The Effectiveness of Intermittent Fasting to Reduce Body Mass Index and Glucose Metabolism: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
1. Introduction
2. Experimental Section
2.1. Data Sources and Search Strategies
2.2. Eligibility Criteria
2.3. Statistical Analysis
3. Results
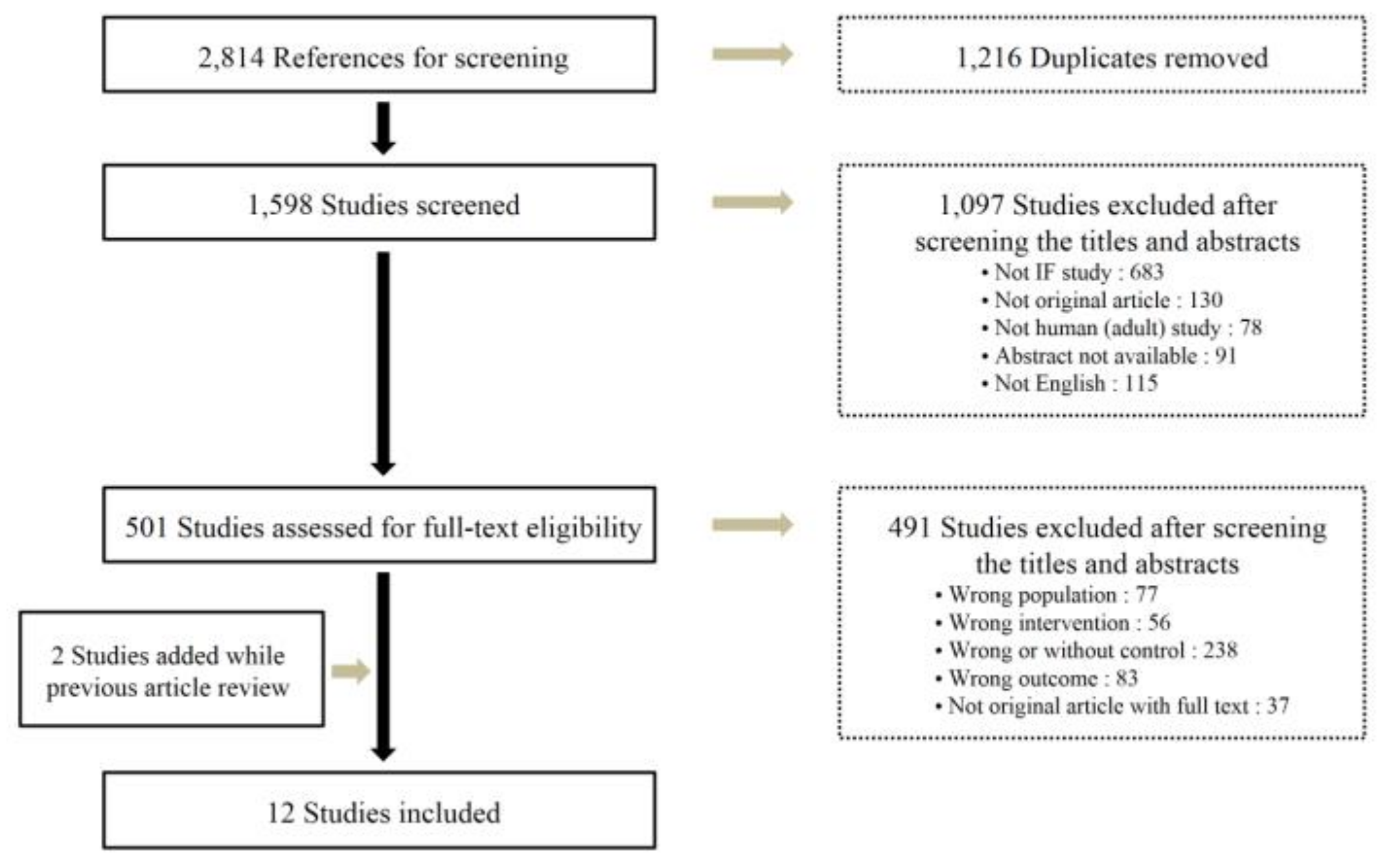
3.1. Search Results and Study Characteristics
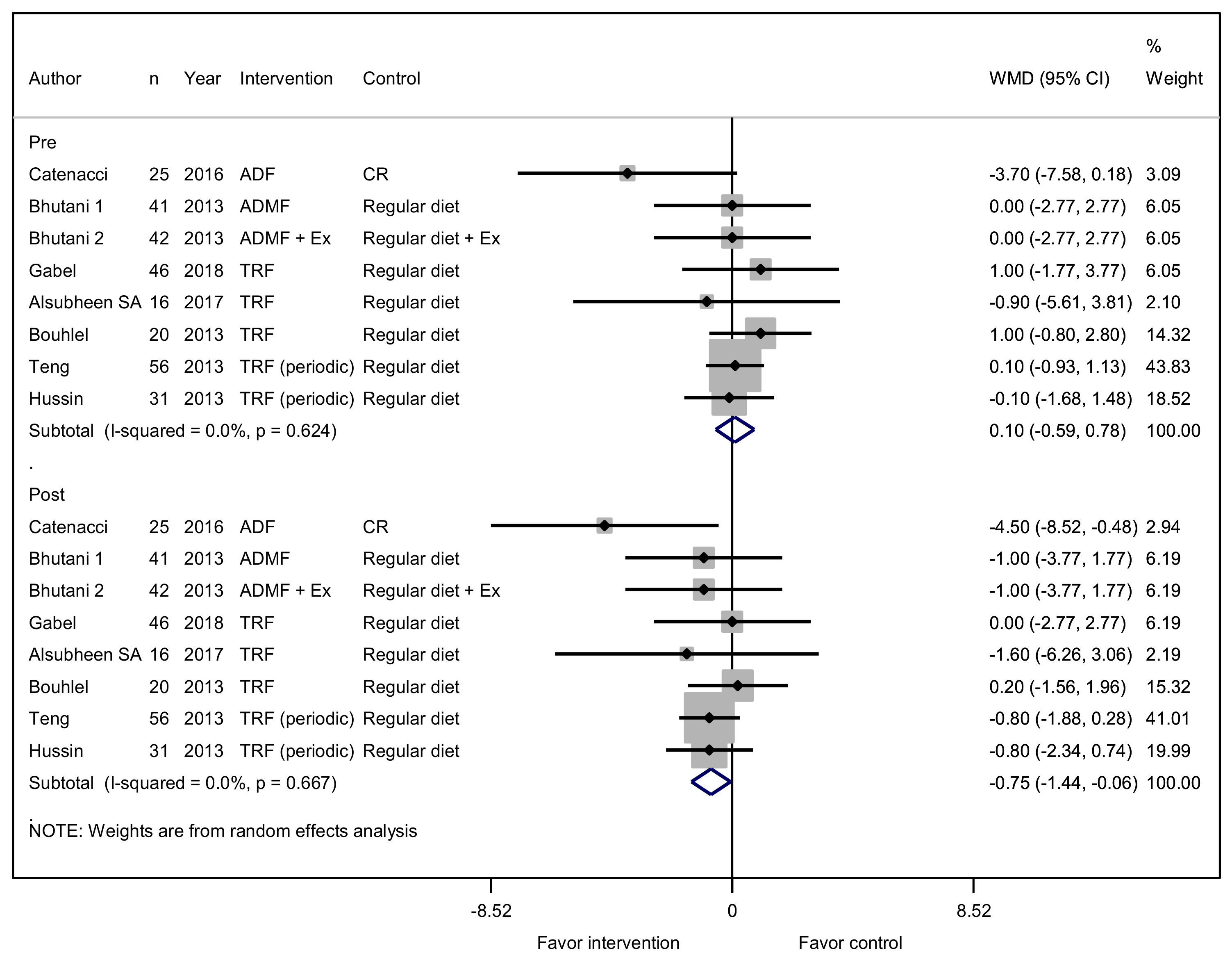
3.2. Effectiveness of Intermittent Fasting on BMI and Body Weight
3.3. Effectiveness of Intermittent Fasting on Glycemic Control
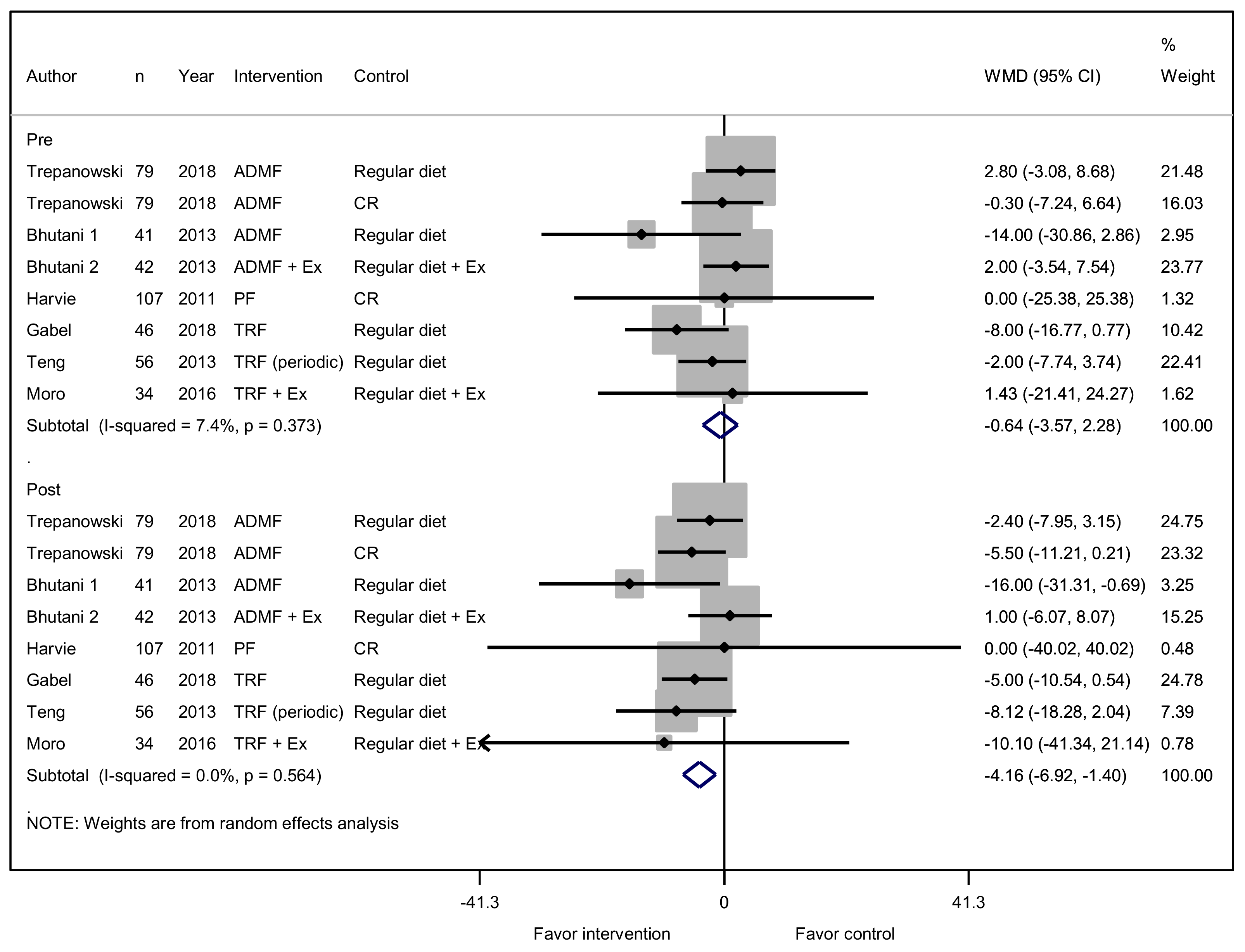
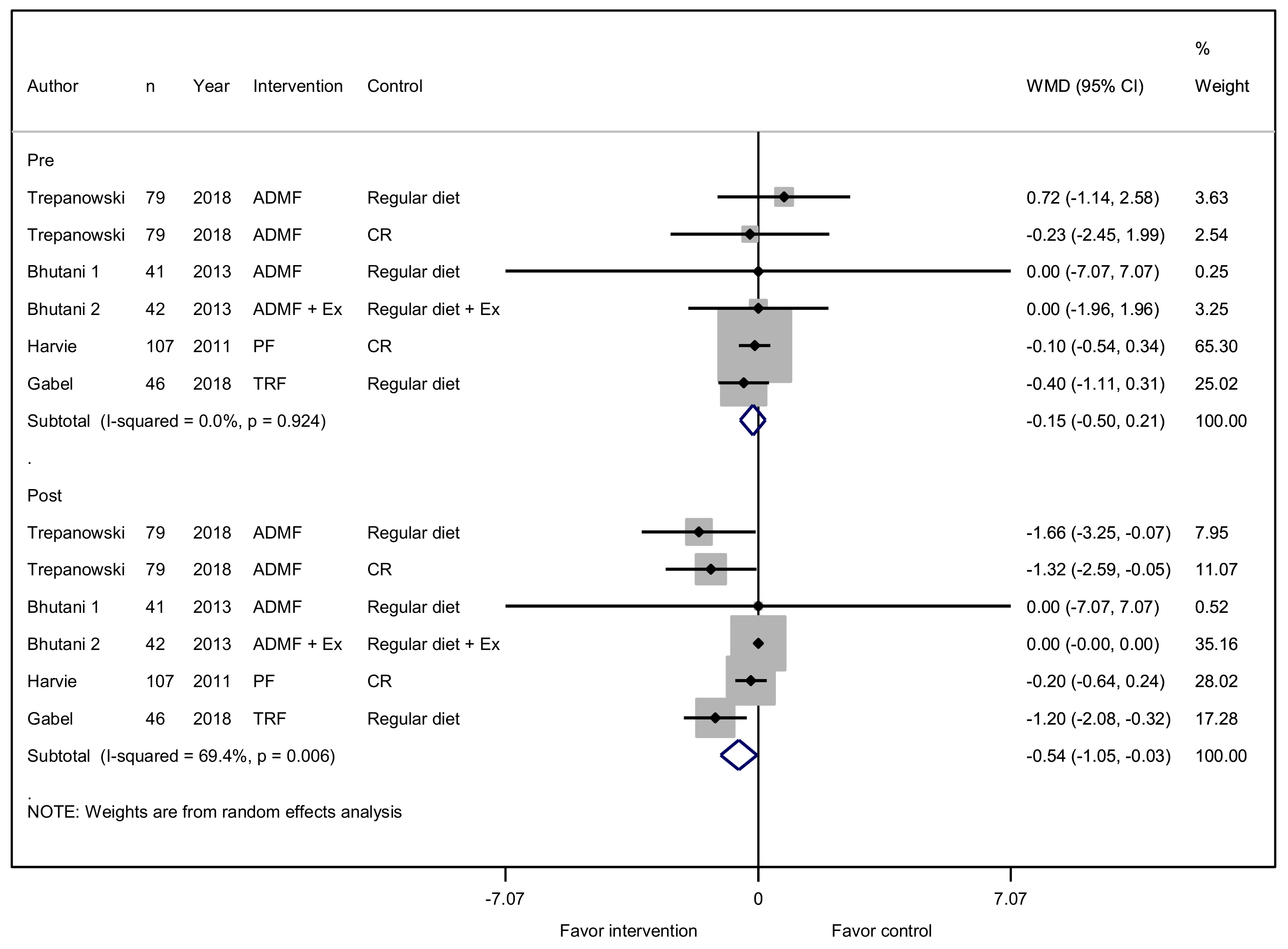
3.4. Effect of Intermittent Fasting on Lean and Fat Mass and Circulating Leptin and Adiponectin
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Redman, L.M.; Ravussin, E. Caloric restriction in humans: Impact on physiological, psychological, and behavioral outcomes. Antioxid. Redox Signal. 2011, 14, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Redman, L.M.; Martin, C.K.; Williamson, D.A.; Ravussin, E. Effect of caloric restriction in non-obese humans on physiological, psychological and behavioral outcomes. Physiol. Behav. 2008, 94, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.L.; Distelmaier, K.; Lanza, I.R.; Irving, B.A.; Robinson, M.M.; Konopka, A.R.; Shulman, G.I.; Nair, K.S. Mechanism by which caloric restriction improves insulin sensitivity in sedentary obese adults. Diabetes 2016, 65, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Scheen, A.J. The future of obesity: New drugs versus lifestyle interventions. Expert Opin. Investig. Drugs 2008, 17, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Anton, S.D.; Moehl, K.; Donahoo, W.T.; Marosi, K.; Lee, S.A.; Mainous, A.G., III; Leeuwenburgh, C.; Mattson, M.P. Flipping the metabolic switch: Understanding and applying the health benefits of fasting. Obesity 2018, 26, 254–268. [Google Scholar] [CrossRef] [PubMed]
