
Orofacial Myofunctional Therapy for Patients with Obstructive Sleep Apnea—A Mixed Methods Study of Facilitators and Barriers to Treatment Adherence

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Participants
2.3. Intervention
2.4. Materials and Measurements
2.5. Data Analysis
3. Results
3.1. Motivation Facilitators
3.1.1. Control of Personal Health
“Give me something I can work on by myself. I’ll do anything… as long as I can influence it.”(P5)
“I don’t mind snoring; that doesn’t bother me. But those breathing pauses—I definitely don’t want those.”(P6)
3.1.2. Quality of Life
“This has done something with the nights. It has done something with my relationship… It has actually been very damaging.”(P1)
3.1.3. CPAP Avoidance
“I didn’t try it any nights because I didn’t dare to lie down… I basically panicked just from thinking about having the mask on while lying down.”(P1)
3.1.4. General Belief in the Positive Effect of Exercise
“I exercise my body, I go for walks, and I do mouth exercises, because these three things are so important for me.”(P5)
3.1.5. Ability to Establish OMT Routines
3.2. Motivation Barriers
3.2.1. Sickness Burden
“I had intense headache. I couldn’t handle light. I couldn’t handle sound… I was just in pain, nothing worked, and nothing helped.”(P1)
3.2.2. Comprehensive and Fixed Protocol
“What I found most challenging was actually doing the exercises… Just getting them done three times a day, that has been very difficult for me.”(P2)
“It was mentally exhausting… it was tiresome to do, but also constantly feeling like: Now I have to do exercises, now I have to do exercises.”(P7)
