
The Burden of Omicron Variant in Pakistan: An Updated Review

Abstract
:1. Introduction
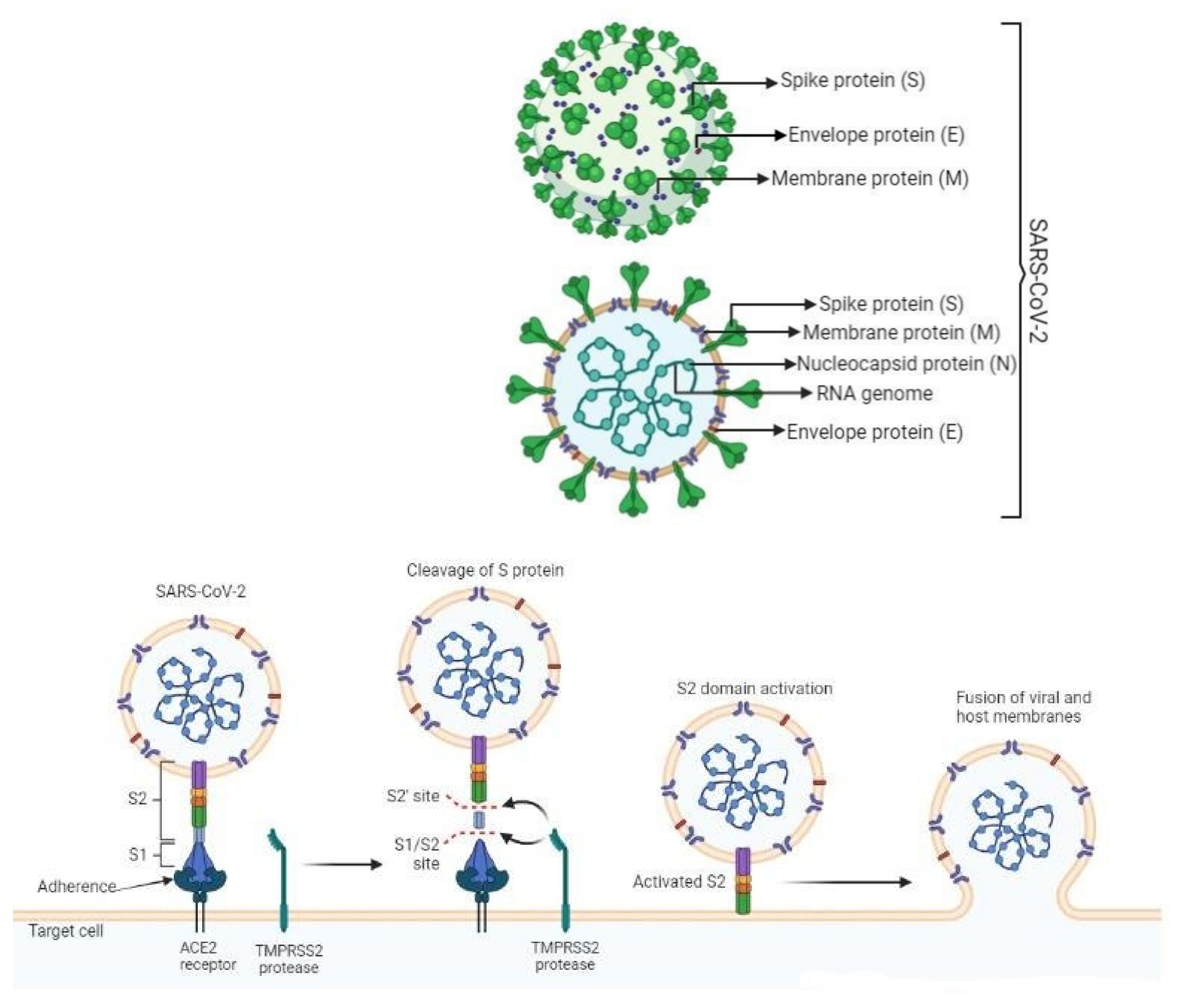
1.1. Genomics Properties of Omicron Variant
Genetic Variation Indistinct Omicron Variants
1.2. Transmissibility of Omicron Variant
The Emergence of Novel Omicron Variants
1.3. Economic Loss Due to Omicron
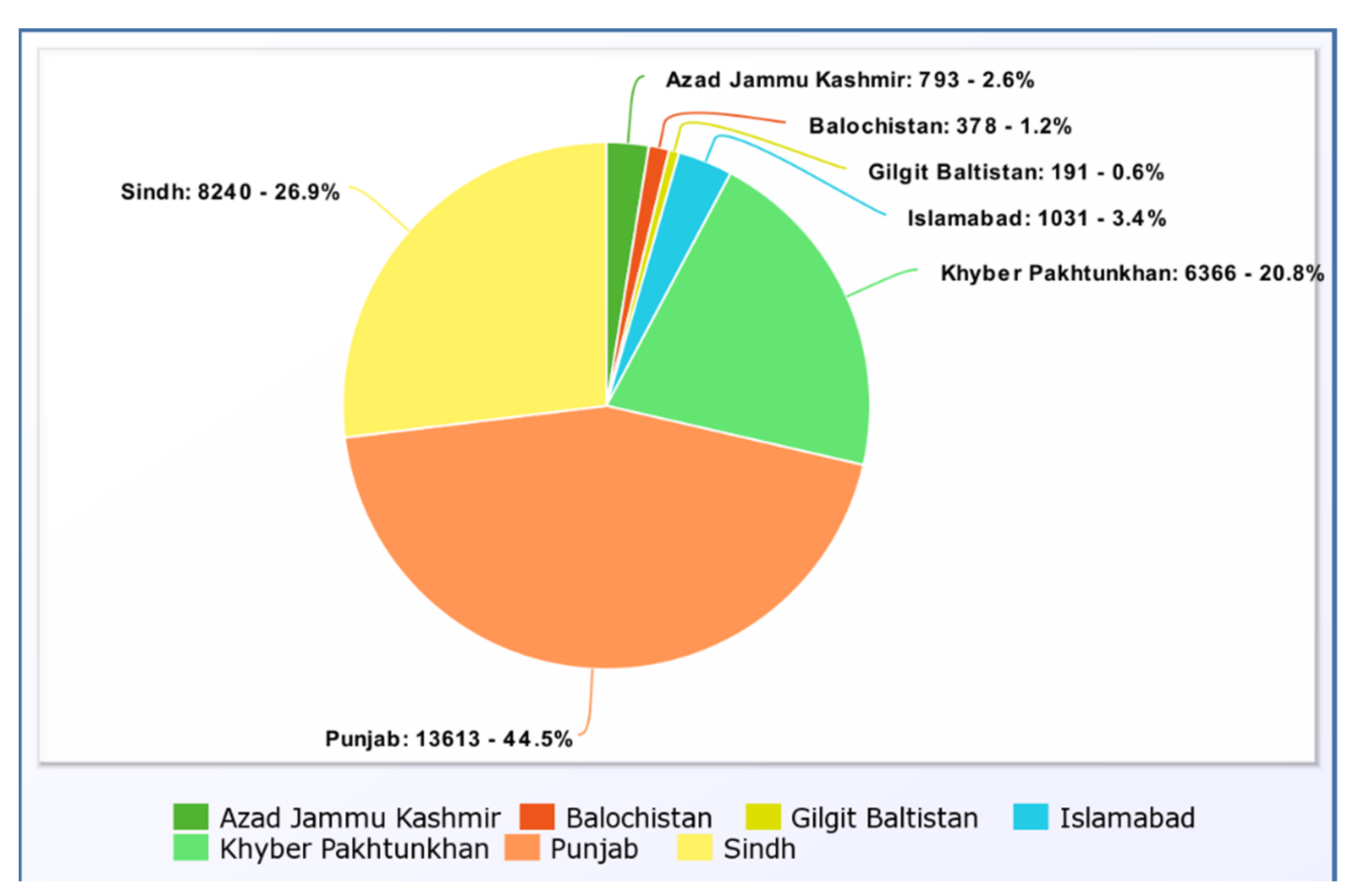
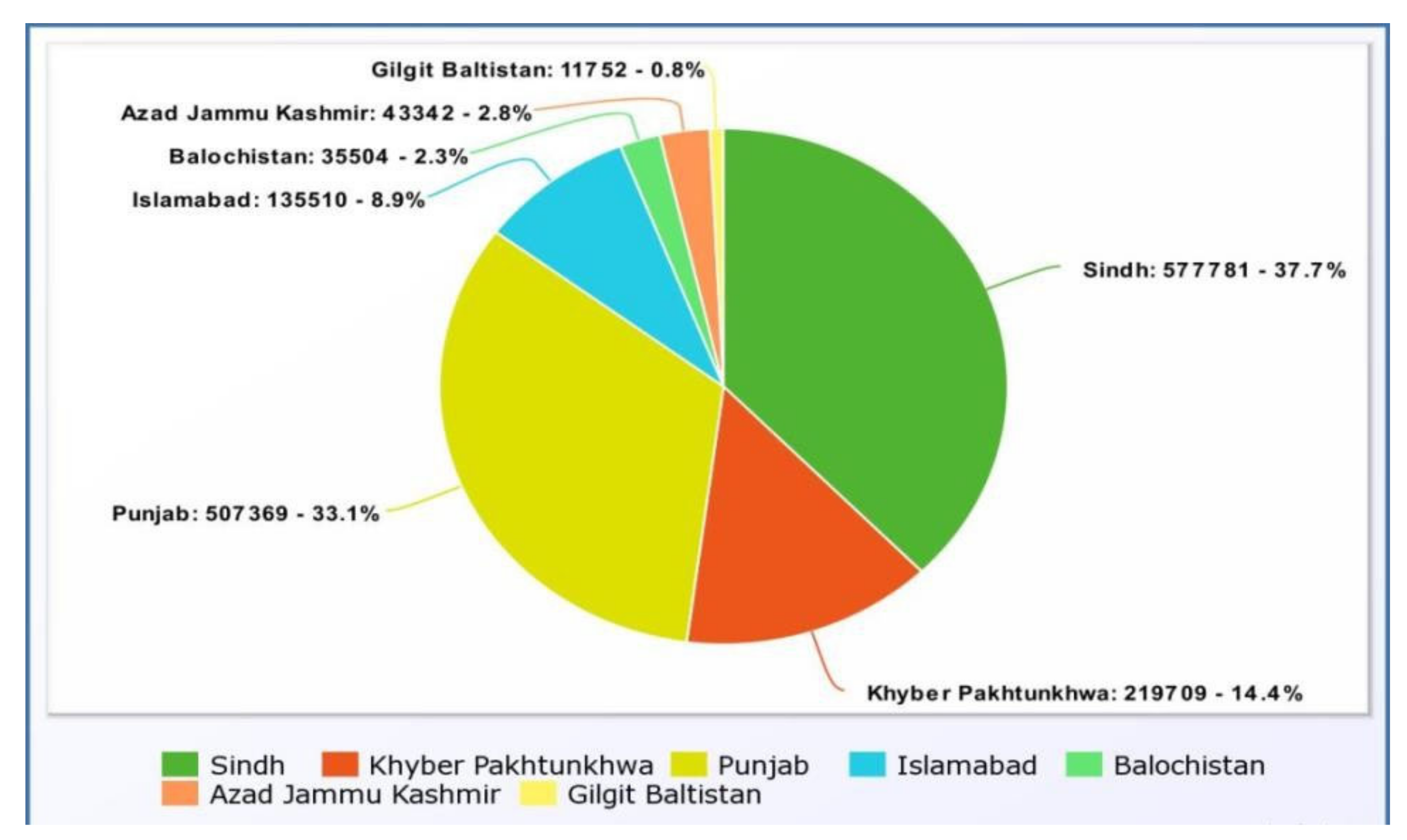
