

Methods for Testing Meniscal Repair Using a 3D-Printed Meniscus
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. 3D-Printed Meniscus Fabrication
2.1.1. Preparation of Ink
2.1.2. 3D Printing
2.1.3. Post-Print Processing
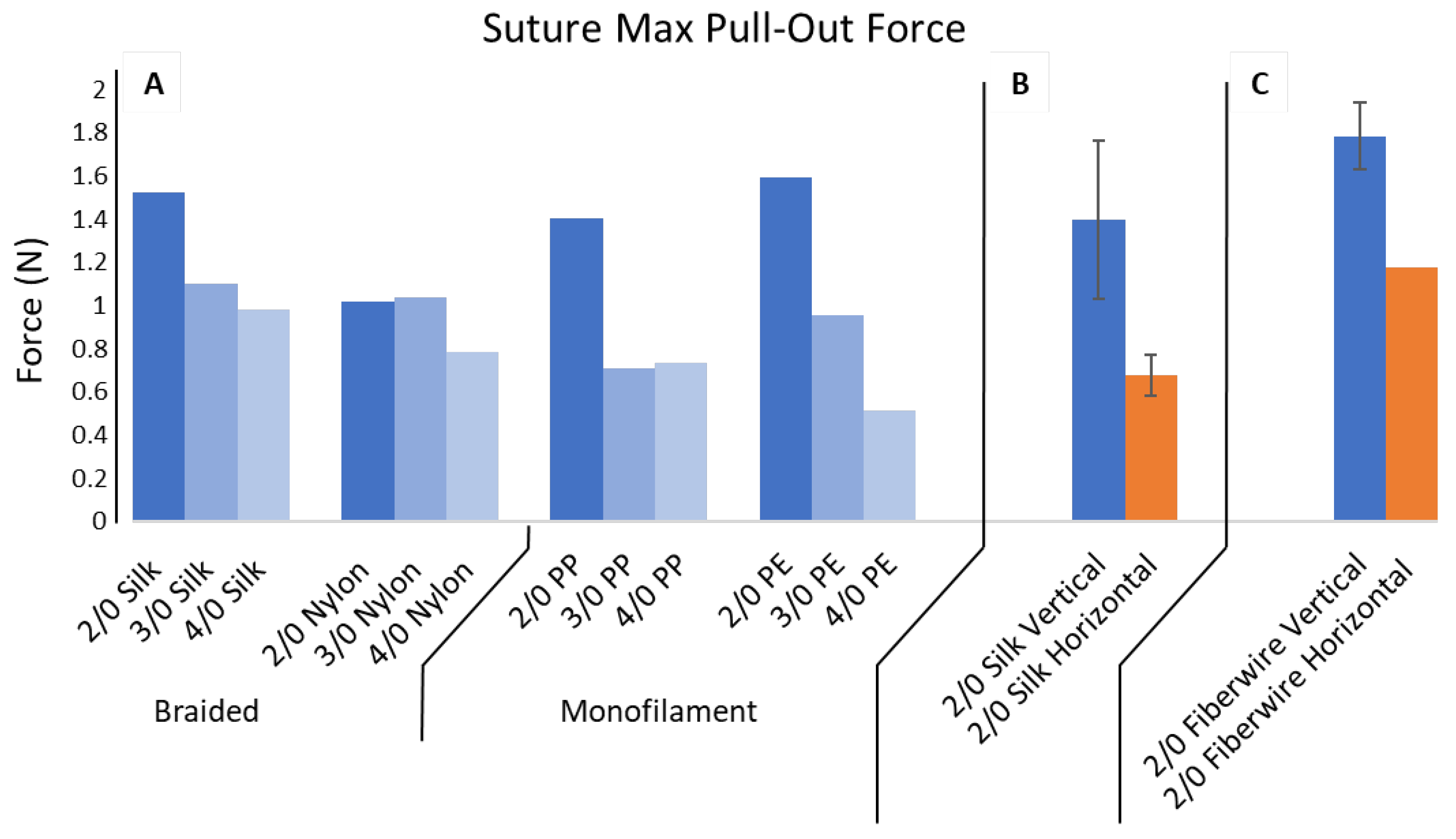
2.2. Suture Pull-Out Force
2.2.1. Custom-Built Test Apparatus
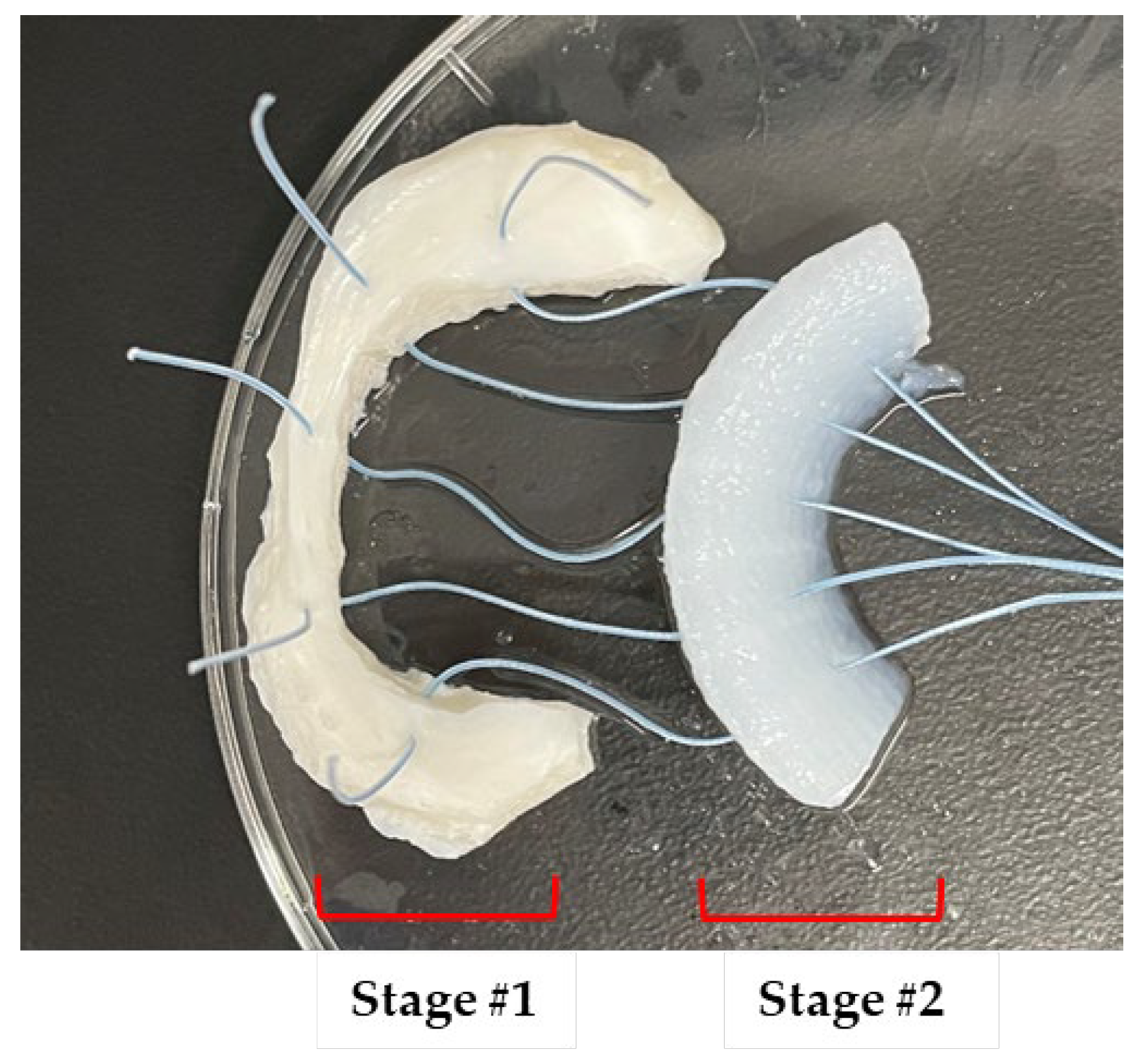
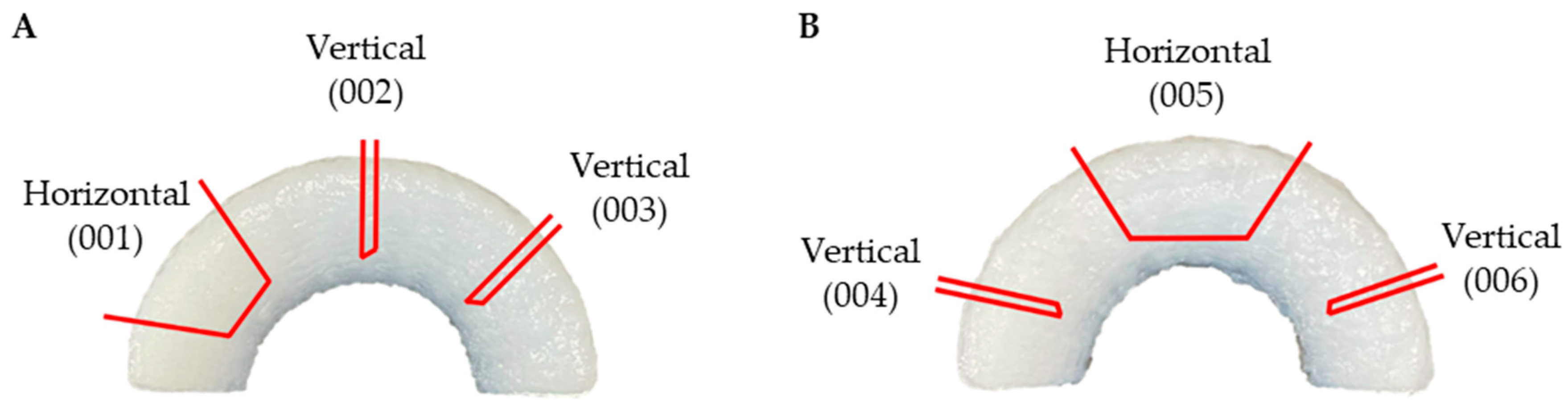
2.2.2. Vertical and Horizontal Suture Placement and Type
2.2.3. Pull-Out Testing
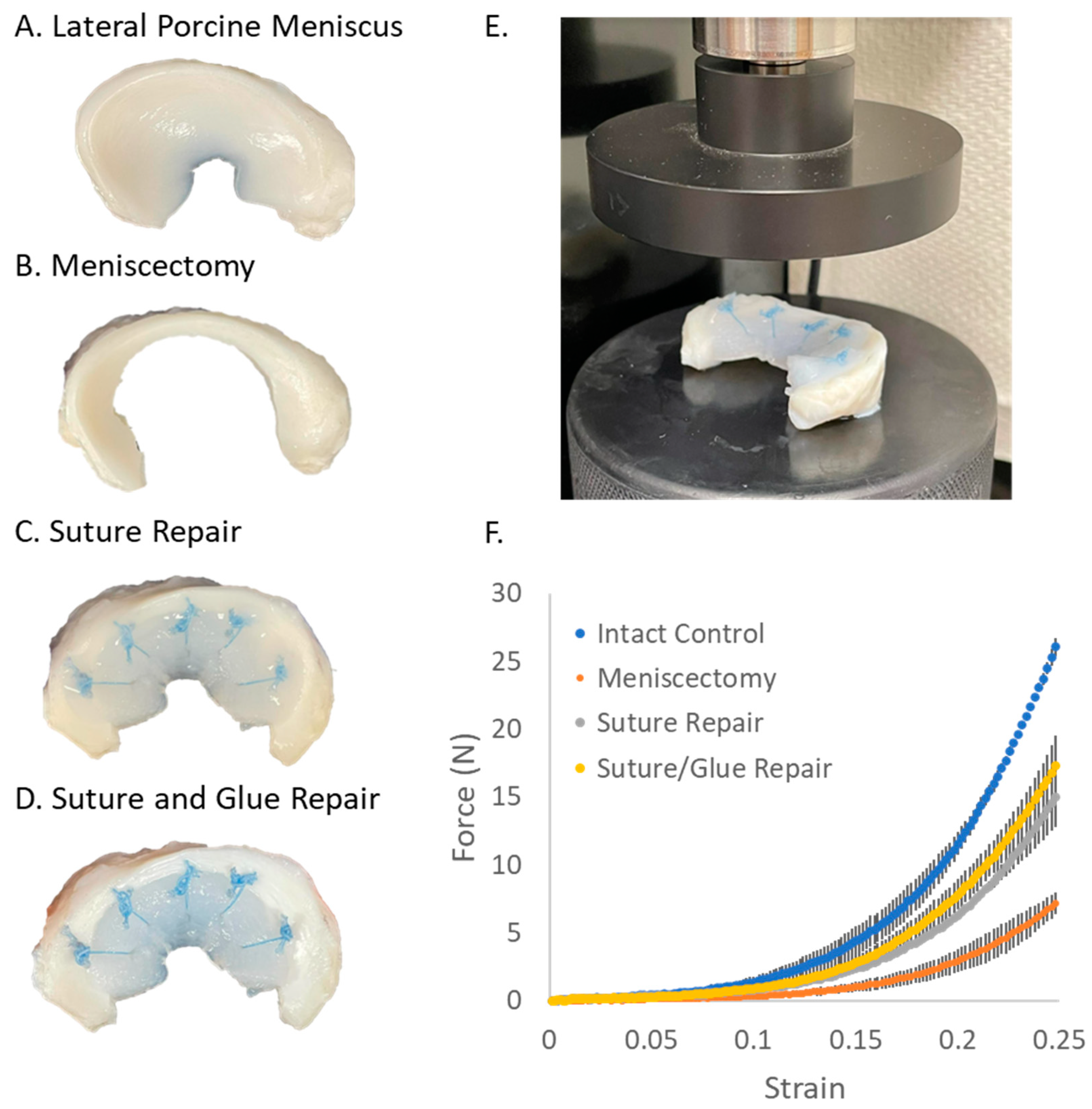
2.3. Compression Testing in Isolated Porcine Menisci
2.3.1. Isolated Porcine Meniscus Preparation
2.3.2. Isolated Porcine Meniscus Compression Testing
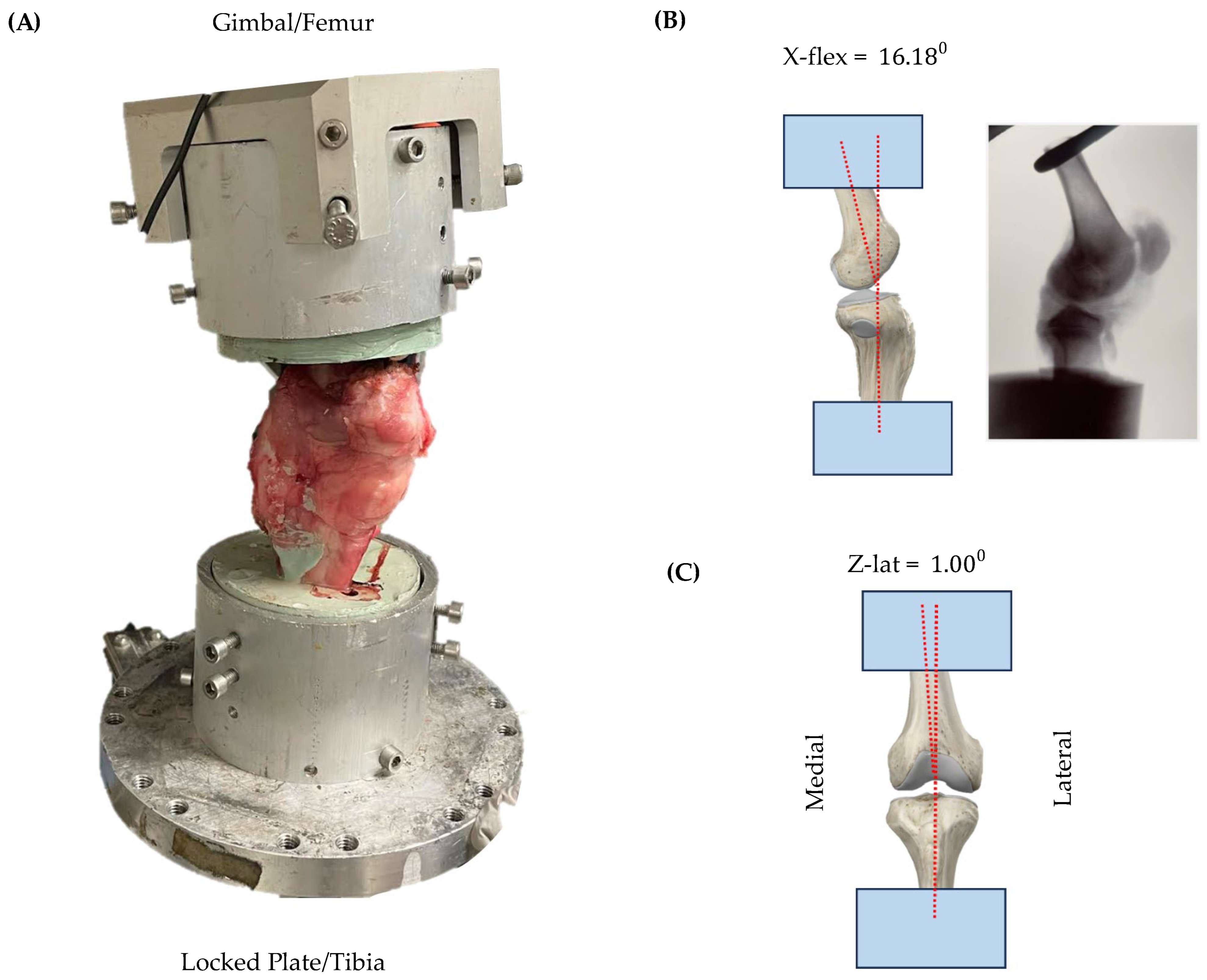
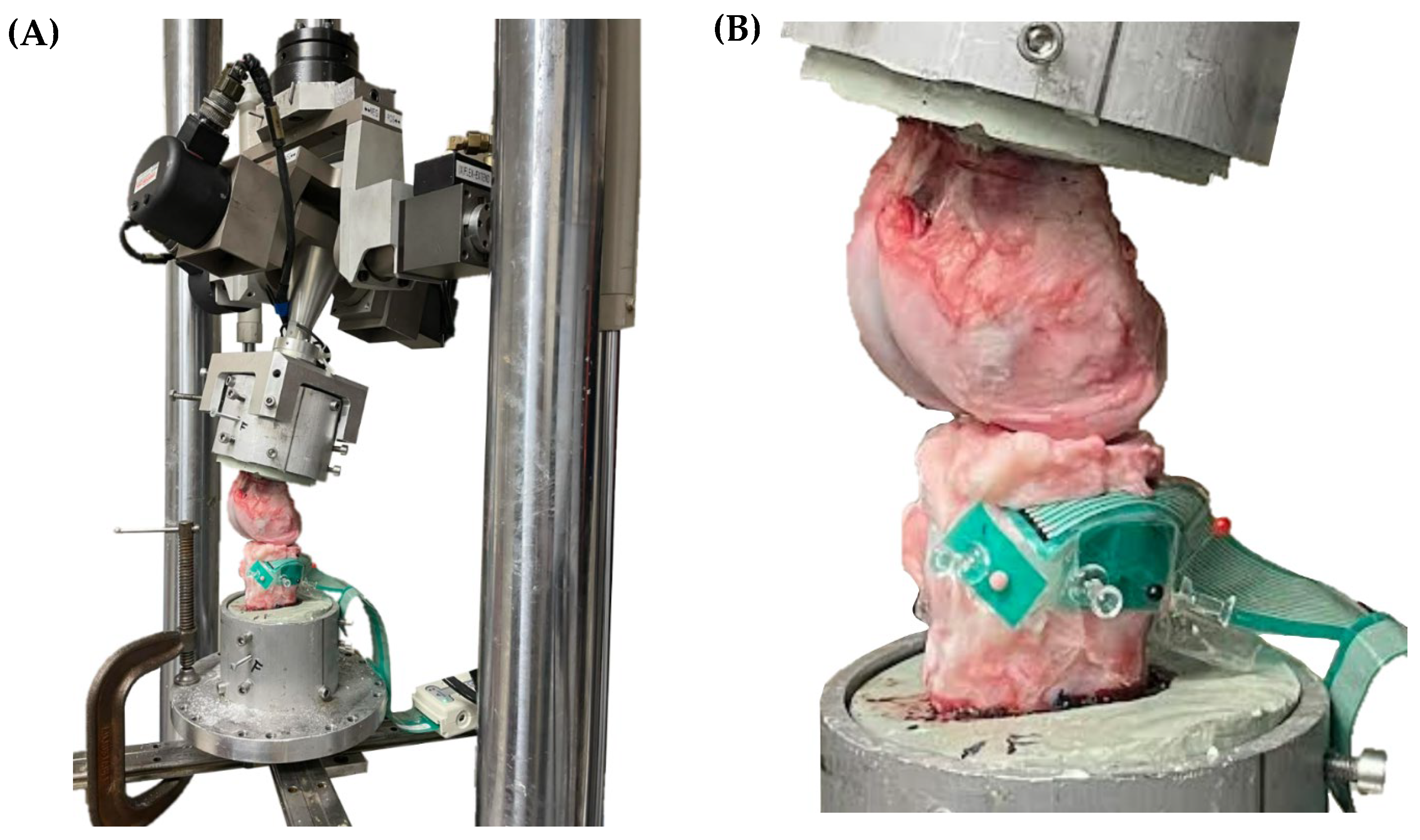
2.4. Compression Testing in Ex Vivo Porcine Knees
2.4.1. Porcine Knee Dissection
2.4.2. Porcine Knee Potting
2.4.3. MTS Calibration
2.4.4. Porcine Knee Disarticulation
2.4.5. Tekscan Sensor Placement
2.4.6. Porcine Meniscus Compression Testing
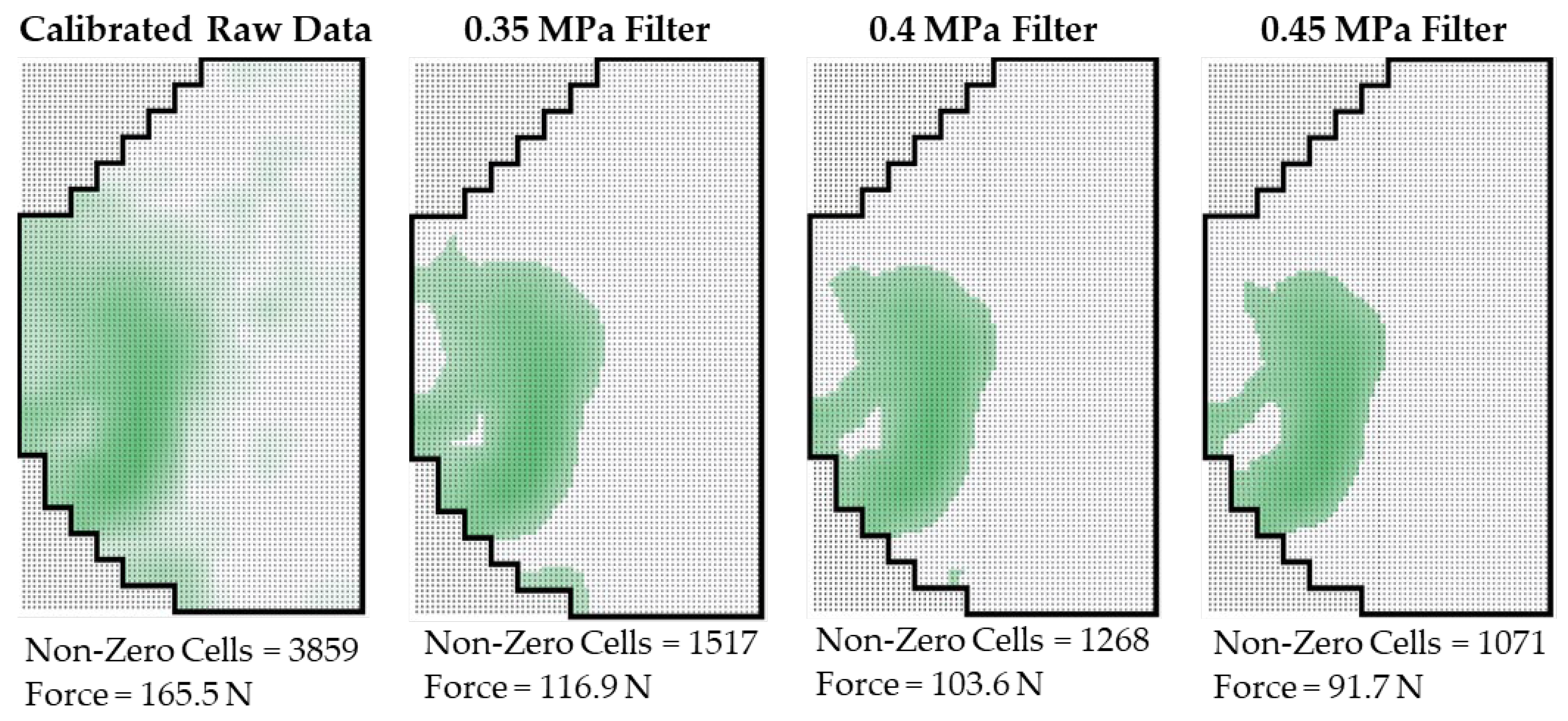
2.4.7. Tekscan Data Calibration
3. Results
3.1. 3D-Printed Meniscus Fabrication
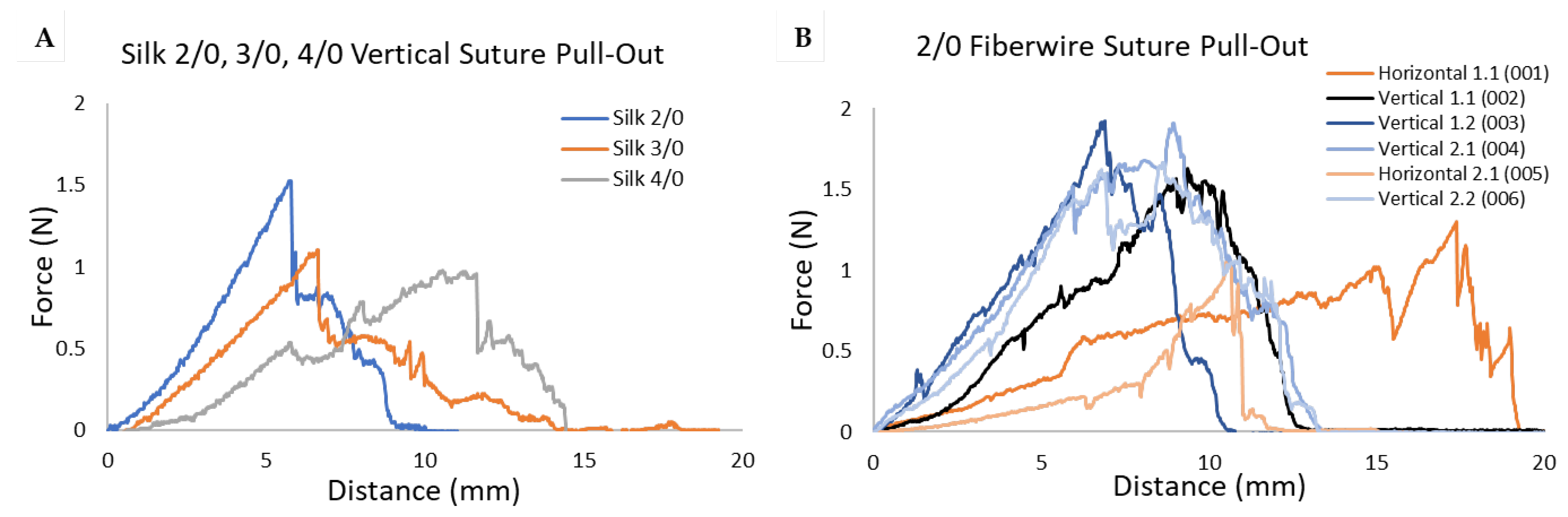
3.2. Suture Pull-Out Force
3.3. Compression Testing in Isolated Porcine Menisci
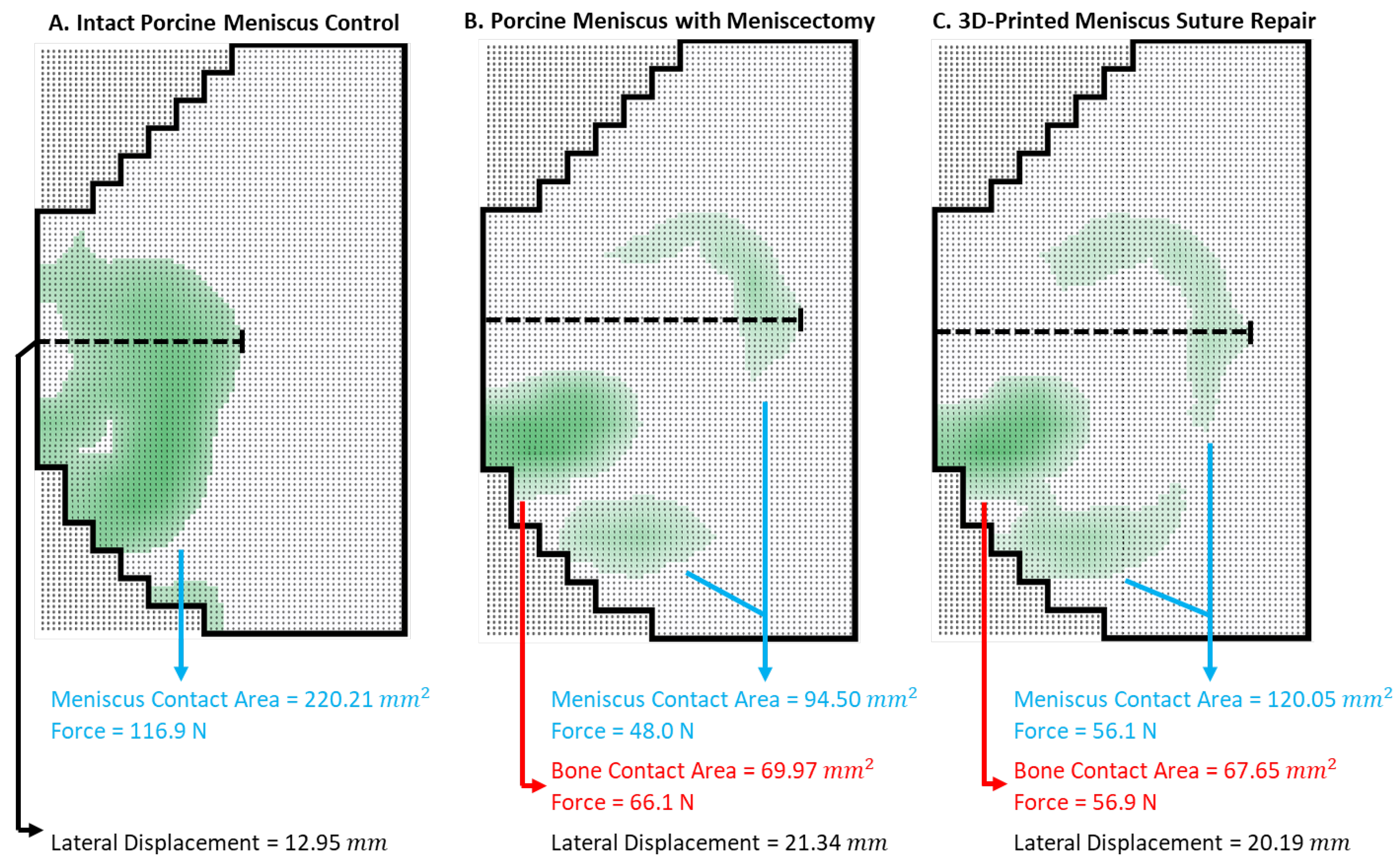
3.4. Compression Testing in Ex Vivo Porcine Knees
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Athanasiou, K.A.; Sanchez-Adams, J. Engineering the Knee Meniscus; Morgan and Claypool: San Rafael, CA, USA, 2009. [Google Scholar]
- Logerstedt, D.S.; Snyder-Mackler, L.; Ritter, R.C.; Axe, M.J.; Orthopedic, A. Section of the American Physical Therapy, Knee pain and mobility impairments: Meniscal and articular cartilage lesions. J. Orthop. Sports Phys. Ther. 2010, 40, A1–A35. [Google Scholar] [PubMed]
- Nielsen, A.B.; Yde, J. Epidemiology of acute knee injuries: A prospective hospital investigation. J. Trauma 1991, 31, 1644–1648. [Google Scholar] [CrossRef] [PubMed]
