
Boron Chemistry for Medical Applications


1
School of Pharmacy, Macau university of Science and Technology, Avenida Wai Long Taipa, Macau 999078, China
2
Department of Chemistry and Biochemistry, Northern Illinois University, DeKalb, IL 60115, USA
*
Authors to whom correspondence should be addressed.
Molecules 2020, 25(4), 828; https://doi.org/10.3390/molecules25040828
Submission received: 20 January 2020
/
Revised: 7 February 2020
/
Accepted: 11 February 2020
/
Published: 13 February 2020
(This article belongs to the Special Issue Boron Chemistry and Its Development in the 21st Century: In Memory of Professor Bohumil Štíbr (1940-2020))
Abstract
:Boron compounds now have many applications in a number of fields, including Medicinal Chemistry. Although the uses of boron compounds in pharmacological science have been recognized several decades ago, surprisingly few are found in pharmaceutical drugs. The boron-containing compounds epitomize a new class for medicinal chemists to use in their drug designs. Carboranes are a class of organometallic compounds containing carbon (C), boron (B), and hydrogen (H) and are the most widely studied boron compounds in medicinal chemistry. Additionally, other boron-based compounds are of great interest, such as dodecaborate anions, metallacarboranes and metallaboranes. The boron neutron capture therapy (BNCT) has been utilized for cancer treatment from last decade, where chemotherapy and radiation have their own shortcomings. However, the improvement in the already existing (BPA and/or BSH) localized delivery agents or new tumor-targeted compounds are required before realizing the full clinical potential of BNCT. The work outlined in this short review addresses the advancements in boron containing compounds. Here, we have focused on the possible clinical implications of the new and improved boron-based biologically active compounds for BNCT that are reported to have in vivo and/or in vitro efficacy.
1. Introduction
Carbon chemistry has been widely studied over the past two centuries. Despite its neighbor in the periodic table, the study of boron chemistry is relatively a newcomer compared to the chemistry of carbon. However it is rich as building block of its own, and has been mostly used in dealing with carbon chemistry [1,2].
Boron is generally found in minute amounts in the human body (in an average individual it’s not more than 18 mg [3]). However, it has the potential to be considered as facilitator in new biological activities and can be utilized in pharmaceutical drug design. Mainly, the boron-containing bioactive molecules are of two types; one type of molecules contains a single boron atom, while the other is in the form of a boron cluster. Boron has the ability to instantly convert from a trigonal planar (sp2 hybridized) form, that is a neutral form, to a tetrahedral (sp3-hybridized) form, which is an anionic form in the single boron atom-containing compounds when used under physiological conditions. This provides the basis for using boron to design inhibitors for enzyme-catalyzed hydrolytic processes by adopting carbon-based transition states [4,5]. While the boron atoms as a whole in the cluster compounds are used rather than a separated or single boron atom, the unique interaction with targeted proteins are possible mainly due to their presence in cage structure [6,7,8].
In boron chemistry, the borane or boron hydride history started from the innovative work of Alfred Stock and his co-workers, who prepared a series of simple boranes [9]. However, the unusual nature of the bonding in borane became apparent in 1954 from the research of Lipscomb and co-workers describing the theoretical prediction in icosahedral borane [B12H12] [10]. The boron clusters concept was introduced by the research of Roberts and Longuet-Higgins suggesting that the stable form of icosahedron would have an overall 2-charge [11]. Hawthorne and Pitochelli validated this statement by reporting a series of synthetic investigations, including the formation and uses of decaborate [B10H10]2- and dodecaborate [B12H12]2- anionic species [2,12]. Similarly, a comparative analysis of the possibilities and characteristic features of the application of various polyhedral boron compounds, viz., the closo-decaborate anion [B10H10]2–, the closo-dodecaborate anion [B12H12]2–, the carba-closo-dodecaborate anion [CB11H12]–, carboranes C2B10H12, and the bis(dicarbollide) complexes [M(C2B9H11)2]– (M = Fe, Co, or Ni), have been discussed by Sivaev et al., [13]. In addition, other scientist reported other boron-based compounds like an icosahedral closo B122- scaffold supporting multiple gadolinium complexes by Goswami et al., [14], and so on.
The actual motivation for the advancement of medicinal chemistry of boron was started from the use of boron neutron capture therapy (BNCT) for cancer treatment [15,16]. This is linked with the development in nuclear research technology and the availability of neutrons source suitable for the clinical treatment of cancers via BNCT. In 1960s, the discovery of polyhedral boron compounds facilitated the mission of BNCT through new boron carriers containing boron clusters rather than those with a single boron atom per molecule [17,18,19,20]. A major area of main group inorganic/organometallic chemistry has been developed from the study of electron-deficient boron clusters that overlaps with medicinal and organic chemistry to form a new area of bioorganic chemistry involving boron carriers for the treatment of tumor using BNCT model. Among new compounds of low-molecular weights for BNCT use are the carborane-containing carbohydrates, amino acids, nucleosides, nucleic acids and bases, lipids, DNA groove binders, and porphyrins [17,18,19,20]. Recently, a new generation of radiosensitizers was described for BNCT that includes biopolymers containing one or more carbonyl deposits. This class of boron species contains nucleic acids (DNA-oligonucleotides), carbonyl oligophosphates, and carbonyl peptides and proteins [5,19,21].
There are some strict requirements before using the boron drugs for BNCT application with regards to their toxicity, solubility and dosage accumulation in the cancer cells. However, the basic knowledge about pharmacokinetics and toxicity of boron compounds has been achieved by broad study of boron carriers for BNCT, that can be useful for the development of boron compounds for other biological applications.
Recently, new biological activities of boron cage molecules and their complexes have been revealed, including anticancer activity, anti-HIV activity, anti-rheumatoid arthritis activity, drug delivery and imaging for diagnosis and treatment of cancer and probing protein-biomolecular interactions [1,22,23,24].
These and other new observations clearly show that boron-containing compounds have great unexplored potential for medical applications and in bioorganic chemistry. It is not essential that boron should be the solution to all medical issues but it will be a welcome addition to the toolbox of medicinal chemistry. Three decades ago, fluorine was a newcomer to the medicinal chemistry and, today, the compounds of fluorine are synthesized on a routine basis in pharmaceutical research, and embrace a considerable part in the pharmaceutical market. The drug analogs bearing a variety of biological activities with a single boron atom or boron cluster molecules show that further exploration is required to realize the potential of boron in medicinal chemistry. Various reviews and books have been recently published showing the advances in boron chemistry and its applications [1,21,25,26,27,28,29,30,31,32,33,34,35,36,37], but this review will reveal many of the applications of boron chemistry in the medical field.
2. Boron Clusters for Medical Applications
Boron clusters are the main topic of several review articles and books [1,19,21,25,38], therefore, in this review only the basic information on boron clusters is provided; however, a little detail is given about their applications in medical field.
2.1. Structure Features of Boron Clusters
Carborane clusters and polyhedral boranes are characterized by delocalized electron deficient bonding, meaning that there are too few valence electrons for bonding to be described exclusively in terms of 2-center-2-electron (2c2e) pair bonds [39,40]. One characteristic of electron deficient structures is the aggregation of atoms to form 3-center-2-electron (3c2e) bonds, which typically results in the formation of trigonal faces and in hypercoordination [41]. The high connectivity of atoms in a cluster compensates for the relatively low electron density in skeletal bonds [41]. In drawing these polyhedral structures, it is common not to indicate the atoms at each vertex specifically. The typical boron and carborane clusters form the three-dimensional deltahedral shapes. Wade explained the clusters in their closo polyhedral forms, where n is the number of boron atoms containing n + 1 skeletal bonding electron pairs, typically resulting in anions of the type closo-[BxHx]2- (x = 6−12 and above) [42].
The best-known types of polyhedral boron compounds which are most often used in medicinal chemistry are icosahedral dicarbadodecarboranes (C2B10H12), in which two CH units replaced the two BH vertices. Icosahedral carboranes have been known for more than half a century and are topologically symmetrical or globular molecules [25,43]. The molecular size of carboranes is almost larger than the volume of a rotated benzene ring and or adamantine, and the bonds of B–B and C–B in carboranes are of 12-vertex and are approximately 1.8 angstroms (Å) in length.
Carboranes have a highly delocalized electron hydrophobic surface, and are reflected to be inorganic benzenes or three-dimensional aromatic compounds [44]. The carborane occupied almost 50% greater space than that of the rotating phenyl group. The carboranes are found in three isomeric forms due to the position of two carbon atoms within the cage as shown in Figure 1 The carborane system has the ability to enter in the substitution reaction at both boron and carbon atoms without degradation of the carborane cage. This is considered to be one of the most important features of this system for participation in various types of substitution reactions.
2.2. Properties of Boron Clusters for Medical Applications
Boron clusters have the following properties that are helpful in drug design: (a) the unique non-covalent interaction ability, including ionic interactions, σ-hole bonding and dihydrogen bond formation, is different from that of pure organic molecules due to its interaction with biological targets [21,44,45]; (b) ellipsoidal or spherical geometry and 3D arrangement which are helpful in the construction for 3D molecule; (c) the hydrophilicity, amphiphilicity, or lipophilicity allows the alteration of bioavaliabilty and pharmazcokinetics which is subject to the type of boron cluster utilized; (d) bioorthogonality, lessened vulnerability to metabolism and stability in a biological environment; (e) chemical stability and concurrent vulnerability to functionalization; (f) resistance to ionizing radiation, this property is essential for the radiopharmaceutical drug designing; and (g) high content of boron in the cluster is an important aspect to explore its application for BNCT [5,6,46].
The most widely studied compounds of boron in medicinal chemistry are carboranes, which are a class of cage-structured borons. In addition to carboranes, other boron clusters of dodecaborate anion and coordination compounds, accommodating different sizes and cage-structural topographies (metallacarboranes and metallaboranes), are also of great interest. Apart from these properties of desirable biological applications, the main advantage of boron cluster and their complexes is their abiotic nature and, consequently, they are biologically and chemically orthogonal to intuitive cellular constituents and resilient to catabolism.
2.3. Boron Cluster Implication for Drug Design
Specific and unspecific binding of boron clusters as protein ligands have been observed as explained in detail elsewhere [47,48]. In order to better understand the interaction modes of boron cluster compounds, these interactions should be carefully mapped, such as photoreactive groups [49]. Promiscuous binding is more frequently observed in fragment- based drug design, which is not desirable. However, it will be able to highlight molecular interactions and structural motifs capable of binding boron clusters.
The ability of boron clusters to influence the integrity and structure of a lipid membrane, and the strong binding of ionic boron clusters towards common cyclodextrins hydrophobic interior is an indication for the penetration of ionic boron clusters towards the hydrophobic environment of cell membranes. These properties are highly desirable for any type of drug design because boron clusters will not only convey water solubility to the compounds, but also allow them to penetrate the membrane. This behavior is required for a drug to reach to its target. Various studies were carried out to show the solubility of such compounds in a hydrophobic environment [50,51], thus Genady et al. [52] have recently demonstrated that a fluorescent dye can penetrate and accumulate in the cellular membrane of mammalian cells.
Computational methods, to handle boron clusters used in medicinal chemistry, have been explored by some studies as reported in the literature [53,54]. In organic structures, force fields have been developed for each functional group and are routinely applied in docking programs. However, no such field exists for boron and, particularly, for boron clusters. Therefore, the carbon force fields were used to treat the boron cluster (almost as an adamantane) to obtain the data in the literature [53,54]. The computational outcomes obtained from imitating boron clusters with carbon force fields must be considered fairly unreliable. The properties of the boron cluster are vastly different in comparison to adamantanes or carboxylic acid, which are shown by the lack of activity of adamantane-substituted m-, and p- carbonyl derivative when compared to o-derivative of indomethacin [55], or the huge difference in nicotinamide phosphoryltransferase inhibitors comprising either a neutral carborane or an adamantane [56]. Therefore, appropriate force fields need to be developed for ionic and neutral boron clusters before incorporating them in docking programs.
3. Boron Neutron Capture Therapy (BNCT)
3.1. Mechanism of BNCT
Recently, boron neutron capture therapy (BNCT) has attracted attention because it is a strategy for binary targeting and noninvasive treatment of cancer. BNCT is a possible treatment methodology for cutaneous melanomas, extramammary Paget’s diseases of genital regions, vulvar melanoma, neck and head cancers, and high-grade gliomas [30,57,58,59,60]. An appropriate number of 10B atoms must be introduced to the neoplastic cells that could be irradiated with adequate number of neutrons to obtain a successful BNCT reaction (the graphical representation of BNCT is shown in Figure 2). It is reported that a cell required an average of 3–7 alpha-particles (from 7Li nuclei) and 10B/g to destroy a tumor tissue of ca. 15 µg [19]. Therefore, the production of clusters having high boron content play an important role if BNCT is clinically accepted to evolve the treatment for cancer. In the early days of formulating boron carriers for BNCT, mostly mixture of 10B (19.9%) and 11B (80.1%) isotopes of natural boron were used. In clinical applications, the 10B enriched boron carriers are used due to its higher neutron capture cross-section 3837 barns as compared to 0.005 barns of 11B. Alpha particles are more valuable than X-ray for radiotherapy, due to their following properties (a) no need of oxygen for alpha particles to increase their biological effectiveness; [59], (b) much higher relative biological effect (RBE) of alpha particles [36], and (c) Both dividing and nondividing tumor cells can be killed by alpha particles [8]. These properties enable alpha particles tagged with B-10 to selectively kill various types of cancer cells without damaging the normal cells, that helps to prevent the side effects for patients.
The ideal boron-containing agent should fulfill the following requirements: (i) low systemic toxicity; (ii) approximately 30 μg 10 B/g tumor concentrations; (iii) high tumor uptake and low normal tissue uptake; and (iv) rapid normal tissue clearance but persistence in tumor tissue during BNCT.
3.2. Current BNCT Agents
In order for BNCT to be successful, it must get enough boron to the tumor cell [8]. Two types of boron-containing drugs have been utilized for clinical treatment for more than 1000 patients using BNCT. These are mercaptoundecahydrodecaborane (BSH) and boronophenylalanine (BPA), whose structures are illustrated in Figure 3 [7]. However, the ideal dosage of either BPA or BSH or the combination of the two in the delivery system to the patients with high grade gliomas has yet to be established. The Swedish group reported [62,63], that by increasing the duration of the infusion time for BPA dose would be a good starting point, but microdistribution and improving tumor uptake could require more than this strategy. Therefore, BNCT for additional clinical applications is somewhat obstructed due to poor boron transfer competence of BSH and BPA [1,35,64]. Nonetheless, an optimal response to BNCT for improving tumor uptake of boronated compounds critically depends on performing the neutron irradiation at the time of maximum boron accumulation (or highest T/N ratio). Determining the maximum boron accumulation in patients’ tumor, reliably, is one of the biggest limitations of BNCT, especially considering the fact that inconsistency always exists in different kinds of tumors among patients. Positron emission tomography (PET) guiding BNCT can potentially overcome this challenge by using a dual modality agent [65] in which the real-time boron accumulation within the tumor of the patients can be monitored. The 4-borono-2-18F-fluorophenylalanine (18F-BPA) is one of the examples of a dual modality BNCT agent, which is a radiolabeled derivative of BPA as shown in Figure 3 The 18F-BPA uptake for head and neck cancers can be correlated with the uptake of 18F-fluorodeoxyglucose [66]. The 18F-BPA administration has also been reported for numerous types of tumors such as malignant melanomas, malignant gliomas and various head and neck cancers with tumor/normal tissue ratios ranging from 1.5 to 7.8 [67,68].
3.3. Development of Novel BNCT Agents
Recently, many small molecule-based boron carriers have been explored in the preclinical trials, some of which are discussed here. However, due to their insufficient accumulation of boron in tumor cells, clinical studies have been limited [34,46].
Researchers tried to overcome this problem by developing boron-containing nanoparticles for delivering at least 20 ppm of boron to the tumor cells [61,69]. Some of the developed boron-containing nanoparticles have significantly improved the delivery efficacy of boron to the tumor cells and exhibited excellent tumor destruction in animal models [61,70]. Nevertheless, boron-containing nanoparticles shows in vivo toxicity i.e., resistance to degradation, which is the main concern for its clinical translation [71,72,73]. To overcome these problems, some researchers have shown interest in preparing biodegradable boron-containing nanomedicines with the help of biodegradable polymers. This includes natural polymers such as chitosan, gelatin, albumin, collagen and alginate [74,75,76], or synthetic polymers such as poly-(ethylene glycol)-block-poly(lactide) copolymer (PEG-b-PLA), poly(D.L-lactide-co-glycolide) (PLGA), and polylactides (PLA) as coating layers [77,78,79,80], and boron compounds as boron carriers [61,81,82,83]. These polymers undergo hydrolysis in a physiological environment due to their polyester structure. Compared to the natural degradation mentioned above, the exogenous response is more precise and controllable [84,85,86], compared to the on-demand decomposition process [46]. A third generation of boron-containing compounds were recently investigated. A stable boron cluster is attached to a tumor-targeting moiety via a hydrolytically stable linkage, such as low or high molecular weight agents [87]. Boron-containing amino acids, biochemical precursors, polyhedral boranes, DNA-binding agents, mannose, glucose, ribose, galactose, fucose, lactose molecules, amines, benzamides, nitroimidazole, nicotinamides, phosphates, phosphonates, isocyanates, azulenes, phenylureas, thioureas, and deualinium derivates are included in low molecular weight agents while high molecular weight agents include liposomes, receptor-targeting agents, and monoclonal antibodies. These new generation boron-containing agents show better selective targeting properties when compared to the old generation boron compounds [87]. However, their biological properties depend on the density of the targeted sites and very little data have been reported to date on the third-generation of boron-containing agents. Some of these newly reported boron-containing agents are discussed below.