- Catenacci, V.A.; Pan, Z.; Ostendorf, D.; Brannon, S.; Gozansky, W.S.; Mattson, M.P.; Martin, B.; MacLean, P.S.; Melanson, E.L.; Troy Donahoo, W. A randomized pilot study comparing zero-calorie alternate-day fasting to daily caloric restriction in adults with obesity. Obesity 2016, 24, 1874–1883. [Google Scholar] [CrossRef]
- Eshghinia, S.; Mohammadzadeh, F. The effects of modified alternate-day fasting diet on weight loss and cad risk factors in overweight and obese women. J. Diabetes Metab. Disord. 2013, 12, 4. [Google Scholar] [CrossRef]
- Trepanowski, J.F.; Kroeger, C.M.; Barnosky, A.; Klempel, M.; Bhutani, S.; Hoddy, K.K.; Rood, J.; Ravussin, E.; Varady, K.A. Effects of alternate-day fasting or daily calorie restriction on body composition, fat distribution, and circulating adipokines: Secondary analysis of a randomized controlled trial. Clin. Nutr. 2018, 37, 1871–1878. [Google Scholar] [CrossRef]
- Gabel, K.; Hoddy, K.K.; Haggerty, N.; Song, J.; Kroeger, C.M.; Trepanowski, J.F.; Panda, S.; Varady, K.A. Effects of 8-hour time restricted feeding on body weight and metabolic disease risk factors in obese adults: A pilot study. Nutr. Healthy Aging 2018, 4, 345–353. [Google Scholar] [CrossRef]
- Harvie, M.N.; Pegington, M.; Mattson, M.P.; Frystyk, J.; Dillon, B.; Evans, G.; Cuzick, J.; Jebb, S.A.; Martin, B.; Cutler, R.G.; et al. The effects of intermittent or continuous energy restriction on weight loss and metabolic disease risk markers: A randomized trial in young overweight women. Int. J. Obes. 2011, 35, 714–727. [Google Scholar] [CrossRef]
- Barnosky, A.R.; Hoddy, K.K.; Unterman, T.G.; Varady, K.A. Intermittent fasting vs daily calorie restriction for type 2 diabetes prevention: A review of human findings. Transl. Res. J. Lab. Clin. Med. 2014, 164, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Adawi, M.; Damiani, G.; Bragazzi, N.L.; Bridgewood, C.; Pacifico, A.; Conic, R.R.; Morrone, A.; Malagoli, P.; Pigatto, P.D.M.; Amital, H. The impact of intermittent fasting (ramadan fasting) on psoriatic arthritis disease activity, enthesitis, and dactylitis: A multicentre study. Nutrients 2019, 11, 601. [Google Scholar] [CrossRef] [PubMed]
