

The Effects of the Leg Position on the Nordic Hamstring Exercise Eccentric Force: A Randomized Cross-Over Study

 ,
,  ,
,
Abstract
1. Introduction
2. Material and Methods
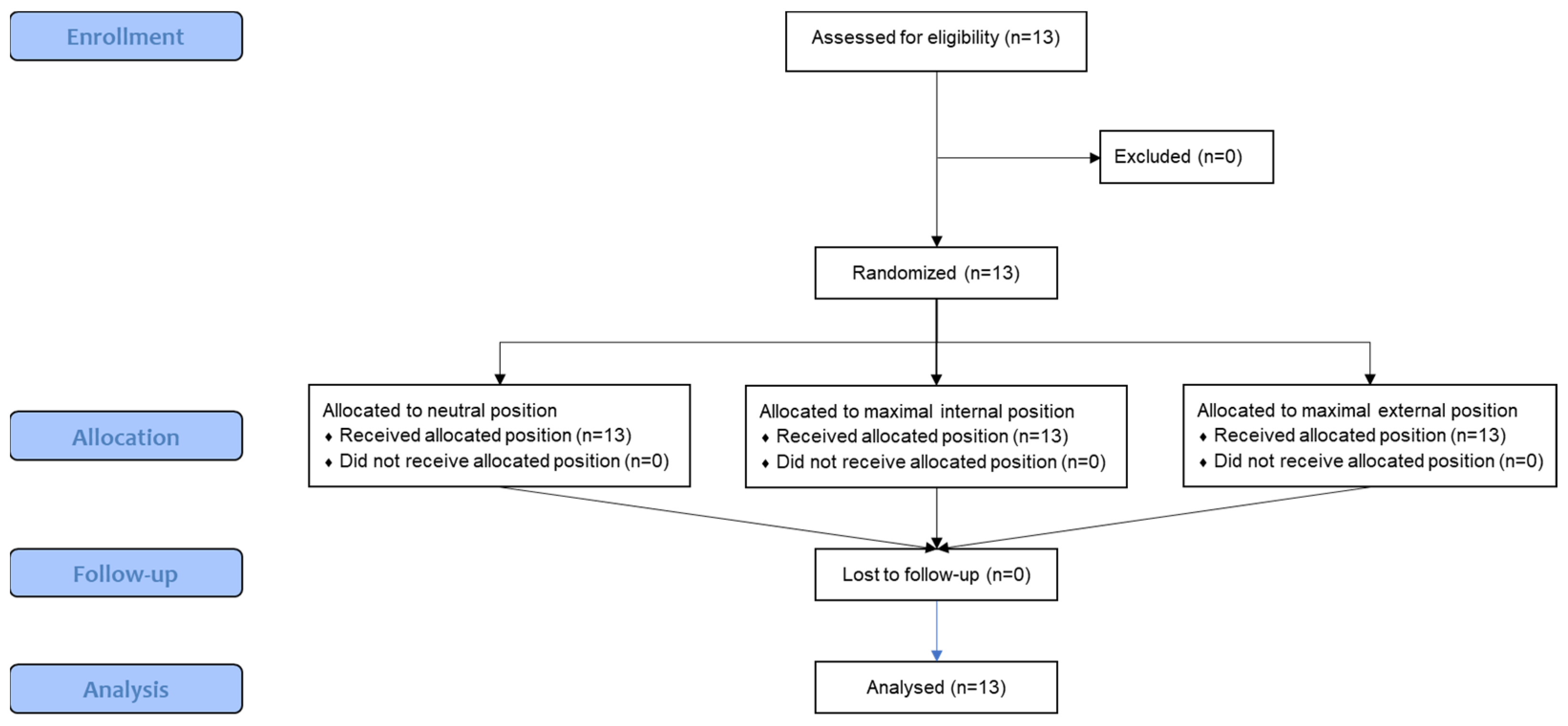
2.1. Sample
2.2. Study Design
2.3. Electromyography (EMG) Procedures
2.4. Nordic Exercises
2.5. Statistical Analysis
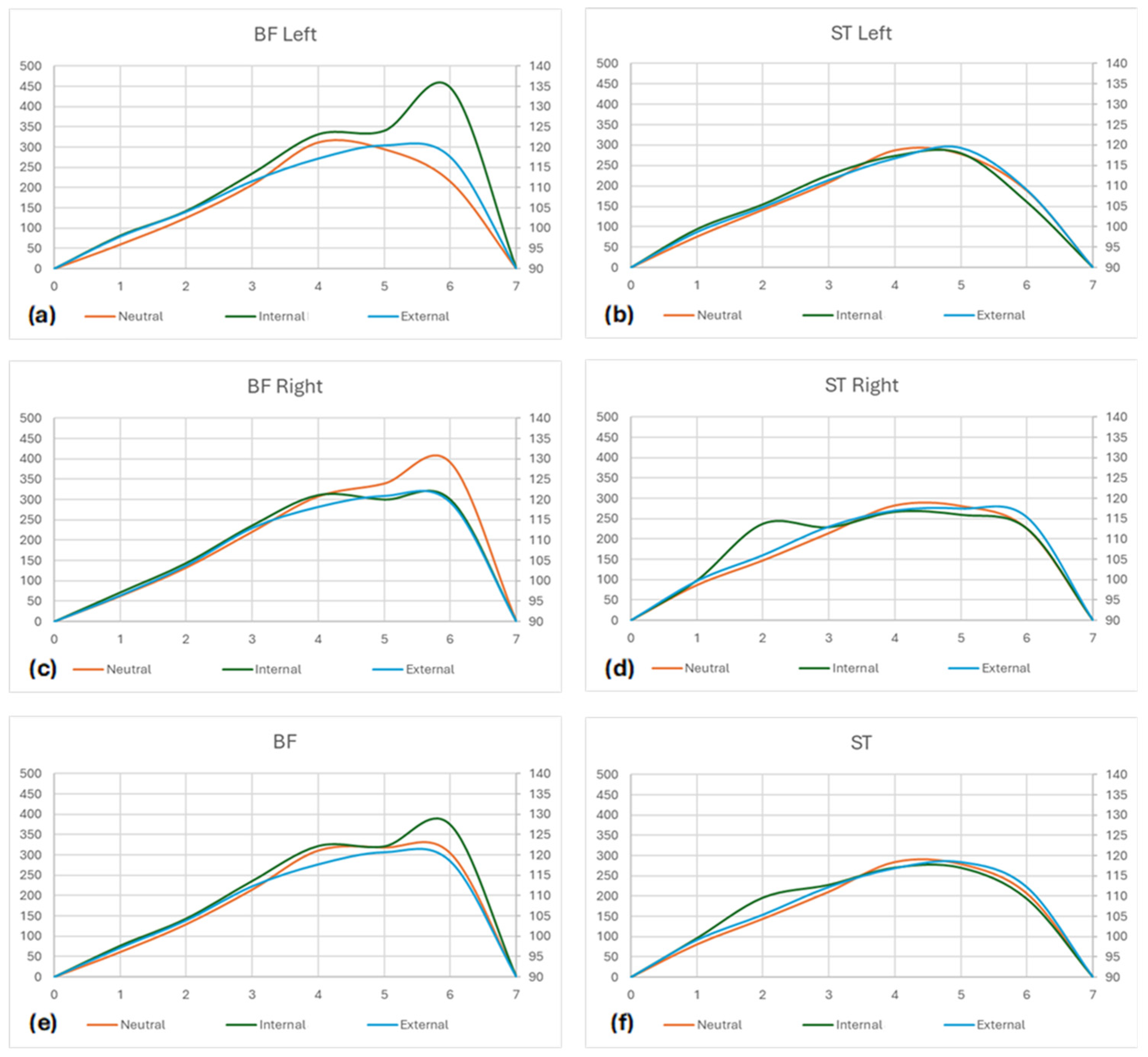
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Llurda-Almuzara, L.; Labata-Lezaun, N.; López-de-Celis, C.; Aiguadé-Aiguadé, R.; Romaní-Sánchez, S.; Rodríguez-Sanz, J.; Fernández-de-Las-Peñas, C.; Pérez-Bellmunt, A. Biceps femoris activation during hamstring strength exercises: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 8733. [Google Scholar] [CrossRef] [PubMed]
- Van Dyk, N.; Behan, F.P.; Whiteley, R. Including the Nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: A systematic review and meta-analysis of 8459 athletes. Br. J. Sports Med. 2019, 53, 1362–1370. [Google Scholar] [CrossRef]
- Green, B.; Bourne, M.N.; van Dyk, N.; Pizzari, T. Recalibrating the risk of hamstring strain injury (HSI): A 2020 systematic review and meta-analysis of risk factors for index and recurrent hamstring strain injury in sport. Br. J. Sports Med. 2020, 54, 1081–1088. [Google Scholar] [CrossRef]
- Freckleton, G.; Pizzari, T. Risk factors for hamstring muscle strain injury in sport: A systematic review and meta-analysis. Br. J. Sports Med. 2013, 47, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Claudino, J.G.; Cardoso Filho, C.A.; Bittencourt, N.F.N.; Gonçalves, L.G.; Couto, C.R.; Quintão, R.C.; Reis, G.F.; de Oliveira Júnior, O.; Amadio, A.C.; Boullosa, D. Eccentric strength assessment of hamstring muscles with new technologies: A systematic review of current methods and clinical implications. Sports Med.-Open 2021, 7, 10. [Google Scholar] [CrossRef] [PubMed]
- Bautista, I.J.; Vicente-Mampel, J.; Baraja-Vegas, L.; Segarra, V.; Martín, F.; Van Hooren, B. The effects of the Nordic hamstring exercise on sprint performance and eccentric knee flexor strength: A systematic review and meta-analysis of intervention studies among team sport players. J. Sci. Med. Sport 2021, 24, 931–938. [Google Scholar] [CrossRef]
- Medeiros, D.M.; Marchiori, C.; Baroni, B.M. Effect of nordic hamstring exercise training on knee flexors eccentric strength and fascicle length: A systematic review and meta-analysis. J. Sport Rehabil. 2020, 30, 482–491. [Google Scholar] [CrossRef] [PubMed]