- Donohue, M.A.; Zhou, L.; Haley, C.A. Meniscus Injuries in the Military Athlete. J. Knee Surg. 2019, 32, 123–126. [Google Scholar] [PubMed]
- Jones, J.C.; Burks, R.; Owens, B.D.; Sturdivant, R.X.; Svoboda, S.J.; Cameron, K.L. Incidence and risk factors associated with meniscal injuries among active-duty US military service members. J. Athl. Train. 2012, 47, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Snoeker, B.A.; Bakker, E.W.; Kegel, C.A.; Lucas, C. Risk factors for meniscal tears: A systematic review including meta-analysis. J. Orthop. Sports Phys. Ther. 2013, 43, 352–367. [Google Scholar] [CrossRef]
- Cook, J.L. The current status of treatment for large meniscal defects. Clin. Orthop. Relat. Res. 2005, 435, 88–95. [Google Scholar] [CrossRef]
- Doral, M.N.; Bilge, O.; Huri, G.; Turhan, E.; Verdonk, R. Modern treatment of meniscal tears. EFORT Open Rev. 2018, 3, 260–268. [Google Scholar] [CrossRef]
- Antosh, I.J.; Cameron, K.L.; Marsh, N.A.; Posner, M.A.; DeBerardino, T.M.; Svoboda, S.J.; Owens, B.D. Likelihood of Return to Duty Is Low After Meniscal Allograft Transplantation in an Active-duty Military Population. Clin. Orthop. Relat. Res. 2020, 478, 722–730. [Google Scholar] [CrossRef]
- Lee, J.M.; Yeong, W.Y. Design and Printing Strategies in 3D Bioprinting of Cell-Hydrogels: A Review. Adv. Healthc. Mater. 2016, 5, 2856–2865. [Google Scholar] [CrossRef]
- Yan, Q.; Dong, H.; Su, J.; Han, J.; Song, B.; Wei, Q.; Shi, Y. A Review of 3D Printing Technology for Medical Applications. Engineering 2018, 4, 729–742. [Google Scholar] [CrossRef]
- Chartrain, N.A.; Gilchrist, K.H.; Ho, V.B.; Klarmann, G.J. 3D bioprinting for the repair of articular cartilage and osteochondral tissue. Bioprinting 2022, 28, e00239. [Google Scholar] [CrossRef]
- Senior, J.J.; Cooke, M.E.; Grover, L.M.; Smith, A.M. Fabrication of Complex Hydrogel Structures Using Suspended Layer Additive Manufacturing (SLAM). Adv. Funct. Mater. 2019, 29, 1904845. [Google Scholar] [CrossRef]
