

Anomaly Detection and Artificial Intelligence Identified the Pathogenic Role of Apoptosis and RELB Proto-Oncogene, NF-kB Subunit in Diffuse Large B-Cell Lymphoma



Abstract

1. Introduction
1.1. Clinicopathological Characteristics and Prognosis of Diffuse Large B-Cell Lymphoma
1.2. Machine Learning and Anomaly Detection
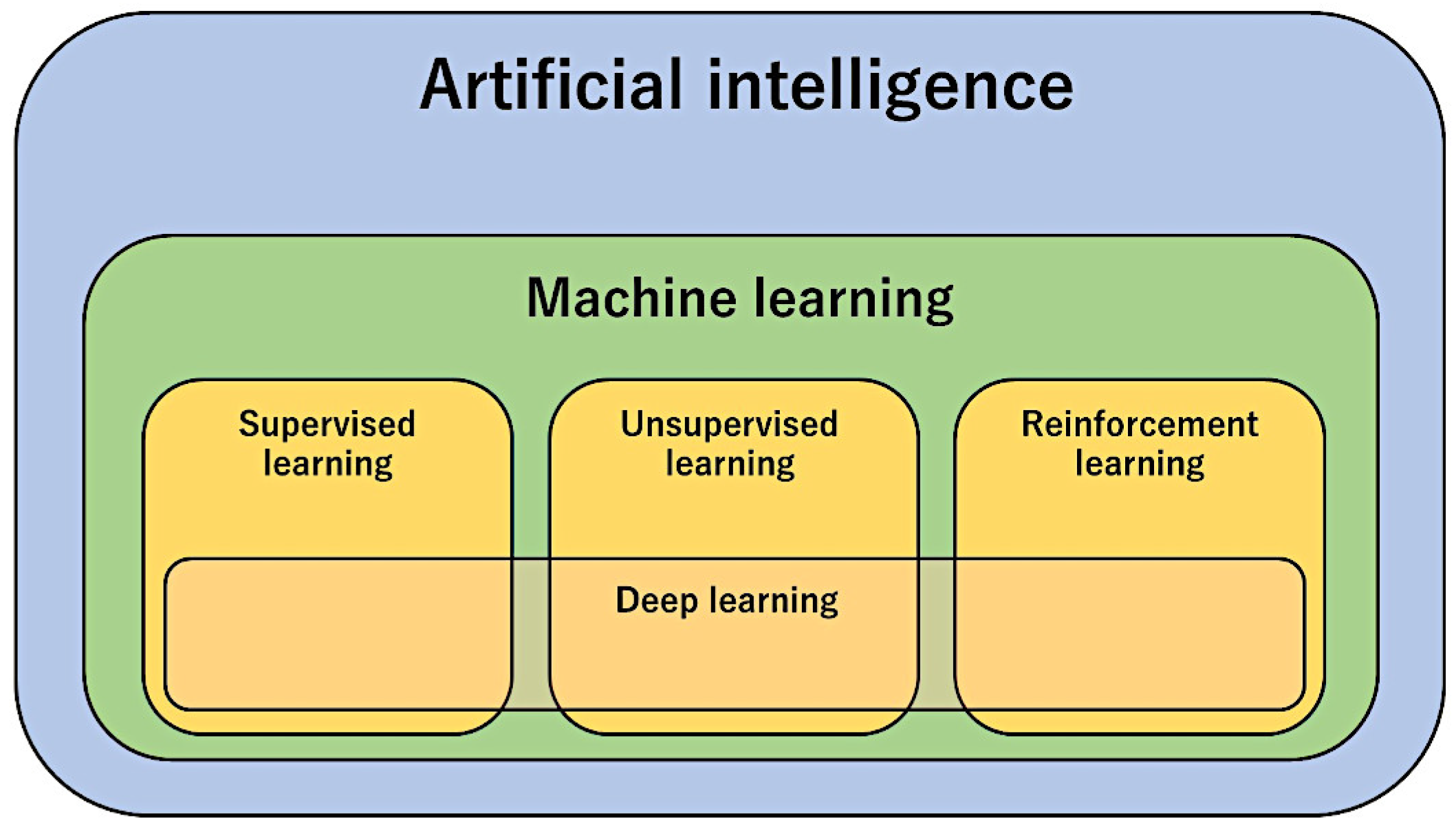
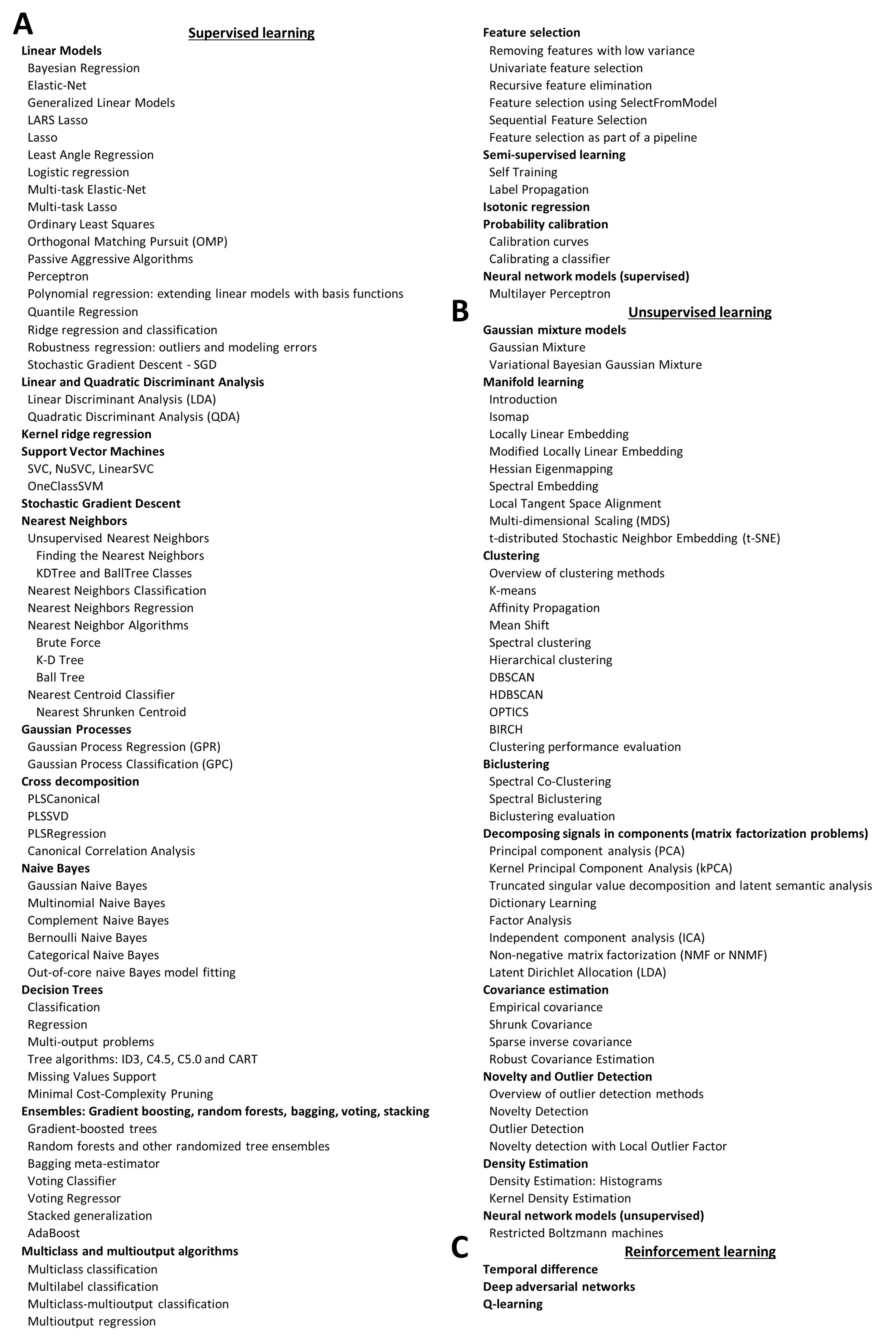
1.2.1. Machine Learning
1.2.2. Segmentation Analysis
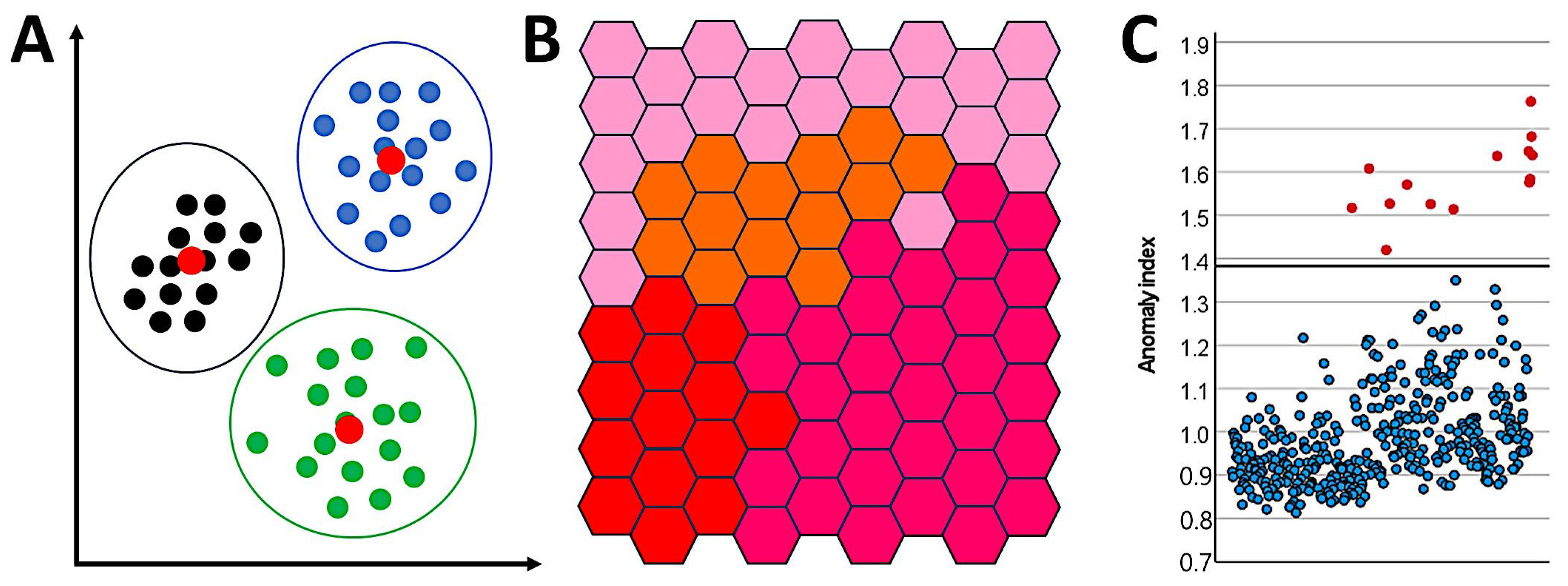
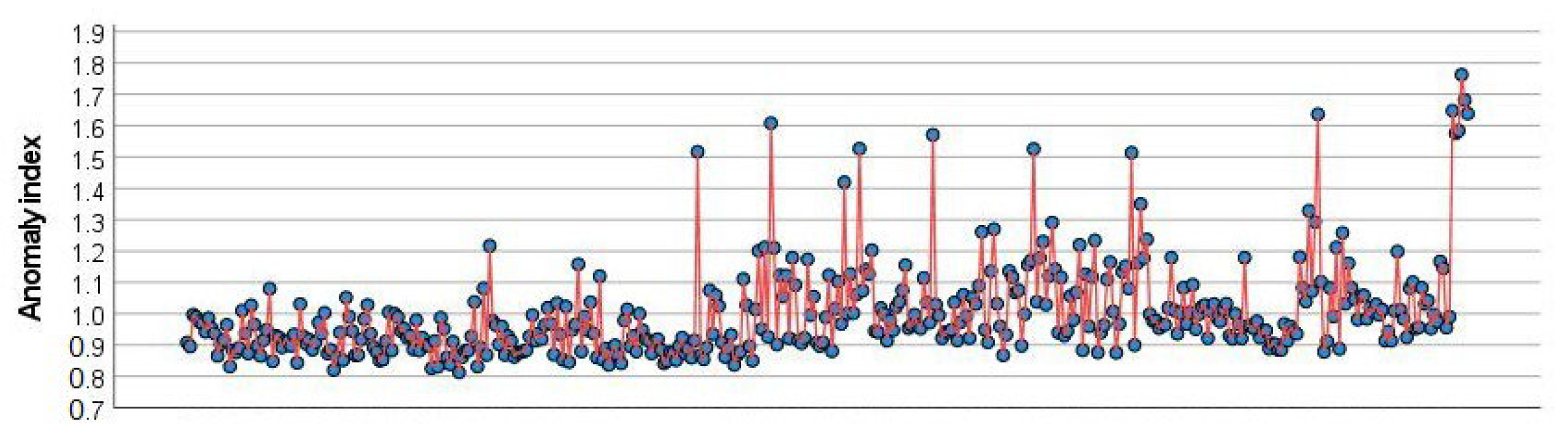
1.2.3. Anomaly Detection Analysis
2. Aim
3. Materials and Methods

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | Description |
|---|---|
| Anomaly detection | Method that quickly looks for unusual cases based on deviations from the norms of their cluster groups [51]. |
| Bayesian Network | Creates a graphical model that shows variables (nodes) linked using arcs. Probabilistic independencies between nodes are displayed. The arcs do not necessarily represent cause and effect [52,53,55,61]. |
| C5.0 | Builds a decision tree. It splits the samples on the basis of the variable that provides more information and has more weight. Then, multiple splits are made based on other variables until the cases cannot be further divided. Finally, splits with few contributions to the model are removed. This model can only predict a categorical target [58,62]. |
| C&R Tree | The classification and regression (C&R) tree is similar to the C5.0 method. All splits are binary [63]. |
| CHAID | Chi-squared Automatic Interaction Detection (CHAID) creates decision trees using calculations based on the chi-square test. Crosstabulations between the input variables and the output are examined, and the variables are ranked according to their significance for selection in the tree model [64,65,66,67,68]. |
| Discriminant | Creates a predictive model for group membership [69,70]. |
| KNN Algorithm | Nearest Neighbor Analysis classifies cases based on their similarity to other cases. This method identifies the pattern of the data [71]. |
| Logistic regression | Also known as nominal regression, it is a method that classifies records based on predictors in a manner similar to linear regression but with a categorical target variable. |