3.2.3. Exercise Performance Difficulties
“I couldn’t do that [lifting soft palate exercise… That was the heaviest and most difficult one.”(P7)
“During the first week the exercises were difficult… it was frustrating… I had to focus immensely to perform the exercises.”(P5)
3.2.4. Uncertainty About OMT Effectiveness
3.3. Perceived Support Facilitators
3.3.1. Therapist Support
“I feel like I can talk about all sorts of things. Also in a professional sense, you [the therapist] can answer so many questions about sleep apnea… I’ve really appreciated that.”(P2)
“It turns into a conversation… it’s been really nice. And maybe that’s also made me more committed, you know, because you feel like you have a relationship.”(P5)
“When I’m part of a project like this, I’d really like to see an effect, you know… and it’s partly out of respect for you.”(P4)
3.3.2. Social Support
“He’s been involved, but not actively. This has to come from within myself… for my own benefit.”(P6)
“I kind of wish there was a group where we could share experiences… When you’re in a group, you motivate each other… I think that would have been really, really useful.”(P10)
3.3.3. Commitment to the Research Project
“I want to stick with the exercises because I’m involved in this study, and I want to see it through.”(P5)
3.4. Perceived Support Barriers
3.4.1. Previous Negative Healthcare Experience
“I’ve totally stopped going to the doctor… I don’t share anything because I don’t trust the system anymore.”(P5)
