
An Interdisciplinary Approach to Biobanking in Cardiac Surgery: Protocol of a Prospective, Single-Center Research Project Involving Longitudinal Biobanking

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Cardiovascular Biobanking at the University Hospital Augsburg
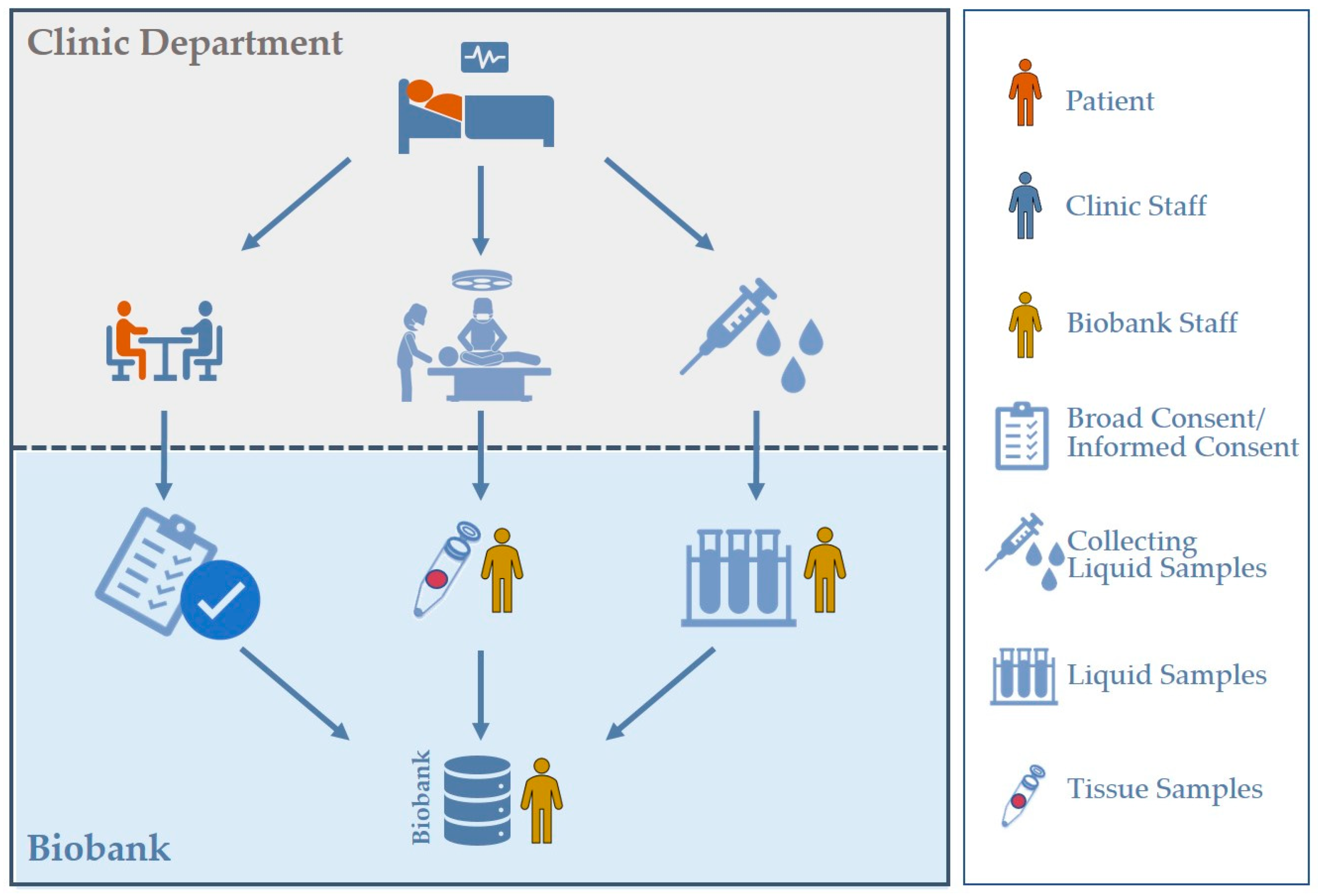
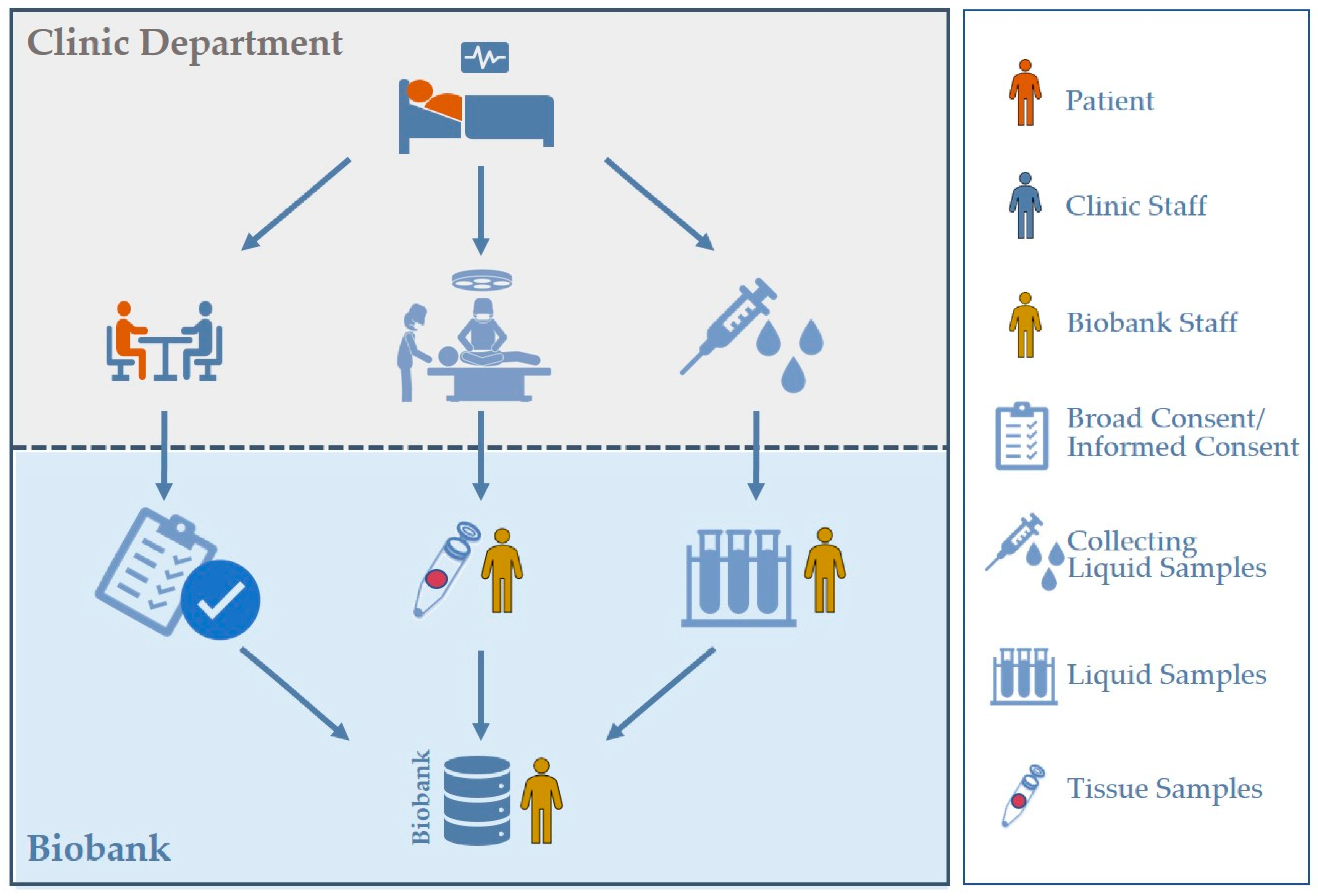
2.1. Broad Consent
2.2. The A-CaRe Protocol for Collection, Processing and Long-Term Storage of Liquid and Tissue Samples
2.3. Longitudinal Biobanking
2.4. Number of Aliquots Obtained and Stored
3. The AortOmics Trial
3.1. Background
3.2. Objectives
3.3. Study Design
3.4. Timeline
3.5. Formal Analysis
4. Outlook
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [PubMed]
- Townsend, N.; Kazakiewicz, D.; Lucy Wright, F.; Timmis, A.; Huculeci, R.; Torbica, A.; Gale, C.P.; Achenbach, S.; Weidinger, F.; Vardas, P. Epidemiology of cardiovascular disease in Europe. Nat. Rev. Cardiol. 2022, 19, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, G.; Bursi, F.; Faggiano, A.; Moscardelli, S.; Simeoli, P.S.; Guazzi, M.; Lorusso, R.; Carugo, S.; Faggiano, P. The Global Burden of Valvular Heart Disease: From Clinical Epidemiology to Management. J. Clin. Med. 2023, 12, 2178. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Coppola, L.; Cianflone, A.; Grimaldi, A.M.; Incoronato, M.; Bevilacqua, P.; Messina, F.; Baselice, S.; Soricelli, A.; Mirabelli, P.; Salvatore, M. Biobanking in health care: Evolution and future directions. J. Transl. Med. 2019, 17, 172. [Google Scholar] [CrossRef] [PubMed]
- Malsagova, K.; Kopylov, A.; Stepanov, A.; Butkova, T.; Sinitsyna, A.; Izotov, A.; Kaysheva, A. Biobanks-A Platform for Scientific and Biomedical Research. Diagnostics 2020, 10, 485. [Google Scholar] [CrossRef]
- Zhu, Y.; Jackson, D.; Hunter, B.; Beattie, L.; Turner, L.; Hambly, B.D.; Jeremy, R.W.; Malecki, C.; Robertson, E.N.; Li, A.; et al. Models of cardiovascular surgery biobanking to facilitate translational research and precision medicine. ESC Heart Fail. 2022, 9, 21–30. [Google Scholar] [CrossRef]