- Damiani, G.; Mahroum, N.; Pigatto, P.D.M.; Pacifico, A.; Malagoli, P.; Tiodorovic, D.; Conic, R.R.; Amital, H.; Bragazzi, N.L.; Watad, A. The safety and impact of a model of intermittent, time-restricted circadian fasting (“ramadan fasting”) on hidradenitis suppurativa: Insights from a multicenter, observational, cross-over, pilot, exploratory study. Nutrients 2019, 11, 1781. [Google Scholar] [CrossRef] [PubMed]
- Damiani, G.; Watad, A.; Bridgewood, C.; Pigatto, P.D.M.; Pacifico, A.; Malagoli, P.; Bragazzi, N.L.; Adawi, M. The impact of ramadan fasting on the reduction of pasi score, in moderate-to-severe psoriatic patients: A real-life multicenter study. Nutrients 2019, 11, 277. [Google Scholar] [CrossRef] [PubMed]
- Bragazzi, N.L.; Sellami, M.; Salem, I.; Conic, R.; Kimak, M.; Pigatto, P.D.M.; Damiani, G. Fasting and its impact on skin anatomy, physiology, and physiopathology: A comprehensive review of the literature. Nutrients 2019, 11, 249. [Google Scholar] [CrossRef] [PubMed]
- Longo, V.D.; Mattson, M.P. Fasting: Molecular mechanisms and clinical applications. Cell Metab. 2014, 19, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Sutton, E.F.; Beyl, R.; Early, K.S.; Cefalu, W.T.; Ravussin, E.; Peterson, C.M. Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell Metab. 2018, 27, 1212–1221. [Google Scholar] [CrossRef] [PubMed]
- Carlson, O.; Martin, B.; Stote, K.S.; Golden, E.; Maudsley, S.; Najjar, S.S.; Ferrucci, L.; Ingram, D.K.; Longo, D.L.; Rumpler, W.V.; et al. Impact of reduced meal frequency without caloric restriction on glucose regulation in healthy, normal-weight middle-aged men and women. Metab. Clin. Exp. 2007, 56, 1729–1734. [Google Scholar] [CrossRef] [PubMed]
- Soeters, M.R.; Lammers, N.M.; Dubbelhuis, P.F.; Ackermans, M.; Jonkers-Schuitema, C.F.; Fliers, E.; Sauerwein, H.P.; Aerts, J.M.; Serlie, M.J. Intermittent fasting does not affect whole-body glucose, lipid, or protein metabolism. Am. J. Clin. Nutr. 2009, 90, 1244–1251. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, S.; Klempel, M.C.; Kroeger, C.M.; Trepanowski, J.F.; Varady, K.A. Alternate day fasting and endurance exercise combine to reduce body weight and favorably alter plasma lipids in obese humans. Obesity 2013, 21, 1370–1379. [Google Scholar] [CrossRef] [PubMed]