3.3.1. Boron Nanoparticles with BNCT
Due to significant boron content in the pure boron nanoparticles, they are considered as potentially promising boron carrier agents. Although they can be prepared by various synthetic methods, the commonly employed techniques are pyrolysis, chemical vapor deposition (CVD), thermal plasma, reduction in solution, ball milling and arc discharge [29,88,89,90]. Icten et al. reported [91] the use of the ball milling method for the preparation of magnetic dopamine-functionalized boron nanoparticles, which show a size range of 100–700 nm. As a result, the ball milling method produces, in one step, both boron nanoparticles and their functionalization [91]. This group further investigated the synthesis of magnetic nanocomposites containing polyethylene glycol, Fe3O4 and mono or bis(ascorbatoborate) [92]. The resulting nanocomposites had an average size of 10–15 nm and show good paramagnetic behavior at 300 K [92]. These materials are considered to be the potential constituents for magnetic biomedicine, since the composites combined with ascorbic acid are recognized as useful antitumor and radical scavenging agents.
Recently, Sing et al. [61], reported the synthesis of pure boron nanoparticles comprised of a liposome of azolectin-based phospholipid using the water-in-oil emulsion method. This new material contains polyethylene glycol (PEG) and poly(maleic anhydride-alt-1-octadecene) (PMAO) on the surface, and boron nanoparticles and Cy5 near infrared (NIR) fluorescent dye in the core (3PCB) as shown in Figure 4, which is considered as an alternative BNCT agent. For improvement in accumulation and targeted delivery of boron to cancer cells, a tumor-specific targeting ligand, folic acid (FA), was conjugated to PEG to produce a folate-functionalized liposome (FA-3PCB). The liposomes exhibited a zeta potential of —38.0 ± 1.5 mV and an average diameter of 100–120 nm. The targeting capability of FA-conjugated liposomes was confirmed by monitoring the cellular uptake by fluorescence microscopy. It was observed that the accumulation of FA-conjugated liposomes in C6-brain tumor cells was much higher than that of non-FA conjugated liposomes under the same conditions. The quantification of sufficient accumulation of boron in cancer cells for therapeutic benefit from BNCT was confirmed by Inductively Coupled Plasma Mass Spectrometry (ICP-MS). These liposomes show blood-brain barrier (BBB) crossing ability, excellent stability, and low cytotoxicity under physiological conditions. Thus, these liposomes are considered to be promising new boron carriers for BNCT.
3.3.2. Boron Nitride Nanotubes/Nanoparticles with BNCT
Recently, highly water dispersible boron nitride (10BN) has been synthesized by using the solvothermal method at relatively low temperature [93]. The morphological structural analysis of 10BN has been carried out along with a cytotoxicity analysis on normal (HEK-293) and cancer (HeLa, MCF-7) cells, the results illustrates that 10BN is relatively less toxic and produces insignificant oxygen species. The promising BNCT antitumor effect was observed in 10BN treated HeLa cells. The thermal neutron fluence of ~6.3× 1012/cm2 resulted in almost 50% cell killing of BN treated HeLa cells. Another study reported the antitumor effects of boron nitride nanotube (BNNTs) with BNCT towards melanoma cells [94]. The accumulation of BNNTs in B16-melanoma cell was three times higher than BSH and their antitumor effect with BNCT was also observed higher than BSH. The BNNTs are also attracting the attention of the scientific community as did the carbon nanotubes (CNTs) earlier. Nonetheless, the BNNTs are lightweight with excellent mechanical properties and offer strong resistance to oxidation when compared to CNTs. Therefore, the BNNTs used in nanocomposites are considered to be multifunctional materials with promising applications in biomedical fields, nanoscale electrical devices, optical systems and in space radiation shielding [95,96,97,98]. In addition, the high boron density of BNNTs make them to be possible aspirants to the boron agents [94,99,100,101].
In 2019, Wei et al. [102] reported the boron nitride nanotubes-conjugated folate (BNNTs-FA)-based targeted drug delivery strategy to improve the efficacy of Auristatin PE (PE). The PE as an anti-microtubule agent possesses good anticancer activity. However, strong side effects and poor targeting ability limits its clinical applications. Therefore, the targeted delivery of PE may overcome the disadvantages associated with PE, being very conducive to continuing clinical trials of PE. As pointed out above, BNNTs have attracted considerable attention for drug delivery due to their unique physical and chemical properties. Wei [102] found that PE was successfully loaded via π-π stacking and hydrogen bonding interactions onto BNNTs-FA and due to the increased cellular uptake of PE, mediated by the FA receptor, the BNNTs-FA@PE exhibited stronger cytotoxicity to Hep G2 cells than free PE and BNNTs@PE complexes, as shown in Figure 5 Also, BNNTs-FA@PE demonstrated excellent antiproliferative activities in time- and dose-dependent manners. Additionally, the BNNTs-FA@PE induced apoptosis of Hep G2 cells by reducing the mitochondrial membrane potential via intrinsic mitochondria–mediated pathway, activating Caspase-9 and Caspase-3. This study, demonstrates the construction of the BNNTs-FA@PE system, that significantly improves the PE effect on the target and may be considered as a promising material for the treatment of liver cancer in the near future.
Recently, it has been reported that boron nitride nanoparticles (BNNPs) exhibited good results in treating triple negative breast cancer in mice [46]. Since BNNPs show good biocompatibility and have high boron content capacity, they are considered as promising boron carriers. On-demand degradable boron carriers were designed and were coated by a phase-transitioned lysozyme (PTL) as shown in Figure 6a. The PTL protects the BNNPs from hydrolysis during blood circulation and can be readily removed by vitamin C after NCT. The report also indicated that the coated BNNPs showed high boron accumulation in the tumor while maintaining its good ratio between tumor and nontumor cells. After neutron irradiation, the tail-vein injections of vitamin C were followed, and it was found that BNNPs were rapidly cleared from major organs according to ex vivo ICP-OES analysis (Figure 6b). Compared with the control group, animals treated with BNCT showed suppression of tumor growth, while almost negligible side effects were observed. This strategy not only utilized the high boron content of BNNPs but also successfully performed an on-demand degradation of BNNPs to avoid the potential toxicity caused by the long-term accumulation of nanoparticles. Even high accumulation of B atoms inside the cells have been shown by these nanoparticles but they have failure in the therapeutic window for BNCT. More improvements are still needed to design a 10B-enriched BNNPs source [103,104].
3.3.3. Gold Nanocluster/Nanoparticles with Borane for BNCT
Recently, gold nanoparticles (AuNPs) have been utilized as delivery agents for releasing selective cytotoxic payloads to the tumor. However, studies demonstrating the in vivo distribution or pharmacokinetics of boron-containing AuNPs via noninvasive imaging are lacking. Chun et. al. [105] have used theranostic AuNPs with boroncage assemblies (B-AuNPs) to estimate its practicality for BNCT application. They subjected the commercial citrate-coated AuNPs to PEGylation, azide addition, and carborane modification on the surface. Further, they conjugated anti-HER2 antibody (61 IgG) with boron-containing PEGylated AuNPs to form 61-BAuNPs. The anti-HER2 antibody (61 IgG), provided by Prof. An-Suei Yang (Academia Sinica, Taiwan), and boron cage-SH (BC-EG-SH; Figure 7A), courtesy of Prof. Ming-Hua Hsu, and the surface modification of AuNPs are shown in Figure 7B. The radio thin-layer chromatography (radio TLC) was used to determine the radiolabeling efficiency and dynamic light scattering (DLS) of boron-containing AuNPs. The pharmacokinetics of radioiodinated AuNPs in N87 gastric cancer xenografts was determined by computed tomography (CT)/noninvasive single-photon emission computed tomography (SPECT) imaging, and boron contents in muscle and tumors were determined by inductive coupled plasma mass spectrometry (ICP-MS). It was observed that the diameter of B-AuNPs increased by approximately 25 nm after the 3-step modification, and the diameter of AuNPs was not affected by antibody conjugation. The radioactive iodine (I123) in AuNPs under copper catalysis was introduced with the help of Click chemistry. The radiolabeling efficiency of 123I-B-AuNPs and 123I-61-B-AuNPs was observed upto 60 ± 5% and the radiochemical purity (RCP) of these NPs after purification was greater than 90%.
It was reported that the micro CT/SPECT imaging exhibited the tumor-to-muscle (T/M) ratio of 123I-B-AuNP-injected mice reached 1.91 ± 0.17 at 12 h post-injection, while that of 123I-61-B-AuNP-injected mice was 12.02 ± 0.94. Therefore, it was indicated that the increased uptake of AuNPs by the thyroid at 36 h after the administration of 123I-61-B-AuNPs was observed due to antibody-mediated phagocytosis. They also reported that the T/M ratio, assessed by ICP-MS, of mice injected by B-AuNP- and 61-B-AuNP was 4.91 ± 2.75 and 41.05 ± 11.15, respectively. The results show the successfully developed detectable HER2-targeting boron-containing AuNPs with high RCP and an acceptable yield. From this study, it may be considered that noninvasive imaging could be a valuable tool for the noninvasive determination of the pharmacokinetics of AuNPs and measurement of boron concentration in the tumor.
Wang et al. [106] reported the gold nanoclusters with carborane amino derivatives for the targeted delivery of the carborane compound to the tumors and precise bioimaging of cancer cells. They prepared carborane derivative (NH2NH3)+[7-NH2(CH2)3S- 7,8-C2B9H11]- according to the literature [107], and stored it at —18 °C. Gold nanoclusters (GNCs) were freshly prepared and dispersed in PBS (pH 7.2). Fluorescent GNCs were produced using glutathione (GSH), according to the reported method in the literature [108]. The accurate tumor imaging by EPR effect and long-term accumulation in tumor cell by nanometer size effect have been observed. This strategy is good for attaining the accurate position of tumor cells with carborane derivatives and thus decreases the chances of normal tissue damage. In addition, it facilitates the real-time fluorescent visualization to monitor delivery process of the carborane to the targeted tumor, thus endorsing the effect of BNCT treatment through imaging guided therapy.
The schematic illustration of this study is shown in Figure 8 In another study, the gold NPs were stabilized with polyethylene glycol (PEG), functionalized with bis(dicarbollide), radiolabeled with 124I at the core and the shell, and examined in vivo with a mouse model by using positron emission tomography (PET). The results showed a poor accumulation in tumor and major accumulation in liver, lungs and spleen suggesting that the tuning the size and geometry of the gold core is essential [109].
3.3.4. Boron-Based Amino Acids for BNCT
Most of the amino acids utilized in BNCT for precise treatment of malignant brain tumors [110], have been reported and the review published recently by Jiyuan et al. [111] reported the development of a metabolically stable boron-derived tyrosine (expressed as fluoroboronotyrosine, FBY) as a theranostic agent for both boron delivery and cancer diagnosis, leading to PET imaging-guided BNCT in the treatment of cancer as shown in Figure 9a. The computational study of FBY, Tyrosine, and BPA showed similarities between them to a greater extent. The FBY, Tyrosine, and BPA chemical structures and molecular electrostatic potential (MEP) images were shown in Figure 9b, where red indicates the distribution of negative charge and blue indicates the distribution of positive charge. The Figure 9c exhibited LAT-1 (gray) in solid ribbon representation, the predicted structure of the LAT-1 and FBY (yellow)/Tyrosine (green)/BPA (pink) complex, LAT-1. The hydrogen bonds between LAT-1 and ligands are known to be highly conservative involving residues Trp202, Ser26, Gly27, Ile205, and Ile23 which are shown as dotted sky-blue lines. The [18F]FBY was synthesized in high radiochemical purity (98%) with high radiochemical yield (50%).
It was also demonstrated that the prepared FBY showed high similarity with natural tyrosine. The uptake of FBY in murine melanoma B16-F10 cells was L-type amino acid transporter (LAT-1) dependent and reached up to 128 μg/106 cells. While the FBY displayed high stability in PBS solution, the [18F]FBY PET showed up to 6% ID/g in B16-F10 tumor and notably low normal tissue uptake (tumor/muscle = 3.16 ± 0.48; tumor/blood = 3.13 ± 0.50; tumor/brain = 14.25 ± 1.54). Moreover, the administration of [18F]FBY tracer along with a therapeutic dose of FBY showed high accumulation in B16-F10 tumor and low normal tissue uptake.
The FBY enriched tumor having more than 20 ppm of boron and a desired correlation was established between tissue boron concentration and uptakes from PET imaging. The PET images, shown in Figure 9d, were recorded nearly 75 min after injection of 20 mg of FBY and [18F]FBY, intravenously. While the CT and PET-CT images of the brain coronal showing the [18F]FBY uptake, the representative transverse CT and PET-CT images of lung tumor and liver showed prominent [18F]FBY uptake in the B16-F10 lung tumor and the increased liver retention of [18F]FBY, respectively. The correlation between PET-image and boron biodistribution was established (Figure 9e) indicating the possibility of estimating boron concentration via a noninvasive approach. Using thermal neutron irradiation, B16-F10 tumor-bearing mice injected with FBY showed significantly prolonged median survival without exhibiting obvious systemic toxicity. In conclusion, FBY holds great potential as an efficient theranostic agent for imaging-guided BNCT by offering a possible solution of measuring local boron concentration through PET imaging and can be used for clinical trials.
3.3.5. Boron-based Polymers for BNCT
A review, published recently by Chauhan et al. [112], covered the syntheses of most of the boron-based polymers and their application in BNCT treatment. This review discusses a few boron-based polymers that could be useful for biomedical applications. Ochiai et al. [113] reported polymer composites based on boron-doped diamond powder (BDDP), which have been utilized for the treatment of dental problems. The BDDP-based polymer was considered to be the practical species, since it possesses qualities, such as hard to crack or peel, and appreciable durability even with repeated bending during electrolysis. Chen et al. [114] proposed the use of iRGD-modified polymeric nanoparticles for active targeted delivery of boron and doxorubicin (DOX) in BNCT. They covalently grafted the 10B-enriched BSH by PEG-PCCL for the prearation of 10B-polymer and then modified its surface by iRGD, followed by incorporation of DOX into polymers, physically. The resulting polymers show enhanced accumulation of 10B in tumors when compared to BSH and prolonged blood circulation, along with the favorable boron concentration ratios for tumor:normal tissue (tumor:muscle = 19.49, tumor:blood = 14.11) in A549 tumor-bearing mice after 24 h of injection. The highest tumor accumulation of DOX was confirmed from both quantitative measurement and fluorescence imaging at 24 hrs after injecting iRGD-modified polymers [114]. However, more future studies are required to utilize these types of polymers for clinical trials. The properties, such as electrical carrier injection, transport, photoluminescence, solid-state luminescent, and reflective index make such boron-based polymers useful for molecular machines, multiphoton microscopy, and waveguides, optical data storage, cell biology, and tumor hypoxia (Table 1).
4. Accelerator-Based BNCT (AB-BNCT)
The reactor-based BNCT facilities are now shifting to accelerator-based BNCT (AB-BNCT). Consequently, various types of AB-BNCT have been planned and developed. Currently, only Japan uses these facilities for treatment purposes. However, in some other countries several new projects have been proposed and the new BNCT facilities are under construction, including those in Finland, China, Taiwan and Argentina [115,116]. Recently, Hirose et al. [116] reported the initial results of the phase-II trial of AB-BNCT by using cyclotron-based neutron generator and 10BPA in patients with recurrent and locally advanced head and neck cancer. The 8-recurrent squamous cell carcinoma (R-HNSCC) and 13 recurrent/locally advanced non-squamous cell carcinoma (R/LA-HNNSCC) patients were enrolled and received AB-BNCT. The tumor response was assessed every 4 weeks for the first 3 months. By the first 3-months, central review of the local control was observed in 20 patients out of total 21 patients. Except for asymptomatic hypermylasemia associated with acute parotitis, all the patients had no ≥ grade 4 toxicity. This data is still immature and needs further exploration to know the treatment efficacy [116]. However, it can be suggested that AB-BNCT could provide a promising treatment option for the R-HNSCC and R/LA-HNNSCC patients. An issue with AB-BNCT is the targets and it required more time to obtain information regarding its lifetime and stability. Low cost of construction and running, as well as high stability, are required for medical practice. Therefore, for future AB-BNCT application the more suitable accelerator development is still desirable.
5. Treatment of Different Cancer Tumor with BNCT
5.1. Recurrent Head and Neck Regional Tumor Treatment with BNCT
The treatment of recurrent tumors of the head and neck (HN) region by using BNCT have been applied to the second largest group of patients who had no other treatment options or reached normal tissue tolerance level. Although the number of patients treated in Taiwan, Finland and Japan by this method are relatively small, the result of this treatment shows some very remarkable clinical consequences [117,118,119,120].
Wang et al. [121] reported that a total number of 17 patients with recurrent HN tumors were treated with two doses of BNCT over 28 day intervals using BPA-F as the boron delivery agent. Although the toxicity was acceptable and the response rate was high (12 out of 17 patients), the tumor recurrence was common near or within the treatment site. Similar results were observed by Finnish and Japanese clinicians, who also treated the recurrent HN tumor patients. The resulting recurrence after treatment with BNCT might be due to the poor microdistribution of BPA-F in some region of the tumor, such as non-homogenous uptake of BPA-F by the tumor cells [30,122].
