A Combined Score of Circulating miRNAs Allows Outcome Prediction in Critically Ill Patients


 , ,
, , 
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Extraction of miRNA and qPCR
2.3. Statistical Analysis
3. Results
3.1. Alterations of Circulating miRNA Concentrations in Critically Ill Patients
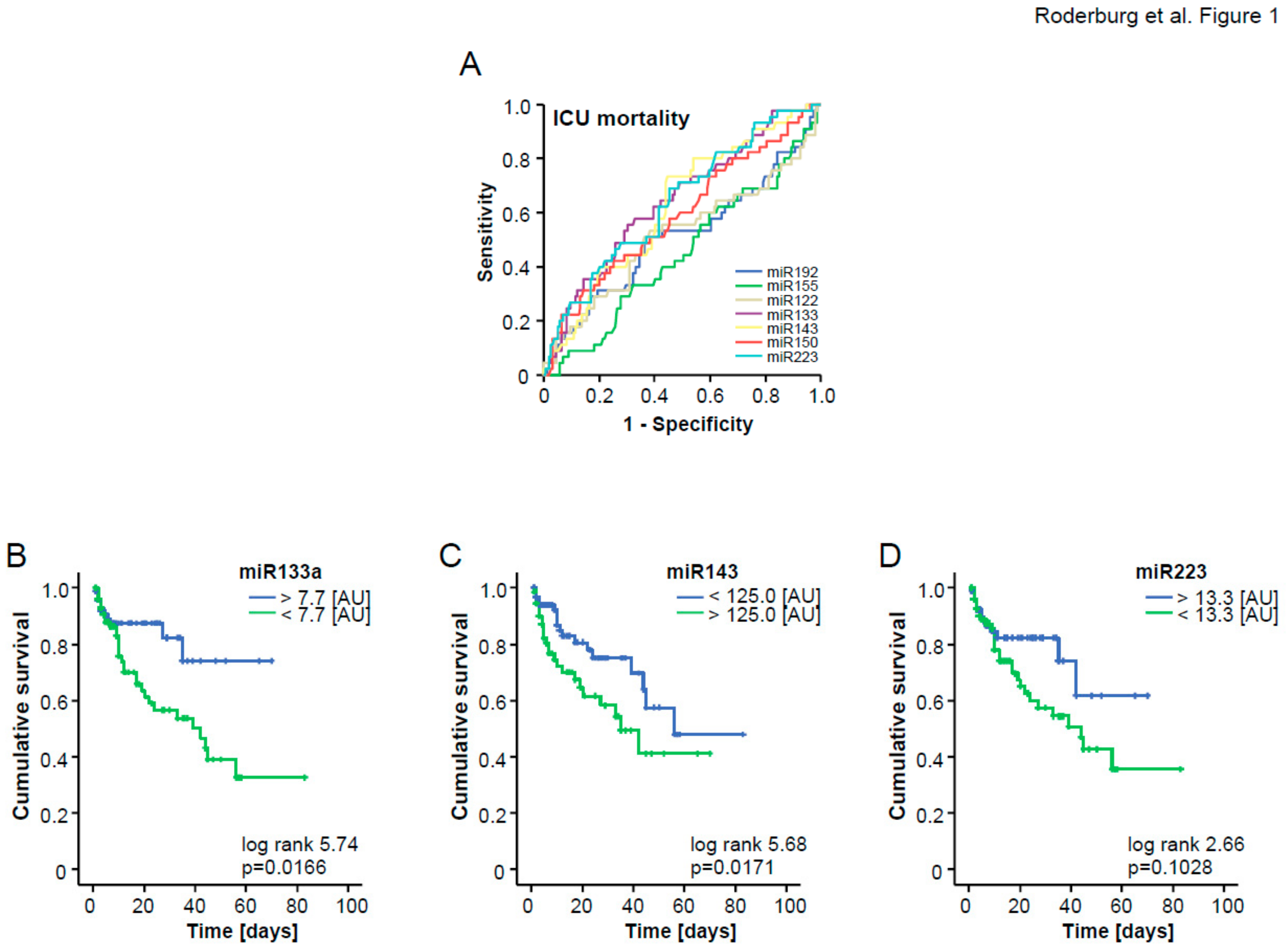
3.2. A Three miRNA Score Predicts Patients’ Survival in ICU Treatment
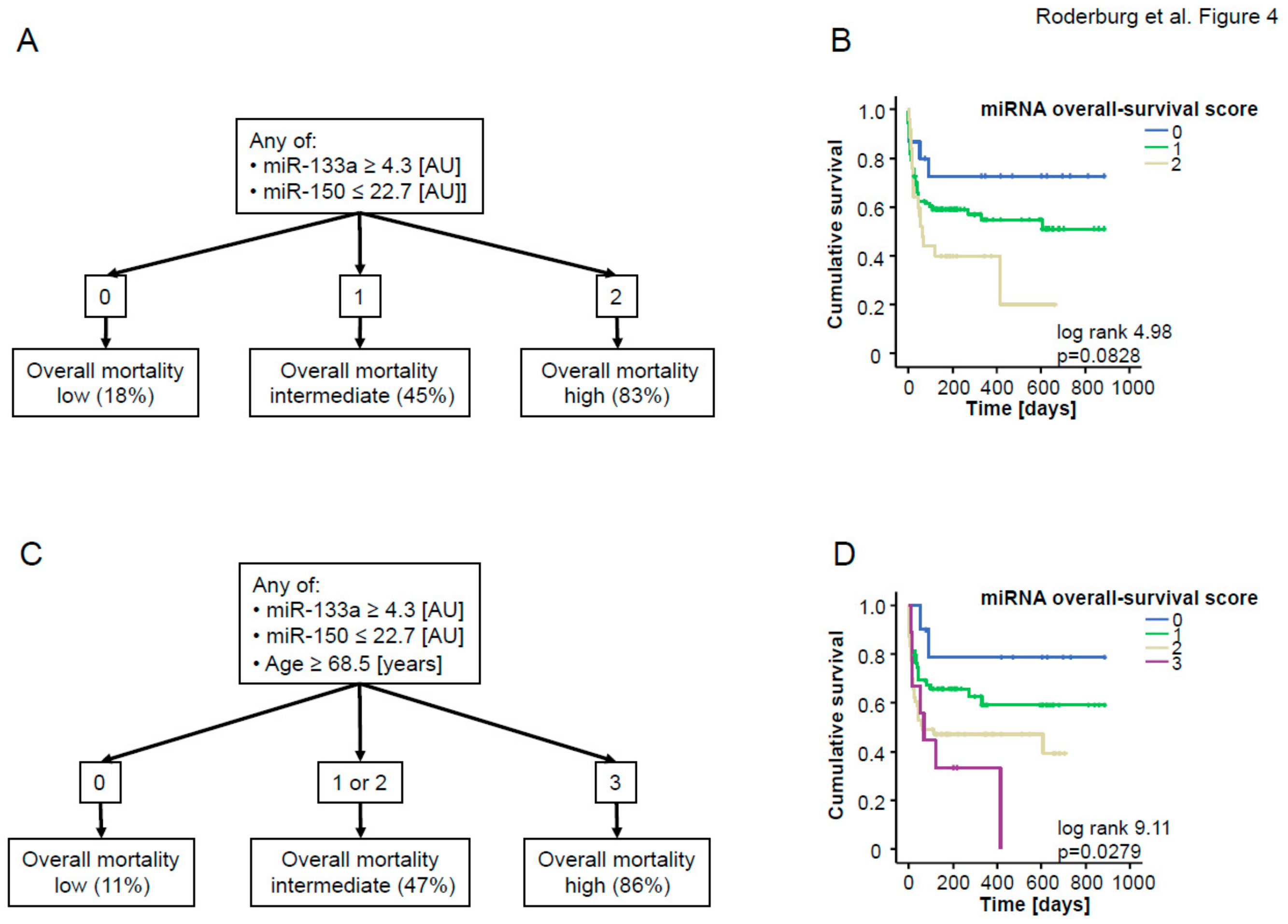
3.3. A Two miRNA Score Predicts Patients’ Long-Term Prognosis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef] [PubMed]
- Pierrakos, C.; Vincent, J.L. Sepsis biomarkers: A review. Crit. Care 2010, 14, R15. [Google Scholar] [CrossRef] [PubMed]
- Andaluz-Ojeda, D.; Bobillo, F.; Iglesias, V.; Almansa, R.; Rico, L.; Gandía, F.; Resino, S.; Tamayo, E.; de Lejarazu, R.O.; Bermejo-Martin, J.F. A combined score of pro- and anti-inflammatory interleukins improves mortality prediction in severe sepsis. Cytokine 2012, 57, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Kofoed, K.; Andersen, O.; Kronborg, G.; Tvede, M.; Petersen, J.; Eugen-Olsen, J.; Larsen, K. Use of plasma C-reactive protein, procalcitonin, neutrophils, macrophage migration inhibitory factor, soluble urokinase-type plasminogen activator receptor, and soluble triggering receptor expressed on myeloid cells-1 in combination to diagnose infections: A prospective study. Crit. Care 2007, 11, R38. [Google Scholar] [PubMed]
- Shapiro, N.I.; Trzeciak, S.; Hollander, J.E.; Birkhahn, R.; Otero, R.; Osborn, T.M.; Moretti, E.; Nguyen, H.B.; Gunnerson, K.J.; Milzman, D.; et al. A prospective, multicenter derivation of a biomarker panel to assess risk of organ dysfunction, shock, and death in emergency department patients with suspected sepsis. Crit. Care Med. 2009, 37, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Ha, M.; Kim, V.N. Regulation of microRNA biogenesis. Nat. Rev. Mol. Cell Biol. 2014, 15, 509–524. [Google Scholar] [CrossRef] [PubMed]
- Roderburg, C.; Luedde, M.; Vargas Cardenas, D.; Vucur, M.; Mollnow, T.; Zimmermann, H.W.; Koch, A.; Hellerbrand, C.; Weiskirchen, R.; Frey, N.; et al. miR-133a mediates TGF-beta-dependent derepression of collagen synthesis in hepatic stellate cells during liver fibrosis. J. Hepatol. 2013, 58, 736–742. [Google Scholar] [CrossRef]
