
Multimorbidity and Anxiety Symptoms among Adults Aged 50 Years and Over from Six Low- and Middle-Income Countries

 ,
,  , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Anxiety Symptoms (Dependent Variable)
2.2. Chronic Physical Conditions and Physical Multimorbidity (Independent Variables)
2.3. Statistical Analysis
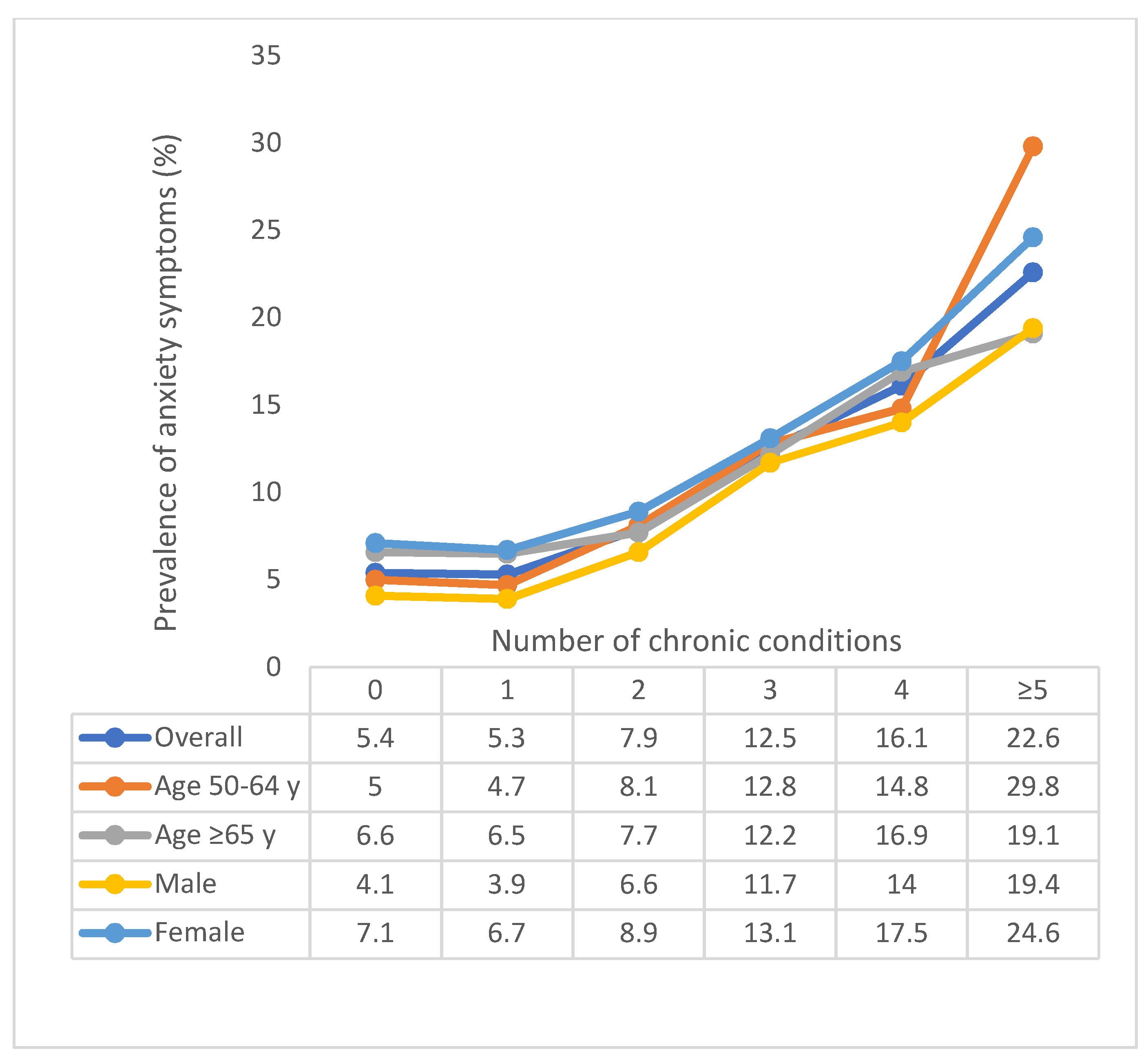
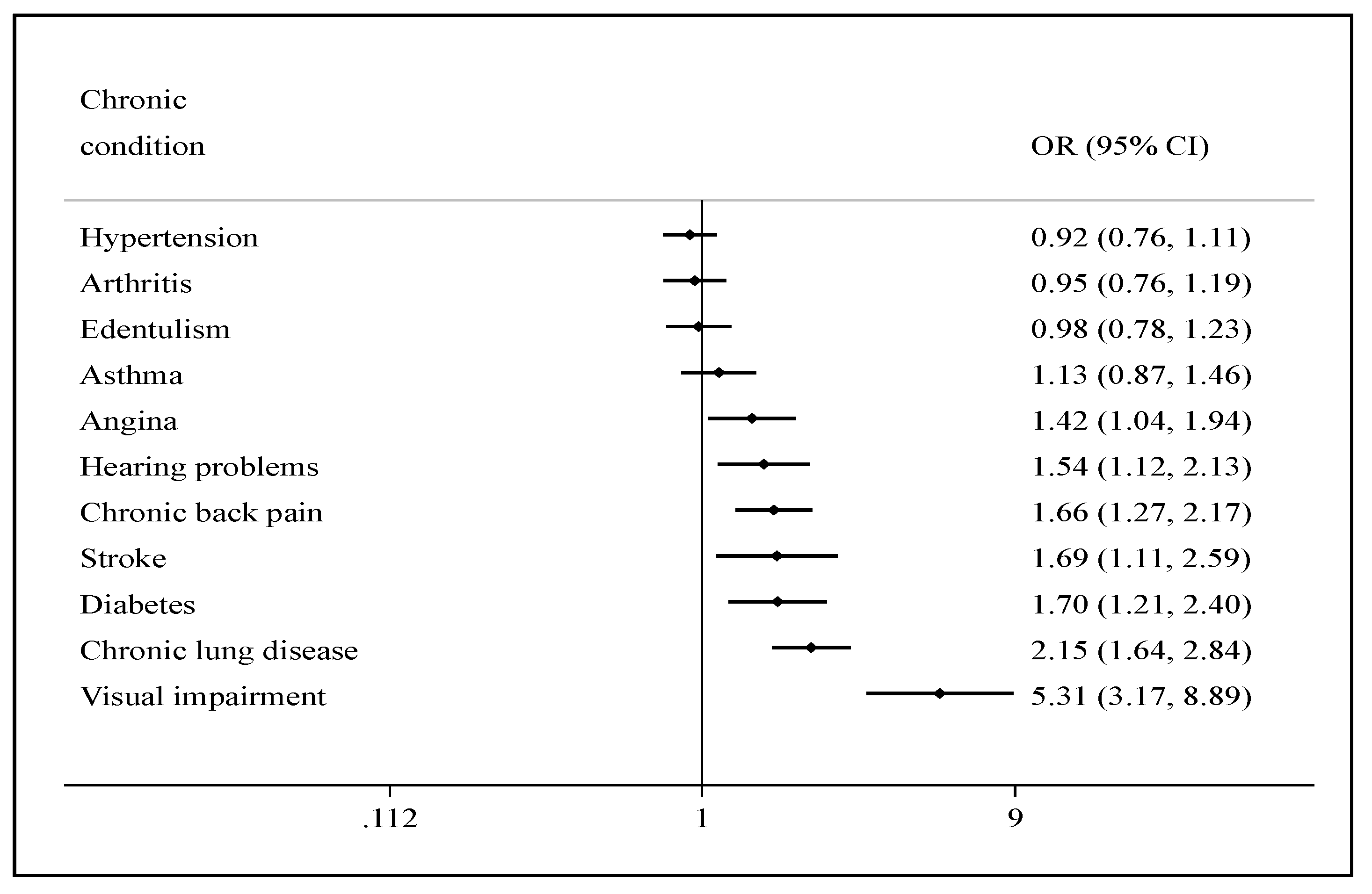
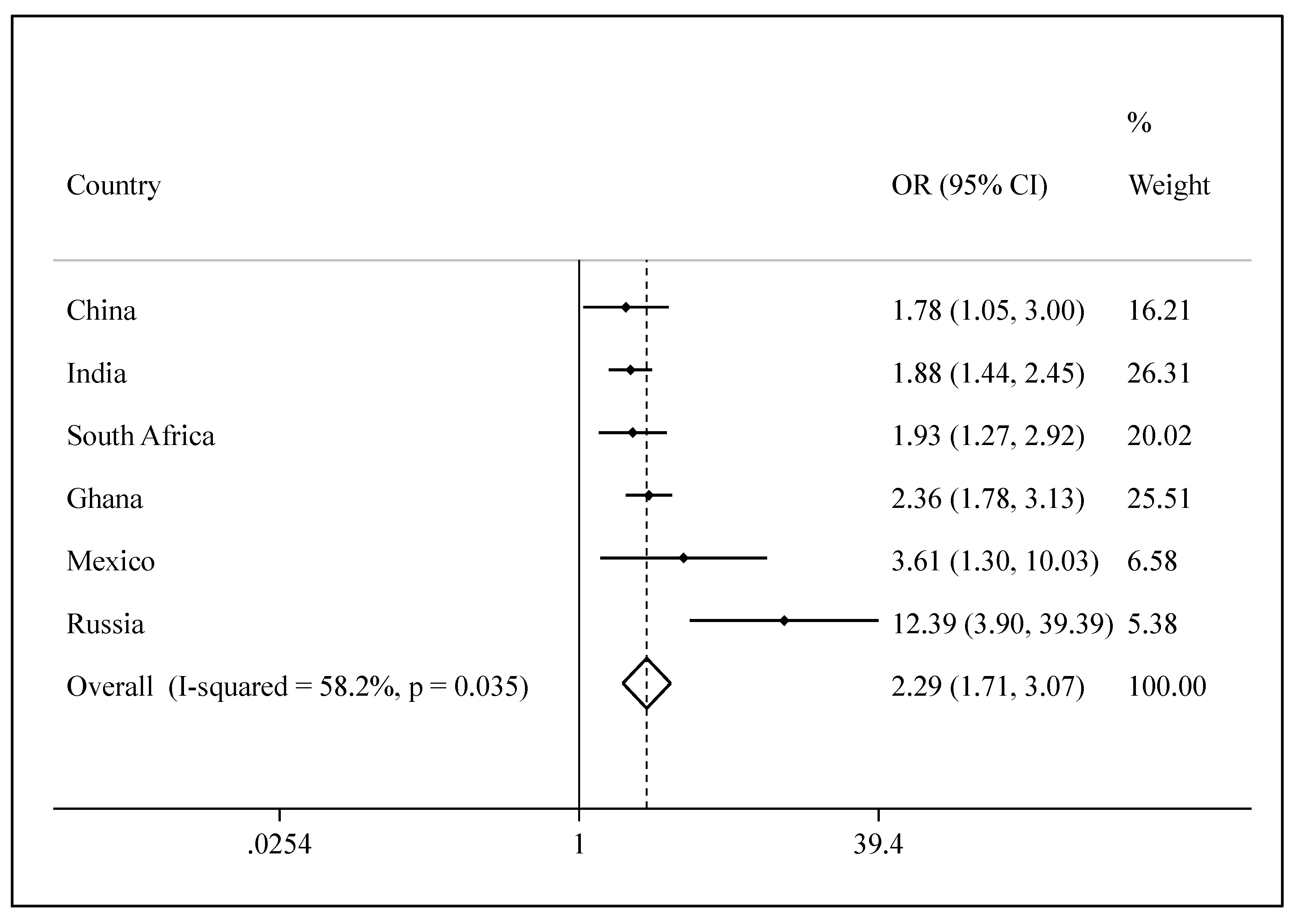
3. Results
4. Discussion
4.1. Main Findings
4.2. Interpretation of the Findings
4.3. Clinical and Public Health Implications
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Condition | (a) Self-Reported Diagnosis | (b) Symptom-Based Algorithm or Other Method of Diagnosis a |
|---|---|---|
| Angina | Have you ever been diagnosed with angina or angina pectoris (a heart disease)? | Rose questionnaire [23] |
| Arthritis | Have you ever been diagnosed with/told you have arthritis (a disease of the joints, or by other names rheumatism or osteoarthritis)? | Affirmative answers to all four of the following: 1. During the last 12 months, have you experienced pain, aching, stiffness, or swelling in or around the joints (e.g., in arms, hands, legs, or feet), which were not related to an injury and lasted for more than a month? 2. During the last 12 months, have you experienced stiffness in the joints in the morning after getting up from bed or after a long rest of the joints without movement? 3. Did this stiffness last for less than 30 min? 4. Did this stiffness go away after exercise or movement in the joints? |