While the “best” boron delivery agent are yet to be developed, the optimal dose and delivery of BPA (alone or in grouping with BSH) is the best hope to improve the response and success rates. Consequently, Soarce et al. [123] and Wu et al. [124] reported that the uptake and microdistribution of BPA-F in HN or glioma cancer patients could be increased by pulsed ultrasound suggesting that it should be evaluated clinically as a possible option for BNCT treatment [123,125,126].
Recently, Jai-Cheng reported the comparison of dose distributions in gross tumor volume between BNCT alone and BNCT combined with intensity modulation radiation therapy (IMRT) for head and neck cancer. He suggested that compared to single-fraction BNCT, the multi-fraction IMRT combined with single-fraction BNCT improves the treatment conformity and homogeneity and possibly local tumor control, especially for tumor whose volume is greater than 100 cm [127]. A recent study, published in Radiotherapy and Oncology, demonstrated the efficiency of BNCT in the treatment of locally recurrent head and neck squamous cell carcinoma (HNSCC) patients and also the factors that are favorable for the treatment response and survival [128]. This study, comprising 79 patients with locally recurrent HNSCC, who were treated with BNCT in Finland, between February 2003 and January 2012.
Some exciting findings of this study, highlighted by Ying Sun [129], are as follows:
- 1)
- Most patients with local recurrent HNSCC responded to BNCT.
- 2)
- A high minimum dose delivered to the tumor was a key predictive factor for treatment response, and the number of BNCT treatments was a minimally important factor for progression-free survival and overall survival.
- 3)
- Tumor size < 25 cm3 was found to be a favorable prognostic factor for survival and achieving complete response.
- 4)
- The minimum dose to the gross tumor volume was associated with the survival rates [128,129]. This was the first study to inspect the treatment outcomes in locally recurrent HNSCC patients in association with tumor dose from BNCT. However, this is a survey study. Thus, some key statistics on critical factors, such as adverse effects related to BNCT, human papilloma virus infection, and treatment-related deaths, were not measured or recorded, and could not control the consequences. This study delivers imperative evidence-based grounds for originating random clinical trials for the comparison of BNCT efficacy with other radiotherapies. To improve patient survival, this type of study is required to determine alternative therapies.
5.2. Cutaneous and Genital Cancer Treatment with BNCT
Another category of tumors that were treated by BNCT is cutaneous melanomas. Zhang et al. [130] reported the clinical treatment of cutaneous melanomas in three Chinese patients by using compact In-Hospital Neutron Irradiator (IHNI), which is specially fabricated and designed for BNCT. Out of these three patients, one has acral melanoma on the sole of his foot who had declined surgery (as indicated in Figure 10).
Yong et al. [122] reported that grade-II acute radiation injury was observed during the first four weeks after BNCT and was healed after treatment. No late radiation injury was found during the 24-month follow-up. The patient showed a complete response to BNCT, based on pathological analysis and gross examination, positron emission tomography-computed tomography (PET/CT) scan, indicating that BNCT is a potent treatment against malignant melanoma.
Two other patients, one with multiple metastatic cutaneous nodules on the right leg and the other with acral lentiginpus subungal melanoma of the right thumb, showed partial response [122] as per the Japanese clinical results in treating the cutaneous melanomas patients using BNCT. Hiratsuka et al. [60] reported four patients with genital malignancies, who were treated with BNCT and the patients included three with genital extramammary Paget’s disease (EMPD) and one patient with vulvar melanoma (VM). They underwent BNCT at the Kyoto University Research Reactor Institute (KURRI) facility between 2005 and 2014 using para-boronophenylalanine (para-BPA) as the boron delivery agent and were irradiated with an epithermal neutron beam between the curative tumor dose and the tolerable skin/mucosal doses. All patients showed similar tumor and normal tissue responses following BNCT and achieved complete responses within 6 months, and there were no recurrences observed during the follow-up periods ranging from 1.6–6.9 years.
The tumors of vulva and penis are very difficult to treat since these tumors are very poorly reactive to conventional photon irradiation and the surgery can be very harmful. As the treating EMPD and VM with BNCT in the above study of four patients resulted in complete local tumor control. Therefore, treating a large number of patients is required before making any definitive statement. The possible combination of new immunotherapeutic tactics [131,132] with BNCT would provide a better foundation for the treatment of cancers in difficult anatomic regions, like vulva, EMPD of the penis and scrotum with BNCT [60].
Lung cancer incidence is increasing worldwide and it’s considered to be the leading cause of cancer mortality. The treatment methods of lung cancer include surgery, chemotherapy and radiotherapy [133,134]. Among these, radiotherapy plays a progressively more important role in lung cancer treatment [135]. In recent years, many researchers proposed the use of BNCT for the treatment of lung cancer because of its significant superiority to conventional radiotherapies.
In its initial stages, the Kyoto University Reseach Team in 2006, performed a dosimetric study on malignant pleural mesothelioma to examine the feasibility of BNCT and confirmed that BNCT offered hope as a treatment modality for these patients [136]. After two years, they did clinical trials by treating a patient with mesothelioma and obtained good outcomes. The patient’s chest pain disappeared without late side effects [137]. In 2014, further studies by Farias, confirmed the effectiveness and feasibility of BNCT for treating lung cancer patients [138].
6. Secondary Cancer risk with BNCT
While performing BNCT, the dose deposited in the tumor, as well as the dose not fully excreted from the healthy organs, could cause secondary cancer. The secondary cancer risk cannot be ignored for cancer survivors, while paying attention to the side effects caused by radiotherapy, especially for younger people expecting to have longer life. Recently, the healthy organs of the younger brain tumor patients, treated with BNCT for secondary cancer risk, were investigated by Xinxin Zhang [139]. The high cancer incidence organs in China were considered and the same dose amount were obtained by tumor and organs using the Monte Carlo method and were radiated by computational phantom with Chinese physiological characteristics [140]. The effects of tumor depth (3-6 cm), irradiation geometry (RLAT/TOP/PA), patients age (10-15 years) and gender (male and female) on the secondary cancer risk were explored. Their results suggest that PA geometry showed the lowest secondary risk of cancer, while TOP show the highest, because under TOP geometry, most of the organs are directly exposed to the neutron beam and the equivalent doses are higher. It has been suggested that the secondary cancer risk in healthy organs would decrease with the age in both male and female patients, which might be related to the shorter life expectancy of the older patients. The higher secondary cancer risk in most organs of female patients than male patients of the same age were related to the higher β values in the LAR formula in female patients than male patients, or can be related to the thickness and height of the patient bodies. For the clinical application of BNCT, their findings provide reference about the secondary cancer risk, that requires further exploration. Hopefully, future research will identify new and better boron delivery agents for clinical use [87,141]. Randomized clinical trials help advance cancer therapy. Few randomized trials have been conducted on BNCT until now. Cooperative research groups are required to best accomplish more randomized clinical trials of BNCT.
7. Conclusions
No inherent limitations have been reported for introducing boron into pharmaceuticals. Only a few boron-containing drugs are available on the market. It is predicted that more boron-based drugs will be explored based on the development in nanotechnology, boron chemistry and newer installations of neutron resources in Asia. In this short review, some of the possible boron-based drugs were discussed, including those currently used in clinical trials.
The BNCT could serve as a promising therapy for malignant tumors, however the only clinically used boron delivery agents BPA and BSH have moderate selectivity. This encourages the search for new boron-based delivery agents. This review summarizes some of the recently reported boron delivery agents utilized with BNCT for in vivo and/or in vitro efficacy in theraupatic area. However, there are several critical issues, as itemized below, that must be addressed before applying BNCT as a useful modality for cancers treatment.
1. More effective boron-containing agents are required so that they can be used alone or in combination with other agents to deliver the necessary amount of boron to cancer cells.
2. The delivery of boron-containing agents to the cancer cells and cellular microdistribution must be optimized to improve its uptake, especially to diverse subpopulation of cancer cells.
3. Methods to provide semi-quantitative estimates of boron content in the residual cancer cells are essential.
4. For safety and efficacy of BNCT, the evaluation of randomized clinical trials are mandatory.
Author Contributions
Conceptualization, Funding acquisition, and Supervision: Y.Z.; Manuscript draft preparing: F.A. Manuscript checking: N.S.H., All authors greed to the published version of the manuscript.
Funding
This work was funded by the Science and Technology Development Fund, Macau SAR (File no. 0030/2018/A1).
Acknowledgments
The authors gratefully acknowledge the School of Pharmacy, Macau University of Science and Technology; the State Key Laboratory of Quality Research in Chinese Medicine, Macau University of Science and Technology, Taipa, Macau, SAR.
Conflicts of Interest
The authors declare that they have no conflicts of interest to disclose.
References
- Axtell, J.C.; Saleh, L.M.; Qian, E.A.; Wixtrom, A.I.; Spokoyny, A.M. Synthesis and applications of perfunctionalized boron clusters. Inorg. Chem. 2018, 57, 2333–2350. [Google Scholar] [CrossRef]
- Pitochelli, A.R.; Hawthorne, F.M. The isolation of the icosahedral B12H12-2 Ion. J. Am. Chem. Soc. 1960, 82, 3228–3229. [Google Scholar] [CrossRef]
- Emsley, J. Nature’s Building Blocks: An AZ Guide to the Elements; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Das, B.C.; Thapa, P.; Karki, R.; Schinke, C.; Das, S.; Kambhampati, S.; Banerjee, S.K.; Van Veldhuizen, P.; Verma, A.; Weiss, L.M. Boron chemicals in diagnosis and therapeutics. Future Med. Chem. 2013, 5, 653–676. [Google Scholar] [CrossRef] [Green Version]
- Leśnikowski, Z.J. Recent developments with boron as a platform for novel drug design. Expert Opin. Drug Discov. 2016, 11, 569–578. [Google Scholar] [CrossRef]
- Lesnikowski, Z.J. Challenges and opportunities for the application of boron clusters in drug design. J. Med. Chem. 2016, 59, 7738–7758. [Google Scholar] [CrossRef]
- Scholz, M.; Hey-Hawkins, E. Carbaboranes as pharmacophores: Properties, synthesis, and application strategies. Chem. Rev. 2011, 111, 7035–7062. [Google Scholar] [CrossRef]
- Issa, F.; Kassiou, M.; Rendina, L.M. Boron in drug discovery: Carboranes as unique pharmacophores in biologically active compounds. Chem. Rev. 2011, 111, 5701–5722. [Google Scholar] [CrossRef]
- Spokoyny, A.M. New ligand platforms featuring boron-rich clusters as organomimetic substituents. Pure Appl. Chem. 2013, 85, 903–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eberhardt, W.; Crawford, B., Jr.; Lipscomb, W.N. The valence structure of the boron hydrides. J. Chem. Phys. 1954, 22, 989–1001. [Google Scholar] [CrossRef]
- Longuet-Higgins, H.C.; Roberts, M.d.V. The electronic structure of an icosahedron of boron atoms. Proc. R. Soc. Lond. Ser. A Math. Phys. Sci. 1955, 230, 110–119. [Google Scholar]
- Hawthorne, M.F.; Pitochelli, A.R. The reactions of bis-acetonitrile decaborane with amines. J. Am. Chem. Soc. 1959, 81, 5519. [Google Scholar] [CrossRef]
- Sivaev, I.; Bregadze, V.; Kuznetsov, N. Derivatives of the closo-dodecaborate anion and their application in medicine. Russ. Chem. Bull. 2002, 51, 1362–1374. [Google Scholar] [CrossRef]
- Goswami, L.N.; Ma, L.; Chakravarty, S.; Cai, Q.; Jalisatgi, S.S.; Hawthorne, M.F. Discrete nanomolecular polyhedral borane scaffold supporting multiple gadolinium (III) complexes as a high performance MRI contrast agent. Inorg. Chem. 2013, 52, 1694–1700. [Google Scholar] [CrossRef] [PubMed]
- Barth, R.F.; Coderre, J.A.; Vicente, M.G.H.; Blue, T.E. Boron neutron capture therapy of cancer: Current status and future prospects. Clin. Cancer Res. 2005, 11, 3987–4002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawthorne, M.F. New horizons for therapy based on the boron neutron capture reaction. Mol. Med. Today 1998, 4, 174–181. [Google Scholar] [CrossRef]
- Armstrong, A.F.; Valliant, J.F. The bioinorganic and medicinal chemistry of carboranes: From new drug discovery to molecular imaging and therapy. Dalton Trans. 2007, 38, 4240–4251. [Google Scholar] [CrossRef] [PubMed]
- Bregadze, V.; Sivaev, I.; Glazun, S. Polyhedral boron compounds as potential diagnostic and therapeutic antitumor agents. Anti-Cancer Agents Med. Chem. 2006, 6, 75–109. [Google Scholar] [CrossRef]
- Lesnikowski, Z.J. New opportunities in boron chemistry for medical applications. In Boron Sciences. New Technologies and Applications; CRC Press: Boca Raton, FL, USA, 2011; pp. 3–19. [Google Scholar]
- Valliant, J.F.; Guenther, K.J.; King, A.S.; Morel, P.; Schaffer, P.; Sogbein, O.O.; Stephenson, K.A. The medicinal chemistry of carboranes. Coord. Chem. Rev. 2002, 232, 173–230. [Google Scholar] [CrossRef]
