
Beyond Statins: Novel Lipid-Lowering Agents for Reducing Risk of Atherosclerotic Cardiovascular Disease

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
3. The Statin-Based Approach to ASCVD
Limitations to Statin-Based Therapies
4. LDL-Lowering Therapies

{kind=link}
{kind=link}
| Drug, Mechanism | Indication on FDA Label | Dosage, Route, Side Effects (SE) |
|---|---|---|
| Ezetimibe Inhibits serol NPC1L1 | As an adjunct to statin and diet to ↓ LDL-C in adults with 1° HLD including HeFH | Dose: 10 mg daily. Route: Oral. SE: Diarrhea, arthralgia, upper respiratory infection, flu-like symptoms |
| Bempedoic acid Inhibits ATP citrate lyase | As an adjunct to diet and maximally tolerated statins for LDL-C reduction in (a) patients with ASCVD and (b) adults with HeFH | Dose: 180 mg daily. Route: Oral. SE: Hyperuricemia, myopathy, leukopenia, thrombocytopenia, ↑ liver enzymes |
| Ezetimibe + bempedoic acid | As an adjunct to diet and maximally tolerated statins for LDL-C reduction in (a) patients with ASCVD and (b) adults with HeFH | Dose: 180 mg bempedoic acid, 10 mg ezetimibe daily. Route: Oral. SE: Upper respiratory infection, muscle spasms, hyperuricemia, back/abdominal pain, bronchitis, anemia, ↑ liver enzymes, diarrhea |
| Fibrates Agonizes PPAR-α | As an adjunct to diet (a) in patients with 1° HLD or mixed HLD to ↓ LDL-C, TC, TG, apoB, and ↑ HDL-C, and (b) in patients with severe hypertriglyceridemia for TG ↓ | Dose: 200 mg TID (bezafibrate), 100–200 mg PO daily (ciprofibrate), 34–201 mg QD (fenofibrate), 60 mg PO BID (gemfibrozil). Route: Oral. SE: Abdominal pain, constipation, myopathy, ↑ liver enzymes, ↑ Cr |
| Alirocumab, evolocumab Antibody that inhibits PCSK9’s interaction with LDL-C receptors | (a) To ↓ risk of MI, UA, and stroke requiring hospitalization in adults with ASCVD; (b) as adjunct to diet, alone or with LDL-C-lowering therapies in adults with 1° HLD and HeFH; (c) as adjunct to LDL-C-lowering therapies in adults with HoFH | Dose for alirocumab: 75 mg/mL biweekly, 150 mg/mL biweekly, 300 mg monthly. Dose for evolocumab: (a) In adults with ASCVD or 1° HLD: 140 mg biweekly, 420 mg monthly; (b) in patients with HoFH: 420 mg monthly. Route: Subcutaneous. SE: Nasopharyngitis, injection site reactions, flu-like symptoms, myalgia, non-cardiac chest pain |
| Nicotinic acid Inhibits hormone-sensitive lipase | To ↓ TC, LDL-C, TG, and Apo B levels, and increase HDL-C, in patients with 1° HLD and mixed HLD | Dose: 500 mg–2000 mg daily. Route: Oral. SE: Flushing, diarrhea, nausea, vomiting, increased cough, pruritus |
| Inclisiran Binds to PCSK9 mRNA | Use in conjunction with statins and diet for LDL-C ↓ in patients with (a) 1° HLD or mixed HLD, or (b) HeFH | Dose: 284 mg/mL every 6 months (second dose is provided at 3 months, every 6 months afterwards). Route: Subcutaneous. SE: Injection site reactions, arthralgia, bronchitis |
| Mipomersen Inhibits ApoB synthesis | As an adjunct to diet for additional ↓ of LDL-C, apoB, TC, and non-HDL-C in patients with HoFH | Dose: 200 mg weekly. Route: Subcutaneous. SE: Injection site reactions, flu-like symptoms, ↑ liver enzymes |
| Lomitapide Blocks VLDL assembly | As an adjunct to diet for additional ↓ of LDL-C, apoB, TC, and non-HDL-C in patients with HoFH | Dose: 5–60 mg daily. Route: Oral. SE: Diarrhea, nausea, dyspepsia, abdominal pain |
| Icosapent ethyl Reduces hepatic VLDL-TG synthesis/secretion | (1) As an adjunct to maximally tolerated statins to ↓ incidence of CV events in adults with elevated TG > 150 mg/dL and (a) ASCVD or (b) diabetes mellitus and two or more additional risk factors for CVD. (2) As an adjunct to diet to decrease TG levels in adults with TG > 500 mg/dL | Dose: 0.5 mg daily, 1 mg BID. Route: Oral. SE: Atrial fibrillation/flutter, bleeding (especially with anticoagulant and antiplatelet use), allergic reactions in patients with fish allergy, GI dysfunction |
| Trial, Sample Size | Study Population | Intervention and Comparator | 1° Outcome, Follow-Up Period | 1° Outcome Result |
|---|---|---|---|---|
| Cannon (2015) IMPROVE-IT [18] n = 18,144 | 2° prevention—Patients ≥ 50 years old stabilized within 10 days of an ACS with LDL-C between 50 and 100 mg/dL if on statins, and between 50 and 125 mg/dL if not receiving statins | Intervention: Simvastatin 40 mg daily in combination with ezetimibe 10 mg daily. Comparator: Simvastatin 40 mg daily in combination with placebo. | A composite of CV death, MI, documented unstable angina requiring hospital admission, PCI/CABG ≥ 30 days after randomization, and non-fatal stroke. F/U: 6 years | Kaplan–Meier event rate for 1° outcome was 32.7% in the simvastatin–ezetimibe group, and 34.7% in the simvastatin monotherapy group (absolute risk difference, 2.0 percentage points; HR, 0.936; 95% CI, 0.89 to 0.99; p = 0.016) |
| Ouchi (2019) EWTOPIA 75 [19] n = 3796 | 1° and 2° prevention—Patients ≥ 75 y/o with elevated LDL-C ≥ 140 mg/dL and no history of CAD | Intervention: Oral ezetimibe 10 mg daily. Control: Usual care (no placebo). | A composite of sudden cardiac death, myocardial infarction, coronary revascularization, or stroke. F/U: 4.1 years | Ezetimibe significantly ↓ the incidence of the 1° outcome (HR, 0.66; 95% CI, 0.50–0.86; p = 0.002) |
| Tsujita (2015): PRECISE-IVUS [20] n = 202 | 2° prevention—Patients 30–85 years of age with CAD, with LDL-C ≥ 100 mg/dL, who underwent successful coronary angiography or percutaneous coronary intervention (PCI) to treat ACS or stable angina pectoris | Intervention: Atorvastatin + ezetimibe 10 mg/day. Comparator: Atorvastatin alone | Absolute change in percent atheroma volume (PAV). F/U: 9–12 months | A −1.538% difference in PAV between intervention and control (95% CI: −3.079% to 0.003%). Absolute change in PAV showed superiority for the dual lipid-lowering strategy (−1.4%; 95% CI: −3.4% to −0.1% vs. −0.3%; 95% CI: −1.9% to 0.9% with atorvastatin alone; p = 0.001). |
| Trial, Sample Size | Study Population | Intervention and Comparator | 1° Outcome, Follow-Up Period | 1° Outcome Result |
|---|---|---|---|---|
| Ballantyne (2018) CLEAR Tranquility [21] n = 269 | 1° and 2° prevention—Patients ≥ 18 y/o with statin intolerance or on no statin with LDL-C ≥ 100 mg/dL | Intervention: Oral bempedoic acid 180 mg daily + ezetimibe 10 mg daily. Comparator: Oral placebo daily + ezetimibe 10 mg daily. | Percent change in LDL-C level at week 12. F/U: 12 weeks | Bempedoic acid resulted in a placebo-corrected difference in mean change in LDL-C of −28.5% (95% CI: −34.4%, −22.5%; p < 0.001) |
| Ray (2019) CLEAR Harmony [22] n = 2230 | HeFH and 2° prevention—Patients ≥ 18 years old with ASCVD, HeFH, or both, with LDL-C ≥ 70 mg/dL, on a maximally tolerated statin | Intervention: Oral bempedoic acid 180 mg daily. Comparator: Oral placebo daily. | Overall safety (incidence of AEs and changes in laboratory safety values). F/U: 52 weeks | Bempedoic acid resulted in a ↓ in the mean LDL-C level by 19.2 mg/dL, a change of −16.5% from baseline, and a placebo-corrected difference of −18.1% (95% CI, −20.0 to −16.1; p < 0.001) |
| Goldberg (2019) CLEAR Wisdom [23] n = 779 | HeFH and 2° prevention—Patients ≥ 18 years old with ASCVD, HeFH, or both, with LDL-C ≥ 70 mg/dL, on maximally tolerated LLT | Intervention: oral bempedoic acid 180 mg daily. Comparator: oral placebo daily. | Percent change in LDL-C level at week 12. F/U: 52 weeks | Bempedoic acid resulted in a −15.1% change from baseline in LDL-C levels (placebo-corrected difference of −17.4% [95% CI, −21.0% to −13.9%]; p < 0.001) |
| Laufs (2019) CLEAR Serenity [24] n = 345 | 1° and 2° prevention—Patients ≥ 18 years old with statin intolerance with LDL-C ≥ 130 mg/dL (1° prevention) and ≥ 100 mg/dL (2° prevention) | Intervention: Oral bempedoic acid 180 mg daily. Comparator: Oral placebo daily. | Percent change in LDL-C level at week 12. F/U: 24 weeks | Bempedoic acid resulted in a placebo-corrected difference of −21.4% in LDL-C levels [95% CI, −25.1% to −17.7%]; p < 0.001 |
| Nissen (2023) CLEAR Outcomes [25] n = 13,970 | 1° and 2° prevention—Patients 18–85 years old with or at high risk of ASCVD, statin intolerance, and LDL-C ≥ 100 mg/dL | Intervention: Oral bempedoic acid 180 mg daily. Comparator: Oral placebo daily. | A composite of CV death, non-fatal MI, non-fatal stroke, or coronary revascularization. F/U: 40.6 months | The incidence of a 1° endpoint event was significantly lower with bempedoic acid than with the placebo (11.7% vs. 13.3%; HR, 0.87; 95% CI 0.79 to 0.96; p = 0.004) |
| Trial | Study Population | Intervention and Comparator | 1° Outcome, Follow-Up Period | 1° Outcome Data |
|---|---|---|---|---|
| Koren (2014) MENDEL-2 [26] n = 614 | 1° prevention—Patients aged 18 to 80 years with LDL-C ≥ 100 mg/dL and <190 mg/dL, TG ≤ 400 mg/dL, and 10-year Framingham coronary heart disease risk scores ≤ 10% | Interventions: Oral placebo and evolocumab 140 mg biweekly, or oral placebo and evolocumab 420 mg monthly. Comparators: Oral placebo and subcutaneous placebo biweekly; oral placebo and subcutaneous placebo monthly; ezetimibe and subcutaneous placebo every two weeks; ezetimibe and subcutaneous placebo monthly. | Percent change in LDL-C level averaged at weeks 10 and 12, and at week 12 | At 12 weeks: −57.1% (−61.1, −53.1) biweekly evolocumab vs. placebo; −39.3% (−43.3, −35.3) biweekly evolocumab vs. ezetimibe; −54.8% (−58.5, −51.1) monthly evolocumab vs. placebo; −37.6% (−41.2, −33.9) monthly evolocumab vs. ezetimibe |
| Robinson (2014) LAPLACE-2 [27] n = 1896 | 1° prevention—Patients aged 18 to 80 years with LDL-C ≥ 150 mg/dL if not on statins at screening, ≥100 mg/dL if on non-intensive statin, or ≥80 mg/dL if on intensive statins, and TG < 400 mg/dL | Intervention: Evolocumab (140 mg biweekly or 420 mg monthly). Comparator: Matching placebo or ezetimibe (10 mg or placebo daily; atorvastatin patients only) | Percent change from baseline in LDL-C level at the mean of weeks 10 and 12, and at week 12 | |
| Stroes (2014) GAUSS-2 [28] n = 307 | 1° prevention—Patients aged 18 to 80 years on no or low-dose statins, with LDL-C ≥ 70 mg/dL, and who had previous intolerance to ≥2 statins | Interventions: Oral placebo and subcutaneous evolocumab 140 mg biweekly, or oral placebo and evolocumab 420 mg monthly. Comparators: daily ezetimibe 10 mg and subcutaneous placebo every two weeks; daily ezetimibe 10 mg and subcutaneous placebo monthly. | Percent change in LDL-C at the mean of weeks 10 and 12, and at week 12 | Difference between evolocumab and ezetimibe at 12 weeks at the following doses: Evolocumab 140 mg biweekly + placebo daily: −36.9% (−42.3, −31.6). Evolocumab 420 mg monthly + placebo daily: −38.7% (−43.1, −34.3) |
| Blom (2014) DESCARTES [29] n = 901 | 1° and 2° prevention—Patients aged 18 to 75 years with LDL-C ≥ 75 mg/dL, and a TG < 400 mg/dL | Intervention: Evolocumab (420 mg) monthly. Comparator: placebo every 4 weeks. Background LLT included diet alone or diet plus atorvastatin | Percent change in LDL-C at week 52 | Treatment differences, baseline vs. placebo: Diet only: −63.8% (4.2); Diet + atorvastatin 10 mg: −64.4% (2.8); Diet + atorvastatin 80 mg: −57.9% (5.9); Diet + atorvastatin 80 mg + ezetimibe 10 mg: −49.1% (5.6); Overall: −59.3% (2.3) |
| Raal (2015) RUTHERFORD-2 [30] n = 331 | 1° prevention—Patients aged 18 to 80 years with HeFH and on a stable dose of a statin | Intervention: Evolocumab 140 mg biweekly or 420 mg monthly. Comparator: Matching placebo biweekly or monthly | Percent change in LDL-C at week 12, and at the mean of weeks 10 and 12 | Treatment differences (95% CI) from baseline: Evolocumab 140 mg every 2 weeks vs. placebo: −59.2% (−65.1 to −53.4); Evolocumab 420 mg monthly vs. placebo: −61·3% (−69.0 to −53.6) |
| Sabatine (2015) OSLER-2 [31] n = 3141 | Patients recruited from parent trials ranged from LDL-C ≥ 85 mg/dL to ≥100 mg/dL, including patients on statins and those with statin intolerance | Intervention: Evolocumab (140 mg biweekly or 420 mg monthly) plus standard therapy. Comparator: standard therapy alone | Incidence of adverse events. F/U: a median of 11.1 months | Adverse events occurred in 2060 of 2976 patients (69.2%) in the evolocumab group, and in 965 of 1489 patients (64.8%) in the standard therapy group |
| Nissen (2016) GAUSS-3 [32] n = 199 | 1° and 2° prevention—Patients aged 18 to 80 years with LDL-C ≥ 100 mg/dL if CAD, ≥130 mg/dL if ≥2 risk factors, ≥160 mg/dL with ≥1 risk factor, or ≥190 mg/dL with no risk factors, and statin intolerance | Intervention: Evolocumab injections (420 mg) monthly. Comparator: Oral ezetimibe (10 mg) daily, or matched placebo | Percent change in LDL-C at week 24 for evolocumab vs. ezetimibe, and percent change in LDL-C at weeks 22 and 24 for evolocumab vs. ezetimibe | At week 24 for evolocumab vs. ezetimibe: −52.8% vs. −16.7%, p < 0.001; At weeks 22 and 24 for evolocumab vs. ezetimibe: −54.5% vs. −16.7%, p < 0.001 |
| Sabatine (2017) FOURIER [33] n = 27,564 | 2° prevention—Patients aged 40 to 85 years with ASCVD, one major risk factor (T1DM, T2DM, age ≥ 65, or current smoking), or two minor risk factors with LDL-C ≥ 70 mg/dL or a non-HDL-C ≥ 100 mg/dL on stable LLT | Intervention: Subcutaneous injections of evolocumab (either 140 mg every 2 weeks or 420 mg monthly, according to patient preference). Comparator: Subcutaneous injections of matching placebo. | A composite of CV death, MI, stroke, hospitalization for unstable angina, or coronary revascularization. F/U: A median of 2.2 years | The 1° endpoint occurred in 1344 patients (9.8%) in the evolocumab group vs. 1563 patients (11.3%) in the placebo group. HR (95% CI) 0.85 (0.79 to 0.92) p < 0.001 |
| Rosenson (2019) BANTING [34] n = 421 | 1° and 2° prevention—Patients aged 18 years and older with T2DM on stable pharmacological therapy for T2DM and the maximum tolerated statin dose | Intervention: Evolocumab 420 mg once per month. Comparator: Placebo once per month | Percent change in LDL-C from baseline to week 12, and at the mean of weeks 10 and 12 | Week 12 results: −54.3% (1.4). Mean treatment difference: −53.1% (2.3). |