- Moxon, S.R.; Cooke, M.E.; Cox, S.C.; Snow, M.; Jeys, L.; Jones, S.W.; Smith, A.M.; Grover, L.M. Suspended Manufacture of Biological Structures. Adv. Mater. 2017, 29, 1605594. [Google Scholar] [CrossRef] [PubMed]
- Hinton, T.J.; Jallerat, Q.; Palchesko, R.N.; Park, J.H.; Grodzicki, M.S.; Shue, H.J.; Ramadan, M.H.; Hudson, A.R.; Feinberg, A.W. Three-dimensional printing of complex biological structures by freeform reversible embedding of suspended hydrogels. Sci. Adv. 2015, 1, e1500758. [Google Scholar] [CrossRef] [PubMed]
- Bahcecioglu, G.; Hasirci, N.; Bilgen, B.; Hasirci, V. A 3D printed PCL/hydrogel construct with zone-specific biochemical composition mimicking that of the meniscus. Biofabrication 2019, 11, 025002. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, L.K.; Huebner, P.; Fisher, M.B.; Spang, J.T.; Starly, B.; Shirwaiker, R.A. 3D-Bioprinting of Polylactic Acid (PLA) Nanofiber-Alginate Hydrogel Bioink Containing Human Adipose-Derived Stem Cells. ACS Biomater. Sci. Eng. 2016, 2, 1732–1742. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.Z.; Wang, S.J.; Zhang, J.Y.; Jiang, W.B.; Huang, A.B.; Qi, Y.S.; Ding, J.X.; Chen, X.S.; Jiang, D.; Yu, J.K. 3D-Printed Poly(epsilon-caprolactone) Scaffold Augmented with Mesenchymal Stem Cells for Total Meniscal Substitution: A 12- and 24-Week Animal Study in a Rabbit Model. Am. J. Sports Med. 2017, 45, 1497–1511. [Google Scholar] [CrossRef]
- Bahcecioglu, G.; Bilgen, B.; Hasirci, N.; Hasirci, V. Anatomical meniscus construct with zone specific biochemical composition and structural organization. Biomaterials 2019, 218, 119361. [Google Scholar] [CrossRef]
- Szojka, A.; Lalh, K.; Andrews, S.H.J.; Jomha, N.M.; Osswald, M.; Adesida, A.B. Biomimetic 3D printed scaffolds for meniscus tissue engineering. Bioprinting 2017, 8, 1–7. [Google Scholar] [CrossRef]