- Roderburg, C.; Mollnow, T.; Bongaerts, B.; Elfimova, N.; Vargas Cardenas, D.; Berger, K.; Zimmermann, H.; Koch, A.; Vucur, M.; Luedde, M.; et al. Micro-RNA profiling in human serum reveals compartment-specific roles of miR-571 and miR-652 in liver cirrhosis. PLoS ONE 2012, 7, e32999. [Google Scholar] [CrossRef]
- Tacke, F.; Roderburg, C.; Benz, F.; Cardenas, D.V.; Luedde, M.; Hippe, H.J.; Frey, N.; Vucur, M.; Gautheron, J.; Koch, A.; et al. Levels of circulating miR-133a are elevated in sepsis and predict mortality in critically ill patients. Crit. Care Med. 2014, 42, 1096–1104. [Google Scholar] [CrossRef]
- Essandoh, K.; Fan, G.C. Role of extracellular and intracellular microRNAs in sepsis. Biochimica Biophysica Acta 2014, 1842, 2155–2162. [Google Scholar] [CrossRef]
- Roderburg, C.; Benz, F.; Vargas Cardenas, D.; Koch, A.; Janssen, J.; Vucur, M.; Gautheron, J.; Schneider, A.T.; Koppe, C.; Kreggenwinkel, K.; et al. Elevated miR-122 serum levels are an independent marker of liver injury in inflammatory diseases. Liver Int. 2015, 35, 1172–1184. [Google Scholar] [CrossRef] [PubMed]
- Roderburg, C.; Luedde, M.; Vargas Cardenas, D.; Vucur, M.; Scholten, D.; Frey, N.; Koch, A.; Trautwein, C.; Tacke, F.; Luedde, T. Circulating microRNA-150 serum levels predict survival in patients with critical illness and sepsis. PLoS ONE 2013, 8, e54612. [Google Scholar] [CrossRef] [PubMed]
- Tacke, F.; Spehlmann, M.E.; Vucur, M.; Benz, F.; Luedde, M.; Cardenas, D.V.; Roy, S.; Loosen, S.; Hippe, H.; Frey, N.; et al. miR-155 Predicts Long-Term Mortality in Critically Ill Patients Younger than 65 Years. Mediat. Inflamm. 2019, 2019, 6714080. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Benz, F.; Alder, J.; Bantel, H.; Janssen, J.; Vucur, M.; Gautheron, J.; Schneider, A.; Schüller, F.; Loosen, S.; et al. Down-regulation of miR-192-5p protects from oxidative stress-induced acute liver injury. Clin. Sci 2016, 130, 1197–1207. [Google Scholar] [CrossRef] [PubMed]
- Benz, F.; Tacke, F.; Luedde, M.; Trautwein, C.; Luedde, T.; Koch, A.; Roderburg, C. Circulating microRNA-223 serum levels do not predict sepsis or survival in patients with critical illness. Dis. Markers 2015, 2015, 384208. [Google Scholar] [CrossRef] [PubMed]