| LSVM | The data were classified on the basis of a linear support vector machine. This method is useful for large datasets with many variables [72,73]. |
| Neural Network | Basic units, known as neurons, are organized into different layers. The input layer contains nodes with input variables (predictors). The output layer contains nodes with the target fields. Nodes are interconnected by different strengths (weights). The number of hidden layers defines the “deep” of the network. Using training, the weights are changed from random to optimized, and the network replicates the known outcomes [74,75,76,77,78,79]. |
| Quest | Quick, Unbiased, Efficient Statistical (QUEST) tree creates a binary classification method. All splits are binary. |
| Random Forest | This is an implementation of the bagging algorithm. A collection of decision trees is used to make predictions [80,81,82]. |
| Random Trees | It is based on the C&R methodology and uses recursive partitioning to split records into segments with similar outputs [83]. |
| SVM | A support vector machine (SVM) is suitable when the dataset contains a very large number of predictors. It is a solid classification and regression technique that does not overfit the training data [84,85]. |
| Tree-AS | This method creates a decision tree using CHAID or exhaustive CHAID, which is more time-consuming [52,53,57]. |
| XGBoost Linear | Implementation of a gradient boosting algorithm with a linear model as the base [86]. |
| XGBoost Tree | Implementation of a gradient boosting algorithm with a tree model as the base [87,88,89,90,91,92,93,94]. |
4. Results
4.1. Anomaly Detection Analysis
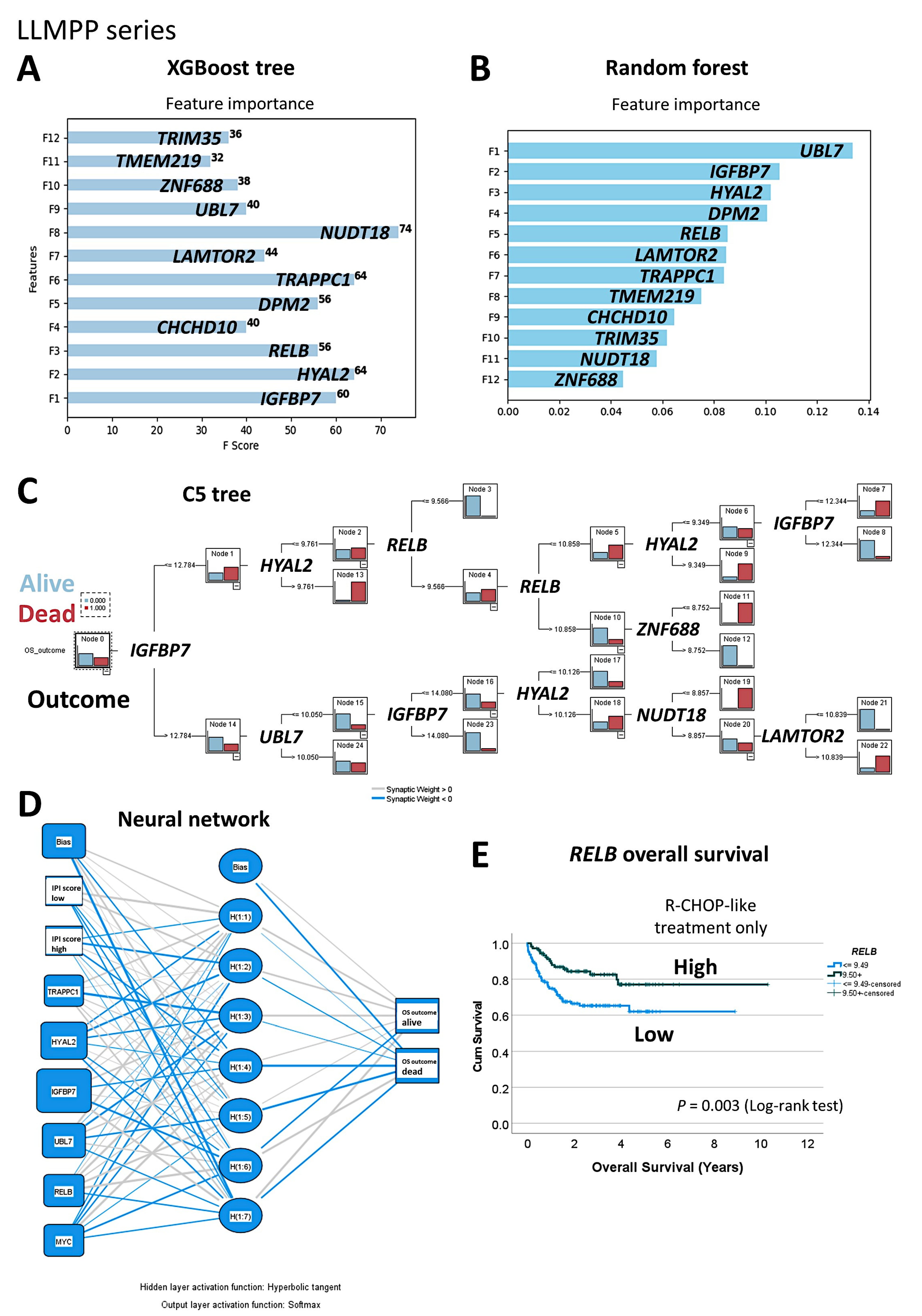
4.2. Prediction of Overall Survival Using Machine Learning and Artificial Neural Networks Based on 12 Genes
4.3. Cox Regression Analysis of Overall Survival Using the 12 Genes
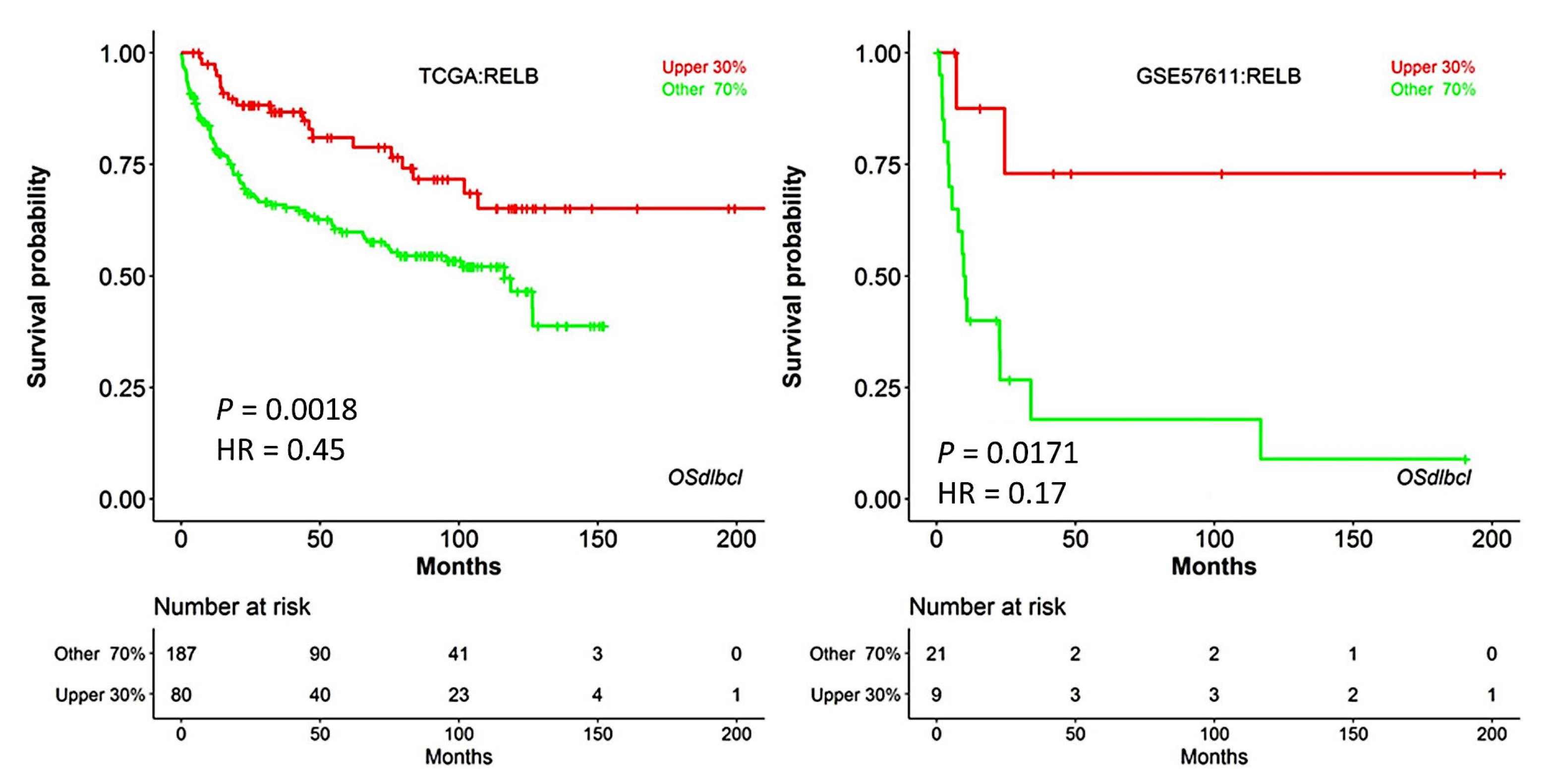
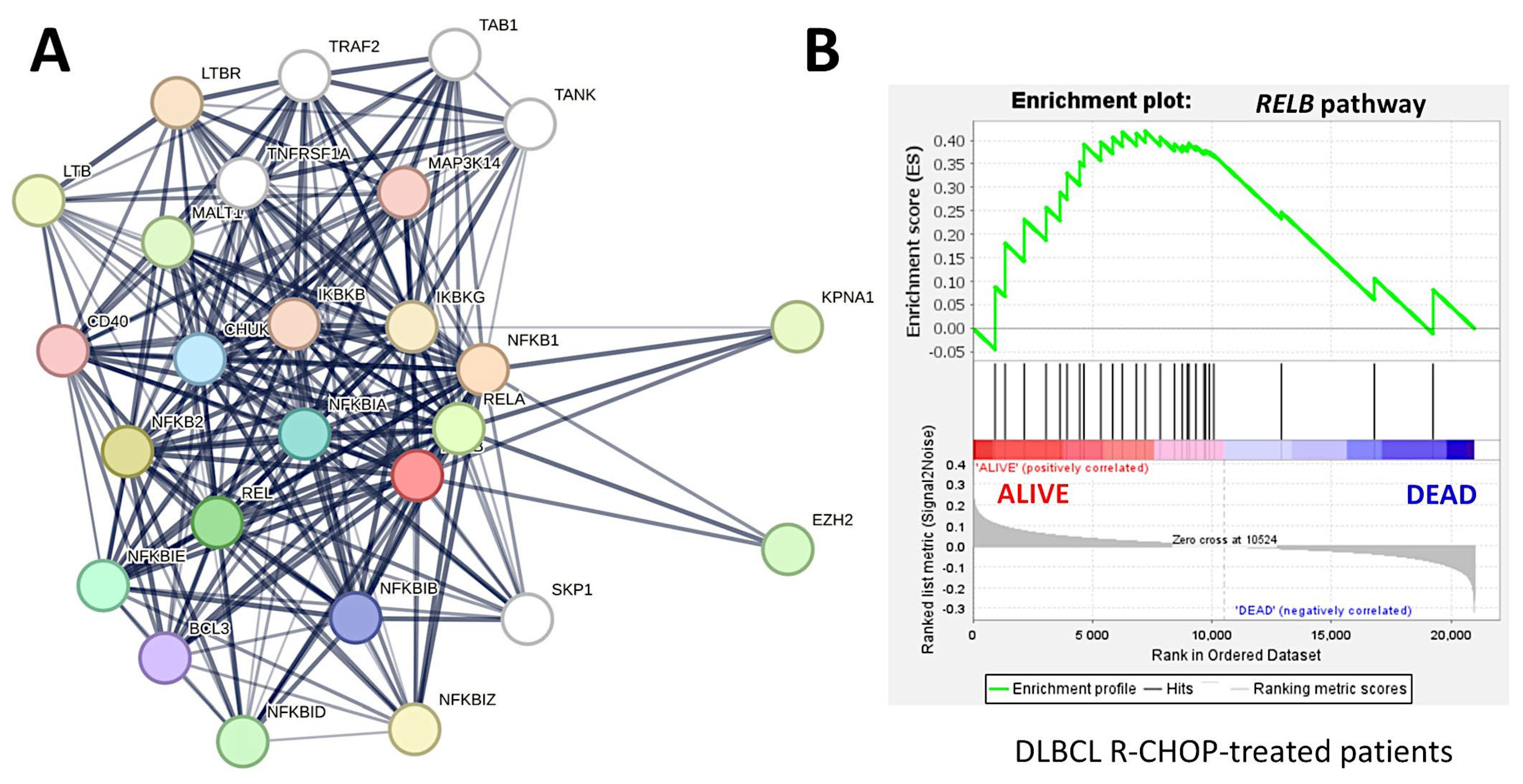
4.4. Validation of the Predictive Value of RELB for Overall Survival of Patients Using Gene Set Enrichment Analysis (RCHOP-Treated Cases)
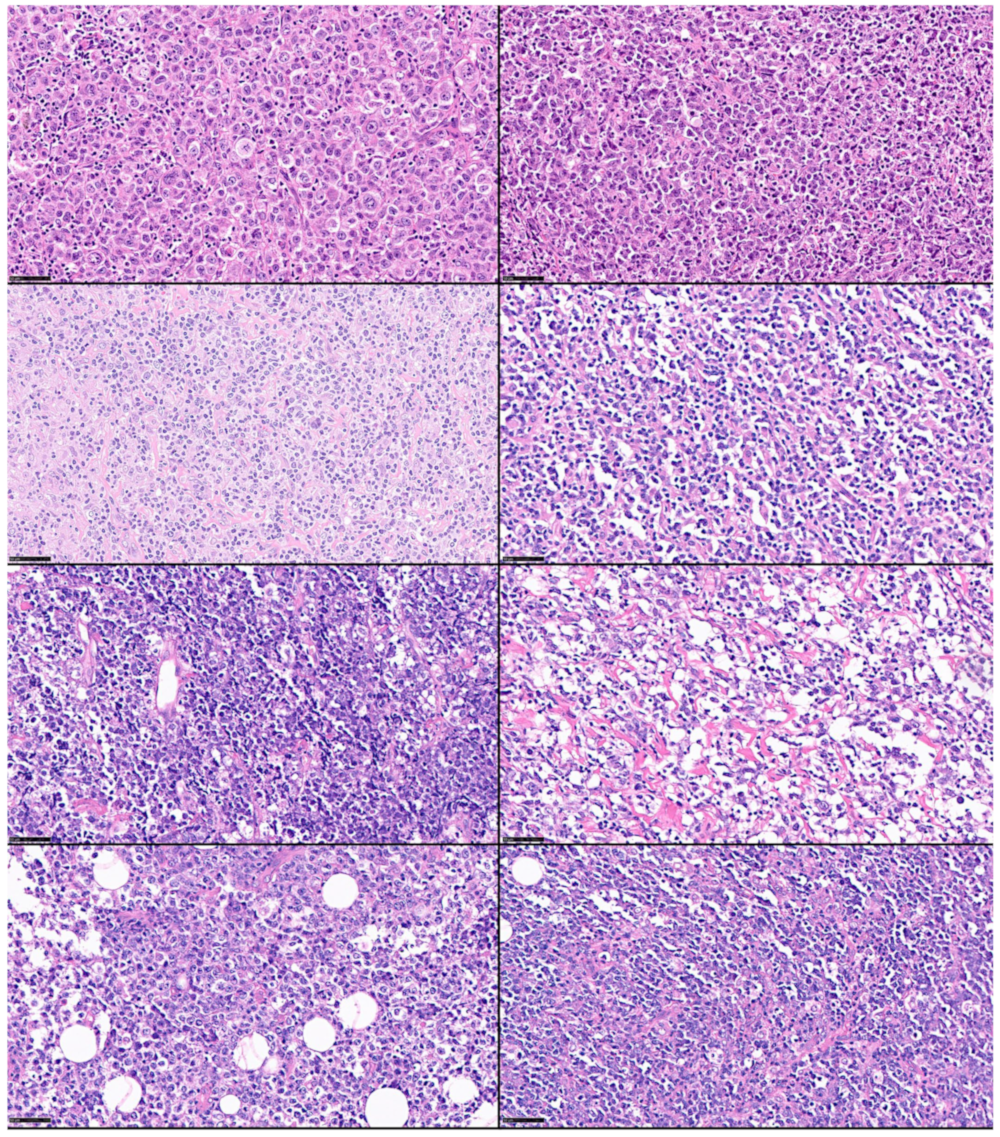
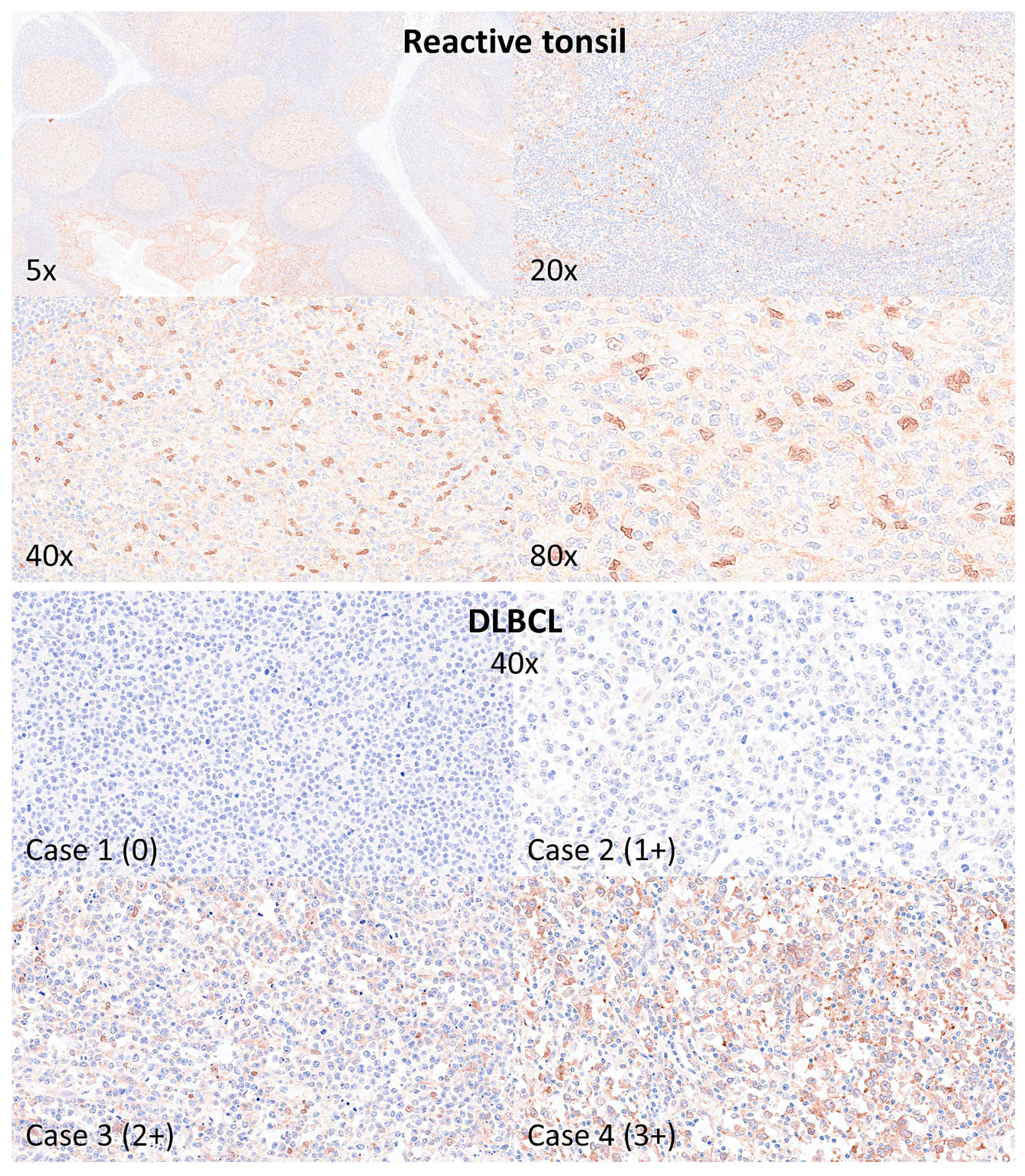
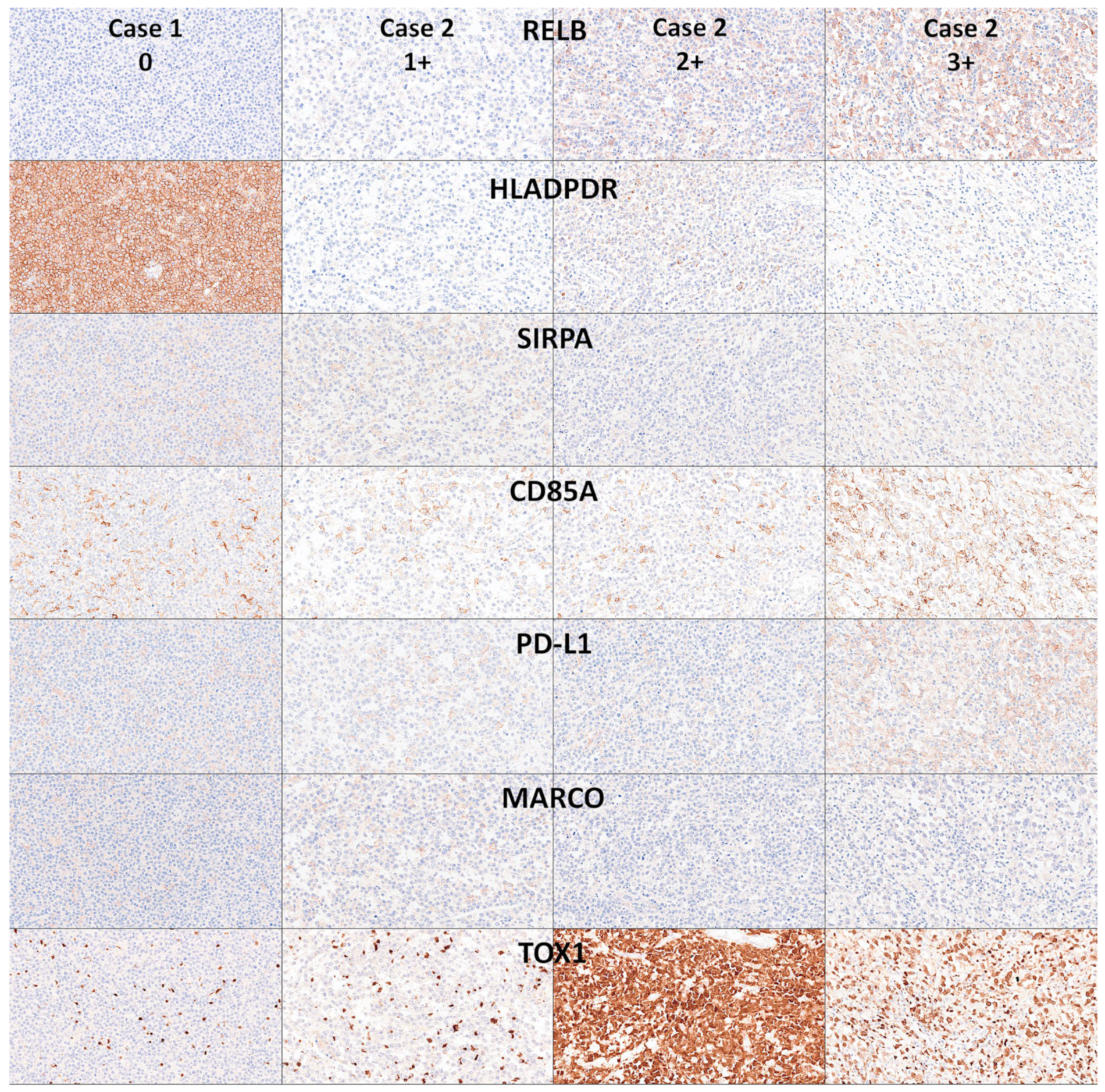
