
Uncommon Carotid Artery Stenting Complications: A Series by Images

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
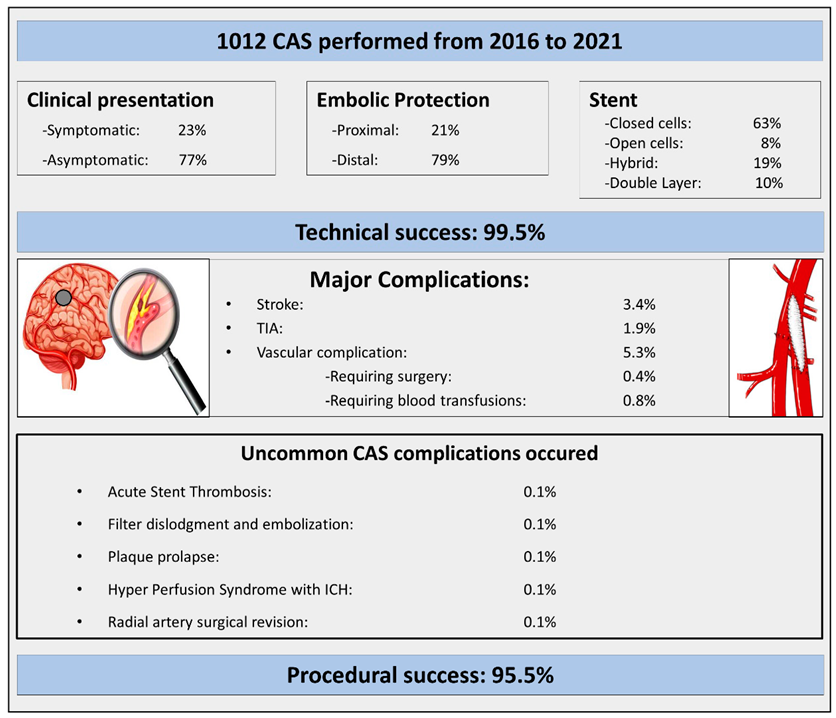
- (1)
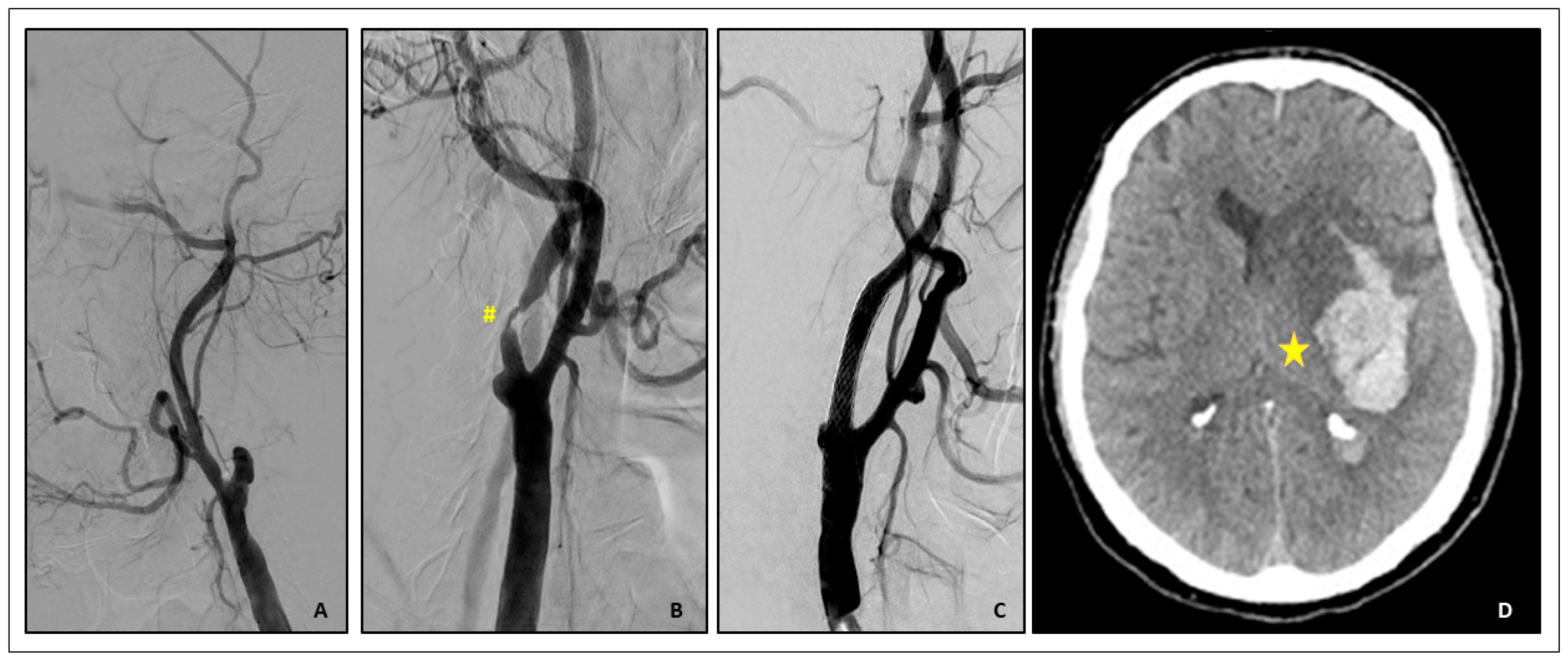
- Acute Carotid Stent thrombosis:
- Brief Case description:
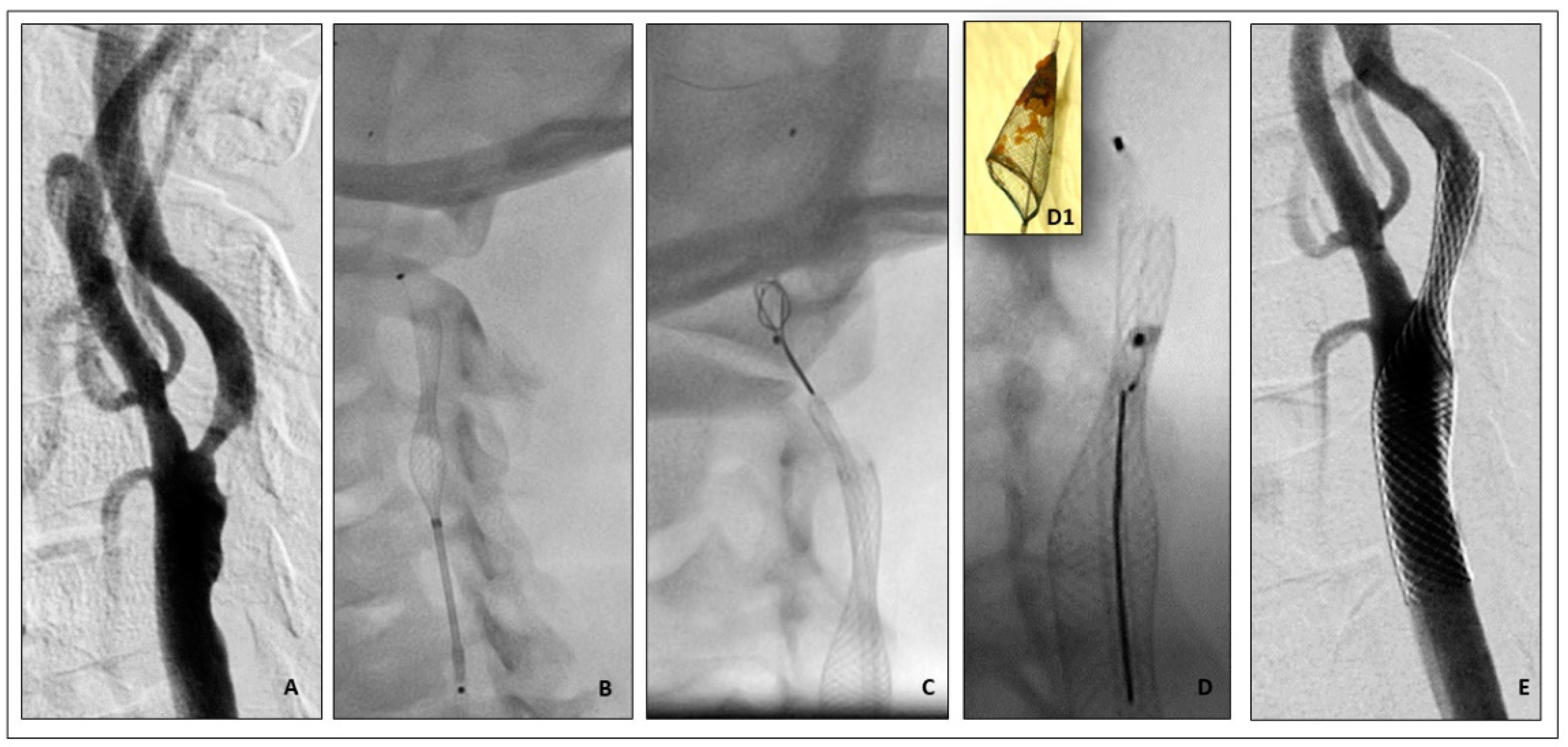
- (2)
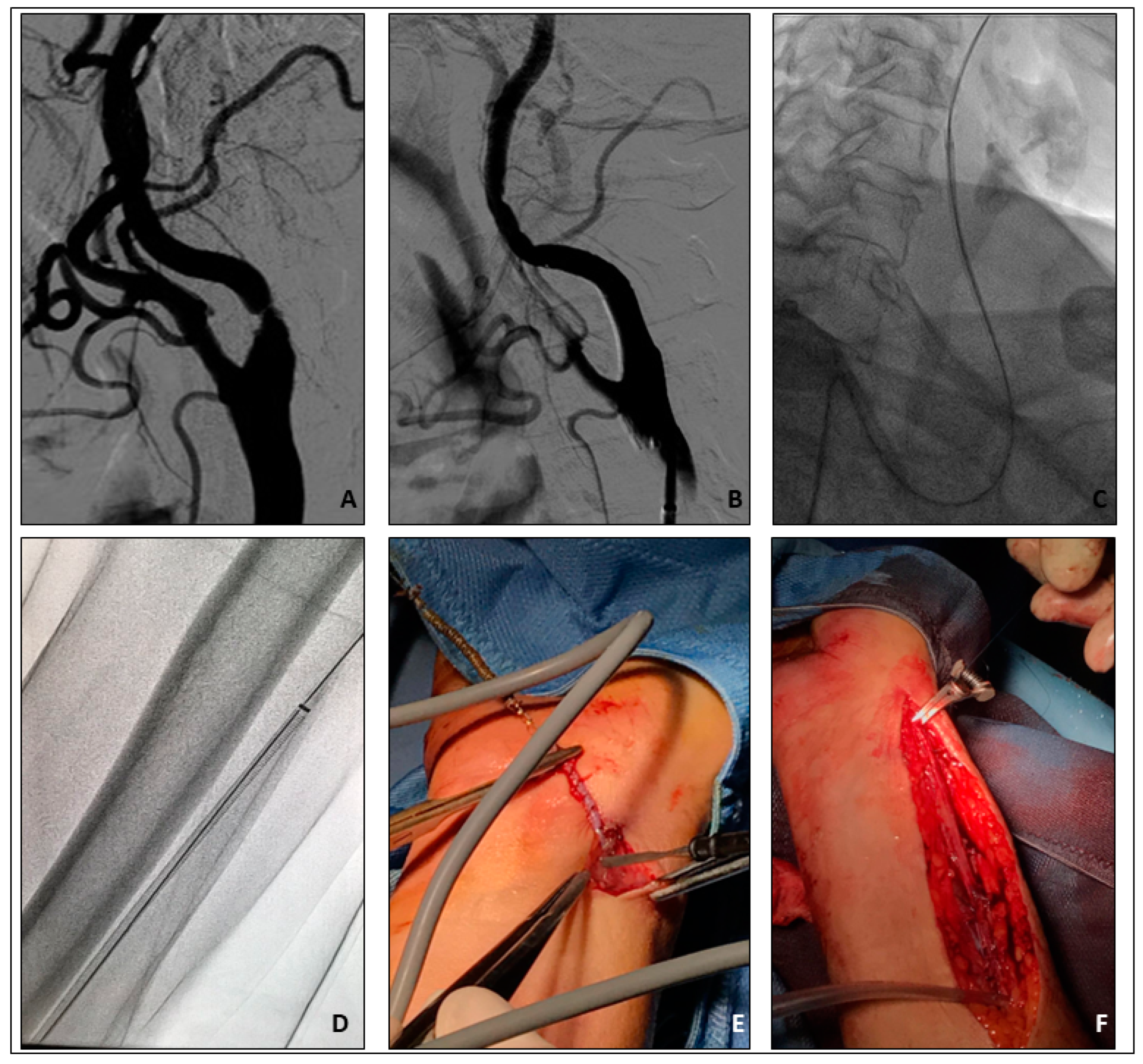
- Rescue retrieval of a disconnected distal cerebral embolic protection device
- Brief Case description:
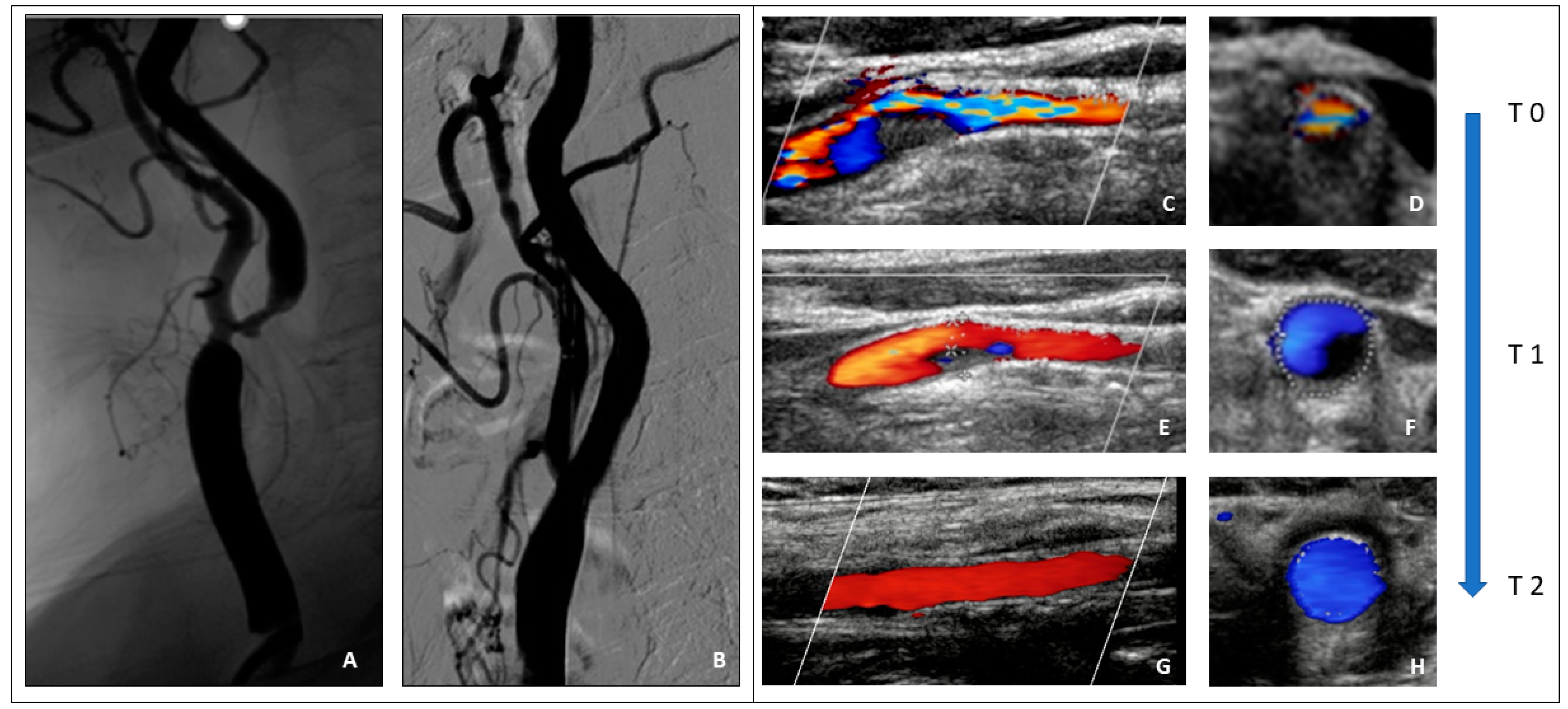
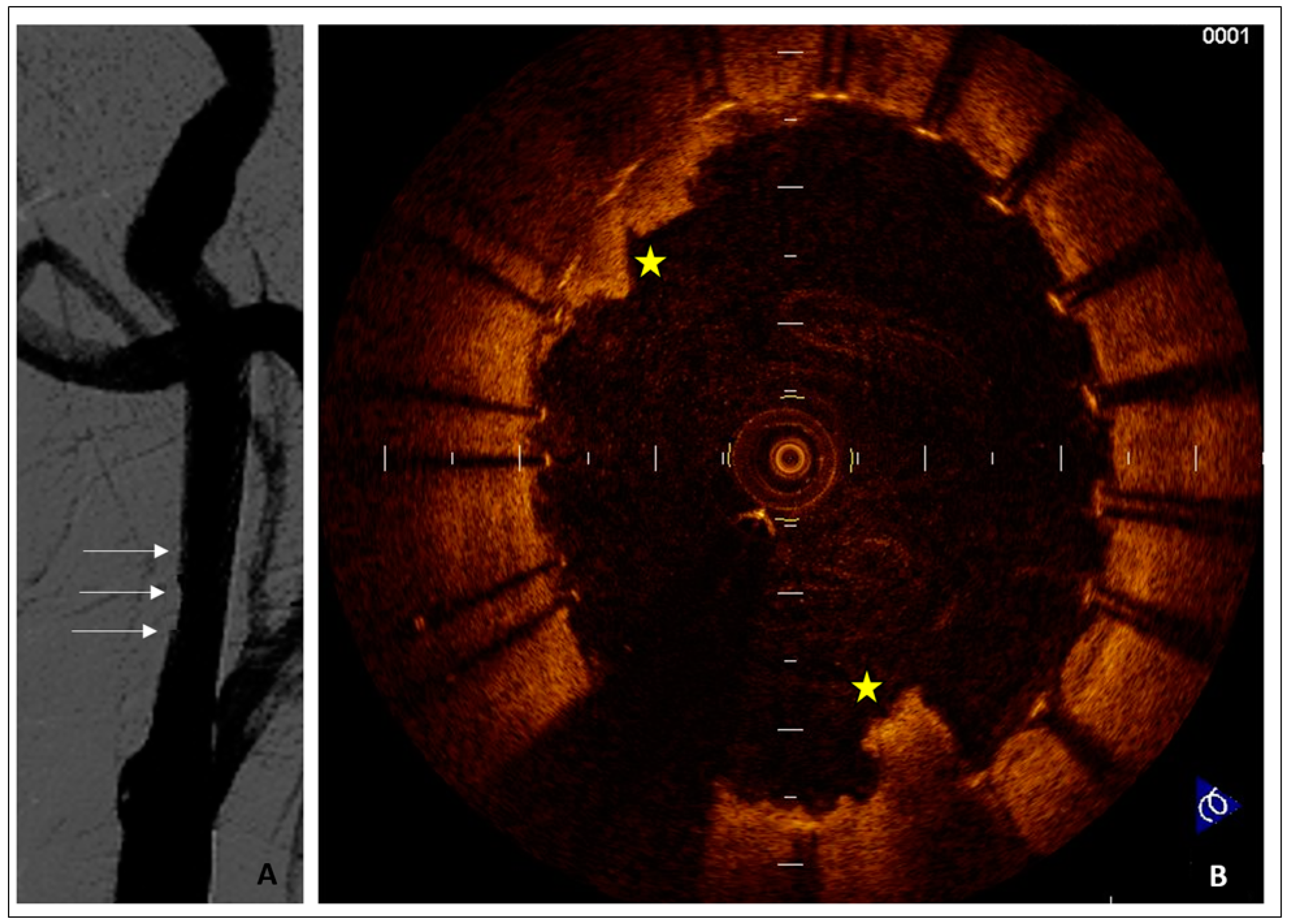
- (3)
- Plaque prolapse after carotid stenting
- Brief case description
- (4)
- Cerebral hyperperfusion syndrome (CHS)
- Brief case description
- (5)
- Vascular access site complications
- Brief Complication description:
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aboyans, V.; Ricco, J.-B.; Bartelink, M.-L.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.-P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [CrossRef]
- Müller, M.D.; Lyrer, P.; Brown, M.M.; Bonati, L.H. Carotid artery stenting versus endarterectomy for treatment of carotid artery stenosis. Cochrane Database Syst. Rev. 2020, 2. [Google Scholar] [CrossRef]
- White, C.J.; Brott, T.G.; Gray, W.A.; Heck, D.; Jovin, T.; Lyden, S.P.; Metzger, D.C.; Rosenfield, K.; Roubin, G.; Sachar, R.; et al. Carotid Artery Stenting: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 80, 155–170. [Google Scholar] [CrossRef]
