1. Introduction
Duchenne muscular dystrophy (DMD) is the most common and severe neuromuscular disease affecting approximately 1 in 3500 persons worldwide. This incurable X-linked recessive disorder is caused by the mutation in the dystrophin gene leading to the impaired production or function of dystrophin protein, which in turn leads to progressive muscle weakness. Boys with DMD in the second decade of life lose ambulation then the ability to stand or change position. The milestones in the disease progression are: lack of ambulation, loss of ability to use upper limbs, gastrointestinal problems resulting in malnutrition, heart failure, and respiratory insufficiency [
1,
2].
Historically, the cardiorespiratory system failure caused death before 18 years of age. Nowadays, there is still no cure for DMD, but the appropriate treatment and medical multidisciplinary care can improve the quality of life of those patients and extend their life expectancy to more than 30 years of age [
2].
The assessment and treatment of the respiratory system are the most important problems for DMD patients. The progression of the disease and muscle weakness lead to progressive scoliosis. Massive deformity raises the risk of cardiopulmonary dysfunction [
2]. The first signs of respiratory failure are obstructive sleep apnoea (OSA), which causes chronic headaches, daytime drowsiness, episodes of distraction, and difficulty falling asleep and waking up. Adult DMD patients, especially with FVC < 60% with a weak cough and airway clearance, are at a high risk of severe respiratory infections [
3,
4].
The pandemic has impacted healthcare systems in the entire world. Due to the fact that DMD patients are at risk of a severe course of COVID-19 [
5], the multidisciplinary healthcare team is seeking the safest way to provide constant care and treatment at the highest possible level. The innovative digital form of physical therapy, which is easily available, free of charge, and adjustable can support the daily routine of home training in the time of social distancing [
6].
The purpose of the study was to investigate whether it is possible to conduct respiratory physical therapy with the use of telerehabilitation methods in boys with Duchenne muscular dystrophy.
2. Materials and Methods
The study included 152 boys with DMD (ambulatory and nonambulatory), and it was conducted during the online conference “DMD–Let’s be together” for Polish families with DMD. During the physical therapy panel, we showed the video with the instruction of respiratory exercises (Video S1): positive inspiratory pressure, glossopharyngeal breathing, and positive expiratory pressure. The exercises could be performed at home without physiotherapist assistance. Patients were encouraged to train every day, three times a day. In the video, patients received following instructions:
1. Breath stacking (positive inspiratory pressure): Patients were asked to take a maximum inhale, then without exhaling, to take another 1–3 inhales and hold for 5 s. The boys were instructed to repeat the exercise 5 times. The aim of the exercise was to increase lung volume. The same exercise was presented with the use of an inflated balloon. Patients were instructed to inhale the air from the balloon without exhaling and to try to hold as much air in the lungs as possible. The boys were encouraged to hold for 5 s and repeat 5 times.
2. Glossopharyngeal breathing: Patients were instructed to push a series of small volumes of air by tongue and pharynx into the lungs by saying ‘cat’ in Polish. The boys were encouraged to repeat the exercise 5 times.
3. Positive expiratory pressure: Inflating the balloon. Patients were instructed to inflate the balloon by inhaling by nose and exhaling by mouth. The exercise should be repeated 3 times. Caregivers were encouraged to try different types of balloons to find the optimal elasticity of material (optimal resistance).
After the conference, all participants (n = 152) were asked to fill in the online survey evaluating this home-based programme. The survey consisted of questions about age, ambulation, and upper limb functional status. Respondents were also asked to assess—using a six-point scale—general satisfaction, appropriateness of the exercises, and intelligibility where 0 meant the worst score, and 5 meant the best score. Moreover, in the questionnaire, we asked whether the exercises were performed. The respondents assessed the difficulty of the exercises and possibility to implement this treatment into their daily routine. Additionally, caregivers were invited to leave an e-mail contact in case they needed expanded individual consultation or training.
The study was conducted as a part of the Multidisciplinary Care Programme for Patients with Duchenne Muscular Dystrophy performed by the Rare Disease Centre (RDC), University Clinical Centre, Medical University of Gdańsk, Poland. The University Clinical Centre is a member of the TREAT NMD Alliance Neuromuscular Network.
The study was accepted by the Ethics Committee and assigned the number NKBBN/105/2018.