- ICengiz, F.; Pitikakis, M.; Cesario, L.; Parascandolo, P.; Vosilla, L.; Viano, G.; Oliveira, J.M.; Reis, R.L. Building the basis for patient-specific meniscal scaffolds: From human knee MRI to fabrication of 3D printed scaffolds. Bioprinting 2016, 1–2, 1–10. [Google Scholar] [CrossRef]
- Romanazzo, S.; Vedicherla, S.; Moran, C.; Kelly, D.J. Meniscus ECM-functionalised hydrogels containing infrapatellar fat pad-derived stem cells for bioprinting of regionally defined meniscal tissue. J. Tissue Eng. Regen. Med. 2018, 12, e1826–e1835. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, A.; Mandal, B.B. A three-dimensional printed silk-based biomimetic tri-layered meniscus for potential patient-specific implantation. Biofabrication 2019, 12, 015003. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.Z.; Chen, Y.R.; Wang, S.J.; Zhao, F.; Wang, X.G.; Yang, F.; Shi, J.J.; Ge, Z.G.; Ding, W.Y.; Yang, Y.C.; et al. Orchestrated biomechanical, structural, and biochemical stimuli for engineering anisotropic meniscus. Sci. Transl. Med. 2019, 11, eaao0750. [Google Scholar] [CrossRef] [PubMed]
- Klarmann, G.J.; Piroli, M.E.; Loverde, J.R.; Nelson, A.F.; Li, Z.; Gilchrist, K.H.; Gaston, J.D.; Ho, V.B. 3D printing a universal knee meniscus using a custom collagen ink. Bioprinting 2023, 31, e00272. [Google Scholar] [CrossRef]
- Puetzer, J.L.; Bonassar, L.J. High density type I collagen gels for tissue engineering of whole menisci. Acta Biomater. 2013, 9, 7787–7795. [Google Scholar] [CrossRef]
- Klarmann, G.J.; Gaston, J.; Ho, V.B. A review of strategies for development of tissue engineered meniscal implants. Biomater. Biosyst. 2021, 4, 100026. [Google Scholar] [CrossRef] [PubMed]
- Drakos, M.C.; Allen, A.A. Meniscal Structure, Function, Repair, and Replacement. In Oncology and Basic Science; Damron, T.A., Ed.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2008; pp. 443–451. [Google Scholar]