4.5. Immunohistochemical Analysis of RELB and Immune Microenvironment
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
References
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J.; Vardiman, J.W. (Eds.) WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th ed.; International Agency for Research on Cancer (IARC): Lyon, France, 2017. [Google Scholar]
- Campo, E.; Jaffe, E.S.; Cook, J.R.; Quintanilla-Martinez, L.; Swerdlow, S.H.; Anderson, K.C.; Brousset, P.; Cerroni, L.; de Leval, L.; Dirnhofer, S.; et al. The International Consensus Classification of Mature Lymphoid Neoplasms: A report from the Clinical Advisory Committee. Blood 2022, 140, 1229–1253. [Google Scholar] [CrossRef]
- Cazzola, M.; Sehn, L.H. Developing a classification of hematologic neoplasms in the era of precision medicine. Blood 2022, 140, 1193–1199. [Google Scholar] [CrossRef]
- De Leval, L.; Alizadeh, A.A.; Bergsagel, P.L.; Campo, E.; Davies, A.; Dogan, A.; Fitzgibbon, J.; Horwitz, S.M.; Melnick, A.M.; Morice, W.G.; et al. Genomic profiling for clinical decision making in lymphoid neoplasms. Blood 2022, 140, 2193–2227. [Google Scholar] [CrossRef]
- Alaggio, R.; Amador, C.; Anagnostopoulos, I.; Attygalle, A.D.; Araujo, I.B.O.; Berti, E.; Bhagat, G.; Borges, A.M.; Boyer, D.; Calaminici, M.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia 2022, 36, 1720–1748. [Google Scholar] [CrossRef]
- Quintanilla-Martinez, L.; Swerdlow, S.H.; Tousseyn, T.; Barrionuevo, C.; Nakamura, S.; Jaffe, E.S. New concepts in EBV-associated B, T, and NK cell lymphoproliferative disorders. Virchows Arch. 2023, 482, 227–244. [Google Scholar] [CrossRef]
- Laurent, C.; Cook, J.R.; Yoshino, T.; Quintanilla-Martinez, L.; Jaffe, E.S. Follicular lymphoma and marginal zone lymphoma: How many diseases? Virchows Arch. 2023, 482, 149–162. [Google Scholar] [CrossRef]
- Kurz, K.S.; Kalmbach, S.; Ott, M.; Staiger, A.M.; Ott, G.; Horn, H. Follicular Lymphoma in the 5th Edition of the WHO-Classification of Haematolymphoid Neoplasms-Updated Classification and New Biological Data. Cancers 2023, 15, 785. [Google Scholar] [CrossRef]
- Gianelli, U.; Thiele, J.; Orazi, A.; Gangat, N.; Vannucchi, A.M.; Tefferi, A.; Kvasnicka, H.M. International Consensus Classification of myeloid and lymphoid neoplasms: Myeloproliferative neoplasms. Virchows Arch. 2023, 482, 53–68. [Google Scholar] [CrossRef]