- Giannopoulos, S.; Speziale, F.; Vadalà, G.; Soukas, P.; Kuhn, B.A.; Stoltz, C.L.; Foteh, M.I.; Mena-Hurtado, C.; Armstrong, E.J. Intravascular Lithotripsy for Treatment of Calcified Lesions During Carotid Artery Stenting. J. Endovasc. Ther. 2020, 28, 93–99. [Google Scholar] [CrossRef]
- Vadalà, G.; Galassi, A.R.; Nerla, R.; Micari, A. Shockwave intravascular lithoplasty for the treatment of calcified carotid artery stenosis: A very early single-center experience. Catheter. Cardiovasc. Interv. 2020, 96, E608–E613. [Google Scholar] [CrossRef]
- Lamanna, A.; Maingard, J.; Barras, C.D.; Kok, H.K.; Handelman, G.; Chandra, R.V.; Thijs, V.; Brooks, D.M.; Asadi, H. Carotid artery stenting: Current state of evidence and future directions. Acta Neurol. Scand. 2019, 139, 318–333. [Google Scholar] [CrossRef]
- Ferrante, G.; Rao, S.V.; Jüni, P.; Da Costa, B.R.; Reimers, B.; Condorelli, G.; Anzuini, A.; Jolly, S.S.; Bertrand, O.F.; Krucoff, M.W.; et al. Radial versus femoral access for coronary interventions across the entire spectrum of patients with coronary artery disease: A meta-analysis of randomized trials. JACC Cardiovasc. Interv. 2016, 9, 1419–1434. [Google Scholar] [CrossRef] [PubMed]
