
A Randomised, Double-Blind, Placebo-Controlled Trial Evaluating Concentrated Phytochemical-Rich Nutritional Capsule in Addition to a Probiotic Capsule on Clinical Outcomes among Individuals with COVID-19—The UK Phyto-V Study

 ,
, 
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
- Probiotic/prebiotic capsule (PP): The daily dose (from two capsules) was 200 mg of inulin and 10 billion colony forming units (CFU’s) of Lactobacillus plantarum, Lactobacillus rhamnosus, Lactobacillus bulgaricus, Lactococcus lactis and Lactobacillus paracasei. The delayed release vegan capsule was made of hypromellose and gellan.
- Phytochemical-rich whole food capsule (PC): Citrus Sinensis fruit (400 mg from 200 mg of 2:1 extract, standardised to contain 70 mg of Bioflavonoids). Chamomile, Matricaria recutita L. flower) (1000 mg from 22 mg of 10:1 extract and 65 mg of 12:1 extract). Curcuma Longa rhizome in Curcumin Complex (1600 mg of curcumin from 25 mg of 64:1 extract, standardised to contain 23.8 mg of curcuminoid). Pomegranate (Punica granatum L. rinds and seeds) (1000 mg from 25 mg of 40:1 extract, standardised to contain 10 mg of Ellagic Acid). Polygonum cuspidatum root containing 100 mg of resveratrol.
- Placebo (P): Inert microcrystalline cellulose, magnesium stearate and silicon dioxide.
- Capsule manufacture and quality assurance: The capsules and their contents were made specifically for this trial by ParkAcre, Lincoln, and The Oxford Health Company Ltd., Oxfordshire, UK, both certified by the Organic Food Federation to conform to Good Manufacturing Practice (GMP—FSSC 22000, ISO 22000), and UK and International food production laws. Their in-house Research and Development department tested each batch for biological contamination of yeast, mould, E. coli and salmonella, and measured lead, arsenic, cadmium, mercury and pesticides, to ensure that they met international thresholds. A unit of each supplement was securely stored by the Trust Secretary and can be sent to any regulatory body at their request.
3. Results
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| DAYTIME COUGH |
| 0 → No cough during the day |
| 1 → Cough for one short period |
| 2 → Cough for more than two short periods |
| 3 → Frequent coughing, which did not interfere with usual daytime activities |
| 4 → Frequent coughing, which did interfere with usual daytime activities |
| 5 → Distressing coughs most of the day |
| NIGHT TIME COUGH |
| 0 → No cough during the night |
| 1 → Cough on waking only |
| 2 → Wake once or early due to cough |
| 3 → Frequent waking due to choughs |
| 4 → Frequent coughs most of the night |
| 5 → Distressing coughs preventing any sleep |
| Subjective Well-Being (SWB) |
|---|
| Overall, how satisfied are you with your life nowadays? 0 → 1 → 2 → 3 → 4 → 5 → 6 → 7 → 8 → 9 → 10 Not at all Completely |
| Overall, to what extent do you feel that the things you do in your life are worthwhile? 0 → 1 → 2 → 3 → 4 → 5 → 6 → 7 → 8 → 9 → 10 Not at all Completely |
| Overall, how happy did you feel yesterday? 0 → 1 → 2 → 3 → 4 → 5 → 6 → 7 → 8 → 9 → 10 Not at all Completely |
| Overall, how anxious did you feel yesterday? 0 → 1 → 2 → 3 → 4 → 5 → 6 → 7 → 8 → 9 → 10 Not at all Completely |
References
- Conlon, M.A.; Bird, A.R. The Impact of Diet and Lifestyle on Gut Microbiota and Human Health. Nutrients 2015, 7, 17–44. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Gu, J.; Hou, P.; Zhang, L.; Bai, Y.; Guo, Z.; Wu, H.; Zhang, B.; Li, P.; Zhao, X. Incidence, clinical characteristics and prognostic factor of patients with COVID-19: A systematic review and meta-analysis. MedRxIV 2020, 72. [Google Scholar] [CrossRef]
- Thomas, C.M.; Versalovic, J. Probiotics-host communication: Modulation of signaling pathways in the intestine. Gut Microbes 2010, 1, 148–163. [Google Scholar] [CrossRef] [PubMed]
- Kurian, S.J.; Unnikrishnan, M.K.; Miraj, S.S.; Bagchi, D.; Banerjee, M.; Reddy, B.S.; Rodrigues, G.S.; Manu, M.K.; Saravu, K.; Mukopadhyay, C.; et al. Probiotics in Prevention and Treatment of COVID-19: Current Perspective and Future Prospects. Arch. Med. Res. 2021, 52, 582–594. [Google Scholar] [CrossRef] [PubMed]
- Budden, K.F.; Gellatly, S.L.; Wood, D.L.A.; Cooper, M.A.; Morrison, M.; Hugenholtz, P.; Hansbro, P.M. Emerging pathogenic links between microbiota and the gut-lung axis. Nat. Rev. Microbiol. 2016, 15, 55–63. [Google Scholar] [CrossRef]
- Yeoh, Y.K.; Zuo, T.; Lui, G.C.Y.; Zhang, F.; Liu, Q.; Li, A.Y.L.; Chung, A.C.K.; Chung, C.P.; Tso, E.Y.K.; Fung, K.S.C.; et al. Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. Gut 2021, 70, 698–706. [Google Scholar] [CrossRef]
- Xu, K.; Cai, H.; Shen, Y.; Ni, Q.; Chen, Y.; Hu, S.; Li, J.; Wang, H.; Yu, L.; Huang, H.; et al. Management of coronavirus disease-19 (COVID-19): The Zhejiang experience. J. Zhejiang Univ. Med. Sci. 2020, 49, 147–157. [Google Scholar]
- Chen, Y.; Gu, S.; Chen, Y.; Lu, H.; Shi, D.; Guo, J.; Wu, W.R.; Yang, Y.; Li, Y.; Xu, K.J.; et al. Six-month follow-up of gut microbiota richness in patients with COVID-19. Gut 2021, 71, 222–225. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-Month consequences of COVID-19 in patients discharged from Hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Gu, S.; Chen, Y.; Wu, Z.; Chen, Y.; Gao, H.; Lv, L.; Guo, F.; Zhang, X.; Luo, R.; Huang, C.; et al. Alterations of the Gut Microbiota in Patients with Coronavirus Disease or H1N1 Influenza. Clin. Infect. Dis. 2020, 71, 2669–2678. [Google Scholar] [CrossRef]