- Żołnierczyk, J.D.; Lesnikowski, Z.J. Boron Cluster Modifications with Antiviral, Anticancer, and Modulation of Purinergic Receptors’ Activities Based on Nucleoside Structures. In Boron-Based Compounds: Potential and Emerging Applications in Medicine; Wiley: Hoboken, NJ, USA, 2018; p. 20. [Google Scholar]
- Hawthorne, M.F.; Maderna, A. Applications of radiolabeled boron clusters to the diagnosis and treatment of cancer. Chem. Rev. 1999, 99, 3421–3434. [Google Scholar] [CrossRef]
- Qian, E.A.; Wixtrom, A.I.; Axtell, J.C.; Saebi, A.; Jung, D.; Rehak, P.; Han, Y.; Moully, E.H.; Mosallaei, D.; Chow, S. Atomically precise organomimetic cluster nanomolecules assembled via perfluoroaryl-thiol S N Ar chemistry. Nat. Chem. 2017, 9, 333. [Google Scholar] [CrossRef] [Green Version]
- Hawthorne, M.F. The role of chemistry in the development of boron neutron capture therapy of cancer. Angew. Chem. Int. Ed. Engl. 1993, 32, 950–984. [Google Scholar] [CrossRef]
- Hey-Hawkins, E.; Teixidor, C.V. Boron-Based Compounds: Potential and Emerging Applications in Medicine; John Wiley & Sons: Hoboken, NJ, USA, 2018. [Google Scholar]
- Yinghuai, Z.; Lin, X.; Xie, H.; Li, J.; Hosmane, N.S.; Zhang, Y. The Current Status and Perspectives of Delivery Strategy for Boronbased Drugs. Curr. Med. Chem. 2019. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Hosmane, N.S. Ionic liquids: Recent advances and applications in boron chemistry. Eur. J. Inorg. Chem. 2017, 2017, 4369–4377. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Gao, S.; Hosmane, N.S. Boron-enriched advanced energy materials. Inorg. Chim. Acta 2018, 471, 577–586. [Google Scholar] [CrossRef]
- Zhu, Y.; Hosmane, N.S. Nanostructured boron compounds for cancer therapy. Pure Appl. Chem. 2018, 90, 653–663. [Google Scholar] [CrossRef] [Green Version]
- Barth, R.F.; Zhang, Z.; Liu, T. A realistic appraisal of boron neutron capture therapy as a cancer treatment modality. Cancer Commun. 2018, 38, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moss, R.L. Critical review, with an optimistic outlook, on Boron Neutron Capture Therapy (BNCT). Appl. Radiat. Isot. 2014, 88, 2–11. [Google Scholar] [CrossRef]
- Körbe, S.; Schreiber, P.J.; Michl, J. Chemistry of the Carba-closo-dodecaborate (−) Anion, CB11H12. Chem. Rev. 2006, 106, 5208–5249. [Google Scholar] [CrossRef]
- Núñez, R.; Tarrés, M.R.; Ferrer-Ugalde, A.; de Biani, F.F.; Teixidor, F. Electrochemistry and photoluminescence of icosahedral carboranes, boranes, metallacarboranes, and their derivatives. Chem. Rev. 2016, 116, 14307–14378. [Google Scholar] [CrossRef]
- Núñez, R.; Romero, I.; Teixidor, F.; Viñas, C. Icosahedral boron clusters: A perfect tool for the enhancement of polymer features. Chem. Soc. Rev. 2016, 45, 5147–5173. [Google Scholar] [CrossRef] [Green Version]
- Olid, D.; Nunez, R.; Vinas, C.; Teixidor, F. Methods to produce B–C, B–P, B–N and B–S bonds in boron clusters. Chem. Soc. Rev. 2013, 42, 3318–3336. [Google Scholar] [CrossRef] [PubMed]
- Hosmane, N.S. Boron Science: New Technologies and Applications; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Grimes, R.N. Carboranes; Academic Press: London, UK, 2016. [Google Scholar]
- Ferrari, P.; Vanbuel, J.; Hansen, K.; Lievens, P.; Janssens, E.; Fielicke, A. Effect of radiative cooling on the size-dependent stability of small boron clusters. Phys. Rev. A 2018, 98, 012501. [Google Scholar] [CrossRef] [Green Version]
- Wade, K. Skeletal Electron Counting in Cluster and Ring Compounds. Nat. Phys. Sci. 1972, 240, 71. [Google Scholar] [CrossRef]
- Olah, G.A. 100 Years of Carbocations and Their Significance in Chemistry1. J. Org. Chem. 2001, 66, 5943–5957. [Google Scholar] [CrossRef] [PubMed]
- Olah, G.A.; Wade, K.; Williams, R.E.; Lipscomb, W.N. Electron Deficient Boron and Carbon Clusters; Wiley: Hoboken, NJ, USA, 1991. [Google Scholar]
- Welch, A.J. The significance and impact of Wade’s rules. Chem. Commun. 2013, 49, 3615–3616. [Google Scholar] [CrossRef] [PubMed]
- Heying, T.; Ager, J., Jr.; Clark, S.; Mangold, D.; Goldstein, H.; Hillman, M.; Polak, R.; Szymanski, J. A new series of organoboranes. I. Carboranes from the reaction of decaborane with acetylenic compounds. Inorg. Chem. 1963, 2, 1089–1092. [Google Scholar] [CrossRef]
- Poater, J.; Solà, M.; Viñas, C.; Teixidor, F. π Aromaticity and Three—Dimensional Aromaticity: Two sides of the Same Coin? Angew. Chem. Int. Ed. 2014, 53, 12191–12195. [Google Scholar] [CrossRef]
- Lo, R.; Fanfrlík, J.; Lepšík, M.; Hobza, P. The properties of substituted 3D-aromatic neutral carboranes: The potential for σ-hole bonding. Phys. Chem. Chem. Phys. 2015, 17, 20814–20821. [Google Scholar] [CrossRef]
- Li, L.; Li, J.; Shi, Y.; Du, P.; Zhang, Z.; Liu, T.; Zhang, R.; Liu, Z. On-Demand Biodegradable Boron Nitride Nanoparticles for Treating Triple Negative Breast Cancer with Boron Neutron Capture Therapy. ACS Nano 2019, 13, 13843–13852. [Google Scholar] [CrossRef]
- Goszczyński, T.M.; Kowalski, K.; Leśnikowski, Z.J.; Boratyński, J. Solid state, thermal synthesis of site-specific protein–boron cluster conjugates and their physicochemical and biochemical properties. Biochim. Biophys. Acta (BBA) Gen. Subj. 2015, 1850, 411–418. [Google Scholar] [CrossRef]
- Assaf, K.I.; Wilińska, J.; Gabel, D. Ionic Boron Clusters as Superchaotropic Anions: Implications for Drug Design. In Boron-Based Compounds: Potential and Emerging Applications in Medicine; Wiley: Hoboken, NJ, USA, 2018; p. 109. [Google Scholar]
- Ban, H.S.; Shimizu, K.; Minegishi, H.; Nakamura, H. Identification of HSP60 as a Primary Target of o-Carboranylphenoxyacetanilide, an HIF-1α Inhibitor. J. Am. Chem. Soc. 2010, 132, 11870–11871. [Google Scholar] [CrossRef] [PubMed]
- Schaffran, T.; Li, J.; Karlsson, G.; Edwards, K.; Winterhalter, M.; Gabel, D. Interaction of N, N, N-trialkylammonioundecahydro-closo-dodecaborates with dipalmitoyl phosphatidylcholine liposomes. Chem. Phys. Lipids 2010, 163, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Schaffran, T.; Justus, E.; Elfert, M.; Chen, T.; Gabel, D. Toxicity of N, N, N-trialkylammoniododecaborates as new anions of ionic liquids in cellular, liposomal and enzymatic test systems. Green Chem. 2009, 11, 1458–1464. [Google Scholar] [CrossRef]
- Genady, A.R.; Ioppolo, J.A.; Azaam, M.M.; Mohamed, E. New functionalized mercaptoundecahydrododecaborate derivatives for potential application in boron neutron capture therapy: Synthesis, characterization and dynamic visualization in cells. Eur. J. Med. Chem. 2015, 93, 574–583. [Google Scholar] [CrossRef]
- Tiwari, R.; Mahasenan, K.; Pavlovicz, R.; Li, C.; Tjarks, W. Carborane clusters in computational drug design: A comparative docking evaluation using AutoDock, FlexX, Glide, and Surflex. J. Chem. Inf. Model. 2009, 49, 1581–1589. [Google Scholar] [CrossRef] [Green Version]
- Calvaresi, M.; Zerbetto, F. In silico carborane docking to proteins and potential drug targets. J. Chem. Inf. Model. 2011, 51, 1882–1896. [Google Scholar] [CrossRef]
- Scholz, M.; Blobaum, A.L.; Marnett, L.J.; Hey-Hawkins, E. Synthesis and evaluation of carbaborane derivatives of indomethacin as cyclooxygenase inhibitors. Bioorg. Med. Chem. 2011, 19, 3242–3248. [Google Scholar] [CrossRef] [Green Version]
- Lee Jr, M.W.; Sevryugina, Y.V.; Khan, A.; Ye, S.Q. Carboranes increase the potency of small molecule inhibitors of nicotinamide phosphoribosyltranferase. J. Med. Chem. 2012, 55, 7290–7294. [Google Scholar]
- Sivaev, I.B.; Bregadze, V.I.; Sjöberg, S. Chemistry of closo-dodecaborate anion [B12H12]2−: A review. Collect. Czechoslov. Chem. Commun. 2002, 67, 679–727. [Google Scholar] [CrossRef]
- Sivaev, I.B.; Bregadze, V.V. Polyhedral boranes for medical applications: Current status and perspectives. Eur. J. Inorg. Chem. 2009, 2009, 1433–1450. [Google Scholar] [CrossRef]
- Kaim, W.; Hosmane, N.S.; Záliš, S.; Maguire, J.A.; Lipscomb, W.N. Boron Atoms as Spin Carriers in Two-and Three-Dimensional Systems. Angew. Chem. Int. Ed. 2009, 48, 5082–5091. [Google Scholar] [CrossRef] [PubMed]
- Hiratsuka, J.; Kamitani, N.; Tanaka, R.; Yoden, E.; Tokiya, R.; Suzuki, M.; Barth, R.F.; Ono, K. Boron neutron capture therapy for vulvar melanoma and genital extramammary Paget’s disease with curative responses. Cancer Commun. 2018, 38, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, A.; Kim, B.K.; Mackeyev, Y.; Rohani, P.; Mahajan, S.D.; Swihart, M.T.; Krishnan, S.; Prasad, P.N. Boron-Nanoparticle-Loaded Folic-Acid-Functionalized Liposomes to Achieve Optimum Boron Concentration for Boron Neutron Capture Therapy of Cancer. J. Biomed. Nanotechnol. 2019, 15, 1714–1723. [Google Scholar] [CrossRef] [PubMed]
- Sköld, K.; Stenstam, H.B.; Diaz, A.; Giusti, V.; Pellettieri, L.; Hopewell, J. Boron Neutron Capture Therapy for glioblastoma multiforme: Advantage of prolonged infusion of BPA-f. Acta Neurol. Scand. 2010, 122, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Hopewell, J.; Gorlia, T.; Pellettieri, L.; Giusti, V.; Stenstam, H.B.; Sköld, K. Boron neutron capture therapy for newly diagnosed glioblastoma multiforme: An assessment of clinical potential. Appl. Radiat. Isot. 2011, 69, 1737–1740. [Google Scholar] [CrossRef]
- Grimes, R. Carboranes in medicine. In Carboranes, 3rd ed.; Grimes, R.N., Ed.; Academic Press: Cambridge, MA, USA, 2016; pp. 945–984. [Google Scholar]
- Luderer, M.J. Development of Novel Tumor-Targeted Compounds for Boron Neutron Capture Therapy. Ph.D. Thesis, Washington University in St. Louis, St. Louis, MO, USA, 2019. Available online: https://openscholarship.wustl.edu/art_sci_etds/1782/ (accessed on 20 January 2020).
- Tani, H.; Kurihara, H.; Hiroi, K.; Honda, N.; Yoshimoto, M.; Kono, Y.; Murakami, R.; Kumita, S.; Arai, Y.; Itami, J. Correlation of 18F-BPA and 18F-FDG uptake in head and neck cancers. Radiother. Oncol. 2014, 113, 193–197. [Google Scholar] [CrossRef]
- Ishiwata, K. 4-Borono-2-18 F-fluoro-l-phenylalanine PET for boron neutron capture therapy-oriented diagnosis: Overview of a quarter century of research. Ann. Nucl. Med. 2019, 33, 223–236. [Google Scholar] [CrossRef]
- Evangelista, L.; Jori, G.; Martini, D.; Sotti, G. Boron neutron capture therapy and 18F-labelled borophenylalanine positron emission tomography: A critical and clinical overview of theliterature. Appl. Radiat. Isot. 2013, 74, 91–101. [Google Scholar] [CrossRef]
- Gao, S.; Zhu, Y.; Hosmane, N. Nanostructured Boron Compounds for Boron Neutron Capture Therapy (BNCT) in Cancer Treatment. In Boron-Based Compounds: Potential and Emerging Applications in Medicine, 1st ed.; John Wiley & Sons: Hoboken, NJ, USA, 2018; pp. 371–388. [Google Scholar]
- Shikata, F.; Tokumitsu, H.; Ichikawa, H.; Fukumori, Y. In vitro cellular accumulation of gadolinium incorporated into chitosan nanoparticles designed for neutron-capture therapy of cancer. Eur. J. Pharm. Biopharm. 2002, 53, 57–63. [Google Scholar] [CrossRef]
- Soenen, S.J.; Montenegro, J.-M.; Abdelmonem, A.M.; Manshian, B.B.; Doak, S.H.; Parak, W.J.; De Smedt, S.C.; Braeckmans, K. The effect of nanoparticle degradation on poly (methacrylic acid)-coated quantum dot toxicity: The importance of particle functionality assessment in toxicology. Acta Biomater. 2014, 10, 732–741. [Google Scholar] [CrossRef] [Green Version]
- Gu, L.; Fang, R.H.; Sailor, M.J.; Park, J.-H. In vivo clearance and toxicity of monodisperse iron oxide nanocrystals. ACS Nano 2012, 6, 4947–4954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.-H.; Gu, L.; Von Maltzahn, G.; Ruoslahti, E.; Bhatia, S.N.; Sailor, M.J. Biodegradable luminescent porous silicon nanoparticles for in vivo applications. Nat. Mater. 2009, 8, 331. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Jin, X.; Cong, Y.; Liu, Y.; Fu, J. Degradable natural polymer hydrogels for articular cartilage tissue engineering. J. Chem. Technol. Biotechnol. 2013, 88, 327–339. [Google Scholar] [CrossRef]
- Justin, R.; Chen, B. Characterisation and drug release performance of biodegradable chitosan–graphene oxide nanocomposites. Carbohydr. Polym. 2014, 103, 70–80. [Google Scholar] [CrossRef]
- Chen, Q.; Feng, L.; Liu, J.; Zhu, W.; Dong, Z.; Wu, Y.; Liu, Z. Intelligent Albumin–MnO2 Nanoparticles as pH-/H2O2-Responsive Dissociable Nanocarriers to Modulate Tumor Hypoxia for Effective Combination Therapy. Adv. Mater. 2016, 28, 7129–7136. [Google Scholar] [CrossRef]
- Tu, Y.; Peng, F.; André, A.A.; Men, Y.; Srinivas, M.; Wilson, D.A. Biodegradable hybrid stomatocyte nanomotors for drug delivery. ACS Nano 2017, 11, 1957–1963. [Google Scholar] [CrossRef] [Green Version]
- Clapper, J.D.; Guymon, C.A. Nanostructured biodegradable polymer composites generated using lyotropic liquid crystalline media. Macromolecules 2007, 40, 7951–7959. [Google Scholar] [CrossRef]
- Song, J.; Pu, L.; Zhou, J.; Duan, B.; Duan, H. Biodegradable theranostic plasmonic vesicles of amphiphilic gold nanorods. ACS Nano 2013, 7, 9947–9960. [Google Scholar] [CrossRef]
- Steinbach, T.; Wurm, F.R. Poly (phosphoester) s: A new platform for degradable polymers. Angew. Chem. Int. Ed. 2015, 54, 6098–6108. [Google Scholar] [CrossRef]
- Di Meo, C.; Panza, L.; Capitani, D.; Mannina, L.; Banzato, A.; Rondina, M.; Renier, D.; Rosato, A.; Crescenzi, V. Hyaluronan as carrier of carboranes for tumor targeting in boron neutron capture therapy. Biomacromolecules 2007, 8, 552–559. [Google Scholar] [CrossRef]
- Sumitani, S.; Nagasaki, Y. Boron neutron capture therapy assisted by boron-conjugated nanoparticles. Polym. J. 2012, 44, 522. [Google Scholar] [CrossRef] [Green Version]
- Takeuchi, I.; Nomura, K.; Makino, K. Hydrophobic boron compound-loaded poly (l-lactide-co-glycolide) nanoparticles for boron neutron capture therapy. Colloids Surf. B Biointerfaces 2017, 159, 360–365. [Google Scholar] [CrossRef]
- Cai, W.; Wang, J.; Chu, C.; Chen, W.; Wu, C.; Liu, G. Metal–Organic Framework—Based Stimuli—Responsive Systems for Drug Delivery. Adv. Sci. 2019, 6, 1801526. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Wang, X.; Jin, S.; Muhammad, N.; Guo, Z. Stimuli-responsive therapeutic metallodrugs. Chem. Rev. 2018, 119, 1138–1192. [Google Scholar] [CrossRef]
- Blum, A.P.; Kammeyer, J.K.; Rush, A.M.; Callmann, C.E.; Hahn, M.E.; Gianneschi, N.C. Stimuli-responsive nanomaterials for biomedical applications. J. Am. Chem. Soc. 2015, 137, 2140–2154. [Google Scholar] [CrossRef] [Green Version]