- Doyle, B.J.; Ting, H.H.; Bell, M.R.; Lennon, R.J.; Mathew, V.; Singh, M.; Holmes, D.R.; Rihal, C.S. Major Femoral Bleeding Complications After Percutaneous Coronary Intervention: Incidence, Predictors, and Impact on Long-Term Survival among 17,901 Patients Treated at the Mayo Clinic from 1994 to 2005. JACC Cardiovasc. Interv. 2008, 1, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418, Erratum in Stroke 2019, 50, e440–e441. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [PubMed]
- Moulakakis, K.G.; Mylonas, S.N.; Lazaris, A.; Tsivgoulis, G.; Kakisis, J.; Sfyroeras, G.S.; Antonopoulos, C.N.; Brountzos, E.N.; Vasdekis, S.N. Acute carotid stent thrombosis: A comprehensive review. Vasc. Endovasc. Surg. 2016, 50, 511–521. [Google Scholar] [CrossRef] [PubMed]
- Köklü, E.; Yüksel, İ.Ö.; Bayar, N.; Arslan, Ş. Is acute carotid artery stent thrombosis an avoidable complication? J. Stroke Cerebrovasc. Dis. 2015, 24, 2219–2222. [Google Scholar] [CrossRef] [PubMed]
- Coelho, A.P.; Lobo, M.; Nogueira, C.; Gouveia, R.; Campos, J.; Augusto, R.; Coelho, N.; Semião, A.C.; Canedo, A. Overview of evidence on risk factors and early management of acute carotid stent thrombosis during the last two decades. J. Vasc. Surg. 2019, 69, 952–964. [Google Scholar] [CrossRef] [PubMed]
- Kawabata, Y.; Nakajima, N.; Miyake, H.; Fukuda, S.; Tsukahara, T. Postoperative ischemic events in patients undergoing carotid artery stenting using algorithmic selection for embolic protection. Neuroradiol. J. 2019, 32, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Arai, S.; Ikeda, H.; Kawamo, M.; Kamiya, Y.; Mizutani, T. Surgical Rescue Retrieval of a Filter Protection Device in Carotid Artery Stenting with Stent Deformation: Case Report and Literature Review. World Neurosurg. 2018, 122, 215–219. [Google Scholar] [CrossRef]
- Micari, A.; Sbarzaglia, P.; Meeks, M.D.M.E.; Liso, A.; Riina, M.; Lunetto, M.L.; Roscitano, G.; Vadalà, G. New imaging modalities in peripheral interventions. Eur. Heart J. Suppl. 2015, 17, A18–A22. [Google Scholar] [CrossRef]
- Nerla, R.; Castriota, F.; Micari, A.; Sbarzaglia, P.; Secco, G.G.; Ruffino, M.A.; de Donato, G.; Setacci, C.; Cremonesi, A. Carotid artery stenting with a new-generation double-mesh stent in three high-volume Italian centres: Clinical results of a multidisciplinary approach. EuroIntervention 2016, 12, e677–e683. [Google Scholar] [CrossRef]
- Han, N.; Ma, Y.; Li, Y.; Zheng, Y.; Wu, C.; Gan, T.; Li, M.; Ma, L.; Zhang, J. Imaging and Hemodynamic Characteristics of Vulnerable Carotid Plaques and Artificial Intelligence Applications in Plaque Classification and Segmentation. Brain Sci. 2023, 13, 143. [Google Scholar] [CrossRef]
- Schillinger, M.; Dick, P.; Wiest, G.; Gentzsch, S.; Sabeti, S.; Haumer, M.; Willfort, A.; Nasel, C.; Wöber, C.; Zeitlhofer, J.; et al. Covered Versus Bare Self-Expanding Stents for Endovascular Treatment of Carotid Artery