
First Scientific Evidence about the Estimation of the Odds Ratio in Vaccinated Individuals and Determination of Vaccine Efficacy against SARS-CoV-2 Infection in Angola—Part I

 ,
,
Abstract
:1. Introduction
Justification
2. Objectives
2.1. Study Main Objective
- To estimate the odds ratio of SARS-CoV-2 infection in vaccinated versus unvaccinated individuals.
2.2. Specifics Objectives
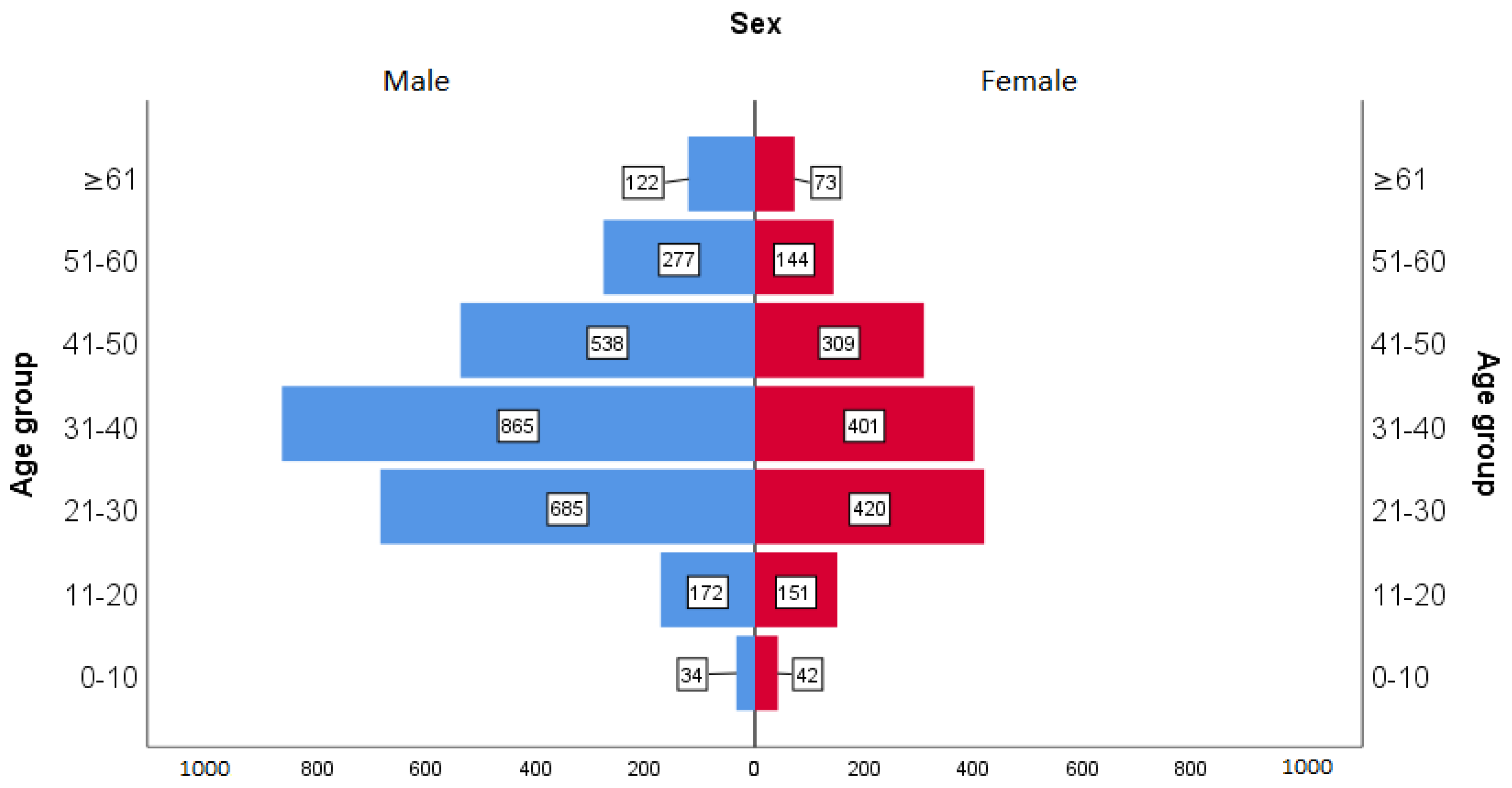
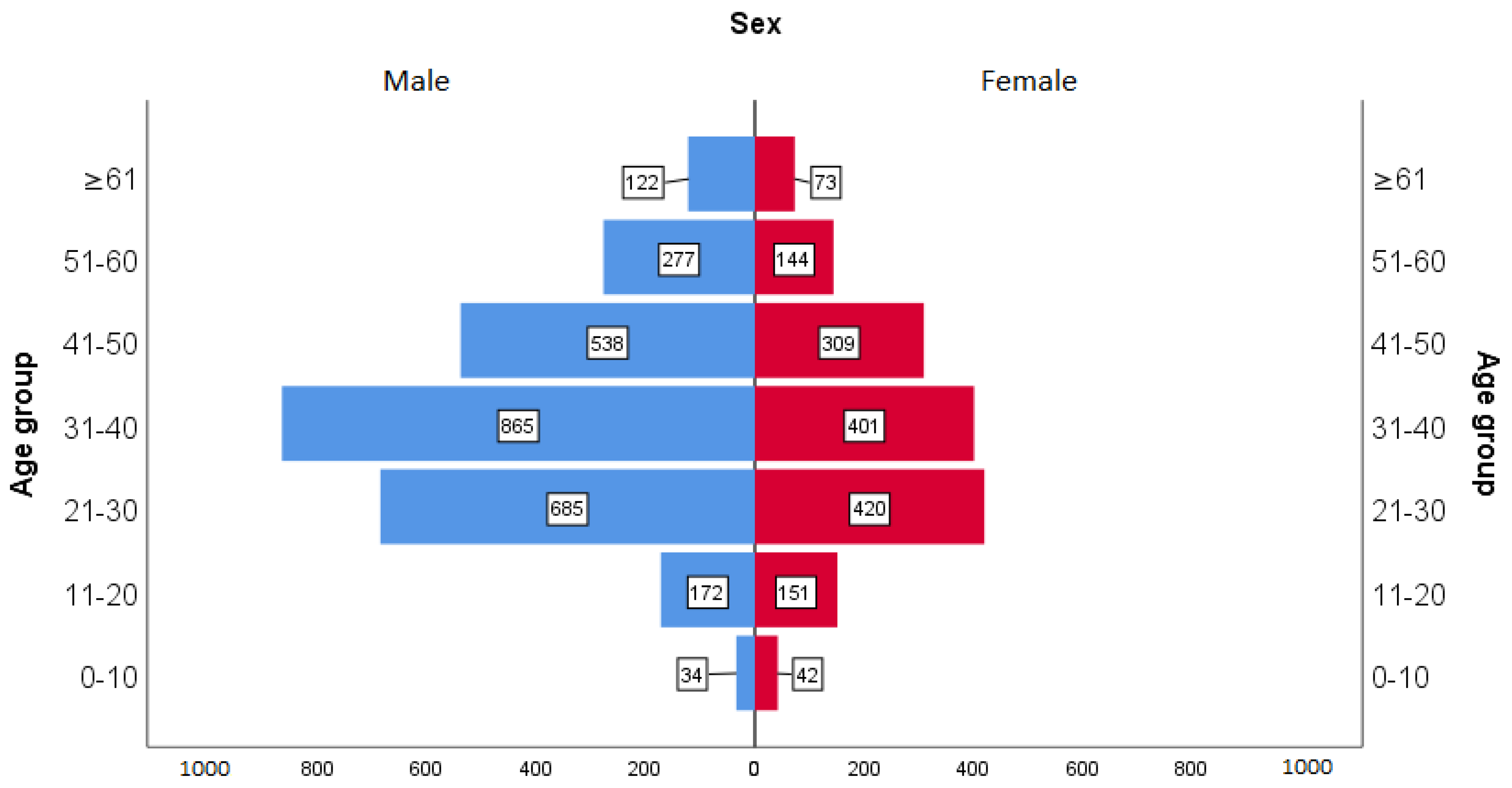
- Characterize the participants according to age group, sex, vaccination status, and rapid diagnostic test result;
- To estimate the odds ratio of SARS-CoV-2 infection in vaccinated versus unvaccinated individuals by sex and age group;
- To determine the overall vaccine efficacy (VE) by sex and age groups against SARS-CoV-2 infection.
