

Self-Rated Effectiveness of Ayahuasca and Breathwork on Well-Being, Psychological Resilience, Self-Compassion, and Personality: An Observational Comparison Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Design and Procedure
2.3. Setting
Ayahuasca Setting
2.4. Breathwork Setting
3. Questionnaires
3.1. Demographic Information
3.2. Motivation to Attend the Ayahuasca Ceremony or Breathwork Session
3.3. World Health Organisation-Five Well-Being Index
3.4. The 14-Item Resilience Scale
3.5. Self-Compassion Scale–Short Form
3.6. Big Five Inventory-10
4. Statistical Analysis
5. Results
5.1. Participants
5.2. Demographic Data
5.3. Motivation to Attend the Ayahuasca Ceremony or Breathwork Session
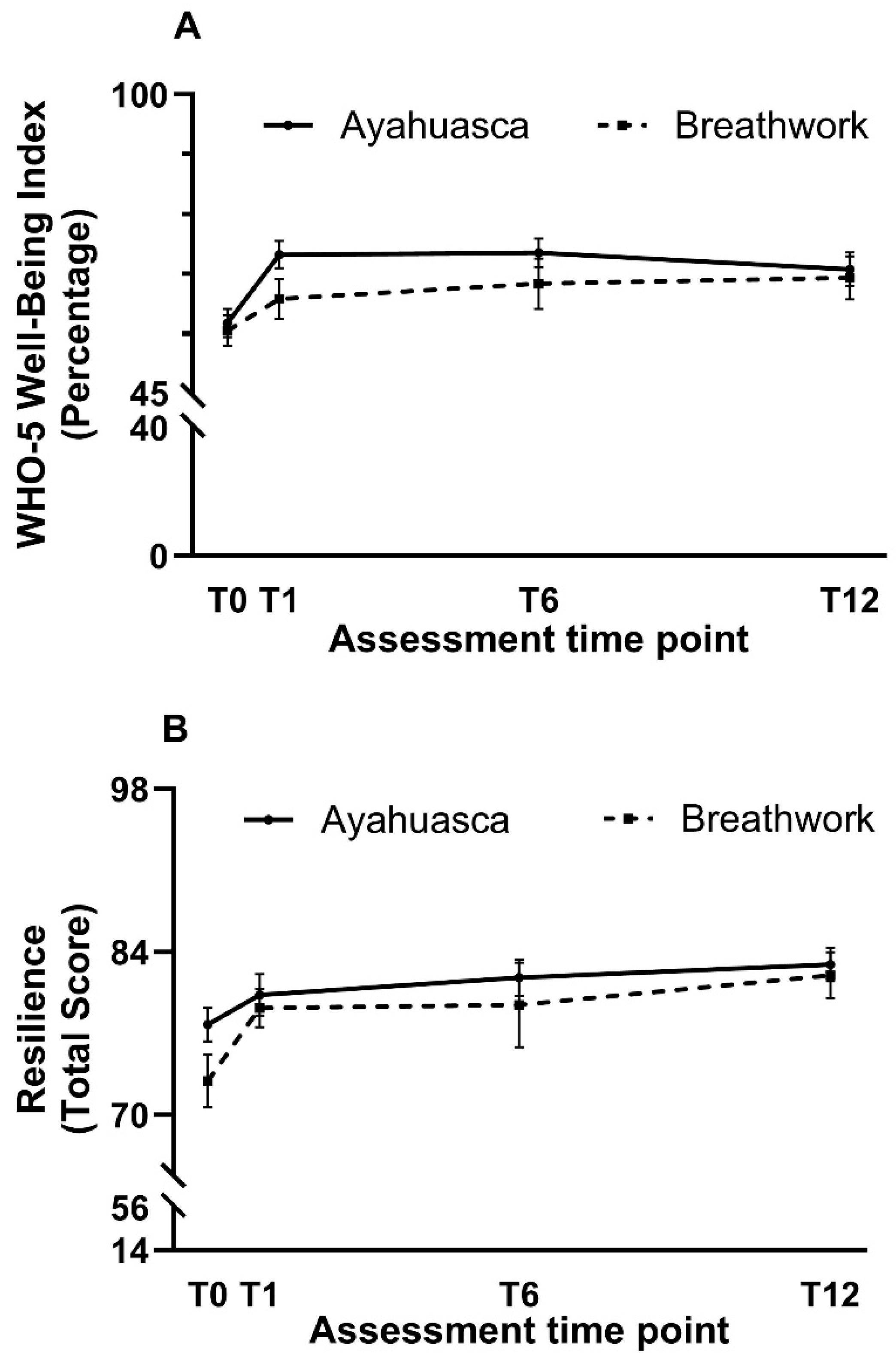
5.4. World Health Organisation-Five Well-Being Index
5.5. The 14-Item Resilience Scale
5.6. Self-Compassion Scale–Short Form
5.6.1. Total Score
5.6.2. Self-Disparagement
5.6.3. Self-Care
5.7. Big Five Inventory-10
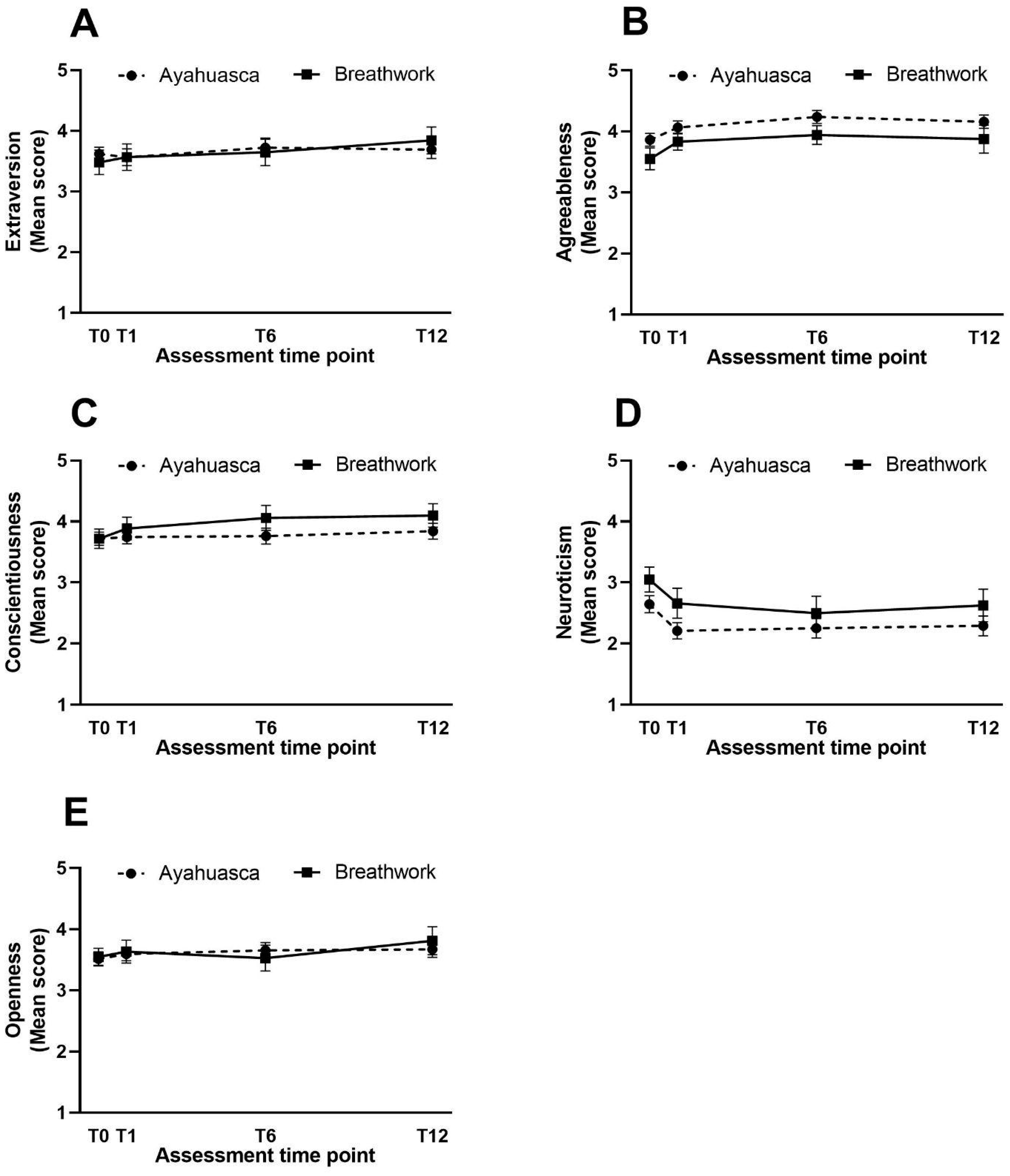
5.7.1. Extraversion
5.7.2. Agreeableness
5.7.3. Conscientiousness
5.7.4. Neuroticism
5.7.5. Openness
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Andersen, K.A.A.; Carhart-Harris, R.; Nutt, D.J.; Erritzoe, D. Therapeutic effects of classic serotonergic psychedelics: A systematic review of modern-era clinical studies. Acta Psychiatr. Scand. 2021, 143, 101–118. [Google Scholar] [CrossRef] [PubMed]
- Malcolm, B.J.; Lee, K.C. Ayahuasca: An ancient sacrament for treatment of contemporary psychiatric illness? Ment. Health Clin. 2017, 7, 39–45. [Google Scholar] [CrossRef]
- McKenna, D.J. Clinical investigations of the therapeutic potential of ayahuasca: Rationale and regulatory challenges. Pharmacol. Ther. 2004, 102, 111–129. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Clavé, E.; Soler, J.; Elices, M.; Pascual, J.C.; Álvarez, E.; de la Fuente Revenga, M.; Friedlander, P.; Feilding, A.; Riba, J. Ayahuasca: Pharmacology, neuroscience and therapeutic potential. Brain Res. Bull. 2016, 126, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Kaasik, H.; Kreegipuu, K. Ayahuasca users in estonia: Ceremonial practices, subjective long-term effects, mental health, and