Stenosis: A Stopped Randomized Trial. J. Endovasc. Ther. 2006, 13, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Stabile, E.; De Donato, G.; Musialek, P.; Deloose, K.; Nerla, R.; Sirignano, P.; Chianese, S.; Mazurek, A.; Tesorio, T.; Bosiers, M.; et al. Use of Dual-Layered Stents in Endovascular Treatment of Extracranial Stenosis of the Internal Carotid Artery: Results of a Patient-Based Meta-Analysis of 4 Clinical Studies. JACC Cardiovasc. Interv. 2018, 11, 2405–2411. [Google Scholar] [CrossRef] [PubMed]
- Huibers, A.E.; Westerink, J.; de Vries, E.E.; Hoskam, A.; Ruijter, H.M.D.; Moll, F.L.; de Borst, G.J. Editor’s choice—Cerebral hyperperfusion syndrome after carotid artery stenting: A systematic review and meta-analysis. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 322–333. [Google Scholar] [CrossRef]
- Lin, Y.-H.; Liu, H.-M. Update on cerebral hyperperfusion syndrome. J. NeuroInterv. Surg. 2020, 12, 788–793. [Google Scholar] [CrossRef] [PubMed]
- García, A.G.; Moniche, F.; Escudero-Martínez, I.; Mancha, F.; Tomasello, A.; Ribó, M.; Delgado-Acosta, F.; Ochoa, J.J.; Heras, J.A.D.L.; López-Mesonero, L.; et al. Clinical predictors of hyperperfusion syndrome following carotid stenting: Results from a national prospective multicenter study. JACC Cardiovasc. Interv. 2019, 12, 873–882. [Google Scholar] [CrossRef]
