Abstract
Background/Objectives: Hypertension is a leading cause of cardiovascular morbidity and mortality, particularly in older adults, pharmacological therapy is effective, but side effects and limited adherence highlight the need for non-pharmacological alternatives. This study investigated the effects of a structured Bodypump (BoP) programme, a choreographed group-based resistance training intervention, on blood pressure (BP) and functional fitness in sedentary older adults with hypertension. Methods: Thirty-two participants (65.4 ± 7.7 years) diagnosed with hypertension were randomly allocated to a BoP group (n = 16) or a control group (CG) (n = 16). The intervention lasted 8-week and consisted of 3 supervised sessions per week. Resting systolic BP (SBP) and diastolic BP (DBP) were measured using a validated automated device (Omron M3 Intellisense, HEM-7051-E), functional capacity was assessed with the Senior Fitness Test (SFT) battery. Results: After the intervention, BoP exhibited significant reductions in SBP (−24.4 ± 4.7 mmHg; p < 0.001) and DBP (−6.4 ± 2.7 mmHg; p = 0.025) compared to CG. BoP improved functional fitness, lower- and upper-body strength, aerobic endurance and agility (p < 0.05), with no changes in the CG. Conclusions: 8-week of BoP programme reduced BP and enhanced physical function in sedentary hypertensive older adults. Given its accessible, motivating and socially engaging format, BoP represents a promising non-pharmacological strategy for hypertension management and functional fitness of healthy ageing.
1. Introduction
High blood pressure (BP) is a leading preventable risk factor for mortality and disability, causing 10.8 million deaths annually and affecting 1.3 billion adults worldwide [1,2]. Nearly half of those affected are unaware of their condition, and only 21% achieve adequate control. Hypertension, defined as systolic BP (SBP) ≥ 140 mmHg and/or diastolic BP (DBP) ≥ 90 mmHg [3], increases with age and is a major risk factor for cardiovascular disease. Lowering BP, even from moderately elevated levels (≥130/80 mmHg), significantly reduces the risk of stroke, ischemic heart disease, and functional decline, especially in older adults [4].
Pharmacological therapy remains the first-line treatment [5], but side effects [6,7] and polypharmacy in older adults [8] may compromise adherence. This highlights the need for complementary non-pharmacological approaches, particularly physical activity (PA). Exercise consistently reduces BP and improves cardiovascular health [9], with acute decreases after a single session [10,11]. Moreover, inactivity accelerates functional decline [12], whereas regular PA improves quality of life [13]. Resistance training is especially effective, simultaneously enhancing muscle function and reducing BP. A recent meta-analysis showed dynamic resistance training reduces SBP by 7 mmHg and DBP by 3 mmHg, clinically meaningful benefits for hypertensive older adults [14].
Adherence is crucial for long-term exercise benefits, yet many older adults discontinue programs early due to motivational and social barriers [15]. Group-based programs achieve higher adherence, often >70% [16], by fostering cohesion, enjoyment, and commitment [17,18]. Gym-based group classes, particularly Bodypump (BoP), have become globally popular [19]. BoP is a choreographed resistance training modality combining high repetitions with light-to-moderate weights, performed to music under instructor supervision [20]. Its engaging format supports adherence and produces acute cardiovascular, hormonal, and perceptual responses [21]. However, evidence on its long-term clinical effects in hypertensive older adults remains scarce.
Beyond cardiovascular outcomes, functional fitness is essential for maintaining independence in ageing populations [22]. Regular PA enhances strength, endurance, flexibility, and agility, helping preserve autonomy [12,13]. To our knowledge this study is the first one to examine the effect of BoP on BP and functional fitness in sedentary hypertensive older adults, this study aimed to evaluate the effects of an 8-week BoP programme on resting BP and functional fitness. We hypothesized that BoP would reduce SBP and DBP while improving functional capacity in sedentary hypertensive older adults.