- Cuthbert, M.; Ripley, N.; McMahon, J.J.; Evans, M.; Haff, G.G.; Comfort, P. The effect of Nordic hamstring exercise intervention volume on eccentric strength and muscle architecture adaptations: A systematic review and meta-analyses. Sports Med. 2020, 50, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Roig, M.; O’Brien, K.; Kirk, G.; Murray, R.; McKinnon, P.; Shadgan, B.; Reid, W. The effects of eccentric versus concentric resistance training on muscle strength and mass in healthy adults: A systematic review with meta-analysis. Br. J. Sports Med. 2009, 43, 556–568. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Ogborn, D.I.; Vigotsky, A.D.; Franchi, M.V.; Krieger, J.W. Hypertrophic effects of concentric vs. eccentric muscle actions: A systematic review and meta-analysis. J. Strength Cond. Res. 2017, 31, 2599–2608. [Google Scholar] [CrossRef]
- Ansari, M.; Hardcastle, S.; Myers, S.; Williams, A.D. The Health and Functional Benefits of Eccentric versus Concentric Exercise Training: A Systematic Review and Meta-Analysis. J. Sports Sci. Med. 2023, 22, 288. [Google Scholar] [CrossRef]
- Ebben, W.P. Hamstring activation during lower body resistance training exercises. Int. J. Sports Physiol. Perform. 2009, 4, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Brockett, C.L.; Morgan, D.L.; Proske, U. Human hamstring muscles adapt to eccentric exercise by changing optimum length. Med. Sci. Sports Exerc. 2001, 33, 783–790. [Google Scholar]
- Mjølsnes, R.; Arnason, A.; Østhagen, T.; Raastad, T.; Bahr, R. A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand. J. Med. Sci. Sports 2004, 14, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Al Attar, W.S.A.; Soomro, N.; Sinclair, P.J.; Pappas, E.; Sanders, R.H. Effect of injury prevention programs that include the Nordic hamstring exercise on hamstring injury rates in soccer players: A systematic review and meta-analysis. Sports Med. 2017, 47, 907–916. [Google Scholar]
- Biz, C.; Nicoletti, P.; Baldin, G.; Bragazzi, N.L.; Crimì, A.; Ruggieri, P. Hamstring strain injury (HSI) prevention in professional and semi-professional football teams: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 8272. [Google Scholar] [CrossRef]