- De Leval, L.; Feldman, A.L.; Pileri, S.; Nakamura, S.; Gaulard, P. Extranodal T- and NK-cell lymphomas. Virchows Arch. 2023, 482, 245–264. [Google Scholar] [CrossRef]
- Coupland, S.E.; Du, M.Q.; Ferry, J.A.; de Jong, D.; Khoury, J.D.; Leoncini, L.; Naresh, K.N.; Ott, G.; Siebert, R.; Xerri, L.; et al. The fifth edition of the WHO classification of mature B-cell neoplasms: Open questions for research. J. Pathol. 2024, 262, 255–270. [Google Scholar] [CrossRef]
- Carreras, J.; Nakamura, N. Artificial Intelligence, Lymphoid Neoplasms, and Prediction of MYC, BCL2, and BCL6 Gene Expression Using a Pan-Cancer Panel in Diffuse Large B-Cell Lymphoma. Hemato 2024, 5, 119–143. [Google Scholar] [CrossRef]
- Jaffe, E.S.; Carbone, A. B- and T-/NK-Cell Lymphomas in the 2022 International Consensus Classification of Mature Lymphoid Neoplasms and Comparison with the WHO Fifth Edition. Hemato 2024, 5, 157–170. [Google Scholar] [CrossRef]
- Morton, L.M.; Wang, S.S.; Devesa, S.S.; Hartge, P.; Weisenburger, D.D.; Linet, M.S. Lymphoma incidence patterns by WHO subtype in the United States, 1992–2001. Blood 2006, 107, 265–276. [Google Scholar] [CrossRef]
- Smith, A.; Howell, D.; Patmore, R.; Jack, A.; Roman, E. Incidence of haematological malignancy by sub-type: A report from the Haematological Malignancy Research Network. Br. J. Cancer 2011, 105, 1684–1692. [Google Scholar] [CrossRef]
- Sant, M.; Allemani, C.; Tereanu, C.; De Angelis, R.; Capocaccia, R.; Visser, O.; Marcos-Gragera, R.; Maynadie, M.; Simonetti, A.; Lutz, J.M.; et al. Incidence of hematologic malignancies in Europe by morphologic subtype: Results of the HAEMACARE project. Blood 2010, 116, 3724–3734. [Google Scholar] [CrossRef]
- Shirley, M.H.; Sayeed, S.; Barnes, I.; Finlayson, A.; Ali, R. Incidence of haematological malignancies by ethnic group in England, 2001–2007. Br. J. Haematol. 2013, 163, 465–477. [Google Scholar] [CrossRef]
- Chadburn, A.; Gloghini, A.; Carbone, A. Classification of B-Cell Lymphomas and Immunodeficiency-Related Lymphoproliferations: What’s New? Hemato 2023, 4, 26–41. [Google Scholar] [CrossRef]
- De Leval, L.; Jaffe, E.S. Lymphoma Classification. Cancer J. 2020, 26, 176–185. [Google Scholar] [CrossRef]