- Ng, S.C.; Tilg, H. COVID-19 and the gastrointestinal tract: More than meets the eye. Gut 2020, 69, 973–974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, C.-L.; Smith, B.J.; Lo, D.-F.; Chyu, M.-C.; Dunn, D.M.; Chen, C.-H.; Kwun, I.-S. Dietary polyphenols and mechanisms of osteoarthritis. J. Nutr. Biochem. 2012, 23, 1367–1377. [Google Scholar] [CrossRef]
- Dhar, D.; Mohanty, A. Gut microbiota and Covid-19-possible link and implications. Virus Res. 2020, 285, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhu, L.; Qin, S. Gut microbiota modulation on intestinal mucosal adaptive immunity. J. Immunol. Res. 2019, 47, 47–54. [Google Scholar] [CrossRef]
- Lin, C.W.; Tsai, F.J.; Tsai, C.H.; Lai, C.C.; Wan, L.; Ho, T.Y.; Hsieh, C.C.; Chao, P.D.L. Anti-SARS coronavirus 3C-like protease effects of plant-derived phenolic compounds. Antivir. Res. 2005, 68, 36–42. [Google Scholar] [CrossRef]
- Olaimat, A.N.; Aolymat, I.; Al-Holy, M.; Ayyash, M.; Abu Ghoush, M.; Al-Nabulsi, A.A.; Osaili, T.; Apostolopoulos, V.; Liu, S.Q.; Shah, N.P. The potential application of probiotics and prebiotics for the prevention and treatment of COVID-19. Nature 2020, 4, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Dickson, R.P. The microbiome and critical illness. Lancet Respir. Med. 2016, 4, 59–72. [Google Scholar] [CrossRef] [Green Version]
- Uchide, N.; Toyoda, H. Antioxidant therapy as a potential approach to severe influenza-associated complications. Molecules 2011, 16, 2032–2052. [Google Scholar] [CrossRef] [Green Version]
- Enaud, R.; Prevel, R.; Ciarlo, E.; Beaufils, F.; Wieërs, G.; Guery, B.; Delhaes, L. The gut-lung axis in health and respiratory diseases: A place for inter-organ and inter-kingdom crosstalks. Front. Cell. Infect. Microbiol. 2020, 10, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Namasivayam, S.; Sher, A.; Glickman, M.S.; Wipperman, M.F. The Microbiome and Tuberculosis: Early Evidence for Cross Talk. Am. Soc. Microbiol. 2018, 9, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Fanos, V.; Pintus, M.C.; Pintus, R.; Marcialis, M.A. Lung microbiota in the acute respiratory disease: From coronavirus to metabolomics. J. Paediatr. Neonatal Individ. Med. 2020, 9, 90–99. [Google Scholar]
- Cecchini, R.; Cecchini, A.L. SARS-CoV-2 infection pathogenesis is related to oxidative stress as a response to aggression. Med. Hypotheses 2020, 11, 102–110. [Google Scholar] [CrossRef]
- Dumas, A.; Bernard, L.; Poquet, Y.; Lugo-Villarino, G.; Neyrolles, O. The role of the lung microbiota and the gut-lung axis in respiratory infectious diseases. Cell. Microbiol. 2018, 20, 129–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, Y.; Lie, J.; Shen, L.; Zou, Y.; Hou, L.; Zhu, L.; Faden, H.S.; Tang, Z.; Shi, M.; Jiao, N.; et al. Enteric involvement in hospitalised patients with COVID-19 outside Wuhan. Lancet Gastroenterol. Hepatol. 2020, 5, 534–535. [Google Scholar] [CrossRef]
- Reinold, J.; Farahpour, F.; Fehring, C.; Dolff, S.; Konik, M.; Korth, J.; Van Baal, L.; Hoffmann, D.; Buer, J.; Witzke, O.; et al. A Pro-Inflammatory Gut Microbiome Characterizes SARS-CoV-2 Infected Patients and a Reduction in the Connectivity of an Anti-Inflammatory Bacterial Network Associates with Severe COVID-19. Front. Cell Infect. Microbiol. 2021, 17, 747816. [Google Scholar] [CrossRef]
- Anand, S.; Mande, S. Diet, Microbiota and Gut-Lung Connection. Front. Microbiol. 2018, 9, 2147–2154. [Google Scholar] [CrossRef]
- Van Heul, A.; Planer, J.; Kau, A.L. The human microbiota and asthma. Clin. Rev. Allergy Immunol. 2019, 57, 350–363. [Google Scholar] [CrossRef]
- Mammen, M.; Sethi, S. COPD and the microbiome. Respiratory 2016, 21, 590–599. [Google Scholar] [CrossRef] [Green Version]
- Martinez, J.E.; Kahana, D.D.; Ghuman, S.; Wilson, H.P.; Wilson, J.; Kim, S.C.J.; Lagishetty, V.; Jacobs, J.P.; Sinha-Hikim, A.P.; Friedman, T.C. Unhealthy Lifestyle and Gut Dysbiosis: A Better Understanding of the Effects of Poor Diet and Nicotine on the Intestinal Microbiome. Front. Endocrinol. 2021, 12, 66–74. [Google Scholar] [CrossRef]
- Carlson, J.L.; Erickson, J.M.; Lloyd, B.B.; Slavin, J.L. Health Effects and Sources of Prebiotic Dietary Fibre. Curr. Dev. Nutr. 2018, 2, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Thomas, R.; Yang, D.; Zollman, C.; Williams, M. Phytochemicals in Cancer Management. Curr. Res. Complement. Altern. Med. 2017, 105, 1–14. [Google Scholar]
- Thomas, R.; Aldous, J.; Forsyth, R.; Chater, A.; Williams, M. The Influence of a blend of Probiotic Lactobacillus and Prebiotic Inulin on the Duration and Severity of Symptoms among Individuals with COVID-19. Infect. Dis. Diagn. Treat. 2021, 5, 1–14. [Google Scholar]
- Nobaek, S.; Johansson, M.L.; Molin, G.; Ahrne, S.; Jeppsson, B. Alteration of intestinal microflora is associated with reduction in abdominal bloating and pain in patients with irritable bowel syndrome. Am. J. Gastroenterol. 2000, 95, 1231–1238. [Google Scholar] [CrossRef]
- Azad, M.A.K.; Sarker, M.; Wan, D. Immunomodulatory Effects of Probiotics on Cytokine Profiles. BioMed Res. Int. 2018, 47, 86–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morshedi, M.; Hashemi, R.; Moazzen, S.; Sahebkar, A.; Hosseinifard, E.S. Immunomodulatory and anti-inflammatory effects of probiotics in multiple sclerosis: A systematic review. J. Neuroinflamm. 2019, 16, 1611–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlFaleh, K.; Anabrees, J. Probiotics for prevention of necrotizing enterocolitis in preterm infants. Cochrane Database Syst. Rev. 2014, 4, 584–671. [Google Scholar]