| O’Donoghue (2022) FOURIER-OLE [35] n = 6635 | 2° prevention—Patients with a history of established ASCVD and LDL-C ≥ 70 mg/dL or non–HDL-C ≥ 100 mg/dL on statin therapy | Original parent trial: Intervention was evolocumab, comparator was placebo. This open-label trial administered evolocumab at either 140 mg every 2 weeks or 420 mg every month, per patient preference | Subject incidence of treatment-emergent adverse events. F/U: a median of 5.0 years | Overall annualized incidence rates for safety events of interest for patients randomized to evolocumab did not exceed the annualized incidence rate for patients treated with the placebo |
| Nicholls (2021) HUYGENS [36] n = 164 | 2° prevention—Patients ≥ 18 years with at least one non-culprit epicardial coronary stenosis ≥ 20% on angiography during NSTEMI, with intervention of the culprit lesion and a target vessel suitable for imaging with ≤50% visual obstruction, on maximally tolerated statin and LDL-C at the time of NSTEMI ≥ 130 mg/dL if not taking a statin, ≥80 mg/dL if on a low- or moderate-intensity statin, or ≥60 mg/dL if on a high-intensity statin | Intervention: Evolocumab 420 mg once per month. Comparator: Placebo once per month | Nominal change in minimum fibrous cap thickness at any point throughout the matched arterial segment, defined by proximal and distal side branches, from baseline to week 50 | Greater increase in minimum fibrous cap thickness (+42.7 vs. +21.5 μm; p = 0.015) and decrease in maximum lipid arc (−57.5 vs. −31.4; p = 0.04) and macrophage index (−3.17 vs. −1.45 mm; p = 0.04) throughout the arterial segment, with similar findings in lipid-rich plaque regions, and greater regression of % atheroma volume (−2.29% ± 0.47% vs. −0.61% ± 0.46%; p = 0.009) in the evolocumab groups |
| TIMI (ongoing) VESALIUS-CV [37] n = 12,301 | 1° prevention—Patients aged ≥ 50 (men) or ≥55 (women) and ˂80 years of age with LDL-C ≥ 90 mg/dL or non-HDL-C ≥ 120 mg/dL, or apoB ≥ 80 mg/dL without prior MI or stroke, and with evidence of CAD, atherosclerotic cerebrovascular disease, PAD, DM, and at least one high-risk factor | Intervention: Evolocumab 140 mg biweekly. Comparator: Placebo biweekly | A composite of coronary death, MI, and ischemic stroke. F/U: a median of 4.5 years | Not yet published |
| (Ongoing) EVOLVE-MI (NCT05284747) n = 4000 | 2° prevention—Patients aged 18 years and older hospitalized for NSTEMI or STEMI due to presumed atherosclerotic disease | Intervention: Open-label evolocumab biweekly plus routine lipid management. Comparator: Routine lipid management | Total (first and subsequent) composite of MI, ischemic stroke, any arterial revascularization procedure, and all-cause death. F/U: a median of 3.5 years | Not yet published |
| (Not yet published) YELLOW III (NCT04710368) n = 137 | 1° prevention—Patients undergoing elective PCI with a non-obstructive lesion (30–50% stenosis identified by angiography in a non-culprit vessel with lipid-rich plaques) and an optimal background statin | Intervention: Subcutaneous evolocumab 140 mg biweekly. No comparator | Changes in the minimal fibrous cap thickness, by OCT, and max 4 mm lipid core burden index, by near-infrared spectroscopy at week 26 | Not yet published |
| Trial | Study Population | Intervention and Comparator | 1° Outcome, Follow-Up Period | 1° Outcome Data |
|---|---|---|---|---|
| Schwartz (2018) and Szarek (2019) ODYSSEY Outcomes [38] n = 18,924 | 2° Prevention—Patients ≥ 40 years old hospitalized for an ACS and with inadequate lipid control (LDL-C ≥ 70 mg/dL, non-HDL-C ≥ 100 mg/dL, or apoB ≥ 80 mg/dL) on a maximally tolerated dose | Intervention: Subcutaneous injections of alirocumab 75 mg every 2 weeks. Comparator: Subcutaneous injections of matched-dose placebo every 2 weeks. | A composite of coronary death, non-fatal MI, fatal or non-fatal ischemic stroke, and hospitalization for unstable angina. F/U: median of 2.8 years | The composite 1° endpoint event occurred in 903 patients (9.5%) in the alirocumab group and in 1052 patients (11.1%) in the placebo group. HR (95% CI) 0.85 (0.78–0.93), p < 0.001) |
| Robinson (2015) ODYSSEY LONG TERM [39] n = 2341 | 1° and 2° prevention—Patients aged 18 and older with LDL-C ≥ 70 mg/dL and with HeFH, ASCVD, or high-risk 1° prevention, including CKD or DM with additional risk factors, on maximally tolerated statins | Intervention: Subcutaneous injections of alirocumab 150 mg every two weeks. Control: Subcutaneous injections of matched placebo every two weeks. | Percent change in LDL-C level at week 24 | At week 24, the difference between the alirocumab and placebo groups was −62% (p < 0.001) |
| Moriarty (2015) ODYSSEY ALTERNATIVE [40] n = 314 | 1° prevention—Patients aged 18 years and older with statin intolerance, and at a moderate, high, or very high CV risk | Intervention: Subcutaneous injections of alirocumab 75 mg every 2 weeks. Comparators: Ezetimibe 10 mg daily or atorvastatin 20 mg daily | Percent change in LDL-C at week 24 | Percent change from baseline: −45.0% (2.2). Comparator-corrected difference: −30.4% (3.1), CI −36.6 to −24.2, p < 0.0001 |
| Kastelein (2015) ODYSSEY FH I [41] n = 486 | 1° and 2° prevention—Patients with HeFH without a history of CV events, or patients with a history of MI or ischemic stroke, and with LDL-C levels not on target according to current guidelines | Intervention: Alirocumab 75 mg every 2 weeks. Comparator: Placebo every 2 weeks. | Percent change in LDL-C at week 24 | Percent change from baseline: −48.8% (1.6). Placebo-corrected difference: −57.9% (2.7), CI −63.3% to −52.6%, p < 0.0001 |
| Kastelein (2015) ODYSSEY FH II [41] n = 249 | 1° and 2° prevention—Patients with HeFH without a history of CV events, or patients with a history of MI or ischemic stroke, and with LDL-C levels not on target according to current guidelines | Intervention: Alirocumab 75 mg every 2 weeks. Comparator: Placebo every 2 weeks | Percent change in LDL-C at week 24 | Percent change from baseline: −48.7% (1.9). Placebo-corrected difference: −51.4% (3.4), CI −58.1% to −44.8%, p < 0.0001 |
| Ginsberg (2016) ODYSSEY HIGH FH [42] n = 107 | 1° and 2° prevention—Patients with HeFH and LDL-C ≥ 160 mg/dL on a maximally tolerated statins | Intervention: Subcutaneous alirocumab 150 mg every 2 weeks. Comparator: Placebo every 2 weeks | Percent change in LDL-C at week 24 | Percent change from baseline: −45.7% (3.5). Placebo-corrected difference: −39.1% (6.0), CI −51.1% to −27.1%, p < 0.0001 |
| Bays (2015) ODYSSEY OPTIONS I [43] n = 355 | 1° and 2° prevention—Patients aged 18 years and older at very high risk of CVD (a history of CVD including CHD, or T2DM with target organ damage) and with LDL-C ≥ 70 mg/dL, or at high risk (no history of CVD or CHD but with other risk factors: 10-year risk of fatal CVD of 5% or greater, moderate CKD, or T2DM with no target organ damage) and with LDL-C ≥ 100 mg/dL | Intervention: Subcutaneous injections of alirocumab 75 mg. Comparators: Add-on therapy with ezetimibe 10 mg daily, doubling of atorvastatin dose to 80 mg daily, or a switch to rosuvastatin 40 mg daily | Percent change in LDL-C at week 24 | Atorvastatin 20 mg group: Alirocumab −44.1% vs. ezetimibe −20.5% (p < 0.001) and doubling of atorvastatin dose −5.0% (p < 0.001). Atorvastatin 40 mg group: Alirocumab −54.0% (p < 0.001), ezetimibe −22.6% (p < 0.001), doubling of atorvastatin dose 4.8% (p < 0.001), and switching atorvastatin 40 mg to rosuvastatin 40 mg −21.4% (p < 0.001) |
| Farnier (2016) ODYSSEY OPTIONS II [44] n = 305 | 1° and 2° prevention—Patients with hypercholesterolemia at very high or high risk of CV, receiving rosuvastatin 10 or 20 mg/day | Intervention: Add-on subcutaneous injection via a prefilled pen of alirocumab 75 mg every 2 weeks. Comparators: Add-on ezetimibe 10 mg daily, or double-dose rosuvastatin | Percent change in LDL-C at week 24 | Rosuvastatin 10 mg group: Alirocumab −50.6% vs. ezetimibe −14.4% (p < 0.0001) and double-dose rosuvastatin −16.3% (p < 0.0001). Rosuvastatin 20 mg group: Alirocumab −36.3% vs. ezetimibe −11.0% (p = 0.0136) and double-dose rosuvastatin −15.9% (p < 0.0453) [pre-specified threshold for significance (p < 0.0125)] |
| Kereiakes (2015) ODYSSEY COMBO I [45] n = 316 | 1° and 2° prevention—Patients aged 18 years and older with LDL-C ≥ 70 mg/dL and established CVD, or LDL-C ≥ 100 mg/dL with CHD risk equivalents (DM with other risk factors or CKD) | Intervention: Alirocumab (75 mg) every 2 weeks. Comparator: Placebo every 2 weeks | Percent change in LDL-C at week 24 | Percent change from baseline: −48.2% (95% CI −52.0 to −44.4). Placebo-corrected difference: −45.9 (95% CI −52.5 to −39.3), p < 0.0001 |
| Cannon (2015) ODYSSEY COMBO II [46] n = 720 | 1° and 2° prevention—Patients with HLD and established CHD or CHD risk equivalents (ischemic stroke, PAD, moderate CKD, or DM plus ≥2 additional risk factors), on maximally tolerated statins | Intervention: Subcutaneous injections of alirocumab 75 mg every 2 weeks plus oral placebo. Comparator: Oral ezetimibe 10 mg daily plus subcutaneous placebo | Percent change in LDL-C at week 24 | Percent change from baseline: −50.6% (1.4). Placebo-corrected difference: −29.8% (2.3; 95% CI −34.4 to −25.3), p < 0.0001 |
| Roth (2016) ODYSSEY CHOICE I [47] n = 803 | 1° and 2° prevention—Patients with T2DM and inadequately controlled hypercholesterolemia and who were at moderate CVD risk with no statin, moderate-to-very-high CVD risk with statin-associated muscle symptoms, or moderate-to-very-high CVD risk with maximally tolerated statins | Intervention: Alirocumab 300 mg monthly. Comparator: Matching placebo monthly | Percent change in LDL-C at week 24 and time-averaged LDL-C over weeks 21 to 24 | Percent change from baseline: −57.4% (3.3). Placebo-corrected difference: −61.6% (5.6), p < 0.0001 |
| Stroes (2016) ODYSSEY CHOICE II [48] n = 233 | 1° prevention—Patients aged 18 years and older with hypercholesterolemia receiving fenofibrate, ezetimibe, or diet alone | Intervention: Alirocumab 150 mg monthly or 75 mg biweekly, with dose adjustment to 150 mg biweekly at week 12 if predefined LDL-C target levels were not met. Comparator: Matching placebo | Percent change in LDL-C at week 24 | Alirocumab 75 mg biweekly: % change from baseline −53.5% (1.6). Placebo-corrected difference: −58.2% (2.8), p < 0.0001. Alirocumab 150 mg monthly: % change from baseline −51.7% (2.3). Placebo-corrected difference: −56.4% (3.3), p < 0.0001 |
| Teramoto (2016) ODYSSEY JAPAN [49] n = 216 | 1° and 2° prevention—Patients aged 18 and older with HeFH, with or without a history of documented CAD, or patients with non-FH at high CVD risk with a history of documented CAD, or classified as JAS category III (1° prevention), with inadequately controlled cholesterol levels | Intervention: Alirocumab 75 mg every 2 weeks, with increase to 150 mg if predefined LDL-C target levels were not met. Comparator: Matching placebo | Percent change in LDL-C at week 24 | Percent change from baseline: −62.5% (1.3). Placebo-corrected difference: −64.1% (2.2; 95% CI −68.5% to −59.8%), p < 0.0001 |
| Koh (2018) ODYSSEY KT [50] n = 199 | 1° prevention—Patients aged 18 years or older with high CV risk who had inadequately controlled hypercholesterolemia on maximally tolerated statins | Intervention: Alirocumab 75 mg every 2 weeks, with dose increase to 150 mg every 2 weeks at week 12 if predefined LDL-C target levels were not met. Comparator: Matching placebo | Percent change in LDL-C at week 24 | Percent change from baseline: −57.1% (3.0). Placebo-corrected difference: −63.4% (4.2; 95% CI −71.6 to −55.2), p < 0.0001 |
| Teramoto (2019) ODYSSEY NIPPON [51] n = 163 | 1° prevention—Patients with LDL-C ≥ 100 mg/dL (HeFH or non-FH with CHD) or LDL-C ≥ 120 mg/dL (non-FH, Japan Atherosclerosis Society category III) on atorvastatin 5 mg/day or non-statin LLT | Intervention: Subcutaneous alirocumab 150 mg monthly or alirocumab 150 mg biweekly. Comparator: Matching placebo | Percent change in LDL-C at week 12 | Alirocumab monthly: % change from baseline −43.8% (2.2). Placebo-corrected difference: −39.5% (3.1), p < 0.0001 Alirocumab biweekly: % change from baseline −70.1% (2.3). Placebo-corrected difference: −65.8% (3.1), p < 0.0001 |
| Han (2020) ODYSSEY EAST [52] n = 615 | 1° and 2° prevention—Patients with hypercholesterolemia and established CHD or CHD risk equivalents who were inadequately controlled with stable maximally tolerated statins | Intervention: Alirocumab 75 mg every 2 weeks, with dose increase to 150 mg biweekly at week 12 if predefined LDL-C target levels were not met. Comparator: Ezetimibe 10 mg daily | Percent change in LDL-C at week 24 | Percent change from baseline: −56.0% (1.5). Placebo-corrected difference: −35.6 (2.5; 95% CI −40.6 to −30.7), p < 0.0001 |
| Perez de Isla (2023) ARCHITECT [53] n = 104 | 1° prevention—Patients with FH, without clinical ASCVD, with LDL-C ≥ 100 mg/dL on maximal statins, a global coronary PB > 30% at baseline, and prescribed alirocumab by the treating physician | Intervention: Subcutaneous alirocumab (150 mg) every 14 days. Comparator: No comparator | Changes in coronary plaque burden. F/U: 78 weeks | Coronary plaque burden changed from 34.6% (32.5 to 36.8) to 30.4% (27.4 to 33.4) at follow-up, p < 0.001. There was an increase in the proportion of calcified (+0.3%; p < 0.001) and mainly fibrous (+6.2%; p < 0.001) plaque, and a decrease in the % fibro-fatty (−3.9%; p < 0.001) and necrotic plaque (−0.6%; p < 0.001). |