“There’s a lot of variation in general practitioners … I don’t have very good experience [laughs]. I go there as rarely as I can, and when I leave, I regret that I went… A GP… is supposed to be a bit of an expert on everything, but at the same time maybe nothing [laughs]. I have much more trust in someone who has spent time specifically on one subject.”(P2)
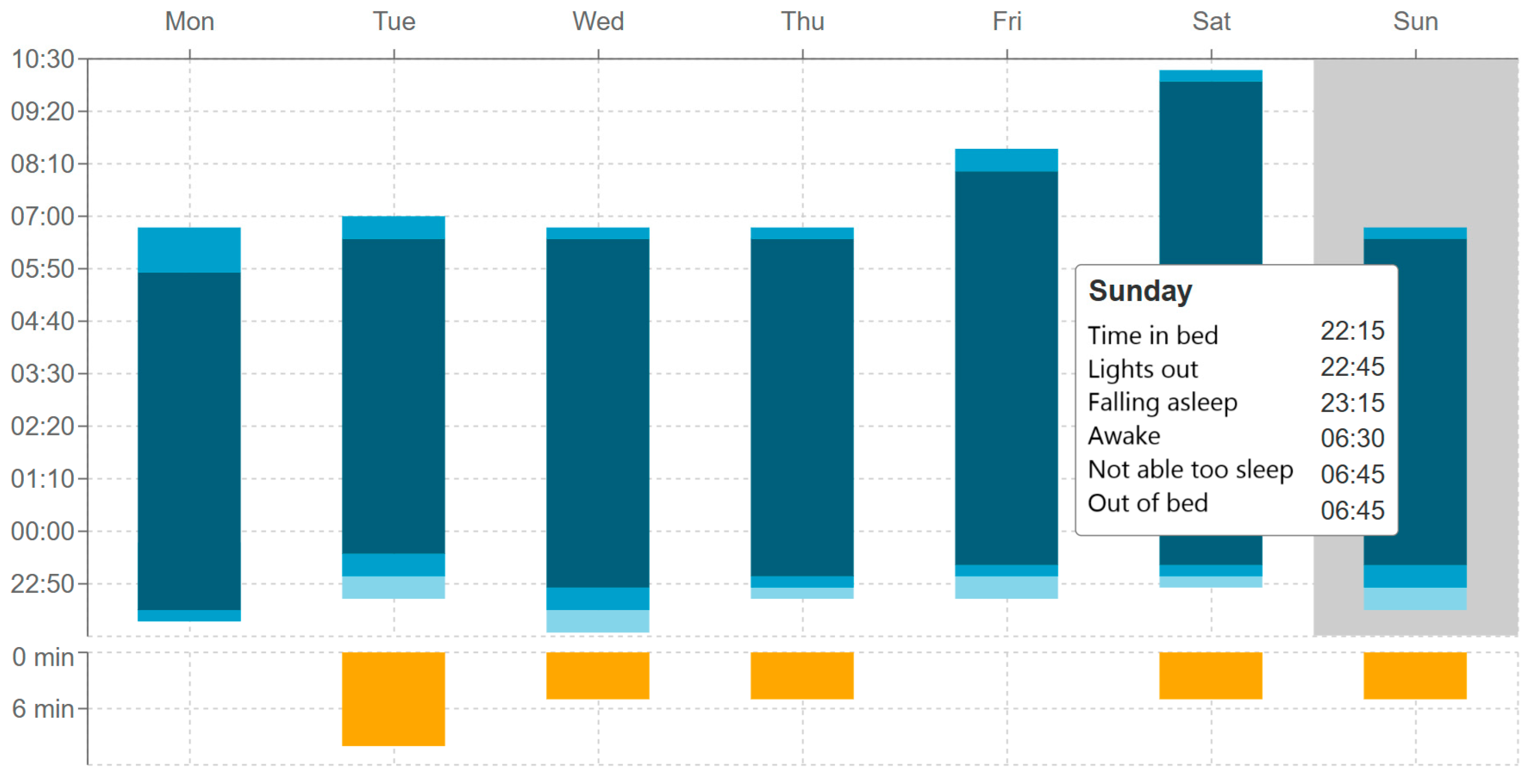
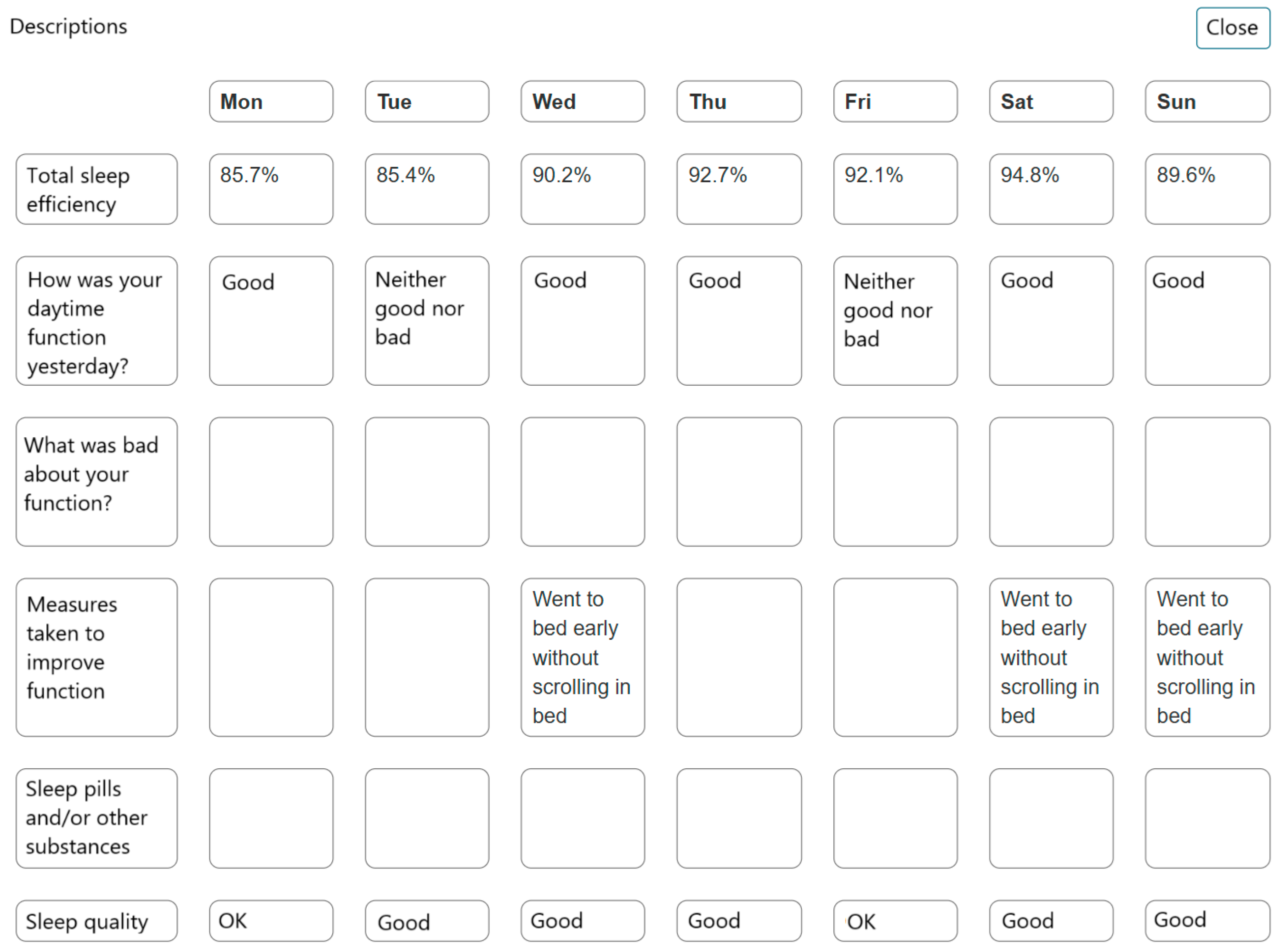
3.4.2. Perceived Burden of the Sleep Diary
“It became very tiring to have to register everything… I hardly had time to sleep when I had to register all the times I was awake… it became very stressful.”(P1)
3.4.3. Lack of Clear Instructions
“I couldn’t quite get the video and the descriptions to add up.”(P2)
3.5. Perceived Effect Facilitators
3.5.1. Subjective Sleep Quality Improvement
“Now I sleep through the night without waking up, and I don’t need to take Oxazepam. I have nights where I don’t use melatonin either, but rather drink milk with honey in it. I also don’t need to sleep in the middle of the day anymore… but I don’t know… it could be related to my sick leave.”(P8)
3.5.2. Improvements in Daytime Functioning
3.5.3. Increased Muscle Control
“I have much better control over my tongue, and I control my muscles much better. And I feel the muscles better… I also think that they are much stronger now.”(P9)
“My motivation got better when the facial palsy [long time diagnosis] disappeared.”(P8)
3.5.4. Technology Reporting Sleep Improvement
“It’s clear that I have had an improvement in the end of this [project] and that is a motivation… I actually haven’t had such low numbers [data from CPAP] since I got that machine.”(P5)
3.6. Perceived Effect Barriers