- Macfarlane, S.; Cleary, S.; Bahrami, B.; Reynolds, N.; Macfarlane, G.T. Synbiotic consumption changes the metabolism and composition of the gut microbiota in older people and modifies inflammatory processes: A randomised, double-blind, placebo-controlled crossover study. Aliment. Pharmacol. Ther. 2013, 38, 804–816. [Google Scholar] [CrossRef]
- Borruel, N.; Carol, M.; Casellas, F.; Antolin, M.; de Lara, F.; Epsin, E.; Naval, J.; Guarner, F.; Malagelda, J.R. Increased mucosal tumour necrosis factor alpha production in Crohn’s disease can be downregulated ex vivo by probiotic bacteria. Gut 2002, 51, 659–664. [Google Scholar] [CrossRef] [Green Version]
- Brito, M.B.; Diaz, J.P.; Muñoz-Quezada, S.; Llorente, C.G.; Gil, A. Probiotic mechanisms of action. Ann. Nutr. Metab. 2012, 61, 160–174. [Google Scholar] [CrossRef]
- Gill, H.S.; Rutherfurd, K.J.; Cross, M.L. Dietary probiotic supplementation enhances natural killer cell activity in the elderly: An investigation of age-related immunological changes. J. Clin. Immunol. 2001, 21, 264–271. [Google Scholar] [CrossRef]
- Plaza-Diaz, J.; Ruiz-Ojeda, F.J.; Gil-Campos, M.; Gil, A. Mechanisms of action of probiotics. Adv. Nutr. 2019, 10, 49–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingston, M.; Loach, D.; Wilson, M.; Tannock, G.W.; Baird, M. Gut commensal Lactobacillus reuteri 100-23 stimulates an immunoregulatory response. Immunol. Cell Biol. 2010, 88, 99–102. [Google Scholar] [CrossRef]
- Dehghan, P.; Gargari, B.P.; Jafarabadi, M.A.; Aliasgharzadeh, A. Inulin controls inflammation and metabolic endotoxemia in women with type 2 diabetes mellitus: A randomized-controlled clinical trial. Int. J. Food Sci. Nutr. 2014, 65, 65–117. [Google Scholar] [CrossRef] [PubMed]
- Gagliardi, A.; Totino, V.; Cacciotti, F.; Lebba, V.; Neroni, B.; Bonfiglio, G.; Trancassini, M.; Passariello, C.; Pantanella, F.; Schippa, S. Rebuilding the Gut Microbiota Ecosystem. Int. J. Environ. Res. Public Health 2018, 15, 1679–1689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishida, A.; Inoue, R.; Inatomi, O.; Bamba, S.; Naito, Y.; Andoh, A. Gut microbiota in the pathogenesis of inflammatory bowel disease. Clin. J. Gastroenterol. 2018, 11, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Gurung, M.; Li, Z.; You, H.; Rodrigues, R.; Jump, D.B.; Morgun, A.; Shulzhenko, N. Role of gut microbiota in type 2 diabetes pathophysiology. EBioMedicine 2020, 51, 102–110. [Google Scholar] [CrossRef] [Green Version]
- Meijnikman, A.S.; Gerdes, V.E.; Nieuwdorp, M.; Herrema, H. Evaluating causality of gut microbiota in obesity and diabetes in humans. Endocr. Rev. 2018, 39, 133–153. [Google Scholar] [CrossRef]
- Jiang, C.; Li, G.; Huang, P.; Liu, Z.; Zhao, B. The gut microbiota and Alzheimer’s disease. J. Alzheimers Dis. 2017, 58, 1–15. [Google Scholar] [CrossRef]
- Van Baarlen, P.; Troost, F.; van der Meer, C.; Hooiveld, G.; Boekschoten, M.; Brummer, R.J.M.; Kleerebezem, M. Human mucosal in vivo transcriptome responses to three Lactobacilli indicate how probiotics may modulate human cellular pathways. Proc. Natl. Acad. Sci. USA 2011, 108, 4562–4569. [Google Scholar] [CrossRef] [Green Version]
- Hiippala, K.; Jouhten, H.; Ronkainen, A.; Hartikainen, A.; Kainulainen, V.; Jalanka, J.; Satokari, R. The Potential of Gut Commensals in Reinforcing Intestinal Barrier Function and Alleviating Inflammation. Nutrients 2018, 10, 988–1005. [Google Scholar] [CrossRef] [Green Version]
- Singh, K.; Rao, A. Probiotics: A potential immunomodulator in COVID-19 infection management. Nutr. Res. 2021, 87, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wu, Y.; Wang, Y.; Xu, H.; Mei, X.; Yu, D.; Wang, Y.; Li, W. Antioxidant properties of probiotic bacteria. Nutrients 2017, 9, 521–534. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.L.; Martoni, C.J.; Prakash, S. Oral supplementation with probiotic L. reuteri increases mean circulating 25-hydroxyvitamin D: A post hoc analysis of a randomized controlled trial. J. Clin. Endocrinol. Metab. 2013, 98, 2944–2951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, P.; Rawat, A.; Alwakeel, M.; Sharif, E.; Al Khodor, S. The potential role of vitamin D supplementation as a gut microbiota modifier in healthy individuals. Sci. Rep. 2020, 10, 21–32. [Google Scholar] [CrossRef]
- Shang, M.; Sun, J. Vitamin D/VDR, Probiotics, and Gastrointestinal Diseases. Curr. Med. Chem. 2017, 24, 876–877. [Google Scholar] [CrossRef]
- Yoon, S.; Wu, S.; Zhang, Y.-G.; Lu, R.; Petrof, E.O.; Yuan, L.; Claud, E.; Sun, J. Probiotic regulation of vitamin D receptor in intestinal inflammation. Gastroenterology 2011, 140, 19. [Google Scholar] [CrossRef]
- Wu, S.; Yoon, S.; Zhang, Y.-G.; Lu, R.; Xia, Y.; Wan, J.; Petrof, E.O.; Claud, E.C.; Chen, D.; Sun, J. Vitamin D receptor pathway is required for probiotic protection in colitis. Am. J. Physiol. Gastrointest. Liver Physiol. 2015, 309, 341–349. [Google Scholar] [CrossRef] [Green Version]
- Jamilian, M.; Amirani, E.; Asemi, Z. The effects of vitamin D and probiotic co-supplementation on glucose homeostasis, inflammation, oxidative stress and pregnancy outcomes in gestational diabetes: A randomized, double-blind, placebo-controlled trial. Clin. Nutr. 2018, 38, 2098–2105. [Google Scholar] [CrossRef]