- Yuan, T.Z.; Xie, S.Q.; Qian, C.N. Boron neutron capture therapy of cancer: Critical issues and future prospects. Thorac. Cancer 2019, 10, 2195. [Google Scholar] [CrossRef]
- Si, P.; Zhang, M.; You, C.; Geng, D.; Du, J.; Zhao, X.; Ma, X.; Zhang, Z. Amorphous boron nanoparticles and BN encapsulating boron nano-peanuts prepared by arc-decomposing diborane and nitriding. J. Mater. Sci. 2003, 38, 689–692. [Google Scholar] [CrossRef]
- Bellott, B.J.; Noh, W.; Nuzzo, R.G.; Girolami, G.S. Nanoenergetic materials: Boron nanoparticles from the pyrolysis of decaborane and their functionalisation. Chem. Commun. 2009, 3214–3215. [Google Scholar] [CrossRef]
- He, X.; Joo, S.; Xiao, H.; Liang, H. Boron-based nanoparticles for chemical-mechanical polishing of copper films. ECS J. Solid State Sci. Technol. 2013, 2, P20–P25. [Google Scholar] [CrossRef]
- Icten, O.; Hosmane, N.S.; Kose, D.A.; Zumreoglu-Karan, B. Production of Magnetic Nano-bioconjugates via Ball Milling of Commercial Boron Powder with Biomolecules. Z. Anorg. Allg. Chem. 2016, 642, 828–832. [Google Scholar] [CrossRef]
- Icten, O.; Hosmane, N.S.; Kose, D.A.; Zumreoglu-Karan, B. Magnetic nanocomposites of boron and vitamin C. New J. Chem. 2017, 41, 3646–3652. [Google Scholar] [CrossRef]
- Kaur, M.; Singh, P.; Singh, K.; Gaharwar, U.S.; Meena, R.; Kumar, M.; Nakagawa, F.; Wu, S.; Suzuki, M.; Nakamura, H. Boron nitride (10BN) a prospective material for treatment of cancer by boron neutron capture therapy (BNCT). Mater. Lett. 2020, 259, 126832. [Google Scholar] [CrossRef]
- Nakamura, H.; Koganei, H.; Miyoshi, T.; Sakurai, Y.; Ono, K.; Suzuki, M. Antitumor effect of boron nitride nanotubes in combination with thermal neutron irradiation on BNCT. Bioorg. Med. Chem. Lett. 2015, 25, 172–174. [Google Scholar] [CrossRef]
- Zhi, C.; Bando, Y.; Tang, C.; Xie, R.; Sekiguchi, T.; Golberg, D. Perfectly dissolved boron nitride nanotubes due to polymer wrapping. J. Am. Chem. Soc. 2005, 127, 15996–15997. [Google Scholar] [CrossRef]
- Wang, W.; Bando, Y.; Zhi, C.; Fu, W.; Wang, E.; Golberg, D. Aqueous noncovalent functionalization and controlled near-surface carbon doping of multiwalled boron nitride nanotubes. J. Am. Chem. Soc. 2008, 130, 8144–8145. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Wu, P.; Rousseas, M.; Okawa, D.; Gartner, Z.; Zettl, A.; Bertozzi, C.R. Boron nitride nanotubes are noncytotoxic and can be functionalized for interaction with proteins and cells. J. Am. Chem. Soc. 2009, 131, 890–891. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Chen, Y.; Elliman, R.G.; Petravic, M. Isotopically enriched 10BN nanotubes. Adv. Mater. 2006, 18, 2157–2160. [Google Scholar] [CrossRef]
- Menichetti, L.; De Marchi, D.; Calucci, L.; Ciofani, G.; Menciassi, A.; Forte, C. Boron nitride nanotubes for boron neutron capture therapy as contrast agents in magnetic resonance imaging at 3 T. Appl. Radiat. Isot. 2011, 69, 1725–1727. [Google Scholar] [CrossRef]
- Yinghuai, Z.; Hosmane, N.S. Applications and perspectives of boron-enriched nanocomposites in cancer therapy. Future Med. Chem. 2013, 5, 705–714. [Google Scholar] [CrossRef]
- Ciofani, G.; Raffa, V.; Menciassi, A.; Cuschieri, A. Folate functionalized boron nitride nanotubes and their selective uptake by glioblastoma multiforme cells: Implications for their use as boron carriers in clinical boron neutron capture therapy. Nanoscale Res. Lett. 2009, 4, 113. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Xie, X.; Wu, T.; Yang, H.; Peng, Y.; Luo, L.; Chen, Y. Targeted delivery of Auristatin PE to Hep G2 cells using folate-conjugated boron nitride nanotubes. Mater. Sci. Eng: C 2019, 109, 110509. [Google Scholar] [CrossRef]
- Ribeiro, H.; Luciano, M.A.; Paula Von Randow, C.; Vilela, D.N.; Andrade, L.M. Functionalized Boron Nitride Applications in Biotechnology. In Recent Advances in Boron-Containing Materials; Intech Open: London, UK, 2019. [Google Scholar]
- Vickers, N.J. Animal Communication: When I’m Calling You, Will You Answer Too? Curr. Biol. 2017, 27, R713–R715. [Google Scholar] [CrossRef]
- Wu, C.-Y.; Lin, J.-J.; Chang, W.-Y.; Hsieh, C.-Y.; Wu, C.-C.; Chen, H.-S.; Hsu, H.-J.; Yang, A.-S.; Hsu, M.-H.; Kuo, W.-Y. Development of theranostic active-targeting boron-containing gold nanoparticles for boron neutron capture therapy (BNCT). Colloids Surf. B Biointerfaces 2019, 183, 110387. [Google Scholar] [CrossRef]
- Wang, J.; Chen, L.; Ye, J.; Li, Z.; Jiang, H.; Yan, H.; Stogniy, M.Y.; Sivaev, I.B.; Bregadze, V.I.; Wang, X. Carborane derivative conjugated with gold nanoclusters for targeted cancer cell imaging. Biomacromolecules 2017, 18, 1466–1472. [Google Scholar] [CrossRef]
- Stogniy, M.Y.; Sivaev, I.B.; Godovikov, I.A.; Starikova, Z.A.; Bregadze, V.I.; Qi, S. Synthesis of new ω-amino-and ω-azidoalkyl carboranes. New J. Chem. 2013, 37, 3865–3868. [Google Scholar] [CrossRef]
- Zhou, C.; Sun, C.; Yu, M.; Qin, Y.; Wang, J.; Kim, M.; Zheng, J. Luminescent gold nanoparticles with mixed valence states generated from dissociation of polymeric Au (I) thiolates. J. Phys. Chem. C 2010, 114, 7727–7732. [Google Scholar] [CrossRef] [Green Version]
- Pulagam, K.R.; Gona, K.B.; Gómez-Vallejo, V.; Meijer, J.; Zilberfain, C.; Estrela-Lopis, I.; Baz, Z.; Cossío, U.; Llop, J. Gold Nanoparticles as Boron Carriers for Boron Neutron Capture Therapy: Synthesis, Radiolabelling and In Vivo Evaluation. Molecules 2019, 24, 3609. [Google Scholar] [CrossRef] [Green Version]
- Timonen, J.M. Amino Acids in Boron Neutron Capture Therapy—Prospects for Precise Treatment of Malignant Brain Tumors. Gen. Chem. 2019, 5, 190024. [Google Scholar]
- Li, J.; Shi, Y.; Zhang, Z.; Liu, H.; Lang, L.; Liu, T.; Chen, X.; Liu, Z. A Metabolically stable boron-derived tyrosine serves as a theranostic agent for positron emission tomography guided boron neutron capture therapy. Bioconj. Chem. 2019, 30, 2870–2878. [Google Scholar] [CrossRef]
- Chauhan, N.; Hosmane, N.; Mozafari, M. Boron-based polymers: Opportunities and challenges. Mater. Today Chem. 2019, 14, 100184. [Google Scholar] [CrossRef]
- Ochiai, T.; Tago, S.; Hayashi, M.; Hirota, K.; Kondo, T.; Satomura, K.; Fujishima, A. Boron-doped diamond powder (BDDP)-based polymer composites for dental treatment using flexible pinpoint electrolysis unit. Electrochem. Commun. 2016, 68, 49–53. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Yang, Q.; Liu, M.; Lin, M.; Wang, T.; Zhang, Z.; Zhong, X.; Guo, N.; Lu, Y.; Xu, J. Remarkable Boron Delivery Of iRGD-Modified Polymeric Nanoparticles For Boron Neutron Capture Therapy. Int. J. Nanomed. 2019, 14, 8161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiyanagi, Y.; Sakurai, Y.; Kumada, H.; Tanaka, H. Status of Accelerator-Based BNCT Projects Worldwide; AIP Conference Proceedings; AIP Publishing: Melville, NY, USA, 2019; p. 050012. [Google Scholar]
- Hirose, K.; Konno, A.; Yoshimoto, S.; Ono, K.; Otsuki, N.; Hatazawa, J.; Hiratsuka, J.; Takai, Y. A Prospective Phase 2 Trial of Accelerator-Based Boron Neutron Capture Therapy for Recurrent and Locally Advanced Head and Neck Cancer: Initial Report of Treatment Outcome. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, E374. [Google Scholar] [CrossRef]
- Barth, R.F.; Vicente, M.H.; Harling, O.K.; Kiger, W.; Riley, K.J.; Binns, P.J.; Wagner, F.M.; Suzuki, M.; Aihara, T.; Kato, I. Current status of boron neutron capture therapy of high grade gliomas and recurrent head and neck cancer. Radiat. Oncol. 2012, 7, 146. [Google Scholar] [CrossRef] [Green Version]
- Kankaanranta, L.; Saarilahti, K.; Mäkitie, A.; Välimäki, P.; Tenhunen, M.; Joensuu, H. Boron neutron capture therapy (BNCT) followed by intensity modulated chemoradiotherapy as primary treatment of large head and neck cancer with intracranial involvement. Radiother. Oncol. 2011, 99, 98–99. [Google Scholar] [CrossRef]
- Kankaanranta, L.; Seppälä, T.; Koivunoro, H.; Saarilahti, K.; Atula, T.; Collan, J.; Salli, E.; Kortesniemi, M.; Uusi-Simola, J.; Välimäki, P. Boron neutron capture therapy in the treatment of locally recurred head-and-neck cancer: Final analysis of a phase I/II trial. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e67–e75. [Google Scholar] [CrossRef]
- Haapaniemi, A.; Kankaanranta, L.; Saat, R.; Koivunoro, H.; Saarilahti, K.; Mäkitie, A.; Atula, T.; Joensuu, H. Boron neutron capture therapy in the treatment of recurrent laryngeal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 404–410. [Google Scholar] [CrossRef]
- Wang, L.-W.; Liu, Y.-W.H.; Chou, F.-I.; Jiang, S.-H. Clinical trials for treating recurrent head and neck cancer with boron neutron capture therapy using the Tsing-Hua Open Pool Reactor. Cancer Commun. 2018, 38, 37. [Google Scholar] [CrossRef] [Green Version]
- Yong, Z.; Song, Z.; Zhou, Y.; Liu, T.; Zhang, Z.; Zhao, Y.; Chen, Y.; Jin, C.; Chen, X.; Lu, J. Boron neutron capture therapy for malignant melanoma: First clinical case report in China. Chin. J.Cancer Res. 2016, 28, 634. [Google Scholar] [CrossRef] [Green Version]
- Sorace, A.G.; Korb, M.; Warram, J.M.; Umphrey, H.; Zinn, K.R.; Rosenthal, E.; Hoyt, K. Ultrasound-stimulated drug delivery for treatment of residual disease after incomplete resection of head and neck cancer. Ultrasound Med. Boil. 2014, 40, 755–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.-Y.; Chan, P.-C.; Chou, L.-S.; Chang, C.-W.; Yang, F.-Y.; Liu, R.-S.; Chiou, S.-H.; Chen, Y.-W.; Yen, S.-H.; Wang, H.-E. Pulsed-focused ultrasound enhances boron drug accumulation in a human head and neck cancer xenograft-bearing mouse model. Mol. Imaging Biol. 2014, 16, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Polat, B.E.; Hart, D.; Langer, R.; Blankschtein, D. Ultrasound-mediated transdermal drug delivery: Mechanisms, scope, and emerging trends. J. Control. Release 2011, 152, 330–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Farha, G.; Poon, I.; Karam, I.; Higgins, K.; Pichardo, S.; Hynynen, K.; Enepekides, D. Magnetic resonance-guided high-intensity focused ultrasound combined with radiotherapy for palliation of head and neck cancer—A pilot study. J. Ther. Ultrasound 2016, 4, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.-C.; Chuang, K.-S.; Liu, Y.-W.H.; Lin, T.-Y.; Teng, Y.-C.; Wang, L.-W. A comparison of dose distributions in gross tumor volume between boron neutron capture therapy alone and combined boron neutron capture therapy plus intensity modulation radiation therapy for head and neck cancer. PLoS ONE 2019, 14, e0210626. [Google Scholar] [CrossRef] [PubMed]
- Koivunoro, H.; Kankaanranta, L.; Seppälä, T.; Haapaniemi, A.; Mäkitie, A.; Joensuu, H. Boron neutron capture therapy for locally recurrent head and neck squamous cell carcinoma: An analysis of dose response and survival. Radiother. Oncol. 2019, 137, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y. Boron neutron capture therapy: Moving towards targeted therapy for locally recurrent head and neck squamous cell carcinoma. Mil. Med. Res. 2019, 6, 32. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Chong, Y.; Chen, X.; Jin, C.; Yang, L.; Liu, T. PGNAA system preliminary design and measurement of In-Hospital Neutron Irradiator for boron concentration measurement. Appl. Radiat. Isot. 2015, 106, 161–165. [Google Scholar] [CrossRef]
- Achkar, T.; Tarhini, A.A. The use of immunotherapy in the treatment of melanoma. J. Hematol. Oncol. 2017, 10, 88. [Google Scholar] [CrossRef] [Green Version]
- Yu, Z.; Si, L. Immunotherapy of patients with metastatic melanoma. Chin. Clin. Oncol. 2017, 6, 20. [Google Scholar] [CrossRef]
- Alvarado-Luna, G.; Morales-Espinosa, D. Treatment for small cell lung cancer, where are we now?—A review. Transl. Lung Cancer Res. 2016, 5, 26. [Google Scholar] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.; Geng, C.; Tang, X.; Bortolussi, S.; Han, Y.; Shu, D.; Gong, C.; Zhang, X.; Tian, F. Dosimetric impact of respiratory motion during boron neutron capture therapy for lung cancer. Radiat. Phys. Chem. 2020, 168, 108527. [Google Scholar] [CrossRef]
- Suzuki, M.; Sakurai, Y.; Masunaga, S.; Kinashi, Y.; Nagata, K.; Maruhashi, A.; Ono, K. Feasibility of boron neutron capture therapy (BNCT) for malignant pleural mesothelioma from a viewpoint of dose distribution analysis. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 1584–1589. [Google Scholar] [CrossRef]
- Suzuki, M.; Suzuki, O.; Sakurai, Y.; Tanaka, H.; Kondo, N.; Kinashi, Y.; Masunaga, S.-i.; Maruhashi, A.; Ono, K. In Reirradiation for locally recurrent lung cancer in the chest wall with boron neutron capture therapy (BNCT). Int. Cancer Conf. J. 2012, 1, 235–238. [Google Scholar] [CrossRef]
- Farías, R.O.; Bortolussi, S.; Menéndez, P.R.; González, S.J. Exploring boron neutron capture therapy for non-small cell lung cancer. Phys. Med. 2014, 30, 888–897. [Google Scholar] [CrossRef]
- Zhang, X.; Geng, C.; Tang, X. Assessment of Secondary Cancer Risk for Patients Treated with BNCT. Available online: https://ybnct10.org/wp-content/uploads/2019/09/26.pdf (accessed on 20 January 2020).
- Geng, C.; Tang, X.; Hou, X.; Shu, D.; Chen, D. Development of Chinese hybrid radiation adult phantoms and their application to external dosimetry. Sci. China Technol. Sci. 2014, 57, 713–719. [Google Scholar] [CrossRef]
- Barth, R.F.; Mi, P.; Yang, W. Boron delivery agents for neutron capture therapy of cancer. Cancer Commun. 2018, 38, 35. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Structure of carborane due to the attachment of carbon at different sites.
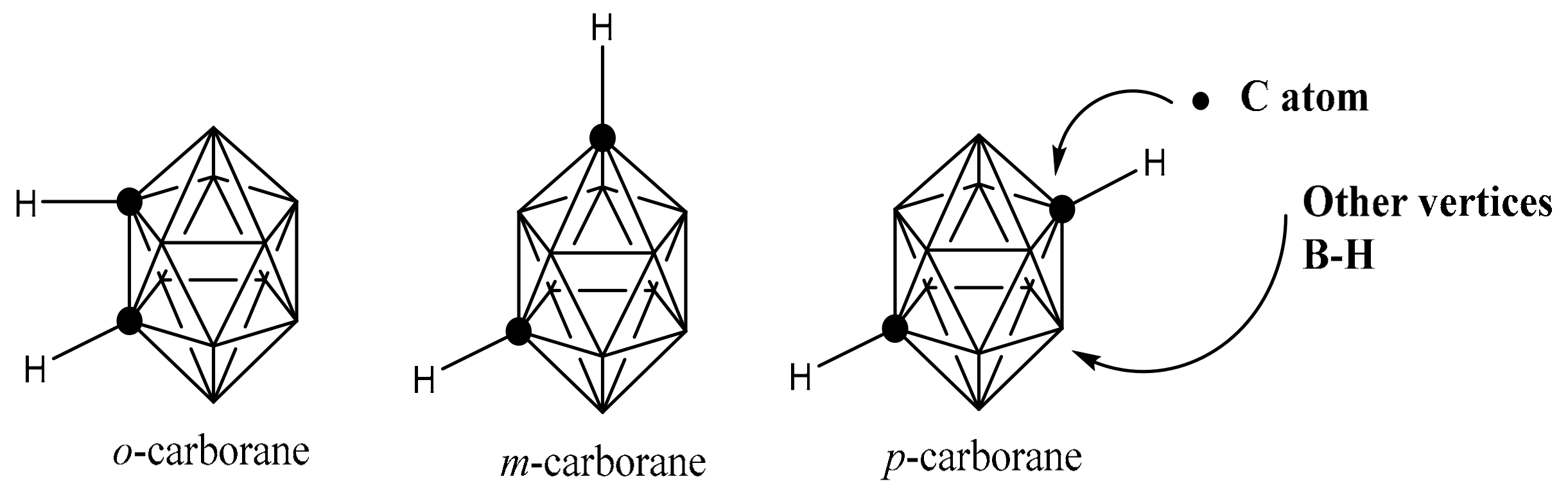
Figure 2.
(a) Graphical depiction of the principle of BNCT, that show how localized boron particles within the tumor can be bombarded with low energy thermal neutrons to produce alpha particles (Reprint from Ref. [61]). (b) BNCT reaction scheme, where the thermal neutrons were bombarded on 10B resulting in a nuclear reaction releasing α particles and 7Li nuclei within a tumor cell, offering a localized lethal effect.
Figure 2.
(a) Graphical depiction of the principle of BNCT, that show how localized boron particles within the tumor can be bombarded with low energy thermal neutrons to produce alpha particles (Reprint from Ref. [61]). (b) BNCT reaction scheme, where the thermal neutrons were bombarded on 10B resulting in a nuclear reaction releasing α particles and 7Li nuclei within a tumor cell, offering a localized lethal effect.