| Sugizaki (2020) ALTAIR [54] n = 24 | 1° prevention—Patients aged 20 years and older who underwent PCI for ACS or stable angina pectoris, with LDL-C > 70 mg/dL despite statin treatment, and OCT evaluation of TCFA characteristics in non-culprit, angiographically intermediate lesions causing 30–70% diameter stenosis | Intervention: Alirocumab 75 mg every 2 weeks and 10 mg rosuvastatin daily. Comparator: Standard-of-care 10 mg rosuvastatin daily | Absolute change in fibrous cap thickness. F/U: 36 weeks | The absolute increase in the fibrous cap thickness was 140 μm (78 to 163 μm) (%age change 273% [155% to 293%]) in the alirocumab group vs. 45 μm (10 to 78 μm) in the standard-of-care group (100% [20% to 155%]), p = 0.002 |
| Räber (2022) PACMAN-AMI [55] n = 300 | 2° prevention—Patients aged 18 years and older who underwent PCI for STEMI or NSTEMI, with LDL-C > 125 mg/dL, and who were suitable for intracoronary imaging | Intervention: Subcutaneous injections of alirocumab 150 mg biweekly. Comparator: Placebo biweekly | Change in intravascular ultrasound-derived % atheroma volume from baseline to week 52 | The mean change in % atheroma volume was −2.13% with alirocumab vs. −0.92% with placebo (difference, −1.21% [95% CI, −1.78% to −0.65%], p < 0.001) |
| Ako (2019) ODYSSEY J-IVUS [56] n = 206 | 2° prevention—Patients aged 20 years and older who had been hospitalized for ACS, had LDL-C ≥ 100 mg/dL at ACS diagnosis, had undergone IVUS imaging as part of usual clinical practice in Japan, and had an analyzable IVUS image of the culprit or non-culprit vessel with ≥50% angiographic stenosis of the culprit vessel within 1 week after ACS onset | Intervention: Alirocumab 75 mg every 2 weeks and up to 150 mg biweekly. Comparator: Standard of care (atorvastatin ≥ 10 mg daily or rosuvastatin ≥ 5 mg daily) | Percent change in normalized total atheroma volume from baseline to week 36 | At week 36, the mean % change in normalized total atheroma volume from baseline was −3.1% (1.0) with the standard of care vs. −4.8% (1.0) with alirocumab (between-group difference: −1.6 [1.4]; p = 0.23). The absolute change from baseline in % atheroma volume was −1.3% (0.4) with the standard of care and −1.4% (0.4) with alirocumab, p = 0.79) |
| Gao (2021) Impact of PCSK9 Inhibitors on Coronary Plaque Composition and Vulnerability Assessed by Optical Coherence Tomography [57] n = 61 | 2° prevention—Patients aged 18 to 80 years with stable CAD or ACS on admission, planned to have clinically indicated coronary angiography and identified as having at least one intermediate lesion (50–70% diameter stenosis) on de novo coronary arteries, identified with elevated LDL-C ≥ 70 mg/dL for patients with ACS or ≥ 100 mg/dL for non-ACS patients, despite maximally tolerated statins | Intervention: Alirocumab 75 mg biweekly plus statin (atorvastatin 20 mg daily or rosuvastatin 10 mg daily) therapy. Comparator: Standard-of-care statin | Optimal-coherence-tomography-derived absolute changes in minimum fibrous cap thickness between baseline and follow-up. F/U: 36 weeks | The increase in minimum fibrous cap thickness in the alirocumab group was 18.0 μm (10.8–29.2) vs. 13.2 μm (7.4–18.6) in the standard-of-care group, p = 0.029. The increase in minimum lumen area in the alirocumab group was 0.20 mm2 (0.10–0.33) vs. 0.13 mm2 (0.12–0.24) in the standard-of-care group, p = 0.006. The diminution in maximum lipid arc in the alirocumab group was 15.1 (7.8–24.5) vs. 8.4% (2.0–10.5) in the standard-of-care group p = 0.008. |
| Trial | Study Population | Intervention and Comparator | 1° Outcome, Follow-Up Period | 1° Outcome Data |
|---|---|---|---|---|
| Ridker (2017) SPIRE-HR [58] n = 711 | 1° and 2° prevention—Patients ≥ 18 and older with LDL-C ≥ 70 mg/dL on the highest statin dose and with a history of CAD, other ASCVD, T1DM, T2DM, or CKD, and with TG ≤ 400 mg/dL | Intervention: Subcutaneous injections of bococizumab 150 mg self-administered every 2 weeks. Comparator: Subcutaneous injections of matched placebo self-administered every 2 weeks. | Percent change in LDL-C at week 12 and persistence for 12 months. F/U: 52 weeks | Meta-analysis of LDL-C ↓ in SPIRE-HR, SPIRE-LDL, SPIRE-FH, SPIRE-LL, SPIRE-SI, and SPIRE-AI: −55.2% at 12 weeks; −42.5% at 52 weeks |
| Ridker (2017) SPIRE-LDL [58] n = 2139 | 1° and 2° prevention—Patients ≥ 18 and older with LDL-C ≥ 70 mg/dL on the highest statin dose if a history of CAD, other ASCVD, T1DM, T2DM, or CKD was present, or with LDL-C ≥ 100 mg/dL on the highest statin dose if equivalent risk factors were present | Intervention: Bococizumab 150 mg subcutaneously self-administered every 2 weeks. Comparator: Placebo. | Percent change in LDL-C at week 12 and long-term persistence of any effects on the LDL-C level for 12 months. F/U: 52 weeks | |
| Ridker (2017) SPIRE-FH [58] n = 370 | HeFH 1° and 2° prevention—Patients ≥ 18 and older with HeFH and LDL-C ≥ 70 mg/dL on highest statin dose if a history of CAD, other ASCVD, T1DM, T2DM, or CKD is present, or LDL-C ≥ 100 mg/dL on highest statin dose if 1° prevention, and with TG ≤ 400 mg/dL | Intervention: Subcutaneous injections of bococizumab 150 mg self-administered every 2 weeks. Comparator: Subcutaneous injections of matched placebo self-administered every 2 weeks. | Percent change in LDL-C at week 12 and long-term persistence of any effects on the LDL-C level for 12 months. F/U: 52 weeks | |
| Ridker (2017) SPIRE-LL [58] n = 746 | 1° and 2° prevention—Patients ≥ 18 and older with LDL-C ≥ 100 mg/dL with ASCVD, T1DM, T2DM, CDK, or equivalent risk factors | Intervention: Subcutaneous injections of bococizumab 150 mg self-administered every 2 weeks. Comparator: Subcutaneous injections of matched placebo self-administered every 2 weeks. | Percent change in LDL-C at week 12 and long-term persistence of any effects on the LDL-C level for 12 months. F/U: 52 weeks | |
| Ridker (2017) SPIRE-SI [58] n = 184 | 1° and 2° prevention—Patients ≥ 18 and older with LDL-C ≥ 70 mg/dL and with statin intolerance | Intervention: Subcutaneous injections of bococizumab 150 mg self-administered every 2 weeks. Comparators: Oral atorvastatin 40 mg or subcutaneous injections of matched placebo self-administered every 2 weeks | Percent change in LDL-C at week 12 and long-term persistence of any effects on the LDL-C level. F/U: 6 months | |
| Ridker (2017) SPIRE-AI [58] n = 299 | 1° and 2° prevention—Patients ≥ 18 and older with LDL-C ≥ 70 mg/dL on stable statins | Interventions: Subcutaneous injections of bococizumab 150 or 75 mg administered with an autoinjector device every 2 weeks. Comparators: Subcutaneous injections matching doses of placebo administered with an autoinjector device every 2 weeks. | Percent change in LDL-C and long-term persistence of any effects on the LDL-C level. F/U: 12 weeks | |
| Ridker (2017) SPIRE-1 [59] n = 16,817 | 1° and 2° prevention—Patients ≥ 18 and older if 2° prevention, ≥35 years (men) and ≥45 years (women) if elevated LDL-C, and ≥50 years (men) and ≥60 years (women) if 1° prevention, with LDL-C ≥ 70 mg/dL or non-HDL-C ≥ 100 mg/dL, and on stable statins | Intervention: Subcutaneous injections of bococizumab 150 mg every 2 weeks (dose was lowered if LDL-C < 10 mg/dL). Comparator: Subcutaneous injections of matching placebo every 2 weeks. | A composite of CV death, non-fatal MI, non-fatal stroke, and hospitalization for unstable angina needing urgent revascularization. F/U: Median of 7 months | HR (95% CI) 0.99 (0.80–1.22) |
| Ridker (2017) SPIRE-2 [59] n = 10,621 | 1° and 2° prevention—Patients ≥ 18 years if 2° prevention, ≥35 years (men) and ≥45 years (women) if elevated LDL-C, and ≥50 years (men) and ≥60 years (women) if 1° prevention with LDL-C ≥ 100 mg/dL or non-HDL-C ≥ 130 mg/dL, and on stable statins | Intervention: Subcutaneous injections of bococizumab 150 mg every 2 weeks (dose was lowered if LDL-C < 10 mg/dL). Comparator: Subcutaneous injections of matching placebo every 2 weeks. | A composite of CV death, non-fatal MI, non-fatal stroke, and hospitalization for unstable angina needing urgent revascularization. F/U: Median of 12 months | HR (95% CI) 0.79 (0.65–0.97) |
| Trial, Sample Size | Study Population | Intervention and Comparator | 1° Outcome, Follow-Up Period | 1° Outcome Result |
|---|---|---|---|---|
| Raal (2020) ORION-9 [60] n = 482 | HeFH 1° and 2° prevention—Patients ≥ 18 years old with HeFH, LDL-C ≥ 100 mg/dL, on maximally tolerated statin dose, or with statin intolerance | Intervention: Inclisiran sodium 300 mg on days 1, 90, 270, and 450. Comparator: Subcutaneous placebo injection on days 1, 90, 270, and 450. | (1) Percent change in LDL-C level at day 510. (2) Time-adjusted % change in LDL-C level between day 90 and day 540. F/U: 540 days | At day 510, inclisiran resulted in a placebo-adjusted difference of −47.9% age points (95% CI, −53.5 to −42.3; p < 0.001) in LDL-C. The time-averaged % change in LDL-C was a placebo-adjusted difference of −44.3 percentage points (95% CI, −48.5 to −40.1; p < 0.001) |
| Ray (2020) ORION-10 [61] n = 1561 | 2° prevention—Patients ≥ 18 years old with ASCVD and LDL-C ≥ 70 mg/dL on maximally tolerated statins or with statin intolerance | Intervention: Inclisiran sodium 284 mg on days 1, 90, 270, and 450. Comparator: Subcutaneous placebo injection on days 1, 90, 270, and 450. | (1) Percent change in LDL-C level at day 510. (2) Time-adjusted % change in LDL-C level from baseline after day 90 and up to day 540. F/U: 540 days | At day 510, inclisiran resulted in a placebo-adjusted difference of −52.3% (95% CI, −55.7 to −48.8; p < 0.001) in LDL-C levels. Inclisiran resulted in a placebo-adjusted difference of −53.8% (95% CI, −56.2 to −51.3; p < 0.001) in time-adjusted changes in LDL-C between day 90 and day 540 |
| Ray (2020) ORION-11 [61] n = 1617 | 1° and 2° prevention—Patients with ASCVD and high-risk 1° prevention | Intervention: Inclisiran sodium 284 mg on days 1, 90, 270, and 450. Comparator: Subcutaneous placebo injection on days 1, 90, 270, and 450. | (1) Percent change in LDL-C level at day 510. (2) Time-adjusted % change in LDL-C level from baseline after day 90 and up to day 540. F/U: 540 days | At day 510, inclisiran resulted in a placebo-adjusted difference of −49.9% (95% CI, −53.1 to −46.6; p < 0.001) in LDL-C levels. Inclisiran resulted in a placebo-adjusted difference of −49.2% (95% CI, −51.6 to −46.8; p < 0.001) in time-adjusted changes in LDL-C between day 90 and day 540 |
| Ray (2023) ORION-3 [62] n = 382 | 1° and 2° prevention—Patients ≥ 18 years old with LDL-C ≥ 70 mg/dL with ASCVD (2° prevention), or with LDL-C ≥ 100 mg/dL at high risk of ASCVD (1° prevention), on statins or with statin intolerance | Intervention: Inclisiran sodium 300 mg twice yearly (after 200, 300, or 500 mg on day 1, or 100, 200, or 300 mg on days 1 and 90 in ORION-1). Comparator: Subcutaneous evolocumab 140 mg every 2 weeks for up to 1 year, followed by subcutaneous inclisiran sodium 300 mg with random allocation to staged switch (day 336, final dose evolocumab; day 360, first dose inclisiran) or concurrent switch (day 360, final dose evolocumab, first dose inclisiran), then 90 days later (day 450) and 6-monthly thereafter (after matched placebo in ORION-1). | Percent change in LDL-C at day 210 of ORION-3 (570 days from the start of ORION-1). F/U: 4 years | At day 210, inclisiran usage resulted in a −47.5% difference (95% CI −50.7 to −44.3; p < 0.0001) in baseline LDL-C levels |
| Trial, Sample Size | Study Population | Intervention and Comparator | 1° Outcome, Follow-Up Period | 1° Outcome Result |
|---|---|---|---|---|
| Stein (2012) RADICHOL II [63] n = 114 | HeFH 2° prevention—Patients ≥ 18 years old with HeFH and CAD with LDL-C ≥ 100 mg/dL on maximally tolerated statins | Intervention: Subcutaneous injections of mipomersen 200 mg self-administered weekly. Comparator: Subcutaneous injections of matched placebo self-administered weekly. | Percent change in LDL-C at week 28, or 2 weeks after the last dose for non-completers. F/U: 28 weeks | Mipomersen significantly ↓ LDL-C by −28% from baseline (95% CI: [−34.0% to −22.1%]), compared with a 5.2% (95% CI: [−0.5% to 10.9%]) increase with placebo (p < 0.001). |
| McGowan (2012) Randomized, Placebo-Controlled Trial of Mipomersen in Patients with Severe Hypercholesterolemia Receiving Maximally Tolerated Lipid-Lowering Therapy [64] n = 58 | 1° and 2° prevention—Patients ≥ 18 years old with severe hypercholesterolemia, with and without ASCVD, on maximally tolerated LLT | Intervention: Subcutaneous injections of mipomersen 200 mg self-administered weekly. Comparator: Subcutaneous injections of matched placebo self-administered weekly. | Percent change in LDL-C at week 28, or 2 weeks after the last dose for non-completers. F/U: 28 weeks | Mipomersen significantly ↓ LDL-C from baseline by −36% (95% CI, −51.3, −15.3; p < 0.001), compared to a 12.5% increase in the placebo group (95% CI, −10.8 to 35.8) |
| Thomas (2013) Safety and Efficacy of Mipomersen (ISIS 301012) As Add-on Therapy in High Risk Hypercholesterolemic Patients [65] n = 104 | 1° and 2° prevention—Patients on statins with LDL-C ≥ 100 mg/dL, with or at high risk of cardiovascular disease | Intervention: Subcutaneous injections of mipomersen 200 mg self-administered weekly. Comparator: Subcutaneous injections of matched placebo self-administered weekly. | Percent change in LDL-C at week 28, or 2 weeks after the last dose for non-completers. F/U: 24 weeks | Mipomersen significantly ↓ LDL-C from baseline by −36.9%, compared with a −4.5% decrease in the placebo group (p < 0.001) |
| Trial, Sample Size, Drug | Study Population | Intervention and Comparator | 1° Outcome, Follow-Up Period | 1° Outcome Result |
|---|---|---|---|---|