- Hibbert, O.; Cheong, K.; Grant, A.; Beers, A.; Moizumi, T. A systematic review of the effectiveness of eccentric strength training in the prevention of hamstring muscle strains in otherwise healthy individuals. N. Am. J. Sports Phys. Ther. NAJSPT 2008, 3, 67. [Google Scholar] [PubMed]
- Fiebert, I.M.; Spielholz, N.I.; Applegate, E.B.; Fox, C.; Jaro, J.; Joel, L.; Raper, L. Comparison of EMG activity of medial and lateral hamstrings during isometric contractions at various cuff weight loads. Knee 2001, 8, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Vatovec, R.; Kozinc, Ž.; Šarabon, N. Exercise interventions to prevent hamstring injuries in athletes: A systematic review and meta-analysis. Eur. J. Sport Sci. 2020, 20, 992–1004. [Google Scholar] [CrossRef]
- Cleather, D.J. An important role of the biarticular hamstrings is to exert internal/external rotation moments on the tibia during vertical jumping. J. Theor. Biol. 2018, 455, 101–108. [Google Scholar] [CrossRef]
- Park, S.; Lim, W. Comparison of muscle activity of hamstrings as knee flexors and hip extensors and effect of tibial and hip rotation on the contribution of hamstrings. J. Bodyw. Mov. Ther. 2023, 34, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Beuchat, A.; Maffiuletti, N.A. Foot rotation influences the activity of medial and lateral hamstrings during conventional rehabilitation exercises in patients following anterior cruciate ligament reconstruction. Phys. Ther. Sport 2019, 39, 69–75. [Google Scholar] [CrossRef]
- Mohamed, O.; Perry, J.; Hislop, H. Synergy of medial and lateral hamstrings at three positions of tibial rotation during maximum isometric knee flexion. Knee 2003, 10, 277–281. [Google Scholar]
- Beyer, E.B.; Lunden, J.B.; Giveans, M.R. Medial and lateral hamstrings response and force production at varying degrees of knee flexion and tibial rotation in healthy individuals. Int. J. Sports Phys. Ther. 2019, 14, 376. [Google Scholar] [CrossRef]
- Fiebert, I.M.; Roach, K.E.; Fingerhut, B.; Levy, J.; Schumacher, A. EMG activity of medial and lateral hamstrings at three positions of tibial rotation during low-force isometric knee flexion contractions. J. Back Musculoskelet. Rehabil. 1997, 8, 215–222. [Google Scholar] [CrossRef]
- Lynn, S.K.; Costigan, P.A. Changes in the medial–lateral hamstring activation ratio with foot rotation during lower limb exercise. J. Electromyogr. Kinesiol. 2009, 19, e197–e205. [Google Scholar] [CrossRef]