- Daneshkhah, A.; Agrawal, V.; Eshein, A.; Subramanian, H.; Roy, H.K.; Backman, V. The possible role of vitamin D in suppressing cytokine storm and associated mortality in COVID-19 patients. MedRxiv 2020, 78, 1–15. [Google Scholar]
- Demir, M.; Demir, F.; Aygun, H. Vitamin D deficiency is associated with COVID-19 positivity and severity of the disease. J. Med. Virol. 2021, 93, 2992–2999. [Google Scholar] [CrossRef]
- Al Kassaa, I.; Hober, D.; Hamze, M.; Chihib, N.E.; Drider, D. Antiviral potential of lactic acid bacteria and their bacteriocins. Probiotics Antimicrob. Proteins 2014, 6, 177–185. [Google Scholar] [CrossRef]
- Salaris, C.; Scarpa, M.; Elli, M.; Bertolini, A.; Guglielmetti, S.; Pregliasco, F.; Brun, P.; Catagliuolo, I. Lacticaseibacillus enhances the lactoferrin anti-SARS-CoV-2 response in Caco-2 cells. Gut Microbes 2021, 13, 1961–1970. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.; Ng, T.B.; Sun, W.Z. Lactoferrin as potential preventative and adjunct treatment for COVID-19. Int. J. Antimicrob. Agents 2020, 56, 106–118. [Google Scholar] [CrossRef] [PubMed]
- Kotwal, G. Natural Antivirals against Human Viruses. Virol. Mycol. 2014, 3, 20–27. [Google Scholar] [CrossRef] [Green Version]
- Jassim, S.A.; Naji, M.A. Novel antiviral agents: A medicinal plant perspective. J. Appl. Microbiol. 2003, 95, 412–427. [Google Scholar] [CrossRef] [Green Version]
- Fujita, R.; Iimuro, S.; Shinozaki, T.; Sakamaki, K.; Uemura, Y.; Takeuchi, A.; Matsuyama, Y.; Ohashi, Y. Decreased duration of acute upper respiratory tract infections with daily intake of fermented milk: A multicenter, double-blinded, randomized comparative study in users of day care facilities for the elderly population. Am. J. Infect. Control 2013, 41, 1231–1235. [Google Scholar] [CrossRef] [PubMed]
- Rerksuppaphol, S.; Rerksuppaphol, L. Randomized controlled trial of probiotics to reduce common cold in schoolchildren. Paediatr. Int. 2012, 54, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Waki, N.; Mastumoto, M.; Fuku, Y.; Suganuma, H. Effects of probiotic Lactobacillus brevis KB290 on incidence of influenza infection among schoolchildren: An open-label pilot study. Lett. Appl. Microbiol. 2014, 59, 565–571. [Google Scholar] [CrossRef] [Green Version]
- Kang, E.J.; Kim, S.Y.; Hwang, I.H.; Ji, Y.J. The effect of probiotics on prevention of common cold: A meta-analysis of randomized controlled trial studies. Korean J. Fam. Med. 2013, 34, 2–10. [Google Scholar] [CrossRef] [Green Version]
- Eguchi, K.; Fujitani, N.; Nakagawa, H.; Miyazaki, T. Prevention of respiratory syncytial virus infection with probiotic lactic acid bacterium Lactobacillus. Sci. Rep. 2019, 9, 4812–4821. [Google Scholar] [CrossRef]
- Li, S.-W.; Yang, T.-C.; Lai, C.-C.; Huang, S.-H.; Liao, J.M.; Wan, L.; Lin, Y.-J.; Lin, C.-W. Antiviral activity of aloe-emodin against Influenza A virus via galectin-3 up-regulation. Eur. J. Pharmacol. 2014, 738, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Su, M.; Jia, Y.; Li, Y.; Zhou, D.; Jia, J. Probiotics for the Prevention of Ventilator-Associated Pneumonia: A Meta-Analysis of Randomized Controlled Trials. Respir. Care 2020, 65, 673–685. [Google Scholar] [CrossRef] [PubMed]
- Powanda, M.; Whitehouse, M.W.; Rainsford, K.D. Celery Seed and Related Extracts with Antiarthritic, Antiulcer, and Antimicrobial Activities. Prog. Drug Res. 2015, 70, 133–153. [Google Scholar] [PubMed]
- Powanda, M.C.; Rainsford, K.D. A toxicological investigation of a celery seed extract having anti-inflammatory activity. Inflammopharmacology 2011, 19, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Karunaweera, N.; Raju, R.; Gyengesi, E.; Munch, G. Plant polyphenols as inhibitors of NF-κB induced cytokine production—A potential anti-inflammatory treatment for Alzheimer’s disease? Front. Mol. Neurosci. 2015, 8, 24–29. [Google Scholar] [CrossRef] [Green Version]
- Funk, J.L.; Oyarzo, J.N.; Frye, J.B.; Chen, G.; Lantz, R.C.; Jolad, S.D.; Solyom, A.M.; Timmermann, B.N. Turmeric extracts containing curcuminoids prevent experimental rheumatoid arthritis. J. Nat. Prod. 2006, 69, 351–355. [Google Scholar] [CrossRef] [Green Version]
- Al-Howiriny, T.; Alsheikh, A.; Alqasoumi, S.; Al-Yahya, M.; ElTahir, K.; Rafatullah, S. Protective Effect of Origanum majorana L. ‘Marjoram’ on various models of gastric mucosal injury in rats. Am. J. Chin. Med. 2009, 37, 531–545. [Google Scholar] [CrossRef] [PubMed]
- Rossi, G.A.; Sacco, O.; Capizzi, A.; Mastromarino, P. Can Resveratrol-Inhaled Formulations Be Considered Potential Adjunct Treatments for COVID-19? Front. Immunol. 2021, 12, 670–679. [Google Scholar] [CrossRef]
- Martinez, J.; Moreno, J. Effect of Resveratrol, a Natural Polyphenolic Compound, on Reactive Oxygen Species and Prostaglandin Production. Biochem. Pharmacol. 2000, 59, 865–870. [Google Scholar] [CrossRef]
- Nencioni, L.; Iuvara, A.; Aquilano, K.; Ciriolo, M.R.; Cozzolino, F.; Rotilio, G.; Garaci, E.; Palamara, E.T. Influenza A Virus Replication is Dependent on an Antioxidant Pathway That Involves GSH and Bcl-2. J. Am. Soc. Exp. Biol. 2003, 17, 758–760. [Google Scholar] [CrossRef]
- Filardo, S.; di Pietro, M.; Mastromarino, P.; Sessa, R. Therapeutic Potential of Resveratrol Against Emerging Respiratory Viral Infections. Pharmacol. Ther. 2020, 214, 107–123. [Google Scholar] [CrossRef] [PubMed]