2. Results
Adherence to the programme was high, with a mean ± SD (standard deviation) of 23.1 ± 0.6 sessions attended (out of a total of 24). All participants (100%) attended at least 90% of the sessions (≥22 sessions).
In the BoP 370 of the 384 possible sessions were completed, representing 96.4% overall programme attendance.
BoP group reduced SBP (−24.44 ± 4.67 mmHg; p < 0.001) and DBP (−6.44 ± 2.72 mmHg; p = 0.025) compared to CG.
At baseline, no significant differences were observed between groups in BP nor functional fitness outcomes. After the 8-week intervention, the BoP group showed a significant reduction in SBP and DBP, whereas no changes were detected in the CG. Significant between-group differences were observed for both SBP and DBP (Table 1 and Table 2).

Table 1.
Functional Fitness and blood pressure outcomes (Mean ± SD) in Bodypump (BoP) and Control Group (CG).
Table 2.
Confidence intervals (95% CI) for pre- and post-intervention values in the Bodypump (BoP) and Control (CG) groups, and difference between groups.
In terms of functional fitness, participants in the BoP group exhibited significant improvements in lower and upper body strength (Chair Stand and Arm Curl tests), aerobic endurance (2-Minute Step test) and agility (8-Foot Up-and-Go test).
Covariate-Adjusted Analyses
The covariate-adjusted results are shown in Table 3.
Table 3.
Covariate-adjusted post-intervention outcomes in Bodypump (BoP) and Control (CG) groups, controlling for baseline values, BMI and medication status.
In terms of flexibility, BoP participants showed significant within-group improvements in both the Chair Sit-and-Reach and Back Scratch tests in the unadjusted analyses (Table 1). However, no significant differences were observed between BoP and CG in the unadjusted comparisons.
After adjusting for baseline values, BMI, and medication status (Table 3), significant between-group differences emerged in both flexibility outcomes, favouring BoP. These findings highlight the importance of adjusting for covariates and support the robustness of the intervention effects on flexibility.
Values are adjusted for baseline scores and Body mass index. Participants taking antihypertensive medication were excluded from the analysis.
To address potential confounding due to antihypertensive medication use, we conducted a sensitivity analysis excluding participants on such treatment. The results remained consistent, confirming the robustness of the intervention effects on both BP and functional capacity outcomes (Table 4).
Table 4.
Covariate-adjusted post-intervention outcomes in Bodypump (BoP) and Control (CG) groups, excluding participants on antihypertensive medication.
3. Discussion
The aim of this study was to analyze the effects of an 8-week BoP programme on both resting BP and functional fitness in sedentary older adults with hypertension. While the results are promising, they should be interpreted with caution due to the small sample size. The main findings were that BoP training significantly reduced SBP, DBP and improved multiple domains of functional fitness, while no changes observed in the CG.
These results are consistent with previous studies reporting that resistance training is an effective non-pharmacological intervention for BP management [9,14]. A systematic review and meta-analysis reported average reductions of approximately −1.8 mmHg in SBP following dynamic resistance training, with even larger effects observed for isometric protocols [23]. Although modest, these decreases are clinically relevant, as they contribute to lowering cardiovascular risk at the population level. In our study, the magnitude of reduction was greater (−24.4 mmHg in SBP, corresponding to a 15.7% decrease, and −7.1 mmHg in DBP, an 8.5% decrease), which could be attributed to the specific format of BoP: a high-volume, low-to-moderate load routine performed continuously and involving both upper and lower body. This design may have induced cardiovascular and muscular adaptations similar to those of combined resistance and aerobic training. Its accessible, structured and socially enriching nature also makes it an attractive alternative to less motivating or sustainable modalities [20].