- Lee, J.E.; Kim, Y.Y. Impact of Preanalytical Variations in Blood-Derived Biospecimens on Omics Studies: Toward Precision Biobanking? Omics 2017, 21, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Dollé, L.; Bekaert, S. High-Quality Biobanks: Pivotal Assets for Reproducibility of OMICS-Data in Biomedical Translational Research. Proteomics 2019, 19, e1800485. [Google Scholar] [CrossRef]
- Sens, A.; Rischke, S.; Hahnefeld, L.; Dorochow, E.; Schäfer, S.M.G.; Thomas, D.; Köhm, M.; Geisslinger, G.; Behrens, F.; Gurke, R. Pre-analytical sample handling standardization for reliable measurement of metabolites and lipids in LC-MS-based clinical research. J. Mass. Spectrom. Adv. Clin. Lab. 2023, 28, 35–46. [Google Scholar] [CrossRef]
- Betsou, F.; Bilbao, R.; Case, J.; Chuaqui, R.; Clements, J.A.; De Souza, Y.; De Wilde, A.; Geiger, J.; Grizzle, W.; Guadagni, F.; et al. Standard PREanalytical Code Version 3.0. Biopreserv. Biobank. 2018, 16, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Iung, B.; Delgado, V.; Rosenhek, R.; Price, S.; Prendergast, B.; Wendler, O.; De Bonis, M.; Tribouilloy, C.; Evangelista, A.; Bogachev-Prokophiev, A.; et al. Contemporary Presentation and Management of Valvular Heart Disease: The EURObservational Research Programme Valvular Heart Disease II Survey. Circulation 2019, 140, 1156–1169. [Google Scholar] [CrossRef] [PubMed]
- Katz, A.M.; Rolett, E.L. Heart failure: When form fails to follow function. Eur. Heart J. 2016, 37, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Thorac. Cardiovasc. Surg. 2021, 77, 450–500. [Google Scholar]
- Seldrum, S.; de Meester, C.; Pierard, S.; Pasquet, A.; Lazam, S.; Boulif, J.; Vanoverschelde, J.L.; Gerber, B.L. Assessment of Left Ventricular Reverse Remodeling by Cardiac MRI in Patients Undergoing Repair Surgery for Severe Aortic or Mitral Regurgitation. J. Cardiothorac. Vasc. Anesth. 2019, 33, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Krayenbuehl, H.P.; Hess, O.M.; Monrad, E.S.; Schneider, J.; Mall, G.; Turina, M. Left ventricular myocardial structure in aortic valve disease before, intermediate, and late after aortic valve replacement. Circulation 1989, 79, 744–755. [Google Scholar] [CrossRef] [PubMed]