- Campagna, M.; Rivas, C. Antiviral Activity of Resveratrol. Biochem. Soc. Trans. 2010, 38, 50–53. [Google Scholar] [CrossRef]
- Tang, R.; Cosentino, M.; Lee, K.H. Apigenin-7-O-β-D-glucopyranoside, an anti-HIV principle from Kummerowia striata. Bioorganic Med. Chem. Lett. 1994, 4, 455–458. [Google Scholar] [CrossRef]
- Critchfield, J.W.; Butera, S.T.; Folks, T.M. Inhibition of HIV Activation in Latently Infected Cells by Flavonoid Compounds. AIDS Res. Hum. Retrovir. 1996, 12, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Beltrán-García, J.; Osca-Verdegal, R.; Pallardó, F.V.; Ferreres, J.; Rodríguez, M.; Mulet, S.; Sanchis-Gomar, F.; Carbonell, N.; Garcia-Gimenez, J.L. Oxidative Stress and Inflammation in COVID-19-Associated Sepsis: The Potential Role of Anti-Oxidant Therapy in Avoiding Disease Progression. Antioxidants 2020, 9, 936–949. [Google Scholar] [CrossRef] [PubMed]
- Poljsak, B. Strategies for reducing or preventing the generation of oxidative stress. Oxidative Med. Cell. Longev. 2011, 19, 194–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ristow, M.; Zarse, K. How increased oxidative stress promotes longevity and metabolic health: The concept of mitochondrial hormesis (mitohormesis). Exp. Gerontol. 2010, 45, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, V.H.; Valente, H.F.; Casal, S.I.; Marques, A.F.; Moreira, P.A. Antioxidant vitamins do not prevent post exercise peroxidation and may delay muscle recovery. Med. Sci. Sports Exerc. 2009, 41, 1752–1760. [Google Scholar] [CrossRef] [PubMed]
- Avery, N.G.; Kaiser, J.L.; Sharman, M.J.; E Scheett, T.; Barnes, D.M.; Gómez, A.L.; Kramer, W.J.; Volek, J.S. Effects of vitamin E supplementation on recovery from repeated bouts of resistance exercise. J. Strength Cond. Res. 2003, 17, 801–809. [Google Scholar]
- Crow, J.P. Dichlorodihydrofluorescein and dihydrorhodamine 123 are sensitive indicators of peroxynitrite in vitro: Implications for intracellular measurement of reactive nitrogen and oxygen species. Nitric Oxide 1997, 1, 145–157. [Google Scholar] [CrossRef]
- Bailey, J.D.; Diotallevi, M.; Nicol, T.; McNeill, E.; Shaw, A.; Chuaiphichai, S.; Hale, A.; Starr, A.; Nandi, M.; Sylianou, E.; et al. Nitric Oxide Modulates Metabolic Remodeling in Inflammatory Macrophages through TCA Cycle Regulation and Itaconate Accumulation. Cell Rep. 2019, 28, 218–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, D.J.; Dawson, E.A.; Groenewoud, H.M.; Jones, H.; Thijssen, D.H. Is Flow-Mediated Dilation Nitric Oxide Mediated? Hypertension 2014, 63, 376–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.-Y.; Chen, C.; Zhang, H.-Q.; Guo, H.-Y.; Wang, H.; Wang, L.; Zhang, X.; Hua, S.-N.; Yu, J.; Xiao, P.-G.; et al. Identification of natural compounds with antiviral activities against SARS-associated coronavirus. Antivir. Res. 2005, 67, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Kwon, M.J.; Yoo, J.Y.; Choi, H.J.; Ahn, Y.J. Antiviral activity and possible mode of action of ellagic acid identified in Lagerstroemia speciosa leaves toward human rhinoviruses. BMC Complementary Med. Ther. 2014, 14, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Tito, A.; Colantuono, A.; Pirone, L.; Pedone, E.; Intartaglia, D.; Giamundo, G.; Conte, I.; Vitaglione, P.; Apone, F. Pomegranate Peel Extract as an Inhibitor of SARS-CoV-2 Spike Binding to Human ACE2 Receptor (in vitro): A Promising Source of Novel Antiviral Drugs. Front. Chem. 2021, 28, 81–87. [Google Scholar] [CrossRef]
- Biancatelli, R.M.L.C.; Berrill, M.; Catravas, J.D.; Marik, P.E. Quercetin and Vitamin C: An Experimental, Synergistic Therapy for the Prevention and Treatment of SARS-CoV-2 Related Disease (COVID-19). Front. Immunol. 2020, 11, 145–151. [Google Scholar] [CrossRef]
- Palamara, A.T.; Nencioni, L.; Aquilano, K.; de Chiara, G.D.; Hernandez, L.; Cozzolino, F.; Ciriolo, M.R.; Garaci, E. Inhibition of Influenza A Virus Replication by Resveratrol. J. Infect. Dis. 2005, 191, 1719–1729. [Google Scholar] [CrossRef]
- Jennings, M.R.; Parks, J.R. Curcumin as an Antiviral Agent. Viruses 2020, 12, 1242–1262. [Google Scholar] [CrossRef]
- Rattis, B.A.C.; Ramos, S.G.; Celes, M.R.N. Curcumin as a Potential Treatment for COVID-19. Front. Pharmacol. 2021, 12, 673–675. [Google Scholar] [CrossRef]
- Kumar, D.; Basu, S.; Parija, L.; Rout, D.; Manna, S.; Dandapat, J.; Debata, P.R. Curcumin and Ellagic acid synergistically induce ROS generation, DNA damage, p53 accumulation and apoptosis in HeLa cervical carcinoma cells. Biomed. Pharmacol. 2016, 81, 31–37. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, H.J.; Lee, Y.S. A New Anti-HIV Flavonoid Glucuronide from Chrysanthemum Morifolium. Planta Medica 2003, 69, 859–861. [Google Scholar]
- Lv, X.; Qiu, M.; Chen, D.; Zheng, N.; Jin, Y.; Wu, Z. Apigenin Inhibits Enterovirus 71 Replication Through Suppressing Viral IRES Activity and Modulating Cellular JNK Pathway. Antivir. Res. 2014, 109, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Qian, S.; Fan, W.; Qian, P.; Zhang, D.; Wei, Y.; Chen, H.; Li, X. Apigenin Restricts FMDV Infection and Inhibits Viral IRES Driven Translational Activity. Viruses 2015, 7, 1613–1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakaryan, H.; Arabyan, E.; Oo, A.; Zandi, K. Flavonoids: Promising natural compounds against viral infections. Arch. Virol. 2017, 162, 2539–2551. [Google Scholar] [CrossRef] [PubMed]