The improvements in functional fitness are also in line with prior evidence demonstrating that structured resistance training enhances muscular strength, endurance, balance, and mobility in older adults [13,22]. Gains in tests such as the Chair Stand and 8-Foot Up-and-Go are clinically relevant, as they are associated with greater independence in daily activities and lower fall risk. However, not all studies involving BoP have demonstrated comprehensive benefits. For instance, a 12-week of BoP training enhanced strength and reduced metabolic stress, but no improvements in aerobic running fitness, body composition nor body fat were observed [24]. This suggests that BoP is effective in certain domains, but effects may be limited in other domains depending on population, outcome measured or programme length. To date, there is limited evidence specifically addressing BoP programs in older adults with hypertension, particularly studies that examine adherence levels and how these impact the achievement of expected outcomes. Studies of other exercise modalities suggest that low uptake and poor adherence often attenuate the benefits [25]. This underscores the importance of ensuring high adherence when implementing BoP interventions in this population.
One plausible explanation for the success of the programme in the present study is adherence. Group-based classes with music, choreography and instructor guidance create an engaging and socially supportive environment, which is recognized as a strong driver of long-term participation in older adults [17,18]. This interpretation is supported by previous studies showing that supervised group-based programs such as BoP typically achieve adherence rates above 70% [16], which likely contributed to the functional and cardiovascular benefits observed. Nevertheless, adherence is not the only factor. The relatively high frequency of sessions (3 times per week), the structured progression, and the use of multiple muscle groups within each class may also have contributed to the broad functional improvements observed. In the present study, exceeding the values reported in the scientific literature on adherence to group classes, which is above 70% [16], with a value of 96,4%. This high level of attendance likely contributed to the significant improvements observed in blood pressure and functional fitness. Instructors monitored attendance, and no participants withdrew from the intervention. However, these findings should be confirmed in larger trials. This underscores the need for future studies to validate these results in more diverse populations and with longer follow-up periods.
Limitations of the Study
Although the findings provide encouraging preliminary evidence, caution is warranted when interpreting the results due to some methodological limitations, particularly the relatively small and geographically limited sample.
This study had some limitations that should be taken into account. First, the sample size was relatively small and limited to sedentary older adults with hypertension recruited from a single geographical area, which may restrict the generalisability of the results. It was determined based on the number of eligible participants available in the target municipality, and no a priori sample size calculation was performed. Although no participants dropped out of the study and there were no missing data, this absence of a formal sample size estimate could be considered a limitation. Second, although BP was assessed under standardised laboratory conditions, 24 h ambulatory monitoring would have provided a more comprehensive assessment of daily BP fluctuations. Third, psychosocial factors such as motivation, social support, or perceived well-being, which may partly explain improvements in functional outcomes, were not systematically measured. Finally, adherence was monitored using attendance records but was not supplemented with objective measures such as accelerometry, which could have provided additional information on overall PA levels during the intervention. Furthermore, only the CG included participants taking medication for hypertension, which constitutes a potential confounding factor that could have affected both the initial values and the observed changes in BP.
4. Materials and Methods
4.1. Participants
Thirty-four sedentary older adults volunteered for this study. Two participants did not meet the inclusion criterion of sedentary behaviour during the previous 12 months and were therefore excluded prior to randomization. Consequently, 32 participants (14 men and 18 women) were finally included and completed the study, 65.4 ± 7.7 years; 85.5 ± 16.9 kg and 31.6 ± 5.0 kg/m2 of body mass index (BMI) with hypertension (SBP 154.5 ± 20.2 mmHg, and DBP 88.4 ± 11.9 mmHg) (Figure 1).
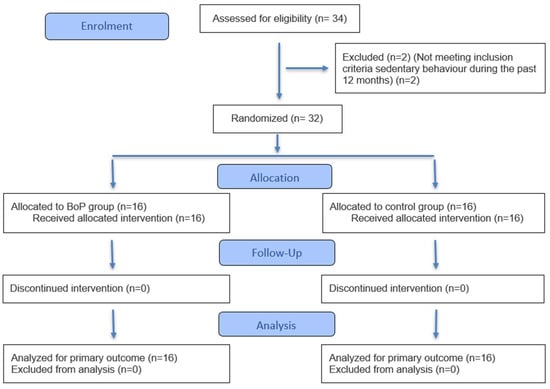
Figure 1.