- Tinsley, G.M.; Forsse, J.S.; Butler, N.K.; Paoli, A.; Bane, A.A.; La Bounty, P.M.; Morgan, G.B.; Grandjean, P.W. Time-restricted feeding in young men performing resistance training: A randomized controlled trial. Eur. J. Sport Sci. 2017, 17, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Headland, M.; Clifton, P.; Carter, S.; Keogh, J. Weight-loss outcomes: A systematic review and meta-analysis of intermittent energy restriction trials lasting a minimum of 6 months. Nutrients 2016, 8, 354. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.; Hamilton, S.; Azevedo, L.B.; Olajide, J.; De Brún, C.; Waller, G.; Whittaker, V.; Sharp, T.; Lean, M.; Hankey, C. Intermittent fasting interventions for treatment of overweight and obesity in adults: A systematic review and meta-analysis. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 507–547. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Moro, T.; Tinsley, G.; Bianco, A.; Marcolin, G.; Pacelli, Q.F.; Battaglia, G.; Palma, A.; Gentil, P.; Neri, M.; Paoli, A. Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males. J. Transl. Med. 2016, 14, 290. [Google Scholar] [CrossRef] [PubMed]
- Teng, N.I.; Shahar, S.; Rajab, N.F.; Manaf, Z.A.; Johari, M.H.; Ngah, W.Z. Improvement of metabolic parameters in healthy older adult men following a fasting calorie restriction intervention. Aging Male Off. J. Int. Soc. Study Aging Male 2013, 16, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Alsubheen, S.A.; Ismail, M.; Baker, A.; Blair, J.; Adebayo, A.; Kelly, L.; Chandurkar, V.; Cheema, S.; Joanisse, D.R.; Basset, F.A. The effects of diurnal ramadan fasting on energy expenditure and substrate oxidation in healthy men. Br. J. Nutr. 2017, 118, 1023–1030. [Google Scholar] [CrossRef]