- Ricard, F.; Cheson, B.; Barrington, S.; Trotman, J.; Schmid, A.; Brueggenwerth, G.; Salles, G.; Schwartz, L.; Goldmacher, G.; Jarecha, R.; et al. Application of the Lugano Classification for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The PRoLoG Consensus Initiative (Part 1-Clinical). J. Nucl. Med. 2023, 64, 102–108. [Google Scholar] [CrossRef]
- Hartmann, S.; Fend, F. Classification of Hodgkin lymphoma and related entities: News and open questions. Pathologie 2023, 44, 184–192. [Google Scholar] [CrossRef]
- Shimkus, G.; Nonaka, T. Molecular classification and therapeutics in diffuse large B-cell lymphoma. Front. Mol. Biosci. 2023, 10, 1124360. [Google Scholar] [CrossRef]
- Goodlad, J.R.; Cerroni, L.; Swerdlow, S.H. Recent advances in cutaneous lymphoma-implications for current and future classifications. Virchows Arch. 2023, 482, 281–298. [Google Scholar] [CrossRef]
- King, R.L.; Hsi, E.D.; Chan, W.C.; Piris, M.A.; Cook, J.R.; Scott, D.W.; Swerdlow, S.H. Diagnostic approaches and future directions in Burkitt lymphoma and high-grade B-cell lymphoma. Virchows Arch. 2023, 482, 193–205. [Google Scholar] [CrossRef]
- Kurz, K.S.; Ott, M.; Kalmbach, S.; Steinlein, S.; Kalla, C.; Horn, H.; Ott, G.; Staiger, A.M. Large B-Cell Lymphomas in the 5th Edition of the WHO-Classification of Haematolymphoid Neoplasms-Updated Classification and New Concepts. Cancers 2023, 15, 2285. [Google Scholar] [CrossRef]
- Carreras, J. The pathobiology of follicular lymphoma. J. Clin. Exp. Hematopathol. 2023, 63, 152–163. [Google Scholar] [CrossRef]
- Rosenwald, A.; Menter, T.; Dirnhofer, S. Classification of aggressive B-cell lymphomas: News and open questions. Pathologie 2023, 44, 166–172. [Google Scholar] [CrossRef]
- Rodriguez-Pinilla, S.M.; Dojcinov, S.; Dotlic, S.; Gibson, S.E.; Hartmann, S.; Klimkowska, M.; Sabattini, E.; Tousseyn, T.A.; de Jong, D.; Hsi, E.D. Aggressive B-cell non-Hodgkin lymphomas: A report of the lymphoma workshop of the 20th meeting of the European Association for Haematopathology. Virchows Arch. 2024, 484, 15–29. [Google Scholar] [CrossRef]