| Raal (2023) LIBerate-HeFH [66] n = 478 Lerodalcibep | HeFH 1° and 2° prevention—Patients ≥ 18 years old with HeFH and LDL-C ≥ 100 mg/dL (primary prevention) or ≥70 mg/dL (secondary prevention) | Intervention: Subcutaneous injections of lerodalcibep 300 mg monthly. Comparator: Subcutaneous injections of matched placebo monthly. | Percent change in LDL-C at week 24, and the mean of weeks 22 and 24. F/U: 24 weeks | Lerodalcibep reduced LDL-C by a placebo-adjusted −58.61 (3.25)% at week 24 (p < 0.0001). For the mean of weeks 22 and 24, lerodalcibep reduced LDL-C by 2.28 (0.10) mmol/L (95% CI −2.47 to −2.09) and −65.0 (2.87)% compared with the placebo (p < 0.0001 for both) |
| Schwartz (2012) dal-OUTCOMES [67] n = 15,871 Dalcetrapib | 2° prevention—Patients ≥ 45 years old hospitalized for acute ACS | Intervention: Oral dalcetrapib 600 mg daily. Comparator: Oral matched placebo daily. | A composite of death from CAD, non-fatal MI, ischemic stroke, unstable angina, or cardiac arrest with resuscitation. F/U: 31 months | Compared to the placebo, dalcetrapib did not alter the risk of the primary endpoint or total mortality (cumulative event rates: 8.0% and 8.3%, respectively; HR with dalcetrapib, 1.04; 95% CI [0.93–1.16]; p = 0.52) |
| HPS3/TIMI55–Reveal Collaborative Group (2017) REVEAL [68] n = 30,449 Anacetrapib | 2° prevention—Patients with established ASCVD | Intervention: Oral anacetrapib 100 mg daily. Comparator: Oral matched placebo daily. | A composite of death from CAD, MI, or coronary revascularization. F/U: 4.1 years | Compared to the placebo, anacetrapib resulted in a lower incidence of major coronary events (1640 of 15,225 patients [10.8%] vs. 1803 of 15,224 patients [11.8%]; rate ratio, 0.91; 95% CI, 0.85 to 0.97; p = 0.004) |
| Barter (2007) ILLUMINATE [69] n = 15,067 Torcetrapib | 1° and 2° prevention—Patients aged 45–75 years with established ASCVD (secondary prevention), and patients with type 2 diabetes without previous ASCVD (primary prevention) | Intervention: Atorvastatin and oral torcetrapib Comparator: Atorvastatin only. | A composite of death from coronary heart disease, non-fatal MI, stroke, and hospitalization for unstable angina. F/U: 4.5 years | Torcetrapib therapy increased the risk of cardiovascular events (HR, 1.25; 95% CI, 1.09 to 1.44; p = 0.001) and death from any cause (HR, 1.58; 95% CI, 1.14 to 2.19; p = 0.006) relative to the placebo. |
| Lincoff (2017) ACCELERATE [70] n = 12,092 Evacetrapib | 2° prevention—Patients ≥ 18 years old with ASCVD on statin therapy | Intervention: Oral dose of 130 mg of evacetrapib once daily, in addition to statin therapy. Comparator: Matching placebo and statin therapy. | A composite of death from cardiovascular causes, MI, stroke, coronary revascularization, and hospitalization from unstable angina. F/U: 26 months | At 26 months, the primary endpoint occurred in 12.9% of patients receiving evacetrapib and in 12.8% of patients receiving the placebo (HR, 1.01; 95% CI, 0.91 to 1.11; p = 0.91) |
| Nicholls (2022) [71] n = 120 Obicetrapib | 1° prevention—Patients 18–75 years old with LDL-C > 70 mg/dL, without significant ASCVD, on high-intensity statin therapy | Intervention: 10 mg oral dose of obicetrapib. Control: matched placebo | Percent change in LDL-C after 8 weeks of treatment. F/U: 8 weeks | Obicetrapib 5 mg and 10 mg significantly reduced LDL-C levels by 42.9% and 45.7%, respectively, compared to 0.0% for the placebo group (p < 0.0001) |
| (Ongoing) BROOKLYN (NCT05425745) n = 300 Obicetrapib | HeFH, 1° and 2° prevention—Patients ≥ 18 years old with HeFH and LDL-C ≥ 70 mg/dL on maximally tolerated statin therapy | Intervention: 10 mg oral dose of obicetrapib. Control: Matched placebo | Percent change in LDL-C after 12 weeks of treatment. F/U: 12 weeks | Results pending |
| (Ongoing) BROADWAY (NCT05142722) n = 2532 Obicetrapib | HeFH and 2° prevention—Patients > 60 years old with either HeFH or ASCVD and a history of MI in the past year, with LDL-C ≥ 100 mg/dL, on maximally tolerated LLT | Intervention: 10 mg oral dose of obicetrapib. Control: Matched placebo | Percent change in LDL-C after 12 weeks of treatment. F/U: 12 weeks | Results pending |
| (Ongoing) PREVAIL (NCT05202509) n = 9000 Obicetrapib | 2° prevention—Patients ≥ 18 years old with established ASCVD and LDL-C ≥ 70 mg/dL on maximally tolerated LLT | Intervention: 10 mg oral dose of obicetrapib. Control: Matched placebo | A composite of major adverse cardiac events. F/U: 32 months | Results pending |
4.1. Ezetimibe
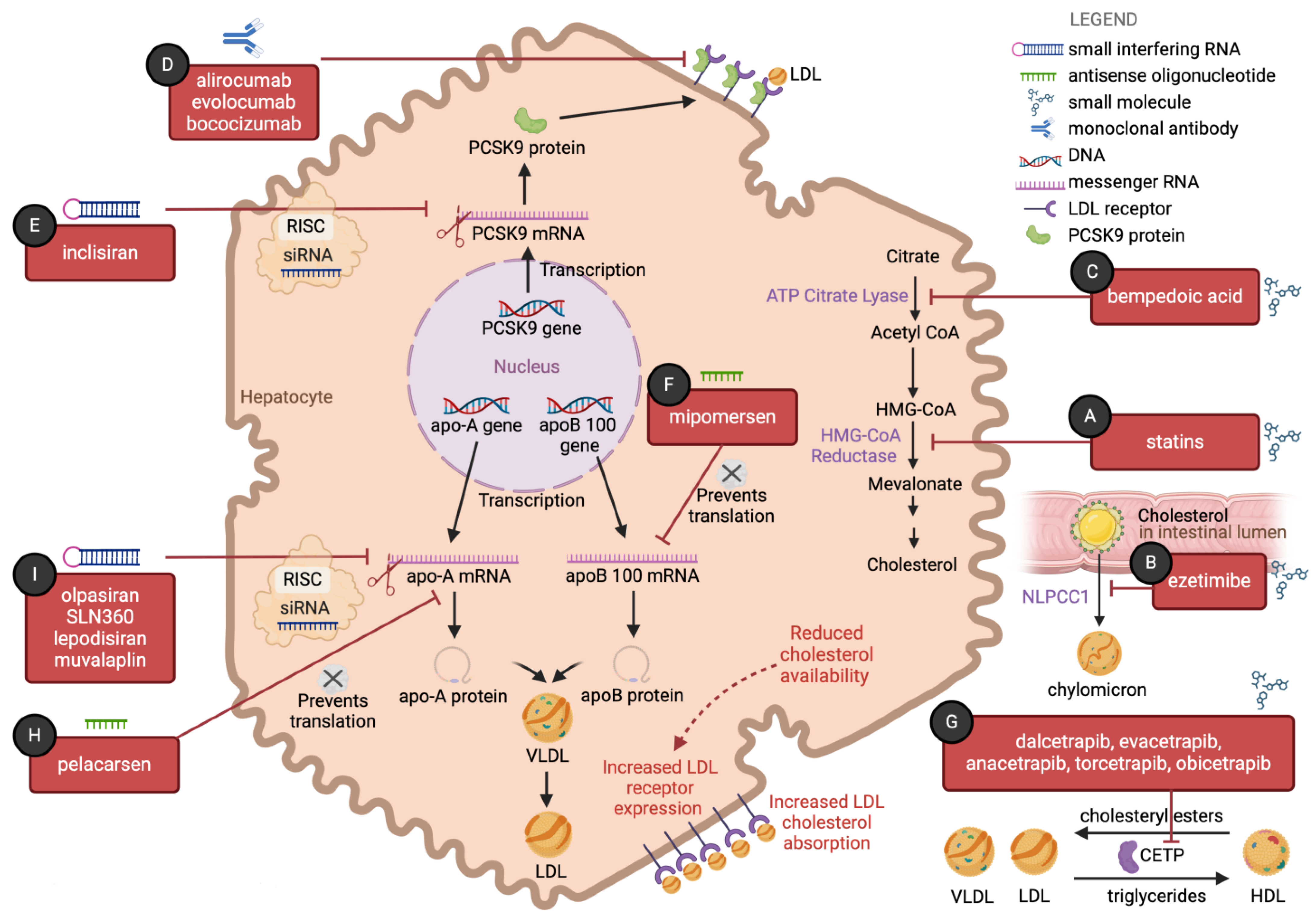
4.1.1. Mechanism of Action
4.1.2. Results of Randomized Trials
4.1.3. Current Indications
4.1.4. Safety Profile
4.1.5. Cost-Effectiveness
4.2. Bempedoic Acid
4.2.1. Mechanism of Action
4.2.2. Results of Randomized Trials
4.2.3. Current Indications
4.2.4. Safety Profile
4.2.5. Cost-Effectiveness
4.3. Monoclonal Antibodies Targeting Proprotein Convertase Subtilisin/Kexin Type 9
4.3.1. Mechanism of Action
4.3.2. Results of Randomized Trials of Evolocumab
4.3.3. Results of Randomized Trials of Alirocumab
4.3.4. Results of Randomized Trials of Bococizumab
4.3.5. Current Indications
4.3.6. Safety Profile
4.3.7. Cost-Effectiveness
4.4. Inclisiran
4.4.1. Mechanism of Action
4.4.2. Results of Randomized Trials
4.4.3. Current Indications
4.4.4. Safety Profile
4.4.5. Cost-Effectiveness
4.5. Mipomersen
4.5.1. Mechanism of Action
4.5.2. Results of Randomized Trials
4.5.3. Current Indications
4.5.4. Safety Profile
4.5.5. Cost-Effectiveness
4.6. CETP Inhibitors
4.6.1. Mechanism of Action
4.6.2. Results of Randomized Trials
4.6.3. Current Indications
4.6.4. Cost-Effectiveness
5. Triglyceride-Lowering Therapies
5.1. Overview
5.2. Omega-3 Fatty Acids (Including Eicosapentaenoic Acids)
5.2.1. Mechanism of Action
5.2.2. Results of Randomized Trials
5.2.3. Current Indications
5.2.4. Safety Profile
5.2.5. Cost-Effectiveness
5.3. Fibric Acid Derivatives
5.3.1. Mechanism of Action
5.3.2. Results of Randomized Trials
5.3.3. Current Indications
5.3.4. Safety Profile
5.3.5. Cost-Effectiveness
6. Lipoprotein-A-Lowering Therapies
6.1. Overview
6.1.1. Current Indications
6.1.2. Mechanism of Action
6.2. Pelacarsen
Safety Profile
6.3. Olpasiran
Safety Profile
6.4. SLN360
6.5. LY3473329 (Muvalaplin)
6.6. LY3819469 (Lepodisiran)
7. Conclusions and Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ↑ | Increase |
| ↓ | Decrease |
| 1° | Primary |
| 2° | Secondary |
| ACC | American College of Cardiology |
| ACCELERATE | Assessment of Clinical Effects of Cholesteryl Ester Transfer Protein Inhibition with Evacetrapib in Patients at a High Risk for Vascular Outcomes |
| ACCORD | Action to Control Cardiovascular Risk in Diabetes |
| ACL | Adenosine triphosphate-citrate lyase |
| ACS | Acute coronary syndrome |
| ApoB | Apolipoprotein B |
| ASCVD | Atherosclerotic cardiovascular disease |
| AHA | American Heart Association |
| ALTAIR | The Efficacy of Alirocumab for Thin-cap fIbroatheroma in Patients With Coronary Artery Disease Estimated by Optical Coherence Tomography |
| ARCHITECT | Alirocumab and Plaque Burden In Familial Hypercholesterolaemia |
| BANTING | Evaluation of Evolocumab Efficacy in Diabetic Adults With Hypercholesterolemia/Mixed Dyslipidemia |
| BID | Twice daily |
| BROADWAY | Randomized Study to Evaluate the Effect of Obicetrapib on Top of Maximum Tolerated Lipid-Modifying Therapies |
| BROOKLYN | Evaluate the Effect of Obicetrapib in Patients With HeFH on Top of Maximum Tolerated Lipid-Modifying Therapies |
| CAD | Coronary artery disease |
| CABG | Coronary artery bypass grafting |
| CETP | Cholesteryl ester transfer protein |
| CI | Confidence interval |
| CLEAR | Cholesterol Lowering via Bempedoic Acid, an ACL-Inhibiting Regimen |
| CV | Cardiovascular |
| dal-OUTCOMES | Effects of Dalcetrapib in Patients with a Recent Acute Coronary Syndrome |
| DESCARTES | Durable Effect of PCSK9 Antibody Compared with placebo Study |
| EPA | Eicosapentaenoic acid |
| EVOLVE-MI | Evolocumab Very Early After Myocardial Infarction |
| EWTOPIA 75 | Ezetimibe Lipid-Lowering Trial on Prevention of Atherosclerotic Cardiovascular Disease in 75 or Older |
| F/U | Follow-up |
| FDA | Food and Drug Administration |
| FIELD | Fenofibrate Intervention and Event Lowering in Diabetes |
| FOURIER | Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk |
| FOURIER-OLE | Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk Open-label Extension |
| GAUSS-2 | Goal Achievement After Utilizing an Anti-PCSK9 Antibody in Statin Intolerant Subjects 2 |
| GAUSS-3 | Goal Achievement After Utilizing an Anti-PCSK9 Antibody in Statin Intolerant Subjects 3 |
| HDL | High-density lipoprotein |
| HeFH | Heterozygous familial hypercholesterolemia |
| HLD | hyperlipidemia |
| HMG-CoA | 3-Hydroxy-3-methylglutaryl coenzyme A |
| HoFH | Homozygous familial hypercholesterolemia |
| HR | Hazard ratio |
| HUYGENS | High-Resolution Assessment of Coronary Plaques in a Global Evolocumab Randomized Study |
| IDL | Intermediate-density lipoprotein |
| iLLUMINATE | Ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab in first-line treatment of chronic lymphocytic leukaemia |
| IMPROVE-IT | IMProved Reduction of Outcomes: Vytorin Efficacy International Trial |
| IPE | Icosapent ethyl |
| JELIS | Japan EPA Lipid Study |
| KRAKEN | A Study of LY3473329 in Adult Participants With Elevated Lipoprotein(a) at High Risk for Cardiovascular Events |
| LAPLACE-2 | LDL-C Assessment With PCSK9 Monoclonal Antibody Inhibition Combined With Statin Therapy-2 |
| LDL | Low-density lipoprotein cholesterol |
| LIBerate-HeFH | Long-term efficacy and safety of lerodalcibep in heterozygous familial hypercholesterolaemia |
| LLT | Lipid-lowering therapy |
| Lp(a) | Lipoprotein A |
| Lp(a) HORIZON | A Randomized Double-blind, Placebo-controlled, Multicenter Trial Assessing the Impact of Lipoprotein (a) Lowering With TQJ230 on Major Cardiovascular Events in Patients With Established Cardiovascular Disease |
| MACE | Major adverse cardiovascular event |
| MENDEL-2 | Monoclonal Antibody Against PCSK9 to Reduce Elevated LDL-C in Subjects Currently Not Receiving Drug Therapy for Easing Lipid Levels-2 |
| mg/dL | Milligrams per deciliter |
| MI | Myocardial infarction |
| mRNA | Messenger ribonucleic acid |
| NPC1L1 | Niemann–Pick C1-like 1 |
| NYHA | New York Heart Association |
| OCT | Optical coherence tomography |
| OCEAN (a) | Olpasiran Trials of Cardiovascular Events and Lipoprotein(a) Reduction |
| ODDYSEY FH I | Efficacy and Safety of Alirocumab (SAR236553/REGN727) Versus Placebo on Top of Lipid-Modifying Therapy in Patients With Heterozygous Familial Hypercholesterolemia Not Adequately Controlled With Their Lipid-Modifying Therapy) |
| ODDYSEY FH II | Study of Alirocumab in Patients With heFH Who Are Not Adequately Controlled With Their Lipid-Modifying Therapy |
| ODYSSEY ALTERNATIVE | Study of Alirocumab in Patients With Primary Hypercholesterolemia and Moderate, High, or Very High Cardiovascular Risk, Who Are Intolerant to Statins |
| ODYSSEY CHOICE I | Study to Evaluate the Efficacy and Safety of an Every Four Weeks Treatment Regimen of Alirocumab (REGN727/SAR236553) in Patients With Primary Hypercholesterolemia |
| ODYSSEY CHOICE II | Phase III Study To Evaluate Alirocumab in Patients With Hypercholesterolemia Not Treated With a Statin |
| ODYSSEY COMBO I | Efficacy and Safety of Alirocumab (SAR236553/REGN727) Versus Placebo on Top of Lipid-Modifying Therapy in Patients With High Cardiovascular Risk and Hypercholesterolemia |
| ODYSSEY COMBO II | Efficacy and Safety of Alirocumab (SAR236553/REGN727) Versus Ezetimibe on Top of Statin in High Cardiovascular Risk Patients With Hypercholesterolemia |
| ODYSSEY EAST | Evaluation of Alirocumab Versus Ezetimibe on Top of Statin in Asia in High Cardiovascular Risk Patients With Hypercholesterolemia |
| ODYSSEY HIGH FH | Efficacy and Safety of Alirocumab Versus Placebo on Top of Lipid-Modifying Therapy in Patients With Heterozygous Familial Hypercholesterolemia |
| ODYSSEY JAPAN | Efficacy and Safety Evaluation of Alirocumab in Patients With Heterozygous Familial Hypercholesterolemia or High Cardiovascular Risk Patients With Hypercholesterolemia on Lipid Modifying Therapy |
| ODYSSEY LONG TERM | RCT of alirocumab and reduction of lipids and cardiovascular events |
| ODYSSEY MONO | Efficacy and Safety of Alirocumab Versus Ezetimibe in Patients With Hypercholesterolemia |
| ODYSSEY NIPPON | Efficacy and Safety of Alirocumab in Patients With Hypercholesterolemia Not Adequately Controlled With Non-statin Lipid Modifying Therapy or the Lowest Strength of Statin |
| ODYSSEY OPTIONS I | Study of the Efficacy and Safety of Alirocumab (REGN727/SAR236553) in Combination With Other Lipid-modifying Treatment) |
| ODYSSEY OPTIONS II | Study of the Efficacy and Safety of Alirocumab (REGN727/SAR236553) in Combination With Other Lipid-modifying Treatment |
| ODYSSEY OUTCOMES | Evaluation of Cardiovascular Outcomes After an Acute Coronary Syndrome During Treatment With Alirocumab) |
| OR | Odds ratio |
| ORION-10 | Inclisiran for Participants With Atherosclerotic Cardiovascular Disease and Elevated Low-density Lipoprotein Cholesterol |
| ORION-11 | Inclisiran for Subjects With ASCVD or ASCVD-Risk Equivalents and Elevated Low-density Lipoprotein Cholesterol |
| ORION-3 | Long-term efficacy and safety of inclisiran in patients with high cardiovascular risk and elevated LDL cholesterol |
| ORION-9 | Trial to Evaluate the Effect of Inclisiran Treatment on Low Density Lipoprotein Cholesterol (LDL-C) in Subjects With Heterozygous Familial Hypercholesterolemia (HeFH) |
| OSLER-2 | Open-Label Study of Long-Term Evaluation against LDL Cholesterol 2 |
| OYDSSEY KD | Evaluation of Alirocumab in Addition to Lipid-Modifying Therapy in Patients With High Cardiovascular Risk and Hypercholesterolemia in South Korea and Taiwan |
| PACMAN-AMI | Vascular Effects of Alirocumab in Acute MI-Patients |
| PAV | Percent atheroma volume |
| PCSK9 | Proprotein convertase subtilisin/kexin type 9 |
| PCI | Percutaneous coronary intervention |
| PPARα | Peroxisome proliferator-activated receptor alpha |