- Skaggs, D.L.; Warden, W.H.; Mow, V.C. Radial tie fibers influence the tensile properties of the bovine medial meniscus. J. Orthop. Res. 1994, 12, 176–185. [Google Scholar] [CrossRef]
- Boenisch, U.W.; Faber, K.J.; Ciarelli, M.; Steadman, J.R.; Arnoczky, S.P. Pull-out strength and stiffness of meniscal repair using absorbable arrows or Ti-Cron vertical and horizontal loop sutures. Am. J. Sports Med. 1999, 27, 626–631. [Google Scholar] [CrossRef]
- Feucht, M.J.; Grande, E.; Brunhuber, J.; Rosenstiel, N.; Burgkart, R.; Imhoff, A.B.; Braun, S. Biomechanical evaluation of different suture materials for arthroscopic transtibial pull-out repair of posterior meniscus root tears. Knee Surg Sports Traumatol. Arthrosc. 2015, 23, 132–139. [Google Scholar] [CrossRef]
- Rimmer, M.G.; Nawana, N.S.; Keene, G.C.; Pearcy, M.J. Failure strengths of different meniscal suturing techniques. Arthroscopy 1995, 11, 146–150. [Google Scholar] [CrossRef]
- Zhang, L.; Li, W.; Lin, C.; Zhou, Z. Friction Behavior at the Interface Between Surgical Sutures and Tissues. Tribol. Lett. 2017, 65, 127. [Google Scholar] [CrossRef]
- Matthews, J.R.; Wang, J.; Zhao, J.; Kluczynski, M.A.; Bisson, L.J. The influence of suture materials on the biomechanical behavior of suture-meniscal specimens: A comparative study in a porcine model. Knee Surg. Relat. Res. 2020, 32, 42. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.L.; Yi, S.J.; Ren, Y.; Zimmerman, T.A.; Zhang, L.-Q. Tibiofemoral Contact Mechanics with Horizontal Cleavage Tear and Resection of the Medial Meniscus in the Human Knee. J. Bone Jt. Surg. 2016, 98, 1829–1836. [Google Scholar] [CrossRef] [PubMed]
- Ode, G.E.; Van Thiel, G.S.; McArthur, S.A.; Dishkin-Paset, J.; Leurgans, S.E.; Shewman, E.F.; Wang, V.M.; Cole, B.J. Effects of serial sectioning and repair of radial tears in the lateral meniscus. Am. J. Sports Med. 2012, 40, 1863–1870. [Google Scholar] [CrossRef] [PubMed]