- Roderburg, C.; Benz, F.; Cardenas, D.V.; Lutz, M.; Hippe, H.J.; Luedde, T.; Trautwein, C.; Frey, N.; Koch, A.; Tacke, F.; et al. Persistently elevated osteopontin serum levels predict mortality in critically ill patients. Crit. Care 2015, 19, 271. [Google Scholar] [CrossRef] [PubMed]
- Ray, P.; Le Manach, Y.; Riou, B.; Houle, T.T. Statistical evaluation of a biomarker. Anesthesiology 2010, 112, 1023–1040. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Roderburg, C.; Luedde, M.; Vargas Cardenas, D.; Vucur, M.; Scholten, D.; Frey, N.; Koch, A.; Trautwein, C.; Tacke, F.; Luedde, T. Serum levels of miR-143 predict survival in critically ill patients. Dis. Markers 2013, in press. [Google Scholar]
- Ginde, A.A.; Moss, M.; Shapiro, N.I.; Schwartz, R.S. Impact of older age and nursing home residence on clinical outcomes of US emergency department visits for severe sepsis. J. Crit. Care 2013, 28, 606–611. [Google Scholar] [CrossRef]
- Koch, A.; Weiskirchen, R.; Zimmermann, H.W.; Sanson, E.; Trautwein, C.; Tacke, F. Relevance of serum leptin and leptin-receptor concentrations in critically ill patients. Mediat. Inflamm. 2010, 2010, 473540. [Google Scholar] [CrossRef] [PubMed]
- Koch, A.; Sanson, E.; Helm, A.; Voigt, S.; Trautwein, C.; Tacke, F. Regulation and prognostic relevance of serum ghrelin concentrations in critical illness and sepsis. Crit. Care 2010, 14, R94. [Google Scholar] [CrossRef] [PubMed]
- Koch, A.; Gressner, O.A.; Sanson, E.; Tacke, F.; Trautwein, C. Serum resistin levels in critically ill patients are associated with inflammation, organ dysfunction and metabolism and may predict survival of non-septic patients. Crit. Care 2009, 13, R95. [Google Scholar] [CrossRef]
- Koch, A.; Tacke, F. Risk stratification and triage in the emergency department: Has this become ‘suPAR’ easy? J. Intern. Med. 2012, 272, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Schwarzenbach, H.; Nishida, N.; Calin, G.A.; Pantel, K. Clinical relevance of circulating cell-free microRNAs in cancer. Nat. Rev. Clin. Oncol. 2014, 11, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Zhang, S.; Marzolf, B.; Troisch, P.; Brightman, A.; Hu, Z.; Hood, L.E.; Galas, D.J. Circulating microRNAs, potential biomarkers for drug-induced liver injury. Proc. Natl. Acad. Sci. USA 2009, 106, 4402–4407. [Google Scholar] [CrossRef]
