
Scoping Review: Environmental Factors Influencing Food Intake in Mental Health Inpatient Settings



Abstract

1. Introduction
- (i)
- Anthropometry—i.e., body mass index, waist-to-hip ratio [85];
- (ii)
- Biochemistry—routine bloods (i.e., liver function test, urea and electrolytes, full blood count, vitamin D, and other micronutrients where indicated) [72];
- (iii)
- Clinical status—diagnosis and associated co-morbidities, using mental health screening tools such as the Patient Health Questionnaire (PHQ-9) or Health of the Nation Outcomes Scales (HoNOS) [85];
- (iv)
- Dietary intake—using a social functioning scale [85] and validated food frequency questionnaires such as EPIC-Norfolk [86] or 15-items FFQ [87], along with the “practical nutrition knowledge about balanced meals” (PKB-7) scale [88] to assess nutritional literacy, dietary adequacy, and adherence to dietary recommendations, respectively; the results can then be used as part of:
- (v)
2. Methods
2.1. Preparing to Scope the Literature and Protocol Development
2.2. Identifying the Research Questions
2.3. Data Sources—Stage 1
2.4. Search Strategy—Stage 2
2.5. Study Selection—Stage 3
2.5.1. Inclusion Criteria
2.5.2. Exclusion Criteria
2.6. Data Extraction—Stage 4
2.7. Collating, Summarizing, and Reporting the Results—Stage 5
3. Results
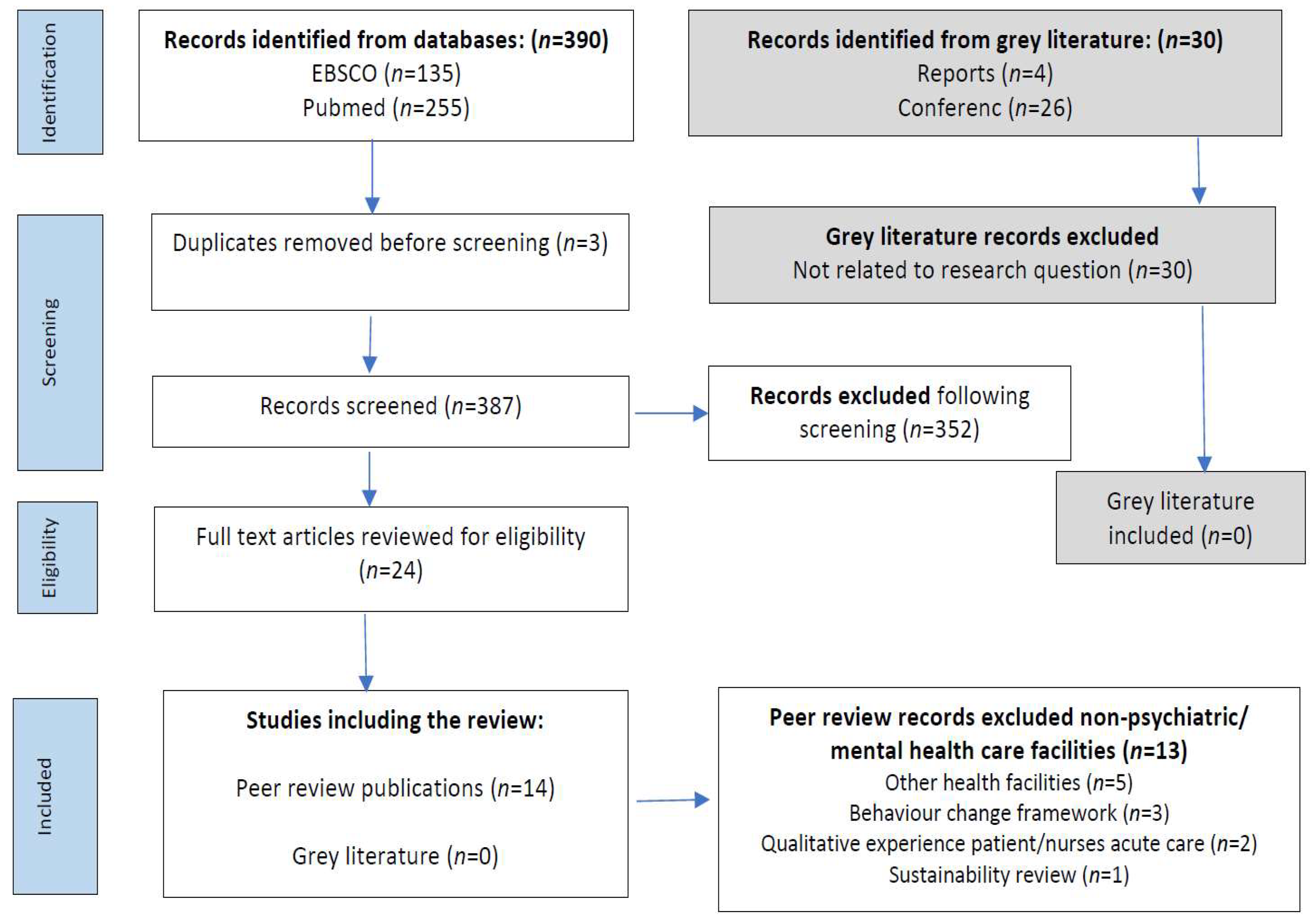
3.1. Selection and Characteristics of Included Articles
3.2. Study Characteristics
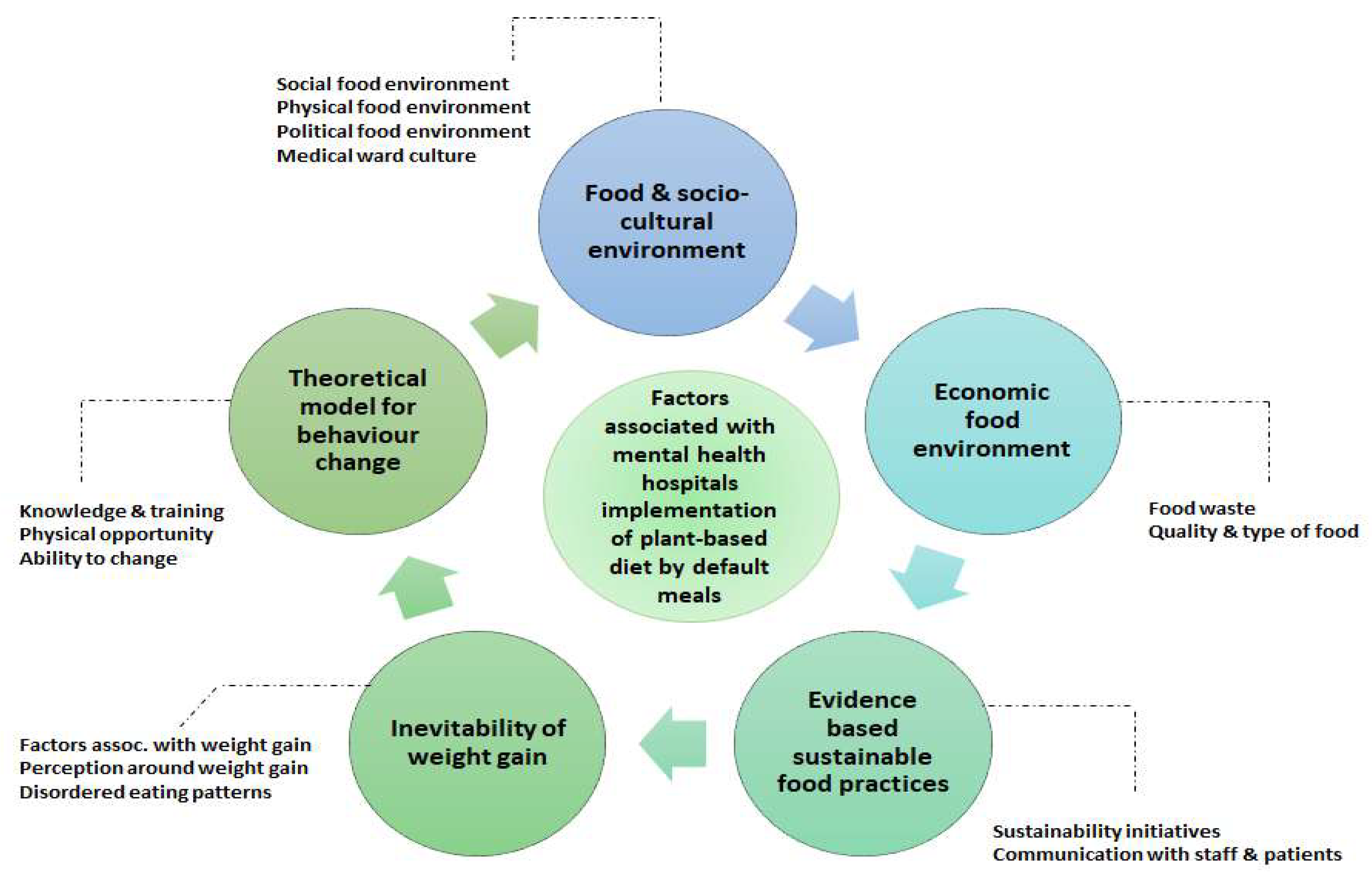
3.3. Content Analysis: Conceptual Framework and Overarching Themes
- Food and socio-cultural environment: (i) physical food environment, (ii) political food environment, (iii) medical ward culture;
- Evidence-based measures to reduce food waste: (i) sustainability initiatives, (ii) communication with staff and patients;
- Economic food environment: (i) quality and type of food, (ii) food waste;
- Inevitability of weight gain: (i) factors associated with weight gain, (ii) perceptions around weight gain;
- Theoretical model for behaviour change: (i) knowledge and training, (ii) physical opportunity, (iii) ability to change.
