
Developing a Sustainable Development Goal 3 (SDG3) Index for Italian Municipalities †



Abstract
1. Introduction
2. Materials and Methods
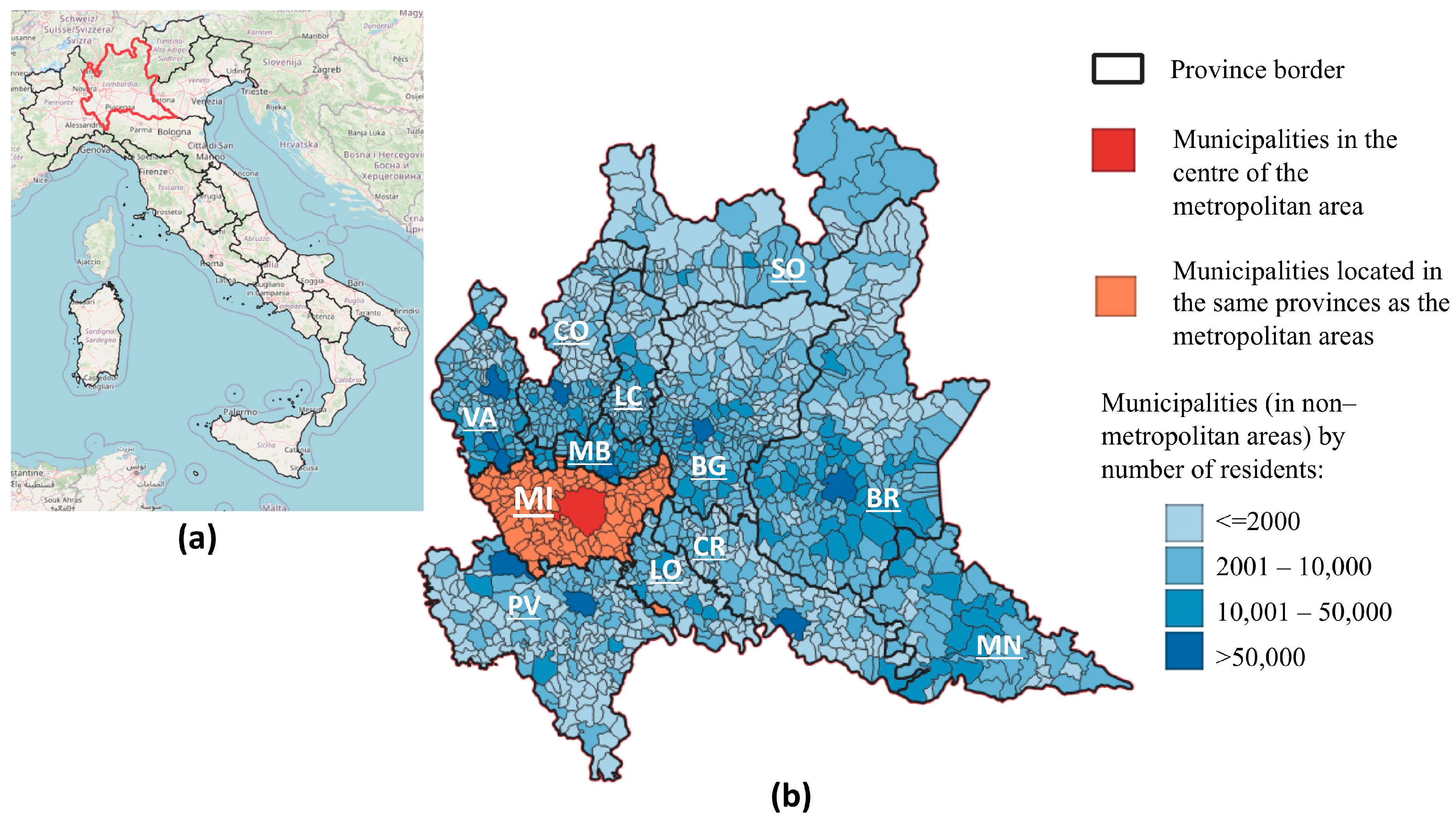
2.1. Study Area
- Municipalities in the centre of the metropolitan area (i.e., 12 municipalities in the whole of Italy, of which Milan is in the Lombardy region);
- Municipalities located in the same provinces as the above-mentioned metropolitan areas (a total of 132 municipalities in Lombardy, i.e., 8.8% of all regions’ municipalities);
- Municipalities (in non-metropolitan areas) with up to 2000 residents (596, i.e., 39.6%);
- Municipalities (in non-metropolitan areas) with 2001–10,000 residents (644, i.e., 42.8%);
- Municipalities (in non-metropolitan areas) with 10,001–50,000 residents (121, i.e., 8.0%);
- Municipalities (in non-metropolitan areas) with more than 50,000 residents (10, i.e., 0.7%).