- Bouhlel, H.; Shephard, R.J.; Gmada, N.; Aouichaoui, C.; Peres, G.; Tabka, Z.; Bouhlel, E. Effect of ramadan observance on maximal muscular performance of trained men. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2013, 23, 222–227. [Google Scholar] [CrossRef]
- Hussin, N.M.; Shahar, S.; Teng, N.I.; Ngah, W.Z.; Das, S.K. Efficacy of fasting and calorie restriction (fcr) on mood and depression among ageing men. J. Nutr. Health Aging 2013, 17, 674–680. [Google Scholar] [CrossRef]
- Varady, K.A.; Bhutani, S.; Klempel, M.C.; Kroeger, C.M.; Trepanowski, J.F.; Haus, J.M.; Hoddy, K.K.; Calvo, Y. Alternate day fasting for weight loss in normal weight and overweight subjects: A randomized controlled trial. Nutr. J. 2013, 12, 146. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 aha/acc/tos guideline for the management of overweight and obesity in adults: A report of the american college of cardiology/american heart association task force on practice guidelines and the obesity society. Circulation 2014, 129, S102–S138. [Google Scholar] [CrossRef] [PubMed]
- Varady, K.A. Intermittent versus daily calorie restriction: Which diet regimen is more effective for weight loss? Obes. Rev. Off. J. Int. Assoc. Study Obes. 2011, 12, e593–e601. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P.; Ard, J.; Baskin, M.L.; Chiuve, S.E.; Johnson, H.M.; Kris-Etherton, P.; Varady, K. Meal timing and frequency: Implications for cardiovascular disease prevention: A scientific statement from the american heart association. Circulation 2017, 135, e96–e121. [Google Scholar] [CrossRef] [PubMed]
- Klempel, M.C.; Kroeger, C.M.; Bhutani, S.; Trepanowski, J.F.; Varady, K.A. Intermittent fasting combined with calorie restriction is effective for weight loss and cardio-protection in obese women. Nutr. J. 2012, 11, 98. [Google Scholar] [CrossRef] [PubMed]
- Gastaldelli, A.; Kozakova, M.; Hojlund, K.; Flyvbjerg, A.; Favuzzi, A.; Mitrakou, A.; Balkau, B. Fatty liver is associated with insulin resistance, risk of coronary heart disease, and early atherosclerosis in a large european population. Hepatology 2009, 49, 1537–1544. [Google Scholar] [CrossRef]