| Asthma | Have you ever been diagnosed with asthma (an allergic respiratory disease)? | 1. During the last 12 months, have you experienced attacks of wheezing or whistling breathing? (Yes) AND 2. “Yes” to at least one of the following (past 12 months): (a) Have you experienced an attack of wheezing that came on after you stopped exercising or some other physical activity? (b) Have you had a feeling of tightness in your chest? (c) Have you woken up with a feeling of tightness in your chest in the morning or any other time? (d) Have you had an attack of shortness of breath that came on without an obvious cause when you were not exercising or doing some physical activity? |
| Chronic lung disease | Have you ever been diagnosed with chronic lung disease (emphysema, bronchitis, COPD)? | 1. During the last 12 months, have you experienced any shortness of breath at rest (while awake)? (Yes) OR 2. “Yes” to both of the following (past 12 months): (a) Have you experienced any coughing or wheezing for 10 min or more at a time? (b) Have you experienced any coughing up of sputum or phlegm on most days of the month for at least 3 months? |
| Diabetes | Have you ever been diagnosed with diabetes (high blood sugar)? (Not including diabetes associated with a pregnancy) | NA |
| Hypertension | Have you ever been diagnosed with high blood pressure (hypertension)? | Blood pressure was measured three times with a one-minute interval with the use of a wrist blood pressure monitor (Medistar Wrist Blood Pressure Model S) and the mean value of the three measurements was calculated. Hypertension was defined as having at least one of the following: systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg. |
| Stroke | Have you ever been told by a health professional that you have had a stroke? | NA |
References
- Barlow, D.H. The experience of anxiety: Shadow of intelligence or specter of death. In Anxiety and Its Disorders: The Nature and Treatment of Anxiety and Panic, 2nd ed.; Guilford Press: New York, NY, USA, 2002; pp. 1–36. [Google Scholar]
- Yang, X.; Fang, Y.; Chen, H.; Zhang, T.; Yin, X.; Man, J.; Yang, L.; Lu, M. Global, regional and national burden of anxiety disorders from 1990 to 2019: Results from the Global Burden of Disease Study 2019. Epidemiol. Psychiatr. Sci. 2021, 30, e36. [Google Scholar] [CrossRef]
- Canuto, A.; Weber, K.; Baertschi, M.; Andreas, S.; Volkert, J.; Dehoust, M.C.; Sehner, S.; Suling, A.; Wegscheider, K.; Ausín, B. Anxiety disorders in old age: Psychiatric comorbidities, quality of life, and prevalence according to age, gender, and country. Am. J. Geriatr. Psychiatry 2018, 26, 174–185. [Google Scholar] [CrossRef]
