [Google Scholar] [CrossRef] [Green Version]
- Labusch, M.; Mancini, L.; Morizet, D.; Bally-Cuif, L. Conserved and Divergent Features of Adult Neurogenesis in Zebrafish. Front. Cell Dev. Biol. 2020, 8, 525. [Google Scholar] [CrossRef] [PubMed]
- Ottoboni, L.; von Wunster, B.; Martino, G. Therapeutic Plasticity of Neural Stem Cells. Front. Neurol. 2020, 11, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleppner, S.R.; Robinson, K.A.; Trojanowski, J.Q.; Lee, V.M. Transplanted human neurons derived from a teratocarcinoma cell line (NTera-2) mature, integrate, and survive for over 1 year in the nude mouse brain. J. Comp. Neurol. 1995, 357, 618–632. [Google Scholar] [CrossRef] [PubMed]
- Trojanowski, J.Q.; Mantione, J.R.; Lee, J.H.; Seid, D.P.; You, T.; Inge, L.J.; Lee, V.M. Neurons derived from a human teratocarcinoma cell line establish molecular and structural polarity following transplantation into the rodent brain. Exp. Neurol. 1993, 122, 283–294. [Google Scholar] [CrossRef] [PubMed]
- Shichinohe, H.; Yamauchi, T.; Saito, H.; Houkin, K.; Kuroda, S. Bone marrow stromal cell transplantation enhances recovery of motor function after lacunar stroke in rats. Acta Neurobiol. Exp. 2013, 73, 354–363. [Google Scholar]
- Chiu, S.C.; Hung, H.S.; Lin, S.Z.; Chiang, E.; Liu, D.D. Therapeutic potential of olfactory ensheathing cells in neurodegenerative diseases. J. Mol. Med. 2009, 87, 1179–1189. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Kang, Y.; Hu, Q.; Chen, C.; Yang, L.; Wang, K.; Chen, L.; Huang, H.; Zhou, C. A long-term observation of olfactory ensheathing cells transplantation to repair white matter and functional recovery in a focal ischemia model in rat. Brain Res. 2010, 1317, 257–267. [Google Scholar] [CrossRef]
- Li, L.; Adnan, H.; Xu, B.; Wang, J.; Wang, C.; Li, F.; Tang, K. Effects of transplantation of olfactory ensheathing cells in chronic spinal cord injury: A systematic review and meta-analysis. Eur. Spine J. 2015, 24, 919–930. [Google Scholar] [CrossRef]
- Lima, C.; Escada, P.; Pratas-Vital, J.; Branco, C.; Arcangeli, C.A.; Lazzeri, G.; Maia, C.A.; Capucho, C.; Hasse-Ferreira, A.; Peduzzi, J.D. Olfactory mucosal autografts and rehabilitation for chronic traumatic spinal cord injury. Neurorehabil. Neural Repair. 2010, 24, 10–22. [Google Scholar] [CrossRef]
- Lima, C.; Pratas-Vital, J.; Escada, P.; Hasse-Ferreira, A.; Capucho, C.; Peduzzi, J.D. Olfactory mucosa autografts in human spinal cord injury: A pilot clinical study. J. Spinal Cord Med. 2006, 29, 191–203. [Google Scholar] [CrossRef] [Green Version]
- Mackay-Sim, A.; Feron, F.; Cochrane, J.; Bassingthwaighte, L.; Bayliss, C.; Davies, W.; Fronek, P.; Gray, C.; Kerr, G.; Licina, P.; et al. Autologous olfactory ensheathing cell transplantation in human paraplegia: A 3-year clinical trial. Brain 2008, 131, 2376–2386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marei, H.E.; Hasan, A.; Rizzi, R.; Althani, A.; Afifi, N.; Cenciarelli, C.; Caceci, T.; Shuaib, A. Potential of Stem Cell-Based Therapy for Ischemic Stroke. Front. Neurol. 2018, 9, 34. [Google Scholar] [CrossRef] [PubMed]
- Rikhtegar, R.; Yousefi, M.; Dolati, S.; Kasmaei, H.D.; Charsouei, S.; Nouri, M.; Shakouri, S.K. Stem cell-based cell therapy for neuroprotection in stroke: A review. J. Cell. Biochem. 2019, 120, 8849–8862. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Wei, Z.Z.; Jiang, M.Q.; Mohamad, O.; Yu, S.P. Stem cell transplantation therapy for multifaceted therapeutic benefits after stroke. Prog. Neurobiol. 2017, 157, 49–78. [Google Scholar] [CrossRef] [PubMed]
- Kawabori, M.; Tanimori, A.; Kitta, S.; Shichinohe, H.; Houkin, K. Evaluation of Novel Stereotactic Cannula for Stem Cell Transplantation against Central Nervous System Disease. Stem Cells Int. 2020, 2020, 4085617. [Google Scholar] [CrossRef] [Green Version]
- Shichinohe, H.; Kawabori, M.; Iijima, H.; Teramoto, T.; Abumiya, T.; Nakayama, N.; Kazumata, K.; Terasaka, S.; Arato, T.; Houkin, K. Research on advanced intervention using novel bone marrOW stem cell (RAINBOW): A study protocol for a phase I, open-label, uncontrolled, dose-response trial of autologous bone marrow stromal cell transplantation in patients with acute ischemic stroke. BMC Neurol. 2017, 17, 179. [Google Scholar] [CrossRef]
Figure 1.