Flow Diagram of the progress through the phases of a randomized trial (CONSORT, 2025, see Supplementary Materials) [26].
All individuals who expressed their willingness to participate were included in order to maximize the available sample size. Recruitment took place in the town of Osuna (Seville, Spain), where the target population was limited.
Recruitment took place in January 2025, and participants completed the eight-week intervention and follow-up assessments in March 2025. Participants were randomly allocated into a BoP group (n = 16, 6 men and 10 women, 64.3 ± 5.0 years, 81.3 ± 16.4 kg, BMI 30.6 ± 4.3 kg/m2, SBP 155.9 ± 27.9 mmHg and DBP 83.9 ± 12.1 mmHg) or control group (CG; n = 16, 8 men and 8 women, 65.6 ± 7.7 years, 89.7 ± 16.9 kg, a BMI of 32.1 ± 5.2 kg/m2, SBP of 153.1 ± 7.9 mmHg and a DBP of 92.9 ± 10.3 mmHg), which maintained in parallel their usual lifestyle without participating in any programmed PA (Table 5). BoP attended 3 BoP sessions per week on non-consecutive days (Monday, Wednesday and Friday), each session lasting 45 min.
Table 5.
Baseline characteristics of participants in the Bodypump (BoP) and Control (CG) groups.
Inclusion criteria were: (a) clinical diagnosis of hypertension defined as SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg [3], (b) sedentary behaviour during the past 12 months, (c) medical clearance to participate in supervised PA, and (d) age over 60 years. Exclusion criteria included: (a) presence of orthopaedic or cardiovascular conditions contraindicating exercise, (b) unstable or uncontrolled hypertension, (c) participation in any other structured exercise programme during the intervention period, (d) having minimal functional fitness for both testing and BP practice and (e) having missed more than 10% of the sessions (missing more than 2 sessions).
Blood pressure medication status was recorded at baseline. None of the participants in the BoP group were taking antihypertensive medication. In contrast, five participants (31.3%) in the CG were under stable antihypertensive pharmacological treatment. No changes in medication use or dosage were reported during the intervention period.
All participants signed informed consent forms before the start of the study. This was approved by the Bioethics and Biosafety Commission of the University of Extremadura (Registration number: 30/2025). The study complies with the fundamental ethical principles and current regulations. This study was retrospectively registered at ClinicalTrials.gov (Identifier: NCT07084337) on 29 July 2025. The study design was interventional, with two parallel arms (BoP group and CG).
4.2. Experimental Design
A longitudinal experimental trial design with randomly assigned parallel groups was used. The study was conducted at the Osuna University College (Seville, Spain) and lasted 10 weeks. Initial tests were performed in week 1, followed by an 8-week intervention, and post-intervention tests were performed in week 10. An external researcher, affiliated with the University of Sevilla, Osuna University College where the trial was conducted, randomly assigned participants to the BoP or CG in a balanced manner, using an online tool to generate groups randomly (https://www.randomlists.com/team-generator (accessed on 24 January 2025)). The randomization sequence was communicated to the researcher (M.C.O.), who subsequently informed the participants individually about the group they had been assigned to, the days of the sessions and the timetable, in a neutral manner, without revealing the study hypotheses or the expected results. To ensure allocation concealment, pre- and post-intervention assessments were conducted by another researcher (M.J.R.C.) from the University of Extremadura, who was unaware of the group allocation throughout the assessment process.
4.3. Bodypump Training Program
The BoP training sessions followed the official Les Mills format and were led by external certified instructor. Each session focused on the major muscle groups through choreographed exercises performed with barbells, weight discs and a step platform. The format included a warm-up (6 min), resistance-based tracks for the lower and upper body as the main component of the class (35 min), and a final cool-down including stretching of the major muscle groups (4 min).