3. Results
The video with respiratory exercises was displayed 127 times in the first month. The online survey was filled in by 31 (20.4%) participants, and the mean age of the patients was 13.8 years. Nineteen (61.3%) were ambulant. Detailed ambulatory status and upper limb functional status are presented in
Table 1.
The general rating of the online respiratory programme was 4.77/5, appropriateness 4.74/5, and intelligibility 4.74/5.
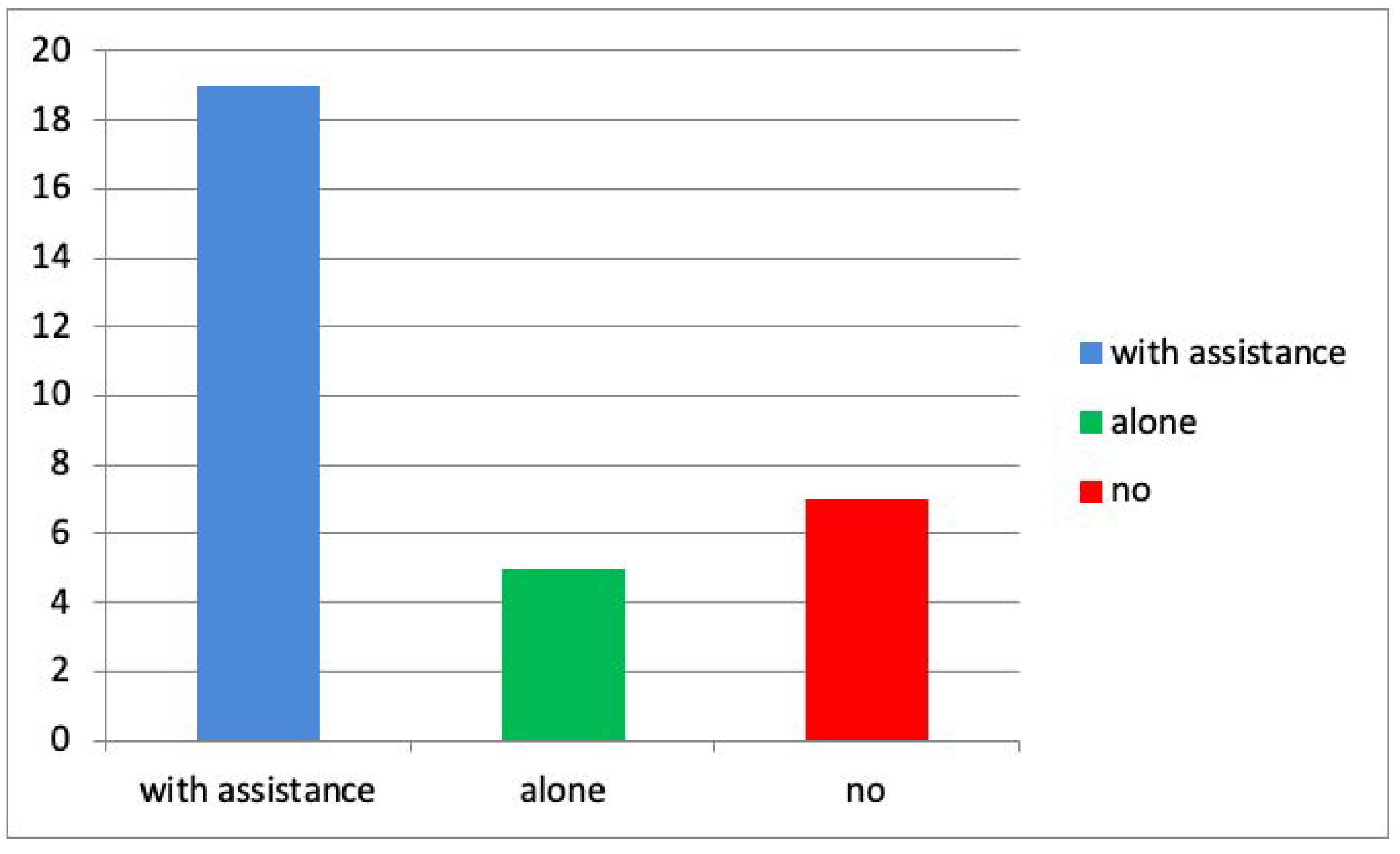
The number of participants who tried to perform the exercise by themselves was 5 (16.1%) and with assistance 19 (61.2%), and 7 (22.6%) did not perform the exercises (
Figure 1).