3.3.1. Food and Socio-Cultural Environment
- (i)
- Physical food environment
- (ii)
- Political food environment
- (iii)
- Medical ward culture
3.3.2. Evidence-Based Sustainable Food Practices
- (i)
- Sustainability initiatives
- (ii)
- Communication with staff and patients
3.3.3. Economic Food Environment
- (i)
- Quality and type of food
- (ii)
- Food waste
3.3.4. Inevitability of Weight Gain
- (i)
- Factors associated with weight gain
- (ii)
- Perceptions around weight gain
3.3.5. Theoretical Model for Behaviour Change
- (i)
- Knowledge and training
- (ii)
- Physical opportunity
- (iii)
- Ability to change
4. Discussion
- (i)
- Knowledge exchange—opportunities to provide patients and staff with information on plant-forward diets and phased approaches to a planet-friendly diet [143];
- (ii)
- Motivational interviewing with prompts around goal setting for changes [144];
- (iii)
- Problem solving—helping patients and staff identify strategies to support advance planning of meals/food, organisation, and access to good quality food, including strategies to reduce the purchase of ultra-high-processed or fast foods [139] and self-monitoring of behaviour—through peer-led support [145].
5. Research Limitations
- (i)
- Information sharing around healthy and planet-friendly food: to staff, patients and visitors, increasing awareness and promoting support for food-based initiatives including maintaining a healthy weight;
- (ii)
- Procurement of sustainable/nutritious food: from local providers, reducing the environmental footprint and showcasing local seasonal foods;
- (iii)
- Quality improvement feedback mechanisms: offering staff, patients, and visitors the opportunity to comment on food quality along with food preferences, as this may help to improve satisfaction. This approach will also identify meals that are disliked, supporting renovation of recipes as well as areas where more information is required, as well as reducing food waste;
- (iv)
- Regular audit and monitoring and collaboration with nutritionist/dietitians: using a standardised approach and regular reviews to help organisations (including leadership teams) set targets for reducing food waste, as well as to identify meals with lower acceptance. This may be true for newer plant-based diets where more information for staff, visitors, and patients is required to increase acceptance of new dishes;
- (v)
- Kitchen staff training and knowledge exchange: to ensure food waste is minimised and to increase understanding of approaches to food waste reduction strategies;
- (vi)
- Ward staff training: to support patients and staff to make healthier planet-friendly food choices.
- (vii)
- Reduced portion sizes: have been shown to be effective in reducing food waste and the obesogenic nature of meals.
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- UNFCCC. The Paris Agreement. Available online: https://unfccc.int/process-and-meetings/the-paris-agreement/the-paris-agreement (accessed on 21 December 2022).
- CCARDESA. IPCC Special Report: Global Warming of 1.5 °C—Summary for Policymakers. 2019. Available online: https://www.ipcc.ch/sr15/chapter/spm/ (accessed on 21 December 2022).
- How Do Greenhouse Gases Actually Warm the Planet? 2022. Available online: https://www.unep.org/news-and-stories/story/how-do-greenhouse-gases-actually-warm-planet (accessed on 28 January 2025).
- Wu, R. The carbon footprint of the Chinese health-care system: An environmentally extended input-output and structural path analysis study. Lancet Planet Health 2019, 10, e413–e419. [Google Scholar] [CrossRef] [PubMed]
- Climate Change and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/climate-change-and-health (accessed on 21 December 2022).
- Erol, A.; Karahan, H. Energy consumption and emission factors of a hospital in Turkey. J. Clean. Prod. 2018, 207, 384–393. [Google Scholar]
- Health-Care Waste. Available online: https://www.who.int/news-room/fact-sheets/detail/health-care-waste (accessed on 16 December 2023).
- Health Care Without Harm. The Role of the Health Care Sector in Climate Change Mitigation. In London. 2022. Available online: https://healthcareclimateaction.org/node/115 (accessed on 16 December 2023).
- Health Care Without Harm (Global). Health Care Climate Footprint Report. Available online: https://global.noharm.org/resources/health-care-climate-footprint-report (accessed on 29 January 2025).
- Ngcamu, B.S. Climate change effects on vulnerable populations in the Global South: A systematic review. Nat. Hazards 2023, 118, 977–991. [Google Scholar] [CrossRef]
- Abbass, K.; Qasim, M.Z.; Song, H.; Murshed, M.; Mahmood, H.; Younis, I. A review of the global climate change impacts, adaptation, and sustainable mitigation measures. Environ. Sci. Pollut. Res. 2022, 29, 42539–42559. [Google Scholar] [CrossRef]
- Tennison, I.; Roschnik, S.; Ashby, B.; Boyd, R.; Hamilton, I.; Oreszczyn, T.; Owen, A.; Romanello, M.; Ruyssevelt, P.; Sherman, J.D.; et al. Health care’s response to climate change: A carbon footprint assessment of the NHS in England. Lancet Planet. Health 2021, 5, e84–e92. [Google Scholar] [CrossRef] [PubMed]
- Wooldridge, G.; Murthy, S. Pediatric Critical Care and the Climate Emergency: Our Responsibilities and a Call for Change. Front. Pediatr. 2020, 8, 472. [Google Scholar] [CrossRef]
- England NHS. National Standards for Healthcare Food and Drink. 2022. Available online: https://www.england.nhs.uk/publication/national-standards-for-healthcare-food-and-drink/ (accessed on 16 January 2025).
- From Farm to Kitchen: The Environmental Impacts of U.S. Food Waste. Available online: https://www.epa.gov/land-research/farm-kitchen-environmental-impacts-us-food-waste#:~:text=Impacts%20include%3A%20greenhouse%20gas%20emissions,to%20California%20and%20New%20York (accessed on 16 January 2025).
- Alam, M.M.; Sujauddin, M.; Iqbal, G.M.A.; Huda, S.M.S. Report: Healthcare waste characterization in Chittagong Medical College Hospital, Bangladesh. Waste Manag. Res. 2008, 26, 291–296. [Google Scholar] [CrossRef]
- Mattoso, V.D.; Schalch, V. Hospital waste management in Brazil: A case study. Waste Manag. Res. 2001, 19, 567–572. [Google Scholar] [CrossRef]
- Nutrition and Hydration Digest, 3rd ed.; British Dietetic Association: Birmingham, UK, 2023; Available online: https://www.bda.uk.com/static/176907a2-f2d8-45bb-8213c581d3ccd7ba/06c5eecf-fa85-4472-948806c5165ed5d9/Nutrition-and-Hydration-Digest-3rd-edition.pdf (accessed on 12 August 2024).
- Food Surplus and Waste in the UK—Key Facts. 2020. Available online: https://www.wrap.ngo/sites/default/files/2020-11/Food-surplus-and-waste-in-the-UK-key-facts-Jan-2020.pdf (accessed on 13 August 2024).
- Chatzipavlou, M.; Karayiannis, D.; Chaloulakou, S.; Georgakopoulou, E.; Poulia, K.A. Implementation of sustainable food service systems in hospitals to achieve current sustainability goals: A scoping review. Clin. Nutr. ESPEN 2024, 61, 237–252. [Google Scholar] [CrossRef]
- Cook, N.; Collins, J.; Goodwin, D.; Porter, J. A systematic review of food waste audit methods in hospital foodservices: Development of a consensus pathway food waste audit tool. J. Hum. Nutr. Diet. 2022, 35, 68–80. [Google Scholar] [CrossRef]
- Cook, N.; Collins, J.; Goodwin, D.; Porter, J. Factors influencing implementation of food and food-related waste audits in hospital foodservices. Front. Nutr. 2022, 9, 1062619. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.; Porter, J.; Goodwin, D.; Collins, J. Diverting Food Waste From Landfill in Exemplar Hospital Foodservices: A Qualitative Study. J. Acad. Nutr. Diet. 2024, 124, 725–739. [Google Scholar] [CrossRef]
- Mahmoudifar, K.; Raeesi, A.; Kiani, B.; Rezaie, M. Food waste in hospitals: Implications and strategies for reduction: A systematic review. Manag. Environ. Qual. Int. J. 2025, 36, 50–71. [Google Scholar] [CrossRef]
- Rinninella, E.; Raoul, P.; Maccauro, V.; Cintoni, M.; Cambieri, A.; Fiore, A.; Zega, M.; Gasbarrini, A.; Mele, M.C. Hospital Services to Improve Nutritional Intake and Reduce Food Waste: A Systematic Review. Nutrients 2023, 15, 310. [Google Scholar] [CrossRef]
- Simzari, K.; Vahabzadeh, D.; Nouri Saeidlou, S.; Khoshbin, S.; Bektas, Y. Food intake, plate waste and its association with malnutrition in hospitalized patients. Nutr. Hosp. 2017, 34, 1376–1381. [Google Scholar]
- Hancox, L.E.; Lee, P.S.; Armaghanian, N.; Hirani, V.; Wakefield, G. Nutrition risk screening methods for adults living with severe mental illness: A scoping review. Nutr. Diet. 2022, 79, 349–363. [Google Scholar] [CrossRef]