- Kablak-Ziembicka, A.; Przewlocki, T.; Pieniazek, P.; Musialek, P.; Tekieli, L.; Rosławiecka, A.; Motyl, R.; Zmudka, K.; Tracz, W.; Podolec, P. Predictors of cerebral reperfusion injury after carotid stenting: The role of transcranial color-coded doppler ultrasonography. J. Endovasc. Ther. 2010, 17, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, M.; Itokawa, H.; Moriya, M.; Okamoto, N.; Sasanuma, J. Evaluation of cerebral hyperperfusion after carotid artery stenting using C-Arm CT measurements of cerebral blood volume. Clin. Neuroradiol. 2016, 28, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, S.; Yamagami, H.; Yoshimoto, T.; Morita, Y.; Yamamoto, H.; Toyoda, K.; Ihara, M. Cerebral hyperperfusion on arterial spin labeling MRI after reperfusion therapy is related to hemorrhagic transformation. J. Cereb. Blood Flow Metab. 2017, 37, 3087–3090. [Google Scholar] [CrossRef]
- Scalise, R.F.M.; Salito, A.M.; Polimeni, A.; Garcia-Ruiz, V.; Virga, V.; Frigione, P.; Andò, G.; Tumscitz, C.; Costa, F. Radial Artery Access for Percutaneous Cardiovascular Interventions: Contemporary Insights and Novel Approaches. J. Clin. Med. 2019, 8, 1727. [Google Scholar] [CrossRef]
- Jaroenngarmsamer, T.; Bhatia, K.D.; Kortman, H.; Orru, E.; Krings, T. Procedural success with radial access for carotid artery stenting: Systematic review and meta-analysis. J. NeuroInterv. Surg. 2019, 12, 87–93. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population: N = 1012 | N% |