quality of life. J. Psychoact. Drugs 2020, 52, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Kavenská, V.; Simonová, H. Ayahuasca tourism: Participants in shamanic rituals and their personality styles, motivation, benefits and risks. J. Psychoact. Drugs 2015, 47, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Winkelman, M. Drug tourism or spiritual healing? Ayahuasca seekers in amazonia. J. Psychoact. Drugs 2005, 37, 209–218. [Google Scholar] [CrossRef]
- Dos Santos, R.G.; Osório, F.L.; Crippa, J.A.S.; Hallak, J.E.C. Antidepressive and anxiolytic effects of ayahuasca: A systematic literature review of animal and human studies. Braz. J. Psychiatry 2016, 38, 65–72. [Google Scholar] [CrossRef]
- Bouso, J.C.; González, D.; Fondevila, S.; Cutchet, M.; Fernández, X.; Barbosa, P.C.R.; Alcázar-Córcoles, M.; Araújo, W.S.; Barbanoj, M.J.; Fábregas, J.M.; et al. Personality, psychopathology, life attitudes and neuropsychological performance among ritual users of ayahuasca: A longitudinal study. PLoS ONE 2012, 7, e42421. [Google Scholar] [CrossRef]
- Perkins, D.; Pagni, B.A.; Sarris, J.; Barbosa, P.C.R.; Chenhall, R. Changes in mental health, wellbeing and personality following ayahuasca consumption: Results of a naturalistic longitudinal study. Front. Pharmacol. 2022, 13, 884703. [Google Scholar] [CrossRef]
- Odaci, H.; Kaya, F. The adaptation of the connor-davidson resilience scale short forminto turkish: A validity and reliability study. HAYEF J. Educ. 2021, 18, 38–54. [Google Scholar] [CrossRef]
- Färber, F.; Rosendahl, J. The association between resilience and mental health in the somatically ill: A systematic review and meta-analysis. Dtsch. Ärzteblatt Int. 2018, 115, 621. [Google Scholar]
- Oshio, A.; Taku, K.; Hirano, M.; Saeed, G. Resilience and big five personality traits: A meta-analysis. Personal. Individ. Differ. 2018, 127, 54–60. [Google Scholar] [CrossRef]
- Inwood, E.; Ferrari, M. Mechanisms of change in the relationship between self-compassion, emotion regulation, and mental health: A systematic review. Appl. Psychol. Health Well-Being 2018, 10, 215–235. [Google Scholar] [CrossRef] [PubMed]