- Bouassida, A.; Chamari, K.; Zaouali, M.; Feki, Y.; Zbidi, A.; Tabka, Z. Review on leptin and adiponectin responses and adaptations to acute and chronic exercise. Br. J. Sports Med. 2010, 44, 620–630. [Google Scholar] [CrossRef]
- Goldstein, B.J.; Scalia, R. Adiponectin: A novel adipokine linking adipocytes and vascular function. J. Clin. Endocrinol. Metab. 2004, 89, 2563–2568. [Google Scholar] [CrossRef]
- Rong, S.; Snetselaar, L.G.; Xu, G.; Sun, Y.; Liu, B.; Wallace, R.B.; Bao, W. Association of skipping breakfast with cardiovascular and all-cause mortality. J. Am. Coll. Cardiol. 2019, 73, 2025–2032. [Google Scholar] [CrossRef]
- Witbracht, M.; Keim, N.L.; Forester, S.; Widaman, A.; Laugero, K. Female breakfast skippers display a disrupted cortisol rhythm and elevated blood pressure. Physiol. Behav. 2015, 140, 215–221. [Google Scholar] [CrossRef]
- Jakubowicz, D.; Barnea, M.; Wainstein, J.; Froy, O. High caloric intake at breakfast vs. Dinner differentially influences weight loss of overweight and obese women. Obesity 2013, 21, 2504–2512. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Design | Duration (wk) | Intervention | Intervention Detail | Fasting Time of Intervention Group (h) | Calorie Reduction (From Baseline, %) | Control (Without Fasting) | Control Detail | Calorie Reduction (From Baseline, %) |
|---|---|---|---|---|---|---|---|---|---|---|
| Trepanowski et al. 1 [8] | 2018 | 66 women, 13 men (aged 18–65 y, overweight to obese, BMI 25–40 kg/m2) | 24 | ADMF | alternating every 24 h between consuming 25% or 125% of energy needs | 24 | 21.0 | RD | consuming 100% of needs every day | Not shown |
| Trepanowski et al. 2 [8] | 2018 | 66 women, 13 men (aged 18–65 y, overweight to obese, BMI 25–40 kg/m2) | 24 | ADMF | alternating every 24 h between consuming 25% or 125% of energy needs | 24 | 21.0 | CR | Consuming 75% of needs every day | 24.0 |