- Villari, B.; Sossalla, S.; Ciampi, Q.; Petruzziello, B.; Turina, J.; Schneider, J.; Turina, M.; Hess, O.M. Persistent diastolic dysfunction late after valve replacement in severe aortic regurgitation. Circulation 2009, 120, 2386–2392. [Google Scholar] [CrossRef] [PubMed]
- Sutton, M.; Plappert, T.; Spiegel, A.; Raichlen, J.; Douglas, P.; Reichek, N.; Edmunds, L. Early postoperative changes in left ventricular chamber size, architecture, and function in aortic stenosis and aortic regurgitation and their relation to intraoperative changes in afterload: A prospective two-dimensional echocardiographic study. Circulation 1987, 76, 77–89. [Google Scholar] [CrossRef]
- Vollema, E.M.; Singh, G.K.; Prihadi, E.A.; Regeer, M.V.; Ewe, S.H.; Ng, A.C.; Mertens, B.J.; Klautz, R.J.; Ajmone Marsan, N.; Bax, J.J.; et al. Time course of left ventricular remodelling and mechanics after aortic valve surgery: Aortic stenosis vs. aortic regurgitation. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 1105–1111. [Google Scholar] [CrossRef]
- Rank, N.; Stoiber, L.; Nasser, M.; Tanacli, R.; Stehning, C.; Knierim, J.; Schoenrath, F.; Pieske, B.; Falk, V.; Kuehne, T.; et al. Assessment of 10-Year Left-Ventricular-Remodeling by CMR in Patients Following Aortic Valve Replacement. Front. Cardiovasc. Med. 2021, 8, 645693. [Google Scholar] [CrossRef] [PubMed]
- Petersen, J.; Kloth, B.; Iqbal, S.; Reichenspurner, H.; Geelhoed, B.; Schnabel, R.; Eschenhagen, T.; Christ, T.; Girdauskas, E. Blunted beta-adrenoceptor-mediated inotropy in valvular cardiomyopathy: Another piece of the puzzle in human aortic valve disease. Eur. J. Cardiothorac. Surg. 2021, 60, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, Y.; Benjamini, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. 1995, 57, 289–300. [Google Scholar]

{kind=link}
| Type of Liquid Sample | Number of Aliquots |
|---|---|
| EDTA plasma | 3915 |
| Citrate plasma | 2728 |
| Serum | 3223 |
| EDTA buffy coat | 1005 |
| RNA-PAXgene® | 429 |
| Type of Tissue | Number of Aliquots |
|---|---|
| Aortic arch | 87 |
| Ascending aorta, greater curvature | 256 |
| Ascending aorta, lesser curvature | 139 |
| Aortic root | 141 |
| Aortic valve leaflet | 852 |
| Anterior mitral valve leaflet | 133 |
| Posterior mitral valve leaflet | 61 |
| Chordae tendineae | 121 |