3. Material and Methods
3.1. Study Design
3.2. Data Source, Population, and Period of Analysis
3.3. Inclusion Criteria
3.4. Exclusion Criteria
3.5. Ethical Aspects
3.6. Statistical Analysis
3.7. Operational Definitions
4. Results
5. Discussion
6. Conclusions
7. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| % | Percentage |
| VE | Vaccine efficacy |
| CI | Confidence interval |
| COVAX | COVID-19 Vaccines Global Access |
| GAVI | The Global Alliance for Vaccines and Immunization |
| OR | Odds ratio |
| WHO | World Health Organization |
| p | Probability |
| RT-PCR | Reverse transcription polymerase chain reaction |
| RAD | Rapid antigen diagnostic |
| Rediv | Registo Digital Individual de Vacinação (Individual Digital Vaccination Record) |
| UNICEF | The United Nations Children’s Fund |
References
- Radio and Television of Portugal—RTP Angola Opens Vaccine Warehouse and Starts Vaccination Campaign. Angola Opens Vaccine Warehouse and Starts Vaccination Campaign. 2021. Available online: https://www.rtp.pt/noticias/mundo/angola-inaugura-vaccine-deposit-and-start-up-with-vaccination-campaign_n1301332 (accessed on 25 January 2022).
- World Health Organization. Interim Recommendations for Use of the ChAdOx1-S [Recombinant] Vaccine against COVID-19 (AstraZeneca COVID-19 Vaccine AZD1222 VaxzevriaTM, SII COVISHIELDTM): Interim Guidance, First Issued 10 February 2021, Updated 21 April 2021, Last Updated 30 July 2021 (WHO/2019-nCoV/Vaccines/SAGE_recommendation/AZD1222/2021.3); World Health Organization: Geneva, Switzerland, 2021; Available online: https://apps.who.int/iris/handle/10665/343388 (accessed on 26 January 2022).
- News from Angola. COVID-19: Mass Vaccination Campaign Begins in This Saturday. News in Angola. Available online: https://noticiasdeangola.co.ao/covid-19-campanha-vacinacao-massa-comeca-neste-sabado/ (accessed on 26 January 2022).
- World Health Organization. Weekly Epidemiological Update—9 March 2021. 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update10-march-2021 (accessed on 26 January 2022).
- World Health Organization. Weekly Epidemiological Update—30 March 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update---31-march-2021 (accessed on 26 January 2022).
- Angola Newspaper. Jornal de Angola—News—Sputnik Vaccine Arrives to Angola; Angola Newspaper: Luanda, Angola, 2021; Available online: https://www.jornaldeangola.ao (accessed on 26 January 2022).
- Gamaleya. НИЦЭМ им. Н. Ф. Гамалеи. 2021. Available online: https://www.gamaleya.org/ (accessed on 26 January 2022).
- Logunov, D.Y.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Tukhvatulin, A.I.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S.; et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomized controlled phase 3 trial in Russia. Lancet 2021, 397, 671–681. [Google Scholar] [CrossRef]
- World Health Organization. WHO Lists Additional COVID-19 Vaccine for Emergency Use and Issues Interim Policy Recommendations. 2021. Available online: https://www.who.int/news/item/07-05-2021-who-lists-additional-covid-19-vaccine-for-emergency-use-and-issues-interim-policy-recommendations (accessed on 26 January 2022).
- World Health Organization. Background Document on the Inactivated COVID-19 Vaccine BIBP Developed by China National Biotec Group (CNBG), Sinopharm: Background Document to the WHO Interim Recommendations for Use of the Inactivated COVID-19 Vaccine BIBP Developed by China National Biotec Group (CNBG), Sinopharm, 7 May 2021 (WHO/2019-nCoV/Vaccines/SAGE_recommendation/BIBP/Background/2021.1); World Health Organization: Geneva, Switzerland, 2021; Available online: https://apps.who.int/iris/handle/10665/341252 (accessed on 26 January 2022).
- Embassy of the Republic of Angola in Portugal. Embassy of the Republic of Angola in Portugal—Angola Receives More Than 100,000 Doses of Vaccines from Pfizer. Embassy of the Republic of Angola in Portugal. Available online: http://www.embaixadadeangola.pt/angola-recebe-mais-de-100-mil-vaccine-dose-from-pfizer/ (accessed on 26 January 2022).