3.6.1. Subjective Lack of Improvements
“I’m sleeping well. How much this program has contributed to this change, I don’t really know. So, if it stays like this, I’ll be very happy, but from what I know about my illness, I think it will probably fluctuate.”(P5)
3.6.2. Negative Side Effects
“[When asked about negative side effects] No, no not at all [laughing].”(P4)
3.6.3. Exercises Perceived as Not Effective
“Blowing up a balloon was so easy that I felt it had no effect, or why am I doing this? So that it got a bit forgotten… and that tongue exercise was also so easy to perform that I didn’t feel it had any effect either.”(P7)
3.7. Distribution of Participants Across Identified Subthemes
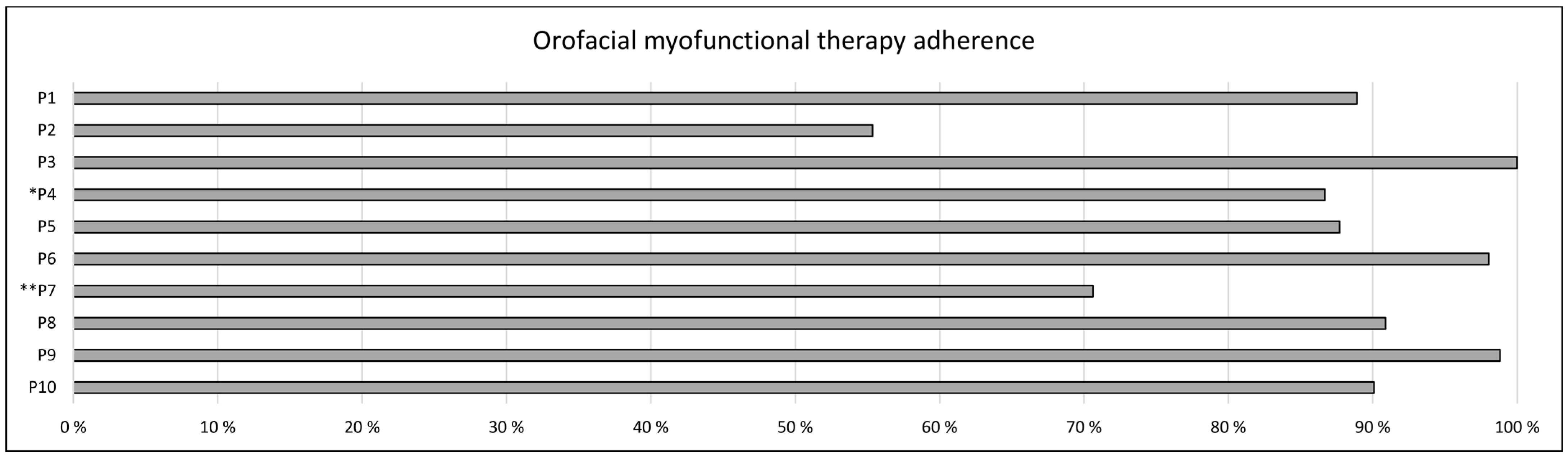
3.8. Exercise Adherence
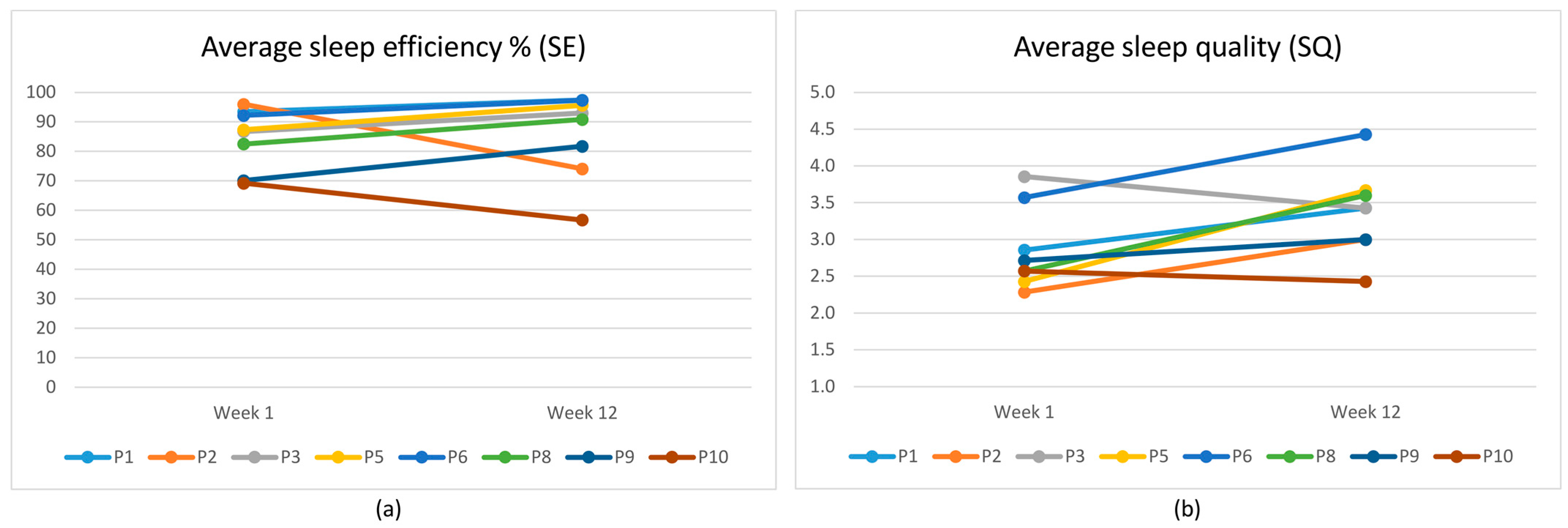
3.9. Sleep Efficiency and Sleep Quality
4. Discussion
4.1. Motivation
4.2. Perceived Support and Trust
4.3. Perceived Effect
4.4. Instructions and Follow-Up
4.5. Clinical Implications
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| OSA | Obstructive sleep apnea |
| CPAP | Continuous positive airway pressure |
| MAD | Mandibular advancement devices |
| OMT | Orofacial myofunctional therapy |
| SDB | Sleep-disordered breathing |
| AOMT | Academy of Orofacial Myofunctional Therapy |
| P1–P10 | Patients 1 to 10 |
| SDT | Self-Determination Theory |
| BCW | Behavior Change Wheel |
| SDM | Shared decision-making |
| RCT | Randomized controlled trial |
Appendix A
A.1. Interview Guide
- Background
- Gender
- Age
- Family
- Occupation
- Marital status
- How did you first hear about this project?