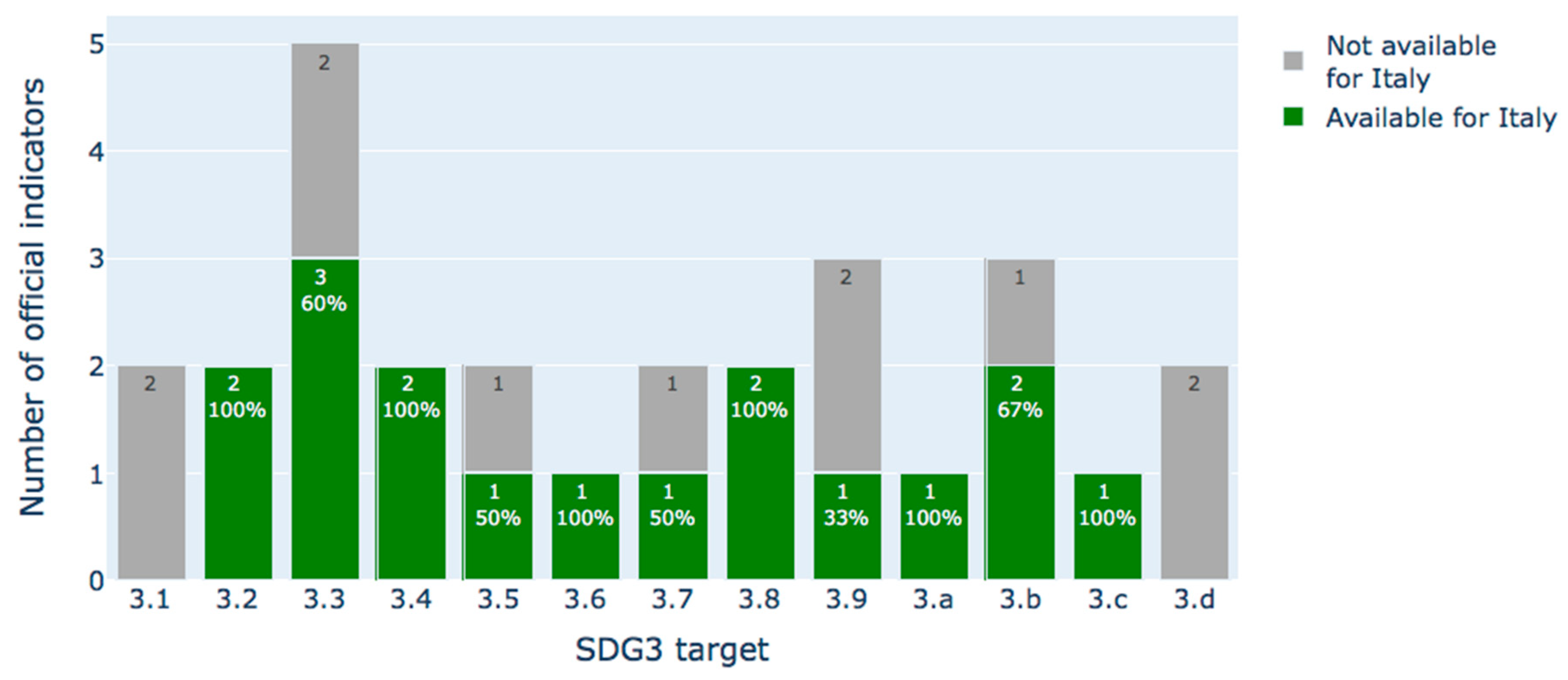
2.2. SDG3 Data
2.3. SDG3 Index Computation
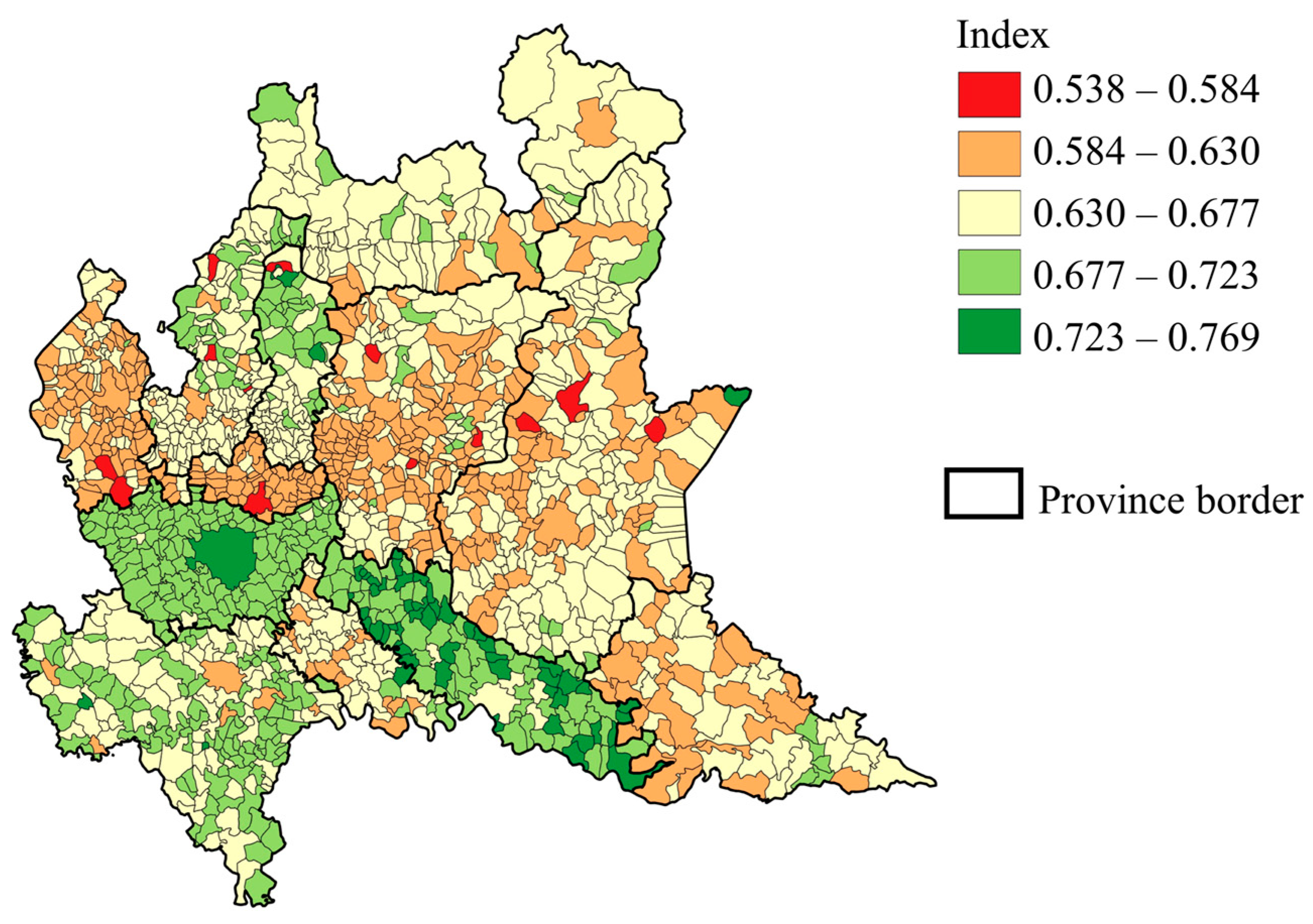
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stafford-Smith, M.; Griggs, D.; Gaffney, O.; Ullah, F.; Reyers, B.; Kanie, N.; Stigson, B.; Shrivastava, P.; Leach, M.; O’Connell, D. Integration: The key to implementing the Sustainable Development Goals. Sustain. Sci. 2017, 12, 911–919. [Google Scholar] [CrossRef] [PubMed]
- D’Adamo, I.; Gastaldi, M.; Ioppolo, G.; Morone, P. An analysis of Sustainable Development Goals in Italian cities: Performance measurements and policy implications. Land Use Policy 2022, 120, 106278. [Google Scholar] [CrossRef]
- D’Adamo, I.; Gastaldi, M.; Imbriani, C.; Morone, P. Assessing regional performance for the Sustainable Development Goals in Italy. Sci. Rep. 2021, 11, 24117. [Google Scholar] [CrossRef] [PubMed]
- Dello Strologo, A.; D’Andrassi, E.; Paoloni, N.; Mattei, G. Italy versus other European countries: Sustainable Development Goals, policies and future hypothetical results. Sustainability 2021, 13, 3417. [Google Scholar] [CrossRef]
- Puertas, R.; Marti, L. Regional analysis of the sustainable development of two Mediterranean countries: Spain and Italy. Sustain. Dev. 2023, 31, 797–811. [Google Scholar] [CrossRef]
- Cavalli, L.; Farnia, L.; Lizzi, G.; Romani, I.G.; Alibegovic, M.; Vergalli, S. The SDSN Italia SDGs City Index Two Years Later: Update Report; FEEM Report No. 08-2020. 2020. Available online: https://www.ssrn.com/abstract=3733706 (accessed on 17 April 2024).