Unsolved issues regarding stem cell treatment for ischemic stroke. The most effective and safest method of stem cell therapy has not been established. The challenges include the choice of cell, cell dose, transplantation routes, and patient type. ES cell: embryonic stem cell, iPS: induced pluripotent stem cell.
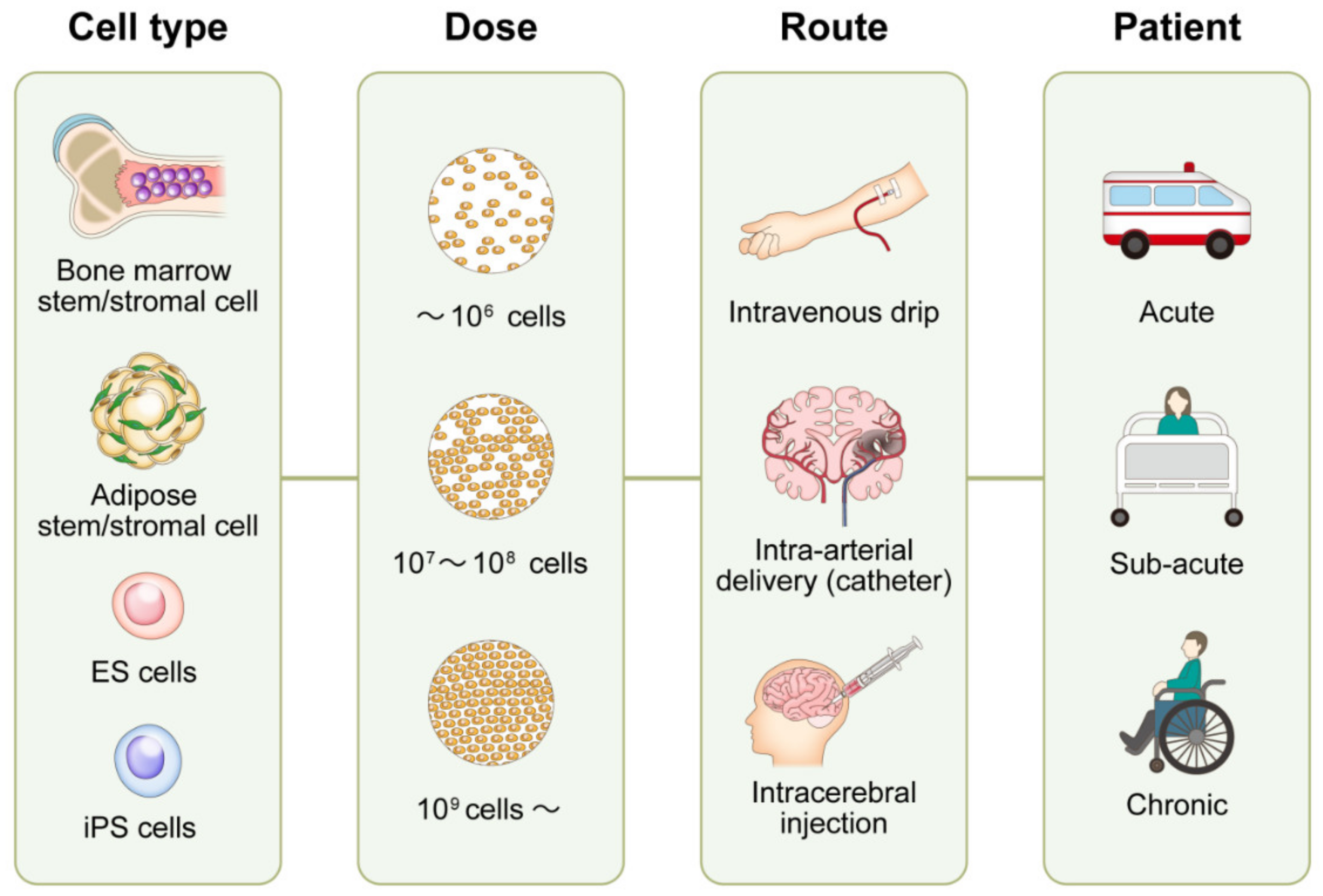
Figure 1.