- How did you experience receiving the sleep apnea diagnosis?
- What was it like to start CPAP treatment?
- Are you aware of any health risks related to sleep apnea? Could you elaborate?
- Has this information affected your motivation to participate in this project?
- Tell us a bit about your sleep three months ago.
- What did you do on your own to improve your sleep before the project started?
- To what extent did your sleep problems affect your daily functioning?
- Have you thought about your breathing patterns?
- Tell us a bit about your sleep now.
- Has the OMT treatment contributed to any changes in your sleep?
- In what way has the OMT treatment improved or worsened your sleep?
- If you have noticed any changes in daily functioning, could you elaborate?
- Have you thought about your current breathing patterns?
- Tell us about the exercise routines.
- What was difficult, and what was easy?
- Did you complete all the exercises every time?
- What motivated you the most to keep performing the exercises?
- How has your motivation changed during the training period?
- What are your thoughts on continuing the exercises after the project?
- Tell us about your experiences with the sleep diary and tracking the exercises.
- Has the sleep and exercise diary contributed to changes in your sleep?
- What was most useful?
- What were the disadvantages?
- How often did you fill out the sleep diary and record your exercises?
- How much time did it take to log the information?
- Is there anything you feel is missing in the sleep diary?
- Did you keep track of your sleep before the project?
- [Only if the participant has a partner] Describe your partner’s role in the treatment over these 12 weeks.
- Can you describe if and how your partner supported you during this project?
- Could your partner have supported or motivated you more?
- Would you have liked your partner to have received information about the OMT treatment from us before the project began?
- If yes, how would you have preferred this information to be shared?
- Tell us about your encounters with healthcare personnel.
- How did you experience the first meeting with the OMT therapist?
- Can you think of anything that was missing or should have been explained during that meeting?
- How did you experience the video consultations with the OMT therapist?
- What were the pros and cons of those meetings?
- How would you describe your collaboration with the OMT therapist regarding the treatment? Is there anything that could have been different?
- Do you have any thoughts on how sleep guidance could have been provided before, during, or after the project?
- Have you used any other sources of information about OSA and sleep during the project?
- Let us shift slightly and ask a few questions about general health: Who or what do you trust most when it comes to health information?
- Why?
- Back to the project: How has it been to participate in the project?
- Is there anything important you would like to add that we have not asked about?