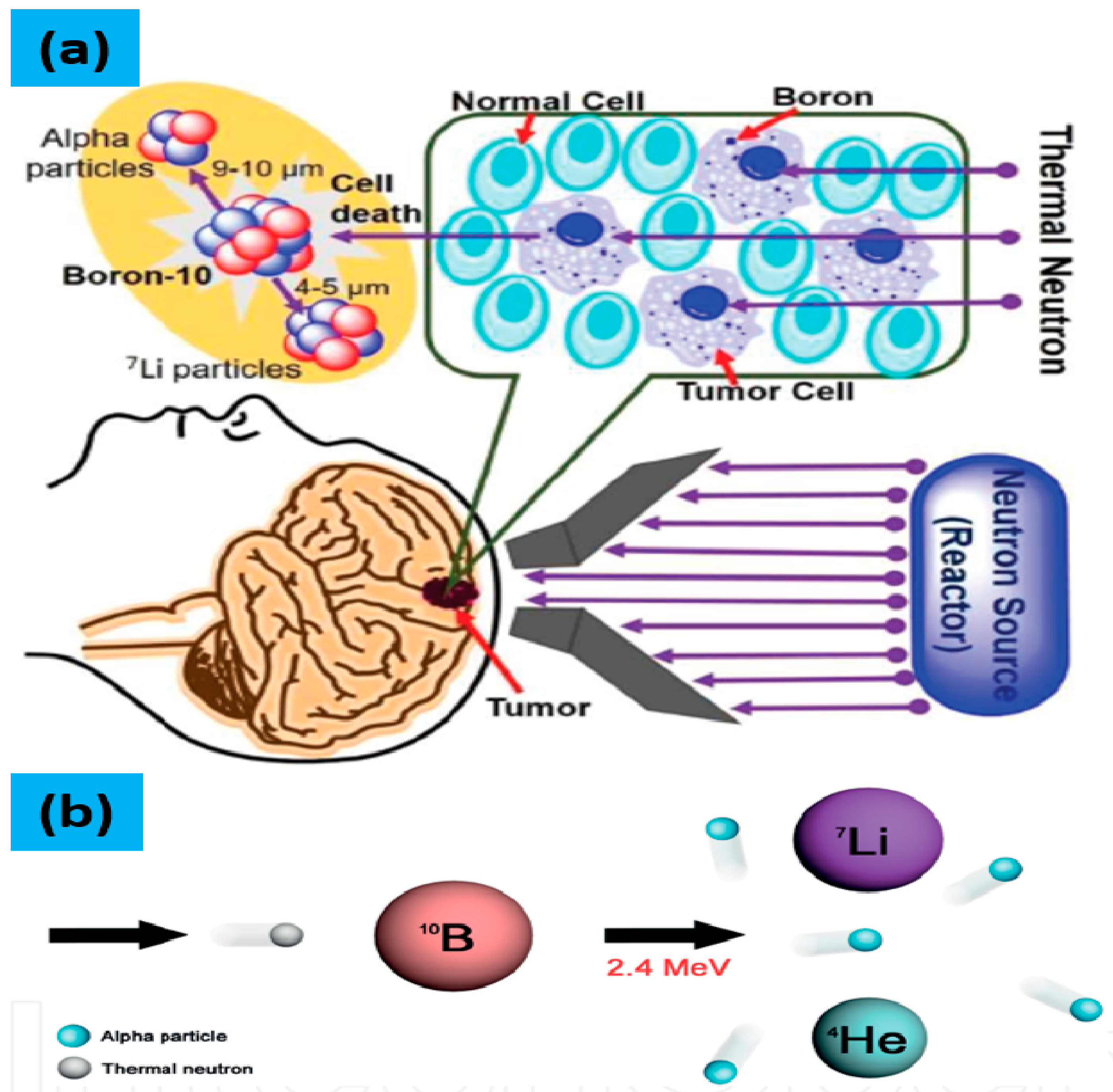
Figure 3.
Structures of BPA, BSH and 18F-BPA.
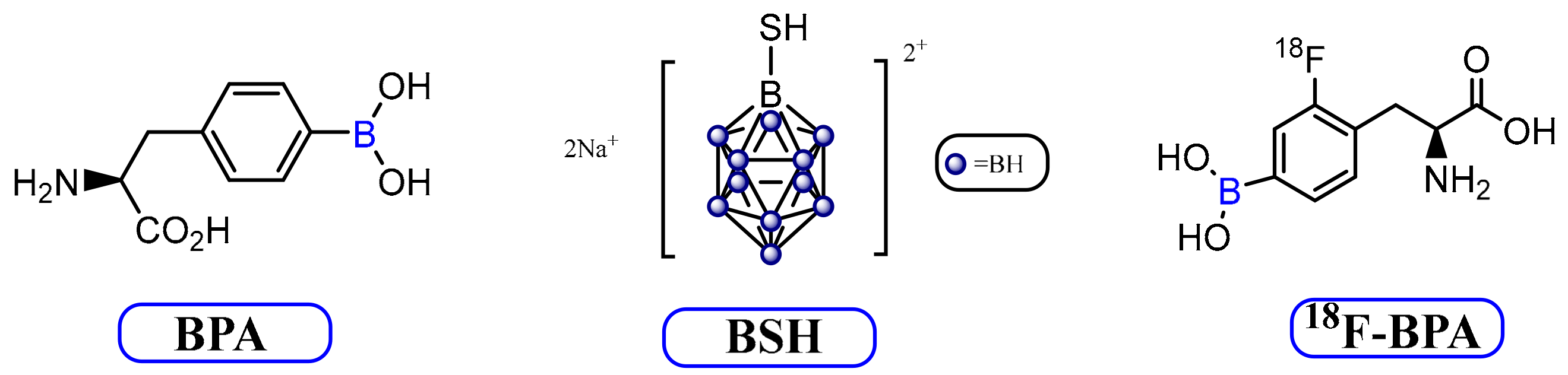
Figure 4.
Schematic image of boron encapsulated liposome (Adopted from Ref. [61]).
Figure 4.
Schematic image of boron encapsulated liposome (Adopted from Ref. [61]).
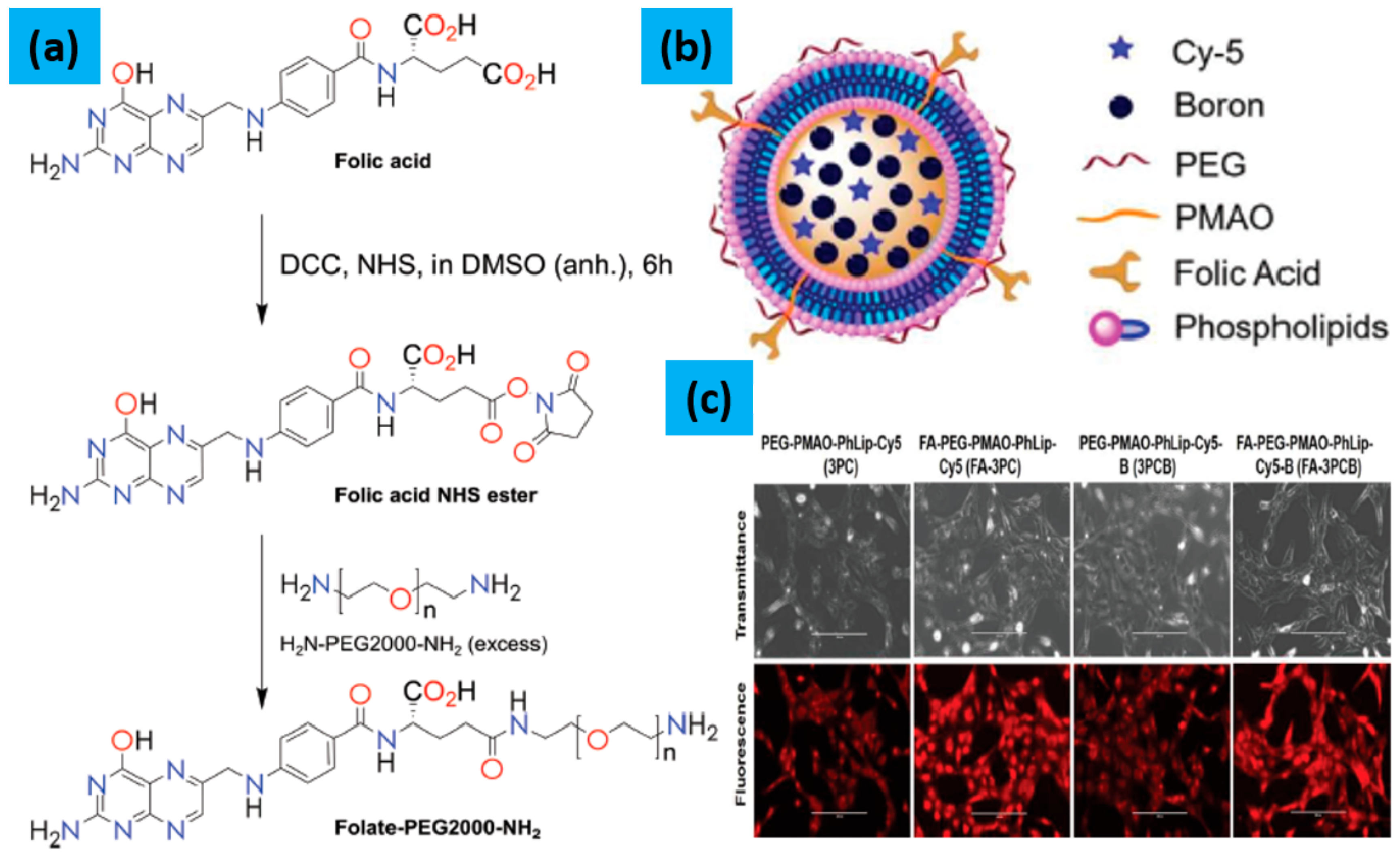
Figure 5.
(a,b) TEM images of BNNTs-OH and BNNTs-FA@PE, respectively (the insert is the enlarged TEM images); (a’,b’) represents the BNNT and the conjugation of FA and PE on the surface of a BNNT, respectively; (c,d) TEM images of Hep G2 cells incubated with BNNTs-FA for 4 h of Low magnification and high-magnification, respectively; (e) the mitochondrial membrane potential (ΔΨ) of control, PE, BNNTs@PE, BNNTs-FA@PE and positive control group, and carbonyl cyanide m-chlorophenylhydrazone was used to conduct positive control (reprint from Ref. [102]).
Figure 5.
(a,b) TEM images of BNNTs-OH and BNNTs-FA@PE, respectively (the insert is the enlarged TEM images); (a’,b’) represents the BNNT and the conjugation of FA and PE on the surface of a BNNT, respectively; (c,d) TEM images of Hep G2 cells incubated with BNNTs-FA for 4 h of Low magnification and high-magnification, respectively; (e) the mitochondrial membrane potential (ΔΨ) of control, PE, BNNTs@PE, BNNTs-FA@PE and positive control group, and carbonyl cyanide m-chlorophenylhydrazone was used to conduct positive control (reprint from Ref. [102]).
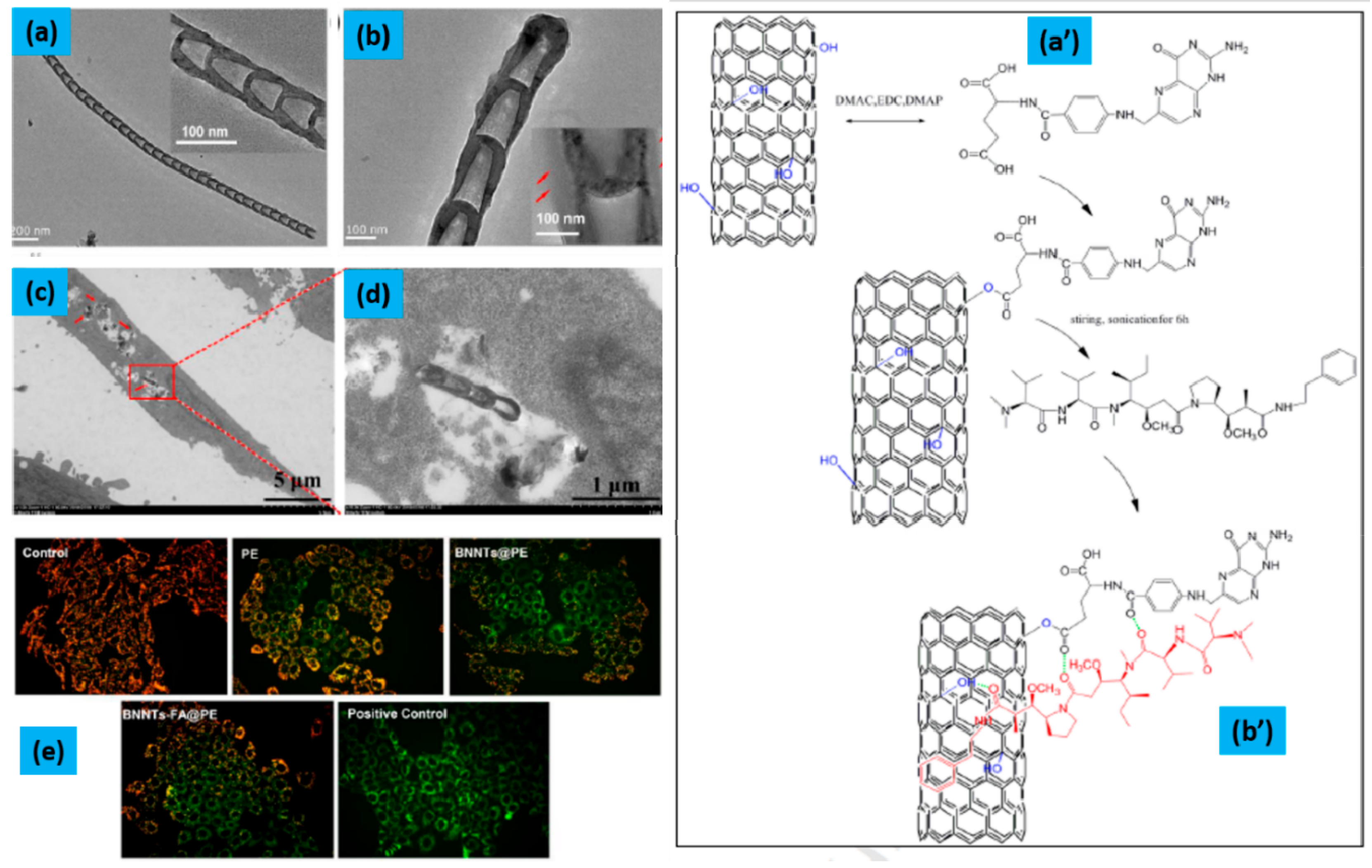
Figure 6.
(a) Schematic representation of the synthesis of the PTL@BNNPs, (b) Illustration of PTL@BNNPs Based BNCT and its degradation (Reprinted from Ref. [46]).
Figure 6.
(a) Schematic representation of the synthesis of the PTL@BNNPs, (b) Illustration of PTL@BNNPs Based BNCT and its degradation (Reprinted from Ref. [46]).
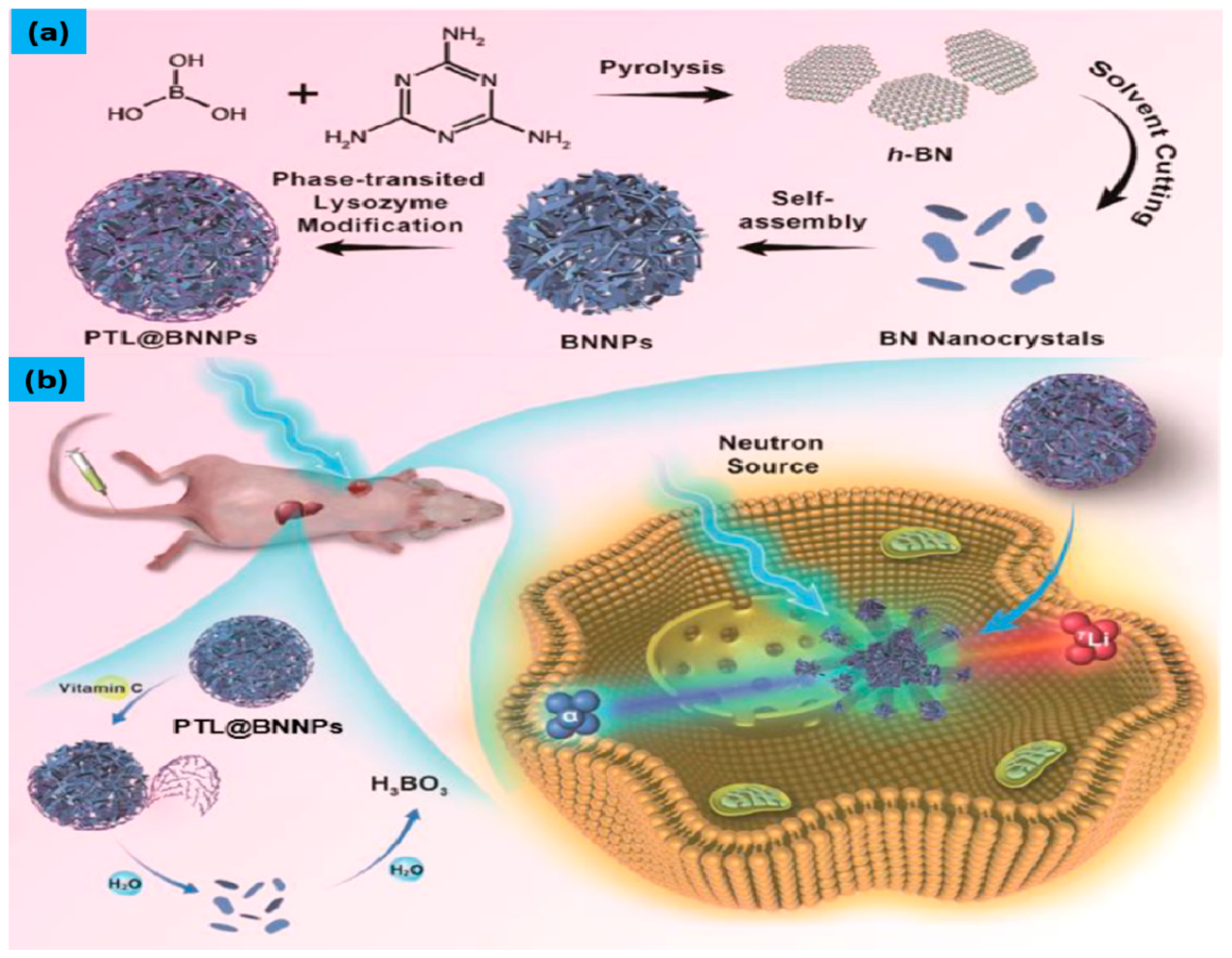
Figure 7.