- Kirmizioglu, Y.; Doğan, O.; Kuğu, N.; Akyüz, G. Prevalence of anxiety disorders among elderly people. Int. J. Geriatr. Psychiatry 2009, 24, 1026–1033. [Google Scholar] [CrossRef]
- Miloyan, B.; Pachana, N.A. Clinical significance of worry and physical symptoms in late-life generalized anxiety disorder. Int. J. Geriatr. Psychiatry 2015, 30, 1186–1194. [Google Scholar] [CrossRef] [PubMed]
- Norton, J.; Ancelin, M.L.; Stewart, R.; Berr, C.; Ritchie, K.; Carrière, I. Anxiety symptoms and disorder predict activity limitations in the elderly. J. Affect. Disord. 2012, 141, 276–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolitzky-Taylor, K.B.; Castriotta, N.; Lenze, E.J.; Stanley, M.A.; Craske, M.G. Anxiety disorders in older adults: A comprehensive review. Depress. Anxiety 2010, 27, 190–211. [Google Scholar] [CrossRef] [PubMed]
- Carriere, I.; Ryan, J.; Norton, J.; Scali, J.; Stewart, R.; Ritchie, K.; Ancelin, M.L. Anxiety and mortality risk in community-dwelling elderly people. Br. J. Psychiatry 2013, 203, 303–309. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization Global Health and Aging. Available online: https://www.who.int/ageing/publications/global_health.pdf (accessed on 13 September 2021).