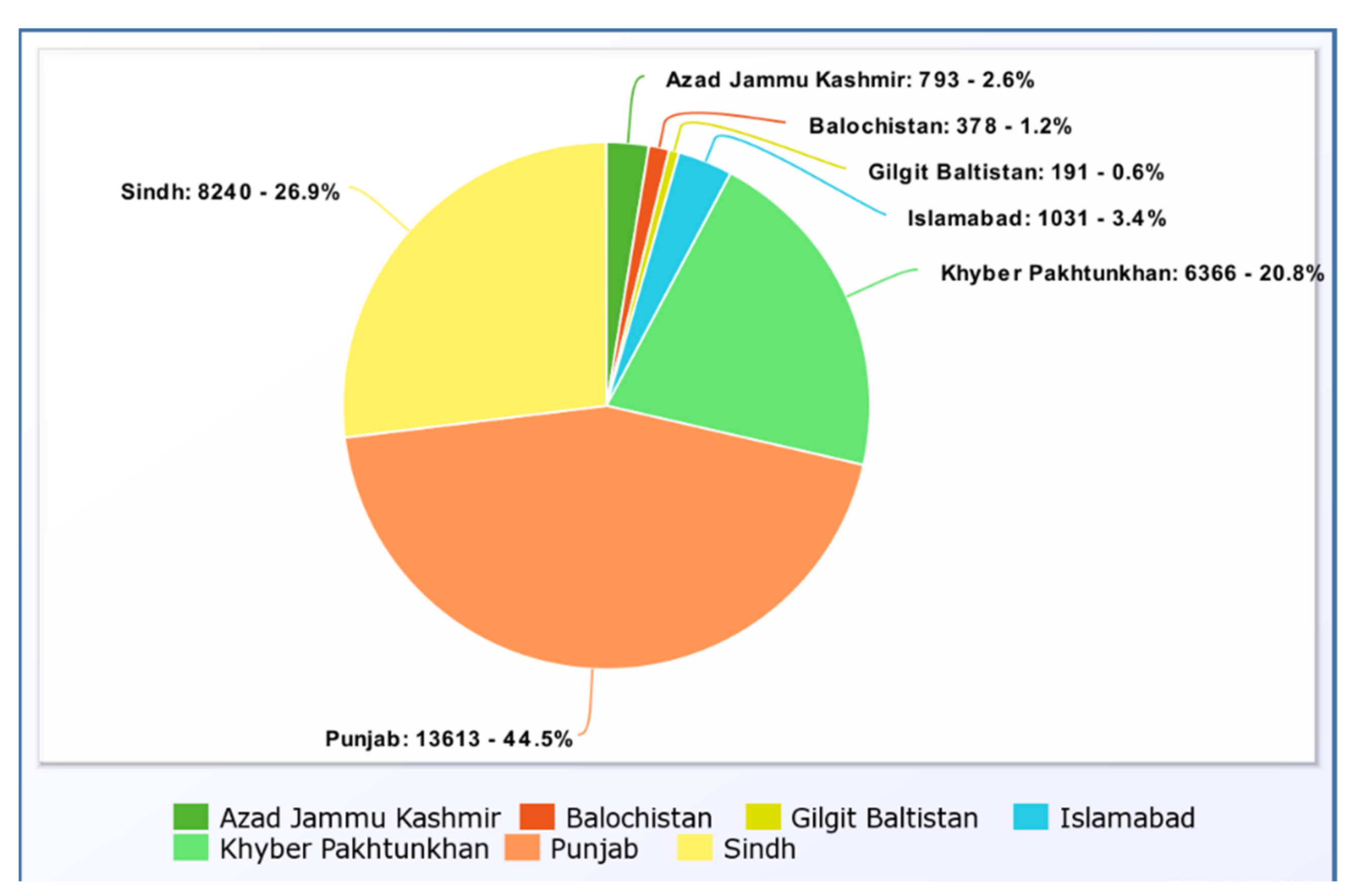
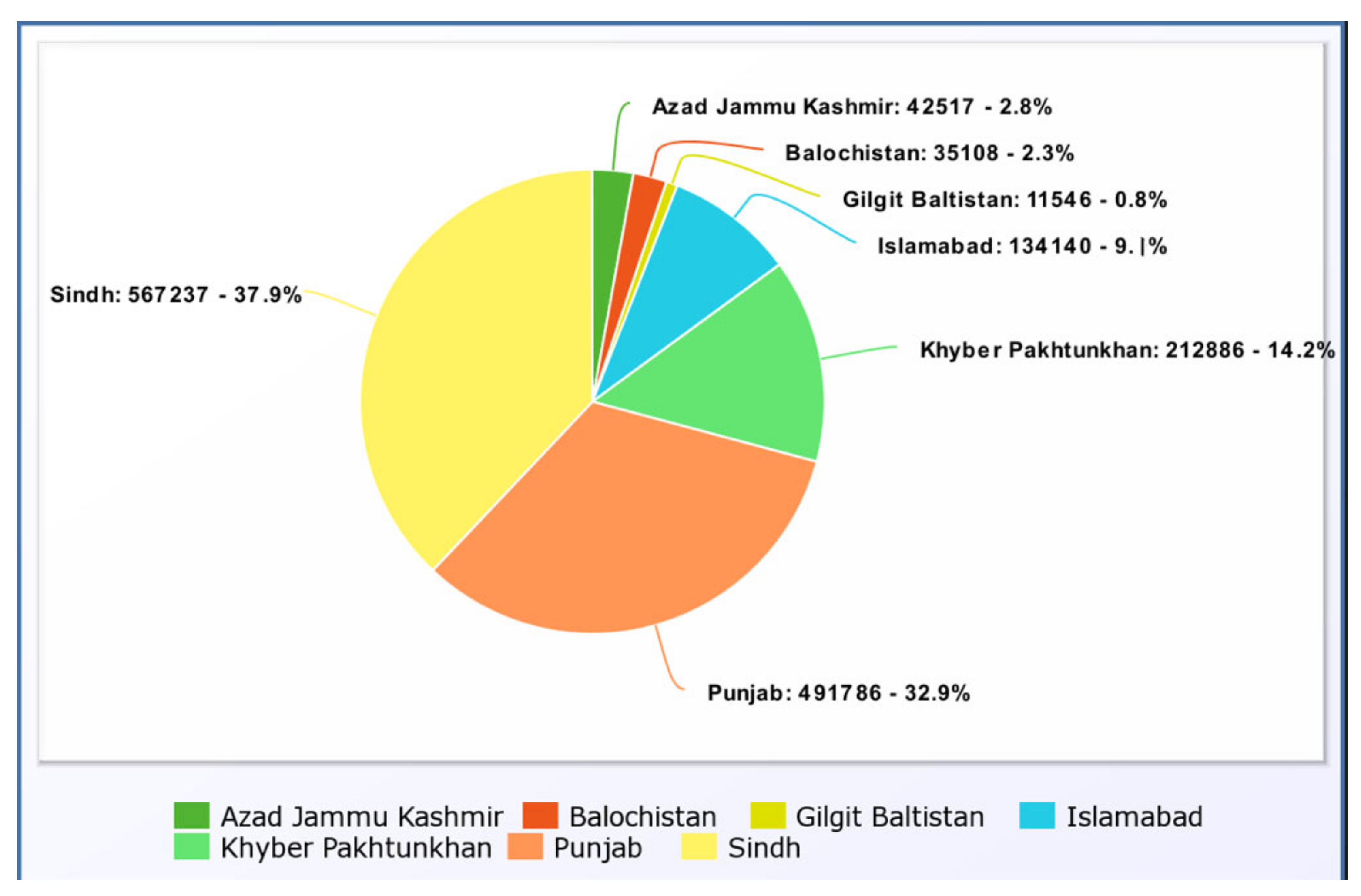
2. Impact on Pakistan
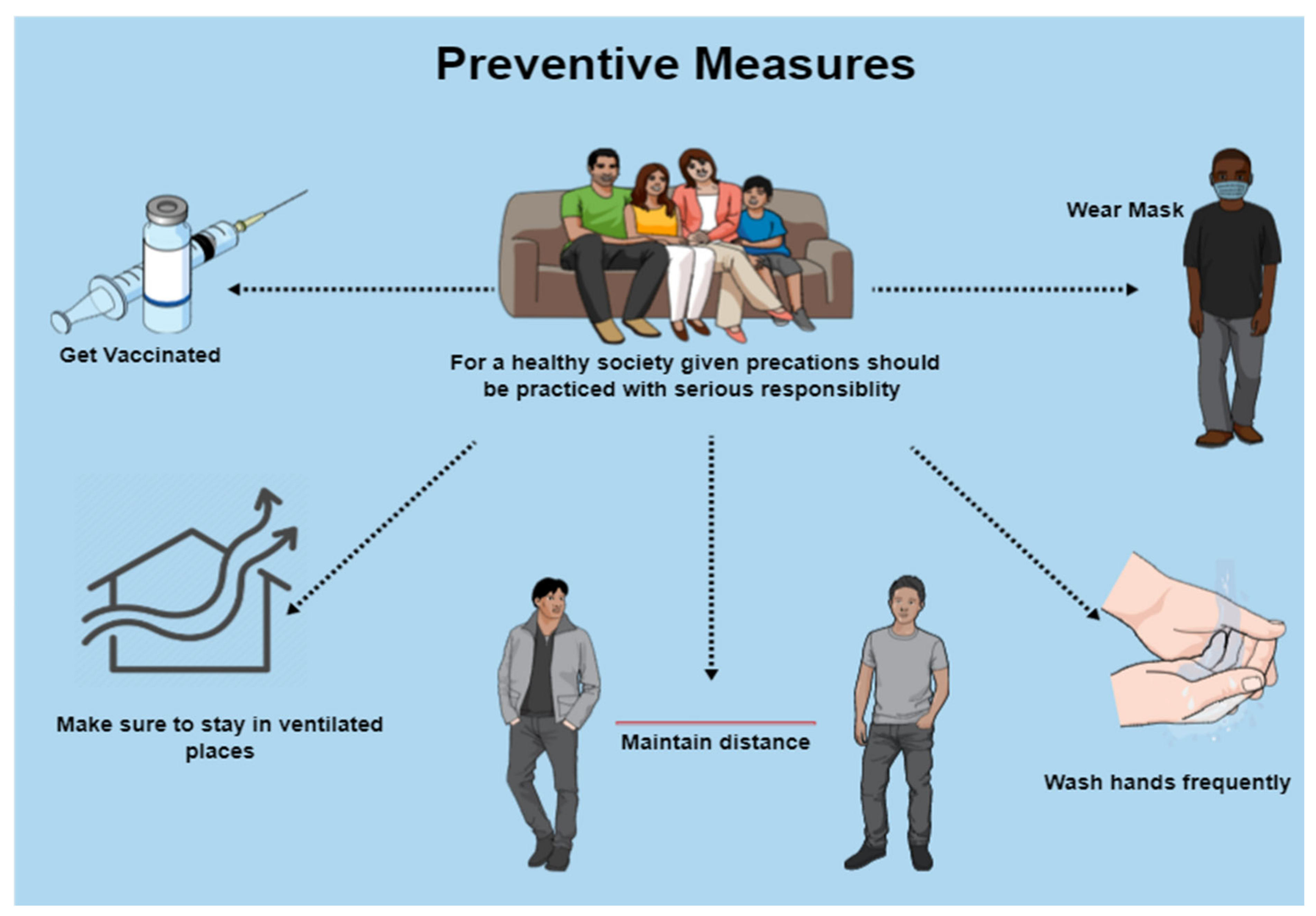
3. Control and Prevention
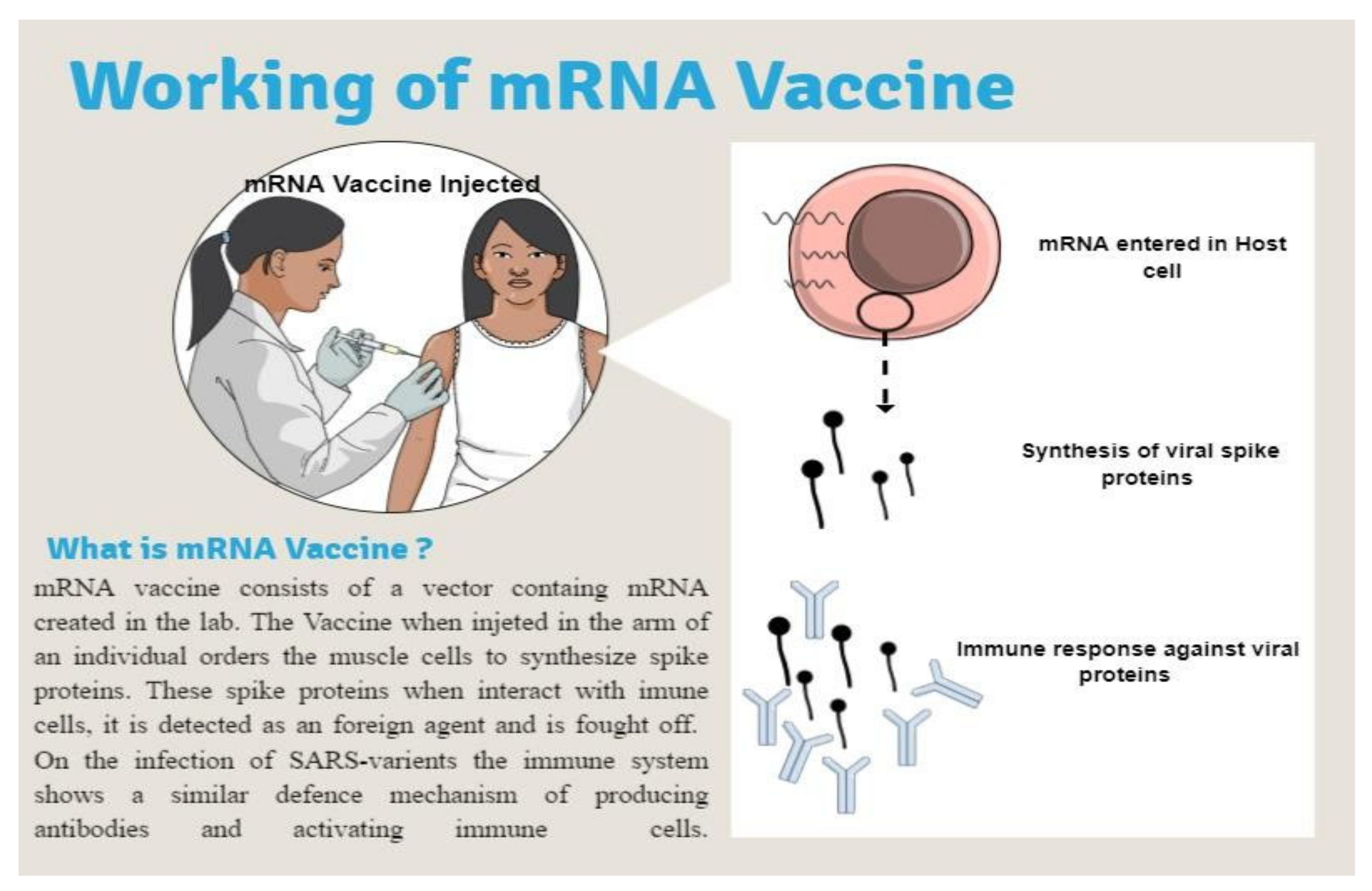
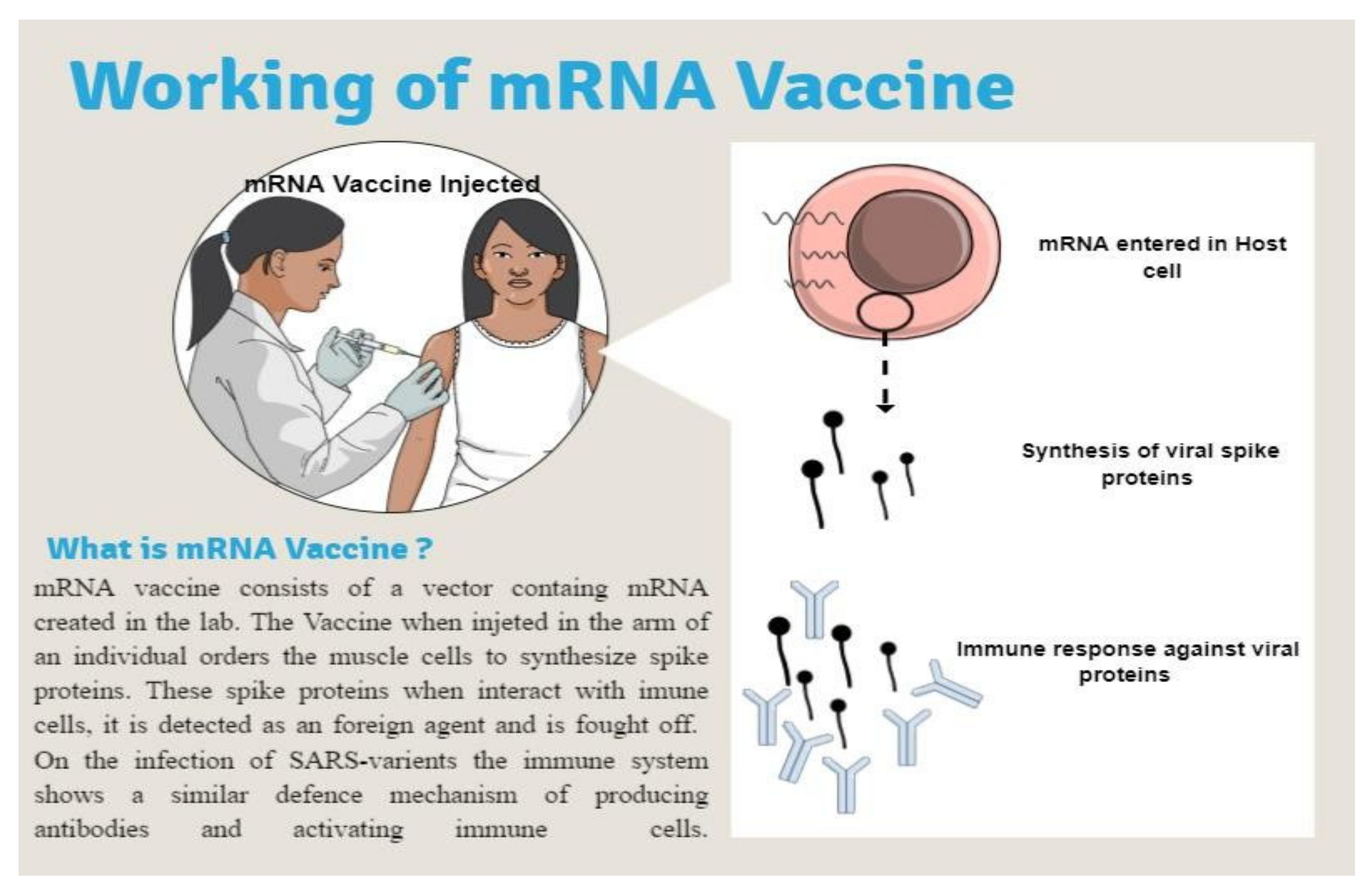
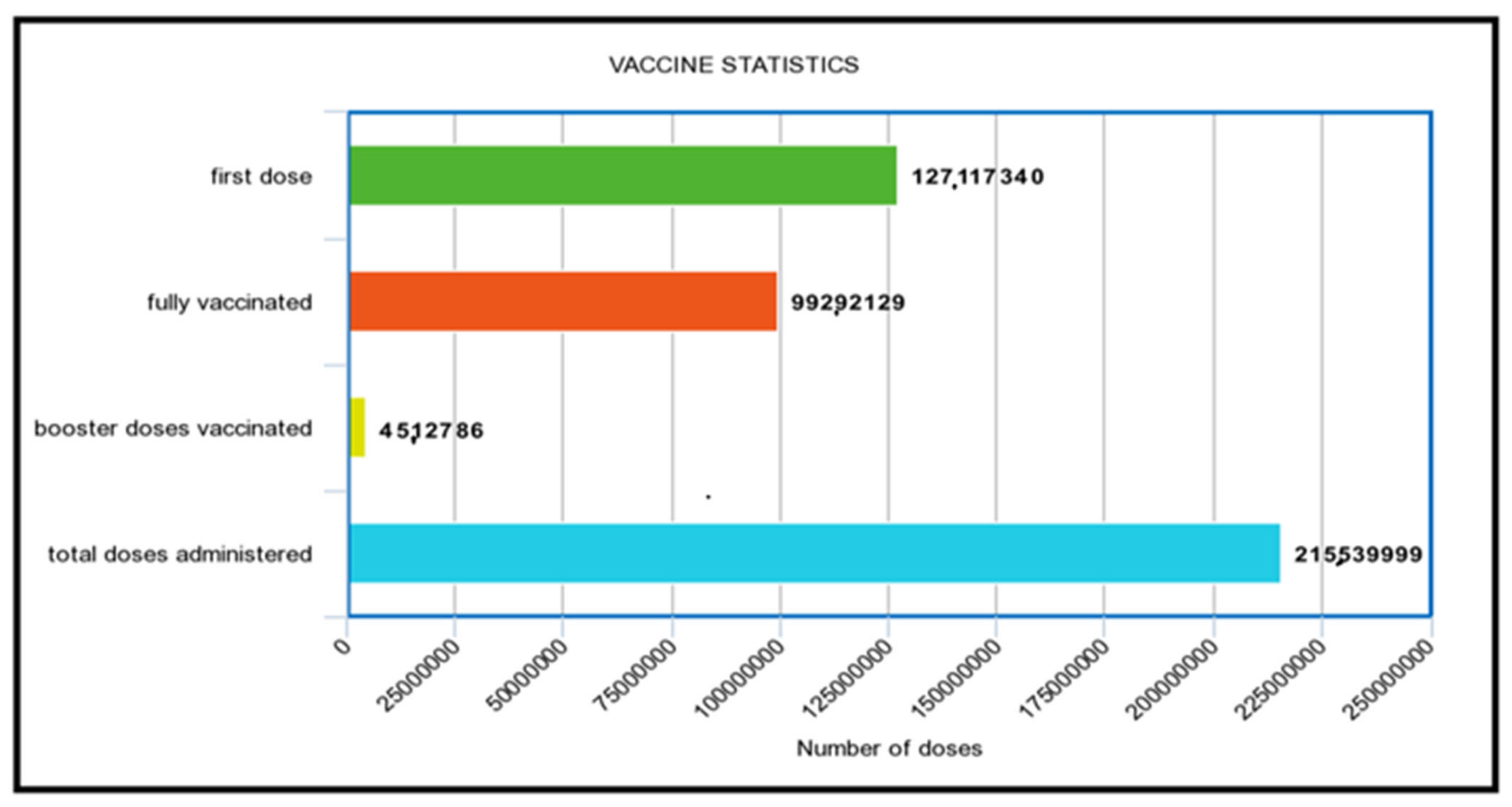
3.1. Vaccination
3.2. Vaccine Efficacy
3.3. Diagnostic Test
4. Treatment
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Enhancing Response to Omicron