- Farnia, L.; Cavalli, L.; Lizzi, G.; Vergalli, S. Methodological insights to measure the Agenda 2030 at urban level in Italy. Sustainability 2019, 11, 4598. [Google Scholar] [CrossRef]
- Italian National Institute of Statistics. Il Rapporto SDGs. Available online: https://www.istat.it/it/benessere-e-sostenibilit%C3%A0/obiettivi-di-sviluppo-sostenibile/il-rapporto-sdgs (accessed on 1 August 2023).
- Fenner, R.; Cernev, T. The implications of the Covid-19 pandemic for delivering the Sustainable Development Goals. Futures 2021, 128, 102726. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Sustainable Development Goals. Available online: https://www.who.int/europe/about-us/our-work/sustainable-development-goals (accessed on 6 October 2023).
- United Nations. Goal 3 Ensure Healthy Lives and Promote Well-Being for All at All Age. Available online: https://sdgs.un.org/goals/goal3 (accessed on 6 October 2023).
- Hák, T.; Janoušková, S.; Moldan, B. Sustainable Development Goals: A need for relevant indicators. Ecol. Indic. 2016, 60, 565–573. [Google Scholar] [CrossRef]
- Rickels, W.; Dovern, J.; Hoffmann, J.; Quaas, M.F.; Schmidt, J.O.; Visbeck, M. Indicators for monitoring sustainable development goals: An application to oceanic development in the European Union. Earth’s Future 2016, 4, 252–267. [Google Scholar] [CrossRef]
- Lu, Y.; Nakicenovic, N.; Visbeck, M.; Stevance, A.S. Policy: Five priorities for the UN sustainable development goals. Nature 2015, 520, 432–433. [Google Scholar] [CrossRef]
- Shi, Y.; Yang, J.; Keith, M.; Song, K.; Li, Y.; Guan, C. Spatial accessibility patterns to public hospitals in shanghai: An improved gravity model. Prof. Geogr. 2022, 74, 265–289. [Google Scholar] [CrossRef]
- Ge, E.; Su, M.; Zhao, R.; Huang, Z.; Shan, Y.; Wei, X. Geographical disparities in access to hospital care in Ontario, Canada: A spatial coverage modelling approach. BMJ Open 2021, 11, e041474. [Google Scholar] [CrossRef] [PubMed]
- Delgado, E.J.; Cabezas, X.; Martin-Barreiro, C.; Leiva, V.; Rojas, F. An equity-based optimization model to solve the location problem for healthcare centers applied to hospital beds and COVID-19 vaccination. Mathematics 2022, 10, 1825. [Google Scholar] [CrossRef]
- Pradhan, P.; Costa, L.; Rybski, D.; Lucht, W.; Kropp, J.P. A systematic study of sustainable development goal (SDG) interactions. Earth’s Future 2017, 5, 1169–1179. [Google Scholar] [CrossRef]
- Griggs, D.J.; Nilsson, M.; Stevance, A.; McCollum, D. A Guide to SDG Interactions: From Science to Implementation; International Council for Science: Paris, France, 2017. [Google Scholar]
- Bennich, T.; Weitz, N.; Carlsen, H. Deciphering the scientific literature on SDG interactions: A review and reading guide. Sci. Total Environ. 2020, 728, 138405. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Fu, B.; Wang, S.; Song, S.; Li, Y.; Xu, Z.; Wei, Y.; Liu, J. Decoupling of SDGs followed by re-coupling as sustainable development progresses. Nat. Sustain. 2022, 5, 452–459. [Google Scholar] [CrossRef]
- Alcamo, J.; Thompson, J.; Alexander, A.; Antoniades, A.; Delabre, I.; Dolley, J.; Marshall, F.; Menton, M.; Middleton, J.; Scharlemann, J.P. Analysing interactions among the sustainable development goals: Findings and emerging issues from local and global studies. Sustain. Sci. 2020, 15, 1561–1572. [Google Scholar] [CrossRef] [PubMed]