Appendix B
B.1. Sleep Diary

References
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pepin, J.L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef]
- Monahan, K.; Redline, S. Role of obstructive sleep apnea in cardiovascular disease. Curr. Opin. Cardiol. 2011, 26, 541–547. [Google Scholar] [CrossRef]
- Spicuzza, L.; Caruso, D.; Di Maria, G. Obstructive sleep apnoea syndrome and its management. Ther. Adv. Chronic Dis. 2015, 6, 273–285. [Google Scholar] [CrossRef]
- Weaver, T.E.; Grunstein, R.R. Adherence to continuous positive airway pressure therapy: The challenge to effective treatment. Proc. Am. Thorac. Soc. 2008, 5, 173–178. [Google Scholar] [CrossRef]
- Truby, H.; Edwards, B.A.; Day, K.; O’Driscoll, D.M.; Young, A.; Ghazi, L.; Bristow, C.; Roem, K.; Bonham, M.P.; Murgia, C.; et al. A 12-month weight loss intervention in adults with obstructive sleep apnoea: Is timing important? A step wedge randomised trial. Eur. J. Clin. Nutr. 2022, 76, 1762–1769. [Google Scholar] [CrossRef]
- Koka, V.; De Vito, A.; Roisman, G.; Petitjean, M.; Filograna Pignatelli, G.R.; Padovani, D.; Randerath, W. Orofacial Myofunctional Therapy in Obstructive Sleep Apnea Syndrome: A Pathophysiological Perspective. Medicina 2021, 57, 323. [Google Scholar] [CrossRef]
- Guilleminault, C.; Huang, Y.S.; Monteyrol, P.J.; Sato, R.; Quo, S.; Lin, C.H. Critical role of myofascial reeducation in pediatric sleep-disordered breathing. Sleep Med. 2013, 14, 518–525. [Google Scholar] [CrossRef]
- Camacho, M.; Certal, V.; Abdullatif, J.; Zaghi, S.; Ruoff, C.M.; Capasso, R.; Kushida, C.A. Myofunctional Therapy to Treat Obstructive Sleep Apnea: A Systematic Review and Meta-analysis. Sleep 2015, 38, 669–675. [Google Scholar] [CrossRef]
- Saba, E.S.; Kim, H.; Huynh, P.; Jiang, N. Orofacial Myofunctional Therapy for Obstructive Sleep Apnea: A Systematic Review and Meta-Analysis. Laryngoscope 2024, 134, 480–495. [Google Scholar] [CrossRef]
- Rueda, J.R.; Mugueta-Aguinaga, I.; Vilaro, J.; Rueda-Etxebarria, M. Myofunctional therapy (oropharyngeal exercises) for obstructive sleep apnoea. Cochrane Database Syst. Rev. 2020, 11, CD013449. [Google Scholar] [CrossRef]
- de Felicio, C.M.; de Oliveira, M.M.; da Silva, M.A. Effects of orofacial myofunctional therapy on temporomandibular disorders. Cranio 2010, 28, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes, K.C.; Drager, L.F.; Genta, P.R.; Marcondes, B.F.; Lorenzi-Filho, G. Effects of oropharyngeal exercises on patients with moderate obstructive sleep apnea syndrome. Am. J. Respir. Crit. Care Med. 2009, 179, 962–966. [Google Scholar] [CrossRef]
- Cakmakci, S.; Ozgen Alpaydin, A.; Ozalevli, S.; Oztura, I.; Itil, B.O. The effect of oropharyngeal exercise in patients with moderate and severe obstructive sleep apnea using CPAP: A randomized controlled study. Sleep Breath. 2022, 26, 567–574. [Google Scholar] [CrossRef]
- Arnardottir, E.S.; Islind, A.S.; Oskarsdottir, M.; Olafsdottir, K.A.; August, E.; Jonasdottir, L.; Hrubos-Strom, H.; Saavedra, J.M.; Grote, L.; Hedner, J.; et al. The Sleep Revolution project: The concept and objectives. J. Sleep Res. 2022, 31, e13630. [Google Scholar] [CrossRef]
- Brinkmann, S.; Kvale, S. InterViews: Learning the Craft of Qualitative Research Interviewing, 3rd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Berry, R.B.; Brooks, R.; Gamaldo, C.E.; Harding, S.M.; Lloyd, R.M.; Quan, S.F.; Troester, M.M.; Vaughn, B.V. American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, Version 2.6; American Academy of Sleep Medicine: Darien, IL, USA, 2020. [Google Scholar]
- Sateia, M.J. (Ed.) International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Carney, C.E.; Buysse, D.J.; Ancoli-Israel, S.; Edinger, J.D.; Krystal, A.D.; Lichstein, K.L.; Morin, C.M. The consensus sleep diary: Standardizing prospective sleep self-monitoring. Sleep 2012, 35, 287–302. [Google Scholar] [CrossRef]
- Orofacial Myofunctional Therapy. Available online: https://www.youtube.com/playlist?list=PLiwLLUadscDGs2dSzcXI6CEc-FItoXlPT (accessed on 18 June 2025).