- Attygalle, A.D.; Chan, J.K.C.; Coupland, S.E.; Du, M.Q.; Ferry, J.A.; Jong, D.; Gratzinger, D.; Lim, M.S.; Naresh, K.N.; Nicolae, A.; et al. The 5th edition of the World Health Organization Classification of mature lymphoid and stromal tumors—An overview and update. Leuk. Lymphoma 2024, 65, 413–429. [Google Scholar] [CrossRef]
- Arber, D.A.; Campo, E.; Jaffe, E.S. Advances in the Classification of Myeloid and Lymphoid Neoplasms. Virchows Arch. 2023, 482, 1–9. [Google Scholar] [CrossRef]
- Song, J.Y.; Dirnhofer, S.; Piris, M.A.; Quintanilla-Martinez, L.; Pileri, S.; Campo, E. Diffuse large B-cell lymphomas, not otherwise specified, and emerging entities. Virchows Arch. 2023, 482, 179–192. [Google Scholar] [CrossRef]
- Campo, E. The 2022 classifications of lymphoid neoplasms: Keynote. Pathologie 2023, 44, 121–127. [Google Scholar] [CrossRef]
- Liu, Y.; Barta, S.K. Diffuse large B-cell lymphoma: 2019 update on diagnosis, risk stratification, and treatment. Am. J. Hematol. 2019, 94, 604–616. [Google Scholar] [CrossRef]
- Ruppert, A.S.; Dixon, J.G.; Salles, G.; Wall, A.; Cunningham, D.; Poeschel, V.; Haioun, C.; Tilly, H.; Ghesquieres, H.; Ziepert, M.; et al. International prognostic indices in diffuse large B-cell lymphoma: A comparison of IPI, R-IPI, and NCCN-IPI. Blood 2020, 135, 2041–2048. [Google Scholar] [CrossRef]
- Zhou, Z.; Sehn, L.H.; Rademaker, A.W.; Gordon, L.I.; Lacasce, A.S.; Crosby-Thompson, A.; Vanderplas, A.; Zelenetz, A.D.; Abel, G.A.; Rodriguez, M.A.; et al. An enhanced International Prognostic Index (NCCN-IPI) for patients with diffuse large B-cell lymphoma treated in the rituximab era. Blood 2014, 123, 837–842. [Google Scholar] [CrossRef]
- Wright, G.W.; Huang, D.W.; Phelan, J.D.; Coulibaly, Z.A.; Roulland, S.; Young, R.M.; Wang, J.Q.; Schmitz, R.; Morin, R.D.; Tang, J.; et al. A Probabilistic Classification Tool for Genetic Subtypes of Diffuse Large B Cell Lymphoma with Therapeutic Implications. Cancer Cell 2020, 37, 551–568.e514. [Google Scholar] [CrossRef]
- What Is Artificial Intelligence? IBM Topics Artificial-Intelligence. Available online: https://www.ibm.com/topics/artificial-intelligence (accessed on 22 January 2024).
- Deep Learning vs. Machine Learning. IBM Topics Artificial-Intelligence. Available online: https://www.ibm.com/think/topics/ai-vs-machine-learning-vs-deep-learning-vs-neural-networks (accessed on 22 January 2024).