| PRECISE-IVUS | Plaque Regression With Cholesterol Absorption Inhibitor or Synthesis Inhibitor Evaluated by Intravascular Ultrasound |
| PREVAIL | Placebo Controlled, Double Blind, Randomized Cardiovascular Outcome Study to Evaluate the Effect of 10 mg Obicetrapib in Participants With ASCVD Not Adequately Controlled Despite Maximally Tolerated Lipid Modifying Therapies |
| PROFICO | Program to Reduce LDL-C and Cardiovascular Outcomes Following Inhibition of PCSK In Different Populations |
| PROMINENT | Pemafibrate to Reduce Cardiovascular Outcomes by Reducing Triglycerides in Patients with Diabetes |
| RADIOCHOL II | Efficacy and Safety Study of ISIS 301012 as Add-on in Familial Hypercholesterolemic Patients With Coronary Artery Disease |
| RCT | Randomized controlled trial |
| REDUCE-IT | Reduction of Cardiovascular Events with Icosapent Ethyl–Intervention Trial |
| RESPECT-EPA | Randomized trial for Evaluation in Secondary Prevention Efficacy of Combination Therapy-Statin and Eicosapentaenoic Acid |
| REVEAL | Randomized Evaluation of the Effects of Anacetrapib through Lipid-modification |
| RUTHERFORD-2 | Reduction of LDL-C With PCSK9 Inhibition in Heterozygous Familial Hypercholesterolemia Disorder Study-2 |
| SPIRE-1, SPIRE-2 | Studies of PCSK9 Inhibition and the Reduction of Vascular Events |
| SPIRE-AI | Efficacy, Safety, Tolerability And Actual Use Study Of Bococizumab And An Autoinjector (Pre-Filled Pen) In Subjects With Hyperlipidemia Or Dyslipidemia |
| SPIRE-FH | A 52 Week Study To Assess The Use Of Bococizumab In Subjects With Heterozygous Familial Hypercholesterolemia |
| SPIRE-HR, SPIRE-LDL | Randomized Clinical Trial Of Bococizumab In Subjects With Hyperlipidemia Or Mixed Dyslipidemia At Risk Of Cardiovascular Events |
| SPIRE-LL | Randomized Clinical Trial of Bococizumab (PF-04950615; RN316) in Subjects With Primary Hyperlipidemia or Mixed Dyslipidemia At Risk Of Cardiovascular Events |
| SPIRE-SI | Randomized Clinical Trial of Bococizumab in Subjects Who Are Intolerant to Statins |
| TC | Total cholesterol |
| TG | Triglycerides |
| TRL | Triglyceride-rich lipoprotein |
| UA | Unstable angina |
| VESALIUS-CV | Effect of Evolocumab in Patients at High Cardiovascular Risk Without Prior Myocardial Infarction or Stroke |
| VLDL | Very-low-density lipoprotein |
| YELLOW III | Effect of Evolocumab on Coronary Plaque Characteristics |
| Shaded rows represent names of trials. | |
References
- GBD 2016 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1603–1658. [Google Scholar] [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Libby, P. Changing concepts of atherogenesis. J. Intern. Med. 2000, 247, 349–358. [Google Scholar] [CrossRef]
- Libby, P. Inflammation in atherosclerosis—No longer a theory. Clin. Chem. 2021, 67, 131–142. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e563–e595. [Google Scholar] [CrossRef]
- Abdul-Rahman, T.; Bukhari, S.M.A.; Herrera, E.C.; Awuah, W.A.; Lawrence, J.; de Andrade, H.; Patel, N.; Shah, R.; Shaikh, R.; Capriles, C.A.A.; et al. Lipid Lowering Therapy: An Era Beyond Statins. Curr. Probl. Cardiol. 2022, 47, 101342. [Google Scholar] [CrossRef]
- Beshir, S.A.; Hussain, N.; Elnor, A.A.; Said, A.S.A. Umbrella Review on Non-Statin Lipid-Lowering Therapy. J. Cardiovasc. Pharmacol. Ther. 2021, 26, 437–452. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Writing, C.; Lloyd-Jones, D.M.; Morris, P.B.; Ballantyne, C.M.; Birtcher, K.K.; Covington, A.M.; DePalma, S.M.; Minissian, M.B.; Orringer, C.E.; Smith, S.C., Jr.; et al. 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2022, 80, 1366–1418. [Google Scholar] [CrossRef]
- Istvan, E.S.; Deisenhofer, J. Structural mechanism for statin inhibition of HMG-CoA reductase. Science 2001, 292, 1160–1164. [Google Scholar] [CrossRef] [PubMed]
- Nawrocki, J.W.; Weiss, S.R.; Davidson, M.H.; Sprecher, D.L.; Schwartz, S.L.; Lupien, P.J.; Jones, P.H.; Haber, H.E.; Black, D.M. Reduction of LDL cholesterol by 25% to 60% in patients with primary hypercholesterolemia by atorvastatin, a new HMG-CoA reductase inhibitor. Arterioscler. Thromb. Vasc. Biol. 1995, 15, 678–682. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists' (CTT) Collaboration; Baigent, C.; Blackwell, L.; Emberson, J.; Holland, L.E.; Reith, C.; Bhala, N.; Peto, R.; Barnes, E.H.; Keech, A.; et al. Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010, 376, 1670–1681. [Google Scholar] [CrossRef]
- Vinogradova, Y.; Coupland, C.; Brindle, P.; Hippisley-Cox, J. Discontinuation and restarting in patients on statin treatment: Prospective open cohort study using a primary care database. BMJ 2016, 353, i3305. [Google Scholar] [CrossRef]
- Bradley, C.K.; Wang, T.Y.; Li, S.; Robinson, J.G.; Roger, V.L.; Goldberg, A.C.; Virani, S.S.; Louie, M.J.; Lee, L.V.; Peterson, E.D.; et al. Patient-Reported Reasons for Declining or Discontinuing Statin Therapy: Insights From the PALM Registry. J. Am. Heart. Assoc. 2019, 8, e011765. [Google Scholar] [CrossRef]
- Banach, M.; Rizzo, M.; Toth, P.P.; Farnier, M.; Davidson, M.H.; Al-Rasadi, K.; Aronow, W.S.; Athyros, V.; Djuric, D.M.; Ezhov, M.V.; et al. Statin intolerance—An attempt at a unified definition. Position paper from an International Lipid Expert Panel. Arch. Med. Sci. 2015, 11, 1–23. [Google Scholar] [CrossRef]
- Wood, F.A.; Howard, J.P.; Finegold, J.A.; Nowbar, A.N.; Thompson, D.M.; Arnold, A.D.; Rajkumar, C.A.; Connolly, S.; Cegla, J.; Stride, C.; et al. N-of-1 Trial of a Statin, Placebo, or No Treatment to Assess Side Effects. N. Engl. J. Med. 2020, 383, 2182–2184. [Google Scholar] [CrossRef]
- Arvanitis, M.; Lowenstein, C.J. Dyslipidemia. Ann. Intern. Med. 2023, 176, ITC81–ITC96. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.P.; Blazing, M.A.; Giugliano, R.P.; McCagg, A.; White, J.A.; Theroux, P.; Darius, H.; Lewis, B.S.; Ophuis, T.O.; Jukema, J.W.; et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N. Engl. J. Med. 2015, 372, 2387–2397. [Google Scholar] [CrossRef]
- Ouchi, Y.; Sasaki, J.; Arai, H.; Yokote, K.; Harada, K.; Katayama, Y.; Urabe, T.; Uchida, Y.; Hayashi, M.; Yokota, N.; et al. Ezetimibe Lipid-Lowering Trial on Prevention of Atherosclerotic Cardiovascular Disease in 75 or Older (EWTOPIA 75): A Randomized, Controlled Trial. Circulation 2019, 140, 992–1003. [Google Scholar] [CrossRef] [PubMed]
- Tsujita, K.; Sugiyama, S.; Sumida, H.; Shimomura, H.; Yamashita, T.; Yamanaga, K.; Komura, N.; Sakamoto, K.; Oka, H.; Nakao, K.; et al. Impact of Dual Lipid-Lowering Strategy With Ezetimibe and Atorvastatin on Coronary Plaque Regression in Patients With Percutaneous Coronary Intervention: The Multicenter Randomized Controlled PRECISE-IVUS Trial. J. Am. Coll. Cardiol. 2015, 66, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Ballantyne, C.M.; Banach, M.; Mancini, G.B.J.; Lepor, N.E.; Hanselman, J.C.; Zhao, X.; Leiter, L.A. Efficacy and safety of bempedoic acid added to ezetimibe in statin-intolerant patients with hypercholesterolemia: A randomized, placebo-controlled study. Atherosclerosis 2018, 277, 195–203. [Google Scholar] [CrossRef]
- Ray, K.K.; Bays, H.E.; Catapano, A.L.; Lalwani, N.D.; Bloedon, L.T.; Sterling, L.R.; Robinson, P.L.; Ballantyne, C.M.; Trial, C.H. Safety and Efficacy of Bempedoic Acid to Reduce LDL Cholesterol. N. Engl. J. Med. 2019, 380, 1022–1032. [Google Scholar] [CrossRef]
- Goldberg, A.C.; Leiter, L.A.; Stroes, E.S.G.; Baum, S.J.; Hanselman, J.C.; Bloedon, L.T.; Lalwani, N.D.; Patel, P.M.; Zhao, X.; Duell, P.B. Effect of Bempedoic Acid vs. Placebo Added to Maximally Tolerated Statins on Low-Density Lipoprotein Cholesterol in Patients at High Risk for Cardiovascular Disease: The CLEAR Wisdom Randomized Clinical Trial. JAMA 2019, 322, 1780–1788. [Google Scholar] [CrossRef] [PubMed]
- Laufs, U.; Banach, M.; Mancini, G.B.J.; Gaudet, D.; Bloedon, L.T.; Sterling, L.R.; Kelly, S.; Stroes, E.S.G. Efficacy and Safety of Bempedoic Acid in Patients With Hypercholesterolemia and Statin Intolerance. J. Am. Heart Assoc. 2019, 8, e011662. [Google Scholar] [CrossRef] [PubMed]
- Nissen, S.E.; Lincoff, A.M.; Brennan, D.; Ray, K.K.; Mason, D.; Kastelein, J.J.P.; Thompson, P.D.; Libby, P.; Cho, L.; Plutzky, J.; et al. Bempedoic Acid and Cardiovascular Outcomes in Statin-Intolerant Patients. N. Engl. J. Med. 2023, 388, 1353–1364. [Google Scholar] [CrossRef] [PubMed]
- Koren, M.J.; Lundqvist, P.; Bolognese, M.; Neutel, J.M.; Monsalvo, M.L.; Yang, J.; Kim, J.B.; Scott, R.; Wasserman, S.M.; Bays, H.; et al. Anti-PCSK9 monotherapy for hypercholesterolemia: The MENDEL-2 randomized, controlled phase III clinical trial of evolocumab. J. Am. Coll. Cardiol. 2014, 63, 2531–2540. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.G.; Nedergaard, B.S.; Rogers, W.J.; Fialkow, J.; Neutel, J.M.; Ramstad, D.; Somaratne, R.; Legg, J.C.; Nelson, P.; Scott, R.; et al. Effect of evolocumab or ezetimibe added to moderate- or high-intensity statin therapy on LDL-C lowering in patients with hypercholesterolemia: The LAPLACE-2 randomized clinical trial. JAMA 2014, 311, 1870–1882. [Google Scholar] [CrossRef]
- Stroes, E.; Colquhoun, D.; Sullivan, D.; Civeira, F.; Rosenson, R.S.; Watts, G.F.; Bruckert, E.; Cho, L.; Dent, R.; Knusel, B.; et al. Anti-PCSK9 antibody effectively lowers cholesterol in patients with statin intolerance: The GAUSS-2 randomized, placebo-controlled phase 3 clinical trial of evolocumab. J. Am. Coll. Cardiol. 2014, 63, 2541–2548. [Google Scholar] [CrossRef]
- Blom, D.J.; Hala, T.; Bolognese, M.; Lillestol, M.J.; Toth, P.D.; Burgess, L.; Ceska, R.; Roth, E.; Koren, M.J.; Ballantyne, C.M.; et al. A 52-week placebo-controlled trial of evolocumab in hyperlipidemia. N. Engl. J. Med. 2014, 370, 1809–1819. [Google Scholar] [CrossRef]
- Raal, F.J.; Stein, E.A.; Dufour, R.; Turner, T.; Civeira, F.; Burgess, L.; Langslet, G.; Scott, R.; Olsson, A.G.; Sullivan, D.; et al. PCSK9 inhibition with evolocumab (AMG 145) in heterozygous familial hypercholesterolaemia (RUTHERFORD-2): A randomised, double-blind, placebo-controlled trial. Lancet 2015, 385, 331–340. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Wiviott, S.D.; Raal, F.J.; Blom, D.J.; Robinson, J.; Ballantyne, C.M.; Somaratne, R.; Legg, J.; Wasserman, S.M.; et al. Efficacy and safety of evolocumab in reducing lipids and cardiovascular events. N. Engl. J. Med. 2015, 372, 1500–1509. [Google Scholar] [CrossRef]
- Nissen, S.E.; Stroes, E.; Dent-Acosta, R.E.; Rosenson, R.S.; Lehman, S.J.; Sattar, N.; Preiss, D.; Bruckert, E.; Ceska, R.; Lepor, N.; et al. Efficacy and Tolerability of Evolocumab vs. Ezetimibe in Patients With Muscle-Related Statin Intolerance: The GAUSS-3 Randomized Clinical Trial. JAMA 2016, 315, 1580–1590. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef]
- Rosenson, R.S.; Daviglus, M.L.; Handelsman, Y.; Pozzilli, P.; Bays, H.; Monsalvo, M.L.; Elliott-Davey, M.; Somaratne, R.; Reaven, P. Efficacy and safety of evolocumab in individuals with type 2 diabetes mellitus: Primary results of the randomised controlled BANTING study. Diabetologia 2019, 62, 948–958. [Google Scholar] [CrossRef]
- O’Donoghue, M.L.; Giugliano, R.P.; Wiviott, S.D.; Atar, D.; Keech, A.; Kuder, J.F.; Im, K.; Murphy, S.A.; Flores-Arredondo, J.H.; Lopez, J.A.G.; et al. Long-Term Evolocumab in Patients With Established Atherosclerotic Cardiovascular Disease. Circulation 2022, 146, 1109–1119. [Google Scholar] [CrossRef]
- Nicholls, S.J.; Nissen, S.E.; Prati, F.; Windecker, S.; Kataoka, Y.; Puri, R.; Hucko, T.; Kassahun, H.; Liao, J.; Somaratne, R.; et al. Assessing the impact of PCSK9 inhibition on coronary plaque phenotype with optical coherence tomography: Rationale and design of the randomized, placebo-controlled HUYGENS study. Cardiovasc. Diagn. Ther. 2021, 11, 120–129. [Google Scholar] [CrossRef]
- Bohula, E.A.; Marston, N.A.; Ruzza, A.; Murphy, S.A.; De Ferrari, G.M.; Diaz, R.; Leiter, L.A.; Elliott-Davey, M.; Wang, H.; Bhatia, A.K.; et al. Rationale and design of the effect of evolocumab in patients at high cardiovascular risk without prior myocardial infarction or stroke (VESALIUS-CV) trial. Am. Heart. J. 2023, 269, 179–190. [Google Scholar] [CrossRef]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A.; et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.G.; Farnier, M.; Krempf, M.; Bergeron, J.; Luc, G.; Averna, M.; Stroes, E.S.; Langslet, G.; Raal, F.J.; El Shahawy, M.; et al. Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. N. Engl. J. Med. 2015, 372, 1489–1499. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, P.M.; Thompson, P.D.; Cannon, C.P.; Guyton, J.R.; Bergeron, J.; Zieve, F.J.; Bruckert, E.; Jacobson, T.A.; Kopecky, S.L.; Baccara-Dinet, M.T.; et al. Efficacy and safety of alirocumab vs. ezetimibe in statin-intolerant patients, with a statin rechallenge arm: The ODYSSEY ALTERNATIVE randomized trial. J. Clin. Lipidol. 2015, 9, 758–769. [Google Scholar] [CrossRef] [PubMed]
- Kastelein, J.J.; Ginsberg, H.N.; Langslet, G.; Hovingh, G.K.; Ceska, R.; Dufour, R.; Blom, D.; Civeira, F.; Krempf, M.; Lorenzato, C.; et al. ODYSSEY FH I and FH II: 78 week results with alirocumab treatment in 735 patients with heterozygous familial hypercholesterolaemia. Eur. Heart J. 2015, 36, 2996–3003. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, H.N.; Rader, D.J.; Raal, F.J.; Guyton, J.R.; Baccara-Dinet, M.T.; Lorenzato, C.; Pordy, R.; Stroes, E. Efficacy and Safety of Alirocumab in Patients with Heterozygous Familial Hypercholesterolemia and LDL-C of 160 mg/dL or Higher. Cardiovasc. Drugs. Ther. 2016, 30, 473–483. [Google Scholar] [CrossRef]
- Bays, H.; Gaudet, D.; Weiss, R.; Ruiz, J.L.; Watts, G.F.; Gouni-Berthold, I.; Robinson, J.; Zhao, J.; Hanotin, C.; Donahue, S. Alirocumab as Add-On to Atorvastatin Versus Other Lipid Treatment Strategies: ODYSSEY OPTIONS I Randomized Trial. J. Clin. Endocrinol. Metab. 2015, 100, 3140–3148. [Google Scholar] [CrossRef] [PubMed]