- Smith, J.; Ker, S.; Archer, D.; Gilbody, S.; Peckham, E.; Hardman, C.A. Food insecurity and severe mental illness: Understanding the hidden problem and how to ask about food access during routine healthcare. BJPsych Adv. 2023, 29, 204–212. [Google Scholar] [CrossRef]
- Kamoi, R.; Mifune, Y.; Soriano, K.; Tanioka, R.; Yamanaka, R.; Ito, H.; Osaka, K.; Umehara, H.; Shimomoto, R.; Bollos, L.A.; et al. Association Between Dynapenia/Sarcopenia, Extrapyramidal Symptoms, Negative Symptoms, Body Composition, and Nutritional Status in Patients with Chronic Schizophrenia. Healthcare 2024, 13, 48. [Google Scholar] [CrossRef] [PubMed]
- Seiler, N.; Tsiglopoulos, J.; Keem, M.; Das, S.; Waterdrinker, A. Prevalence of vitamin D deficiency among psychiatric inpatients: A systematic review. Int. J. Psychiatry Clin. Pract. 2022, 26, 330–336. [Google Scholar] [CrossRef]
- Hsieh, Y.C.; Chou, L.S.; Lin, C.H.; Wu, H.C.; Li, D.J.; Tseng, P.T. Serum folate levels in bipolar disorder: A systematic review and meta-analysis. BMC Psychiatry 2019, 19, 305. [Google Scholar] [CrossRef]
- Williams, P.; Walton, K. Plate waste in hospitals and strategies for change. e-SPEN Eur. E-J. Clin. Nutr. Metab. 2011, 6, e235–e241. [Google Scholar] [CrossRef]
- Kent-Smith, L.; Eisenbraun, C.; Wile, H. Hospital Patients Are Not Eating Their Full Meal: Results of the Canadian 2010–2011 nutritionDay Survey. Can. J. Diet. Pract. Res. 2016, 77, 25–29. [Google Scholar] [CrossRef]
- Hiesmayr, M.; Schindler, K.; Pernicka, E.; Schuh, C.; Schoeniger-Hekele, A.; Bauer, P.; Laviano, A.; Lovell, A.; Mouhieddine, M.; Schuetz, T.; et al. Decreased food intake is a risk factor for mortality in hospitalised patients: The NutritionDay survey 2006. Clin. Nutr. 2009, 28, 484–491. [Google Scholar] [CrossRef]
- Baumgartner, A.; Kägi-Braun, N.; Tribolet, P.; Gomes, F.; Stanga, Z.; Schuetz, P. Individualised nutritional support in medical inpatients—A practical guideline. Swiss Med. Wkly. 2020, 150, w20204. [Google Scholar] [CrossRef] [PubMed]
- Cristancho, C.; Mogensen, K.M.; Robinson, M.K. Malnutrition in patients with obesity: An overview perspective. Nutr. Clin. Pract. 2024, 39, 1300–1316. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Long, Y.; Peng, R.; He, P.; Luo, Y.; Zhang, Y.; Wang, W.; Yu, X.; Deng, L.; Zhu, Z. Epidemiology, Controversies, and Dilemmas of Perioperative Nutritional Risk/Malnutrition: A Narrative Literature Review. Risk Manag. Healthc. Policy 2025, 18, 143–162. [Google Scholar] [CrossRef]
- Wunderle, C.; Gomes, F.; Schuetz, P.; Stumpf, F.; Austin, P.; Ballesteros-Pomar, M.D.; Cederholm, T.; Fletcher, J.; Laviano, A.; Norman, K.; et al. ESPEN practical guideline: Nutritional support for polymorbid medical inpatients. Clin. Nutr. 2024, 43, 674–691. [Google Scholar] [CrossRef]
- Giménez-Palomo, A.; Gomes-da-Costa, S.; Borràs, R.; Pons-Cabrera, M.T.; Doncel-Moriano, A.; Arbelo, N.; Leyes, P.; Forga, M.; Mateu-Salat, M.; Pereira-Fernandes, P.M.; et al. Effects of malnutrition on length of stay in patients hospitalized in an acute psychiatric ward. Acta Psychiatr. Scand. 2023, 148, 316–326. [Google Scholar] [CrossRef]
- Johnson, M.; Day, M.; Moholkar, R.; Gilluley, P.; Goyder, E. Tackling obesity in mental health secure units: A mixed method synthesis of available evidence. BJPsych Open 2018, 4, 294–301. [Google Scholar] [CrossRef]
- Osman, N.S.; Md Nor, N.; Md Sharif, M.S.; Hamid, S.B.A.; Rahamat, S. Hospital Food Service Strategies to Improve Food Intakes among Inpatients: A Systematic Review. Nutrients 2021, 13, 3649. [Google Scholar] [CrossRef]
- The King’s Fund. Mental Health 360|Acute Care for Adults. Available online: https://www.kingsfund.org.uk/insight-and-analysis/long-reads/mental-health-360-acute-mental-health-care-adults (accessed on 13 August 2024).
- The Health Foundation. Longer Hospital Stays and Fewer Admissions. Available online: https://www.health.org.uk/publications/long-reads/longer-hospital-stays-and-fewer-admissions (accessed on 13 August 2024).
- Porter, J.; Collins, J. Nutritional intake and foodservice satisfaction of adults receiving specialist inpatient mental health services. Nutr. Diet. 2022, 79, 411–418. [Google Scholar] [CrossRef]
- Vancampfort, D.; Wampers, M.; Mitchell, A.J.; Correll, C.U.; De Herdt, A.; Probst, M.; De Hert, M. A meta-analysis of cardio-metabolic abnormalities in drug naïve, first-episode and multi-episode patients with schizophrenia versus general population controls. World Psychiatry 2013, 12, 240–250. [Google Scholar] [CrossRef]
- Rakshasa-Loots, A.M.; Steyn, C.; Swiffen, D.; Marwick, K.F.M.; Semple, R.K.; Reynolds, R.M.; Burgess, K.; Lawrie, S.M.; Lightman, S.L.; Luz, S.; et al. Metabolic biomarkers of clinical outcomes in severe mental illness (METPSY): Protocol for a prospective observational study in the Hub for metabolic psychiatry. BMC Psychiatry 2025, 25, 122. [Google Scholar] [CrossRef]
- Mozaffarian, D. Defining a healthy diet globally: The good, the bad, and the ugly. Am. J. Clin. Nutr. 2024, 120, 1003–1004. [Google Scholar] [CrossRef]
- Fanzo, J.; Rudie, C.; Sigman, I.; Grinspoon, S.; Benton, T.G.; Brown, M.E.; Covic, N.; Fitch, K.; Golden, C.D.; Grace, D.; et al. Sustainable food systems and nutrition in the 21st century: A report from the 22nd annual Harvard Nutrition Obesity Symposium. Am. J. Clin. Nutr. 2021, 115, 18–33. [Google Scholar] [CrossRef] [PubMed]
- Viroli, G.; Kalmpourtzidou, A.; Cena, H. Exploring Benefits and Barriers of Plant-Based Diets: Health, Environmental Impact, Food Accessibility and Acceptability. Nutrients 2023, 15, 4723. [Google Scholar] [CrossRef] [PubMed]
- Owino, V.; Kumwenda, C.; Ekesa, B.; Parker, M.E.; Ewoldt, L.; Roos, N.; Lee, W.T.; Tome, D. The impact of climate change on food systems, diet quality, nutrition, and health outcomes: A narrative review. Front. Clim. 2022, 4, 941842. [Google Scholar] [CrossRef]
- Clemente-Suárez, V.J.; Beltrán-Velasco, A.I.; Redondo-Flórez, L.; Martín-Rodríguez, A.; Tornero-Aguilera, J.F. Global Impacts of Western Diet and Its Effects on Metabolism and Health: A Narrative Review. Nutrients 2023, 15, 2749. [Google Scholar] [CrossRef]
- One Health. Available online: https://www.who.int/health-topics/one-health (accessed on 26 January 2025).
- Department of Economic and Social Affairs. Food Security and Nutrition and Sustainable Agriculture. Available online: https://sdgs.un.org/topics/food-security-and-nutrition-and-sustainable-agriculture (accessed on 27 January 2025).
- Xu, X.; Sharma, P.; Shu, S.; Lin, T.S.; Ciais, P.; Tubiello, F.N.; Smith, P.; Campbell, N.; Jain, A.K. Global greenhouse gas emissions from animal-based foods are twice those of plant-based foods. Nat. Food 2021, 2, 724–732. [Google Scholar] [CrossRef]
- Hemler, E.C.; Hu, F.B. Plant-Based Diets for Personal, Population, and Planetary Health. Adv. Nutr. 2019, 10, S275–S283. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, J.; Cappuccio, F.P. Plant-Based Dietary Patterns for Human and Planetary Health. Nutrients 2022, 14, 1614. [Google Scholar] [CrossRef] [PubMed]
- Food Compliance Solutions. Ultra-Processed Foods: Nova Classification. 2021. Available online: https://regulatory.mxns.com/en/ultra-processed-foods-nova-classification (accessed on 29 January 2025).
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- EAT. EAT-Lancet Commission Brief for Everyone. Available online: https://eatforum.org/lancet-commission/eatinghealthyandsustainable/ (accessed on 4 February 2025).
- Hoenink, J.C.; Garrott, K.; Jones, N.R.V.; Conklin, A.I.; Monsivais, P.; Adams, J. Changes in UK price disparities between healthy and less healthy foods over 10 years: An updated analysis with insights in the context of inflationary increases in the cost-of-living from 2021. Appetite 2024, 197, 107290. [Google Scholar] [CrossRef]
- Drewnowski, A. Analysing the affordability of the EAT–Lancet diet. Lancet Glob. Health 2020, 8, e6–e7. [Google Scholar] [CrossRef]
- Hirvonen, K.; Bai, Y.; Headey, D.; Masters, W.A. Affordability of the EAT-Lancet reference diet: A global analysis. Lancet Glob. Health 2020, 8, e59–e66. [Google Scholar] [CrossRef] [PubMed]
- Pais, D.F.; Marques, A.C.; Fuinhas, J.A. The cost of healthier and more sustainable food choices: Do plant-based consumers spend more on food? Agric. Food Econ. 2022, 10, 18. [Google Scholar] [CrossRef] [PubMed]
- Mambrini, S.P.; Penzavecchia, C.; Menichetti, F.; Foppiani, A.; Leone, A.; Pellizzari, M.; Sileo, F.; Battezzati, A.; Bertoli, S.; De Amicis, R. Plant-based and sustainable diet: A systematic review of its impact on obesity. Obes. Rev. 2025, p. e13901. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/obr.13901?msockid=12382da5a90f6ceb15f838b7ad0f67c3 (accessed on 2 February 2025).