- Mascayano, F.; Armijo, J.E.; Yang, L.H. Addressing stigma relating to mental illness in low-and middle-income countries. Front. Psychiatry 2015, 6, 38. [Google Scholar] [CrossRef] [Green Version]
- Willadsen, T.G.; Siersma, V.; Nicolaisdottir, D.R.; Jarbol, D.; Guassora, A.D.; Reventlow, S.; Køster-Rasmussen, R. Symptom burden in multimorbidity: A population-based combined questionnaire and registry study from Denmark. BMJ Open 2021, 11, e041877. [Google Scholar] [CrossRef]
- Jindai, K.; Nielson, C.M.; Vorderstrasse, B.A.; Quiñones, A.R. Peer reviewed: Multimorbidity and functional limitations among adults 65 or older, NHANES 2005–2012. Prev. Chronic Dis. 2016, 13. [Google Scholar] [CrossRef] [Green Version]
- NICE | The National Institute for Health and Care Excellence Multimorbidity and Polypharmacy. Available online: https://www.nice.org.uk/advice/ktt18/resources/multimorbidity-and-polypharmacy-pdf-58757959453381 (accessed on 13 September 2021).
- Gould, C.E.; O’Hara, R.; Goldstein, M.K.; Beaudreau, S.A. Multimorbidity is associated with anxiety in older adults in the Health and Retirement Study. Int. J. Geriatr. Psychiatry 2016, 31, 1105–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vancampfort, D.; Koyanagi, A.; Hallgren, M.; Probst, M.; Stubbs, B. The relationship between chronic physical conditions, multimorbidity and anxiety in the general population: A global perspective across 42 countries. Gen. Hosp. Psychiatry 2017, 45, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization Chronic Diseases in Low and Middle Income Countries. Available online: https://www.who.int/chp/chronic_disease_report/media/Factsheet3.pdf (accessed on 2 September 2021).
- Kowal, P.; Chatterji, S.; Naidoo, N.; Biritwum, R.; Fan, W.; Lopez Ridaura, R.; Maximova, T.; Arokiasamy, P.; Phaswana-Mafuya, N.; Williams, S. Data resource profile: The World Health Organization Study on global AGEing and adult health (SAGE). Int. J. Epidemiol. 2012, 41, 1639–1649. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Stubbs, B.; Hallgren, M.; Veronese, N.; Mugisha, J.; Probst, M.; Koyanagi, A. Correlates of physical activity among community-dwelling individuals aged 65 years or older with anxiety in six low-and middle-income countries. Int. Psychogeriatr. 2018, 30, 705. [Google Scholar] [CrossRef]
- Vancampfort, D.; Stubbs, B.; Herring, M.P.; Hallgren, M.; Koyanagi, A. Sedentary behavior and anxiety: Association and influential factors among 42,469 community-dwelling adults in six low-and middle-income countries. Gen. Hosp. Psychiatry 2018, 50, 26–32. [Google Scholar] [CrossRef] [Green Version]
- Freeman, E.E.; Roy-Gagnon, M.; Samson, E.; Haddad, S.; Aubin, M.; Vela, C.; Zunzunegui, M.V. The global burden of visual difficulty in low, middle, and high income countries. PLoS ONE 2013, 8, e63315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arokiasamy, P.; Kowal, P.; Capistrant, B.D.; Gildner, T.E.; Thiele, E.; Biritwum, R.B.; Yawson, A.E.; Mensah, G.; Maximova, T.; Wu, F. Chronic noncommunicable diseases in 6 low-and middle-income countries: Findings from wave 1 of the World Health Organization’s study on global Ageing and adult health (SAGE). Am. J. Epidemiol. 2017, 185, 414–428. [Google Scholar] [CrossRef]
