Lower Serum n-3 Fatty Acid Level in Older Adults with Sarcopenia

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Sarcopenia Assessment
2.3. Measurement of Serum Levels of n-3 and n-6 FAs
2.4. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Direct. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2018, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, G.; Kim, J.H. Impact of Skeletal Muscle Mass on Metabolic Health. Endocrinol. Metab. 2020, 35, 1–6. [Google Scholar] [CrossRef]
- Kim, S.H.; Shin, M.J.; Shin, Y.B.; Kim, K.U. Sarcopenia Associated with Chronic Obstructive Pulmonary Disease. J. Bone Metab. 2019, 26, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Hirani, V.; Blyth, F.; Naganathan, V.; Le Couteur, D.G.; Seibel, M.J.; Waite, L.M.; Handelsman, D.J.; Cumming, R.G. Sarcopenia Is Associated With Incident Disability, Institutionalization, and Mortality in Community-Dwelling Older Men: The Concord Health and Ageing in Men Project. J. Am. Med. Direct. Assoc. 2015, 16, 607–613. [Google Scholar] [CrossRef]
- Jang, I.-Y.; Lee, E.; Lee, H.; Park, H.; Kim, S.; Kim, K.-I.; Jung, H.-W.; Kim, D.H. Characteristics of sarcopenia by European consensuses and a phenotype score. J. Cachexia Sarcopenia Muscle 2020, 11, 497–504. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Arai, H.; Kritchevsky, S.B.; Guralnik, J.; Bauer, J.M.; Pahor, M.; Clark, B.C.; Cesari, M.; et al. International Clinical Practice Guidelines for Sarcopenia (ICFSR): Screening, Diagnosis and Management. J. Nutr. Health Aging 2018, 22, 1148–1161. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Direct. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [Green Version]
- Dupont, J.; Dedeyne, L.; Dalle, S.; Koppo, K.; Gielen, E. The role of omega-3 in the prevention and treatment of sarcopenia. Aging Clin. Exp. Res. 2019, 31, 825–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simopoulos, A.P. Essential fatty acids in health and chronic disease. Am. J. Clin. Nutr. 1999, 70, 560s–569s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorente-Cebrián, S.; Costa, A.G.; Navas-Carretero, S.; Zabala, M.; Martínez, J.A.; Moreno-Aliaga, M.J. Role of omega-3 fatty acids in obesity, metabolic syndrome, and cardiovascular diseases: A review of the evidence. J. Physiol. Biochem. 2013, 69, 633–651. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.J.; Yoo, H.J.; Park, S.J.; Kwak, M.K.; Lee, S.H.; Kim, S.J.; Hamrick, M.W.; Isales, C.M.; Ahn, S.H.; Koh, J.M. Association of blood n-3 fatty acid with bone mass and bone marrow TRAP-5b in the elderly with and without hip fracture. Osteoporos. Int. 2019, 30, 1071–1078. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Bonafè, M.; Valensin, S.; Olivieri, F.; De Luca, M.; Ottaviani, E.; De Benedictis, G. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann. N.Y. Acad. Sci. 2000, 908, 244–254. [Google Scholar] [CrossRef]
- Dalle, S.; Rossmeislova, L.; Koppo, K. The Role of Inflammation in Age-Related Sarcopenia. Front. Physiol. 2017, 8, 1045. [Google Scholar] [CrossRef] [Green Version]
- Oh, J.H.; Song, S.; Rhee, H.; Lee, S.H.; Kim, D.Y.; Choe, J.C.; Ahn, J.; Park, J.S.; Shin, M.J.; Jeon, Y.K.; et al. Normal Reference Plots for the Bioelectrical Impedance Vector in Healthy Korean Adults. J. Korean Med. Sci. 2019, 34, e198. [Google Scholar] [CrossRef]
- Jang, I.Y.; Jung, H.W.; Lee, C.K.; Yu, S.S.; Lee, Y.S.; Lee, E. Comparisons of predictive values of sarcopenia with different muscle mass indices in Korean rural older adults: A longitudinal analysis of the Aging Study of PyeongChang Rural Area. Clin. Int. Aging 2018, 13, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.W.; Roh, H.; Cho, Y.; Jeong, J.; Shin, Y.S.; Lim, J.Y.; Guralnik, J.M.; Park, J. Validation of a Multi-Sensor-Based Kiosk for Short Physical Performance Battery. J. Am. Geriatr. Soc. 2019, 67, 2605–2609. [Google Scholar] [CrossRef]
- Peel, N.M.; Kuys, S.S.; Klein, K. Gait speed as a measure in geriatric assessment in clinical settings: A systematic review. J. Gerontol. Ser. A 2013, 68, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.W.; Roh, H.C.; Kim, S.W.; Kim, S.; Kim, M.; Won, C.W. Cross-Comparisons of Gait Speeds by Automatic Sensors and a Stopwatch to Provide Converting Formula Between Measuring Modalities. Ann. Geriatr. Med. Res. 2019, 23, 71–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossato, L.T.; Schoenfeld, B.J.; de Oliveira, E.P. Is there sufficient evidence to supplement omega-3 fatty acids to increase muscle mass and strength in young and older adults? Clin. Nutr. 2020, 39, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.M.; Jameson, K.A.; Batelaan, S.F.; Martin, H.J.; Syddall, H.E.; Dennison, E.M.; Cooper, C.; Sayer, A.A. Diet and its relationship with grip strength in community-dwelling older men and women: The Hertfordshire cohort study. J. Am. Geriatr. Soc. 2008, 56, 84–90. [Google Scholar] [CrossRef]