- Scharlemann, J.P.; Brock, R.C.; Balfour, N.; Brown, C.; Burgess, N.D.; Guth, M.K.; Ingram, D.J.; Lane, R.; Martin, J.G.C.; Wicander, S.; et al. Towards understanding interactions between Sustainable Development Goals: The role of environment–human linkages. Sustain. Sci. 2020, 15, 1573–1584. [Google Scholar] [CrossRef]
- Kubiszewski, I.; Mulder, K.; Jarvis, D.; Costanza, R. Toward better measurement of sustainable development and wellbeing: A small number of SDG indicators reliably predict life satisfaction. Sustain. Dev. 2022, 30, 139–148. [Google Scholar] [CrossRef]
- Biermann, F.; Kanie, N.; Kim, R.E. Global governance by goal-setting: The novel approach of the UN Sustainable Development Goals. Curr. Opin. Environ. Sustain. 2017, 26, 26–31. [Google Scholar] [CrossRef]
- Mustajoki, J.; Borchardt, S.; Büttner, L.; Köhler, B.; Lepenies, R.; Lyytimäki, J.; Mille, R.; Pedersen, A.B.; Reis, S.; Richard, D. Ambitiousness of Sustainable Development Goal (SDG) targets: Classification and implications for policy making. Discov. Sustain. 2022, 3, 36. [Google Scholar] [CrossRef]
- Swain, R.B.; Ranganathan, S. Modeling interlinkages between sustainable development goals using network analysis. World Dev. 2021, 138, 105136. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Lowe, M.; Arundel, J. Achieving the SDGs: Evaluating indicators to be used to benchmark and monitor progress towards creating healthy and sustainable cities. Health Policy 2020, 124, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Hsu, A.; Weinfurter, A. Sustainable and inclusive–Evaluating urban sustainability indicators’ suitability for measuring progress towards SDG-11. Environ. Plan. B Urban Anal. City Sci. 2021, 48, 2346–2362. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Province | Median SDG3 Index | 25th–75th Percentile |
|---|---|---|
| Cremona | 0.720 | 0.704–0.731 |
| Milan | 0.694 | 0.688–0.698 |
| Pavia | 0.679 | 0.660–0.690 |
| Lecco | 0.666 | 0.657–0.685 |
| Sondrio | 0.660 | 0.644–0.672 |
| Como | 0.657 | 0.646–0.674 |
| Lodi | 0.640 | 0.631–0.660 |
| Brescia | 0.638 | 0.625–0.654 |
| Mantua | 0.633 | 0.625–0.649 |
| Bergamo | 0.630 | 0.620–0.651 |
| Varese | 0.622 | 0.612–0.640 |
| Monza and Brianza | 0.608 | 0.600–0.614 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nawaro, J.; Gianquintieri, L.; Caiani, E.G. Developing a Sustainable Development Goal 3 (SDG3) Index for Italian Municipalities. Med. Sci. Forum 2024, 25, 6. https://doi.org/10.3390/msf2024025006
Nawaro J, Gianquintieri L, Caiani EG. Developing a Sustainable Development Goal 3 (SDG3) Index for Italian Municipalities. Medical Sciences Forum. 2024; 25(1):6. https://doi.org/10.3390/msf2024025006
Chicago/Turabian StyleNawaro, Julia, Lorenzo Gianquintieri, and Enrico G. Caiani. 2024. "Developing a Sustainable Development Goal 3 (SDG3) Index for Italian Municipalities" Medical Sciences Forum 25, no. 1: 6. https://doi.org/10.3390/msf2024025006
APA StyleNawaro, J., Gianquintieri, L., & Caiani, E. G. (2024). Developing a Sustainable Development Goal 3 (SDG3) Index for Italian Municipalities. Medical Sciences Forum, 25(1), 6. https://doi.org/10.3390/msf2024025006