- What Is Unsupervised Learning? IBM Topics Unsupervised-Learning. Available online: https://www.ibm.com/topics/unsupervised-learning (accessed on 22 January 2024).
- What Is Reinforcement Learning? IBM Developer. Available online: https://developer.ibm.com/learningpaths/get-started-automated-ai-for-decision-making-api/what-is-automated-ai-for-decision-making/ (accessed on 22 January 2024).
- Prince, S.J.D. Understanding Deep Learning; MIT Press: Cambridge, MA, USA, 2023. [Google Scholar]
- McLachlan, G.J.; Bean, R.W.; Ng, S.K. Clustering. Methods Mol. Biol. 2017, 1526, 345–362. [Google Scholar] [CrossRef]
- Orsoni, M.; Giovagnoli, S.; Garofalo, S.; Magri, S.; Benvenuti, M.; Mazzoni, E.; Benassi, M. Preliminary evidence on machine learning approaches for clusterizing students’ cognitive profile. Heliyon 2023, 9, e14506. [Google Scholar] [CrossRef]
- Zampighi, L.M.; Kavanau, C.L.; Zampighi, G.A. The Kohonen self-organizing map: A tool for the clustering and alignment of single particles imaged using random conical tilt. J. Struct. Biol. 2004, 146, 368–380. [Google Scholar] [CrossRef]
- RStudio. Anomaly Detection in R (DataCamp), Ch. 1—Statistical Outlier Detection. Available online: https://rpubs.com/michaelmallari/anomaly-detection-r (accessed on 22 January 2024).
- Developer, I. Anomaly Detection. Available online: https://developer.ibm.com/apis/catalog/ai4industry--anomaly-detection-product/Introduction (accessed on 22 January 2024).
- Corporation, I. IBM Business Predictive Analytics, Algorithms Guide; IBM Software Group 1994; IBM Corporation: Armonk, NY, USA, 2021. [Google Scholar]
- Cardesa-Salzmann, T.M.; Colomo, L.; Gutierrez, G.; Chan, W.C.; Weisenburger, D.; Climent, F.; Gonzalez-Barca, E.; Mercadal, S.; Arenillas, L.; Serrano, S.; et al. High microvessel density determines a poor outcome in patients with diffuse large B-cell lymphoma treated with rituximab plus chemotherapy. Haematologica 2011, 96, 996–1001. [Google Scholar] [CrossRef]
- Lenz, G.; Wright, G.; Dave, S.S.; Xiao, W.; Powell, J.; Zhao, H.; Xu, W.; Tan, B.; Goldschmidt, N.; Iqbal, J.; et al. Stromal gene signatures in large-B-cell lymphomas. N. Engl. J. Med. 2008, 359, 2313–2323. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.Y.; Miyaoka, M.; Roncador, G.; Garcia, J.F.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; et al. Integrative Statistics, Machine Learning and Artificial Intelligence Neural Network Analysis Correlated CSF1R with the Prognosis of Diffuse Large B-Cell Lymphoma. Hemato 2021, 2, 182–206. [Google Scholar] [CrossRef]
- Carreras, J. Supplementary Data 2 (Version 2). Zenodo. 2024. Available online: https://zenodo.org/records/11058101 (accessed on 24 April 2024).
- Carreras, J. Artificial Intelligence Analysis of Ulcerative Colitis Using an Autoimmune Discovery Transcriptomic Panel. Healthcare 2022, 10, 1476. [Google Scholar] [CrossRef]
- Carreras, J. Artificial Intelligence Analysis of Celiac Disease Using an Autoimmune Discovery Transcriptomic Panel Highlighted Pathogenic Genes including BTLA. Healthcare 2022, 10, 1550. [Google Scholar] [CrossRef]
- Carreras, J.; Hamoudi, R.; Nakamura, N. Artificial Intelligence Analysis of Gene Expression Data Predicted the Prognosis of Patients with Diffuse Large B-Cell Lymphoma. Tokai J. Exp. Clin. Med. 2020, 45, 37–48. [Google Scholar]
- Carreras, J.; Hiraiwa, S.; Kikuti, Y.Y.; Miyaoka, M.; Tomita, S.; Ikoma, H.; Ito, A.; Kondo, Y.; Roncador, G.; Garcia, J.F.; et al. Artificial Neural Networks Predicted the Overall Survival and Molecular Subtypes of Diffuse Large B-Cell Lymphoma Using a Pancancer Immune-Oncology Panel. Cancers 2021, 13, 6384. [Google Scholar] [CrossRef]
- Carreras, J.; Nakamura, N.; Hamoudi, R. Artificial Intelligence Analysis of Gene Expression Predicted the Overall Survival of Mantle Cell Lymphoma and a Large Pan-Cancer Series. Healthcare 2022, 10, 155. [Google Scholar] [CrossRef]
- Carreras, J.; Roncador, G.; Hamoudi, R. Artificial Intelligence Predicted Overall Survival and Classified Mature B-Cell Neoplasms Based on Immuno-Oncology and Immune Checkpoint Panels. Cancers 2022, 14, 5318. [Google Scholar] [CrossRef]
- Carreras, J.; Yukie Kikuti, Y.; Miyaoka, M.; Miyahara, S.; Roncador, G.; Hamoudi, R.; Nakamura, N. Artificial Intelligence Analysis and Reverse Engineering of Molecular Subtypes of Diffuse Large B-Cell Lymphoma Using Gene Expression Data. BioMedInformatics 2024, 4, 295–320. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.Y.; Miyaoka, M.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; Nagase, S.; Miura, H.; et al. Mutational Profile and Pathological Features of a Case of Interleukin-10 and RGS1-Positive Spindle Cell Variant Diffuse Large B-Cell Lymphoma. Hematol. Rep. 2023, 15, 188–200. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.Y.; Hiraiwa, S.; Miyaoka, M.; Tomita, S.; Ikoma, H.; Ito, A.; Kondo, Y.; Itoh, J.; Roncador, G.; et al. High PTX3 expression is associated with a poor prognosis in diffuse large B-cell lymphoma. Cancer Sci. 2022, 113, 334–348. [Google Scholar] [CrossRef]
- Li, Q.; Dou, M.; Zhang, J.; Jia, P.; Wang, X.; Lei, D.; Li, J.; Yang, W.; Yang, R.; Yang, C.; et al. A Bayesian network model to predict neoplastic risk for patients with gallbladder polyps larger than 10 mm based on preoperative ultrasound features. Surg. Endosc. 2023, 37, 5453–5463. [Google Scholar] [CrossRef]
- C5.0 Node. Available online: https://www.ibm.com/us-en (accessed on 25 April 2024).
- Asadi, F.; Salehnasab, C.; Ajori, L. Supervised Algorithms of Machine Learning for the Prediction of Cervical Cancer. J. Biomed. Phys. Eng. 2020, 10, 513–522. [Google Scholar] [CrossRef]
- Bottel, L.; Brand, M.; Dieris-Hirche, J.; Pape, M.; Herpertz, S.; Te Wildt, B.T. Predictive power of the DSM-5 criteria for internet use disorder: A CHAID decision-tree analysis. Front. Psychol. 2023, 14, 1129769. [Google Scholar] [CrossRef]
- Diaz-Perez, F.M.; Garcia-Gonzalez, C.G.; Fyall, A. The use of the CHAID algorithm for determining tourism segmentation: A purposeful outcome. Heliyon 2020, 6, e04256. [Google Scholar] [CrossRef]
- Kaya, S.; Guven, G.S.; Aydan, S.; Toka, O. A comprehensive framework identifying readmission risk factors using the CHAID algorithm: A prospective cohort study. Int. J. Qual. Health Care 2018, 30, 366–374. [Google Scholar] [CrossRef]
- Meydanlioglu, A.; Akcan, A.; Oncel, S.; Adibelli, D.; Cicek Gumus, E.; Sarvan, S.; Kavla, I. Prevalence of obesity and hypertension in children and determination of associated factors by CHAID analysis. Arch. Pediatr. 2022, 29, 30–35. [Google Scholar] [CrossRef]
- Murphy, E.L.; Comiskey, C.M. Using chi-Squared Automatic Interaction Detection (CHAID) modelling to identify groups of methadone treatment clients experiencing significantly poorer treatment outcomes. J. Subst. Abus. Treat. 2013, 45, 343–349. [Google Scholar] [CrossRef]
- Solberg, H.E. Discriminant analysis. CRC Crit. Rev. Clin. Lab. Sci. 1978, 9, 209–242. [Google Scholar] [CrossRef]
- Chan, Y.H. Biostatistics 303. Discriminant analysis. Singap. Med. J. 2005, 46, 54–61, quiz 62. [Google Scholar]
- Carreras, J. KNN Algorithms (Version 1). Zenodo. 2024. Available online: https://zenodo.org/records/11058452 (accessed on 24 April 2024).