- Liu, J.; Shen, Q.; Wang, X. Emerging EAT-Lancet planetary health diet is associated with major cardiovascular diseases and all-cause mortality: A global systematic review and meta-analysis. Clin. Nutr. 2024, 43, 167–179. [Google Scholar] [CrossRef]
- Adan, R.A.H.; van der Beek, E.M.; Buitelaar, J.K.; Cryan, J.F.; Hebebrand, J.; Higgs, S.; Schellekens, H.; Dickson, S.L. Nutritional psychiatry: Towards improving mental health by what you eat. Eur. Neuropsychopharmacol. 2019, 29, 1321–1332. [Google Scholar] [CrossRef]
- Haghighatdoost, F.; Mahdavi, A.; Mohammadifard, N.; Hassannejad, R.; Najafi, F.; Farshidi, H.; Lotfizadeh, M.; Kazemi, T.; Karimi, S.; Roohafza, H.; et al. The relationship between a plant-based diet and mental health: Evidence from a cross-sectional multicentric community trial (LIPOKAP study). PLoS ONE 2023, 18, e0284446. [Google Scholar] [CrossRef]
- Fadnes, L.T.; Celis-Morales, C.; Økland, J.M.; Parra-Soto, S.; Livingstone, K.M.; Ho, F.K.; Pell, J.P.; Balakrishna, R.; Arjmand, E.J.; Johansson, K.A.; et al. Life expectancy can increase by up to 10 years following sustained shifts towards healthier diets in the United Kingdom. Nat. Food 2023, 4, 961–965. [Google Scholar] [CrossRef]
- Ocklenburg, S.; Borawski, J. Vegetarian diet and depression scores: A meta-analysis. J. Affect. Disord. 2021, 294, 813–815. [Google Scholar] [CrossRef] [PubMed]
- Dobersek, U.; Teel, K.; Altmeyer, S.; Adkins, J.; Wy, G.; Peak, J. Meat and mental health: A meta-analysis of meat consumption, depression, and anxiety. Crit. Rev. Food Sci. Nutr. 2023, 63, 3556–3573. [Google Scholar] [CrossRef] [PubMed]
- Aucoin, M.; LaChance, L.; Cooley, K.; Kidd, S. Diet and Psychosis: A Scoping Review. Neuropsychobiology 2020, 79, 20–42. [Google Scholar] [CrossRef]
- Firth, J.; Carney, R.; Stubbs, B.; Teasdale, S.B.; Vancampfort, D.; Ward, P.B.; Berk, M.; Sarris, J. Nutritional Deficiencies and Clinical Correlates in First-Episode Psychosis: A Systematic Review and Meta-analysis. Schizophr. Bull. 2018, 44, 1275–1292. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, S.B.; Ward, P.B.; Samaras, K.; Firth, J.; Stubbs, B.; Tripodi, E.; Burrows, T.L. Dietary intake of people with severe mental illness: Systematic review and meta-analysis. Br. J. Psychiatry 2019, 214, 251–259. [Google Scholar] [CrossRef]
- Gill, R.; Tyndall, S.F.; Vora, D.; Hasan, R.; Megna, J.L.; Leontieva, L. Diet Quality and Mental Health Amongst Acute Inpatient Psychiatric Patients. Cureus 2021, 13, e12434. [Google Scholar] [CrossRef]
- Storz, M.A. Should plant-based hospital meals be the law? An American experience. Hosp. Pract. 2020, 48, 241–243. [Google Scholar] [CrossRef]
- Joiner, A.B. Dietary advice for people with severe mental illness. Lancet Psychiatry 2018, 5, 299. [Google Scholar] [CrossRef]
- Karczewski, K.J.; Snyder, M.P. Integrative omics for health and disease. Nat. Rev. Genet. 2018, 19, 299–310. [Google Scholar] [CrossRef]
- Bekdash, R.A. Methyl Donors, Epigenetic Alterations, and Brain Health: Understanding the Connection. Int. J. Mol. Sci. 2023, 24, 2346. [Google Scholar] [CrossRef]
- Rondinella, D.; Raoul, P.C.; Valeriani, E.; Venturini, I.; Cintoni, M.; Severino, A.; Galli, F.S.; Mora, V.; Mele, M.C.; Cammarota, G.; et al. The Detrimental Impact of Ultra-Processed Foods on the Human Gut Microbiome and Gut Barrier. Nutrients 2025, 17, 859. [Google Scholar] [CrossRef] [PubMed]
- Hoeylaerts, S.; Van Opstal, A.; Huybrechts, I.; Koppen, G.; Devlieger, R.; Godderis, L.; Pauwels, S. Validation of a food-frequency questionnaire to assess methyl-group donor intake in preschoolers. Eur. J. Pediatr. 2022, 181, 1871–1881. [Google Scholar] [CrossRef] [PubMed]
- Medawar, E.; Huhn, S.; Villringer, A.; Veronica Witte, A. The effects of plant-based diets on the body and the brain: A systematic review. Transl. Psychiatry 2019, 9, 226. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.E.; Georgestone, K.; Mutindori, C.; Nicanord, E.J. Exploring Plant-Based Nutrition for Patients with Substance Use Disorders: A Scoping Review of Dietary Intake and Potential Applications. Subst. Use Addict. J. 2025, 1–11. [Google Scholar] [CrossRef]
- Kemp, T.; Lopez, N.V.; Ward, S.; Sherzai, D.; Sherzai, A.; Sutliffe, J. The INFINITE Study: Pilot Research Exploring Plant-Based Nutrition in Treatment for Substance Use Disorders. Am. J. Lifestyle Med. 2022, 19, 572–584. [Google Scholar] [CrossRef]
- Cortés-Aguilar, R.; Malih, N.; Abbate, M.; Fresneda, S.; Yañez, A.; Bennasar-Veny, M. Validity of nutrition screening tools for risk of malnutrition among hospitalized adult patients: A systematic review and meta-analysis. Clin. Nutr. 2024, 43, 1094–1116. [Google Scholar] [CrossRef]
- Mötteli, S.; Provaznikova, B.; Vetter, S.; Jäger, M.; Seifritz, E.; Hotzy, F. Examining Nutrition Knowledge, Skills, and Eating Behaviours in People with Severe Mental Illness: A Cross-Sectional Comparison among Psychiatric Inpatients, Outpatients, and Healthy Adults. Nutrients 2023, 15, 2136. [Google Scholar] [CrossRef]
- FFQ. Available online: https://www.epic-norfolk.org.uk/about-epic-norfolk/nutritional-methods/ffq/ (accessed on 2 April 2025).
- Rothenberg, E.; Strandhagen, E.; Samuelsson, J.; Ahlner, F.; Rydberg Sterner, T.; Skoog, I.; Lundberg, C.E. Relative Validity of a Short 15-Item Food Frequency Questionnaire Measuring Dietary Quality, by the Diet History Method. Nutrients 2021, 13, 3754. [Google Scholar] [CrossRef]
- Mötteli, S.; Barbey, J.; Keller, C.; Bucher, T.; Siegrist, M. Measuring practical knowledge about balanced meals: Development and validation of the brief PKB-7 scale. Eur. J. Clin. Nutr. 2016, 70, 505–510. [Google Scholar] [CrossRef]
- BDA. The Model and Process. Available online: https://www.bda.uk.com/practice-and-education/nutrition-and-dietetic-practice/professional-guidance/model-and-process-for-dietetic-practice.html (accessed on 22 February 2023).
- Vitolins, M.Z.; Rand, C.S.; Rapp, S.R.; Ribisl, P.M.; Sevick, M.A. Measuring Adherence to Behavioral and Medical Interventions. Control. Clin. Trials 2000, 21 (Suppl. 1), S188–S194. [Google Scholar] [CrossRef]
- Profeta, A.; Baune, M.C.; Smetana, S.; Broucke, K.; Van Royen, G.; Weiss, J.; Heinz, V.; Terjung, N. Discrete Choice Analysis of Consumer Preferences for Meathybrids—Findings from Germany and Belgium. Foods 2020, 10, 71. [Google Scholar] [CrossRef] [PubMed]
- Graça, J.; Calheiros, M.M.; Oliveira, A. Attached to meat? (Un)Willingness and intentions to adopt a more plant-based diet. Appetite 2015, 95, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Graça, J.; Oliveira, A.; Calheiros, M.M. Meat, beyond the plate. Data-driven hypotheses for understanding consumer willingness to adopt a more plant-based diet. Appetite 2015, 90, 80–90. [Google Scholar] [CrossRef]
- Pliner, P.; Hobden, K. Development of a scale to measure the trait of food neophobia in humans. Appetite 1992, 19, 105–120. [Google Scholar] [CrossRef]
- Carrara, A.; Schulz, P.J. The role of health literacy in predicting adherence to nutritional recommendations: A systematic review. Patient Educ. Couns. 2018, 101, 16–24. [Google Scholar] [CrossRef]
- Burrows, T.; Teasdale, S.; Rocks, T.; Whatnall, M.; Schindlmayr, J.; Plain, J.; Latimer, G.; Roberton, M.; Harris, D.; Forsyth, A. Effectiveness of dietary interventions in mental health treatment: A rapid review of reviews. Nutr. Diet. 2022, 79, 279–290. [Google Scholar] [CrossRef] [PubMed]
- Kirkbride, J.B.; Anglin, D.M.; Colman, I.; Dykxhoorn, J.; Jones, P.B.; Patalay, P.; Pitman, A.; Soneson, E.; Steare, T.; Wright, T.; et al. The social determinants of mental health and disorder: Evidence, prevention and recommendations. World Psychiatry 2024, 23, 58–90. [Google Scholar] [CrossRef]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of healthcare interventions: An overview of reviews and development of a theoretical framework. BMC Health Serv. Res. 2017, 17, 88. [Google Scholar] [CrossRef]
- Klapp, A.L.; Wyma, N.; Alessandrini, R.; Ndinda, C.; Perez-Cueto, A.; Risius, A. Recommendations to address the shortfalls of the EAT–Lancet planetary health diet from a plant-forward perspective. Lancet Planet. Health 2025, 9, e23–e33. [Google Scholar] [CrossRef]
- Operational Framework for Monitoring Social Determinants of Health Equity. Available online: https://www.who.int/publications/i/item/9789240088320 (accessed on 26 March 2025).
- Valentin, G.; Maribo, T.; Nielsen, C.V.; Tonnesen, M.; Oestergaard, L.G. Bridging inequity gaps in healthcare through tailored support: Implementation perspectives of the Social Health Bridge-Building Programme. BMC Health Serv. Res. 2025, 25, 208. [Google Scholar] [CrossRef]
- Jiao, L. Social Determinants of Health, Diet, and Health Outcome. Nutrients 2024, 16, 3642. [Google Scholar] [CrossRef] [PubMed]
- Onwezen, M.C.; Bouwman, E.P.; Reinders, M.J.; Dagevos, H. A systematic review on consumer acceptance of alternative proteins: Pulses, algae, insects, plant-based meat alternatives, and cultured meat. Appetite 2021, 159, 105058. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.-J.; Kassam, S. Plants First Healthcare; Normalising Plant-Based Meals in Healthcare. 2024. Available online: https://blogs.bmj.com/bmjleader/2024/10/01/plants-first-healthcare-normalising-plant-based-meals-in-healthcare-by-dr-laura-jane-smith-and-dr-shireen-kassam/ (accessed on 16 January 2025).