|---|---|
| Age (years) | 72 ± 8.9 |
| Men | 739 (73) |
| Octogenarians | 233 (23) |
| Hypertension | 789 (78) |
| Hyperlipemia | 749 (74) |
| Diabetes mellitus | 575 (31.8) |
| Current or former smokers | 993 (54.9) |
| Symptomatic | 232 (23) |
| Asymptomatic | 780 (77) |
| Coronary artery disease | 210 (21) |
| Peripheral arterial disease | 187 (18.5) |
| Vascular Characteristics | |
| Left ICA lesions | 537 (53) |
| Right ICA lesions | 475 (47) |
| % Stenosis | 83±11 |
| Contralateral disease | 956 (52.9) |
| >70% | 101 (10) |
| Total occlusion | 30 (3) |
| Procedural Characteristics | |
| Technical success | 1007 (99.5) |
| Radial access | 132 (13) |
| Use of EPD | 1012 (100) |
| Proximal protection | 213 (21) |
| Distal protection | 799 (79) |
| Pre-dilatation | 213 (21) |
| Post-dilatation | 951 (94) |
| Stent Type | |
| Open cells | 81 (8) |
| Hybrid stent | 192 (19) |
| Closed cells | 638 (63) |
| Double layer | 113 (11) |
| Population: N = 1012 | N% |
|---|---|
| Procedural success | 967 (95.5) |
| MACCEs | |
| Total number | 64 (6.3) |
| Stroke | 35 (3.4) |
| Minor stroke | 22 (2.1) |
| Major stroke | 13 (1.3) |
| TIA | 20 (1.9) |
| Death | 6 (0.6) |
| Myocardial infarction | 1 (0.3) |
| Vascular Complications | |
| Total number | 54 (5.3) |
| Major hematoma | 24 (2.3) |
| Minor hematoma | 12 (1.1) |