| Papillary muscle | 29 |
| Left atrium | 20 |
| Left atrial appendage | 6 |
| Left ventricle | 25 |
| Left ventricular outflow tract | 11 |
| Pulmonary artery | 13 |
| Pulmonary valve | 6 |
| Tricuspid valve | 10 |
| Right atrium | 17 |
| Right ventricle | 6 |
| Right ventricular outflow tract | 6 |
| Pericardium | 190 |
| Epicardial adipose tissue | 1046 |
| Left internal mammary artery | 142 |
| Right internal mammary artery | 51 |
| Radial artery | 15 |
| Saphenous vein | 226 |
| Thymus gland | 273 |
| Tumor | 28 |
| Other non-specified tissue | 198 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holst, T.; Langer, A.; Sequeira Gross, T.M.; Abdelmoteleb, N.; Miskovic, V.; Müller, L.; Stock, S.; Märkl, B.; Girdauskas, E. An Interdisciplinary Approach to Biobanking in Cardiac Surgery: Protocol of a Prospective, Single-Center Research Project Involving Longitudinal Biobanking. Int. J. Transl. Med. 2024, 4, 238-246. https://doi.org/10.3390/ijtm4020014
Holst T, Langer A, Sequeira Gross TM, Abdelmoteleb N, Miskovic V, Müller L, Stock S, Märkl B, Girdauskas E. An Interdisciplinary Approach to Biobanking in Cardiac Surgery: Protocol of a Prospective, Single-Center Research Project Involving Longitudinal Biobanking. International Journal of Translational Medicine. 2024; 4(2):238-246. https://doi.org/10.3390/ijtm4020014
Chicago/Turabian StyleHolst, Theresa, Angela Langer, Tatiana M. Sequeira Gross, Noureldin Abdelmoteleb, Valentina Miskovic, Lisa Müller, Sina Stock, Bruno Märkl, and Evaldas Girdauskas. 2024. "An Interdisciplinary Approach to Biobanking in Cardiac Surgery: Protocol of a Prospective, Single-Center Research Project Involving Longitudinal Biobanking" International Journal of Translational Medicine 4, no. 2: 238-246. https://doi.org/10.3390/ijtm4020014
APA StyleHolst, T., Langer, A., Sequeira Gross, T. M., Abdelmoteleb, N., Miskovic, V., Müller, L., Stock, S., Märkl, B., & Girdauskas, E. (2024). An Interdisciplinary Approach to Biobanking in Cardiac Surgery: Protocol of a Prospective, Single-Center Research Project Involving Longitudinal Biobanking. International Journal of Translational Medicine, 4(2), 238-246. https://doi.org/10.3390/ijtm4020014