- Alzaabi, M.M.; Hamdy, R.; Ashmawy, N.S.; Hamoda, A.M.; Alkhayat, F.; Khademi, N.N.; Abo Al Joud, S.M.; El-Keblawy, A.A.; Soliman, S.S.M. Flavonoids are promising safe therapy against COVID-19. Phytochem. Rev. Proc. Phytochem. Soc. Eur. 2021, 21, 291–312. [Google Scholar] [CrossRef]
- Horvat, M.; Avbelj, M.; Duran-Alonso, M.B.; Banjanac, M.; Petkovic, H.; Iskra, J. Antiviral Activities of Halogenated Emodin Derivatives against Human Coronavirus NL63. Molecules 2021, 26, 6825–6847. [Google Scholar] [CrossRef]
- Alves-Santos, A.M.; Sugizaki, C.S.A.; Lima, G.C.; Naves, M.M.V. Prebiotic effect of dietary polyphenols: A systematic review. J. Funct. Foods 2020, 74, 3–104. [Google Scholar] [CrossRef]
- Al Azzaz, J.; Al Tarraf, A.; Heumann, A.; da Silva Barreira, D.; Laurent, J.; Assifaoui, A.; Rieu, A.; Guzzo, J.; Lapaquette, P. Resveratrol Favors Adhesion and Biofilm Formation of Lacticaseibacillus paracasei subsp. paracasei Strain ATCC334. Int. J. Mol. Sci. 2020, 21, 5423–5446. [Google Scholar] [CrossRef]
- Arcanjo, N.O.; Andrade, M.J.; Padilla, P.; Rodríguez, A.; Madruga, M.S.; Estévez, M. Resveratrol protects Lactobacillus reuteri against H2O2-induced oxidative stress and stimulates antioxidant defenses through upregulation of the dhaT gene. Free. Radic. Biol. Med. 2019, 135, 38–45. [Google Scholar] [CrossRef]
- Morrison, D.J.; Preston, T. Formation of short chain fatty acids by the gut microbiota and their impact on human metabolism. Gut Microbes 2016, 7, 189–200. [Google Scholar] [CrossRef] [Green Version]
- Koh, A.; de Vadder, F.; Kovatcheva-Datchary, P.; Backhed, F. From dietary fibre to host physiology: Short-chain fatty acids as key bacterial metabolites. Cell 2016, 165, 1332–1345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, G.; Jacobs, D.M.; Peters, S.; Possemiers, S.; van Duynhoven, J.; Vaughan, E.E.; Van de Wiele, T. In vitro bioconversion of polyphenols from black tea and red wine/grape juice by human intestinal microbiota displays strong inter-individual variability. J. Agric. Food Chem. 2010, 58, 10236–10246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolte, L.A.; Vich Vila, A.; Imhann, F.; Collij, V.; Gacesa, R.; Peters, V.; Wijmenga, C.; Kurilshikov, A.L.; Campmans-Kuijpers, M.J.E.; Fu, J.; et al. Long-term dietary patterns are associated with pro-inflammatory and anti-inflammatory features of the gut microbiome. Gut 2021, 70, 1287–1298. [Google Scholar] [CrossRef] [PubMed]
- David, L.A.; Maurice, C.F.; Carmody, R.N.; Gootenberg, D.B.; Button, J.E.; Wolfe, B.E.; Ling, A.V.; Develin, S.; Varma, Y.; Fischbach, M.A.; et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2014, 505, 559–563. [Google Scholar] [CrossRef] [Green Version]
- Pontin, E.; Schwannauer, M.; Tai, S.; Kinderman, P. A UK validation of a general measure of subjective well-being: The modified BBC subjective well-being scale (BBC-SWB). Health Qual. Life Outcomes 2013, 11, 150–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
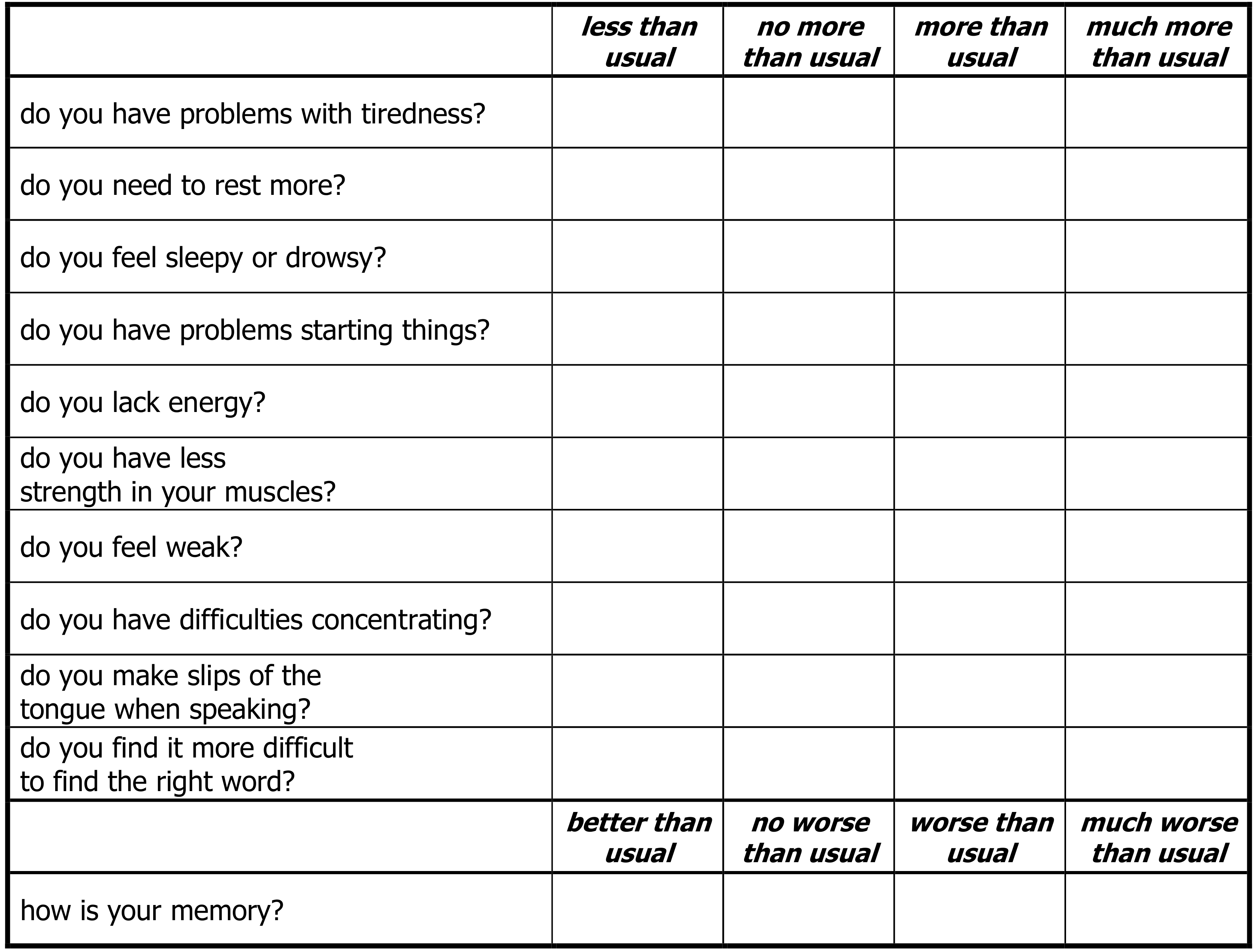
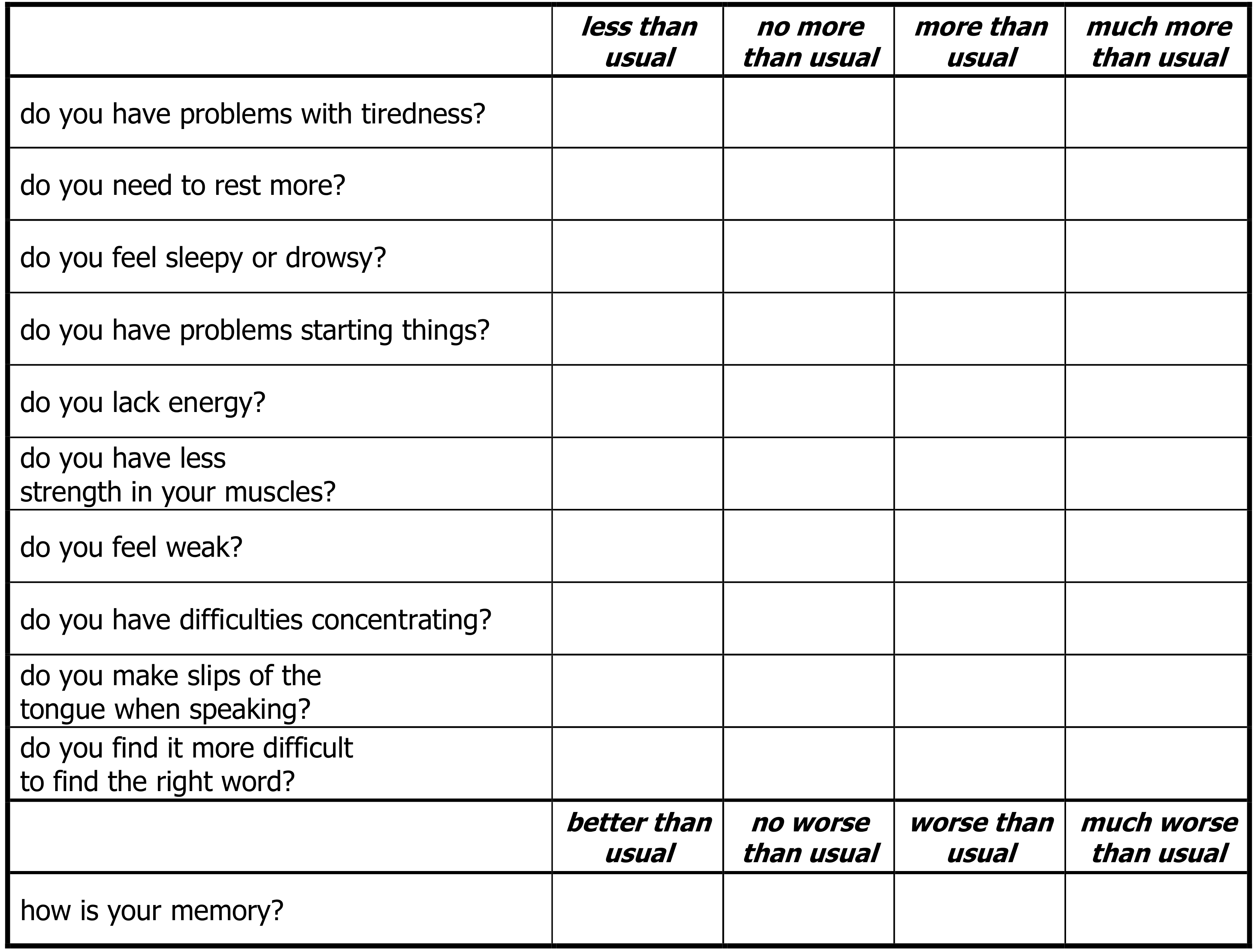
- Chalder, T.; Berelowitz, G.; Pawlikowska, T.; Watts, L.; Wessely, S.; Wright, D.; Wallace, E.P. Development of a fatigue scale. J. Psychosom. Res. 1993, 37, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Jiang, X.; Zhang, Z.; Huang, S.; Zhang, Z.; Fang, Z.; Gu, Z.; Gao, L.; Shi, H.; Mai, L.; et al. Gastrointestinal symptoms of 95 cases with SARS-CoV-2 infection. Gut 2020, 69, 997–1001. [Google Scholar] [CrossRef]
- Baud, D.; Agri, V.D.; Gibson, G.R.; Reid, G.; Giannoni, E. Using Probiotics to Flatten the Curve of Coronavirus Disease COVID-2019 Pandemic. Front. Public Health 2020, 8, 186–194. [Google Scholar] [CrossRef]
- Pourhossein, M.; Moravejolahkami, A. Probiotics in viral infections, with a focus on COVID-19: A systematic review. Authorea 2020, 1–2. [Google Scholar] [CrossRef]
- Adnan, M.L.; Dewi, M.D. Potential Effects Immunomodulators on Probiotics in COVID-19 Preventing Infection in the Future. A Narrative Review. Int. J. Med. Stud. 2020, 8, 121–125. [Google Scholar] [CrossRef]
- Gutiérrez-Castrellón, P.; Gandara-Martí, T.; Abreu, A.T.A.Y.; Nieto-Rufino, C.D.; López-Orduña, E.; Jiménez-Escobar, I.; Jiménez-Gutiérrez, C.; López-Velazquez, G.; Espadaler-Mazo, J. Probiotic improves symptomatic and viral clearance in Covid19 outpatients: A randomized, quadruple-blinded, placebo-controlled trial. Gut Microbes 2022, 14, 2018899. [Google Scholar] [CrossRef] [PubMed]
- Wischmeyer, P.E.; Tang, H.; Ren, Y.; Bohannon, L.; Ramirez, Z.; Andermann, T.; Messina, J.A.; Sung, J.A.; Jensen, D.; Jung, S.-H.; et al. Daily Lactobacillus Probiotic versus Placebo in COVID-19-Exposed Household Contacts (PROTECT-EHC): A Randomized Clinical Trial. medRxiv 2022. [Google Scholar] [CrossRef]
- Louca, P.; Murray, B.; Klaser, K.; Graham, M.S.; Mazidi, M.; Leeming, E.R.; Thompson, E.; Bowyer, R.; Drew, D.A.; Nguyen, L.H.; et al. Modest effects of dietary supplements during the COVID-19 pandemic: Insights from 445 850 users of the COVID-19 Symptom Study app. BMJ Nutr. Prev. Health 2021, 4, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Meijvis, S.C.; Hardeman, H.; Remmelts, H.H.; Heijligenberg, R.; Rijkers, G.T.; van Velzen-Blad, H.; Voorn, G.P.; van de Garde, E.M.W.; Endeman, H.; Grutters, J.C.; et al. Dexamethasone and length of hospital stay in patients with community-acquired pneumonia: A randomised, double-blind, placebo-controlled trial. Lancet 2011, 377, 2023–2030. [Google Scholar] [CrossRef]