- Garin, N.; Koyanagi, A.; Chatterji, S.; Tyrovolas, S.; Olaya, B.; Leonardi, M.; Lara, E.; Koskinen, S.; Tobiasz-Adamczyk, B.; Ayuso-Mateos, J.L. Global multimorbidity patterns: A cross-sectional, population-based, multi-country study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 205–214. [Google Scholar] [CrossRef] [Green Version]
- Rose, G.A. The diagnosis of ischaemic heart pain and intermittent claudication in field surveys. Bull. World Health Organ. 1962, 27, 645. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Koyanagi, A.; Lara, E.; Stubbs, B.; Carvalho, A.F.; Oh, H.; Stickley, A.; Veronese, N.; Vancampfort, D. Chronic physical conditions, multimorbidity, and mild cognitive impairment in low-and middle-income countries. J. Am. Geriatr. Soc. 2018, 66, 721–727. [Google Scholar] [CrossRef]
- Koyanagi, A.; Garin, N.; Olaya, B.; Ayuso-Mateos, J.L.; Chatterji, S.; Leonardi, M.; Koskinen, S.; Tobiasz-Adamczyk, B.; Haro, J.M. Chronic conditions and sleep problems among adults aged 50 years or over in nine countries: A multi-country study. PLoS ONE 2014, 9, e114742. [Google Scholar]
- Binder, K.W.; Wrzesińska, M.A.; Kocur, J. Anxiety in persons with visual impairment. Psychiatr. Pol. 2020, 54, 279–288. [Google Scholar] [CrossRef] [PubMed]
- American Lung Association Coping with COPD and Anxiety. Available online: https://www.lung.org/blog/coping-with-copd-and-anxiety (accessed on 13 September 2021).
- Burvill, P.W.; Johnson, G.A.; Jamrozik, K.D.; Anderson, C.S.; Stewart-Wynne, E.G.; Chakera, T. Anxiety disorders after stroke: Results from the Perth Community Stroke Study. Br. J. Psychiatry 1995, 166, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Leppävuori, A.; Pohjasvaara, T.; Vataja, R.; Kaste, M.; Erkinjuntti, T. Generalized anxiety disorders three to four months after ischemic stroke. Cerebrovasc. Dis. 2003, 16, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Chun, H.Y.; Whiteley, W.N.; Dennis, M.S.; Mead, G.E.; Carson, A.J. Anxiety after stroke: The importance of subtyping. Stroke 2018, 49, 556–564. [Google Scholar] [CrossRef]
- Anxiety and Depression Association of America Chronic Pain. Available online: https://adaa.org/understanding-anxiety/related-illnesses/other-related-conditions/chronic-pain (accessed on 13 September 2021).
- Taylor, D.J.; Lichstein, K.L.; Durrence, H.H.; Reidel, B.W.; Bush, A.J. Epidemiology of insomnia, depression, and anxiety. Sleep 2005, 28, 1457–1464. [Google Scholar] [CrossRef]
- Backe, I.F.; Patil, G.G.; Nes, R.B.; Clench-Aas, J. The relationship between physical functional limitations, and psychological distress: Considering a possible mediating role of pain, social support and sense of mastery. SSM-Popul. Health 2018, 4, 153–163. [Google Scholar] [CrossRef]