- Saldivar, B.; Al-Turk, B.; Brown, M.; Aggarwal, M. Successful Incorporation of a Plant-Based Menu Into a Large Academic Hospital. Am. J. Lifestyle Med. 2021, 16, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Morgenstern, S.; Redwood, M.; Herby, A. An Innovative Program for Hospital Nutrition. Am. J. Lifestyle Med. 2024, 19, 320–323. [Google Scholar] [CrossRef]
- Roland. Hayek Hospital, The Very 1st Hospital in the World to Serve Exclusively Plant-Based Vegan Food!—Hayek Hospital. 2021. Available online: https://hayekhospital.org/2021/06/14/hayek-hospital-the-very-1st-hospital-in-the-world-to-serve-exclusively-plant-based-vegan-food/ (accessed on 26 January 2025).
- Tso, R.; Forde, C.G. Unintended Consequences: Nutritional Impact and Potential Pitfalls of Switching from Animal- to Plant-Based Foods. Nutrients 2021, 13, 2527. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid.-Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- Hotzy, F.; Risch, L.; Mötteli, S. Nutritional Needs in Mental Healthcare: Study Protocol of a Prospective Analytic Observational Study Assessing Nutritional Status, Eating Behavior and Barriers to Healthy Eating in Psychiatric Inpatients and Outpatients Compared to Healthy Adults. Front. Psychiatry 2022, 13, 906234. [Google Scholar] [CrossRef]
- Teasdale, S.B.; Ardill-Young, O.; Crawford, P.; Gould, P.; Hennessy, E.; Inall, B.; King, S.; Lancaster, R.; Millett, O.; Pearson, A.; et al. Feasibility of a targeted nutrition-risk screening tool in Australian mental health services: The NutriMental screener. Nutr. Diet. 2025. online version of record before inclusion in an issue. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.K.; Barron, C.T.; Chiu, Y.L.; Jang, S.H.; Touhid, S.; Bang, H. Weight changes and characteristics of patients associated with weight gain during inpatient psychiatric treatment. Issues Ment. Health Nurs. 2012, 33, 505–512. [Google Scholar] [CrossRef]
- Wang, P.S.; Wu, S.L.; Ching, H.Y. The use of psychiatric drugs and worsening body mass index among inpatients with schizophrenia. Int. Clin. Psychopharmacol. 2014, 29, 235–238. [Google Scholar] [CrossRef]
- Vieweg, W.V.; Thomas, M.; Janisko, M.; Booth, M.; Fernandez, A.; Pandurangi, A.; Silverman, J.J. Patient and direct-care staff body mass index in a state mental hospital: Implications for management. Acta Psychiatr. Scand. 2004, 110, 69–72. [Google Scholar] [CrossRef]
- Pedersen, A.L.W.; Gildberg, F.A.; Hjorth, P.; Højlund, M.; Andersen, K. Hospitalisation time is associated with weight gain in forensic mental health patients with schizophrenia or bipolar disorder. Nord. J. Psychiatry 2023, 77, 46–54. [Google Scholar] [CrossRef]
- Mills, S.; Kaner, E.F.S.; Ramsay, S.E.; McKinnon, I. What are the key influences and challenges around weight management faced by patients in UK adult secure mental health settings? A focused ethnographic approach. BMJ Open 2024, 14, e079406. [Google Scholar] [CrossRef]
- Megna, J.L.; Raj Kunwar, A.; Wade, M.J. A retrospective study of weight changes and the contributing factors in short term adult psychiatric inpatients. Ann. Clin. Psychiatry 2006, 18, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, G.E.; Gorczynski, P.F.; Cohn, T.A. Psychiatric illness and obesity: Recognizing the “obesogenic” nature of an inpatient psychiatric setting. Psychiatr. Serv. 2009, 60, 538–541. [Google Scholar] [CrossRef]
- Wierda, J.J.; de Vet, E.; Troost, E.; Poelman, M.P. Characterizing food environments of hospitals and long-term care facilities in the Netherlands: A mixed methods approach. BMC Health Serv. Res. 2024, 24, 31. [Google Scholar] [CrossRef]
- Cook, N.; Collins, J.; Porter, J.; Goodwin, D. Applying the theoretical domains framework and behavior change wheel to inform interventions for food and food-related waste audits in hospital foodservices. Front. Nutr. 2023, 10, 1204980. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.D.; Pitts, S.J.; Onufrak, S.J.; Sirois, E.; Utech, A.; Wood, M.; Silverman, J.; Ajenikoko, F.; Murphy, M.; Warnock, A.L. A qualitative exploration of barriers, facilitators and best practices for implementing environmental sustainability standards and reducing food waste in veterans affairs hospitals. J. Hum. Nutr. Diet. 2024, 37, 1420–1431. [Google Scholar] [CrossRef]
- Liwinski, T.; Bocek, I.; Schmidt, A.; Kowalinski, E.; Dechent, F.; Rabenschlag, F.; Moeller, J.; Sarlon, J.; Brühl, A.B.; Nienaber, A.; et al. Sustainability initiatives in inpatient psychiatry: Tackling food waste. Front. Psychiatry 2024, 15, 1374788. [Google Scholar] [CrossRef]
- Miller, C.; Taylor, J.; Tong, R.; Thompson, S.; Thomson, E.; Robertson, A.; Bishara, R. Something to Chew on; Plate-Waste at an Ontario Veteran’s Centre. Can. J. Diet. Pract. Res. 2024, 85, 106–110. [Google Scholar] [CrossRef]
- Wilson, E.D.; Garcia, A.C. “Going green” in food services: Can health care adopt environmentally friendly practices? Can. J. Diet. Pract. Res. 2011, 72, 43–47. [Google Scholar] [CrossRef]
- Wilson, E.D.; Garcia, A.C. Environmentally friendly health care food services: A survey of beliefs, behaviours, and attitudes. Can. J. Diet. Pract. Res. 2011, 72, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Meis-Harris, J.; Rramani-Dervishi, Q.; Seffen, A.E.; Dohle, S. Food for future: The impact of menu design on vegetarian food choice and menu satisfaction in a hypothetical hospital setting. J. Environ. Psychol. 2024, 97, 102348. [Google Scholar] [CrossRef]
- Beavan, S.; Baker, R.; Sadler, H.; Collinson, A. Improving the nutritional intake of hospital patients: How far have we come? A re-audit. J. Hum. Nutr. Diet. 2019, 32, 372–384. [Google Scholar] [CrossRef]
- Moody, S.C. Enhancing food sustainability in the acute hospital setting—A nurse-led study of patient food. Br. J. Nurs. 2024, 33, S8–S17. [Google Scholar] [CrossRef]
- Rogers, E.; Papathomas, A.; Kinnafick, F.E. Inpatient perspectives on physical activity in a secure mental health setting. Psychol. Sport Exerc. 2021, 52, 101827. [Google Scholar] [CrossRef]
- McKenna, C.; Moyo, B.; Goodwin, J. Barriers to using physical exercise as an intervention within inpatient mental health settings: A systematic review. Int. J. Ment. Health Nurs. 2024, 33, 817–833. [Google Scholar] [CrossRef]
- Giles, E.L.; Becker, F.; Ternent, L.; Sniehotta, F.F.; McColl, E.; Adams, J. Acceptability of Financial Incentives for Health Behaviours: A Discrete Choice Experiment. PLoS ONE 2016, 11, e0157403. [Google Scholar] [CrossRef]
- Lancsar, E.; Louviere, J. Conducting discrete choice experiments to inform healthcare decision making: A user’s guide. Pharmacoeconomics 2008, 26, 661–677. [Google Scholar] [CrossRef]
- Ryan, M.; Gerard, K. Using discrete choice experiments to value health care programmes: Current practice and future research reflections. Appl. Health Econ. Health Policy 2003, 2, 55–64. [Google Scholar] [PubMed]
- Ryan, M.; Gerard, K.; Amaya-Amaya, M. (Eds.) Using Discrete Choice Experiments to Value Health and Health Care; The Economics of Non-Market Goods and Resources (Bateman, I.J., Ed.); Springer: Dordrecht, The Netherlands, 2008; Volume 11, Available online: http://link.springer.com/10.1007/978-1-4020-5753-3 (accessed on 3 March 2025).
- Timlin, D.; McCormack, J.M.; Simpson, E.E. Using the COM-B model to identify barriers and facilitators towards adoption of a diet associated with cognitive function (MIND diet). Public Health Nutr. 2021, 24, 1657–1670. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef]
- West, R.; Michie, S. A Brief Introduction to the COM-B Model of Behaviour and the PRIME Theory of Motivation. Qeios. 7 April 2020. Available online: https://www.qeios.com/read/WW04E6 (accessed on 30 January 2025).