- World Health Organization. Interim Recommendations for Use of the Pfizer–BioNTech COVID-19 Vaccine, BNT162b2, under Emergency Use Listing: Interim Guidance, First Issued 8 January 2021, Updated 15 June 2021, Updated 19 November 2021, Updated 21 January 2022 (WHO/2019-nCoV/Vaccines/SAGE_recommendation/BNT162b2/2022.1); World Health Organization: Geneva, Switzerland, 2022; Available online: https://apps.who.int/iris/handle/10665/351139 (accessed on 26 January 2022).
- Lusa, A. COVID-19. Angola Received 165,000 Doses of Janssen Vaccines. Observer. 2021. Available online: https://observador.pt/2021/08/08/covid-19-angola-recebeu-165-thousand-dose-of-vaccines-janssen/ (accessed on 26 January 2022).
- World Health Organization. Interim Recommendations for the Use of the Janssen Ad26.COV2.S (COVID-19) Vaccine: Interim Guidance, 17 March 2021 (WHO/2019-nCoV/Vaccines/SAGE_recommendation/Ad26.COV2.S/2021.1); World Health Organization: Geneva, Switzerland, 2021; Available online: https://apps.who.int/iris/handle/10665/340203 (accessed on 26 January 2022).
- AngoRussia. National Director of Public Health Warns That Outbreak in the Flu He Can to Be Signal in COVID-19. Available online: https://angorussia.com/noticias/directora-nacional-de-saude-publica-adverte-que-surto-de-gripe-pode-ser-sinal-de-covid-19/ (accessed on 27 January 2022).
- Angola Newspaper. Jornal de Angola—Notícias—Angola Already Has Community Circulation of the Omicron Variant; Angola Newspaper: Luanda, Angola, 2021. [Google Scholar]
- RFI. Omicron Forces Mass Testing of the Angolan Population. RFI. Available online: https://www.rfi.fr/pt/angola/20211227-%C3%B3micron-obriga-the-mass-testing-%C3%A0-population%C3%A7%C3%A3o-Angolan (accessed on 27 December 2021).
- Clemens, J.; Aziz, A.B.; Tadesse, B.T.; Kang, S.; Marks, F.; Kim, J. Evaluation of protection by COVID-19 vaccines after deployment in low and lower-middle income countries. EClinicalMedicine 2022, 43, 101253. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (Regional Office for Europe). Estimating COVID-19 Vaccine Effectiveness against Severe Acute Respiratory Infections (SARI) Hospitalisations Associated with Laboratory-Confirmed SARS-CoV-2: An Evaluation Using the Test-Negative Design: Guidance Document; Report No.: WHO/EURO: 2021-2481-42237-58308; World Health Organization: Geneva, Switzerland, 2021; Available online: https://apps.who.int/iris/handle/10665/341111 (accessed on 26 January 2022).
- Vandenbroucke, J.P.; Brickley, E.B.; Vandenbroucke-Grauls, C.M.J.E.; Pearce, N. A Test-Negative Design with Additional Population Controls Can Be Used to Rapidly Study Causes of the SARS-CoV-2 Epidemic. Epidemiology 2020, 31, 836–843. [Google Scholar] [CrossRef] [PubMed]
- Silva, B. Estatística para Ciências Humanas, 3rd ed; Gráfica Lito-Tipo: Luanda, Angola, 2006; 179p, ISBN 97897729202445. [Google Scholar]
- Tavares, C. Understand How the Effectiveness of a Vaccine Is Measured—Fiotec. 2021. Available online: https://www.fiotec.fiocruz.br/noticias/outros/7353-entenda-como-e-medida-a-effectiveness-of-a-vaccine (accessed on 15 March 2022).
- UOL. Vaccine with 50% Effectiveness Could Be Approved, Admits Chief Scientist Gives WHO. 2021. Available online: https://www.uol.com.br/vivabem/noticias/redacao/2020/09/21/vacina-com-50-de-efficacy-can-be-approved-admits-who-chief-scientist.htm (accessed on 27 January 2022).
- UKHSA. SARS-CoV-2 Variants of Concern and Variants under Investigation in England: Technical Briefing 34. 2022. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1050236/technical-briefing-34-14-january-2022.pdf (accessed on 18 February 2022).