- Farnier, M.; Jones, P.; Severance, R.; Averna, M.; Steinhagen-Thiessen, E.; Colhoun, H.M.; Du, Y.; Hanotin, C.; Donahue, S. Efficacy and safety of adding alirocumab to rosuvastatin versus adding ezetimibe or doubling the rosuvastatin dose in high cardiovascular-risk patients: The ODYSSEY OPTIONS II randomized trial. Atherosclerosis 2016, 244, 138–146. [Google Scholar] [CrossRef]
- Kereiakes, D.J.; Robinson, J.G.; Cannon, C.P.; Lorenzato, C.; Pordy, R.; Chaudhari, U.; Colhoun, H.M. Efficacy and safety of the proprotein convertase subtilisin/kexin type 9 inhibitor alirocumab among high cardiovascular risk patients on maximally tolerated statin therapy: The ODYSSEY COMBO I study. Am. Heart. J. 2015, 169, 906–915. [Google Scholar] [CrossRef]
- Cannon, C.P.; Cariou, B.; Blom, D.; McKenney, J.M.; Lorenzato, C.; Pordy, R.; Chaudhari, U.; Colhoun, H.M.; Investigators, O.C.I. Efficacy and safety of alirocumab in high cardiovascular risk patients with inadequately controlled hypercholesterolaemia on maximally tolerated doses of statins: The ODYSSEY COMBO II randomized controlled trial. Eur. Heart J. 2015, 36, 1186–1194. [Google Scholar] [CrossRef]
- Roth, E.M.; Moriarty, P.M.; Bergeron, J.; Langslet, G.; Manvelian, G.; Zhao, J.; Baccara-Dinet, M.T.; Rader, D.J.; ODYSSEY CHOICE I investigators. A phase III randomized trial evaluating alirocumab 300 mg every 4 weeks as monotherapy or add-on to statin: ODYSSEY CHOICE I. Atherosclerosis 2016, 254, 254–262. [Google Scholar] [CrossRef]
- Stroes, E.; Guyton, J.R.; Lepor, N.; Civeira, F.; Gaudet, D.; Watts, G.F.; Baccara-Dinet, M.T.; Lecorps, G.; Manvelian, G.; Farnier, M.; et al. Efficacy and Safety of Alirocumab 150 mg Every 4 Weeks in Patients with Hypercholesterolemia Not on Statin Therapy: The ODYSSEY CHOICE II Study. J. Am. Heart. Assoc. 2016, 5, e003421. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, T.; Kobayashi, M.; Tasaki, H.; Yagyu, H.; Higashikata, T.; Takagi, Y.; Uno, K.; Baccara-Dinet, M.T.; Nohara, A. Efficacy and Safety of Alirocumab in Japanese Patients With Heterozygous Familial Hypercholesterolemia or at High Cardiovascular Risk With Hypercholesterolemia Not Adequately Controlled With Statins—ODYSSEY JAPAN Randomized Controlled Trial. Circ. J. 2016, 80, 1980–1987. [Google Scholar] [CrossRef]
- Koh, K.K.; Nam, C.W.; Chao, T.H.; Liu, M.E.; Wu, C.J.; Kim, D.S.; Kim, C.J.; Li, I.; Li, J.; Baccara-Dinet, M.T.; et al. A randomized trial evaluating the efficacy and safety of alirocumab in South Korea and Taiwan (ODYSSEY KT). J. Clin. Lipidol. 2018, 12, 162–172.e166. [Google Scholar] [CrossRef]
- Teramoto, T.; Kiyosue, A.; Ishigaki, Y.; Harada-Shiba, M.; Kawabata, Y.; Ozaki, A.; Baccara-Dinet, M.T.; Sata, M. Efficacy and safety of alirocumab 150mg every 4 weeks in hypercholesterolemic patients on non-statin lipid-lowering therapy or lowest strength dose of statin: ODYSSEY NIPPON. J. Cardiol 2019, 73, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Chen, J.; Chopra, V.K.; Zhang, S.; Su, G.; Ma, C.; Huang, Z.; Ma, Y.; Yao, Z.; Yuan, Z.; et al. ODYSSEY EAST: Alirocumab efficacy and safety vs. ezetimibe in high cardiovascular risk patients with hypercholesterolemia and on maximally tolerated statin in China, India, and Thailand. J. Clin. Lipidol. 2020, 14, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Perez de Isla, L.; Diaz-Diaz, J.L.; Romero, M.J.; Muniz-Grijalvo, O.; Mediavilla, J.D.; Argueso, R.; Sanchez Munoz-Torrero, J.F.; Rubio, P.; Alvarez-Banos, P.; Ponte, P.; et al. Alirocumab and Coronary Atherosclerosis in Asymptomatic Patients with Familial Hypercholesterolemia: The ARCHITECT Study. Circulation 2023, 147, 1436–1443. [Google Scholar] [CrossRef] [PubMed]
- Sugizaki, Y.; Otake, H.; Kawamori, H.; Toba, T.; Nagano, Y.; Tsukiyama, Y.; Yanaka, K.I.; Yamamoto, H.; Nagasawa, A.; Onishi, H.; et al. Adding Alirocumab to Rosuvastatin Helps Reduce the Vulnerability of Thin-Cap Fibroatheroma: An ALTAIR Trial Report. JACC Cardiovasc. Imaging 2020, 13, 1452–1454. [Google Scholar] [CrossRef]
- Raber, L.; Ueki, Y.; Otsuka, T.; Losdat, S.; Haner, J.D.; Lonborg, J.; Fahrni, G.; Iglesias, J.F.; van Geuns, R.J.; Ondracek, A.S.; et al. Effect of Alirocumab Added to High-Intensity Statin Therapy on Coronary Atherosclerosis in Patients With Acute Myocardial Infarction: The PACMAN-AMI Randomized Clinical Trial. JAMA 2022, 327, 1771–1781. [Google Scholar] [CrossRef]
- Ako, J.; Hibi, K.; Tsujita, K.; Hiro, T.; Morino, Y.; Kozuma, K.; Shinke, T.; Otake, H.; Uno, K.; Louie, M.J.; et al. Effect of Alirocumab on Coronary Atheroma Volume in Japanese Patients With Acute Coronary Syndrome—The ODYSSEY J-IVUS Trial. Circ. J. 2019, 83, 2025–2033. [Google Scholar] [CrossRef]
- Gao, F.; Wang, Z.J.; Ma, X.T.; Shen, H.; Yang, L.X.; Zhou, Y.J. Effect of alirocumab on coronary plaque in patients with coronary artery disease assessed by optical coherence tomography. Lipids Health Dis. 2021, 20, 106. [Google Scholar] [CrossRef]
- Ridker, P.M.; Tardif, J.C.; Amarenco, P.; Duggan, W.; Glynn, R.J.; Jukema, J.W.; Kastelein, J.J.P.; Kim, A.M.; Koenig, W.; Nissen, S.; et al. Lipid-Reduction Variability and Antidrug-Antibody Formation with Bococizumab. N. Engl. J. Med. 2017, 376, 1517–1526. [Google Scholar] [CrossRef]
- Ridker, P.M.; Revkin, J.; Amarenco, P.; Brunell, R.; Curto, M.; Civeira, F.; Flather, M.; Glynn, R.J.; Gregoire, J.; Jukema, J.W.; et al. Cardiovascular Efficacy and Safety of Bococizumab in High-Risk Patients. N. Engl. J. Med. 2017, 376, 1527–1539. [Google Scholar] [CrossRef]
- Raal, F.J.; Kallend, D.; Ray, K.K.; Turner, T.; Koenig, W.; Wright, R.S.; Wijngaard, P.L.J.; Curcio, D.; Jaros, M.J.; Leiter, L.A.; et al. Inclisiran for the Treatment of Heterozygous Familial Hypercholesterolemia. N. Engl. J. Med. 2020, 382, 1520–1530. [Google Scholar] [CrossRef]
- Ray, K.K.; Wright, R.S.; Kallend, D.; Koenig, W.; Leiter, L.A.; Raal, F.J.; Bisch, J.A.; Richardson, T.; Jaros, M.; Wijngaard, P.L.J.; et al. Two Phase 3 Trials of Inclisiran in Patients with Elevated LDL Cholesterol. N. Engl. J. Med. 2020, 382, 1507–1519. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Troquay, R.P.T.; Visseren, F.L.J.; Leiter, L.A.; Scott Wright, R.; Vikarunnessa, S.; Talloczy, Z.; Zang, X.; Maheux, P.; Lesogor, A.; et al. Long-term efficacy and safety of inclisiran in patients with high cardiovascular risk and elevated LDL cholesterol (ORION-3): Results from the 4-year open-label extension of the ORION-1 trial. Lancet Diabetes Endocrinol. 2023, 11, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Stein, E.A.; Dufour, R.; Gagne, C.; Gaudet, D.; East, C.; Donovan, J.M.; Chin, W.; Tribble, D.L.; McGowan, M. Apolipoprotein B synthesis inhibition with mipomersen in heterozygous familial hypercholesterolemia: Results of a randomized, double-blind, placebo-controlled trial to assess efficacy and safety as add-on therapy in patients with coronary artery disease. Circulation 2012, 126, 2283–2292. [Google Scholar] [CrossRef]
- McGowan, M.P.; Tardif, J.C.; Ceska, R.; Burgess, L.J.; Soran, H.; Gouni-Berthold, I.; Wagener, G.; Chasan-Taber, S. Randomized, placebo-controlled trial of mipomersen in patients with severe hypercholesterolemia receiving maximally tolerated lipid-lowering therapy. PLoS ONE 2012, 7, e49006. [Google Scholar] [CrossRef]
- Thomas, G.S.; Cromwell, W.C.; Ali, S.; Chin, W.; Flaim, J.D.; Davidson, M. Mipomersen, an apolipoprotein B synthesis inhibitor, reduces atherogenic lipoproteins in patients with severe hypercholesterolemia at high cardiovascular risk: A randomized, double-blind, placebo-controlled trial. J. Am. Coll. Cardiol. 2013, 62, 2178–2184. [Google Scholar] [CrossRef]
- Raal, F.; Fourie, N.; Scott, R.; Blom, D.; De Vries Basson, M.; Kayikcioglu, M.; Caldwell, K.; Kallend, D.; Stein, E.; Investigators, L.I.-H. Long-term efficacy and safety of lerodalcibep in heterozygous familial hypercholesterolaemia: The LIBerate-HeFH trial. Eur. Heart J. 2023, 44, 4272–4280. [Google Scholar] [CrossRef]
- Schwartz, G.G.; Olsson, A.G.; Abt, M.; Ballantyne, C.M.; Barter, P.J.; Brumm, J.; Chaitman, B.R.; Holme, I.M.; Kallend, D.; Leiter, L.A.; et al. Effects of dalcetrapib in patients with a recent acute coronary syndrome. N. Engl. J. Med. 2012, 367, 2089–2099. [Google Scholar] [CrossRef]
- Group, H.T.R.C.; Bowman, L.; Hopewell, J.C.; Chen, F.; Wallendszus, K.; Stevens, W.; Collins, R.; Wiviott, S.D.; Cannon, C.P.; Braunwald, E.; et al. Effects of Anacetrapib in Patients with Atherosclerotic Vascular Disease. N. Engl. J. Med. 2017, 377, 1217–1227. [Google Scholar] [CrossRef]
- Barter, P.J.; Caulfield, M.; Eriksson, M.; Grundy, S.M.; Kastelein, J.J.; Komajda, M.; Lopez-Sendon, J.; Mosca, L.; Tardif, J.C.; Waters, D.D.; et al. Effects of torcetrapib in patients at high risk for coronary events. N. Engl. J. Med. 2007, 357, 2109–2122. [Google Scholar] [CrossRef] [PubMed]
- Lincoff, A.M.; Nicholls, S.J.; Riesmeyer, J.S.; Barter, P.J.; Brewer, H.B.; Fox, K.A.A.; Gibson, C.M.; Granger, C.; Menon, V.; Montalescot, G.; et al. Evacetrapib and Cardiovascular Outcomes in High-Risk Vascular Disease. N. Engl. J. Med. 2017, 376, 1933–1942. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Ditmarsch, M.; Kastelein, J.J.; Rigby, S.P.; Kling, D.; Curcio, D.L.; Alp, N.J.; Davidson, M.H. Lipid lowering effects of the CETP inhibitor obicetrapib in combination with high-intensity statins: A randomized phase 2 trial. Nat. Med. 2022, 28, 1672–1678. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, M.; Origasa, H.; Matsuzaki, M.; Matsuzawa, Y.; Saito, Y.; Ishikawa, Y.; Oikawa, S.; Sasaki, J.; Hishida, H.; Itakura, H.; et al. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): A randomised open-label, blinded endpoint analysis. Lancet 2007, 369, 1090–1098. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]
- Nishizaki, Y.; Miyauchi, K.; Iwata, H.; Inoue, T.; Hirayama, A.; Kimura, K.; Ozaki, Y.; Murohara, T.; Ueshima, K.; Kuwabara, Y.; et al. Study protocol and baseline characteristics of Randomized trial for Evaluation in Secondary Prevention Efficacy of Combination Therapy-Statin and Eicosapentaenoic Acid: RESPECT-EPA, the combination of a randomized control trial and an observational biomarker study. Am. Heart. J. 2023, 257, 1–8. [Google Scholar] [CrossRef]
- Das Pradhan, A.; Glynn, R.J.; Fruchart, J.C.; MacFadyen, J.G.; Zaharris, E.S.; Everett, B.M.; Campbell, S.E.; Oshima, R.; Amarenco, P.; Blom, D.J.; et al. Triglyceride Lowering with Pemafibrate to Reduce Cardiovascular Risk. N. Engl. J. Med. 2022, 387, 1923–1934. [Google Scholar] [CrossRef]
- Group, A.S.; Ginsberg, H.N.; Elam, M.B.; Lovato, L.C.; Crouse, J.R., 3rd; Leiter, L.A.; Linz, P.; Friedewald, W.T.; Buse, J.B.; Gerstein, H.C.; et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N. Engl. J. Med. 2010, 362, 1563–1574. [Google Scholar] [CrossRef]
- Keech, A.; Simes, R.J.; Barter, P.; Best, J.; Scott, R.; Taskinen, M.R.; Forder, P.; Pillai, A.; Davis, T.; Glasziou, P.; et al. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): Randomised controlled trial. Lancet 2005, 366, 1849–1861. [Google Scholar] [CrossRef]
- Patel, J.; Sheehan, V.; Gurk-Turner, C. Ezetimibe (Zetia): A new type of lipid-lowering agent. In Baylor University Medical Center Proceedings; Taylor & Francis: Abingdon, UK, 2003; Volume 16, pp. 354–358. [Google Scholar] [CrossRef]
- Hammersley, D.; Signy, M. Ezetimibe: An update on its clinical usefulness in specific patient groups. Ther. Adv. Chronic. Dis. 2017, 8, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Mitka, M. Ezetimibe prescribing fails to keep up with evidence. JAMA 2014, 311, 1279–1280. [Google Scholar] [CrossRef]
- Nicholls, S.J.; Hsu, A.; Wolski, K.; Hu, B.; Bayturan, O.; Lavoie, A.; Uno, K.; Tuzcu, E.M.; Nissen, S.E. Intravascular ultrasound-derived measures of coronary atherosclerotic plaque burden and clinical outcome. J. Am. Coll. Cardiol. 2010, 55, 2399–2407. [Google Scholar] [CrossRef]
- Organon. Zetia (Ezetimibe)–U.S. Food and Drug Website. Available online: https://www.organon.com/product/usa/pi_circulars/z/zetia/zetia_pi.pdf (accessed on 30 December 2023).
- Lewek, J.; Banach, M. Dyslipidemia Management in Pregnancy: Why Is It not Covered in the Guidelines? Curr. Atheroscler. Rep. 2022, 24, 547–556. [Google Scholar] [CrossRef]
- Sasidharan, A.; Bagepally, B.S.; Kumar, S.S.; Jagadeesh, K.V.; Natarajan, M. Cost-effectiveness of Ezetimibe plus statin lipid-lowering therapy: A systematic review and meta-analysis of cost-utility studies. PLoS ONE 2022, 17, e0264563. [Google Scholar] [CrossRef]
- Schlackow, I.; Kent, S.; Herrington, W.; Emberson, J.; Haynes, R.; Reith, C.; Collins, R.; Landray, M.J.; Gray, A.; Baigent, C.; et al. Cost-effectiveness of lipid lowering with statins and ezetimibe in chronic kidney disease. Kidney Int. 2019, 96, 170–179. [Google Scholar] [CrossRef]
- Yang, H.; Li, N.; Zhou, Y.; Xiao, Z.; Tian, H.; Hu, M.; Li, S. Cost-Effectiveness Analysis of Ezetimibe as the Add-on Treatment to Moderate-Dose Rosuvastatin versus High-Dose Rosuvastatin in the Secondary Prevention of Cardiovascular Diseases in China: A Markov Model Analysis. Drug Des. Dev. Ther. 2020, 14, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Masana Marin, L.; Plana Gil, N. Bempedoic acid. Mechanism of action and pharmacokinetic and pharmacodynamic properties. Clin. Investig. Arterioscler. 2021, 33 (Suppl. 1), 53–57. [Google Scholar] [CrossRef] [PubMed]
- Ballantyne, C.M.; Laufs, U.; Ray, K.K.; Leiter, L.A.; Bays, H.E.; Goldberg, A.C.; Stroes, E.S.; MacDougall, D.; Zhao, X.; Catapano, A.L. Bempedoic acid plus ezetimibe fixed-dose combination in patients with hypercholesterolemia and high CVD risk treated with maximally tolerated statin therapy. Eur. J. Prev. Cardiol. 2020, 27, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Nexlizethcp. Nexletol (Bempedoic Acid)–U.S. Food and Drug Website. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/211616s000lbl.pdf (accessed on 30 December 2023).