- Neff, K.D. Self-compassion, self-esteem, and well-being. Soc. Personal. Psychol. Compass 2011, 5, 1–12. [Google Scholar] [CrossRef]
- Zessin, U.; Dickhäuser, O.; Garbade, S. The relationship between self-compassion and well-being: A meta-analysis. Appl. Psychol. Health Well-Being 2015, 7, 340–364. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, L.S.; Rossi, G.N.; Rocha, J.M.; Osório, F.L.; Bouso, J.C.; Hallak, J.E.C.; dos Santos, R.G. Effects of ayahuasca and its alkaloids on substance use disorders: An updated (2016–2020) systematic review of preclinical and human studies. Eur. Arch. Psychiatry Clin. Neurosci. 2022, 272, 541–556. [Google Scholar] [CrossRef]
- Kiraga, M.K.; Mason, N.L.; Uthaug, M.V.; van Oorsouw, K.I.; Toennes, S.W.; Ramaekers, J.G.; Kuypers, K.P.C. Persisting effects of ayahuasca on empathy, creative thinking, decentering, personality, and well-being. Front. Pharmacol. 2021, 12, 721537. [Google Scholar] [CrossRef]
- Weiss, B.; Miller, J.D.; Carter, N.T.; Campbell, W.K. Examining changes in personality following shamanic ceremonial use of ayahuasca. Sci. Rep. 2021, 11, 6653. [Google Scholar] [CrossRef]
- Uthaug, M.V.; Mason, N.L.; Toennes, S.W.; Reckweg, J.T.; de Sousa Fernandes Perna, E.B.; Kuypers, K.P.C.; van Oorsouw, K.; Riba, J.; Ramaekers, J.G. A placebo-controlled study of the effects of ayahuasca, set and setting on mental health of participants in ayahuasca group retreats. Psychopharmacology 2021, 238, 1899–1910. [Google Scholar] [CrossRef]
- Miller, T.; Nielsen, L. Measure of significance of holotropic breathwork in the development of self-awareness. J. Altern. Complement. Med. 2015, 21, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The who-5 well-being index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Wagnild, G.M. The Resilience Scale User’s Guide: For the Us English Version of the Resilience Scale and the 14-Item Resilience Scale (rs-14); The Resilience Center: Tulsa, Oklahoma, 2011. [Google Scholar]
- Raes, F.; Pommier, E.; Neff, K.D.; Van Gucht, D. Construction and factorial validation of a short form of the self-compassion scale. Clin. Psychol. Psychother. 2011, 18, 250–255. [Google Scholar] [CrossRef]