- Jara, A.; Undurraga, E.A.; González, C.; Paredes, F.; Fontecilla, T.; Jara, G.; Pizarro, A.; Acevedo, J.; Leo, K.; Leon, F.; et al. Effectiveness of an Inactivated SARS-CoV-2 Vaccine in Chile. N. Engl. J. Med. 2021, 385, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J.L.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on COVID-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef] [PubMed]
- Dickerman, B.A.; Gerlovin, H.; Madenci, A.L.; Kurgansky, K.E.; Ferolito, B.R.; Figueroa Muñiz, M.J.; Gagnon, D.R.; Gaziano, J.M.; Cho, K.; Casas, J.P.; et al. Comparative Effectiveness of BNT162b2 and mRNA-1273 Vaccines in US Veterans. N. Engl. J. Med. 2022, 386, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Eyre, D.W.; Taylor, D.; Purver, M.; Chapman, D.; Fowler, T.; Pouwels, K.B.; Walker, A.S.; Peto, T.E.A. Effect of Covid-19 Vaccination on Transmission of Alpha and Delta Variants. N. Engl. J. Med. 2022, 386, 744–756. [Google Scholar] [CrossRef] [PubMed]
- Young-Xu, Y.; Korves, C.; Roberts, J.; Powell, E.I.; Zwain, G.M.; Smith, J.; Izurieta, H.S. Coverage and Estimated Effectiveness of mRNA COVID-19 Vaccines among US Veterans. JAMA Netw. Open 2021, 4, e2128391. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Stella, A.O.; Walker, G.; Akerman, A.; Milogiannakis, V.; Brilot, F.; Amatayakul-Chantler, S.; Roth, N.; Coppola, G.; Schofield, P.; et al. SARS-CoV-2 Omicron: Evasion of Potent Humoral Responses and Resistance to Clinical Immunotherapeutics Relative to Viral Variants of Concern. 2022, 16. Available online: https://kirby.unsw.edu.au/sites/default/files/kirby/news/Pre-Print_Omicronevasion%20of%20potent%20humoral%20responses%20%26%20resistance%20to%20clinical%20immunotherapeutics%20relative%20to%20viral%20variants%20of%20concern.pdf/ (accessed on 21 February 2022).


{kind=link}
{kind=link}
| n | % | ||
|---|---|---|---|
| Vaccination status | Vaccinate | 3524 | 83.27 |
| Not vaccinated | 708 | 16.73 | |
| Total | 4232 | 100.00 | |
| RAD test result | Positive | 923 | 21.81 |
| Negative | 3309 | 78.19 | |
| Total | 4232 | 100.00 |
| Vaccination Status | RAD Test Result | Total | OR | 95% CI for OR | p | VE% | 95% CI for VE | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Positive | Negative | Lower | Higher | Lower | Higher | ||||||
| Overall | Vaccinated | 732 | 2793 | 3525 | 0.85 | 0.70 | 1.03 | 0.09 | 15 | −3 | 30 |
| Not vaccinated | 167 | 541 | 708 | ||||||||
| Total | 899 | 3334 | 4233 | ||||||||
| Male | Vaccinated | 450 | 1813 | 2263 | 0.68 | 0.54 | 0.86 | 0.00 ** | 32 | 14 | 46 |
| Not vaccinated | 115 | 315 | 430 | ||||||||
| Total | 565 | 2128 | 2693 | ||||||||
| Female | Vaccinated | 282 | 980 | 1262 | 1.25 | 0.90 | 1.75 | 0.18 | 25 | −75 | 10 |
| Not vaccinated | 52 | 226 | 278 | ||||||||
| Total | 334 | 1206 | 1540 | ||||||||
| 0–10 | Vaccinated | 0 | 0 | 0 | |||||||
| Not vaccinated | 21 | 64 | 85 | - | - | - | - | - | - | - | |
| Total | 21 | 64 | 85 | ||||||||
| 11–20 | Vaccinated | 33 | 117 | 150 | 0.63 | 0.38 | 1.05 | 0.08 | 37 | −5 | 62 |
| Not vaccinated | 53 | 120 | 173 | ||||||||
| Total | 86 | 237 | 323 | ||||||||