SARS-CoV-2 Variant: Technical Brief and Priority Actions for Member States. 2022. Available online: https://www.who.int/docs/defaultsource/coronaviruse/2022-01-21-global-technical-brief-and-priority-action-on-omicron-sars-cov-2-variant.pdf (accessed on 27 February 2022).
- Omicron Variant: What You Need to Know. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/omicron-variant.html (accessed on 27 February 2022).
- Constantino, A. WHO Says Omicron Variant Could Change the Course of the Covid Pandemic. 2021. Available online: https://www.cnbc.com/2021/12/08/who-says-omicron-covid-variant-could-change-the-course-of-the-pandemic.html (accessed on 27 February 2022).
- Explained: Why Omicron Is Still a Threat? WHO on Symptoms, Long COVID. 2022. Available online: https://www.livemint.com/science/health/explained-why-omicron-is-still-a-threat-who-on-symptoms-long-covid-11644574508909.html (accessed on 27 February 2022).
- Episode#63-Omicron Variant. 2021. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/media-resources/science-in-5/episode-63---omicron-variant (accessed on 27 February 2022).
- Omicron: Mild or Severe Impact on Economy? 2022. Available online: https://www.thenews.com.pk/print/923463-omicron-mild-or-severe-impact-on-economy (accessed on 27 February 2022).