Participants performed a high volume of repetitions per muscle group, ranging between 70 and 120 repetitions per track, depending on the targeted muscle. Specifically, each session included approximately 100 squats, 70–90 chest presses, 70–80 back exercises (deadlifts, rows, clean and presses), 60–80 lunges, and 70–90 repetitions for smaller muscle groups such as triceps, biceps, and shoulders. Core exercises accounted for 60–80 repetitions. In total, participants accumulated 800–1000 repetitions per session.
Training loads were intentionally kept light and were self-selected by participants according to their perceived exertion [27], aiming for a level corresponding to “light-to-somewhat hard” on the Borg CR-10 scale [28]. This ensured that all participants were able to complete the prescribed repetitions with correct technique and without undue fatigue. Progressive overload was encouraged by gradually increasing the load (approximately 2.5–5%) whenever participants reported that the session felt “too easy” (rating of perceived exertion, RPE ≤ 3) [29]. All sessions were supervised by certified instructors to guarantee safety, correct execution, and progression according to individual capacities.
The mean RPE across all BoP sessions was 5.2 ± 0.13, corresponding to a “hard” effort on the Borg CR-10 scale (0 = nothing at all, 5 = hard, 10 = maximal). Although participants were instructed to aim for “light-to-somewhat hard” (CR-10 ≈ 3–4), the observed intensity suggests a slightly higher perceived exertion. Training loads were adjusted when RPE values consistently exceeded 6 or fell below 4 to ensure appropriate progression and safety.
4.4. Measurements
All measurements were carried out by a researcher (M.J.R.C.) who did not know whether the participants belonged to GC or BoP.
4.4.1. Resting Blood Pressure
Resting SBP and DBP were measured using an automatic digital BP monitor, Omron M3 Intellisense (HEM-7051-E) (Kyoto, Japan), which features technology that ensures accurate and comfortable inflation, adapted to the individual characteristics of the user’s arm. The measurements were taken on the left arm using an adult-size cuff corresponding to a 32 cm arm circumference, ensuring accurate and standardized BP measurement, guaranteeing the accuracy and validity of the evaluations. This device provides reliable readings by detecting irregular movements and errors during measurement, ensuring the validity of the results. In addition, it meets the validation criteria established by the International Protocol of the European Society of Hypertension [30]. Measurements were taken in the morning (9:00 a.m.) once a day for three consecutive days, with participants sitting and resting for at least five minutes beforehand. The value recorded was the average of the three measurements. Small groups of four participants were scheduled at 20 min intervals to minimize waiting time and maintain standardized conditions.
No participant had an arm circumference < 22 cm or >42 cm. Therefore, the same adult cuff recommended by the manufacturer (validated range 22–42 cm) was used in all cases. Participants were instructed to avoid caffeine, tobacco and exercise prior to each measurement, and to maintain their habitual lifestyle during the 8-week intervention. The device performs automatic internal calibration according to manufacturer specifications.
4.4.2. Physical Fitness—Senior Fitness Test (SFT)
Functional fitness was assessed using the SFT battery, which has been validated as a reliable tool for evaluating physical fitness in older adults [22]. The SFT included the following components: Chair Stand Test (lower body strength), Arm Curl Test (upper body strength), 2-Minute Step Test (aerobic endurance), Chair Sit and Reach Test (lower body flexibility), Back Scratch Test (upper body flexibility), and 8-Foot Up-and-Go Test (agility and dynamic balance). All assessments were conducted according to the standardized protocols described by trained exercise science professionals and were conducted by the same researcher to ensure consistency across all assessments [22].