- Mazy, D.; Chung-Tze-Cheong, C.; Ma, Z.; Huo, R.; Lamer, S.; Li, J.; Nault, M.L. Tough gel adhesive is an effective method for meniscal repair in a bovine cadaveric study. J. Exp. Orthop. 2023, 10, 139. [Google Scholar] [CrossRef]
- Aros, B.C.; Pedroza, A.; Vasileff, W.K.; Litsky, A.S.; Flanigan, D.C. Mechanical comparison of meniscal repair devices with mattress suture devices in vitro. Knee Surg Sports Traumatol. Arthrosc. 2010, 18, 1594–1598. [Google Scholar] [CrossRef]
- Chia, H.N.; Hull, M.L. Compressive moduli of the human medial meniscus in the axial and radial directions at equilibrium and at a physiological strain rate. J. Orthop. Res. 2008, 26, 951–956. [Google Scholar] [CrossRef]
- Long, T.; Shende, S.; Lin, C.Y.; Vemaganti, K. Experiments and hyperelastic modeling of porcine meniscus show heterogeneity at high strains. Biomech. Model Mechanobiol. 2022, 21, 1641–1658. [Google Scholar] [CrossRef]
- Morejon, A.; Norberg, C.D.; De Rosa, M.; Best, T.M.; Jackson, A.R.; Travascio, F. Compressive Properties and Hydraulic Permeability of Human Meniscus: Relationships With Tissue Structure and Composition. Front. Bioeng. Biotechnol. 2020, 8, 622552. [Google Scholar] [CrossRef]
- Kubota, R.; Koga, H.; Ozeki, N.; Matsuda, J.; Kohno, Y.; Mizuno, M.; Katano, H.; Sekiya, I. The effect of a centralization procedure for extruded lateral meniscus on load distribution in porcine knee joints at different flexion angles. BMC Musculoskelet. Disord. 2020, 21, 205. [Google Scholar] [CrossRef]
- Bao, X.; Li, W.; Lu, M.; Zhou, Z.R. Experiment study on puncture force between MIS suture needle and soft tissue. Biosurface Biotribol. 2016, 2, 49–58. [Google Scholar] [CrossRef]
- Zantop, T.; Temmig, K.; Weimann, A.; Eggers, A.K.; Raschke, M.J.; Petersen, W. Elongation and structural properties of meniscal repair using suture techniques in distraction and shear force scenarios: Biomechanical evaluation using a cyclic loading protocol. Am. J. Sports Med. 2006, 34, 799–805. [Google Scholar] [CrossRef]