| 21–30 | Vaccinated | 180 | 764 | 944 | 1.11 | 0.72 | 1.73 | 0.61 | −10 | −73 | 28 |
| Not vaccinated | 28 | 133 | 61 | ||||||||
| Total | 208 | 897 | 105 | ||||||||
| 31–40 | Vaccinated | 242 | 873 | 1115 | 1.71 | 1.05 | 2.78 | 0.02 * | −71 | −178 | −5 |
| Not vaccinated | 21 | 130 | 151 | ||||||||
| Total | 263 | 1003 | 1266 | ||||||||
| 41–50 | Vaccinated | 158 | 614 | 772 | 0.75 | 0.43 | 1.31 | 0.32 | 25 | −31 | 57 |
| Not vaccinated | 19 | 56 | 75 | ||||||||
| Total | 177 | 670 | 847 | ||||||||
| 51–60 | Vaccinated | 90 | 288 | 378 | 1.18 | 0.54 | 2.55 | 0.67 | −18 | −155 | 46 |
| Not vaccinated | 9 | 34 | 43 | ||||||||
| Total | 99 | 322 | 421 | ||||||||
| ≥61 | Vaccinated | 53 | 112 | 165 | 0.41 | 0.18 | 0.91 | 0.02 * | 52 | 9 | 82 |
| Not vaccinated | 16 | 14 | 30 | ||||||||
| Total | 69 | 126 | 195 | ||||||||
| Age Group | Sex | OR | 95% CI for OR | p | VE (%) | 95% CI for VE | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Higher | Lower | Higher | |||||
| 0–10 | Male | - | - | - | - | - | - | - |
| Female | - | - | - | - | - | - | - | |
| 11–20 | Male | 0.60 | 0.30 | 1.20 | 0.15 | 40 | −20 | 70 |
| Female | 0.71 | 0.34 | 1.50 | 0.37 | 29 | −50 | 66 | |
| 21–30 | Male | 0.89 | 0.52 | 1.51 | 0.66 | 11 | −51 | 48 |
| Female | 1.46 | 0.66 | 3.22 | 0.35 | −46 | −222 | 34 | |
| 31–40 | Male | 1.49 | 0.84 | 2.65 | 0.17 | −49 | −165 | 16 |
| Female | 2.10 | 0.86 | 5.10 | 0.10 | −110 | −410 | 14 | |
| 41–50 | Male | 0.34 | 0.18 | 0.63 | 0.00 ** | 66 | 37 | 82 |
| Female | 8.63 | 1.15 | 64.62 | 0.01 * | −763 | −6362 | −15 | |
| 51–60 | Male | 0.87 | 0.36 | 2.15 | 0.77 | 13 | −115 | 64 |
| Female | 2.02 | 0.42 | 9.66 | 0.37 | −102 | 866 | 58 | |
| ≥61 | Male | 0.27 | 0.10 | 0.75 | 0.01 * | 73 | 25 | 90 |
| Female | 0.66 | 0.18 | 2.41 | 0.53 | 34 | −141 | 82 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Lemos, S.S.A.; da Silva, B.; de Sousa, C.A.P. First Scientific Evidence about the Estimation of the Odds Ratio in Vaccinated Individuals and Determination of Vaccine Efficacy against SARS-CoV-2 Infection in Angola—Part I. COVID 2022, 2, 1477-1490. https://doi.org/10.3390/covid2100106
de Lemos SSA, da Silva B, de Sousa CAP. First Scientific Evidence about the Estimation of the Odds Ratio in Vaccinated Individuals and Determination of Vaccine Efficacy against SARS-CoV-2 Infection in Angola—Part I. COVID. 2022; 2(10):1477-1490. https://doi.org/10.3390/covid2100106
Chicago/Turabian Stylede Lemos, Santland Sebastião Alberto, Belchior da Silva, and Carlos Alberto Pinto de Sousa. 2022. "First Scientific Evidence about the Estimation of the Odds Ratio in Vaccinated Individuals and Determination of Vaccine Efficacy against SARS-CoV-2 Infection in Angola—Part I" COVID 2, no. 10: 1477-1490. https://doi.org/10.3390/covid2100106
APA Stylede Lemos, S. S. A., da Silva, B., & de Sousa, C. A. P. (2022). First Scientific Evidence about the Estimation of the Odds Ratio in Vaccinated Individuals and Determination of Vaccine Efficacy against SARS-CoV-2 Infection in Angola—Part I. COVID, 2(10), 1477-1490. https://doi.org/10.3390/covid2100106