- Hassan, N.E.; Wahba, S.A.; El-Masry, S.A.; Elhamid, E.R.A.; Boseila, S.A.W.; Ahmed, N.H.; Ibrahim, T.S. Eating Habits and Lifestyles among a Sample of Obese Working Egyptian Women. Open Access Maced. J. Med. Sci. 2015, 3, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Bwire, G. Coronavirus: Why Men are More Vulnerable to Covid-19 Than Women? SN Compr. Clin. Med. 2020, 2, 874–876. [Google Scholar] [CrossRef]
- Yurkovetskiy, L.; Burrows, M.; Khan, A.A.; Graham, L.; Volchkov, P.; Becker, L.; Antonopoulos, D.; Umesaki, Y.; Chervonsky, A.V. Gender bias in autoimmunity is influenced by microbiota. Immunity 2013, 39, 400–412. [Google Scholar] [CrossRef] [Green Version]
- Dantzer, R.; Heijnen, C.J.; Kavelaars, A.; Laye, S.; Capuron, L. The neuroimmune basis of fatigue. Trends Neurosci. 2014, 37, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Giloteaux, L.; Goodrich, J.K.; Walters, W.A.; Levine, S.M.; Ley, R.E.; Hanson, M. R Reduced diversity and altered composition of the gut microbiome in individuals with myalgic encephalomyelitis/chronic fatigue syndrome. Microbiome 2016, 4, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Williamson, C.B.; Burns, C.M.; Gossard, C.M.; Pizano, J.M.; E Dolan, K.; Finley, H.J.; Gasta, M.G.; Parker, E.C.; Lipski, E.A. Probiotics and Disease: A Comprehensive Summary-Part 3, Cardiometabolic Disease and Fatigue Syndromes. Integr. Med. A Clin. J. 2017, 16, 30–41. [Google Scholar]
- Galland, L. The gut microbiome and the brain. J. Med. Food 2014, 17, 1261–1272. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, A.; Nord, C.E.; Evengård, B. Effect of supplement with lactic-acid producing bacteria on fatigue and physical activity in patients with chronic fatigue syndrome. Nutr. J. 2009, 8, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.K.; Chopra, K.; Kuhad, A.; Kaur, I.P. Role of Lactobacillus acidophilus loaded floating beads in chronic fatigue syndrome: Behavioural and biochemical evidences. Neurogastroenterol. Motil. 2012, 24, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Doron, S.; Snydman, D. Risk and safety of probiotics. Clin. Infect. Dis. 2015, 60, 129–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernardeau, M.; Vernoux, J.P.; Henri-Dubernet, S.; Guéguen, M. Safety assessment of dairy microorganisms: The Lactobacillus genus. Int. J. Food Microbiol. 2008, 126, 278–285. [Google Scholar] [CrossRef]
- Preidis, G.; Weizman, A.V.; Kashyap, P.C.; Morgan, R.L. AGA Technical Review on the Role of Probiotics in the Management of Gastrointestinal Disorders. Gastroenterology 2020, 159, 708–738. [Google Scholar] [CrossRef]
- Hempel, S.; Newberry, S.; Ruelaz, A.; Wang, Z.; Miles, J.N.V.; Suttorp, M.J.; Johnsen, B.; Shanman, R.; Slusser, W.; Fu, N.; et al. Safety of probiotics used to reduce risk and prevent or treat disease. Evid. Rep. Technol. Assess. 2011, 200, 1–645. [Google Scholar]
- Sanders, M.E.; Akkermans, L.M.; Haller, D.; Hammerman, C.; Heimbach, J.T.; Hörmannsperger, G.; Huys, G.; Levy, D.D.; Lutgendorff, F.; Mack, D.; et al. Safety assessment of probiotics for human use. Gut Microbes 2010, 1, 164–185. [Google Scholar] [CrossRef]
- Borriello, S.P.; Hammes, W.P.; Holzapfel, W.; Marteau, P.; Schrezenmeir, J.; Vaara, M.; Valtonen, V. Safety of probiotics that contain lactobacilli or bifidobacteria. Clin. Infect. Dis. 2003, 36, 775–780. [Google Scholar] [CrossRef]
- Bernardeau, M.; Guguen, M.; Vernoux, J.P. Beneficial lactobacilli in food and feed: Long-term use, biodiversity and proposals for specific and realistic safety assessments. FEMS Microbiol. Rev. 2006, 30, 487–513. [Google Scholar] [CrossRef]
- Lu, D.; Yan, J.; Liu, F.; Ding, P.; Chen, B.; Lu, Y.; Sun, Z. Probiotics in preventing and treating chemotherapy-induced diarrhoea: A meta-analysis. Asia Pac. J. Clin. Nutr. 2019, 28, 701–710. [Google Scholar] [PubMed]
- Salminen, M.K.; Tynkkynen, S.; Rautelin, H.; Saxelin, M.; Vaara, M.; Ruutu, P.; Sarna, S.; Valtonen, V.; Jarvinen, A. Lactobacillus bacteremia during a rapid increase in probiotic use of Lactobacillus rhamnosus GG in Finland. Clin. Infect. Dis. 2002, 35, 1155–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Category Description | All Patients Number (%) | PC Group (n = 74) Number (%) | P Group (n = 73) Number (%) | Difference (Significance) |
|---|---|---|---|---|
| Male gender | 82 (56%) | 42 (29%) | 40 (27%) | diff 1% (ns) |
| Average age | 53 yrs | 55 yrs | 51 yrs | diff 4 yrs (ns) |
| Given probiotics | 126 (86%) | 62 (42%) | 64 (44%) | diff 2% (ns) |
| Duration of symptoms * | 108 days | 110 days | 107 days | diff 3 days (ns) |
| Overweight (BMI > 25–30 Kg/m2) | 44 (31%) | 20 (15%) | 24 (16%) | diff 1% (ns) |
| Obese (BMI > 30 Kg/m2) | 52 (35%) | 27 (18%) | 25 (17%) | diff 1% (ns) |
| Smokers | 99 (66%) | 50 (33%) | 49(33%) | diff 0% (ns) |
| Exercised > 3 h/wk | 38 (26%) | 22 (15%) | 16 (11%) | diff 4% (ns) |
| Ethnic group (non-white) | 40 (27%) | 18 (12%) | 22 (15%) | diff 3% (ns) |
| Hospitalised | 92 (63%) | 44 (30%) | 48 (33%) | diff 3% (ns) |
| Symptom | Number (%) | Symptom | Number (%) |
|---|---|---|---|
| Fatigue | 117 (92%) | Sore throat | 7 (6%) |
| Breathlessness | 53 (42%) | Anxiety or depression | 7 (6%) |
| Joint, muscle or chest pains | 43 (34%) | Altered hearing or vision | 6 (5%) |
| Bowel symptoms, nausea | 31 (25%) | Increased blood pressure | 6 (5%) |
| Cough | 31 (25%) | Peripheral neuropathy | 5 (4%) |