- Hayes, J.A.; Lockard, A.J.; Janis, R.A.; Locke, B.D. Construct validity of the self-compassion scale-short form among psychotherapy clients. Couns. Psychol. Q. 2016, 29, 405–422. [Google Scholar] [CrossRef]
- Rammstedt, B.; John, O.P. Measuring personality in one minute or less: A 10-item short version of the big five inventory in english and german. J. Res. Personal. 2007, 41, 203–212. [Google Scholar] [CrossRef]
- Rammstedt, B.; Kemper, C.; Klein, M.; Beierlein, C.; Kovaleva, A. Big Five Inventory (BFI-10): Zusammenstellung Sozialwissenschaftlicher Items und Skalen; ZIS-GESIS Leibniz Institute for the Social Sciences: Mannheim, Germany, 2014. [Google Scholar]
- Richardson, J.T. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Wilke, J.; Hollander, K.; Mohr, L.; Edouard, P.; Fossati, C.; González-Gross, M.; Ramírez, C.S.; Laiño, F.; Tan, B.; Pillay, J.D.; et al. Drastic reductions in mental well-being observed globally during the covid-19 pandemic: Results from the asap survey. Front. Med. 2021, 8, 578959. [Google Scholar] [CrossRef]
- Bech, P.; Olsen, L.R.; Kjoller, M.; Rasmussen, N.K. Measuring well-being rather than the absence of distress symptoms: A comparison of the sf-36 mental health subscale and the who-five well-being scale. Int. J. Methods Psychiatr. Res. 2003, 12, 85–91. [Google Scholar] [CrossRef]
- Lawn, W.; Hallak, J.E.; Crippa, J.A.; dos Santos, R.; Porffy, L.; Barratt, M.J.; Ferris, J.A.; Winstock, A.R.; Morgan, C.J.A. Well-being, problematic alcohol consumption and acute subjective drug effects in past-year ayahuasca users: A large, international, self-selecting online survey. Sci. Rep. 2017, 7, 15201. [Google Scholar] [CrossRef]
- Grof, S. Holotropic breathwork: A new experiential method of psychotherapy and self-exploration. J. Transpers. Res. 2014, 6, 7–24. [Google Scholar]
- Uthaug, M.V.; Mason, N.L.; Havenith, M.N.; Vancura, M.; Ramaekers, J.G. An experience with holotropic breathwork is associated with improvement in non-judgement and satisfaction with life while reducing symptoms of stress in a czech-speaking population. J. Psychedelic Stud. 2022, 5, 176–189. [Google Scholar] [CrossRef]