- Zaffagnini, S.; Giordano, G.; Vascellari, A.; Bruni, D.; Neri, M.P.; Iacono, F.; Kon, E.; Presti, M.L.; Marcacci, M. Arthroscopic collagen meniscus implant results at 6 to 8 years follow up. Knee Surg Sports Traumatol. Arthrosc. 2007, 15, 175–183. [Google Scholar] [CrossRef]
- Herregodts, S.; Baets, P.D.; Victor, J.; Verstraete, M.A. Use of Tekscan pressure sensors for measuring contact pressures in the human knee joint. Int. J. Sustain. Constr. Des. 2015, 6, 7. [Google Scholar] [CrossRef]
- Sharma, L.; Chmiel, J.S.; Almagor, O.; Dunlop, D.; Guermazi, A.; Bathon, J.M.; Eaton, C.B.; Hochberg, M.C.; Jackson, R.D.; Kwoh, C.K.; et al. Significance of preradiographic magnetic resonance imaging lesions in persons at increased risk of knee osteoarthritis. Arthritis Rheumatol. 2014, 66, 1811–1819. [Google Scholar] [CrossRef] [PubMed]
- Willinger, L.; Foehr, P.; Achtnich, A.; Forkel, P.; Voss, A.; Liska, F.; Lacheta, L.; Imhoff, A.B.; Burgkart, R. Effect of Lower Limb Alignment in Medial Meniscus-Deficient Knees on Tibiofemoral Contact Pressure. Orthop. J. Sports Med. 2019, 7, 2325967118824611. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Lee, S.K.; Kim, S.H.; Jeong, J.H.; Kim, H.S.; Lee, S.W.; Lee, J.H.; Jung, M. Does decreased meniscal thickness affect surgical outcomes after medial meniscectomy? Am. J. Sports Med. 2015, 43, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Huey, D.J.; Athanasiou, K.A. Tension-compression loading with chemical stimulation results in additive increases to functional properties of anatomic meniscal constructs. PLoS ONE 2011, 6, e27857. [Google Scholar] [CrossRef] [PubMed]
- Loverde, J.R.; Piroli, M.; Klarmann, G.J.; Gaston, J.; Wickiser, J.K.; Barnhill, J.; Gilchrist, K.H.; Ho, V.B. Development of a bioreactor for in-vitro compression cycling of tissue engineered meniscal implants. HardwareX 2023, 14, e00433. [Google Scholar] [CrossRef] [PubMed]