- Banach, M.; Duell, P.B.; Gotto, A.M., Jr.; Laufs, U.; Leiter, L.A.; Mancini, G.B.J.; Ray, K.K.; Flaim, J.; Ye, Z.; Catapano, A.L. Association of Bempedoic Acid Administration With Atherogenic Lipid Levels in Phase 3 Randomized Clinical Trials of Patients With Hypercholesterolemia. JAMA Cardiol. 2020, 5, 1124–1135. [Google Scholar] [CrossRef]
- Agboola, F.; Lin, G.A.; Kazi, D.S.; McKenna, A.; Pearson, S.D. The effectiveness and value of bempedoic acid and inclisiran for heterozygous familial hypercholesterolemia and secondary prevention of ASCVD. J. Manag. Care Spec. Pharm. 2021, 27, 961–966. [Google Scholar] [CrossRef]
- ICER. Icer Publishes Evidence Report on Therapies for High Cholesterol. Available online: https://icer.org/news-insights/press-releases/icer-publishes-evidence-report-on-therapies-for-high-cholesterol/ (accessed on 11 February 2024).
- Benn, M.; Nordestgaard, B.G.; Grande, P.; Schnohr, P.; Tybjaerg-Hansen, A. PCSK9 R46L, low-density lipoprotein cholesterol levels, and risk of ischemic heart disease: 3 independent studies and meta-analyses. J. Am. Coll. Cardiol. 2010, 55, 2833–2842. [Google Scholar] [CrossRef]
- Catapano, A.L.; Papadopoulos, N. The safety of therapeutic monoclonal antibodies: Implications for cardiovascular disease and targeting the PCSK9 pathway. Atherosclerosis 2013, 228, 18–28. [Google Scholar] [CrossRef]
- Koba, S.; Inoue, I.; Cyrille, M.; Lu, C.; Inomata, H.; Shimauchi, J.; Kajinami, K. Evolocumab vs. Ezetimibe in Statin-Intolerant Hyperlipidemic Japanese Patients: Phase 3 GAUSS-4 Trial. J. Atheroscler. Thromb. 2020, 27, 471–484. [Google Scholar] [CrossRef]
- Hirayama, A.; Honarpour, N.; Yoshida, M.; Yamashita, S.; Huang, F.; Wasserman, S.M.; Teramoto, T. Effects of evolocumab (AMG 145), a monoclonal antibody to PCSK9, in hypercholesterolemic, statin-treated Japanese patients at high cardiovascular risk--primary results from the phase 2 YUKAWA study. Circ. J. 2014, 78, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Dent, R.; Joshi, R.; Stephen Djedjos, C.; Legg, J.; Elliott, M.; Geller, M.; Meyer, D.; Somaratne, R.; Recknor, C.; Weiss, R. Evolocumab lowers LDL-C safely and effectively when self-administered in the at-home setting. Springerplus 2016, 5, 300. [Google Scholar] [CrossRef] [PubMed]
- Erviti, J.; Wright, J.; Bassett, K.; Ben-Eltriki, M.; Jauca, C.; Saiz, L.C.; Leache, L.; Gutierrez-Valencia, M.; Perry, T.L. Restoring mortality data in the FOURIER cardiovascular outcomes trial of evolocumab in patients with cardiovascular disease: A reanalysis based on regulatory data. BMJ Open 2022, 12, e060172. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Puri, R.; Anderson, T.; Ballantyne, C.M.; Cho, L.; Kastelein, J.J.; Koenig, W.; Somaratne, R.; Kassahun, H.; Yang, J.; et al. Effect of Evolocumab on Progression of Coronary Disease in Statin-Treated Patients: The GLAGOV Randomized Clinical Trial. JAMA 2016, 316, 2373–2384. [Google Scholar] [CrossRef]
- Roth, E.M.; McKenney, J.M. ODYSSEY MONO: Effect of alirocumab 75 mg subcutaneously every 2 weeks as monotherapy versus ezetimibe over 24 weeks. Future Cardiol. 2015, 11, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Szarek, M.; White, H.D.; Schwartz, G.G.; Alings, M.; Bhatt, D.L.; Bittner, V.A.; Chiang, C.E.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; et al. Alirocumab Reduces Total Nonfatal Cardiovascular and Fatal Events: The ODYSSEY OUTCOMES Trial. J. Am. Coll. Cardiol. 2019, 73, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Amgen. Repatha (Evolocumab)–U.S. Food and Drug Website. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/125522orig2s000lbl.pdf (accessed on 30 December 2023).
- Sanofi, R.A. Praluent (Alirocumab)–U.S. Food and Drug Website. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/125559s029s030lbl.pdf (accessed on 30 December 2023).
- Ference, B.A.; Robinson, J.G.; Brook, R.D.; Catapano, A.L.; Chapman, M.J.; Neff, D.R.; Voros, S.; Giugliano, R.P.; Davey Smith, G.; Fazio, S.; et al. Variation in PCSK9 and HMGCR and Risk of Cardiovascular Disease and Diabetes. N. Engl. J. Med. 2016, 375, 2144–2153. [Google Scholar] [CrossRef]
- Guedeney, P.; Giustino, G.; Sorrentino, S.; Claessen, B.E.; Camaj, A.; Kalkman, D.N.; Vogel, B.; Sartori, S.; De Rosa, S.; Baber, U.; et al. Efficacy and safety of alirocumab and evolocumab: A systematic review and meta-analysis of randomized controlled trials. Eur. Heart J. 2022, 43, e17–e25. [Google Scholar] [CrossRef]
- Choi, H.D.; Kim, J.H. An Updated Meta-Analysis for Safety Evaluation of Alirocumab and Evolocumab as PCSK9 Inhibitors. Cardiovasc. Ther. 2023, 2023, 7362551. [Google Scholar] [CrossRef]
- Gurgoze, M.T.; Muller-Hansma, A.H.G.; Schreuder, M.M.; Galema-Boers, A.M.H.; Boersma, E.; Roeters van Lennep, J.E. Adverse Events Associated With PCSK9 Inhibitors: A Real-World Experience. Clin. Pharmacol. Ther. 2019, 105, 496–504. [Google Scholar] [CrossRef]
- Fonarow, G.C.; van Hout, B.; Villa, G.; Arellano, J.; Lindgren, P. Updated Cost-effectiveness Analysis of Evolocumab in Patients With Very High-risk Atherosclerotic Cardiovascular Disease. JAMA Cardiol. 2019, 4, 691–695. [Google Scholar] [CrossRef]
- Michaeli, D.T.; Michaeli, J.C.; Boch, T.; Michaeli, T. Cost-Effectiveness of Icosapent Ethyl, Evolocumab, Alirocumab, Ezetimibe, or Fenofibrate in Combination with Statins Compared to Statin Monotherapy. Clin. Drug. Investig. 2022, 42, 643–656. [Google Scholar] [CrossRef] [PubMed]
- Migliorati, J.M.; Jin, J.; Zhong, X.B. siRNA drug Leqvio (inclisiran) to lower cholesterol. Trends Pharmacol. Sci. 2022, 43, 455–456. [Google Scholar] [CrossRef] [PubMed]
- Albosta, M.S.; Grant, J.K.; Taub, P.; Blumenthal, R.S.; Martin, S.S.; Michos, E.D. Inclisiran: A New Strategy for LDL-C Lowering and Prevention of Atherosclerotic Cardiovascular Disease. Vasc. Health Risk Manag. 2023, 19, 421–431. [Google Scholar] [CrossRef] [PubMed]
- Novartis. Leqvio (Inclisiran)–U.S. Food and Drug Website. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/214012s009lbl.pdf (accessed on 30 December 2023).
- Cicero, A.F.; Fogacci, F.; Zambon, A.; Toth, P.P.; Borghi, C. Efficacy and safety of inclisiran a newly approved FDA drug: A systematic review and pooled analysis of available clinical studies. Am. Heart J. Plus Cardiol. Res. Pract. 2022, 13, 100127. [Google Scholar] [CrossRef]
- Desai, N.R.; Campbell, C.; Electricwala, B.; Petrou, M.; Trueman, D.; Woodcock, F.; Cristino, J. Cost Effectiveness of Inclisiran in Atherosclerotic Cardiovascular Patients with Elevated Low-Density Lipoprotein Cholesterol Despite Statin Use: A Threshold Analysis. Am. J. Cardiovasc. Drugs 2022, 22, 545–556. [Google Scholar] [CrossRef] [PubMed]
- Agarwala, A.; Jones, P.; Nambi, V. The role of antisense oligonucleotide therapy in patients with familial hypercholesterolemia: Risks, benefits, and management recommendations. Curr. Atheroscler. Rep. 2015, 17, 467. [Google Scholar] [CrossRef] [PubMed]
- Parham, J.S.; Goldberg, A.C. Mipomersen and its use in familial hypercholesterolemia. Expert Opin Pharmacother. 2019, 20, 127–131. [Google Scholar] [CrossRef]
- Fogacci, F.; Ferri, N.; Toth, P.P.; Ruscica, M.; Corsini, A.; Cicero, A.F.G. Efficacy and Safety of Mipomersen: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Drugs 2019, 79, 751–766. [Google Scholar] [CrossRef]
- Wong, E.; Goldberg, T. Mipomersen (kynamro): A novel antisense oligonucleotide inhibitor for the management of homozygous familial hypercholesterolemia. Pharm. Ther. 2014, 39, 119–122. [Google Scholar]
- Inazu, A.; Brown, M.L.; Hesler, C.B.; Agellon, L.B.; Koizumi, J.; Takata, K.; Maruhama, Y.; Mabuchi, H.; Tall, A.R. Increased high-density lipoprotein levels caused by a common cholesteryl-ester transfer protein gene mutation. N. Engl. J. Med. 1990, 323, 1234–1238. [Google Scholar] [CrossRef]
- Armitage, J.; Holmes, M.V.; Preiss, D. Cholesteryl Ester Transfer Protein Inhibition for Preventing Cardiovascular Events: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 73, 477–487. [Google Scholar] [CrossRef]
- Tall, A.R.; Rader, D.J. Trials and Tribulations of CETP Inhibitors. Circ. Res. 2018, 122, 106–112. [Google Scholar] [CrossRef]
- Davidson, M.; Liu, S.X.; Barter, P.; Brinton, E.A.; Cannon, C.P.; Gotto, A.M., Jr.; Leary, E.T.; Shah, S.; Stepanavage, M.; Mitchel, Y.; et al. Measurement of LDL-C after treatment with the CETP inhibitor anacetrapib. J. Lipid Res. 2013, 54, 467–472. [Google Scholar] [CrossRef]
- Khoueiry, G.; Abi Rafeh, N.; Sullivan, E.; Saiful, F.; Jaffery, Z.; Kenigsberg, D.N.; Krishnan, S.C.; Khanal, S.; Bekheit, S.; Kowalski, M. Do omega-3 polyunsaturated fatty acids reduce risk of sudden cardiac death and ventricular arrhythmias? A meta-analysis of randomized trials. Heart Lung 2013, 42, 251–256. [Google Scholar] [CrossRef]
- Harris, W.S.; Tintle, N.L.; Imamura, F.; Qian, F.; Korat, A.V.A.; Marklund, M.; Djousse, L.; Bassett, J.K.; Carmichael, P.H.; Chen, Y.Y.; et al. Blood n-3 fatty acid levels and total and cause-specific mortality from 17 prospective studies. Nat. Commun. 2021, 12, 2329. [Google Scholar] [CrossRef]
- Shen, S.; Gong, C.; Jin, K.; Zhou, L.; Xiao, Y.; Ma, L. Omega-3 Fatty Acid Supplementation and Coronary Heart Disease Risks: A Meta-Analysis of Randomized Controlled Clinical Trials. Front. Nutr. 2022, 9, 809311. [Google Scholar] [CrossRef]
- Martinez-Gonzalez, J.; Badimon, L. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: Results of the GISSI-Prevenzione trial–Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Lancet 1999, 354, 447–455. [Google Scholar]
- Aung, T.; Halsey, J.; Kromhout, D.; Gerstein, H.C.; Marchioli, R.; Tavazzi, L.; Geleijnse, J.M.; Rauch, B.; Ness, A.; Galan, P.; et al. Associations of Omega-3 Fatty Acid Supplement Use With Cardiovascular Disease Risks: Meta-analysis of 10 Trials Involving 77 917 Individuals. JAMA Cardiol. 2018, 3, 225–234. [Google Scholar] [CrossRef]
- Bowman, L.; Mafham, M.; Stevens, W.; Haynes, R.; Aung, T.; Chen, F.; Buck, G.; Collins, R.; Armitage, J.; Group, A.S.C. ASCEND: A Study of Cardiovascular Events iN Diabetes: Characteristics of a randomized trial of aspirin and of omega-3 fatty acid supplementation in 15,480 people with diabetes. Am. Heart J. 2018, 198, 135–144. [Google Scholar] [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Albert, C.M.; Gordon, D.; Copeland, T.; et al. Marine n-3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer. N. Engl. J. Med. 2019, 380, 23–32. [Google Scholar] [CrossRef]
- Ridker, P.M.; Rifai, N.; MacFadyen, J.; Glynn, R.J.; Jiao, L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Tardif, J.C.; et al. Effects of Randomized Treatment With Icosapent Ethyl and a Mineral Oil Comparator on Interleukin-1beta, Interleukin-6, C-Reactive Protein, Oxidized Low-Density Lipoprotein Cholesterol, Homocysteine, Lipoprotein(a), and Lipoprotein-Associated Phospholipase A2: A REDUCE-IT Biomarker Substudy. Circulation 2022, 146, 372–379. [Google Scholar] [CrossRef]
- Nicholls, S.J.; Lincoff, A.M.; Garcia, M.; Bash, D.; Ballantyne, C.M.; Barter, P.J.; Davidson, M.H.; Kastelein, J.J.P.; Koenig, W.; McGuire, D.K.; et al. Effect of High-Dose Omega-3 Fatty Acids vs. Corn Oil on Major Adverse Cardiovascular Events in Patients at High Cardiovascular Risk: The STRENGTH Randomized Clinical Trial. JAMA 2020, 324, 2268–2280. [Google Scholar] [CrossRef]
- Gupta, K.; Hirsch, J.R.; Kalsi, J.; Patel, V.; Gad, M.M.; Virani, S.S. Highlights of Cardiovascular Disease Prevention Studies Presented at the 2022 American Heart Association Scientific Sessions. Curr. Atheroscler. Rep. 2023, 25, 31–41. [Google Scholar] [CrossRef]
- Amarin. Vascepa (Icosapent Ethyl)—U.S. Food and Drug Website. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/202057s035lbl.pdf (accessed on 30 December 2023).
- Pharma, W. Lovaza (Omega-3-Acid Ethyl Esters)—U.S. Food and Drug Website. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/021654s043lbl.pdf (accessed on 30 December 2023).
- Virani, S.S.; Morris, P.B.; Agarwala, A.; Ballantyne, C.M.; Birtcher, K.K.; Kris-Etherton, P.M.; Ladden-Stirling, A.B.; Miller, M.; Orringer, C.E.; Stone, N.J. 2021 ACC Expert Consensus Decision Pathway on the Management of ASCVD Risk Reduction in Patients With Persistent Hypertriglyceridemia: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2021, 78, 960–993. [Google Scholar] [CrossRef]
- Khan, S.U.; Lone, A.N.; Khan, M.S.; Virani, S.S.; Blumenthal, R.S.; Nasir, K.; Miller, M.; Michos, E.D.; Ballantyne, C.M.; Boden, W.E.; et al. Effect of omega-3 fatty acids on cardiovascular outcomes: A systematic review and meta-analysis. EClinicalMedicine 2021, 38, 100997. [Google Scholar] [CrossRef]
- Qian, F.; Tintle, N.; Jensen, P.N.; Lemaitre, R.N.; Imamura, F.; Feldreich, T.R.; Nomura, S.O.; Guan, W.; Laguzzi, F.; Kim, E.; et al. Omega-3 Fatty Acid Biomarkers and Incident Atrial Fibrillation. J. Am. Coll. Cardiol. 2023, 82, 336–349. [Google Scholar] [CrossRef]
- Schmier, J.K.; Rachman, N.J.; Halpern, M.T. The cost-effectiveness of omega-3 supplements for prevention of secondary coronary events. Manag. Care 2006, 15, 43–50. [Google Scholar]
- Michaeli, D.T.; Michaeli, J.C.; Boch, T.; Michaeli, T. Cost-Effectiveness of Lipid-Lowering Therapies for Cardiovascular Prevention in Germany. Cardiovasc. Drugs Ther. 2023, 37, 683–694. [Google Scholar] [CrossRef]
- Gao, L.; Moodie, M.; Li, S.C. The cost-effectiveness of omega-3 polyunsaturated fatty acids — The Australian healthcare perspective. Eur. J. Intern. Med. 2019, 67, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Lachaine, J.; Charron, J.N.; Gregoire, J.C.; Hegele, R.A.; Leiter, L.A. Cost-Effectiveness of Icosapent Ethyl (IPE) for the Reduction of the Risk of Ischemic Cardiovascular Events in Canada. Clinicoecon Outcomes Res. 2023, 15, 295–308. [Google Scholar] [CrossRef] [PubMed]
- Staels, B.; Dallongeville, J.; Auwerx, J.; Schoonjans, K.; Leitersdorf, E.; Fruchart, J.C. Mechanism of action of fibrates on lipid and lipoprotein metabolism. Circulation 1998, 98, 2088–2093. [Google Scholar] [CrossRef] [PubMed]
- Rubins, H.B.; Robins, S.J.; Collins, D.; Fye, C.L.; Anderson, J.W.; Elam, M.B.; Faas, F.H.; Linares, E.; Schaefer, E.J.; Schectman, G.; et al. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. N. Engl. J. Med. 1999, 341, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Tenkanen, L.; Manttari, M.; Kovanen, P.T.; Virkkunen, H.; Manninen, V. Gemfibrozil in the treatment of dyslipidemia: An 18-year mortality follow-up of the Helsinki Heart Study. Arch. Intern. Med. 2006, 166, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Frick, M.H.; Elo, O.; Haapa, K.; Heinonen, O.P.; Heinsalmi, P.; Helo, P.; Huttunen, J.K.; Kaitaniemi, P.; Koskinen, P.; Manninen, V.; et al. Helsinki Heart Study: Primary-prevention trial with gemfibrozil in middle-aged men with dyslipidemia. Safety of treatment, changes in risk factors, and incidence of coronary heart disease. N. Engl. J. Med. 1987, 317, 1237–1245. [Google Scholar] [CrossRef]
- Tricor. Tricor (Fenofibrate)—U.S. Food and Drug Website. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/021656s029lbl.pdf (accessed on 30 December 2023).