- Fincham, G.W.; Kartar, A.; Uthaug, M.V.; Anderson, B.; Hall, L.; Nagai, Y.; Critchley, H.; Colasanti, A. High ventilation breathwork practices: An overview of their effects, mechanisms, and considerations for clinical applications. Neurosci. Biobehav. Rev. 2023, 155, 105453. [Google Scholar] [CrossRef] [PubMed]
- Schmid, J.T.; Jungaberle, H.; Verres, R. Subjective theories about (self-) treatment with ayahuasca. Anthropol. Conscious. 2010, 21, 188–204. [Google Scholar] [CrossRef]
- Domínguez-Clavé, E.; Soler, J.; Elices, M.; Franquesa, A.; Álvarez, E.; Pascual, J.C. Ayahuasca may help to improve self-compassion and self-criticism capacities. Hum. Psychopharmacol. Clin. Exp. 2022, 37, e2807. [Google Scholar] [CrossRef] [PubMed]
- Puente, I. A quasi-experimental study of holorenic breathwork in a psychotherapeutical context: Preliminary results. J. Transpers. Res. 2013, 5, 7–18. [Google Scholar]
- Damian, R.I.; Spengler, M.; Sutu, A.; Roberts, B.W. Sixteen going on sixty-six: A longitudinal study of personality stability and change across 50 years. J. Personal. Soc. Psychol. 2019, 117, 674–695. [Google Scholar] [CrossRef] [PubMed]
- Gooding, P.A.; Hurst, A.; Johnson, J.; Tarrier, N. Psychological resilience in young and older adults. Int. J. Geriatr. Psychiatry 2012, 27, 262–270. [Google Scholar] [CrossRef]
- Kuypers, K.; Riba, J.; De La Fuente Revenga, M.; Barker, S.; Theunissen, E.; Ramaekers, J. Ayahuasca enhances creative divergent thinking while decreasing conventional convergent thinking. Psychopharmacology 2016, 233, 3395–3403. [Google Scholar] [CrossRef]
- Palhano-Fontes, F.; Barreto, D.; Onias, H.; Andrade, K.C.; Novaes, M.M.; Pessoa, J.A.; Mota-Rolim, S.A.; Osório, F.L.; Sanches, R.; dos Santos, R.G.; et al. Rapid antidepressant effects of the psychedelic ayahuasca in treatment-resistant depression: A randomized placebo-controlled trial. Psychol. Med. 2019, 49, 655–663. [Google Scholar] [CrossRef]
- Sarris, J.; Perkins, D.; Cribb, L.; Schubert, V.; Opaleye, E.; Bouso, J.C.; Scheidegger, M.; Aicher, H.; Simonova, H.; Horák, M.; et al. Ayahuasca use and reported effects on depression and anxiety symptoms: An international cross-sectional study of 11,912 consumers. J. Affect. Disord. Rep. 2021, 4, 100098. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ayahuasca Group | Breathwork Group | |