- Smith, G.I.; Julliand, S.; Reeds, D.N.; Sinacore, D.R.; Klein, S.; Mittendorfer, B. Fish oil-derived n-3 PUFA therapy increases muscle mass and function in healthy older adults. Am. J. Clin. Nutr. 2015, 102, 115–122. [Google Scholar] [CrossRef] [Green Version]
- Rousseau, J.H.; Kleppinger, A.; Kenny, A.M. Self-reported dietary intake of omega-3 fatty acids and association with bone and lower extremity function. J. Am. Geriatr. Soc. 2009, 57, 1781–1788. [Google Scholar] [CrossRef]
- Boutry-Regard, C.; Gerard, V.P.; Denis, B.; Toshio, M. Supplementation with Whey Protein, Omega-3 Fatty Acids and Polyphenols Combined with Electrical Muscle Stimulation Increases Muscle Strength in Elderly Adults with Limited Mobility: A Randomized Controlled Trial. Nutrients 2020, 12, 1866. [Google Scholar] [CrossRef]
- Huang, F.; Wei, H.; Luo, H.; Jiang, S.; Peng, J. EPA inhibits the inhibitor of κBα (IκBα)/NF-κB/muscle RING finger 1 pathway in C2C12 myotubes in a PPARγ-dependent manner. Br. J. Nutr. 2011, 105, 348–356. [Google Scholar] [CrossRef] [Green Version]
- Kamolrat, T.; Gray, S.R. The effect of eicosapentaenoic and docosahexaenoic acid on protein synthesis and breakdown in murine C2C12 myotubes. Biochem. Biophys. Res. Commun. 2013, 432, 593–598. [Google Scholar] [CrossRef]
- Logan, S.L.; Spriet, L.L. Omega-3 Fatty Acid Supplementation for 12 Weeks Increases Resting and Exercise Metabolic Rate in Healthy Community-Dwelling Older Females. PLoS ONE 2015, 10, e0144828. [Google Scholar] [CrossRef]
- Krzymińska-Siemaszko, R.; Czepulis, N.; Lewandowicz, M.; Zasadzka, E.; Suwalska, A.; Witowski, J.; Wieczorowska-Tobis, K. The Effect of a 12-Week Omega-3 Supplementation on Body Composition, Muscle Strength and Physical Performance in Elderly Individuals with Decreased Muscle Mass. Int. J. Environ. Res. Public Health 2015, 12, 10558–10574. [Google Scholar] [CrossRef] [Green Version]