- Jónasson, G.; Helgason, A.; Ingvarsson, Þ.; Kristjánsson, A.M.; Briem, K. The effect of tibial rotation on the contribution of medial and lateral hamstrings during isometric knee flexion. Sports Health 2016, 8, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Lim, W. Appropriateness of tibial rotation for isolation of the medial and lateral hamstrings. Ann. Appl. Sport Sci. 2020, 8, e907. [Google Scholar] [CrossRef]
- Šarabon, N.; Marušič, J.; Marković, G.; Kozinc, Ž. Kinematic and electromyographic analysis of variations in Nordic hamstring exercise. PLoS ONE 2019, 14, e0223437. [Google Scholar] [CrossRef] [PubMed]
- Hegyi, A.; Lahti, J.; Giacomo, J.-P.; Gerus, P.; Cronin, N.J.; Morin, J.-B. Impact of hip flexion angle on unilateral and bilateral nordic hamstring exercise torque and high-density electromyography activity. J. Orthop. Sports Phys. Ther. 2019, 49, 584–592. [Google Scholar] [CrossRef]
- Keerasomboon, T.; Soga, T.; Hirose, N. Influence of altered knee angle on electromyographic activity of hamstring muscles between Nordic Hamstring Exercise and Nordic Hamstring Exercise with incline slope lower leg board. Int. J. Sports Phys. Ther. 2022, 17, 832. [Google Scholar] [PubMed]
- Soga, T.; Nishiumi, D.; Furusho, A.; Akiyama, K.; Hirose, N. Effect of different slopes of the lower leg during the Nordic Hamstring Exercise on hamstring electromyography activity. J. Sports Sci. Med. 2021, 20, 216. [Google Scholar] [CrossRef] [PubMed]
- Nishida, S.; Ito, W.; Ohishi, T.; Yoshida, R.; Sato, S.; Nakamura, M. The effect of ankle position on peak eccentric force during the Nordic hamstring exercise. J. Sports Sci. Med. 2022, 21, 43. [Google Scholar] [CrossRef] [PubMed]
- Vicente-Mampel, J.; Bautista, I.J.; Martín, F.; Maroto-Izquierdo, S.; Van Hooren, B.; Baraja-Vegas, L. Effects of ankle position during the Nordic Hamstring exercise on range of motion, heel contact force and hamstring muscle activation. Sports Biomech. 2022, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Alt, T.; Schmidt, M. The ANHEQ evaluation criteria: Introducing reliable rating scales for assessing Nordic hamstring exercise quality. Sports Med.-Open 2021, 7, 91. [Google Scholar] [CrossRef] [PubMed]