- Petri, M.; Ufer, K.; Toma, I.; Becher, C.; Liodakis, E.; Brand, S.; Haas, P.; Liu, C.; Richter, B.; Haasper, C.; et al. Effects of perfusion and cyclic compression on in vitro tissue engineered meniscus implants. Knee Surg Sports Traumatol. Arthrosc. 2012, 20, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Puetzer, J.L.; Bonassar, L.J. Physiologically Distributed Loading Patterns Drive the Formation of Zonally Organized Collagen Structures in Tissue-Engineered Meniscus. Tissue Eng. Part A 2016, 22, 907–916. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Extrusion Pressure | Volume | [X] | [Y] | [Z] | R (avg) | |
|---|---|---|---|---|---|---|
| Meniscus #1 | 52 kPa | 2.17 mL | 40.55 mm | 21.64 mm | 8.13 mm | 10.56 mm |
| Meniscus #2 | 55 kPa | 2.26 mL | 40.26 mm | 21.69 mm | 8.64 mm | 10.38 mm |
| Meniscus #3 | 54 kPa | 2.23 mL | 40.28 mm | 21.81 mm | 8.56 mm | 10.45 mm |
| Meniscus #4 | 55 kPa | 2.31 mL | 40.71 mm | 21.74 mm | 8.70 mm | 10.53 mm |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nelson, A.; Voinier, S.; Tran, J.; Gilchrist, K.H.; Helgeson, M.; Ho, V.B.; Klarmann, G.J. Methods for Testing Meniscal Repair Using a 3D-Printed Meniscus. Appl. Biosci. 2024, 3, 102-122. https://doi.org/10.3390/applbiosci3010007
Nelson A, Voinier S, Tran J, Gilchrist KH, Helgeson M, Ho VB, Klarmann GJ. Methods for Testing Meniscal Repair Using a 3D-Printed Meniscus. Applied Biosciences. 2024; 3(1):102-122. https://doi.org/10.3390/applbiosci3010007
Chicago/Turabian StyleNelson, Andrew, Steven Voinier, Jeremy Tran, Kristin H. Gilchrist, Melvin Helgeson, Vincent B. Ho, and George J. Klarmann. 2024. "Methods for Testing Meniscal Repair Using a 3D-Printed Meniscus" Applied Biosciences 3, no. 1: 102-122. https://doi.org/10.3390/applbiosci3010007
APA StyleNelson, A., Voinier, S., Tran, J., Gilchrist, K. H., Helgeson, M., Ho, V. B., & Klarmann, G. J. (2024). Methods for Testing Meniscal Repair Using a 3D-Printed Meniscus. Applied Biosciences, 3(1), 102-122. https://doi.org/10.3390/applbiosci3010007