| Catenacci et al. [6] | 2016 | 19 women, 6 men (aged 18–55 y, obese, BMI over 30 kg/m2) | 8 | ADF | fast on alternate days, fasting day, at libitum | 24 | 47.0 | CR | 400 kcal/d deficit from estimated energy requirements | 28.0 |
| Gabel et al. [9] | 2018 | 41 women, 5 men (aged 25–65 y, obese, BMI 30–45 kg/m2) | 12 | TRF | ad libitum feeding between 10 am to 6pm, fasting between 6pm to 10am | 16 | 20.3 | RD | not to change their eating or physical activity habits | Not shown |
| Moro et al. [25] | 2016 | 34 men (aged 29.21 ± 3.8 y, weighted 84.6 ± 6.2 kg) | 8 | TRF + Ex | 1 p.m., 4 p.m., 8 p.m. feeding | 16 | 3.2 | RD + Ex | 8 a.m., 1 p.m., 8 p.m. feeding | Not shown |
| Bhutani et al. 1 [20] | 2013 | 80 women, 3 men (aged 25–65 y, obese, BMI 30–39.9 kg/m2) | 12 | ADMF | 25% of their baseline energy needs on the fast day (24 h), ad libitum on feed day, 12 p.m. to 2 p.m. meals on fast day, 3 days/wk | 22 | Not shown (450 kcal/d reduction) | RD | maintain regular food habits | Not shown |
| Bhutani et al. 2 [20] | 2013 | 80 women, 3 men (aged 25–65 y, obese, BMI 30–39.9 kg/m2) | 12 | ADMF + Ex | 25% of their baseline energy needs on the fast day (24 h), ad libitum on feed day, 12 p.m. to 2 p.m. meals on fast day, 3 days/wk | 22 | Not shown (450 kcal/d reduction) | RD + Ex | maintain regular food habits + Ex | Not shown |
| Teng et al. [26] | 2013 | 56 men (aged 50–70 y, BMI 23–29.9 kg/m2) | 12 | TRF (periodic) | reduction of 300–500 kcal/d from participants baseline energy intake combined with two days of Muslim Sunnah fasting per weeks | 13, approximately | 19.2 | RD | maintain regular food habits | Not shown |
| Alsubheen et al. [27] | 2017 | 16 men | 4 | TRF | Muslim Ramadan | 13 | 16.0 | RD | maintain regular food habits | 7.8 |
| Bouhlel et al. [28] | 2013 | 20 men (aged 20 y) | 4 | TRF | Muslim Ramadan | Muslim Sunnah fasting | 10.9 | RD | maintain regular food habits | Not shown |
| Hussin et al. [29] | 2013 | 31 men (aged 50–70 y, BMI 23–29.9 kg/m2) | 12 | TRF (periodic) | reduction of 300–500 kcal/d from participants baseline energy intake combined with two days of Muslim Sunnah fasting per week | Muslim Sunnah fasting | 10.3 | RD | maintain regular food habits | Not shown |