(A) The synthetic scheme of boron cage-SH (4), (B) The synthetic scheme of B-AuNPs, 123I-B-AuNPs and 123I-61-B-AuNPs.
Figure 7.
(A) The synthetic scheme of boron cage-SH (4), (B) The synthetic scheme of B-AuNPs, 123I-B-AuNPs and 123I-61-B-AuNPs.
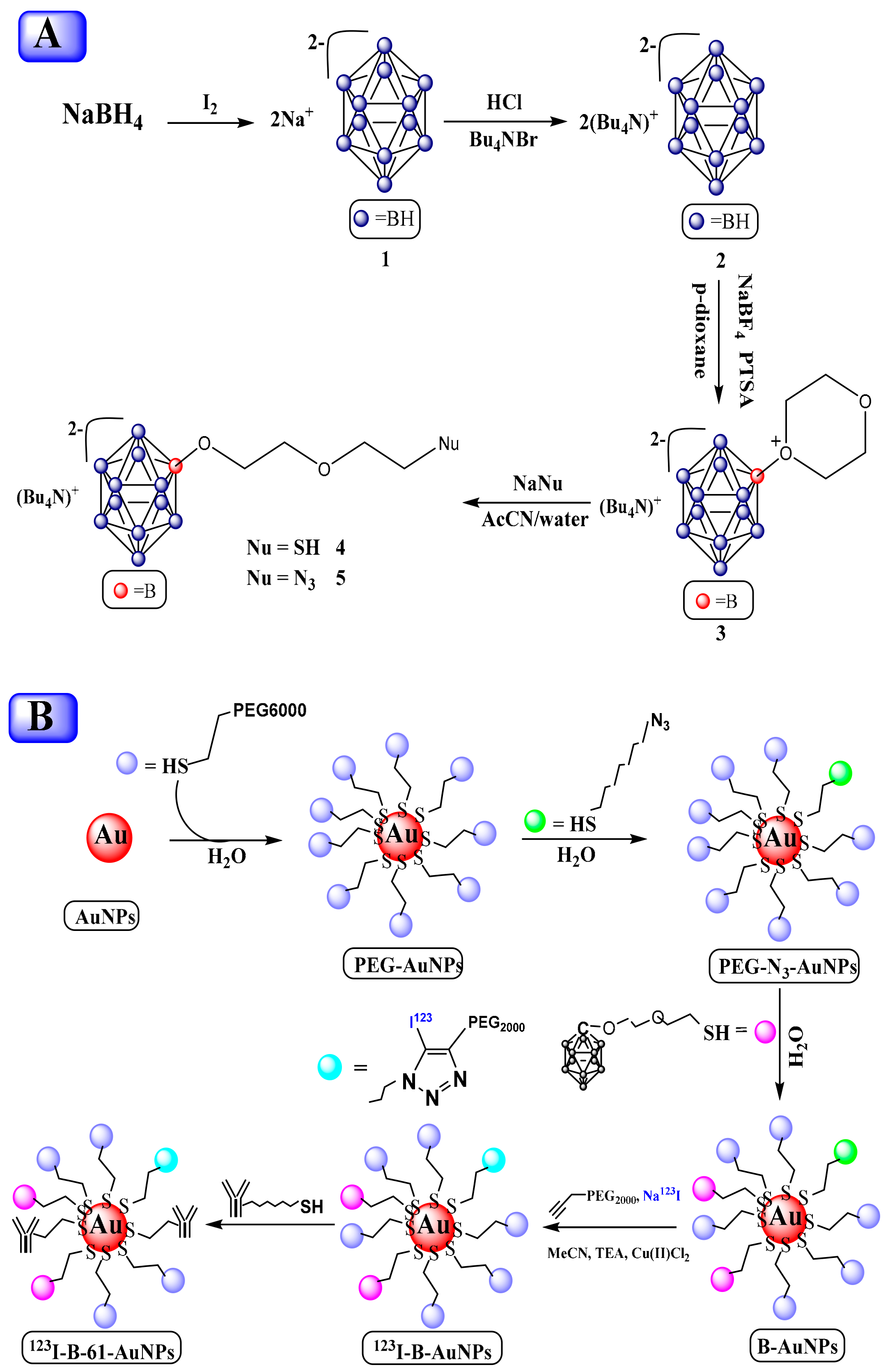
Figure 8.
Illustration of the bioimaging process for cancer cells using gold nanocluster with carborane derivative (reprint from Ref. [106]).
Figure 8.
Illustration of the bioimaging process for cancer cells using gold nanocluster with carborane derivative (reprint from Ref. [106]).
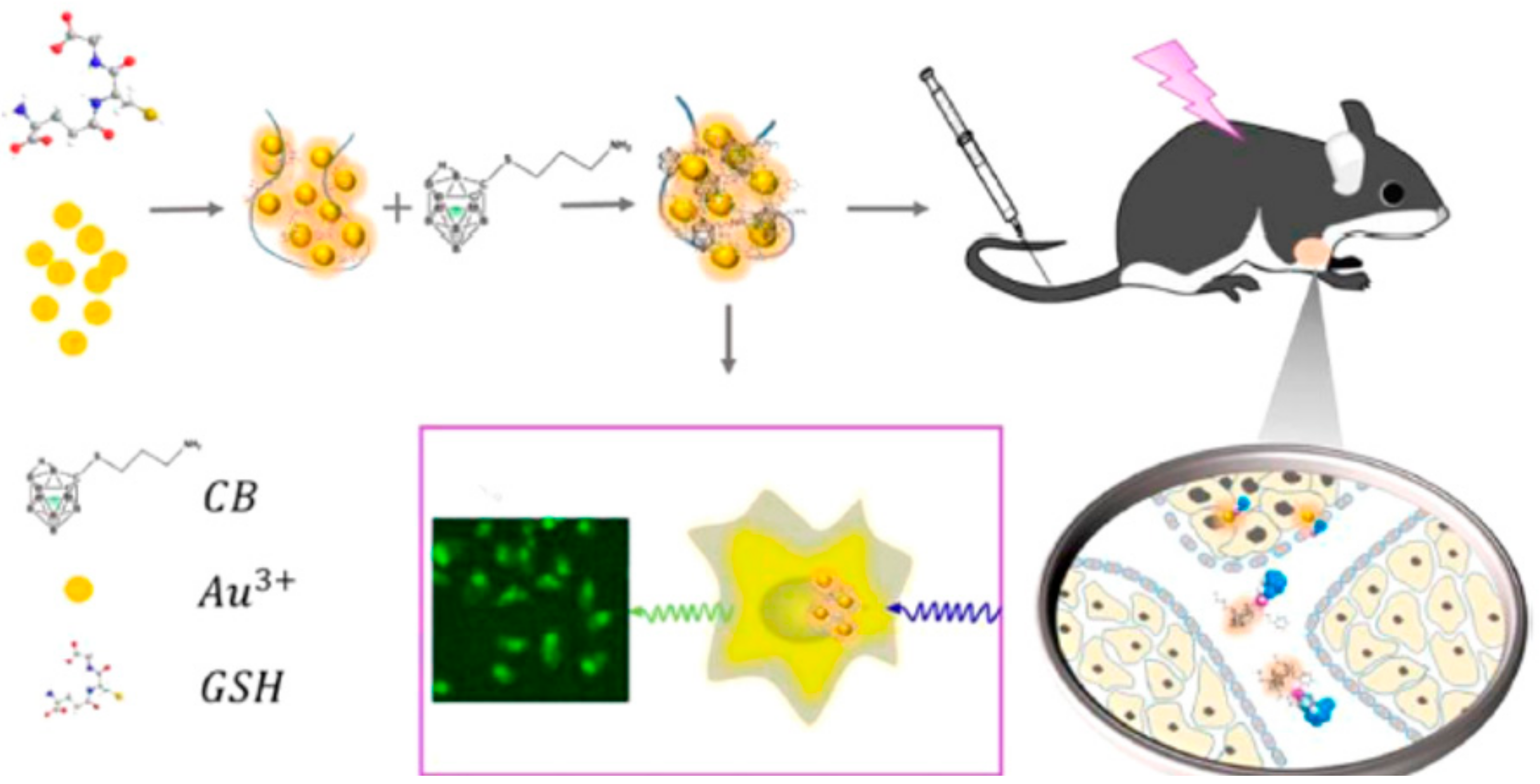
Figure 9.
(a) The schematic presentation of the method reported by Ref. [111]. (b,c) The computational studies of FBY, Tyrosine, and BPA. (d) CT and PET-CT images of the brain, lung tumor and liver retention of [18F]FBY. (e) Correlation between standard uptake value (SUV) of organs and boron concentration of [18F] FBY. (adopted from Ref. [111]).
Figure 9.
(a) The schematic presentation of the method reported by Ref. [111]. (b,c) The computational studies of FBY, Tyrosine, and BPA. (d) CT and PET-CT images of the brain, lung tumor and liver retention of [18F]FBY. (e) Correlation between standard uptake value (SUV) of organs and boron concentration of [18F] FBY. (adopted from Ref. [111]).
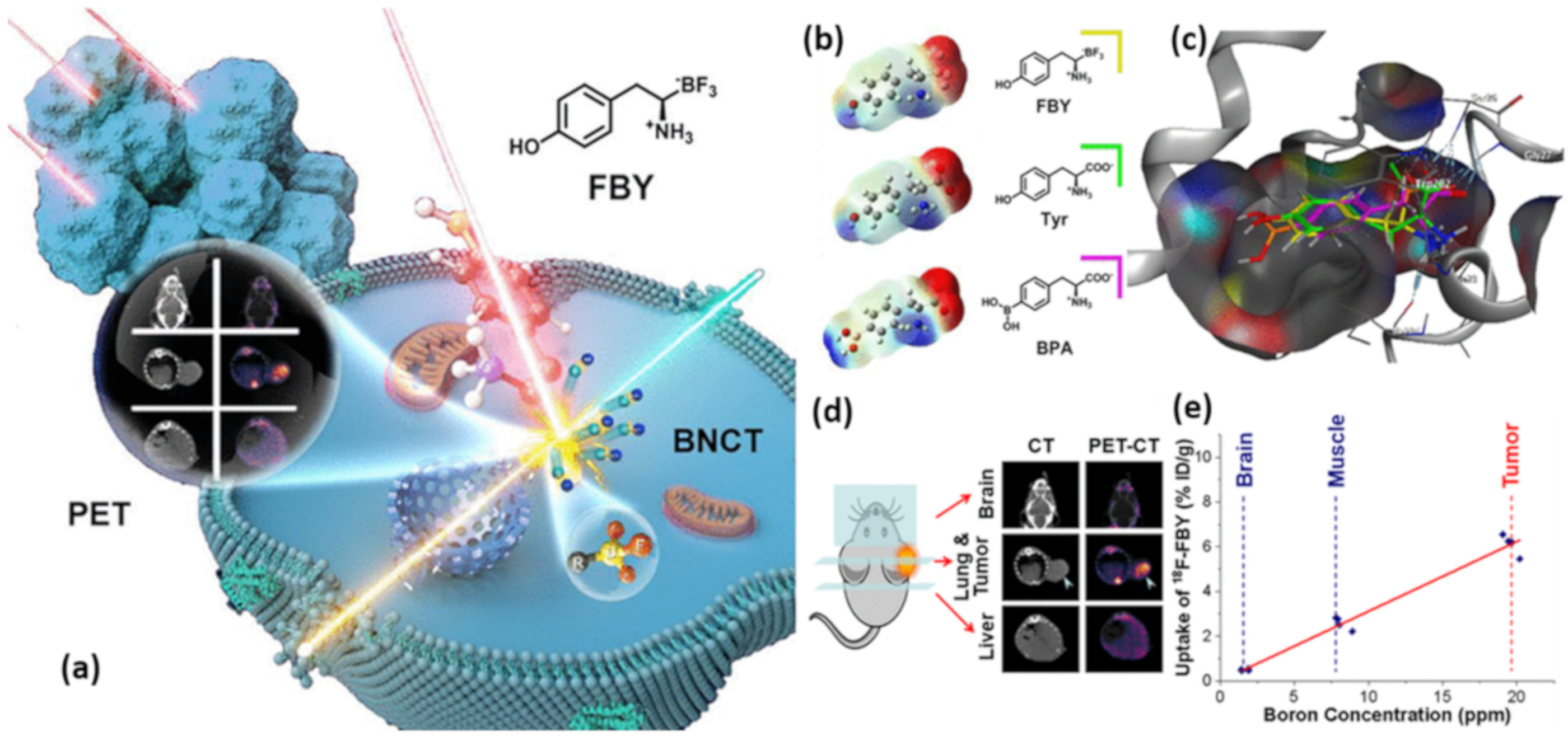
Figure 10.
Gross examination of the skin lesions in the patient’s left foot 2 weeks (A), 5 weeks (B) and 24 months (C) after BNCT; (D) Pathological analysis after BNCT; (E) PET/CT scan after BNCT (reprint from Ref. [122]).
Figure 10.
Gross examination of the skin lesions in the patient’s left foot 2 weeks (A), 5 weeks (B) and 24 months (C) after BNCT; (D) Pathological analysis after BNCT; (E) PET/CT scan after BNCT (reprint from Ref. [122]).