- Roberts, S.; Hopper, Z.; Chaboyer, W.; Gonzalez, R.; Banks, M.; Desbrow, B.; Marshall, A.P. Engaging hospitalised patients in their nutrition care using technology: Development of the NUTRI-TEC intervention. BMC Health Serv. Res. 2020, 20, 148. [Google Scholar] [CrossRef]
- Bischof, G.; Bischof, A.; Rumpf, H.J. Motivational Interviewing: An Evidence-Based Approach for Use in Medical Practice. Dtsch. Arztebl. Int. 2021, 118, 109–115. [Google Scholar] [CrossRef]
- Rigby, R.R.; Mitchell, L.J.; Hamilton, K.; Williams, L.T. The Use of Behavior Change Theories in Dietetics Practice in Primary Health Care: A Systematic Review of Randomized Controlled Trials. J. Acad. Nutr. Diet. 2020, 120, 1172–1197. [Google Scholar] [CrossRef]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.; Craig, N.; French, D.; McIntosh, E.; et al. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef] [PubMed]
- Spanakis, P.; Wadman, R.; Walker, L.; Heron, P.; Mathers, A.; Baker, J.; Johnston, G.; Gilbody, S.; Peckham, E. Measuring the digital divide among people with severe mental ill health using the essential digital skills framework. Perspect. Public Health 2024, 144, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.A.; Blease, C.; Faurholt-Jepsen, M.; Firth, J.; Van Daele, T.; Moreno, C.; Carlbring, P.; Ebner-Priemer, U.W.; Koutsouleris, N.; Riper, H.; et al. Digital mental health: Challenges and next steps. BMJ Ment. Health 2023, 26, e300670. [Google Scholar] [CrossRef]
- Stein, O.A.; Prost, A. Exploring the societal implications of digital mental health technologies: A critical review. SSM—Ment. Health 2024, 6, 100373. [Google Scholar] [CrossRef]
- Jameel, L.; Valmaggia, L.; Barnes, G.; Cella, M. mHealth technology to assess, monitor and treat daily functioning difficulties in people with severe mental illness: A systematic review. J. Psychiatr. Res. 2021, 145, 35–49. [Google Scholar] [CrossRef]
- Carpenter-Song, E.; Noel, V.A.; Acquilano, S.C.; Drake, R.E. Real-World Technology Use Among People With Mental Illnesses: Qualitative Study. JMIR Ment. Health 2018, 5, e10652. [Google Scholar] [CrossRef]
- GOV.UK. Independent Review of NHS Hospital Food. Available online: https://www.gov.uk/government/publications/independent-review-of-nhs-hospital-food (accessed on 16 January 2025).
- Holt, R.I.G.; Mitchell, A.J. Diabetes mellitus and severe mental illness: Mechanisms and clinical implications. Nat. Rev. Endocrinol. 2015, 11, 79–89. [Google Scholar] [CrossRef]
- NYC Health + Hospitals. NYC Health + Hospitals Celebrates 1.2 Million Plant-Based Meals Served. Available online: https://www.nychealthandhospitals.org/pressrelease/nyc-health-hospitals-celebrates-1-2-million-plant-based-meals-served/ (accessed on 16 January 2025).
- Berardy, A.J.; Rubín-García, M.; Sabaté, J. A Scoping Review of the Environmental Impacts and Nutrient Composition of Plant-Based Milks. Adv. Nutr. 2022, 13, 2559–2572. [Google Scholar] [CrossRef]
- Sadler, I.; Bauer, A.; Kassam, S. How Sustainable Are Hospital Menus in the United Kingdom? Identifying Untapped Potential Based on a Novel Scoring System for Plant-Based Provisions. J. Hum. Nutr. Diet. 2025, 38, e70019. [Google Scholar] [CrossRef]
- Risch, L.; Hotzy, F.; Vetter, S.; Hiller, S.; Wallimann, K.; Seifritz, E.; Mötteli, S. Assessment of Nutritional Status and Risk of Malnutrition Using Adapted Standard Tools in Patients with Mental Illness and in Need of Intensive Psychiatric Treatment. Int. J. Environ. Res. Public Health 2022, 20, 109. [Google Scholar] [CrossRef]
- Abayomi, J.; Hackett, A. Assessment of malnutrition in mental health clients: Nurses’ judgement vs. a nutrition risk tool. J. Adv. Nurs. 2004, 45, 430–437. [Google Scholar] [CrossRef] [PubMed]
- NHS England. Recipe Bank. Available online: https://foodplatform.england.nhs.uk/ (accessed on 19 February 2025).
- Greig, S.; Hekmat, S.; Garcia, A.C. Current Practices and Priority Issues Regarding Nutritional Assessment and Patient Satisfaction with Hospital Menus. Can. J. Diet. Pract. Res. 2018, 79, 48–54. [Google Scholar] [CrossRef]
- Brumbaugh, J.E.; Tschida-Reuter, D.J.; Barwise, A.K. Meeting the needs of the patient with non-English language preference in the hospital setting. Health Serv. Res. 2023, 58, 965–969. [Google Scholar] [CrossRef] [PubMed]
- Waterall, J.; Newland, R.; Campos-Matos, I.; Stannard, J. What is inclusion health and why is it important for all nurses and midwives? Br. J. Nurs. 2021, 30, 866–867. [Google Scholar] [CrossRef]
- Issa, R.; Forbes, C.; Baker, C.; Morgan, M.; Womersley, K.; Klaber, B.; Mulcahy, E.; Stancliffe, R. Sustainability is critical for future proofing the NHS. BMJ 2024, 385, e079259. [Google Scholar] [CrossRef] [PubMed]
- May, C.R.; Cummings, A.; Girling, M.; Bracher, M.; Mair, F.S.; May, C.M.; Murray, E.; Myall, M.; Rapley, T.; Finch, T. Using Normalization Process Theory in feasibility studies and process evaluations of complex healthcare interventions: A systematic review. Implement. Sci. 2018, 13, 80. [Google Scholar] [CrossRef]
- May, C.R.; Albers, B.; Bracher, M.; Finch, T.L.; Gilbert, A.; Girling, M.; Greenwood, K.; MacFarlane, A.; Mair, F.S.; May, C.M.; et al. Translational framework for implementation evaluation and research: A normalisation process theory coding manual for qualitative research and instrument development. Implement. Sci. 2022, 17, 19. [Google Scholar] [CrossRef]
- Johnson, M.J.; May, C.R. Promoting professional behaviour change in healthcare: What interventions work, and why? A theory-led overview of systematic reviews. BMJ Open 2015, 5, e008592. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Reardon, C.M.; Widerquist, M.A.O.; Lowery, J. The updated Consolidated Framework for Implementation Research based on user feedback. Implement. Sci. 2022, 17, 75. [Google Scholar] [CrossRef]
- King, D.K.; Shoup, J.A.; Raebel, M.A.; Anderson, C.B.; Wagner, N.M.; Ritzwoller, D.P.; Bender, B.G. Planning for Implementation Success Using RE-AIM and CFIR Frameworks: A Qualitative Study. Front. Public Health 2020, 8, 59. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Area of Interest | Primary Outcome Measure | Measurement/Instrument |
|---|---|---|
| Changing body habitus on admission to a mental health hospital—nutritional status | Anthropometry
Secondary measures
Biochemistry
Clinical–diagnosis
Dietary
Environment
|
|
| Exploring food waste in mental health hospitals | Food and food waste
|
|
| Knowledge and training needs of stakeholders for a plant-based diet to be implemented | Knowledge and skills
|
|
| Initial Coding (n = 68) | Sub-Categories (n = 12) | Overarching Themes/Categories (n = 5) |
|---|---|---|
| Inadequacy of catered hospital food Food consumption—unmonitored Portion sizes too small or too big Vending machines—source of high calorie drinks/snacks Water policy—health and safety Health promotion—healthy snacks, lower cost Limited choice of healthy options Buffet style—overeating, unhealthy choices Hoarding—milk, creamers, sugar Control over food—acting out Patients’ right to choose—wider choice Purchasing food close to hospital—lack of healthy options—takeaways Few opportunities to engage in physical activity Healthcare professionals (HCPs)’ respect for patient autonomy Staff dissatisfaction with catering HCPs not wishing to restrict choices of takeout food, portion sizes, number of servings at mealtimes, or purchases from food carts or vending machines HCPs not wishing to stop patients from eating food from other patients’ untouched trays Ward culture—not conducive to healthy eating Eating in silence and at speed—no social engagement Eating together—staff and patients Rule breaking around food—variation in staff practice Healthcare settings (acute vs. mental health) shaping the socio-cultural environment Policies and procedures—top-down | Physical food environment Political food environment Ward culture | Food and socio-cultural environment |
| Reduced portion sizes Selling surplus foods Collaboration with nutritionists Cook-to-order Regular monitoring Sustainable sourcing | Sustainability initiatives Communication with staff and patients | Evidence-based sustainable food practices |
| Environmental impact Evidence-based measures Ecological footprint of food waste Segregating food waste Weighing food Food waste—carbon footprint—carbon dioxide equivalent emissions per kg (CO2e/kg) Food waste water footprint—(i.e., total volume of freshwater use per kg of produced food waste (L/kg)) Food waste quantification Fish, meat, and protein—highest CO2e/kg Vegetables, salad, and fruits—highest water footprint (L/kg) Preparation method (i.e., bulk, cook–chill, plated) Food appearance and delivery method Reduced food waste High burden of food waste in forensic psychiatry, addictive disorders, and psychotic disorders Visual estimation of consumption/food waste Portion size (i.e., meal vs. snack) Meal occasion—greatest waste (e.g., lunch, afternoon snack) Healthy vs. unhealthy Dislike of vegetables | Quality and type of food Food waste | Economic food environment |
| Body habitus Lower or normal body weight on hospital admission—associated with greater weight gain Diagnosis-associated weight gain—anti-psychotics Smokers Male vs. female Age at onset Duration of illness Inactivity—low levels of physical activity Co-morbidity—type 2 diabetes, heart disease, hypertension Length of hospital stay Staff who are obese | Factors associated with weight gain Perceptions around weight gain | Inevitability of weight gain |
| Knowledge, skills Environmental context and resource Social, professional role and identity, beliefs about capabilities Education Training Environmental restructuring Modelling Enablement | Knowledge and training Physical opportunity Ability to change | Theoretical model for behaviour change |
| Author, Country | Title | Aim | Demo-Graphics Mean ± Standard Deviation | Methods | Findings | Outcome Measures | Food Environment | Food Waste | Summary |
|---|---|---|---|---|---|---|---|---|---|
| Cook C et al. Australia, 2023 [124] | Applying the theoretical domains framework and behaviour change wheel to inform interventions for food and food related waste audits in hospital food services. | The aim of this study was to use behaviour change theories and frameworks to (1) describe the drivers of behaviour to complete food and food-related waste audits and (2) identify possible interventions that support the implementation and uptake of these audits. | n = 20 particiapnts (60% female, mean age 44 years) from nine hospitals. Food service dietitians (n = 4), hotel service coordinators (n = 2), project coordinators (n = 2). Manager/supervisor roles including: support services (n = 1), catering (n = 1), facilities services (n = 1), food safety (n = 1), dietetics (n = 1), and sustainability (n = 1). Hospital sizes ranged from 18 to 600 beds—the most common food service type was cook–chill. | Qualitative interviews of food service staff working in a variety of hospital settings, including mental health hospitals. | Twenty interviews. Participants reported food service staff’s lack of knowledge, labour, and time, and hospitals avoiding the need to complete audits. Interventions which may have the greatest impact around the implementation of waste audits were education, training, environmental restructuring, modelling and enablement. Suggested enablers were obtaining staff buy-in, reinforcing behaviour through incentives, and establishing audit champions. | Dominant COM-B constructs (theoretical domains framework) (1) psychological capability (knowledge, skills), (2) physical opportunity (environmental context and resources), (3) reflective motivation (social/professional role and identity beliefs about capabilities). | Food waste audits require education, training, and environmental restructuring. | Using a behaviour change model may be beneficial for waste audits implementation strategies, including staff education, training, and environmental restructuring. | |