- Cornish, S.M.; Chilibeck, P.D. Alpha-linolenic acid supplementation and resistance training in older adults. Appl. Physiol. Nutr. Metabol. 2009, 34, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P. Redefining dietary reference values and food safety. World Rev. Nutr. Dietet. 1998, 83, 219–222. [Google Scholar] [CrossRef]
- Sun, Q.; Ma, J.; Campos, H.; Hankinson, S.E.; Hu, F.B. Comparison between plasma and erythrocyte fatty acid content as biomarkers of fatty acid intake in US women. Am. J. Clin. Nutr. 2007, 86, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.; Charbonneau, L.; Ouellet, N.; Ouellet, H.; Blier, P.U.; Dufresne, F.; Fortin, S. Eicosapentaenoic acid monoglyceride resolves inflammation in an ex vivo model of human peripheral blood mononuclear cell. Eur. J. Pharmacol. 2017, 807, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Vedin, I.; Cederholm, T.; Freund Levi, Y.; Basun, H.; Garlind, A.; Faxén Irving, G.; Jönhagen, M.E.; Vessby, B.; Wahlund, L.O.; Palmblad, J. Effects of docosahexaenoic acid-rich n-3 fatty acid supplementation on cytokine release from blood mononuclear leukocytes: The OmegAD study. Am. J. Clin. Nutr. 2008, 87, 1616–1622. [Google Scholar] [CrossRef]
- Merritt, E.K.; Stec, M.J.; Thalacker-Mercer, A.; Windham, S.T.; Cross, J.M.; Shelley, D.P.; Craig Tuggle, S.; Kosek, D.J.; Kim, J.S.; Bamman, M.M. Heightened muscle inflammation susceptibility may impair regenerative capacity in aging humans. J. Appl. Physiol. (Bethesda, Md. 1985) 2013, 115, 937–948. [Google Scholar] [CrossRef]
- Wåhlin-Larsson, B.; Carnac, G.; Kadi, F. The influence of systemic inflammation on skeletal muscle in physically active elderly women. Age 2014, 36, 9718. [Google Scholar] [CrossRef] [Green Version]
- Tachtsis, B.; Camera, D.; Lacham-Kaplan, O. Potential Roles of n-3 PUFAs during Skeletal Muscle Growth and Regeneration. Nutrients 2018, 10, 309. [Google Scholar] [CrossRef] [Green Version]
- Briolay, A.; Jaafar, R.; Nemoz, G.; Bessueille, L. Myogenic differentiation and lipid-raft composition of L6 skeletal muscle cells are modulated by PUFAs. Biochim. Biophys. Acta (BBA)-Biomembr. 2013, 1828, 602–613. [Google Scholar] [CrossRef]