| Retroperitoneal hematoma | 3 (0.3) |
| Pseudoaneurysm | 9 (0.9) |
| Arteriovenous fistula | 4 (0.4) |
| Requiring surgery | 4 (0.4) |
| Requiring blood transfusion | 8 (0.8) |
| Others | 2 (0.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vadalà, G.; Sucato, V.; Costa, F.; Castriota, F.; Nerla, R.; Roscitano, G.; Versace, A.G.; Galassi, A.R.; Micari, A. Uncommon Carotid Artery Stenting Complications: A Series by Images. J. Pers. Med. 2024, 14, 250. https://doi.org/10.3390/jpm14030250
Vadalà G, Sucato V, Costa F, Castriota F, Nerla R, Roscitano G, Versace AG, Galassi AR, Micari A. Uncommon Carotid Artery Stenting Complications: A Series by Images. Journal of Personalized Medicine. 2024; 14(3):250. https://doi.org/10.3390/jpm14030250
Chicago/Turabian StyleVadalà, Giuseppe, Vincenzo Sucato, Francesco Costa, Fausto Castriota, Roberto Nerla, Giuseppe Roscitano, Antonio Giovanni Versace, Alfredo Ruggero Galassi, and Antonio Micari. 2024. "Uncommon Carotid Artery Stenting Complications: A Series by Images" Journal of Personalized Medicine 14, no. 3: 250. https://doi.org/10.3390/jpm14030250
APA StyleVadalà, G., Sucato, V., Costa, F., Castriota, F., Nerla, R., Roscitano, G., Versace, A. G., Galassi, A. R., & Micari, A. (2024). Uncommon Carotid Artery Stenting Complications: A Series by Images. Journal of Personalized Medicine, 14(3), 250. https://doi.org/10.3390/jpm14030250