- Vasilescu, C.; Rossi, S.; Shimizu, M.; Tudor, S.; Veronese, A.; Ferracin, M.; Nicoloso, M.S.; Barbarotto, E.; Popa, M.; Stanciulea, O.; et al. MicroRNA fingerprints identify miR-150 as a plasma prognostic marker in patients with sepsis. PLoS ONE 2009, 4, e7405. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, W.M.; Spiel, A.O.; Jilma, B.; Wolzt, M.; Müller, M. In vivo profile of the human leukocyte microRNA response to endotoxemia. Biochem. Biophys. Res. Commun. 2009, 380, 437–441. [Google Scholar] [CrossRef]
- Wang, J.F.; Yu, M.L.; Yu, G.; Bian, J.J.; Deng, X.M.; Wan, X.J.; Zhu, K.M. Serum miR-146a and miR-223 as potential new biomarkers for sepsis. Biochem. Biophys. Res. Commun. 2010, 394, 184–188. [Google Scholar] [CrossRef]
- Wang, H.J.; Zhang, P.J.; Chen, W.J.; Feng, D.; Jia, Y.H.; Xie, L.X. Four serum microRNAs identified as diagnostic biomarkers of sepsis. J. Trauma Acute Care Surg. 2012, 73, 850–854. [Google Scholar] [CrossRef]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef] [PubMed]
- Benz, F.; Roderburg, C.; Vargas Cardenas, D.; Vucur, M.; Gautheron, J.; Koch, A.; Zimmermann, H.; Janssen, J.; Nieuwenhuijsen, L.; Luedde, M.; et al. U6 is unsuitable for normalization of serum miRNA levels in patients with sepsis or liver fibrosis. Exp. Mol. Med. 2013, 45, e42. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.S.; Huang, X.; Cao, H.; Christman-Skieller, C.; Bennewith, K.; Le, Q.T.; Koong, A.C. Circulating miR-210 as a Novel Hypoxia Marker in Pancreatic Cancer. Transl. Oncol. 2010, 3, 109–113. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All Patients |
|---|---|
| Number | 204 |
| Sex (male/female) | 132/72 |
| Age median (range) [years] | 63 (18–89) |
| APACHE-II score median (range) | 16 (2–40) |
| SAPS2 score median (range) | 43 (8–79) |
| ICU days median (range) | 7 (1–83) |
| Death during ICU [%] | 22.1 |
| Ventilation [%] | 64.7 |
| Body mass index median (range) [kg/m2] | 26.1 (16.6–86.5) |
| Creatinine (range) [mg/dL] | 1.3 (0–15) |
| WBC median (range) [×103/µL] | 12.2 (0.1–67.4) |
| CRP median (range) [mg/dL] | 100 (<5–230) |
| Procalcitonin median (range) [µg/L] | 0.71 (0–180.6) |
| Interleukin-6 median (range) [pg/mL] | 105 (0–83,000) |
| INR median (range) | 1.18 (0–9.2) |
| Sepsis | Non-Sepsis | |
|---|---|---|
| n = 127 | n = 77 | |
| Sepsis critical illness Source of infection n (%) | ||
| Pulmonary | 67 (52.8) | |