Unsolved issues regarding stem cell treatment for ischemic stroke. The most effective and safest method of stem cell therapy has not been established. The challenges include the choice of cell, cell dose, transplantation routes, and patient type. ES cell: embryonic stem cell, iPS: induced pluripotent stem cell.
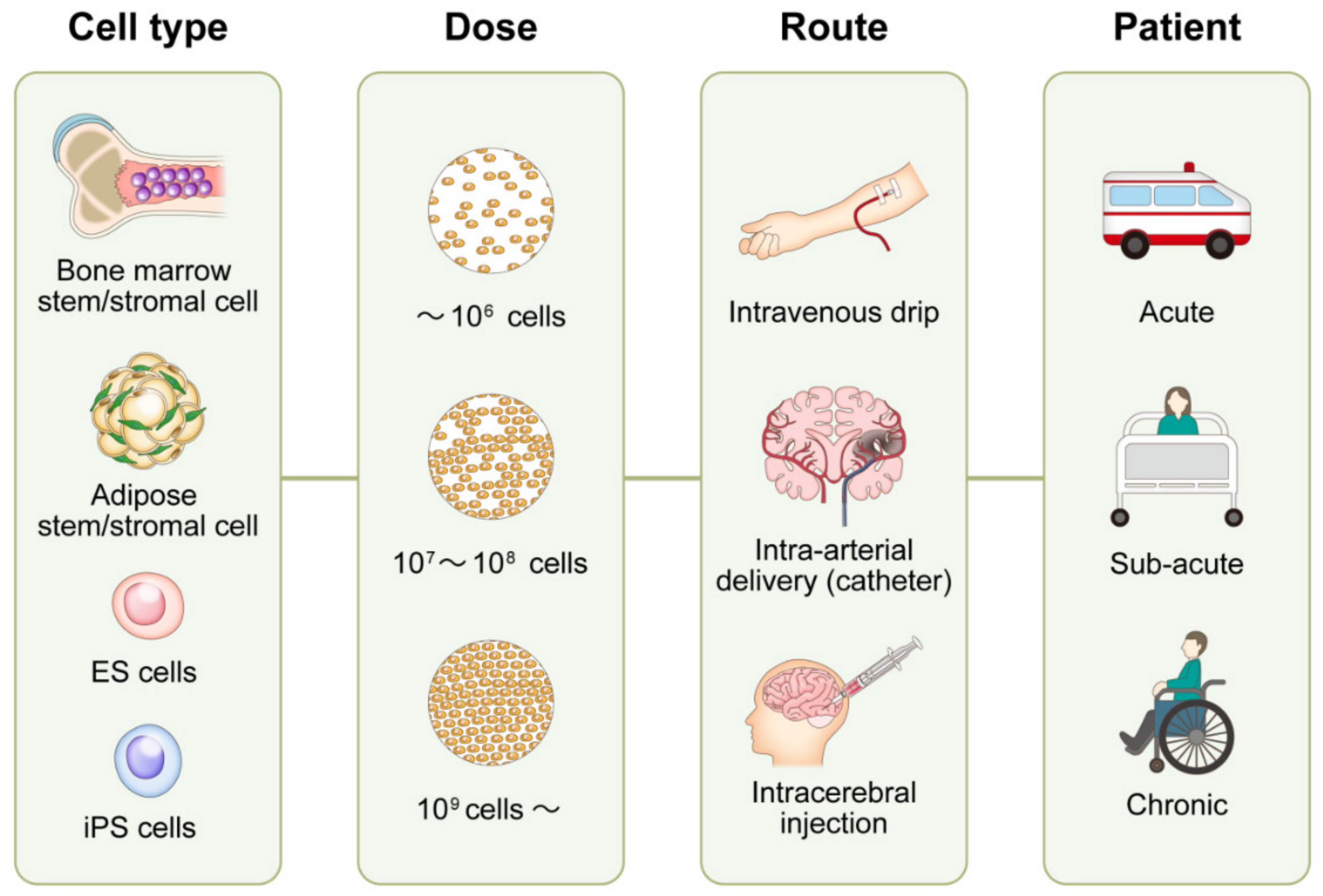
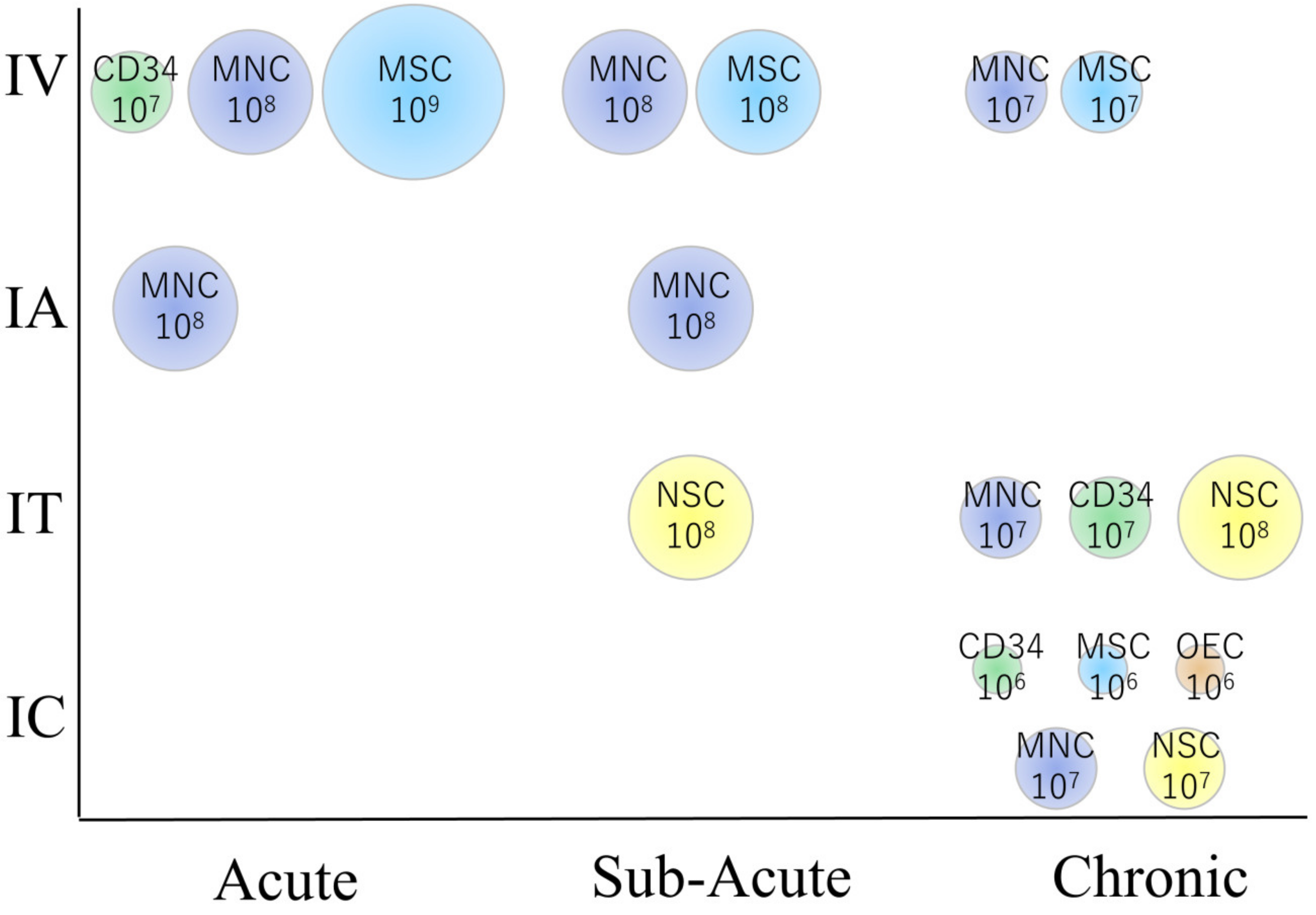
Figure 2.