| Faulkner G et al. United States, 2009 [122] | Psychiatric illness and obesity: recognizing the “obesogenic” nature of an inpatient psychiatric setting. | The aim of this study was to examine environmental factors contributing to obesity in one psychiatric hospital in Canada. | A total of 25 stakeholders including: recreation therapists (n = 5), registered nurses (n = 4), food service dietitian (n = 3), clinical dietitians (n = 3), psychiatrists (n = 3), schizophrenic program administrators (n = 2), patient service staff member (n = 1), general physician (n = 1), site redevelopment advisor (n = 1), housing member (n = 1), occupational therapist (n = 1) | Semi-structured interviews were conducted with 25 key stakeholders from multiple professional disciplines at the hospital. | Factors contributing to obesity in this setting were related to increased energy intake, such as easy access to high-calorie snacks and beverages and reduced energy expenditure, and lack of access to spaces to engage in physical activity. | BMI, food knowledge, and skills | Easy access to high-calorie foods and reduced levels of physical activity led to an obesogenic environment. | Psychiatric settings may contribute to the high prevalence of obesity among individuals with psychiatric illness, and interventions considering environmental factors within an inpatient environment are required. | |
| Liwinski T et al. Switzerland, 2024 [126] | Sustainability initiatives in inpatient psychiatry: tackling food waste. | The aim of this paper was to explore sustainability initiatives within an inpatient psychiatric hospital. | Inpatient facility with n = 277 beds; 3-year interventional study. Study partipants: healthcare administrators, facility managers, and policy makers as people overlooked in discussions of food waste within healthcare facilities. | Systematic food wastage audits were completed over three years (2020–2022) in May and June, for a four-week period. These audits collected costs associated with food, staff, infrastructure, and disposal. Environmental impact was assessed using environmental impact points and CO2e/kg emissions, alongside water usage L/kg. | Economic losses due to food wastage were substantial, primarily from untouched plates and partially consumed dinners, prompting meal planning adjustments. Despite a >3% increase in meals served, both food waste mass and costs decreased by nearly 6%. Environmental impact indicators showed a reduction > 20%. Vegetables, salad, and fruits constituted a significant portion of waste. Overproduction minimally contributed to waste, validating portion control efficacy. This study highlights significant economic and environmental losses due to hospital food waste, emphasizing the importance of resource efficiency. The strategies outlined offer promising avenues for enhanced efficiency. The decrease in food waste observed over the three-year period underscores the potential for improvement. | Food wastage—categories: (1) vegetables, salads, fruit, (2) soups and sauces, (3) fish, meat and protein, (4) bread and bakery, (5) milk & dairy, (6) desserts | High economic losses arose from untouched meals. Evidence-based strategies to minimise food waste included (i) communication, (ii) sustainable sourcing of food, (iii) feedback mechanisms for staff and patients to iterate meals, (iv) regular food-waste audits, (v) kitchen staff training, (vi) cook-to-order, (vii) collaboration with nutritionists, (viii) selling surplus food to staff at low cost, and (ix) reduced portion sizes. | This study reports high economic and environmental loss arising from hospital food waste. Quality improvement strategies demonstrated reductions in food waste and increased satisfaction with catering services. | |
| Megna et al. USA, 2006 [121] | A retrospective study of weight changes and the contributing factors in short term adult psychiatric inpatients | The aim of this study was to explore factors associated with significant weight gain during acute psychiatric inpatient hospitalization for adults. | Patient characteristics: Patients n = 96 Sex: 56% male Age: 39.5 ± 15.3 years Baseline BMI: 28.2 ± 7.5 Discharge BMI: 28.8 ± 7.2 Length of stay: 17.2 ± 18.2 | A retrospective chart review of all patients admitted to the psychiatric inpatient unit. | In total, 535 charts were reviewed, and 96 patients met the inclusion criteria. Individuals with diagnoses of bipolar disorder and schizophrenia gained more weight compared with those diagnosed with major depressive disorder. Those prescribed atypical antipsychotics gained more weight compared with those who were not prescribed such medications. Smokers gained more weight than nonsmokers, and males gained more than females. There was an inverse relationship with weight at the time of the admission and the strongest predictors of weight gain. | Length of stay, medications, Psychiatric diagnosis DSM-IV, BMI at admission/discharge, nutrition-related diseases | Following admission patients on average gained 1.8 +/− 6.0 kg. (p = 0.005). Individuals with a lower body weight at admissions were associated with more weight gain. | Patients with a diagnosis of bipolar disorder and schizophrenia prescribed atypical antipsychotics and overweight at the time of admission may be at risk of greater weight gain during admission. | |
| Miller C et al. Canada, 2024 [127] | Something to Chew on: Plate Waste at an Ontario Veteran’s Centre. | The aim of this study was to explore food waste within a long-term mental health facility. | Patient characteristics n = 165 residents receiving tray service Patients n = 33 Sex: 94% male Age: 95.6 ± 6.9 years Diet type: No texture/therapeutic modifications 18% (n = 6) Texture modified only 45% (n = 15) Therapeutic modified ony 12% (n = 4) Texture and therapeutic modification 24% (n = 8) | A 3-day waste-audit of food/beverage items provided explored factors associated with food waste. | In total, 28% of items served to individuals were wasted. Lunch was the meal with the greatest waste at 31% and waste of solid items was 12% higher than that of liquids. There was a large variability in waste between and within individuals, with 15% of residents wasting more than >50% of items provided. | Meal occasion -food waste: vegetable, carbohydrate and protein food | Food waste audits reported that lunch was the meal associated with the greatest waste, although there was a high variability in waste between individuals. | This study proposes individualized strategies to address waste. | |
| Mills S et al. England, 2024 [120] | What are the key influences and challenges around weight management faced by patients in UK adult secure mental health settings? A focused ethnographic approach. | The aim of this study was to identify the key influences and challenges around weight management in UK adult secure mental health settings. | Patient characteristics Patients n = 12 Sex: 100% (n = 12) males Ethnicity: white Age: range 25–50 years 22 staff employed on the ward (sex, age, ethnicity not recorded) | Qualitative focused ethnography of 12 male patients within a low secure male mental health ward. | Within this study, key themes highlighted included (i) the increased importance of food in secure settings, (ii) the inadequacy of catered hospital food and shortcomings of alternative food options, limited physical activity opportunities, and (iv) a ward culture that did not support healthy behaviours. | Weight management | The environment within secure mental healthcare is obesogenic, increasing the risk of excessive weight gain and sedentary behaviour in patients. Excess weight gain is often perceived as inevitable. | Weight management within mental health services is a complex challenge. Whole setting-based interventions involving staff and patients are required to promote a culture of promoting weight management. The maintenance of a healthy weight should integrate physical and mental health strategies with sufficient staffing. | |
| Mötteli et al. Switzerland, 2023 [85] | Examining Nutrition Knowledge, Skills, and Eating Behaviours in People with Severe Mental Illness: A Cross-Sectional Comparison among Psychiatric Inpatients, Outpatients, and Healthy Adults | The aim of this study was to explore eating behaviours, dietary habits, and motivation for healthy eating among psychiatric inpatients and outpatients with severe mental illness. | Patient charaterstics: In patients: n = 65 Outpatients: n = 67 Healthy controls: n = 64 Age: 38.7 ± 11.9 years Inpatients BMI 25.3 ± 5 Outpatients BMI 27.9 ± 5.3 Healthy control BMI 24.0 ± 3.7 | This prospective, cross-sectional study was based on semi-structured interview data and anthropometric measurements from people with severe mental illness treated at a psychiatric hospital including both inpatient (acute wards) and outpatient (day clinic) settings. | In total, 65 inpatients, 67 outpatients, and 64 healthy controls were included in the study. The psychiatric patients had a higher BMI and waist-to-hip ratio and had an increased incidence of nutrition-related diseases and food intolerances versus healthy controls. Most patients with severe mental illness had experienced weight changes in the previous three to six months, whereas the healthy controls had more stable weights. Psychiatric patients were also less likely to engage in healthy behaviours such as physical activity and not smoking. | Mental health assessed: nine-item symptom checklist (SCL-K-9), nine-item patient health questionnaire, obesogenic medication, BMI, waist to hip ratio, abdominal girth, hip girth, changes in weight over time, nutrition-related diseases, nutrition counselling | Inpatients with severe mental illness were more likely to be overweight and have diabetes. They were also more likely to experience disordered eating habits and have unhealthy lifestyles. | Nutrition, knowledge, cooking, and food skills did not appear to be important barriers although they may be prerequisites for healthy eating. Inpatients with severe mental illness would benefit from nutritional support that aims at improving their daily structure and social inclusion, using behavioural approaches related to meal planning and social eating. | |