- Bhullar, A.S.; Putman, C.T.; Mazurak, V.C. Potential Role of Omega-3 Fatty Acids on the Myogenic Program of Satellite Cells. Nutr. Metab. Insights 2016, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGlory, C.; Galloway, S.D.; Hamilton, D.L.; McClintock, C.; Breen, L.; Dick, J.R.; Bell, J.G.; Tipton, K.D. Temporal changes in human skeletal muscle and blood lipid composition with fish oil supplementation. Prostaglandins Leukotrienes Essent. Fat. Acids 2014, 90, 199–206. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, S.C.; Perez, M.R.; Hammond, K.E.; Sheader, E.A.; Negretti, N. Direct and indirect modulation of rat cardiac sarcoplasmic reticulum function by n-3 polyunsaturated fatty acids. J. Physiol. 2002, 538, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Belury, M.A.; Cole, R.M.; Snoke, D.B.; Banh, T.; Angelotti, A. Linoleic acid, glycemic control and Type 2 diabetes. Prostaglandins Leukotrienes Essent. Fat. Acids 2018, 132, 30–33. [Google Scholar] [CrossRef]
- Shearer, G.C.; Walker, R.E. An overview of the biologic effects of omega-6 oxylipins in humans. Prostaglandins Leukotrienes Essent. Fat. Acids 2018, 137, 26–38. [Google Scholar] [CrossRef]
- Patterson, E.; Wall, R.; Fitzgerald, G.F.; Ross, R.P.; Stanton, C. Health implications of high dietary omega-6 polyunsaturated Fatty acids. J. Nutr. Metab. 2012, 2012, 539426. [Google Scholar] [CrossRef]
- Ahn, S.H.; Park, S.Y.; Baek, J.E.; Lee, S.Y.; Baek, W.Y.; Lee, S.Y.; Lee, Y.S.; Yoo, H.J.; Kim, H.; Lee, S.H.; et al. Free Fatty Acid Receptor 4 (GPR120) Stimulates Bone Formation and Suppresses Bone Resorption in the Presence of Elevated n-3 Fatty Acid Levels. Endocrinology 2016, 157, 2621–2635. [Google Scholar] [CrossRef] [Green Version]
- Cho, H.J.; Ahn, S.H.; Lee, Y.S.; Lee, S.H.; Im, D.S.; Kim, I.; Koh, J.M.; Kim, S.; Kim, B.J. Free Fatty Acid Receptor 4 Mediates the Beneficial Effects of n-3 Fatty Acids on Body Composition in Mice. Calcif. Tissue Int. 2017, 101, 654–662. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Sarcopenia (n = 21) | No Sarcopenia (n = 104) | P |
|---|---|---|---|
| Sex, n (%) | 0.216 | ||
| Female | 14 (66.7) | 54 (51.9) | |
| Male | 7 (33.3) | 50 (48.1) | |
| Age, years | 71.9 ± 4.7 | 68.6 ± 6.5 | 0.034 |
| Weight, kg | 58.6 ± 9.6 | 68.0 ± 10.1 | <0.001 |
| Height, cm | 156.0 ± 5.7 | 160.0 ± 9.3 | 0.011 |
| Body mass index, kg/m2 | 24.0 ± 3.3 | 26.5 ± 3.1 | 0.001 |
| ASM, kg | 13.4 ± 2.6 | 18.3 ± 4.7 | <0.001 |
| SMI, kg/m2 | 5.48 ± 0.78 | 7.03 ± 1.06 | <0.001 |
| Grip strength, kg | 21.9 ± 6.2 | 28.9 ± 9.3 | <0.001 |