The relationship between cell types, dose, and patient characteristics in clinical trials. Note that intravenous transplantation is preferred in the acute phase, while intracerebral transplantation is preferred in the chronic phase. MNC: CD34: CD34 positive hematopoietic stem cells derived from mononuclear cells, MSC: Mesenchymal stem/stromal cell, NSC: Neural stem/progenitor cell, OEC: Olfactory ensheathing cell. The number represents the approximate amount of cells transplanted per patient (cells/body).
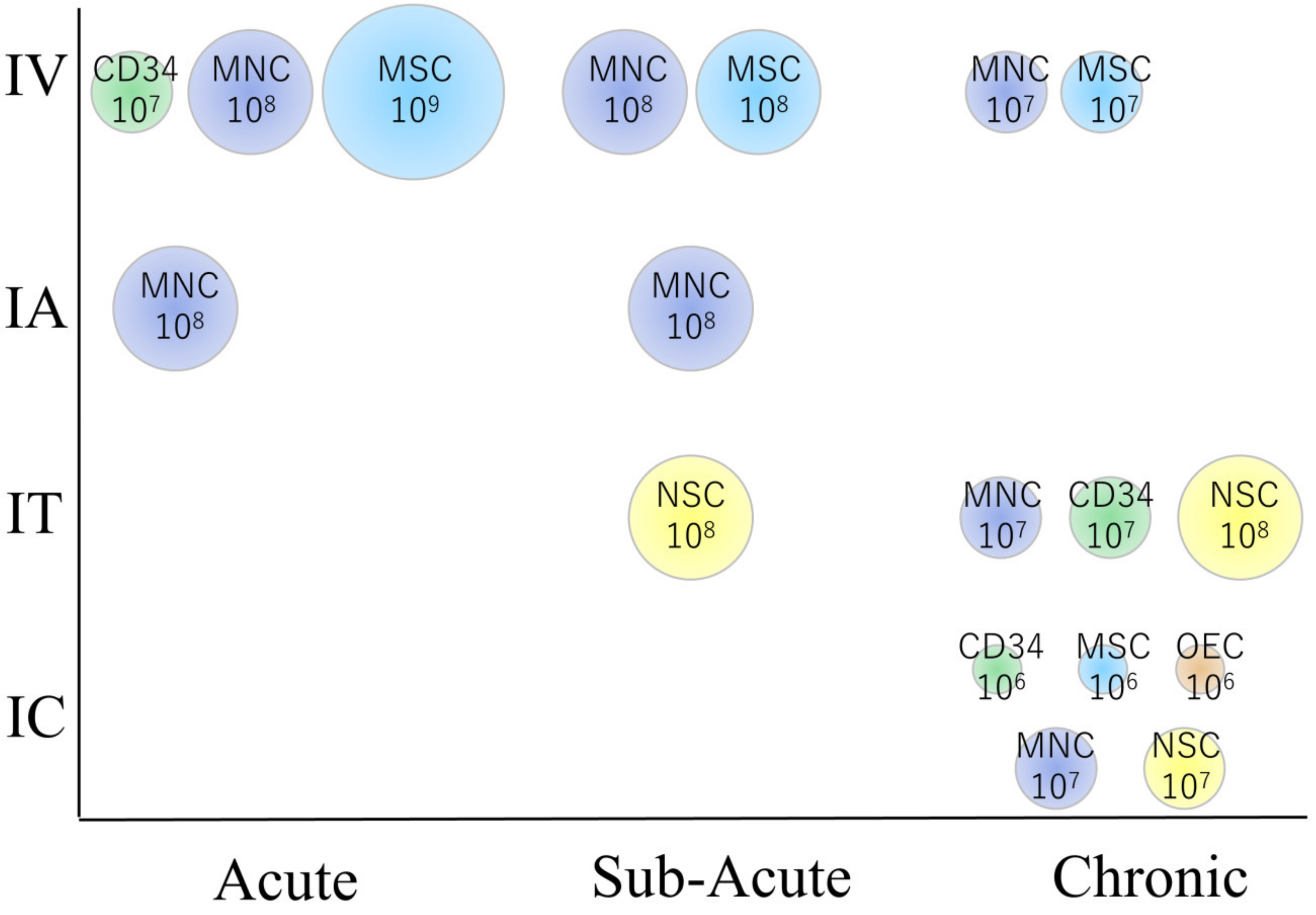
Figure 2.