|---|---|---|
| n | 69 | 30 |
| Mean age (SD) | 37.2 (9.2) | 45.9 (12.8) |
| Age range | 22–61 | 27–72 |
| Gender (n (%)) | ||
| Male | 28 (40.6) | 7 (23.3) |
| Female | 40 (58.0) | 23 (76.7) |
| Other | 1 (1.4) | 0 (0.0) |
| Level of education (n (%)) | ||
| Primary | 1 (1.4) | 0 (0.0) |
| Secondary | 6 (8.7) | 5 (16.7) |
| Tertiary | 62 (89.8) | 25 (83.3) |
| Daily occupation (n (%)) | ||
| Learning/studying | 4 (5.8) | 3 (10.0) |
| Physical work | 4 (5.8) | 1 (3.3) |
| Computer/office work | 19 (27.5) | 13 (43.3) |
| Working with people | 36 (52.2) | 9 (30.0) |
| Travelling | 1 (1.4) | 0 (0.0) |
| Creative work | 5 (7.2) | 4 (13.3) |
| Diagnosed with mental illness (n (%)) | ||
| Yes | 15 (22.1) | 12 (40.0) |
| No | 54 (78.3) | 18 (60.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khubsing, R.S.I.; Leerdam, M.v.; Haijen, E.C.H.M.; Kuypers, K.P.C. Self-Rated Effectiveness of Ayahuasca and Breathwork on Well-Being, Psychological Resilience, Self-Compassion, and Personality: An Observational Comparison Study. Psychoactives 2024, 3, 167-183. https://doi.org/10.3390/psychoactives3020011
Khubsing RSI, Leerdam Mv, Haijen ECHM, Kuypers KPC. Self-Rated Effectiveness of Ayahuasca and Breathwork on Well-Being, Psychological Resilience, Self-Compassion, and Personality: An Observational Comparison Study. Psychoactives. 2024; 3(2):167-183. https://doi.org/10.3390/psychoactives3020011
Chicago/Turabian StyleKhubsing, Rishma S. I., Martin van Leerdam, Eline C. H. M. Haijen, and Kim P. C. Kuypers. 2024. "Self-Rated Effectiveness of Ayahuasca and Breathwork on Well-Being, Psychological Resilience, Self-Compassion, and Personality: An Observational Comparison Study" Psychoactives 3, no. 2: 167-183. https://doi.org/10.3390/psychoactives3020011
APA StyleKhubsing, R. S. I., Leerdam, M. v., Haijen, E. C. H. M., & Kuypers, K. P. C. (2024). Self-Rated Effectiveness of Ayahuasca and Breathwork on Well-Being, Psychological Resilience, Self-Compassion, and Personality: An Observational Comparison Study. Psychoactives, 3(2), 167-183. https://doi.org/10.3390/psychoactives3020011