- Reed, D.L.; Sacco, W.P. Measuring Sleep Efficiency: What Should the Denominator Be? J. Clin. Sleep. Med. 2016, 12, 263–266. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Teixeira, P.J.; Carraca, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef]
- Dyrlund, A.K.; Wininger, S.R. An Evaluation of Barrier Efficacy and Cognitive Evaluation Theory as Predictors of Exercise Attendance. J. Appl. Biobehav. Res. 2007, 11, 133–146. [Google Scholar] [CrossRef]
- Grimen, H. Power, trust, and risk: Some reflections on an absent issue. Med. Anthropol. Q. 2009, 23, 16–33. [Google Scholar] [CrossRef] [PubMed]
- Mayer, R.C.; Davis, J.H.; Schoorman, F.D. An Integrative Model of Organizational Trust. Acad. Manag. Rev. 1995, 20, 709–734. [Google Scholar] [CrossRef]
- Skirbekk, H.; Middelthon, A.L.; Hjortdahl, P.; Finset, A. Mandates of trust in the doctor-patient relationship. Qual. Health Res. 2011, 21, 1182–1190. [Google Scholar] [CrossRef]
- Hadden, B.W.; Rodriguez, L.M.; Knee, C.R.; Porter, B. Relationship autonomy and support provision in romantic relationships. Motiv. Emot. 2014, 39, 359–373. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Intrinsic and Extrinsic Motivations: Classic Definitions and New Directions. Contemp. Educ. Psychol. 2000, 25, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Thorshov, T.C.; Overby, C.T.; Hansen, D.D.; Bong, W.K.; Skifjeld, K.; Hurlen, P.; Dammen, T.; Moen, A.; Hrubos-Strom, H. Experience with the use of a digital sleep diary in symptom management by individuals with insomnia -a pilot mixed method study. Sleep. Med. X 2023, 6, 100093. [Google Scholar] [CrossRef]
- Kim, K.; Kim, S.J. Orthodontics in Obstructive Sleep Apnea Patients; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Niemeijer, A.; Lund, H.; Stafne, S.N.; Ipsen, T.; Goldschmidt, C.L.; Jorgensen, C.T.; Juhl, C.B. Adverse events of exercise therapy in randomised controlled trials: A systematic review and meta-analysis. Br. J. Sports Med. 2020, 54, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Giroldi, E.; Veldhuijzen, W.; Mannaerts, A.; van der Weijden, T.; Bareman, F.; van der Vleuten, C. “Doctor, please tell me it’s nothing serious”: An exploration of patients’ worrying and reassuring cognitions using stimulated recall interviews. BMC Fam. Pract. 2014, 15, 73. [Google Scholar] [CrossRef]
- Bryant, M.J.; Simons, A.D.; Thase, M.E. Therapist Skill and Patient Variables in Homework Compliance: Controlling an Uncontrolled Variable in Cognitive Therapy Outcome Research. Cogn. Ther. Res. 1999, 23, 381–399. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- Khan, N.N.S.; Todem, D.; Bottu, S.; Badr, M.S.; Olomu, A. Impact of patient and family engagement in improving continuous positive airway pressure adherence in patients with obstructive sleep apnea: A randomized controlled trial. J. Clin. Sleep Med. 2022, 18, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Pattipati, M.; Gudavalli, G.; Zin, M.; Dhulipalla, L.; Kolack, E.; Karki, M.; Devarakonda, P.K.; Yoe, L. Continuous Positive Airway Pressure vs Mandibular Advancement Devices in the Treatment of Obstructive Sleep Apnea: An Updated Systematic Review and Meta-Analysis. Cureus 2022, 14, e21759. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.; Bakhit, M.; Michaleff, Z. Shared decision making and physical therapy: What, when, how, and why? Braz. J. Phys. Ther. 2022, 26, 100382. [Google Scholar] [CrossRef]
- Krysta, K.; Bratek, A.; Zawada, K.; Stepanczak, R. Cognitive deficits in adults with obstructive sleep apnea compared to children and adolescents. J. Neural Transm. 2017, 124, 187–201. [Google Scholar] [CrossRef] [PubMed]
- Lal, C.; Weaver, T.E.; Bae, C.J.; Strohl, K.P. Excessive Daytime Sleepiness in Obstructive Sleep Apnea. Mechanisms and Clinical Management. Ann. Am. Thorac. Soc. 2021, 18, 757–768. [Google Scholar] [CrossRef]
- Woodbridge, H.R.; Norton, C.; Jones, M.; Brett, S.J.; Alexander, C.M.; Gordon, A.C. Clinician and patient perspectives on the barriers and facilitators to physical rehabilitation in intensive care: A qualitative interview study. BMJ Open 2023, 13, e073061. [Google Scholar] [CrossRef]