- Gapstur, R.L. Symptom burden: A concept analysis and implications for oncology nurses. Oncol. Nurs. Forum 2007, 34, 673–680. [Google Scholar] [CrossRef] [Green Version]
- Cavalcanti, G.; Doring, M.; Portella, M.R.; Bortoluzzi, E.C.; Mascarelo, A.; Dellani, M.P. Multimorbidity associated with polypharmacy and negative self-perception of health. Rev. Bras. Geriatr. Gerontol. 2017, 20, 634–642. [Google Scholar] [CrossRef] [Green Version]
- Ziere, G.; Dieleman, J.P.; Hofman, A.; Pols, H.A.; Van Der Cammen, T.; Stricker, B.C. Polypharmacy and falls in the middle age and elderly population. Br. J. Clin. Pharmacol. 2006, 61, 218–223. [Google Scholar] [CrossRef] [Green Version]
- Sindi, S.; Pérez, L.M.; Vetrano, D.L.; Triolo, F.; Kåreholt, I.; Sjöberg, L.; Darin-Mattsson, A.; Kivipelto, M.; Inzitari, M.; Calderón-Larrañaga, A. Sleep disturbances and the speed of multimorbidity development in old age: Results from a longitudinal population-based study. BMC Med. 2020, 18, 382. [Google Scholar] [CrossRef]
- Kankeu, H.T.; Saksena, P.; Xu, K.; Evans, D.B. The financial burden from non-communicable diseases in low-and middle-income countries: A literature review. Health Res. Policy Syst. 2013, 11, 31. [Google Scholar] [CrossRef] [PubMed]
- Anker, J.J.; Kushner, M.G. Co-occurring alcohol use disorder and anxiety: Bridging psychiatric, psychological, and neurobiological perspectives. Alcohol. Res. Curr. Rev. 2019, 40. [Google Scholar] [CrossRef] [PubMed]
- Nanthakumar, C. Yoga for anxiety and depression—A literature review. J. Ment. Health Train. Educ. Pract. 2020, 3, 157–169. [Google Scholar] [CrossRef]
- Kubo, A.; Hung, Y.; Ritterman, J. Yoga for heart failure patients: A feasibility pilot study with a multiethnic population. Int. J. Yoga Therap. 2011, 21, 77–83. [Google Scholar] [CrossRef]
- Vogelzangs, N.; Beekman, A.; De Jonge, P.; Penninx, B. Anxiety disorders and inflammation in a large adult cohort. Transl. Psychiatry 2013, 3, e249. [Google Scholar] [CrossRef] [Green Version]
- Moussavi, S.; Chatterji, S.; Verdes, E.; Tandon, A.; Patel, V.; Ustun, B. Depression, chronic diseases, and decrements in health: Results from the World Health Surveys. Lancet 2007, 370, 851–858. [Google Scholar] [CrossRef]



| Characteristic | Overall | China | Ghana | India | Mexico | Russia | South Africa | |
|---|---|---|---|---|---|---|---|---|
| Anxiety symptoms | Yes | 8.1 | 0.7 | 7.1 | 17.8 | 5.2 | 4.4 | 9.4 |
| No. of chronic | 0 | 22.2 | 22.1 | 21.6 | 27.0 | 12.8 | 15.3 | 11.1 |
| conditions | 1 | 32.3 | 38.9 | 43.3 | 29.7 | 43.9 | 21.4 | 45.8 |
| 2 | 22.4 | 22.7 | 24.3 | 21.4 | 23.9 | 23.6 | 21.6 | |
| 3 | 12.2 | 10.0 | 7.9 | 12.2 | 11.1 | 16.8 | 12.7 | |
| 4 | 6.4 | 4.2 | 2.0 | 5.7 | 5.0 | 12.2 | 5.7 | |
| ≥ 5 | 4.6 | 2.2 | 0.8 | 4.0 | 3.3 | 10.8 | 3.1 | |
| Age (years) | Mean (SD) | 62.4 (16.0) | 62.6 (16.7) | 64.4 (19.9) | 61.5 (13.7) | 63.0 (18.9) | 63.9 (15.4) | 61.6 (18.4) |
| Sex | Female | 52.1 | 50.2 | 47.6 | 49.0 | 53.2 | 61.1 | 55.9 |