- Alt, T.; Severin, J.; Schmidt, M. Quo Vadis Nordic Hamstring Exercise-Related Research?—A Scoping Review Revealing the Need for Improved Methodology and Reporting. Int. J. Environ. Res. Public Health 2022, 19, 11225. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.A. The consolidated standards of reporting trials (CONSORT): Guidelines for reporting randomized trials. Nurs. Res. 2005, 54, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. European recommendations for surface electromyography. Roessingh Res. Dev. 1999, 8, 13–54. [Google Scholar]
- Drost, G.; Stegeman, D.F.; van Engelen, B.G.; Zwarts, M.J. Clinical applications of high-density surface EMG: A systematic review. J. Electromyogr. Kinesiol. 2006, 16, 586–602. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Lim, W. Effects of hip rotation on the electromyographic activity of the medial and lateral hamstrings and muscle force. J. Back Musculoskelet. Rehabil. 2021, 34, 1023–1029. [Google Scholar] [CrossRef]
- Charlton, J.M.; Hatfield, G.L.; Guenette, J.A.; Hunt, M.A. Toe-in and toe-out walking require different lower limb neuromuscular patterns in people with knee osteoarthritis. J. Biomech. 2018, 76, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Behan, F.P.; Moody, R.; Patel, T.S.; Lattimore, E.; Maden-Wilkinson, T.M.; Balshaw, T.G. Biceps femoris long head muscle fascicle length does not differ between sexes. J. Sports Sci. 2019, 37, 2452–2458. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Age (Years) | Weight (kg) | Height (m) | BMI (kg/m2) | RPE (0–10) | Volleyball Years | Dominate Side | Volleyball Position |
|---|---|---|---|---|---|---|---|---|
| 1 | 18 | 75.1 | 1.86 | 21.7 | 2 | 10 | Right | Outside Hitter |
| 2 | 16 | 62.8 | 1.71 | 21.5 | 4 | 4 | Right | Libero |
| 3 | 17 | 73.2 | 1.85 | 21.4 | 3 | 9 | Right | Opposite Hitter |
| 4 | 18 | 69.6 | 1.82 | 21.0 | 2 | 7 | Right | Setter |
| 5 | 17 | 74.8 | 1.85 | 21.9 | 4 | 7 | Left | Middle Blocker |
| 6 | 18 | 57.9 | 1.76 | 18.7 | 1 | 14 | Right | Outside Hitter |
| 7 | 17 | 68.9 | 1.86 | 19.9 | 4 | 2 | Right | Middle Blocker |
| 8 | 17 | 57.8 | 1.68 | 20.5 | 2 | 9 | Right | Libero |
| 9 | 17 | 57.4 | 1.76 | 18.5 | 4 | 6 | Left | Setter |
| 10 | 17 | 68.3 | 1.70 | 23.6 | 3 | 5 | Right | Middle Blocker |
| 11 | 17 | 78.2 | 1.84 | 23.1 | 1 | 6 | Right | Opposite Hitter |
| 12 | 18 | 73.7 | 1.76 | 23.8 | 2 | 9 | Right | Setter |
| 13 | 18 | 72.5 | 1.81 | 22.1 | 4 | 7 | Right | Setter |