- Lamers, M.M.; Haagmans, B.L. SARS-CoV-2 pathogenesis. Nat. Rev. Genet. 2022, 20, 270–284. [Google Scholar] [CrossRef] [PubMed]
- Bansal, K.; Kumar, S. Mutational cascade of SARS-CoV-2 leading to evolution and emergence of omicron variant. Virus Res. 2022, 2, 198765. [Google Scholar] [CrossRef] [PubMed]
- Daria, S.; Bhuiyan, M.A.; Islam, R. Detection of highly muted coronavirus variant Omicron (B.1.1.529) is triggering the alarm for South Asian countries: Associated risk factors and preventive actions. J. Med. Virol. 2021, 94, 1267–1268. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Beltran, W.F.; St Denis, K.J.; Hoelzemer, A.; Lam, E.C.; Nitido, A.D.; Sheehan, M.L.; Berrios, C.; Ofoman, O.; Chang, C.C.; Hauser, B.M.; et al. mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant. Cell 2022, 185, 457–466.e4. [Google Scholar] [CrossRef]
- Med, E. Plasma Neutralization of the SARS-CoV-2 Omicron Variant. N. Engl. J. Med. 2022, 386, 599–601. [Google Scholar]
- Hoffmann, M.; Krüger, N.; Schulz, S.; Cossmann, A.; Rocha, C.; Kempf, A.; Nehlmeier, I.; Graichen, L.; Moldenhauer, A.-S.; Winkler, M.S.; et al. The Omicron variant is highly resistant against antibody-mediated neutralization: Implications for control of the COVID-19 pandemic. Cell 2022, 185, 447–456.e11. [Google Scholar] [CrossRef]
- Li, M.; Lou, F.; Fan, H. SARS-CoV-2 variants: A new challenge to convalescent serum and mRNA vaccine neutralization efficiency. Signal Transduct. Target. Ther. 2021, 6, 1–3. [Google Scholar] [CrossRef]
- Quarleri, J.; Galvan, V.; Delpino, M.V. Omicron variant of the SARS-CoV-2: A quest to define the consequences of its high mutational load. GeroScience 2021, 44, 53–56. [Google Scholar] [CrossRef]
- Kumar, S.; Thambiraja, T.S.; Karuppanan, K.; Subramaniam, G. Omicron and Delta variant of SARS-CoV-2: A comparative computational study of spike protein. J. Med. Virol. 2021, 94, 1641–1649. [Google Scholar] [CrossRef]
- Kandeel, M.; Mohamed, M.E.M.; El-Lateef, H.M.A.; Venugopala, K.N.; El-Beltagi, H.S. Omicron variant genome evolution and phylogenetics. J. Med. Virol. 2021, 94, 1627–1632. [Google Scholar] [CrossRef]
- Wang, L.; Cheng, G. Sequence analysis of the emerging SARS-CoV-2 variant Omicron in South Africa. J. Med. Virol. 2021, 94, 1728–1733. [Google Scholar] [CrossRef]
- Med, E. Third BNT162b2 Vaccination Neutralization of SARS-CoV-2 Omicron Infection. N. Engl. J. Nal. Med. 2022, 386, 492–494. [Google Scholar]
- Desingu, P.A.; Nagarajan, K.; Dhama, K. Emergence of Omicron third lineage BA.3 and its importance. J. Med. Virol. 2022, 94, 1808–1810. [Google Scholar] [CrossRef]
- Tuekprakhon, A.; Nutalai, R.; Dijokaite-Guraliuc, A.; Zhou, D.; Ginn, H.M.; Selvaraj, M.; Liu, C.; Mentzer, A.J.; Supasa, P.; Duyvesteyn, H.M.; et al. Antibody escape of SARS-CoV-2 Omicron BA.4 and BA.5 from vaccine and BA.1 serum. Cell 2022, 185, 2422–2433.e13. [Google Scholar] [CrossRef]
- Callaway, E. Heavily mutated Omicron variant puts scientists on alert. Nature 2021, 600, 21. [Google Scholar] [CrossRef]
- Wu, L.; Zhou, L.; Mo, M.; Liu, T.; Wu, C.; Gong, C.; Lu, K.; Gong, L.; Zhu, W.; Xu, Z. SARS-CoV-2 Omicron RBD shows weaker binding affinity than the currently dominant Delta variant to human ACE2. Signal Transduct. Target. Ther. 2022, 7, 1–3. [Google Scholar] [CrossRef]
- Pascarella, S.; Ciccozzi, M.; Bianchi, M.; Benvenuto, D.; Cauda, R.; Cassone, A. The electrostatic potential of the Omicron variant spike is higher than in Delta and Delta-plus variants: A hint to higher transmissibility? J. Med. Virol. 2021, 94, 1277–1280. [Google Scholar] [CrossRef]
- Meng, B.; Abdullahi, A.; Ferreira, I.A.T.M.; Goonawardane, N.; Saito, A.; Kimura, I.; Yamasoba, D.; Gerber, P.P.; Fatihi, S.; Rathore, S.; et al. Altered TMPRSS2 usage by SARS-CoV-2 Omicron impacts infectivity and fusogenicity. Nature 2022, 603, 706–714. [Google Scholar] [CrossRef]
- Suzuki, R.; Yamasoba, D.; Kimura, I.; Wang, L.; Kishimoto, M.; Ito, J.; Morioka, Y.; Nao, N.; Nasser, H.; Uriu, K.; et al. Attenuated fusogenicity and pathogenicity of SARS-CoV-2 Omicron variant. Nature 2022, 603, 700–705. [Google Scholar] [CrossRef]
- Shuai, H.; Chan, J.F.-W.; Hu, B.; Chai, Y.; Yuen, T.T.-T.; Yin, F.; Huang, X.; Yoon, C.; Hu, J.-C.; Liu, H.; et al. Attenuated replication and pathogenicity of SARS-CoV-2 B.1.1.529 Omicron. Nature 2022, 603, 693–699. [Google Scholar] [CrossRef]
- Berger, I.; Schaffitzel, C. The SARS-CoV-2 spike protein: Balancing stability and infectivity. Cell Res. 2020, 30, 1059–1060. [Google Scholar] [CrossRef]
- Maslo, C.; Friedland, R.; Toubkin, M.; Laubscher, A.; Akaloo, T.; Kama, B. Characteristics and Outcomes of Hospitalized Patients in South Africa During the COVID-19 Omicron Wave Compared With Previous Waves. JAMA 2022, 327, 583. [Google Scholar] [CrossRef]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D.G.; Everatt, J.; Bhiman, J.N.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef]
- Ulloa, A.C.; Buchan, S.A.; Daneman, N.; Brown, K.A. Estimates of SARS-CoV-2 Omicron Variant Severity in Ontario, Canada. JAMA 2022, 327, 1286. [Google Scholar] [CrossRef]
- Nasir, A.; Aamir, U.B.; Kanji, A.; Samreen, A.; Ansar, Z.; Ghanchi, N.K.; Bukhari, A.R.; Masood, K.I.; Islam, N.; Ghani, S.; et al. SARS-CoV-2 Variants of Concern (VOC) Alpha, Beta, Gamma, Delta, and Omicron coincident with consecutive pandemic waves in Pakistan. bio-Rxiv 2022. [Google Scholar] [CrossRef]
- Madhi, S.A.; Kwatra, G.; Myers, J.E.; Jassat, W.; Dhar, N.; Mukendi, C.K.; Nana, A.J.; Blumberg, L.; Welch, R.; Ngorima-Mabhena, N.; et al. Population Immunity and Covid-19 Severity with Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 1314–1326. [Google Scholar] [CrossRef]
- Duong, B.V.; Larpruenrudee, P.; Fang, T.; Hossain, S.I.; Saha, S.C.; Gu, Y.; Islam, M.S. Is the SARS CoV-2 Omicron Variant Deadlier and More Transmissible Than Delta Variant? Int. J. Environ. Res. Public Health 2022, 19, 4586. [Google Scholar] [CrossRef]
- Cloete, J.; Kruger, A.; Masha, M.; du Plessis, N.M.; Mawela, D.; Tshukudu, M.; Manyane, T.; Komane, L.; Venter, M.; Jassat, W.; et al. Paediatric hospitalisations due to COVID-19 during the first SARS-CoV-2 omicron (B.1.1.529) variant wave in South Africa: A multicentre observational study. Lancet Child Adolesc. Health 2022, 6, 294–302. [Google Scholar] [CrossRef]
- Kozlov, M. Does Omicron Hit Kids Harder? Scientists are Trying to Find Out. Nature. 2022. Available online: https://www.nature.com/articles/d41586-022-00309-x (accessed on 27 February 2022).