The relationship between cell types, dose, and patient characteristics in clinical trials. Note that intravenous transplantation is preferred in the acute phase, while intracerebral transplantation is preferred in the chronic phase. MNC: CD34: CD34 positive hematopoietic stem cells derived from mononuclear cells, MSC: Mesenchymal stem/stromal cell, NSC: Neural stem/progenitor cell, OEC: Olfactory ensheathing cell. The number represents the approximate amount of cells transplanted per patient (cells/body).

{kind=link}
{kind=link}
Table 1.
Published clinical trials using stem cells for ischemic stroke.
| Reference Number | Country | Cell Type | Cell Source | Dose | Route | Transplant Timing | Treated Patient Number (Control) | Assessment Modality | Major Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Acute | |||||||||
| [16] | USA | Autologous | BMMNC | 4–6 × 108 | IV | 1–3 D | 10 | BI, mRS, NIHSS | showed good neurological recovery |
| [25] | USA | Allogeneic | BMSC | 1.2 × 109 | IV | 1–2 D | 65 (58) | mRS, NIHSS, BI | No difference for neurological recovery (primary endpoint), but earlier timing (24-36 h) may be beneficial |
| [35] | USA | Allogeneic | UCBC | 1.2 × 106 (CD34+) | IV | 3–9 D | 10 | mRS, NIHSS | Safe |
| [10] | Brazil | Autologous | BMMNC | 5–60 × 107 | IA | 3–10 D | 20 | mRS, NIHSS | 30% of the patients showed satisfactory clinical outcome |
| [12] | Spain | Autologous | BMMNC | 1.6 × 108 | IA | 5–9 D | 10(10) | mRS, BI, NIHSS | No difference in neurological function |
| [9] | Brazil | Autologous | BMMNC | 3 × 107 | IA | 9 D | 1 | SPECT | Brain/liver/spleen uptake at 8 h |
| [32] | UK | Autologous | CD34+ (BM) | 1–3 × 106 | IA | 1 W | 5 | mRS, NIHSS | Good recovery was observed |
| [36] | China | Allogeneic | UCBC & NPC | 3 × 107 (UC: IV), 1.5 × 107 (UC: IT), 1.8 × 107 (NPC: IT) | IV &IT | 1 W | 1 | NIHSS, BI, mRS | Showed some degree of neurological recovery |
| Sub-Acute | |||||||||
| [13] | India | Autologous | BMMNC | 2–19 × 108 | IV | 2–4 W | 11 | NIHSS, BI, mRS, PET | Favorable outcomes were mostly found in early treatment group |
| [5] | India | Autologous | BMMNC | 5 × 107 | IV | 3–4 M | 1(3) | FM, mBI | Safe |
| [15] | Brazil | Autologous | BMMNC | 2–5 × 108 | IV | 1–3 M | 5 | NIHSS | Cells in brain were scarce (1%), IV (21%) showed high cell distribution in lung compared with IV (7%) |
| [14] | India | Autologous | BMMNC | 2.8 × 10e7 | IV | 18 D | 59(59) | BI, mRS, NIHSS, PET | No significant recovery compared with control |
| [20] | Japan | Autologous | BMMNC | 2.5–3.4 × 108 | IV | 7–10 D | 12 | mRS, NIHSS, SPECT, PET | Better NIHSS (but not mRS, BI) recovery compared with historical control |
| [22] | Korea | Autologous | BMSC | 1 × 108 | IV | 1–2 M | 5 (25) | BI, mRS, NIHSS | Cell treatment group showed better neurological recovery than control |
| [28] | Korea | Autologous | BMSC | 1 × 108 | IV | 2 M | 16(36) | mRS, Survival | Better recovery, less mortality for 5 years |