Only 1 respondent declared that the patient was able to perform all the exercises properly; 16 were able to perform all the exercises after practicing, and 14 declared that some exercises were too difficult for the patient.
The respondents declared that it was possible to implement respiratory exercises into a home-based rehabilitation routine. The frequency of the exercises as declared by caregivers/patients is presented in
Figure 2.
Only two caregivers responded to the invitation for further individual consultation or assistance with exercise performance.
One respondent chose phone consultation—a nonambulant 18-year-old patient. The patient and his parents asked questions about symptoms of dyspnoea, eventual disturbing symptoms regarding the respiratory condition requiring hospitalization, and the efficacy of home use of a pulse oximeter. Parents were also worried because of the cancelling of regular multidisciplinary consultations due to the pandemic. However, they admitted that the patients did not try to perform the proposed respiratory exercises.
Another respondent chose the e-mail consultation. The mother of 6-year-old ambulant boy reported that her son had difficulties with the respiratory exercises and performing the pulmonary function tests because of an inability to perform forced expiration.
4. Discussion
Nowadays, the multidisciplinary DMD healthcare team is facing the challenge to ensure consistency in care and treatment. Respiratory rehabilitation is one of the most pressing problems.
Before the pandemic in 2015, the American Thoracic Society (ATS) and European Respiratory Society (ERS) suggested of perform telerehabilitation to increase the availability of pulmonary rehabilitation to more patients [
7].
Current studies concerning respiratory telerehabilitation report that this intervention is effective in reducing disability and improving quality of life and may reduce the risk of severe exacerbations [
8,
9,
10]. Moreover, there is evidence that telerehabilitation in the paediatric population may be as effective as face-to-face treatment [
11]. However, to our knowledge, this is the first study concerning respiratory digital in DMD.
Unfortunately, we noticed a low response rate to the online survey conducted after the conference, and a low number of patients made an effort to perform the proposed exercises.
Our previous study concerning digital physical therapy showed a similar low response rate to the online physical therapy workshops. Moreover, the survey also showed that 57.8% of DMD patients included in the above-mentioned study felt overloaded with home-schooling responsibilities [
6]. This may be the reason for the low response to the survey and/or treatment provided online. Another reason may be related to not enough trust in the healthcare interventions conducted indirectly. It has to be mentioned that telerehabilitation is a new method in Poland and is not widely known among parents/caregivers of DMD patients.
Similarly, the low response rate is described in telerehabilitation studies involving patients with different disorders. The study of Hensen concerning pulmonary telerehabilitation in 134 patients with COPD revealed that only 12.19% of the group members that met the inclusion criteria managed to complete the intervention protocol [
8].
The ratings of the quality and understanding of the instructions as well as the acceptance of the proposed exercise programmes indicate that it is possible to implement such intervention in a daily home-based rehabilitation routine. Additionally, our results reveal that most patients performed the exercises with the caregiver’s assistance. This observation may be a hint for the future design of online interventions. Promising findings show that the majority of respondents declared that it would be possible to exercise more frequently than 1–2 times a day; however, the question about the effectiveness of the home-based respiratory exercises in this group of patients remains open.
A limitation of our study, in addition to the low response rate, is the fact that the outcomes were only assessed on the basis of respondent declarations. The objective assessment of the results of the proposed programme is under investigation.
In summary, online rehabilitation during the COVID-19 pandemic as well as the conventional care of DMD boys should always rely on an individual approach while taking into consideration the patient’s age, functional abilities, cognitive limitations, and level of cooperation.
5. Conclusions
The study shows that respiratory telerehabilitation may be implemented in DMD patients; however, it should include caregiver assistance. The interest in digital rehabilitation among caregivers of DMD boys in Poland is low, which requires further research. Moreover, there is a need for a well-designed randomized clinical trial assessing the effectiveness of the proposed interventions.
Author Contributions
Conceptualization, A.S.-R. and Ł.M.; methodology, A.S.-R.; validation, A.S.-R., and J.J.-B.; formal analysis, A.S.-R. and Ł.M.; investigation, A.S.-R. and Ł.M.; resources, K.Ś.; data curation, A.S.-R. and Ł.M.; writing—original draft preparation, A.S.-R., Ł.M., J.J.-B. and K.Ś.; writing—review and editing, A.S.-R., Ł.M., J.J.-B. and K.Ś.; visualization, A.S.-R. and Ł.M.; supervision, J.J.-B.; project administration, A.S.-R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethical Committee of Independent Bioethics Committee for Scientific Research at Medical University of Gdańsk: NKBBN/105/2018.