4.5. Statistical Analysis
Statistical processing of the data was carried out using SPSS version 30.0 software (IBM Corp., Chicago, IL, USA) for the Windows operating system. Data were expressed as mean ± standard deviation. Normality and homogeneity of variances were assessed using the Shapiro–Wilk and Levene’s tests, respectively. Within-group pre–post differences were evaluated using paired-sample t-tests. Between-group differences were assessed using independent-sample t-tests. Statistical significance was set at p ≤ 0.05.
Effect sizes (ES) for within-group pre–post changes were calculated using Cohen’s d. According to Cohen, ES were interpreted as trivial (<0.2), small (0.2–0.49), moderate (0.5–0.79), and large (≥0.8).
Covariate-adjusted analyses were additionally conducted. The primary outcome was SBP. ES were reported as adjusted mean differences with 95% confidence intervals. All primary and secondary outcomes were re-analyzed using ANCOVA models including baseline values, medication status and BMI as covariates. To address multiplicity across SFT domains, false discovery rate (FDR) control was applied (Benjamini–Hochberg procedure).
For covariate-adjusted between-group comparisons, partial eta squared (η2p) was reported as the ES.
5. Conclusions
The 8-week BoP training programme led to significant improvements in cardiovascular health and functional fitness in sedentary older adults with hypertension. BoP reduced SBP, DBP and improved lower- and upper-body strength, aerobic endurance, agility and flexibility. These findings demonstrate that BoP can simultaneously improve BP and functional fitness, supporting its role as an effective, enjoyable, and accessible non-pharmacological strategy for hypertension management. Furthermore, integrating structured group-based exercise such as BoP into community or clinical programs may represent a practical and sustainable approach to complement pharmacological treatment and promote healthy ageing.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/physiologia5040052/s1, CONSORT 2025 checklist.
Author Contributions
Conceptualization, M.J.R.C. and J.P.-G.; methodology, M.C.-O.; validation, J.P.-G.; formal analysis, M.J.R.C.; investigation, M.J.R.C.; writing—original draft preparation, M.J.R.C.; writing—review and editing, J.P.-G. and M.C.-O.; supervision, J.P.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics and Biosafety Commission of the University of Extremadura (Registration number: 30/2025, date: 21 January 2025).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AC | Arm Curl |
| BP | Blood Pressure |
| BoP | Bodypump |
| CG | Control Group |
| CS | Chair Stand |
| CS&R | Chair sit and reach |
| BS | Back Scratch |
| DBP | Diastolic Blood Pressure |
| RPE | Rating of Perceived Exertion |
| SBP | Systolic Blood Pressure |
| SFT | Senior Fitness Test |
| 2MS | 2-Minute Step |
| 8FUG | 8-Foot Up-and-Go |
References
- DeGuire, J.; Clarke, J.; Rouleau, K.; Roy, J.; Bushnik, T. Blood pressure and hypertension. Health Rep. 2019, 30, 14–21. [Google Scholar] [CrossRef]
- World Health Organization. Hypertension. 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed on 25 August 2025).