| [26] | Japan | Autologous | BMSC | 0.8–1.5 × 108 | IV | 1–4 M | 12 | NIHSS | Recoveries were mainly seen 0–1 W from transplantation |
| [24] | China | Autologous | BMSC | 3 × 108 | IV | 1 M | 12 (6) | mRS, NIHSS, BI | No neurological difference compared with control |
| [27] | France | Autologous | BMSC | 1 or 3 × 108 | IV | 1–2 M | 16(15) | NIHSS, mRS, BI | No overall change, but motor functional evaluations indicated improvement |
| [36] | China | Allogeneic | UCBC & NPC | 1.2 × 108 (UC) | IV | 2 & 3 M | 2 | NIHSS, BI, mRS | Showed some degree of neurological recovery |
| [2] | Brazil | Autologous | BMMNC | 1–5 × 108 | IA | 2–3 M | 6 | SPECT | Cells were found in the brain after 2 h, but not after 24 h |
| [3] | Brazil | Autologous | BMMNC | 1–5 × 108 | IA | 2–3 M | 6 | NIHSS, SPECT | Safe, but cells could not be seen 24 h after injection in 4 out of 6 patients |
| [15] | Brazil | Autologous | BMMNC | 1-5 x 108 | IA | 1–3 M | 7 | NIHSS | Cells in brain were scarce (1%), IA (41%) showed high cell distribution in liver compared with IV (13%) |
| [11] | Egypt | Autologous | BMMNC | 1 × 106 | IA | 2–4 W | 21(18) | NIHSS, mRS, BI, | IA treatment did not improve neurological recovery compare with control |
| [8] | India | Autologous | BMMNC | 5 × 108 | IA | 1–2 W | 10 (10) | BI, NIHSS, mRS | Good recovery was observed in treatment group (P = 0.06) |
| [17] | USA | Autologous | BMMNC (ALD) | 3 × 106 | IA | 2–3 W | 29 (17) | mRS, NIHSS, BI | No statistical difference compared to control |
| [34] | China | Allogeneic | UCBC & NPC | 2 × 107 | IA | 11–22 D | 3 | mRS | Showed neurological recovery in 2 out of 3 patients |
| [42] | Russia | Allogeneic | Fetus neuronal cell | 2 × 108 | IT | 4 M | 1 | Karnovskii score | Cell treatment showed 33% increase in Score |
| [36] | China | Allogeneic | UCBC & NPC | 3 × 107 (UC: IV), 1.5 × 107 (UC: IT), 1.8 × 107 (NPC: IT) | IV & IT | 2 W | 1 | NIHSS, BI, mRS | Showed some degree of neurological recovery |
| Chronic | |||||||||
| India | Autologous | BMMNC | 6–7 × 107 | IV | 5–14 M | 20(20) | FM, mBI, Ashworth | No difference compared with control | |
| [21] | India | Autologous | BMMNC | 5 × 107 | IV | 6–15 M | 11(9) | FM, mBI | Significant improvement in mBI, but not in FM |
| [4,5] | India | Autologous | BMSC | 5–6 × 107 | IV | 8–12 M | 6(6) | BI, FM, Ashworth | No significant difference compared with control up to 4 years |
| [29] | USA | Allogeneic | BMSC (hypoxia treated) | 1 × 108 | IV | 7 M-25 Y | 36 | NIHSS, BI | Significant recovery was observed compared with baseline |
| [7] | India | Autologous | BMSC/BMMNC | 5-6 × 107 | IV | 3 M-2 Y | 20(20) | FM, mBI | mBI showed significant improvement |
| [18] | India | Autologous | BMMNC | 6 × 107 | IT | 4 M-12 Y | 14 | FIM | Showed recovery, but this study included hemorrhagic stroke |
| [37] | China | Autologous | CD34+ (peripheral) | 1–3 × 107 | IT | 1–7 Y | 8 | NIHSS, BI | Patients showed recovery, but this may have been due to natural history |