| Abdominal | 28 (22.0) | |
| Urogenital | 3 (2.4) | |
| Other | 29 (22.8) | |
| Non-sepsis critical illness n (%) | ||
| Cardiopulmonary disease | 26 (33.8) | |
| Decompensated liver cirrhosis | 11 (14.3) | |
| Non-sepsis other | 40 (51.9) |
| Mir-122 | Mir-133a | Mir-143 | Mir-150 | Mir-155 | Mir-192 | Mir-223 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Published [11] | 204 Patients Cohort | Published [9] | 204 Patients Cohort | Published * [19] | 204 Patients Cohort | Published [12] | 204 Patients Cohort | Published [13] | 204 Patients Cohort | Published [14] | 204 Patients Cohort | Published [15] | 204 Patients Cohort | |
| Patients vs. Control | ↑ | ↑ | ↑ | ↑ | = | = | = | = | ↑ | ↑ | ↑ | rauf | ≈(↓) | ↓ |
| Sepsis vs. Non-Sepsis | = | = | ↑ | ↑ | = | = | = | = | = | = | = | = | = | = |
| ICU Survival vs. Non-Survival | = | = | ↓ | ↓ | ↑ | ↑ | = | = | = | = | = | = | ↑ | ↑ |
| Overall Survival vs. Non-Survival | = | = | ↓ | ↓ | = | = | ↑ | ↑ | = | = | = | = | = | = |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roderburg, C.; Benz, F.; Koch, A.; Loosen, S.H.; Spehlmann, M.; Luedde, M.; Wree, A.; Vucur, M.; Trautwein, C.; Tacke, F.; et al. A Combined Score of Circulating miRNAs Allows Outcome Prediction in Critically Ill Patients. J. Clin. Med. 2019, 8, 1644. https://doi.org/10.3390/jcm8101644
Roderburg C, Benz F, Koch A, Loosen SH, Spehlmann M, Luedde M, Wree A, Vucur M, Trautwein C, Tacke F, et al. A Combined Score of Circulating miRNAs Allows Outcome Prediction in Critically Ill Patients. Journal of Clinical Medicine. 2019; 8(10):1644. https://doi.org/10.3390/jcm8101644
Chicago/Turabian StyleRoderburg, Christoph, Fabian Benz, Alexander Koch, Sven H. Loosen, Martina Spehlmann, Mark Luedde, Alexander Wree, Mihael Vucur, Christian Trautwein, Frank Tacke, and et al. 2019. "A Combined Score of Circulating miRNAs Allows Outcome Prediction in Critically Ill Patients" Journal of Clinical Medicine 8, no. 10: 1644. https://doi.org/10.3390/jcm8101644
APA StyleRoderburg, C., Benz, F., Koch, A., Loosen, S. H., Spehlmann, M., Luedde, M., Wree, A., Vucur, M., Trautwein, C., Tacke, F., & Luedde, T. (2019). A Combined Score of Circulating miRNAs Allows Outcome Prediction in Critically Ill Patients. Journal of Clinical Medicine, 8(10), 1644. https://doi.org/10.3390/jcm8101644