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- The SPRINT Research Group. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N. Engl. J. Med. 2015, 373, 2103–2116. [Google Scholar] [CrossRef]
- Wright, J.M.; Musini, V.M. First-line drugs for hypertension. Cochrane Database Syst. Rev. 2009, 8, CD001841. [Google Scholar] [CrossRef]
- Cheung, B.M.Y.; Wong, Y.L.; Lau, C.P. Queen Mary Utilization of Antihypertensive Drugs Study: Side-effects of antihypertensive drugs. J. Clin. Pharm Ther. 2005, 30, 391–399. [Google Scholar] [CrossRef]
- Rivasi, G.; Coscarelli, A.; Capacci, M.; Ceolin, L.; Turrin, G.; Tortù, V.; D’Andria, M.F.; Testa, G.D.; Ungar, A. Tolerability of Antihypertensive Medications: The Influence of Age. High Blood Press. Cardiovasc. Prev. 2024, 31, 261–269. [Google Scholar] [CrossRef]
- Mohamed, M.R.; Mohile, S.G.; Juba, K.M.; Awad, H.; Wells, M.; Loh, K.P.; Flannery, M.; Culakova, E.; Tylock, R.; Ramsdale, E. Association of polypharmacy and potential drug-drug interactions with adverse treatment outcomes in older adults with advanced cancer. Cancer 2023, 129, 1096. [Google Scholar] [CrossRef]
- Herrod, P.J.J.; Doleman, B.; Blackwell, J.; O’Boyle, F.; Lund, J.N.; Phillips, B.E. Non-pharmacological strategies to reduce blood pressure in older adults: A systematic review and meta-analysis. Lancet 2017, 390, S43. [Google Scholar] [CrossRef][Green Version]
- Carpio-Rivera, E.; Moncada-Jiménez, J.; Salazar-Rojas, W.; Solera-Herrera, A. Acute effects of exercise on blood pressure: A meta-analytic investigation. Arq. Bras. Cardiol. 2016, 106, 422–433. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.J.; Deenmamode, A.H.P.; Griffiths, M.; Arnold, O.; Cooper, N.J.; Wiles, J.D.; O’Driscoll, J.M. Exercise training and resting blood pressure: A large-scale pairwise and network meta-analysis of randomised controlled trials. Br. J. Sports Med. 2023, 57, 1317–1326. Available online: https://bjsm.bmj.com/content/57/20/1317 (accessed on 3 September 2025). [CrossRef] [PubMed]
- Mello, G.M.d.V.d.; Frajácomo, F.T.T.; Haagsma, A.B.; Souza, D.L.B.; de Oliveira, V.B.; Olandoski, M.; Neto, J.R.F.; Jerez-Roig, J.; Baena, C.P. Physical activity and functional preservation in older adults with hip osteoarthritis: A comparative analysis of age cohorts in the SHARE study. PLoS ONE 2025, 20, e0317578. [Google Scholar] [CrossRef]
- Acree, L.S.; Longfors, J.; Fjeldstad, A.S.; Fjeldstad, C.; Schank, B.; Nickel, K.J.; Montgomery, P.S.; Gardner, A.W. Physical activity is related to quality of life in older adults. Health Qual Life Outcomes 2006, 4, 37. [Google Scholar] [CrossRef]
- Henkin, J.S.; Pinto, R.S.; Machado, C.L.F.; Wilhelm, E.N. Chronic effect of resistance training on blood pressure in older adults with prehypertension and hypertension: A systematic review and meta-analysis. Exp. Gerontol. 2023, 177, 112193. [Google Scholar] [CrossRef] [PubMed]
- Collins, K.A.; Huffman, K.M.; Wolever, R.Q.; Smith, P.J.; Siegler, I.C.; Ross, L.M.; Hauser, E.R.; Jiang, R.; Jakicic, J.M.; Costa, P.T.; et al. Determinants of Dropout from and Variation in Adherence to an Exercise Intervention: The STRRIDE Randomized Trials. Transl. J. Am. Coll. Sports Med. 2022, 7, e000190. [Google Scholar] [CrossRef]
- Farrance, C.; Tsofliou, F.; Clark, C. Adherence to community based group exercise interventions for older people: A mixed-methods systematic review. Prev. Med. 2016, 87, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, M.R.; Ruissen, G.R.; Dunlop, W.L.; Estabrooks, P.A.; Harden, S.M.; Wolf, S.A.; Liu, Y.; Schmader, T.; Puterman, E.; Sheel, A.W.; et al. Group-based physical activity for older adults (GOAL) randomized controlled trial: Exercise adherence outcomes. Health Psychol. 2018, 37, 451–461. [Google Scholar] [CrossRef]