| Harvie et al. [10] | 2011 | 107 women (aged 30–45 y) | 24 | PF | VLCD for 2 days per week | unknown | 29.7 | CR | 25% restriction | 20.4 |
| Tinsley et al. [21] | 2017 | 18 men | 8 | TRF (periodic) + Ex | On non-workout days (four days per week), consume all calories in any four hour window between 4 p.m. and midnight / unrestricted on RT day | 20 | 13.8 | RD + Ex | RT | 20.3 |
| Varady et al. [30] | 2013 | 22 women, 8 men (aged 35–63 y, BMI 20–29.9 kg/m2) | 12 | ADMF | 25% of their baseline energy needs on the fast day (24 h), ad libitum on feed day, 12 p.m. to 2 p.m. meals on fast day | 22 | 38.0 | RD | Ad libitum | Not shown |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, Y.; Hong, N.; Kim, K.-w.; Cho, S.j.; Lee, M.; Lee, Y.-h.; Lee, Y.-h.; Kang, E.S.; Cha, B.-S.; Lee, B.-W. The Effectiveness of Intermittent Fasting to Reduce Body Mass Index and Glucose Metabolism: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 1645. https://doi.org/10.3390/jcm8101645
Cho Y, Hong N, Kim K-w, Cho Sj, Lee M, Lee Y-h, Lee Y-h, Kang ES, Cha B-S, Lee B-W. The Effectiveness of Intermittent Fasting to Reduce Body Mass Index and Glucose Metabolism: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2019; 8(10):1645. https://doi.org/10.3390/jcm8101645
Chicago/Turabian StyleCho, Yongin, Namki Hong, Kyung-won Kim, Sung joon Cho, Minyoung Lee, Yeon-hee Lee, Yong-ho Lee, Eun Seok Kang, Bong-Soo Cha, and Byung-Wan Lee. 2019. "The Effectiveness of Intermittent Fasting to Reduce Body Mass Index and Glucose Metabolism: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 8, no. 10: 1645. https://doi.org/10.3390/jcm8101645
APA StyleCho, Y., Hong, N., Kim, K.-w., Cho, S. j., Lee, M., Lee, Y.-h., Lee, Y.-h., Kang, E. S., Cha, B.-S., & Lee, B.-W. (2019). The Effectiveness of Intermittent Fasting to Reduce Body Mass Index and Glucose Metabolism: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 8(10), 1645. https://doi.org/10.3390/jcm8101645