| Education | ≤ Primary | 57.4 | 63.0 | 75.3 | 76.1 | 79.6 | 7.5 | 71.4 |
| Secondary | 35.2 | 32.5 | 21.1 | 18.8 | 12.3 | 74.2 | 22.8 | |
| Tertiary | 7.4 | 4.5 | 3.6 | 5.1 | 8.1 | 18.2 | 5.7 | |
| Depression | Yes | 6.0 | 1.1 | 7.2 | 12.9 | 10.8 | 3.5 | 3.0 |
| Angina | Yes | 17.6 | 9.4 | 12.8 | 17.0 | 6.7 | 37.3 | 8.9 |
| Arthritis | Yes | 29.5 | 26.7 | 26.2 | 27.9 | 14.5 | 38.2 | 30.6 |
| Asthma | Yes | 7.9 | 4.3 | 5.0 | 12.5 | 4.9 | 6.5 | 7.7 |
| Chronic back pain | Yes | 8.6 | 5.6 | 7.5 | 9.6 | 8.4 | 13.0 | 5.7 |
| Chronic lung disease | Yes | 15.8 | 11.3 | 3.7 | 17.2 | 13.2 | 24.4 | 7.4 |
| Diabetes | Yes | 6.8 | 6.6 | 3.8 | 6.9 | 17.6 | 7.0 | 9.2 |
| Edentulism | Yes | 12.9 | 9.1 | 3.0 | 15.1 | 21.7 | 18.1 | 8.5 |
| Hearing problems | Yes | 5.6 | 5.5 | 2.9 | 5.6 | 9.3 | 6.1 | 5.0 |
| Hypertension | Yes | 55.0 | 60.6 | 59.6 | 37.5 | 61.9 | 72.1 | 78.3 |
| Stroke | Yes | 3.0 | 3.0 | 2.8 | 2.0 | 4.3 | 4.8 | 4.0 |
| Visual impairment | Yes | 1.3 | 0.5 | 1.0 | 2.4 | 0.8 | 0.9 | 0.8 |
| Age | Sex | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of | Overall | 50–64 Years | ≥ 65 Years | Male | Female | |||||
| Chronic Conditions | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI |
| 0 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||
| 1 | 1.12 | (0.87, 1.44) | 1.05 | (0.72, 1.53) | 1.35 | (0.82, 2.23) | 1.17 | (0.76, 1.82) | 1.07 | (0.78, 1.48) |
| 2 | 1.47 * | (1.08, 1.98) | 1.49 * | (1.04, 2.14) | 1.54 | (0.97, 2.46) | 1.81 * | (1.10, 2.99) | 1.28 | (0.87, 1.89) |
| 3 | 2.46 *** | (1.74, 3.47) | 2.45 *** | (1.57, 3.83) | 2.72 *** | (1.50, 4.92) | 3.65 *** | (2.14, 6.22) | 1.93 ** | (1.26, 2.95) |
| 4 | 3.04 *** | (2.15, 4.30) | 2.32 ** | (1.38, 3.88) | 3.74 *** | (2.32, 6.03) | 3.19 *** | (1.82, 5.57) | 2.89 *** | (1.88, 4.43) |
| ≥5 | 4.70 *** | (2.99, 7.38) | 6.89 *** | (3.48, 13.63) | 4.07 *** | (2.27, 7.29) | 4.94 *** | (2.69, 9.06) | 4.53 *** | (2.38, 8.62) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, L.; López Sánchez, G.F.; Shin, J.I.; Soysal, P.; Veronese, N.; Kostev, K.; Jacob, L.; Oh, H.; Schuch, F.; Butler, L.; et al. Multimorbidity and Anxiety Symptoms among Adults Aged 50 Years and Over from Six Low- and Middle-Income Countries. J. Ageing Longev. 2021, 1, 36-47. https://doi.org/10.3390/jal1010005
Smith L, López Sánchez GF, Shin JI, Soysal P, Veronese N, Kostev K, Jacob L, Oh H, Schuch F, Butler L, et al. Multimorbidity and Anxiety Symptoms among Adults Aged 50 Years and Over from Six Low- and Middle-Income Countries. Journal of Ageing and Longevity. 2021; 1(1):36-47. https://doi.org/10.3390/jal1010005
Chicago/Turabian StyleSmith, Lee, Guillermo F. López Sánchez, Jae Il Shin, Pinar Soysal, Nicola Veronese, Karel Kostev, Louis Jacob, Hans Oh, Felipe Schuch, Laurie Butler, and et al. 2021. "Multimorbidity and Anxiety Symptoms among Adults Aged 50 Years and Over from Six Low- and Middle-Income Countries" Journal of Ageing and Longevity 1, no. 1: 36-47. https://doi.org/10.3390/jal1010005