- Graupensperger, S.; Gottschall, J.S.; Benson, A.J.; Eys, M.; Hastings, B.; Evans, M.B. Perceptions of groupness during fitness classes positively predict recalled perceptions of exertion, enjoyment, and affective valence: An intensive longitudinal investigation. Sport Exerc. Perform. Psychol. 2019, 8, 290–304. [Google Scholar] [CrossRef]
- Rustaden, A.M.; Gjestvang, C.; Bø, K.; Haakstad, L.A.H.; Paulsen, G. Similar Energy Expenditure During BodyPump and Heavy Load Resistance Exercise in Overweight Women. Front. Physiol. 2020, 11, 570. [Google Scholar] [CrossRef] [PubMed]
- Chavarrías-Olmedo, M.; Franco-García, J.M.; García-Paniagua, R.; Calzada-Rodríguez, J.I.; Pérez-Gómez, J. Efectos agudos y crónicos de la práctica de Bodypump. J. Negat. No Posit. Results 2021, 6, 258–270. [Google Scholar] [CrossRef]
- Harris, N.; Kilding, A.; Sethi, S.; Merien, F.; Gottschall, J. A comparison of the acute physiological responses to BODYPUMPTM versus iso-caloric and iso-time steady state cycling. J. Sci. Med. Sport 2018, 21, 1085–1089. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and Validation of Criterion-Referenced Clinically Relevant Fitness Standards for Maintaining Physical Independence in Later Years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef]
- Cornelissen, V.A.; Smart, N.A. Exercise training for blood pressure: A systematic review and meta-analysis. J. Am. Heart Assoc. 2013, 2, e004473. [Google Scholar] [CrossRef]
- Greco, C.C.; Oliveira, A.S.; Pereira, M.P.; Figueira, T.R.; Ruas, V.D.; Goncxalves, M.; Denadai, B.S. Improvements in metabolic and neuromuscular fitness after 12-week bodypump® training. J. Strength Cond Res. 2011, 25, 3422–3431. [Google Scholar] [CrossRef]
- Herrod, P.J.J.; Lund, J.N.; Phillips, B.E. Time-efficient physical activity interventions to reduce blood pressure in older adults: A randomised controlled trial. Age Ageing 2021, 50, 980–984. [Google Scholar] [CrossRef]
- Hopewell, S.; Chan, A.W.; Collins, G.S.; Hróbjartsson, A.; Moher, D.; Schulz, K.F.; Tunn, R.; Aggarwal, R.; Berkwits, M.; Berlin, J.A.; et al. CONSORT 2025 statement: Updated guideline for reporting randomised trials. BMJ 2025, 389, e081123. [Google Scholar] [CrossRef]
- Lea, J.W.D.; O’Driscoll, J.M.; Hulbert, S.; Scales, J.; Wiles, J.D. Convergent Validity of Ratings of Perceived Exertion During Resistance Exercise in Healthy Participants: A Systematic Review and Meta-Analysis. Sports Med. Open 2022, 8, 2. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.P.; Borg, G.A.V. Borg’s scales in strength training; from theory to practice in young and older adults. Appl. Physiol. Nutr. Metab. 2011, 36, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, S.S.; Krinski, K.; Alves, R.C.; Benites, M.L.; Redkva, P.E.; Elsangedy, H.M.; Buzzachera, C.F.; Souza-Junior, T.P.; da Silva, S.G. The Use of Session RPE to Monitor the Intensity of Weight Training in Older Women: Acute Responses to Eccentric, Concentric, and Dynamic Exercises. J. Aging Res. 2014, 2014, 749317. [Google Scholar] [CrossRef]
- Asmar, R.; Khabouth, J.; Topouchian, J.; El Feghali, R.; Mattar, J. Validation of three automatic devices for self-measurement of blood pressure according to the International Protocol: The Omron M3 Intellisense (HEM-7051-E), the Omron M2 Compact (HEM 7102-E), and the Omron R3-I Plus (HEM 6022-E). Blood Press. Monit. 2010, 15, 49–54. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).