- Bhattacharyya, R.P.; Hanage, W.P. Challenges in Inferring Intrinsic Severity of the SARS-CoV-2 Omicron Variant. N. Engl. J. Med. 2022, 386, e14. [Google Scholar] [CrossRef] [PubMed]
- Halfmann, P.J.; Iida, S.; Iwatsuki-Horimoto, K.; Maemura, T.; Kiso, M.; Scheaffer, S.M.; Darling, T.L.; Joshi, A.; Loeber, S.; Singh, G.; et al. SARS-CoV-2 Omicron virus causes attenuated disease in mice and hamsters. Nature 2022, 603, 687–692. [Google Scholar] [CrossRef]
- Yu, J.; Collier, A.-R.Y.; Rowe, M.; Mardas, F.; Ventura, J.D.; Wan, H.; Miller, J.; Powers, O.; Chung, B.; Siamatu, M.; et al. Neutralization of the SARS-CoV-2 omicron BA.1 and BA.2 variants. N. Engl. J. Med. 2022, 386, 1579–1580. [Google Scholar] [CrossRef] [PubMed]
- Mohapatra, R.K.; Kandi, V.; Sarangi, A.K.; Verma, S.; Tuli, H.S.; Chakraborty, S.; Chakraborty, C.; Dhama, K. The recently emerged BA.4 and BA.5 lineages of Omicron and their global health concerns amid the ongoing wave of COVID-19 pandemic–Correspondence. Int. J. Surg. 2022, 103, 106698. [Google Scholar] [CrossRef] [PubMed]
- Tegally, H.; Moir, M.; Everatt, J.; Giovanetti, M.; Scheepers, C.; Wilkinson, E.; Subramoney, K.; Makatini, Z.; Moyo, S.; Amoako, D.G.; et al. Emergence of SARS-CoV-2 Omicron lineages BA.4 and BA.5 in South Africa. Nat. Med. 2022, 28, 1785–1790. [Google Scholar] [CrossRef] [PubMed]
- Umair, M.; Ikram, A.; Rehman, Z.; Haider, S.A.; Ammar, M.; Badar, N.; Ali, Q.; Rana, M.S.; Salman, M. Genomic surveillance of-SARS-CoV-2 reveals emergence of Omicron BA.2 in Islamabad, Pakistan. InbioRxiv 2022. [Google Scholar] [CrossRef]
- Bukhari, M.H. Is Omicron a Tsunami? What should be the strategy to prevent the loss? J. Pak. Med. Assoc. 2022, 72, 798–799. [Google Scholar] [CrossRef]
- Sandra, A.O.; Nnamdi, U.A. The Challenges of International Real Estate Investment in The Emerging Economy as Results of The Restriction of Movement Due to Omicron Variants. Int. Peer-Rev. J. 2022, 5, 2456–8880. [Google Scholar]
- Islam, M.; Hossain, M. Detection of SARS-CoV-2 Omicron (B.1.1.529) variant has created panic among the people across the world: What should we do right now? J. Med. Virol. 2021, 4, 1768–1769. [Google Scholar] [CrossRef]
- Harrison, D. What is driving all cause excess mortality? BMJ 2022, 14, o100. [Google Scholar] [CrossRef]
- Karim, S.; Karim, Q. Omicron SARS-CoV-2 variant: A new chapter in the COVID-19 pandemic. Lancet 2021, 398, 2126–2128. [Google Scholar] [CrossRef]
- Covid.gov.pk. COVID-19 Health Advisory Platform by Ministry of National Health Services Regula-tions and Coordination. 2022. Available online: http://www.covid.gov.pk (accessed on 3 March 2022).
- He, X.; Hong, W.; Pan, X.; Lu, G.; Wei, X. SARS-CoV-2 Omicron variant: Characteristics and prevention. Med. Comm. 2021, 2, 838–845. [Google Scholar] [CrossRef]
- Wang, X.; Powell, C.A. How to translate the knowledge of COVID-19 into prevention of Omicron variants. Clin. Transl. Discov. 2021, 1, e22. [Google Scholar] [CrossRef]
- Cdc.gov. HowmRNACOVID-19VaccinesWork. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/downloads/vaccines/COVID-19-mRNA-infographic_G_508.pdf (accessed on 27 February 2022).
- Pollard, A.J.; Bijker, E.M. A guide to vaccinology: From basic principles to new developments. Nat. Rev. Immunol. 2020, 21, 83–100. [Google Scholar] [CrossRef]
- de Azevedo, T.C.P.; de Freitas, P.V.; da Cunha, P.H.P.; Moreira, E.A.P.; Rocha, T.J.M.; Barbosa, F.T.; de Sousa-Rodrigues, C.F.; Ramos, F.W.D.S. Efficacy and landscape of Covid-19 vaccines: A review article. Rev. da Assoc. Médica Bras. 2021, 67, 474–478. [Google Scholar] [CrossRef]
- Singhal, T. The Emergence of Omicron: Challenging Times Are Here Again! Indian J. Pediatr. 2022, 89, 490–496. [Google Scholar] [CrossRef]
- Ghiasi, N.; Valizadeh, R.; Arabsorkhi, M.; Hoseyni, T.S.; Esfandiari, K.; Sadighpour, T.; Jahantigh, H.R. Efficacy and side effects of SputnikV, Sinopharm and AstraZeneca vaccines to stop COVID-19; A review and discussion. Immunopathol. Persa 2021, 7, 31. [Google Scholar] [CrossRef]
- Nundy, S.; Ghosh, A.; Mesloub, A.; Albaqawy, G.A.; Alnaim, M.M. Impact of COVID-19pandemic on socio-economic, energy-environment and transport sector globally and sustainabledevelopment goal (SDG). J. Clean. Prod. 2021, 312, 127705. [Google Scholar] [CrossRef]
- Somasundaram, D.; Rajeshkannan, N.; Kumarendran, B.; Kumanan, T.; Sugirthan, N.; Aloysius, I.D.; Sasikumar, S.; Jegathesan, N. Mental Health Consequences from COVID-19 Pandemic and Community Level Recovery. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Brands, H.; Gavin, F.J. (Eds.) COVID-19 and World Order: The Future of Conflict, Competition, and Cooperation; Johns Hopkins University Press: Baltimore, MA, USA, 2020. [Google Scholar]
- Choi, A.; Koch, M.; Wu, K.; Chu, L.; Ma, L.; Hill, A.; Nunna, N.; Huang, W.; Oestreicher, J.; Colpitts, T.; et al. Safety and immunogenicity of SARS-CoV-2 variant mRNA vaccine boosters inhealthy adults: An inter-im analysis. Nat. Med. 2021, 27, 2025–2031. [Google Scholar] [CrossRef]
- Mevorach, D.; Anis, E.; Cedar, N.; Bromberg, M.; Haas, E.J.; Nadir, E.; Olsha-Castell, S.; Arad, D.; Hasin, T.; Le-vi, N.; et al. Myocarditis after BNT162b2 mRNA vaccine against Covid-19 in Israel. N. Engl. J. Med. 2022, 385, 2140–2149. [Google Scholar] [CrossRef]
- Corbett, K.S.; Edwards, D.K.; Leist, S.R.; Abiona, O.M.; Boyoglu-Barnum, S.; Gillespie, R.A.; Himansu, S.; Schäfer, A.; Ziwawo, C.T.; DiPiazza, A.T.; et al. SARS-CoV-2 mRNA vaccine design enabled by prototype pathogen preparedness. Nature 2020, 586, 567–571. [Google Scholar] [CrossRef]
- Alberer, M.; Gnad-Vogt, U.; Hong, H.S.; Mehr, K.T.; Backert, L.; Finak, G.; Gottardo, R.; Bica, M.A.; Garofano, A.; Koch, S.D.; et al. Safety and immunogenicity of a mRNA rabies vaccine in healthy adults: An open-label, non-randomised, prospective, first-in-human phase 1 clinical trial. Lancet 2017, 390, 1511–1520. [Google Scholar] [CrossRef]
- Fang, E.; Liu, X.; Li, M.; Zhang, Z.; Song, L.; Zhu, B.; Wu, X.; Liu, J.; Zhao, D.; Li, Y. AdvancesinCOVID-19mRNAvaccinedevelopment. Signal Transduct. Target. Ther. 2022, 7, 94. [Google Scholar] [CrossRef]
- Rufino, J.; Baquero, C.; Frey, D.; Glorioso, C.; Ortega, A.; Reščič, N.; Roberts, J.; Lillo, R.; Menezes, R.; Champati, J.; et al. Using Survey Data to Estimate the Impact of the Omicron Varianton Vaccine Efficacy against COVID-19 Infection. medRxiv 2022, 1, 21. [Google Scholar] [CrossRef]