| Mean ± SD; n (%) | 17.3 ± 0.6 | 68.5 ± 7.2 | 1.79 ± 0.06 | 21.4 ± 1.7 | 2.8 ± 1.2 | 7.3 ± 3 | Right—11 (84.6%) Left—2 (15.4%) | Setter—4 (30.8%) Opposite Hitter—2 (15.4%) Outside Hitter—2 (15.4%) Middle Blocker—3 (23.1%) Libero—2 (15.4%) |
| Positions | Statistics | Effect Size | |||
|---|---|---|---|---|---|
| Neutral | Internal | External | p | η2 | |
| BF Left | 201.98 ± 64.69 | 227.84 ± 78.09 | 204.02 ± 63.10 | 0.57 | 0.03 |
| ST Left | 199.37 ± 71.59 | 203.38 ± 71.92 | 202.35 ± 79.85 | 0.99 | 0.00 |
| p | 0.82 | 0.32 | 0.88 | ||
| d | 0.07 | 0.84 | 0.04 | ||
| BF Right | 219.14 ± 57.49 | 212.16 ± 61.25 | 206.61 ± 67.57 | 0.88 | 0.01 |
| ST Right | 204.19 ± 59.26 | 217.45 ± 100.74 | 207.69 ± 68.03 | 0.90 | 0.01 |
| p | 0.41 | 0.85 | 0.95 | ||
| d | 0.24 | 0.49 | 0.02 | ||
| BF (Left + Right) | 210.56 ± 53.62 | 220.00 ± 62.89 | 205.31 ± 63.11 | 0.82 | 0.01 |
| ST (Left + Right) | 201.78 ± 63.11 | 210.41 ± 83.08 | 205.02 ± 69.77 | 0.95 | 0.00 |
| p | 0.74 | 0.68 | 0.98 | ||
| d | 0.20 | 0.66 | 0.01 | ||
| Left (BF + ST) | 200.68 ± 65.20 | 215.61 ± 62.00 | 203.18 ± 69.17 | 0.83 | 0.01 |
| Right (BF + ST) | 211.67 ± 49.29 | 214.81 ± 67.15 | 207.15 ± 61.16 | 0.95 | 0.00 |
| p | 0.33 | 0.94 | 0.67 | ||
| d | 0.28 | 0.56 | 0.12 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, R.M.; Martins, P.N.; Nunes, H.; Fernandes, L.G.; Amorim, C.F.; Ferreira, L.M.A. The Effects of the Leg Position on the Nordic Hamstring Exercise Eccentric Force: A Randomized Cross-Over Study. Muscles 2024, 3, 259-270. https://doi.org/10.3390/muscles3030023
Ferreira RM, Martins PN, Nunes H, Fernandes LG, Amorim CF, Ferreira LMA. The Effects of the Leg Position on the Nordic Hamstring Exercise Eccentric Force: A Randomized Cross-Over Study. Muscles. 2024; 3(3):259-270. https://doi.org/10.3390/muscles3030023
Chicago/Turabian StyleFerreira, Ricardo Maia, Pedro Nunes Martins, Hugo Nunes, Luís Gonçalves Fernandes, César Ferreira Amorim, and Luciano Maia Alves Ferreira. 2024. "The Effects of the Leg Position on the Nordic Hamstring Exercise Eccentric Force: A Randomized Cross-Over Study" Muscles 3, no. 3: 259-270. https://doi.org/10.3390/muscles3030023
APA StyleFerreira, R. M., Martins, P. N., Nunes, H., Fernandes, L. G., Amorim, C. F., & Ferreira, L. M. A. (2024). The Effects of the Leg Position on the Nordic Hamstring Exercise Eccentric Force: A Randomized Cross-Over Study. Muscles, 3(3), 259-270. https://doi.org/10.3390/muscles3030023