| Pederson et al. Denmark, 2022 [119] | Hospitalisation time is associated with weight gain in forensic mental health patients with schizophrenia or bipolar disorder | The aim of this study was to explore body habitus amongst inpatients within forensic mental health inpatients. | Patient characteristics: Patients n = 490 Sex: males 81.6% (n = 400) Age: 40.4 ± 13.0 years Patients included with body habitus measures (n = 328) Baseline: ≤18.5: (n = 9) ≥18.5 and ≤25 (n = 113) ≥25 and ≤30 (n = 89) ≥30 (n = 112) | A retrospective cohort study including forensic mental health patients with schizophrenia or bipolar disorder. Patient characteristics and data on body weight were extracted from electronic medical records. The association between duration of hospital stay and weight change per year was analysed using linear regression. Proportional hospital duration was determined between each measurement as the total number of days hospitalized divided by the total number of days. Analyses were adjusted for gender, age, smoking, and antipsychotic medication. | In total, 328 forensic mental health patients were included, of which 91% were diagnosed with schizophrenia. Compared with outpatients, inpatients underweight at the point of admission had the largest difference in weight gain (+18.0 kg/year, p = 0.006), and the weight gain difference was smallest in patients who were obese (+2.3 kg/year, p = 0.21) at the point of admission. | Changes in weight, BMI, Biochemistry: estimated average glucose, lipid profile, Psychiatric diagnosis ICD-10, obesogenic medication, biochemistry | The duration of hospital stay in forensic mental health wards was associated the with greater weight gain. | Duration of length of hospital stay was associated with an estimated difference of +4.0 kg/year for forensic mental health inpatients, compared with individuals managed within an outpatient setting. | |
| Shin J et al. England, 2012 [116] | Weight changes and characteristics of patients associated with weight gain during inpatient psychiatric treatment. | The aim of this study was to investigate weight changes of patients in a public psychiatric hospital. | Patient characteristics: Patients n = 400 Sex: females 41% (n = 164) Age: 43.6 ± 14.9 years Ethnicity: White 25% Black 25% Non-black Latino 25% Asian 25% Baseline BMI: 27.6 ± 6.3 Discharge BMI: 28.5 ± 6.2 | A retrospective chart review of weight changes during an inpatient admission was conducted on a multi-racial population admitted for psychiatric inpatient treatment. | In total, 400 patient records were included, with 59% males and an average BMI of 27.6 ± 6.3 on admission. Patients gained an average of 2.45 kg during psychiatric hospitalization. Patients with normal weight at admission were significantly more likely to gain weight compared with overweight or obese patients. Black patients showed the greatest weight gain, while Asian patients showed the least weight gain. | Anthropometry: BMI changes from admission to discharge; Clinical: DSM-IV, obseogenic medication; Dietary adherence, nutrition-related diseases Environment: physical activity | Patients with normal weight at the point of admission were significantly more likely to gain weight compared to overweight or obese patients. | Patients were likely to gain weight during inpatient admission. | |
| Vieweg W et al. United States, 2004 [118] | Patient and direct-care staff body mass index in a state mental hospital: implications for management. | The aim of this study was to explore the body habitus amongst inpatients within a mental health hospital. | Patient characteristics: Patients n = 95 Sex: men 77% (n = 73) Age: men 37.2 ± 10.5 years; average length of stay: 5.4 ± 6.2 years Age: women 39.5 ± 12.5 years; average length of stay: 5.0 ± 6.2 years Basline BMI: 26.4 ± 5.8 Follow up BMI: 29.1 ± 5.8 Staff characteristics Staff n = 97 Sex: 91% (n = 89) Age: 45.9 ± 11.9 years Staff BMI: 29.1 ± 5.8 | BMI of chronically psychotic patients on admission to a mental hospital and in follow-up, along with staff BMI. | At admission, patient BMI (26.4 +/− 5.8 kg/m2) was in the overweight range. Patients’ BMI (29.1 +/− 5.8 kg/m2) significantly increased (p < 0.0001) to the level of obesity on follow-up. Staff BMI (35.1 +/− 8.6 kg/m2) was in the obese range, with 65% meeting criteria of obesity and 30% meeting criteria of morbid obesity. African American women made up 85% of clinical-care staff and constitute the race-sex mix most vulnerable to obesity in the USA. Morbid obesity (BMI > or =40 kg/m2) was five times more common among these African American female clinical care staff than among African American women in the general US population. These findings may have treatment implications for chronically psychotic patients at risk for obesity. | Anthropometry: BMI changes from admission to discharge; BMI of staff; Clinical: obesogenic medication | Patients gained a significant amount of weight on admission. Most of the clinical staff working on the wards had excess weight. | Patients experienced significant weight gain following hospital admission. Weight gain may be exacerbated further by a culture that normalises excess weight. | |
| Wang P et al. England, 2014 [117] | The use of psychiatric drugs and worsening body mass index among inpatients with schizophrenia. | The aim of this study was to investigate the relationship between psychotropic agents and overweight to obese inpatients with schizophrenia. | Patient charatersistics Patients n = 138 Sex: men 60.9% (n = 84) Average length of stay: 4.5 ± 3.0 years | Retrospective chart review. | A total of 138 patients with schizophrenia were recruited in this retrospective study comparing characteristics of those who gained weight from overweight to obesity (n = 23) compared with those who did not (n = 115). Of the 138 patients, 60.9% were men. Mean age of patients 47.2 ± 9.7 years, mean age of onset of disease 32.2 ± 10.4 years, mean length of illness 15.0 ± 6.5 years. Valproic acid was found to have a significant impact on the worsening of BMI from overweight to obesity (p < 0.05). Age at onset of disease, length of illness, and duration of hospitalization were not significantly associated with worsening of BMI from overweight to obesity. | Anthropometry: BMI duration of disease, length of hospital stay, Clinical: obesogenic medication | Valproic acid in patients with schizophrenia was associated with increased weight gain. | Psychotropic medication in individuals with severe mental illness is associated with significant weight gain. | |
| Wierda J et al. The Netherlands, 2024 [123] | Characterizing food environments of hospitals and long-term care facilities in the Netherlands: a mixed methods approach. | The aim of this study was to characterize the physical, socio-cultural, political, and economic dimensions of the food environment for staff, patients, and visitors within long-term mental health care facilities. | Semi structured interviews: Staff members (n = 46) Interviewees represented: hospitals (n = 11), nursing homes (n = 6), rehabiliation centres (n = 6), people with intelectual disability(n = 6), mental healthcare institutions (n = 9) | Semi-structured interviews were held with staff members (n = 46) representing 11 hospitals and 26 long-term care facilities (rehabilitation centres, nursing homes, institutions for people with intellectual disabilities and mental healthcare institutions). In sub-study 2, staff members audited the food environment in hospitals (n = 28) and long-term care facilities (n = 36) using a predefined checklist. | The type of healthcare shaped the socio-cultural food environment, with acute hospitals emphasising nutrition for fast recovery, and long-term care facilities using food more of an instrument to structure the day. Study participants highlighted the importance of organisational and food policies for regulating and improving the food environment. Economic aspects associated with food budgets and contracts with external providers affected the food in all healthcare settings. | Food environments | Sustainability and healthiness should be prioritised. | Research in the future should investigate the underlying mechanisms of the healthcare environment for staff, visitors, and patients whilst prioritising sustainability alongside healthiness. | |
| Williams B et al. USA, 2024 [125] | A qualitative exploration of barriers, facilitators and best practices for implementing environmental sustainability standards and reducing food waste in veterans’ affairs hospitals. | The aim of this study was to explore barriers, facilitators, and best practices for implementing environmental sustainability standards in food service in mental health hospitals. | Staff characteristics Staff role: food service director Experience: 6.3 years (range 0.5–21 years) Experience of sustainable practice: 5 years (range 0–12 years). 80% of food purchased from approved vendors | Online survey with hospital food service directors and qualitative interviews. The survey assessed self-reported motivators around five standards with regards to initiating sustainability standards and implementation, (i) increasing plant-forward dishes, (ii) procuring and serving sustainable foods that meet organic/fair trade and other certifications, (iii) procuring and serving locally produced foods, (iv) reducing food waste, and (v) reducing energy consumption. | The top three motivators cited were (i) reducing food waste, (ii) serving healthier foods, and (iii) increasing efficiency or cost savings. Barriers were reported including (i) patient preferences, (ii) contractual difficulties, and (iii) costs related to reducing waste. Facilitators included (i) taste-testing new recipes that include more sustainable food options and (ii) easy access to sustainable products from the main supplier. Best practices included (i) making familiar dishes plant-forward and (ii) plate waste studies to prevent overproduction. | Feelings towards nutrition | Food waste audits are central to better understanding which dishes need to be changed, and where overproduction may be contributing to food waste. | Although there were many barriers to implementation, directors of food service offered solutions for overcoming challenges and implementing food service sustainability standards, many of which included involving staff, visitors, and patients with regards to taste-testing familiar dishes made with plant-based alternatives. | |
| Wilson E et al. Canada. 2011 [128] | Going green in food services: Can health care adopt environmentally friendly practices? | The aim of this study was to examine reported environmentally friendly practices being implemented in the food service industry and consider ways in which health care or hospital food services can adopt some of these programs. | None to report | A review article | Suggestions are made for small changes to start the green initiative in each of these areas. A health care food service department is a large consumer of resources, and therefore, food service workers, managers, dietitians, and administrators can make a significant difference by supporting and adopting environmentally friendly practices. | None to report | Knowledge mobilisation with regards to small changes towards sustainable practices. | Further studies are needed to determine which practices are currently being implemented in health care facilities, as well as perceived facilitators and barriers to these practices in the food service area. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marino, L.V.; Meyer, R.; Veale, S.; Brown, J.V.E. Scoping Review: Environmental Factors Influencing Food Intake in Mental Health Inpatient Settings. Dietetics 2025, 4, 18. https://doi.org/10.3390/dietetics4020018
Marino LV, Meyer R, Veale S, Brown JVE. Scoping Review: Environmental Factors Influencing Food Intake in Mental Health Inpatient Settings. Dietetics. 2025; 4(2):18. https://doi.org/10.3390/dietetics4020018
Chicago/Turabian StyleMarino, Luise V., Rosan Meyer, Sarah Veale, and Jennifer V. E. Brown. 2025. "Scoping Review: Environmental Factors Influencing Food Intake in Mental Health Inpatient Settings" Dietetics 4, no. 2: 18. https://doi.org/10.3390/dietetics4020018
APA StyleMarino, L. V., Meyer, R., Veale, S., & Brown, J. V. E. (2025). Scoping Review: Environmental Factors Influencing Food Intake in Mental Health Inpatient Settings. Dietetics, 4(2), 18. https://doi.org/10.3390/dietetics4020018