- Imran, M.; Khan, S.; Khan, S.; Uddin, A.; Khan, M.S.; Ambade, P. COVID-19 Situation in Pakistan: A Broad Overview; Respirology: Carlton, VIC, Australia, 2021. [Google Scholar]
- Deerain, J.; Druce, J.; Tran, T.; Batty, M.; Yoga, Y.; Fennell, M.; Dwyer, D.; Kok, J.; Williamson, D. Assessment of the Analytical Sensitivity of 10 Lateral Flow Devices against the SARS-CoV-2 Omicron Variant. J. Clin. Microbiol. 2022, 60, e0247921. [Google Scholar] [CrossRef]
- Metzger, C.M.; Lienhard, R.; Seth-Smith, H.M.; Roloff, T.; Wegner, F.; Sieber, J.; Egli, A. PCR performance in the SARS-CoV-2 Omicron variant of concern? Swiss Med. Wkly. 2021, 151, w30120. [Google Scholar]
- Wen, W.; Chen, C.; Tang, J.; Wang, C.; Zhou, M.; Cheng, Y.; Zhou, X.; Wu, Q.; Zhang, X.; Feng, Z.; et al. Efficacy and safety of three new oral antiviral treatment (molnupiravir, fluvoxamine and Paxlovid) for COVID-19: A meta-analysis. Ann. Med. 2022, 54, 516–523. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. Therapeutic Management of Non-Hospitalized Adults with COVID-19. 2022. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/statement-on-therapies-for-high-risk-nonhospitalized-patients/ (accessed on 28 February 2022).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vaccine Type | Vaccine Name/Sponsor | Efficacy | Approval Status | Dosing Regimen | Storage |
|---|---|---|---|---|---|
| mRNA | BNT16b2 (Pfizer/BioNTech) | 95% | Approved for ≥16 yrs in 84 countries | 2 dosages with gap of 21 days | −60 to −80 °C; 2 to 8 °C for a single month |
| mRNA | mRNA-1273 (Moderna) | 94% | Approved for ≥16 yrs in 46 countries | 2 dosages with gap of 28 days | −50 to −15 °C; 2 to 25 °C for a single month |
| mRNA | CVnCoV(CureVac) | 47% | Did not meet the approval criteria/Withdrawal from Phase 3 trials | 2 dosages with gap of 28 days | 5–60 °C |
| Human adenovirus vectors (rAd26 and rAd5) | Gamaleya National Research Centre for Epidemiology and Microbiology | 92% | Approved for ≥18 yrs in 68 countries | 2 dosages with gap of 1–3 months | 2–8 °C |
| Chimpanzee adenovirus vector | ZD1222 (AstraZeneca/Oxford) | 70% | Approved for ≥18 yrs in 98 countries | 3 dosages with gap of 21 days | 2–8 °C |
| Human adenovirus vector | Ad26. COV2.S (Johnson & Johnson) Janssen | 67% | Approved for ≥18 yrs in 41 countries | single dose | 20 °C, 2–8 °C; 3 months |
| Human adenovirus vector | CanSino | 66% | Approved for ≥18 yrs in 5 countries | single dose | 2–8 °C |
| Inactivated vaccine based on the CZ02 strain; aluminium hydroxide- adjuvanted | CoronaVacSinov ac/China National Pharmaceutical Group | 50.65% to 83.5% | Approved for ≥18 yrs in 3 countries (Brazil, Indonesia, and Turkey) | 2 dosages with gap of 14 days | 2–8 °C/5 months 25 °C/42 days 37 °C/28 days |
| Inactivated vaccine based on the 19nCOV-CDC-TAN-HB02 strain; aluminium hydroxide-adjuvanted | BBIBP-CorV (Sinopharm/Beijing Institute of Biological Products) | 78.1 | Approved for ≥18 yrs in 4 countries | 2 dosages with gap of 21 days | 2–8 °C |
| Whole-virion inactivated SARS-CoV-2 vaccine formulated with a toll-like receptor 7/8 agonist molecule (IMDG) adsorbed to alum (Algel) | Covaxin/Bharat Biotech | 78% | Approved for ≥18 yrs in India | 2 dosages with gap of 28 days | 37 °C/7 day |
| Multitope peptide-based spike protein S1 subunit RBD CpG1 And aluminum | UB-612 (COVAXX and United Biomedical Inc. | N/A | Withdrawn from trials | N/A | 2–8 °C |
| Dimeric form of RBD adjuvant with aluminium hydroxide | ZF2001 (Chinese Academy of science) | N/A | N/A | NA | 2–8 °C |
| Recombinant protein (insect cell) + matrix M adjuvant | Novavax | 90.4% | Approved for ≥16 yrs in 84 countries | 2 dosages with gap of 21 days | 2–8 °C |
| Recombinant protein (insect cell) + AS03 adjuvant | Sanofi/GSK | N/A | N/A | 2 dosages with gap of 21 days | 2–8 °C |
| Protein subunit vaccine | EpiVacCorona (Vector Institute) | N/A | Early use in Russia | 2 dosages with gap of 21 days | 2–8 °C |
| Drugs | Doses | Recommended Population |
|---|---|---|
| Ritonavir boosted Nirmatrelvir (PAXLOVID) | Oral intake of Nirmatrelvir 300 mg with ritonavir 100 mg for 5 days | Adult outpatients older than 18 years old who have nonhypoxic COVID-19 and are at high risk of severe disease progression (e.g., due to advanced age, comorbidities, not having been vaccinated, or being immunosuppressed) are candidates for treatment |
| Sotrovimab | IV infusion once in the initial ten days of symptoms | Approved for the treatment of COVID-19 in adolescents (aged less than 12 years and weighing nearly40 kg) and adults who do not require oxygen supplementation but who are at a high risk of advancing to severe COVID-19 |
| Remdesivir (VEKLURY) | Within seven days of symptoms emergence, 200 mg IV infusion on Day one and 100 mg infusion on 2nd and 3rd day. | Adults and children over the age of 12 who weigh a minimum of up to 40 kilos and are hospitalized can administer this medication |
| Molnupiravir | Oral intake of 800 mg for five days on the initial five days of symptoms | It is predicted that molnupiravir will be effective against the Omicron VOC |
| Treatment for immunocompromised and patients with medical contraindications [68] | ||
| Tixagevimab and Cilgavimab (EVUSHELD) | Intramuscular injection once of 150 mg Tixagevimab and 150 mg cilgavimab | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, S.; Khan, S.H.; Haider, F.; Malik, J.; Khan, F.; Khan, I.; Ullah, I.; Zia, M.A.; Kousar, S. The Burden of Omicron Variant in Pakistan: An Updated Review. COVID 2022, 2, 1460-1476. https://doi.org/10.3390/covid2100105
Khan S, Khan SH, Haider F, Malik J, Khan F, Khan I, Ullah I, Zia MA, Kousar S. The Burden of Omicron Variant in Pakistan: An Updated Review. COVID. 2022; 2(10):1460-1476. https://doi.org/10.3390/covid2100105
Chicago/Turabian StyleKhan, Sarmir, Samra Hayat Khan, Fatima Haider, Jaweria Malik, Feroz Khan, Ikram Khan, Ihsan Ullah, Muhammad Amir Zia, and Shazia Kousar. 2022. "The Burden of Omicron Variant in Pakistan: An Updated Review" COVID 2, no. 10: 1460-1476. https://doi.org/10.3390/covid2100105
APA StyleKhan, S., Khan, S. H., Haider, F., Malik, J., Khan, F., Khan, I., Ullah, I., Zia, M. A., & Kousar, S. (2022). The Burden of Omicron Variant in Pakistan: An Updated Review. COVID, 2(10), 1460-1476. https://doi.org/10.3390/covid2100105