| Gait speed, m/s | 0.87 ± 0.37 | 1.10 ± 0.37 | 0.012 |
| Chair stand, s | 15.9 ± 11.4 | 10.4 ± 6.4 | 0.047 |
| SPPB score (range, 0–12) | 9.2 ± 2.6 | 10.8 ± 1.7 | 0.001 |
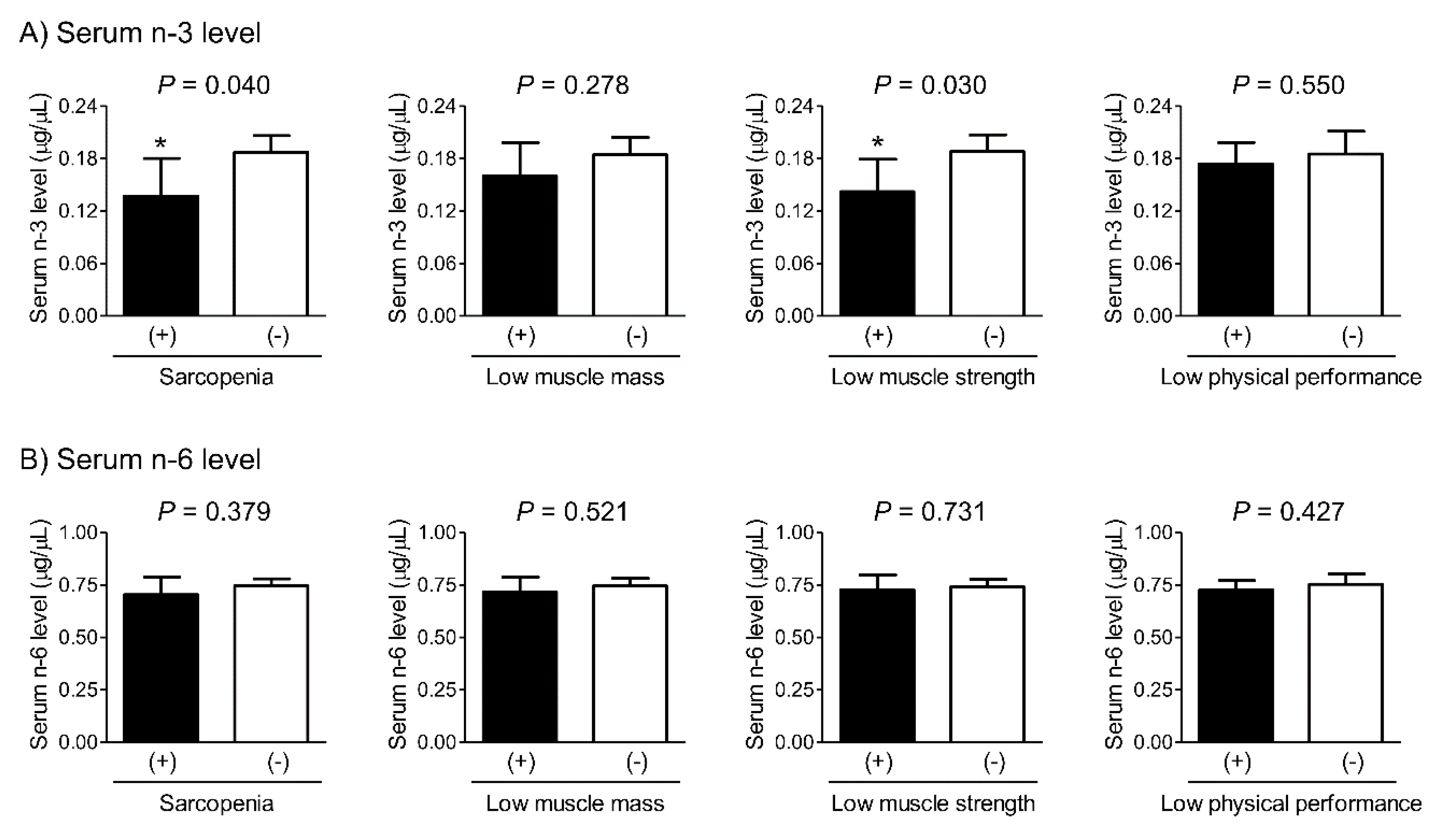
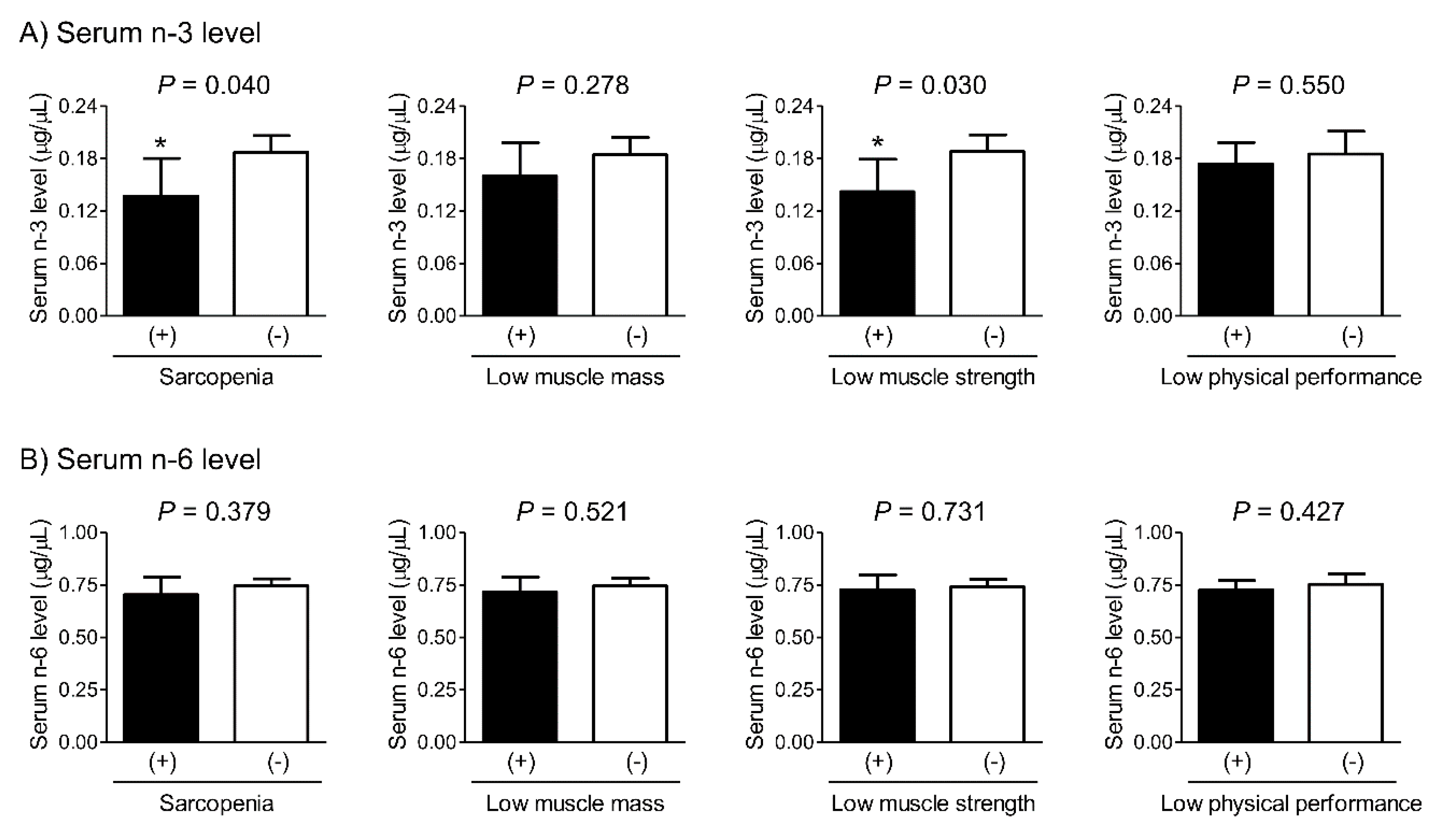
| OR (95% CIs) per SD Increment in Serum n-3 Level | P | OR (95% CIs) per SD Increment in Serum n-6 Level | P | |
|---|---|---|---|---|
| Sarcopenia | 0.29 (0.11–0.79) | 0.015 | 0.84 (0.49–1.45) | 0.537 |
| Low muscle mass | 0.68 (0.35–1.33) | 0.258 | 0.90 (0.55–1.45) | 0.649 |
| Low muscle strength | 0.40 (0.18–0.91) | 0.028 | 0.93 (0.58–1.49) | 0.749 |
| Low physical performance | 0.89 (0.61–1.30) | 0.545 | 0.85 (0.57–1.26) | 0.417 |
| Serum n-3 Level | Serum n-6 Level | |||||||
|---|---|---|---|---|---|---|---|---|
| β | SE | β | P | β | SE | β | P | |
| SMI | 1.153 | 0.761 | 0.096 | 0.132 | 0.068 | 0.408 | 0.011 | 0.867 |
| Grip strength | 13.130 | 6.261 | 0.138 | 0.038 | 2.634 | 3.378 | 0.053 | 0.437 |
| Gait speed | 0.215 | 0.332 | 0.055 | 0.518 | –0.001 | 0.177 | –0.001 | 0.994 |
| Chair stand | −6.814 | 6.973 | –0.086 | 0.330 | 1.522 | 3.716 | 0.036 | 0.683 |
| SPPB score | 1.675 | 1.781 | 0.083 | 0.349 | 0.034 | 0.950 | 0.003 | 0.971 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, I.-Y.; Jung, H.-W.; Park, J.H.; Kim, J.H.; Lee, S.; Lee, E.; Lee, J.Y.; Park, S.J.; Kim, D.A.; Kim, S.J.; et al. Lower Serum n-3 Fatty Acid Level in Older Adults with Sarcopenia. Nutrients 2020, 12, 2959. https://doi.org/10.3390/nu12102959
Jang I-Y, Jung H-W, Park JH, Kim JH, Lee S, Lee E, Lee JY, Park SJ, Kim DA, Kim SJ, et al. Lower Serum n-3 Fatty Acid Level in Older Adults with Sarcopenia. Nutrients. 2020; 12(10):2959. https://doi.org/10.3390/nu12102959
Chicago/Turabian StyleJang, Il-Young, Hee-Won Jung, Jin Hoon Park, Jeoung Hee Kim, Seungjoo Lee, Eunju Lee, Jin Young Lee, So Jeong Park, Da Ae Kim, Su Jung Kim, and et al. 2020. "Lower Serum n-3 Fatty Acid Level in Older Adults with Sarcopenia" Nutrients 12, no. 10: 2959. https://doi.org/10.3390/nu12102959
APA StyleJang, I.-Y., Jung, H.-W., Park, J. H., Kim, J. H., Lee, S., Lee, E., Lee, J. Y., Park, S. J., Kim, D. A., Kim, S. J., Yoo, H. J., & Kim, B.-J. (2020). Lower Serum n-3 Fatty Acid Level in Older Adults with Sarcopenia. Nutrients, 12(10), 2959. https://doi.org/10.3390/nu12102959