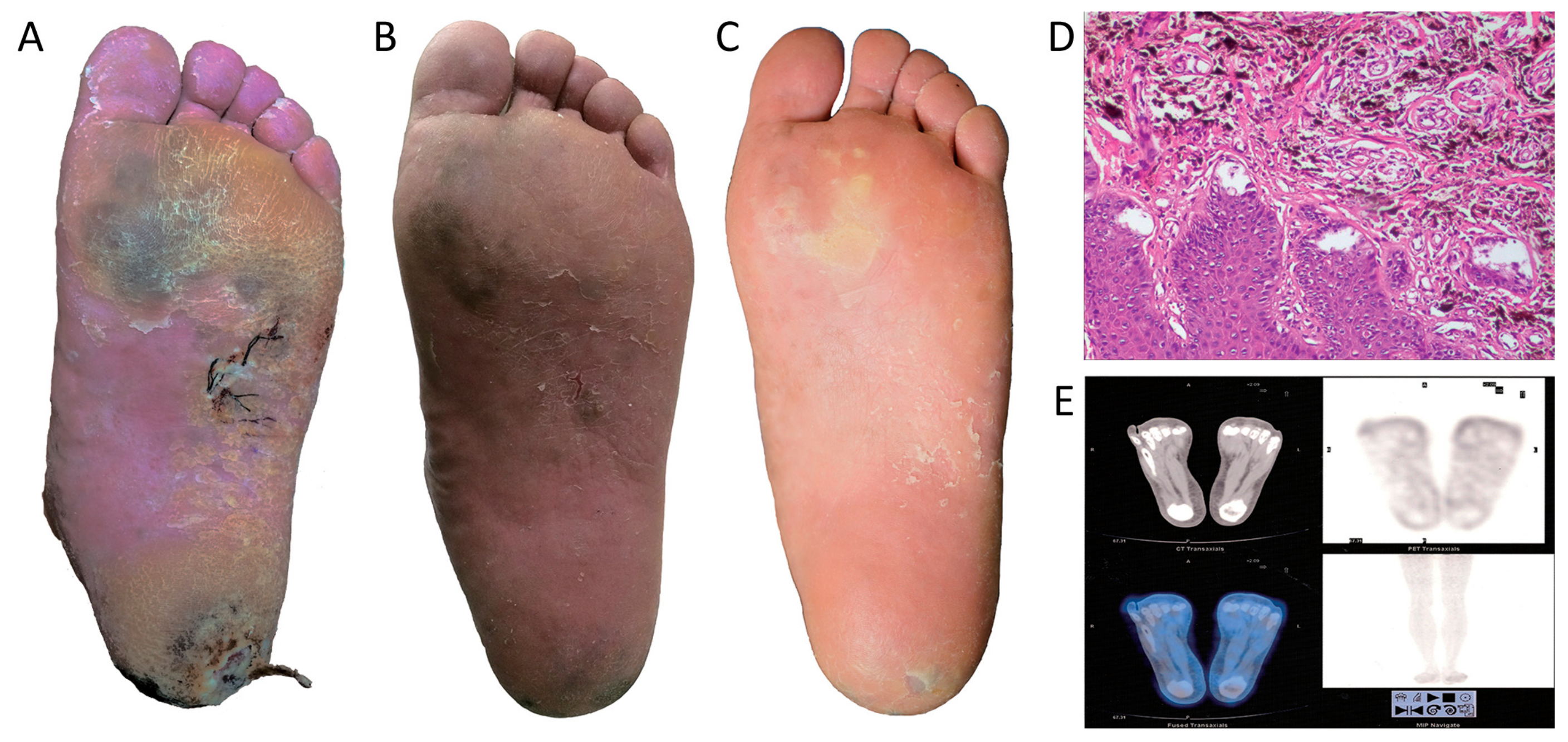

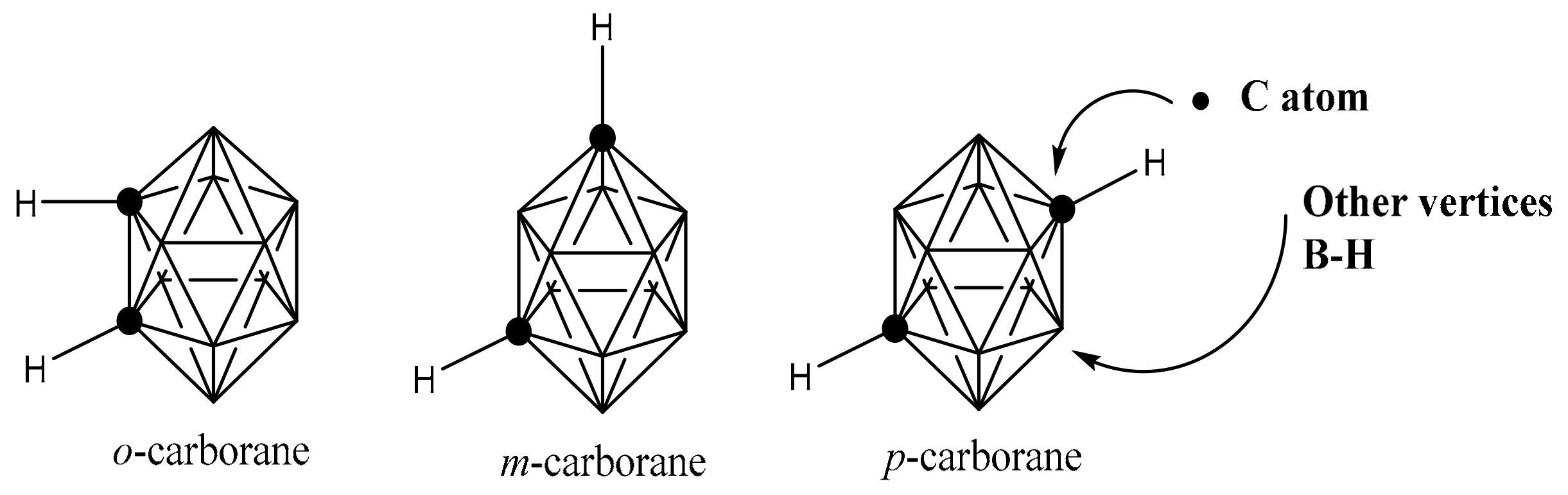{kind=link}
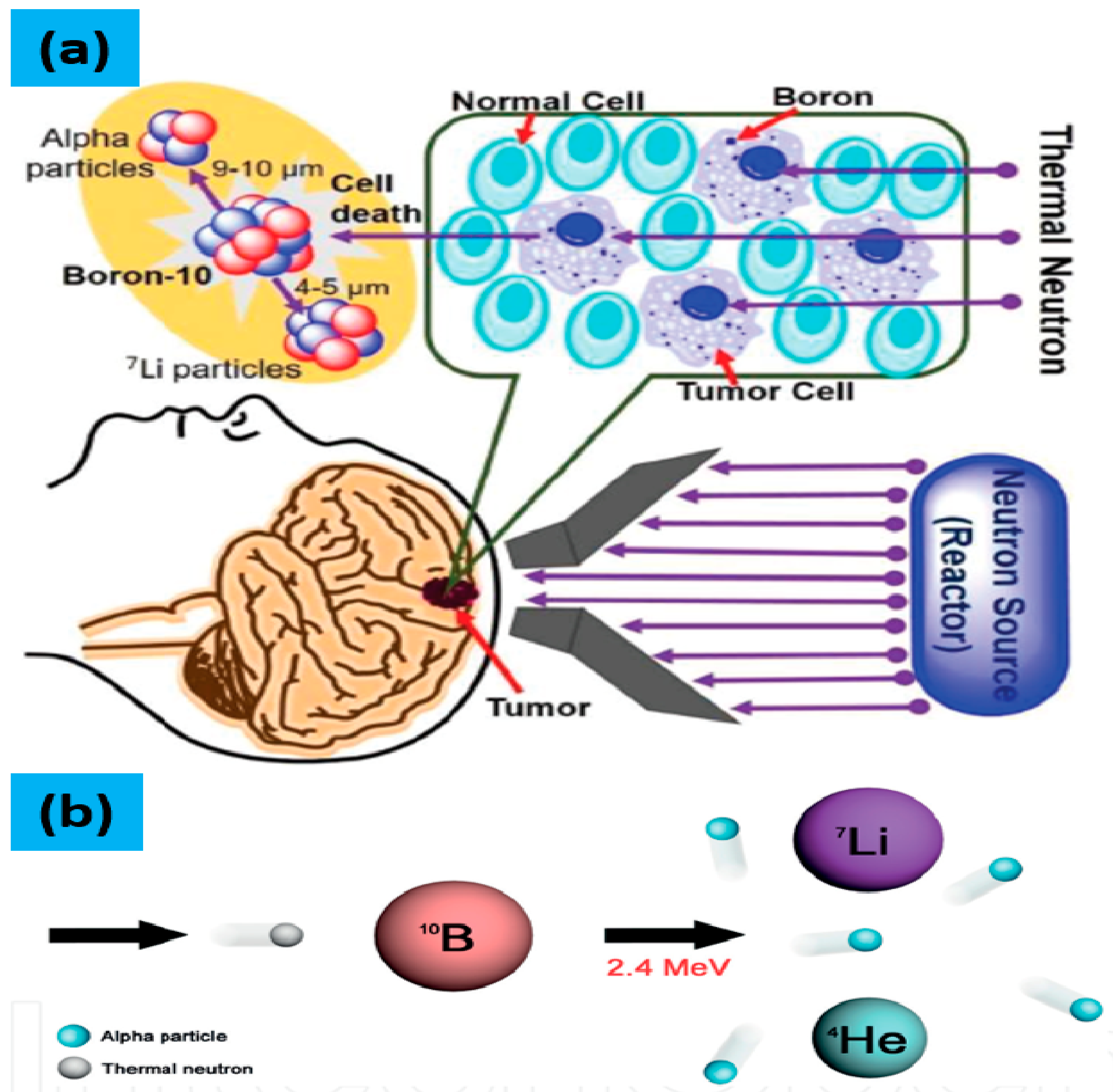{kind=link}
{kind=link}
{kind=link}
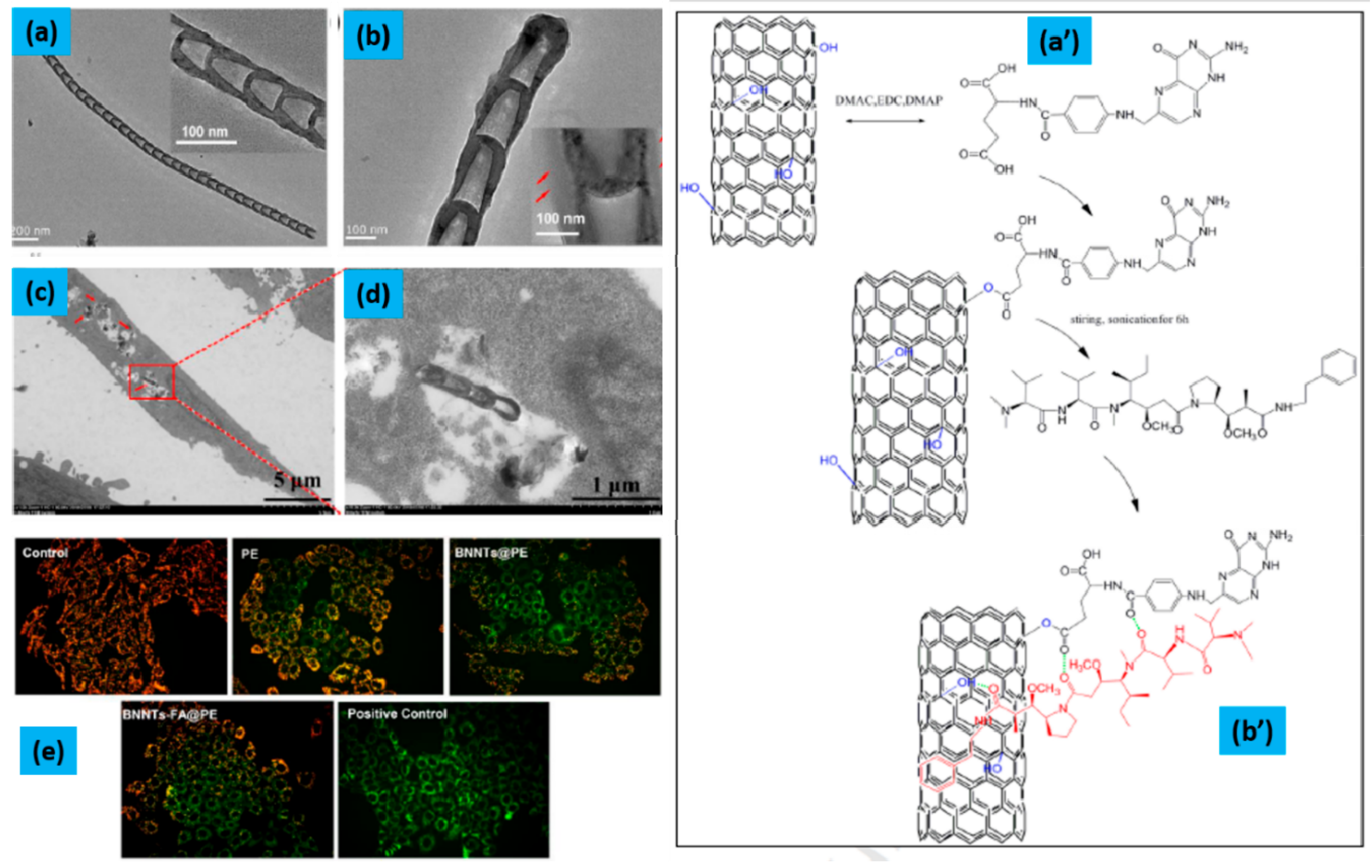{kind=link}
{kind=link}
{kind=link}
{kind=link}
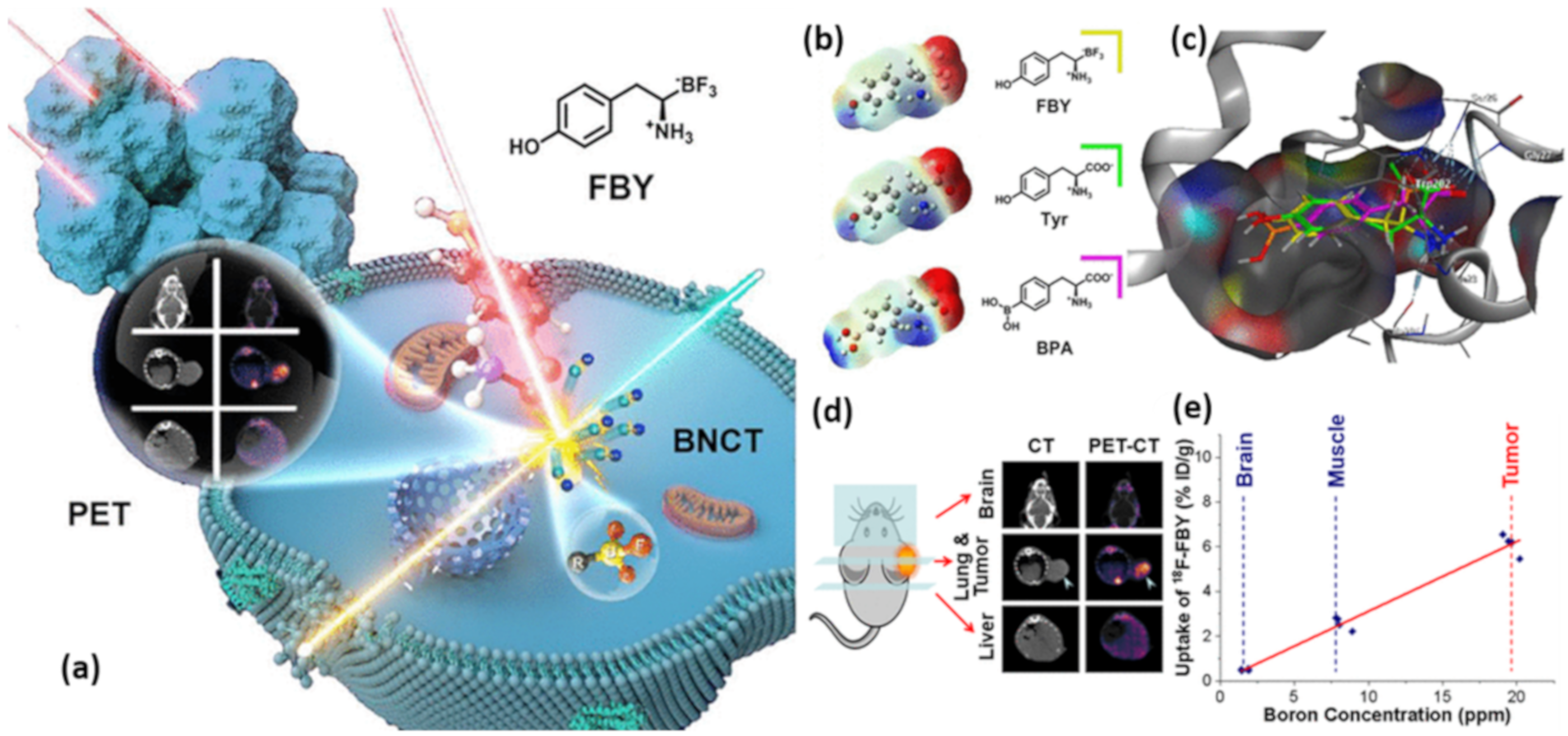{kind=link}
{kind=link}
Table 1.
Summary of recently reported boron-based delivery agents in BNCT.
| Materials | In Cell/In Tumor Model | Observation | Ref. |
|---|---|---|---|
| 10BN | normal (HEK-293) and cancer (HeLa, MCF-7) cells | The promising antitumor effect was observed in HeLa cells. The thermal neutron fluence of ~6.3 × 1012/cm2 resulted in almost 50% cell killing of BN treated HeLa cells | [93] |
| BNNTs | B16-melanoma cell | The accumulation of BNNTs in B16-melanoma cell was three times higher than BSH and their antitumor effect with BNCT was also observed higher than BSH. | [94] |
| BNNTs-FA@PE | Hep G2 cells | Exhibited stronger cytotoxicity than free PE and BNNTs@PE complexes. Also, excellent antiproliferative activities in time- and dose-dependent manners. Additionally, it induced apoptosis of Hep G2 cells by reducing the mitochondrial membrane potential, activating Caspase-9 and Caspase-3. | [102] |
| PTL coated BNNPs | Triple negative breast cancer in mice | The coated BNNPs showed high boron accumulation in the tumor while maintaining its good ratio between tumor and nontumor cells. Suppression of tumor growth was observed with almost negligible side effects. Even these BNNPs shows high accumulation of B atoms inside the cells but they have failure in the therapeutic window for BNCT. | [46] |
| B-AuNP, 61-B-AuNP, 123I-B-AuNP, and 123I-61-B-AuNP | HER2 | The The micro CT/SPECT imaging show the T/M ratio, assessed by ICP-MS, of mice injected by B-AuNP, 61-B-AuNP, 123I-B-AuNP, and 123I-61-B-AuNP was 4.91 ± 2.75, 41.05 ± 11.15, 1.91 ± 0.17, and 12.02 ± 0.94 respectively, at 12 h post-injection. The results show the successfully developed detectable HER2-targeting boron-containing AuNPs with high RCP and an acceptable yield. | [105] |
| (NH2NH3)+[7-NH2(CH2)3S- 7,8-C2B9H11]- in Fluorescent GNCs dispersed in PBS | Cancer tumor in mice model | The accurate tumor imaging by EPR effect and long-term accumulation in tumor cell by nanometer size effect have been observed. This strategy is good for attaining the accurate position of tumor cells with CB and thus decreases the chances of normal tissue damage. In addition, it facilitates the real-time fluorescent visualization to monitor delivery process of the carborane to the targeted tumor, thus endorsing the effect of BNCT treatment through imaging guided therapy. | [106] |
| Gold NPs with PEG, functionalized with bis(dicarbollide), radiolabeled with 124I | in vivo with a mouse model | The results showed a poor accumulation in tumor and major accumulation in liver, lungs and spleen suggesting that the tuning the size and geometry of the gold core is essential | [109] |
| [18F]FBY PET | B16-F10 tumor | showed up to 6 % ID/g in B16-F10 tumor and notably low normal tissue uptake (tumor/muscle = 3.16 ± 0.48; tumor/blood = 3.13 ± 0.50; tumor/brain = 14.25 ± 1.54). Moreover, the administration of [18F]FBY tracer along with a therapeutic dose of FBY showed high accumulation in B16-F10 tumor and low normal tissue uptake. | [111] |
| iRGD-Modified Polymeric Nanoparticles | A549 tumor-bearing mice | Boron concentration ratios for tumor:normal tissue (tumor:muscle = 19.49, tumor:blood = 14.11) in A549 tumor-bearing mice was observed after 24 h of injection. The highest tumor accumulation of DOX was confirmed from both quantitative measurement and fluorescence imaging at 24 hrs after injecting iRGD-modified polymers | [114] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ali, F.; S Hosmane, N.; Zhu, Y. Boron Chemistry for Medical Applications. Molecules 2020, 25, 828. https://doi.org/10.3390/molecules25040828
AMA Style
Ali F, S Hosmane N, Zhu Y. Boron Chemistry for Medical Applications. Molecules. 2020; 25(4):828. https://doi.org/10.3390/molecules25040828
Chicago/Turabian StyleAli, Fayaz, Narayan S Hosmane, and Yinghuai Zhu. 2020. "Boron Chemistry for Medical Applications" Molecules 25, no. 4: 828. https://doi.org/10.3390/molecules25040828