Informed Consent Statement
Patient consent was waived due to the survey’s anonymity.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Birnkrant, D.J.; Bushby, K.; Bann, C.M.; Apkon, S.D.; Blackwell, A.; Brumbaugh, D.; Case, L.E.; Clemens, P.R.; Hadjiyannakis, S.; Pandya, S.; et al. Diagnosis and management of Duchenne muscular dystrophy, part 1: Diagnosis, and neuromuscular, rehabilitation, endocrine, and gastrointestinal and nutritional management. Lancet Neurol. 2018, 17, 251–267. [Google Scholar] [CrossRef] [Green Version]
- Wasilewska, E.; Małgorzewicz, S.; Sobierajska-Rek, A.; Jabłońska-Brudło, J. Transition from Childhood to Adulthood in Patients with Duchenne Muscular Dystrophy. Medicina 2020, 56, 426. [Google Scholar] [CrossRef] [PubMed]
- Birnkrant, D.J.; Bushby, K.; Bann, C.M.; Alman, B.A.; Apkon, S.D.; Blackwell, A.; Case, L.E.; Cripe, L.; Hadjiyannakis, S.; Olson, A.K.; et al. Diagnosis and management of Duchenne muscular dystrophy, part 2: Respiratory, cardiac, bone health, and orthopaedic management. Lancet Neurol. 2018, 17, 347–361. [Google Scholar] [CrossRef] [Green Version]
- LoMauro, A.; D’Angelo, M.G.; Aliverti, A. Assessment and management of respiratory function in patients with Duchenne muscular dystrophy: Current and emerging options. Ther. Clin. Risk Manag. 2015, 11, 1475–1488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veerapandiyan, A.; Wagner, K.R.; Apkon, S.; McDonald, C.M.; Mathews, K.D.; Parsons, J.A.; Wong, B.L.; Eichinger, K.; Shieh, P.B.; Butterfield, R.J.; et al. The care of patients with Duchenne, Becker, and other muscular dystrophies in the COVID-19 pandemic. Muscle Nerve 2020, 62, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Sobierajska-Rek, A.; Mański, Ł.; Jabłońska-Brudło, J.; Śledzińska, K.; Ucińska, A.; Wierzba, J. Establishing a telerehabilitation program for patients with Duchenne muscular dystrophy in the COVID-19 pandemic. Wien Klin Wochenschr. 2020, 133, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Rochester, C.L.; Vogiatzis, I.; Holland, A.E.; Lareau, S.C.; Marciniuk, D.D.; Puhan, M.A.; Spruit, M.A.; Masefield, S.; Casaburi, R.; Clini, E.M.; et al. An Official American Thoracic Society/European Respiratory Society Policy Statement: Enhancing Implementation, Use, and Delivery of Pulmonary Rehabilitation. Am. J. Respir. Crit. Care Med. 2015, 192, 1373–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, H.; Bieler, T.; Beyer, N.; Kallemose, T.; Wilcke, J.T.; Østergaard, L.M.; Andeassen, H.F.; Martinez, G.; Lavesen, M.; Frølich, A.; et al. Supervised pulmonary tele-rehabilitation versus pulmonary rehabilitation in severe COPD: A randomised multicentre trial. Thorax 2020, 75, 413–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tousignant, M.; Marquis, N.; Pagé, C.; Imukuze, N.; Métivier, A.; St-Onge, V.; Tremblay, A. In-home Telerehabilitation for Older Persons with Chronic Obstructive Pulmonary Disease: A Pilot Study. Int. J. Telerehabilitation 2012, 4, 15–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourne, S.; DeVos, R.; North, M.; Chauhan, A.; Green, B.; Brown, T.; Cornelius, V.; Wilkinson, T. Online versus face-to-face pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: Randomised controlled trial. BMJ Open 2017, 7, e014580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camden, C.; Pratte, G.; Fallon, F.; Couture, M.; Berbari, J.; Tousignant, M. Diversity of practices in telerehabilitation for children with disabilities and effective intervention characteristics: Results from a systematic review. Disabil. Rehabil. 2020, 42, 3424–3436. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).






{kind=link}
{kind=link}