| [42] | Russia | Allogeneic | Fetus neuronal cell | 2 × 108 | IT | 8 M-1.5 Y | 6 (6) | Karnovskii score | Cell treatment groups showed better recovery |
| [23] | USA | Autologous | ADSC (no culture) | N.D. | IT (ICV) | 1 Y | 1 | N.D. | Stable |
| [19] | Cuba | Autologous | BMMNC | 1–5 × 107 | IC | 3–5 Y | 3 | BI, NIHSS, SSS | Recovery compared with pre-operation was found |
| [33] | Taiwan | Autologous | CD34+ (peripheral) | 3–8 × 106 | IC | 6 M-5 Y | 15(15) | NIHSS, ESS, mRS | Statistically significant recovery |
| [30,31] | USA | Allogeneic | BMSC (Gene modified) | 2.5, 5, 10 × 106 | IC | 7–36 M | 18 | ESS, NIHSS, FM | Neurological recovery (ESS, NIHSS, F-M test) was observed up to 2 years |
| [41] | USA | Allogeneic | Fetus neuronal cell | 2 × 106 (n = 8) or 6 × 106 (n = 4) | IC | 7 M-5 Y | 12 | BI, ESS, NIHSS | 6 x 106 showed better recovery than 2 x 106 |
| [39] | UK | Allogeneic | Fetus neuronal cell | 2, 5, 10, 20 × 106 | IC | 1–4 Y | 11 | NIHSS, BI, Ashworth | Neurological recovery (median NIHSS of 2) was observed |
| [43] | UK | Allogeneic | Fetus neuronal cell | 2 × 107 | IC | 2M-1 Y | 23 | ARAT | Upper limb function recovered from baseline |
| [40] | USA | Allogeneic | Fetus neuronal cell | 5, 10 × 106 | IC | 1–6 Y | 18(4) | ESS, NIHSS, FM, ARAT | No difference for neurological recovery (primary endpoint), but showed partial recovery in some tests |
| [38] | China | Allogeneic | OEC | 1 × 106 | IC | 3 Y | 1 | BI | Recovery in speech and gait |
| [38] | China | Allogeneic | OEC & NPC | 1 × 106 & 2 × 106 | IC | 5 Y | 1 | BI | Recovery in motor function |
| [44] | USA | Xenogeneic | Fetal Porcine cell | 2 × 107 | IC | 1.5–10 Y | 5 | BI, RS, NIHSS | Slight recovery, but 2 patients exhibited adverse events (seizure and motor deficit) |
| [38] | China | Allogeneic | OEC & NPC | 1 × 106 & 2 × 106 | IC & IT (NPC) | 1–20 Y | 4 | BI | Recovery in gait |
| [36] | China | Allogeneic | UCBC & NPC | 3 × 107 (UC: IV), 1.5 × 107 (UC: IT), 1.8 × 107 (NPC: IT) | IV & IT | 10 M & 2 Y | 2 | NIHSS, BI, mRS | Showed some degree of neurological recovery |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kawabori, M.; Shichinohe, H.; Kuroda, S.; Houkin, K. Clinical Trials of Stem Cell Therapy for Cerebral Ischemic Stroke. Int. J. Mol. Sci. 2020, 21, 7380. https://doi.org/10.3390/ijms21197380
AMA Style
Kawabori M, Shichinohe H, Kuroda S, Houkin K. Clinical Trials of Stem Cell Therapy for Cerebral Ischemic Stroke. International Journal of Molecular Sciences. 2020; 21(19):7380. https://doi.org/10.3390/ijms21197380
Chicago/Turabian StyleKawabori, Masahito, Hideo Shichinohe, Satoshi Kuroda, and Kiyohiro Houkin. 2020. "Clinical Trials of Stem Cell Therapy for Cerebral Ischemic Stroke" International Journal of Molecular Sciences 21, no. 19: 7380. https://doi.org/10.3390/ijms21197380
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.