- DiMatteo, M.R.; Haskard, K.B.; Williams, S.L. Health beliefs, disease severity, and patient adherence: A meta-analysis. Med. Care 2007, 45, 521–528. [Google Scholar] [CrossRef]
- Silverman, D. Interpreting Qualitative Data; Sage publications: London, UK, 2024; 496p. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Research ID | Age | Employment Fraction (%) | Treatment | BMI | AHI | Duration of Sleep Difficulties (Years) |
|---|---|---|---|---|---|---|
| P1 | 61–65 | 100 | CPAP non-adherent | 27.4 | 13.9 | 1.7 |
| P2 | 56–60 | 100 | CPAP | 23.7 | 32.6 | 17.5 |
| P3 | 56–60 | <50 | CPAP | 19.3 | 29.2 | 12.5 |
| P4 | 61–65 | 100 | CPAP, MAD | 23.8 | 46.3 | 6.0 |
| P5 | 51–55 | <50 | CPAP | 29.8 | 55.1 | 15.0 |
| P6 | 56–60 | 100 | CPAP non-adherent, MAD | 24.4 | 9.0 | 30.0 |
| P7 | 46–50 | <50 | CPAP non-adherent, MAD non-adherent | 28.4 | 22.2 | 20.0 |
| P8 | 61–65 | 100 | CPAP | 24.4 | 6.9 | 31.0 |
| P9 | 36–40 | 100 | CPAP | 30.3 | 39.3 | 9.0 |
| P10 | 66–70 | 100 | CPAP non-adherent | 28.7 | 38.7 | 5.0 |
| W1 | 36–40 | 100 | CPAP | 27.5 | 23.0 | 4.5 |
| W2 | 56–60 | <50 | none | 37.6 | 81.4 | 1.5 |
| Overarching Theme | Theme | Subtheme | Number of Participants | Participant Count Visualization | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Facilitators | Motivation | Control of personal health | 10 | ||||||||||
| Quality of life | 5 | ||||||||||||
| CPAP avoidance | 10 | ||||||||||||
| General belief in positive effect of exercise | 8 | ||||||||||||
| Ability to establish OMT routine | 6 | ||||||||||||
| Perceived Support | Therapist support | 10 | |||||||||||
| Social support | 8 | ||||||||||||
| Commitment to the research project | 3 | ||||||||||||
| Perceived Effect | Subjective sleep quality improvement | 8 | |||||||||||
| Improvement of daytime functioning | 7 | ||||||||||||
| Increased muscle control | 5 | ||||||||||||
| Technology reporting sleep improvement | 5 | ||||||||||||
| Barriers | Motivation | Sickness burden | 6 | ||||||||||
| Comprehensive and fixed protocol | 7 | ||||||||||||
| Exercise performance difficulties | 5 | ||||||||||||
| Uncertainty about OMT effectiveness | 3 | ||||||||||||
| Perceived Support | Previous negative healthcare experience | 8 | |||||||||||
| Perceived burden of the sleep diary | 5 | ||||||||||||
| Lack of clear instructions | 2 | ||||||||||||
| Perceived effect | Subjective lack of improvements | 4 | |||||||||||
| Negative side effects | 4 | ||||||||||||
| Exercises perceived as not effective | 2 | ||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the International Association of Orofacial Myology (IAOM). Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hansen, D.D.; Tinbod, U.; Feng, X.; Dammen, T.; Hrubos-Strøm, H.; Skirbekk, H. Orofacial Myofunctional Therapy for Patients with Obstructive Sleep Apnea—A Mixed Methods Study of Facilitators and Barriers to Treatment Adherence. Int. J. Orofac. Myol. Myofunct. Ther. 2025, 51, 6. https://doi.org/10.3390/ijom51020006
Hansen DD, Tinbod U, Feng X, Dammen T, Hrubos-Strøm H, Skirbekk H. Orofacial Myofunctional Therapy for Patients with Obstructive Sleep Apnea—A Mixed Methods Study of Facilitators and Barriers to Treatment Adherence. International Journal of Orofacial Myology and Myofunctional Therapy. 2025; 51(2):6. https://doi.org/10.3390/ijom51020006
Chicago/Turabian StyleHansen, Diana Dobran, Unn Tinbod, Xin Feng, Toril Dammen, Harald Hrubos-Strøm, and Helge Skirbekk. 2025. "Orofacial Myofunctional Therapy for Patients with Obstructive Sleep Apnea—A Mixed Methods Study of Facilitators and Barriers to Treatment Adherence" International Journal of Orofacial Myology and Myofunctional Therapy 51, no. 2: 6. https://doi.org/10.3390/ijom51020006
APA StyleHansen, D. D., Tinbod, U., Feng, X., Dammen, T., Hrubos-Strøm, H., & Skirbekk, H. (2025). Orofacial Myofunctional Therapy for Patients with Obstructive Sleep Apnea—A Mixed Methods Study of Facilitators and Barriers to Treatment Adherence. International Journal of Orofacial Myology and Myofunctional Therapy, 51(2), 6. https://doi.org/10.3390/ijom51020006