| Altered sense of smell | 31 (25%) | Dizziness | 5 (4%) |
| Headache | 24 (19%) | Increased perspiration | 4 (3%) |
| Muscle weakness | 22 (17%) | Sneezing | 4 (3%) |
| Fever/chills | 18 (14%) | New onset asthma/asthma flare | 4 (3%) |
| Poor appetite, nausea | 14 (11%) | Altered voice/hoarseness | 3 (2%) |
| Insomnia | 10 (8%) | Hyperesthesia | 3 (2%) |
| Heart palpitations | 8 (6%) | Urinary problems | 3 (2%) |
| Brain fog | 8 (6%) | Weight loss | 3 (2%) |
| Skin rash/‘COVID toes’ | 8 (6%) | Altered menstrual cycle | 2 (1%) |
| P Arm (n = 73) Mean Diff (D1–30) | PC Arm (n = 74) Mean Diff (D1-30) | P vs. PC * Diff in Means (CI ± 95%) | p Value | |
|---|---|---|---|---|
| Cough Score (CSS) | 0.4 ± 1.5 | 1.1 ± 2.0 | 0.7 (CI −1.3 to −0.1) | 0.02 |
| Subjective Well-being Score (SWS) | 1.2 ± 7.4 | 6.6 ± 10.5 | 5.4 (2.4 to 8.4) | <0.001 |
| Chalder Fatigue Scale (CFS) | 3.4 ± 6.1 | 6.1 ± 7.5 | 2.7 (CI −5.0 to −0.3) | 0.02 |
| Symptom Scores | Mean & SD (Day 1 vs. 30) | Difference Day 1 to 30 (95% CI) | p Value |
|---|---|---|---|
| All participants Given Probiotic Capsules (n = 126) | |||
| Cough Score | 1.4 ± 0.6 vs. 0.6 ± 1.4 | 0.8 (CI 0.5 to 1.1) | <0.001 |
| SWS | 24.5 ± 8.3 vs. 28.5 ± 7.2 | 4.0 (CI −5.5 to −2.4) | <0.001 |
| Fatigue Score | 21.2 ± 5.7 vs. 16.5 ± 6.7 | 4.7 (CI 3.5 to 5.8) | <0.001 |
| Early COVID * Cohort (n = 30) | |||
| Cough Score | 1.84 ± 2.33 vs. 0.61 ± 1.27 | 1.24 (CI 0.42 to 2.07) | p = 0.004 |
| Fatigue Score | 20.19 ± 5.69 vs. 14.44 ± 4.53 | 4.70 (CI 2.88 to 8.61) | p < 0.001 |
| SWS | 24.45 ± 9.69 vs. 30.94 ± 6.06 | 6.48 (CI 10.17 to −2.8) | p = 0.001 |
| Late COVID + Cohort (n = 96) | |||
| Cough Score | 1.03 ± 1.82 vs. 0.35 ± 0.89 | 0.67 (CI 0.38 to 0.98) | p < 0.001 |
| Fatigue Score | 21.66 ± 5.55 vs. 17.18 ± 7.20 | 4.70 (CI 3.13 to 5.82) | p < 0.001 |
| SWS | 23.99 ± 8.04 vs. 27.51 ± 7.03 | 3.23 (CI −5.33 to −0.70) | p < 0.001 |
| Symptom Scores | Difference in Mean Score Day 1 to 30 SD | Difference (95% CI) | p Value |
|---|---|---|---|
| Gender Male (70) vs. Female (56) | |||
| Cough Score | 1.1 ± 2.0 vs. 0.5 ± 1.2 | 0.6 (0.1 to 1.6) | p = 0.04 |
| Fatigue Score | 6.4 ± 7.2 vs. 3.2 ± 6.2 | 3.2 (0.6 to 0.5) | p = 0.01 |
| SWS * | 5.3 ± 10.6 vs. 2.6 ± 8.0 | 2.7 (−0.6 to 5.6) | p = 0.10 |
| Age <60 years (89) vs. ≥60 years (37) | |||
| Cough Score | 0.6 ± 1.8 vs. 0.9 ± 1.7 | 0.3 (0.9 to −0.4) | p = 0.46 |
| Fatigue Score | 1.6 ± 5.3 vs. 6.4 ± 7.0 | 4.8 (7.2 to 2.5) | p < 0.001 |
| SWS | 1.4 ± 9.8 vs. 5.2 ± 9.4 | 3.8 (0.2 to 7.5) | p = 0.04 |
| BMI Normal (46) vs. OW and O (80) | |||
| Cough Score | 0.8 ± 1.5 vs. 0.7 ± 1.9 | 0.1 (−0.8 to 1.5) | p = 1.00 |
| Fatigue Score | 2.7 ± 10.1 vs. 4.7 ± 9.3 | 2 (−2.6 to 4.7) | p = 1.00 |
| SWS | 4.2 ± 10.3 vs. 3.8 ± 7.5 | 0.4 (−2.0 to 4.0) | p = 0.13 |
| Hospitalised Yes (79) vs. No (47) | |||
| Cough Score | 0.9 ± 1.6 vs. 0.7 ± 1.9 | 0.2 (−0.5 to 0.7) | p = 0.77 |
| Fatigue Score | 6.1 ± 7.4. vs. 2.9 ± 5.5 | 3.2 (0.9 to 5.6) | p < 0.01 |
| SWS | 3.5 ± 9.0 vs. 5.1 ± 10.5 | 1.6 (−2.0 to 5) | p = 0.39 |
| Prior indigestion Yes (113) vs. No (13) | |||
| Cough Score | 0.8 ± 1.7 vs. 1.0 ± 2.1 | 0.2 (0.8 to −1.2) | p = 0.70 |
| Fatigue Score | 9.4 ± 7.9 vs. 4.4 ± 6.6 | 5 (0.1 to 11.1) | p < 0.01 |
| SWS | 9.1 ± 11.5 vs. 3.5 ± 9.2 | 5.6 (8.9 to 1.1) | p = 0.04 |
| New GI symptoms at baseline Yes (41) vs. No (85) | |||
| Cough Score | 0.7 ± 1.9 vs. 0.8 ± 1.7 | 0.1 (−0.5 to 0.8) | p = 0.59 |
| Fatigue Score | 5.4 ± 7.0 vs. 4.2 ± 6.8 | 1.2 (1.5 to 3.8) | p = 0.01 |
| SWS | 2.7 ± 10.1 vs. 4.7 ± 9.3 | 2 (−5.6 to 1.6) | p = 0.274 |
| Exercise >3 h/wk (93) vs. <3 h/wk (33) | |||
| Cough Score | 0.5 ± 1.3 vs. 1.6 ± 2.4 | 1.1 (0.2 to 1.9) | p = 0.02 |
| Fatigue Score | 4.1 ± 6.4 vs. 7.6 ± 7.8 | 3.5 (0.3 to 6.7) | p = 0.03 |
| SWS | 2.7 ± 6.4 vs. 8.0 ± 11.4 | 5.3 (−9.7 to −0.9) | p = 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thomas, R.; Williams, M.; Aldous, J.; Yanagisawa, Y.; Kumar, R.; Forsyth, R.; Chater, A. A Randomised, Double-Blind, Placebo-Controlled Trial Evaluating Concentrated Phytochemical-Rich Nutritional Capsule in Addition to a Probiotic Capsule on Clinical Outcomes among Individuals with COVID-19—The UK Phyto-V Study. COVID 2022, 2, 433-449. https://doi.org/10.3390/covid2040031
Thomas R, Williams M, Aldous J, Yanagisawa Y, Kumar R, Forsyth R, Chater A. A Randomised, Double-Blind, Placebo-Controlled Trial Evaluating Concentrated Phytochemical-Rich Nutritional Capsule in Addition to a Probiotic Capsule on Clinical Outcomes among Individuals with COVID-19—The UK Phyto-V Study. COVID. 2022; 2(4):433-449. https://doi.org/10.3390/covid2040031
Chicago/Turabian StyleThomas, Robert, Madeleine Williams, Jeffrey Aldous, Yuuki Yanagisawa, Rajeev Kumar, Rachel Forsyth, and Angel Chater. 2022. "A Randomised, Double-Blind, Placebo-Controlled Trial Evaluating Concentrated Phytochemical-Rich Nutritional Capsule in Addition to a Probiotic Capsule on Clinical Outcomes among Individuals with COVID-19—The UK Phyto-V Study" COVID 2, no. 4: 433-449. https://doi.org/10.3390/covid2040031
APA StyleThomas, R., Williams, M., Aldous, J., Yanagisawa, Y., Kumar, R., Forsyth, R., & Chater, A. (2022). A Randomised, Double-Blind, Placebo-Controlled Trial Evaluating Concentrated Phytochemical-Rich Nutritional Capsule in Addition to a Probiotic Capsule on Clinical Outcomes among Individuals with COVID-19—The UK Phyto-V Study. COVID, 2(4), 433-449. https://doi.org/10.3390/covid2040031