- Hay, J.W.; Sterling, K.L. Cost effectiveness of treating low HDL-cholesterol in the primary prevention of coronary heart disease. Pharmacoeconomics 2005, 23, 133–141. [Google Scholar] [CrossRef]
- Abushanab, D.; Al-Badriyeh, D.; Marquina, C.; Bailey, C.; Jaam, M.; Liew, D.; Ademi, Z. A Systematic Review of Cost-Effectiveness of Non-Statin Lipid-Lowering Drugs for Primary and Secondary Prevention of Cardiovascular Disease in Patients with Type 2 Diabetes Mellitus. Curr. Probl. Cardiol. 2023, 48, 101211. [Google Scholar] [CrossRef]
- Maranhao, R.C.; Carvalho, P.O.; Strunz, C.C.; Pileggi, F. Lipoprotein (a): Structure, pathophysiology and clinical implications. Arq. Bras. Cardiol. 2014, 103, 76–84. [Google Scholar] [CrossRef]
- Reyes-Soffer, G.; Ginsberg, H.N.; Berglund, L.; Duell, P.B.; Heffron, S.P.; Kamstrup, P.R.; Lloyd-Jones, D.M.; Marcovina, S.M.; Yeang, C.; Koschinsky, M.L.; et al. Lipoprotein(a): A Genetically Determined, Causal, and Prevalent Risk Factor for Atherosclerotic Cardiovascular Disease: A Scientific Statement From the American Heart Association. Arterioscler. Thromb. Vasc. Biol. 2022, 42, e48–e60. [Google Scholar] [CrossRef]
- O’Donoghue, M.L.; Rosenson, R.S.; Gencer, B.; Lopez, J.A.G.; Lepor, N.E.; Baum, S.J.; Stout, E.; Gaudet, D.; Knusel, B.; Kuder, J.F.; et al. Small Interfering RNA to Reduce Lipoprotein(a) in Cardiovascular Disease. N. Engl. J. Med. 2022, 387, 1855–1864. [Google Scholar] [CrossRef]
- Tsimikas, S.; Karwatowska-Prokopczuk, E.; Gouni-Berthold, I.; Tardif, J.C.; Baum, S.J.; Steinhagen-Thiessen, E.; Shapiro, M.D.; Stroes, E.S.; Moriarty, P.M.; Nordestgaard, B.G.; et al. Lipoprotein(a) Reduction in Persons with Cardiovascular Disease. N. Engl. J. Med. 2020, 382, 244–255. [Google Scholar] [CrossRef]
- Thompson, G.; Parhofer, K.G. Current Role of Lipoprotein Apheresis. Curr. Atheroscler. Rep. 2019, 21, 26. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Prado, R.; Perez-Gomez, M.V.; Ortiz, A. Pelacarsen for lowering lipoprotein(a): Implications for patients with chronic kidney disease. Clin. Kidney J. 2020, 13, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Rambaran, C.; Wilson, R.J.; Swerdlow, D.I.; Campion, G.V.; Scrimgeour, A.C.; Nissen, S.E. Time Averaged Lipoprotein (a) Reduction With Sln360, a Novel Sirna Targeting Lp (a,) in Healthy Adults With Elevated Lp(a). Circulation 2022, 146, A10469. [Google Scholar] [CrossRef]
- Nissen, S.E.; Linnebjerg, H.; Shen, X.; Wolski, K.; Ma, X.; Lim, S.; Michael, L.F.; Ruotolo, G.; Gribble, G.; Navar, A.M.; et al. Lepodisiran, an Extended-Duration Short Interfering RNA Targeting Lipoprotein(a): A Randomized Dose-Ascending Clinical Trial. JAMA 2023, 330, 2075–2083. [Google Scholar] [CrossRef]
| Trial, Sample Size | Study Population | Intervention and Comparator | 1° Outcome, Follow-Up Period | 1° Outcome Result |
|---|---|---|---|---|
| Yokoyama (2007) JELIS [72] n = 18,645 | 1° and 2° prevention—Patients 40–75 years old with total cholesterol ≥ 6.5 mmol/L (LDL-C 4.4 mmol/L), with and without coronary artery disease | Intervention: 1800 mg EPA daily with statin. Comparator: Statin only | Composite of sudden cardiac death, fatal and non-fatal MI, unstable angina, angioplasty, stenting, and coronary artery bypass. F/U: 4.6 years | Overall, EPA treatment decreased major coronary events by 19% (2.8% in EPA, 3.5% in controls; p = 0.011). In patients with a history of CAD, EPA treatment ↓ major coronary events by 19% (8.7% in EPA group, 10.7% in controls; p = 0.048). In patients without a history of CAD, EPA treatment ↓ major coronary events by 18%, but this finding was not significant (1.4% in EPA group, 1.7% in control; p = 0.132) |
| Bhatt (2019) REDUCE-IT [73] n = 8179 | 1° and 2° prevention—Patients ≥ 45 years old with ASCVD (2° prevention) or ≥50 years old with diabetes mellitus and one additional risk factor (1° prevention) on statins | Interventio n: Icosapent ethyl 4 g/d. Comparator: Oral matching placebo | Composite of cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, coronary revascularization, and unstable angina. F/U: 4.9 years | The 1° endpoint occurred in 17.2% of patients on EPA compared to 22.0% of patients on placebo (HR, 0.75; 95% CI, 0.68 to 0.83; p < 0.001), representing a placebo-corrected difference of 4.8% (95% CI, 3.1% to 6.5%). The number needed to treat to avoid one 1° endpoint event was 21 (95% CI, 15 to 33). |
| Nishizaki (2023) RESPECT-EPA [74] n = 2460 | 2° prevention—Patients aged 20–79 years with CAD who took statins for >1 month | Intervention: 1800 mg/day highly purified EPA + standard statin. Control: Standard statin only | Composite of cardiovascular death, non-fatal myocardial infarction, non-fatal ischemic stroke, unstable angina, and clinically indicated coronary revascularization. F/U: 6 years | At the 6-year follow-up, there was no significant difference in adverse cardiac events between the EPA and control groups (HR 0.785, 95% CI: 0.616–1.001, p = 0.055). |
| Trial, Sample Size, Drug | Study Population | Intervention and Comparator | 1° Outcome, Follow-Up Period | 1° Outcome Result |
|---|---|---|---|---|
| Das Pradhan (2022) PROMINENT [75] n = 10,497 Pemafibrate | 1° and 2° prevention—Men ≥ 50 and women ≥ 55 years old with type 2 diabetes, TG levels between 200 and 499 mg/dL, and HDL ≤ 40 mg/dL, with and without prior ASCVD | Intervention: Pemafibrate 0.2 mg tablets twice daily. Comparator: Matching placebo | Composite of non-fatal myocardial infarction, ischemic stroke, coronary revascularization, and death from cardiovascular causes. F/U: 4 years | A 1° endpoint event occurred in 572 patients in the pemafibrate group and in 560 of those in the placebo group (HR, 1.03; 95% CI, 0.91 to 1.15), with no apparent effect modification in any pre-specified subgroup |
| Accord Study Group (2010) ACCORD [76] n = 5518 Fenofibrate | 2° prevention—Type 2 diabetic patients 55–79 years old with LDL-C ranging from 80 to 160 mg/dL, TG < 750 mg/dL (if not on lipid therapy) or TG < 400 mg/dL (if on lipid therapy) with evidence of subclinical ASCVD, and at least two additional cardiovascular risk factors | Intervention: Initially at 160 mg per day in 2001–2004 participants, after which the dose was managed relative to the estimated GFR (due to rises in creatinine levels). Comparator: Matched placebo | Composite of first occurrence of a major cardiovascular event, including non-fatal myocardial infarction, non-fatal stroke, and death from cardiovascular causes. F/U: 5.6 years | The annual rate of the 1° outcome was 2.2% in the fenofibrate group and 2.4% in the placebo group (HR in the fenofibrate group, 0.92; 95% CI, 0.79 to 1.08; p = 0.32) |
| Keech (2005) FIELD [77] n = 9795 Fenofibrate | 1° prevention—Patients aged 50–75 years old with type 2 diabetes, total cholesterol concentration between 3 and 6.5 mmol/L, and no indications for statins | Intervention: Micronized fenofibrate 200 mg daily. Comparator: Matched placebo | A composite of coronary heart disease deaths, MI, stroke, and coronary and carotid revascularization. F/U: 5 years | 5.2% of patients on fenofibrate had a coronary event, compared to 5.9% on placebo (relative reduction of 11%; HR 0.89, 95% CI 0.75–1.05; p = 0.16) |
| Trial, Sample Size, Drug | Study Population | Intervention and Comparator | 1° Outcome, Follow-Up Period | 1° Outcome Results |
|---|---|---|---|---|
| O’Donoghue (2022) OCEAN(a) [151] n = 281 Olpasiran | 2° prevention—Patients 18–80 years old with established ASCVD and Lp(a) > 150 nmol/L | Intervention: Olpasiran at four doses (10 mg every 12 weeks, 75 mg every 12 weeks, 225 mg every 12 weeks, or 225 mg every 24 weeks) administered subcutaneously. Comparator: Matched placebo administered subcutaneously. | Percent change in lipoprotein A concentration from baseline to week 36. F/U: 48 weeks | The placebo-adjusted mean percent change in the Lp(a) concentration was −70.5% (95% CI, −75.1 to −65.9) with the 10 mg dose every 12 weeks, −97.4% (95%, CI, −102.0 to −92.8) with the 75 mg dose every 12 weeks, −101.1% (95% CI, −105.8 to −96.5) with the 225 mg dose every 12 weeks, and −100.5% (95% CI, −105.2 to −95.8) with the 225 mg dose every 24 weeks (p < 0.001 for all comparisons with baseline) |
| (Ongoing) Evaluate SLN360 in Participants with Elevated Lipoprotein(a) at High Risk of Atherosclerotic Cardiovascular Disease Events (NCT05537571) n = 160 SLN360 | 2° prevention—Patients 18–80 years old with Lp(a) > 125 nmol/L at high risk of ASCVD events | Intervention: Subcutaneous administration of SLN360 at 30, 100, 300, or 600 mg. Comparator: Matched placebo | Change in Lp(a) from baseline at weeks 48 and 60. F/U: 60 weeks | Results pending |
| (Ongoing) Lp(a)HORIZON (NCT04023552) n = 8323 Pelacarsen | 2° prevention—Patients 18–90 years old with LDL-C ≥ 70 mg/dL and established CVD | Intervention: Subcutaneous administration of 80 mg pelacarsen monthly. Comparator: Subcutaneous injection of matching placebo every month | Time to occurrence of MACE in 4 years. F/U: 4 years | Results pending |
| Tsimikas (2020) AKCEA-APO(a)-LRx [152] n = 286 Pelacarsen | 2° prevention—Patients 18–80 years old with established ASCVD and elevated lipoprotein A > 60 mg/dL or 150 nMol/L on standard-of-care preventative therapy | Intervention: s = Subcutaneous injection of APOa -LRx at 20, 40, or 60 mg every 4 weeks, 20 mg every 2 weeks, or 20 mg every week vs. placebo for 6–12 months. Comparator: Matched placebo subcutaneous injections. | Percent change in Lp(a) from baseline to month 6 of exposure (week 25 in groups that received monthly doses and week 27 in groups that received more frequent doses). F/U: 1 year | Olpasiran therapy demonstrated mean percent decreases in lipoprotein A of 35% at a dose of 20 mg every 4 weeks, 56% at 40 mg every 4 weeks, 58% at 20 mg every 2 weeks, 72% at 60 mg every 4 weeks, and 80% at 20 mg every week, as compared with 6% with placebo (p-values for the comparison with the placebo ranged from 0.003 to <0.001). |
| (Ongoing) OCEAN(a)–Outcomes Trial (NCT05581303) n = 6000 Olpasiran | 2° prevention—Patients 18–85 years old with Lp(a) ≥ 200 nmol/L and a history of ASCVD | Intervention: Subcutaneous injections of olpasiran every 12 weeks. Comparator: Matched placebo subcutaneous injections | Time to CHD death, MI, or urgent coronary revascularization. F/U: 4 years | Results pending |
| (Ongoing) A Multicenter Trial Assessing the Impact of Lp(a) Lowering With Pelacarsen on the Rate of Weekly Lipoprotein Apheresis Sessions in Patients With Hyperlipoproteinemia(a) and Established Cardiovascular Disease in Germany (NCT05305664) n = 60 Pelacarsen | 2° prevention—Patients 60 adults aged 18–80 with Lp(a) > 60 mg/dL and prior MI/stroke/PVD undergoing lipoprotein apheresis in Germany | Intervention: Subcutaneous injections of pelacarsen 80 mg monthly. Comparator: Matched placebo subcutaneous injections | Rate of lipoprotein apheresis sessions performed over 52 weeks, normalized to the weekly lipoprotein apheresis schedule. F/U: 52 weeks | Results pending |
| (Ongoing) KRAKEN (NCT05563246) n = 233 LY3473329 | 1° and 2° prevention—Patients ≥ 40 years old with Lp(a) ≥ 175 nmol/L at high risk of cardiovascular events | Intervention: Three different oral doses of LY3473329. Comparator: Oral placebo | Percent change from baseline in Lp(a). F/U: 12 weeks | Results pending |
| (Ongoing) A Study of LY3819469 in Participants with Elevated Lp(a) (NCT05565742) n = 254 LY3819469 | 1° and 2° prevention—Patients ≥40 years old with Lp(a) ≥175 nmol/L at high risk of cardiovascular events | Intervention: 4 experimental groups: (1) LY3819469 Dose 1 SC; (2) LY3819469 Dose 2 SC; (3) LY3819469 Dose 3 SC; (4) LY3819469 Dose 4 SC + placebo. Comparator: Matched placebo | Percent change from baseline in time-averaged Lp(a) F/U: 180 days | Results pending |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kayani, T.; Ahmad, B.; Chang, R.S.; Qian, F.; Sahinoz, M.; Rehan, M.W.; Giaimo, A.; Spatz, E.S.; Hu, J.-R. Beyond Statins: Novel Lipid-Lowering Agents for Reducing Risk of Atherosclerotic Cardiovascular Disease. Pharmacoepidemiology 2024, 3, 117-168. https://doi.org/10.3390/pharma3010009
Kayani T, Ahmad B, Chang RS, Qian F, Sahinoz M, Rehan MW, Giaimo A, Spatz ES, Hu J-R. Beyond Statins: Novel Lipid-Lowering Agents for Reducing Risk of Atherosclerotic Cardiovascular Disease. Pharmacoepidemiology. 2024; 3(1):117-168. https://doi.org/10.3390/pharma3010009
Chicago/Turabian StyleKayani, Teimur, Bachar Ahmad, Rachel S. Chang, Frank Qian, Melis Sahinoz, Muhammad Waqar Rehan, Antonio Giaimo, Erica S. Spatz, and Jiun-Ruey Hu. 2024. "Beyond Statins: Novel Lipid-Lowering Agents for Reducing Risk of Atherosclerotic Cardiovascular Disease" Pharmacoepidemiology 3, no. 1: 117-168. https://doi.org/10.3390/pharma3010009
APA StyleKayani, T., Ahmad, B., Chang, R. S., Qian, F., Sahinoz, M., Rehan, M. W., Giaimo, A., Spatz, E. S., & Hu, J.-R. (2024). Beyond Statins: Novel Lipid-Lowering Agents for Reducing Risk of Atherosclerotic Cardiovascular Disease. Pharmacoepidemiology, 3(1), 117-168. https://doi.org/10.3390/pharma3010009