- Lu, J.; Chen, Q.; Li, D.; Zhang, W.; Xing, S.; Wang, J.; Zhang, X.; Liu, J.; Qing, Z.; Dai, Y.; et al. Reconfiguration of Dynamic Functional Connectivity States in Patients With Lifelong Premature Ejaculation. Front. Neurosci. 2021, 15, 721236. [Google Scholar] [CrossRef]
- Arabi, E.M.; Ahmed, K.S.; Mohra, A.S. Advanced Diagnostic Technique for Alzheimer’s Disease using MRI Top-Ranked Volume and Surface-based Features. J. Biomed. Phys. Eng. 2022, 12, 569–582. [Google Scholar] [CrossRef]
- Ali, R.; Hussain, J.; Lee, S.W. Multilayer perceptron-based self-care early prediction of children with disabilities. Digit. Health 2023, 9, 20552076231184054. [Google Scholar] [CrossRef]
- Ivanov, A.S.; Nikolaev, K.G.; Novikov, A.S.; Yurchenko, S.O.; Novoselov, K.S.; Andreeva, D.V.; Skorb, E.V. Programmable Soft-Matter Electronics. J. Phys. Chem. Lett. 2021, 12, 2017–2022. [Google Scholar] [CrossRef]
- Majidzadeh Gorjani, O.; Byrtus, R.; Dohnal, J.; Bilik, P.; Koziorek, J.; Martinek, R. Human Activity Classification Using Multilayer Perceptron. Sensors 2021, 21, 6207. [Google Scholar] [CrossRef]
- Lyu, J.; Shi, H.; Zhang, J.; Norvilitis, J. Prediction model for suicide based on back propagation neural network and multilayer perceptron. Front. Neuroinform. 2022, 16, 961588. [Google Scholar] [CrossRef]
- Fujita, T.; Sato, A.; Narita, A.; Sone, T.; Iokawa, K.; Tsuchiya, K.; Yamane, K.; Yamamoto, Y.; Ohira, Y.; Otsuki, K. Use of a multilayer perceptron to create a prediction model for dressing independence in a small sample at a single facility. J. Phys. Ther. Sci. 2019, 31, 69–74. [Google Scholar] [CrossRef]
- Radhakrishnan, S.; Nair, S.G.; Isaac, J. Multilayer perceptron neural network model development for mechanical ventilator parameters prediction by real time system learning. Biomed. Signal Process. Control 2022, 71, 103170. [Google Scholar] [CrossRef]
- Rigatti, S.J. Random Forest. J. Insur. Med. 2017, 47, 31–39. [Google Scholar] [CrossRef]
- Rhodes, J.S.; Cutler, A.; Moon, K.R. Geometry- and Accuracy-Preserving Random Forest Proximities. IEEE Trans. Pattern Anal. Mach. Intell. 2023, 45, 10947–10959. [Google Scholar] [CrossRef]
- Asadi, S.; Roshan, S.; Kattan, M.W. Random forest swarm optimization-based for heart diseases diagnosis. J. Biomed. Inform. 2021, 115, 103690. [Google Scholar] [CrossRef]
- Elbeltagi, A.; Pande, C.B.; Kumar, M.; Tolche, A.D.; Singh, S.K.; Kumar, A.; Vishwakarma, D.K. Prediction of meteorological drought and standardized precipitation index based on the random forest (RF), random tree (RT), and Gaussian process regression (GPR) models. Environ. Sci. Pollut. Res. Int. 2023, 30, 43183–43202. [Google Scholar] [CrossRef]
- Mehta, S.D.; Sebro, R. Computer-Aided Detection of Incidental Lumbar Spine Fractures from Routine Dual-Energy X-Ray Absorptiometry (DEXA) Studies Using a Support Vector Machine (SVM) Classifier. J. Digit. Imaging 2020, 33, 204–210. [Google Scholar] [CrossRef]
- Han, H.; Jiang, X. Overcome support vector machine diagnosis overfitting. Cancer Inform. 2014, 13, 145–158. [Google Scholar] [CrossRef]
- Yehuda, B.; Rabinowich, A.; Link-Sourani, D.; Avisdris, N.; Ben-Zvi, O.; Specktor-Fadida, B.; Joskowicz, L.; Ben-Sira, L.; Miller, E.; Ben Bashat, D. Automatic Quantification of Normal Brain Gyrification Patterns and Changes in Fetuses with Polymicrogyria and Lissencephaly Based on MRI. AJNR Am. J. Neuroradiol. 2023, 44, 1432–1439. [Google Scholar] [CrossRef]
- Raubitzek, S.; Neubauer, T. An Exploratory Study on the Complexity and Machine Learning Predictability of Stock Market Data. Entropy 2022, 24, 332. [Google Scholar] [CrossRef]
- Thedinga, K.; Herwig, R. A gradient tree boosting and network propagation derived pan-cancer survival network of the tumor microenvironment. iScience 2022, 25, 103617. [Google Scholar] [CrossRef]
- Thedinga, K.; Herwig, R. Gradient tree boosting and network propagation for the identification of pan-cancer survival networks. STAR Protoc. 2022, 3, 101353. [Google Scholar] [CrossRef]
- Pfob, A.; Sidey-Gibbons, C.; Lee, H.B.; Tasoulis, M.K.; Koelbel, V.; Golatta, M.; Rauch, G.M.; Smith, B.D.; Valero, V.; Han, W.; et al. Identification of breast cancer patients with pathologic complete response in the breast after neoadjuvant systemic treatment by an intelligent vacuum-assisted biopsy. Eur. J. Cancer 2021, 143, 134–146. [Google Scholar] [CrossRef]
- Nistal-Nuno, B. Machine learning applied to a Cardiac Surgery Recovery Unit and to a Coronary Care Unit for mortality prediction. J. Clin. Monit. Comput. 2022, 36, 751–763. [Google Scholar] [CrossRef]
- Tran, T.; Le, U.; Shi, Y. An effective up-sampling approach for breast cancer prediction with imbalanced data: A machine learning model-based comparative analysis. PLoS ONE 2022, 17, e0269135. [Google Scholar] [CrossRef]
- Pfob, A.; Mehrara, B.J.; Nelson, J.A.; Wilkins, E.G.; Pusic, A.L.; Sidey-Gibbons, C. Machine learning to predict individual patient-reported outcomes at 2-year follow-up for women undergoing cancer-related mastectomy and breast reconstruction (INSPiRED-001). Breast 2021, 60, 111–122. [Google Scholar] [CrossRef]
- Janjua, H.; Barry, T.M.; Cousin-Peterson, E.; Kuo, P.C. Defining the relative contribution of health care environmental components to patient outcomes in the model of 30-day readmission after coronary artery bypass graft (CABG). Surgery 2021, 169, 557–566. [Google Scholar] [CrossRef]
- Dominguez-Gutierrez, P.R.; Kwenda, E.P.; Donelan, W.; O’Malley, P.; Crispen, P.L.; Kusmartsev, S. Hyal2 Expression in Tumor-Associated Myeloid Cells Mediates Cancer-Related Inflammation in Bladder Cancer. Cancer Res. 2021, 81, 648–657. [Google Scholar] [CrossRef]
- Tan, X.; Cao, F.; Tang, F.; Lu, C.; Yu, Q.; Feng, S.; Yang, Z.; Chen, S.; He, X.; He, J.; et al. Suppression of DLBCL Progression by the E3 Ligase Trim35 Is Mediated by CLOCK Degradation and NK Cell Infiltration. J. Immunol. Res. 2021, 2021, 9995869. [Google Scholar] [CrossRef]
- Wang, R.; Huang, K.L.; Xing, L.X. TRIM35 functions as a novel tumor suppressor in breast cancer by inducing cell apoptosis through ubiquitination of PDK1. Neoplasma 2022, 69, 370–382. [Google Scholar] [CrossRef]
- Dang, W.; Cao, P.; Yan, Q.; Yang, L.; Wang, Y.; Yang, J.; Xin, S.; Zhang, J.; Li, J.; Long, S.; et al. IGFBP7-AS1 is a p53-responsive long noncoding RNA downregulated by Epstein-Barr virus that contributes to viral tumorigenesis. Cancer Lett. 2021, 523, 135–147. [Google Scholar] [CrossRef]
- Wu, S.G.; Chang, T.H.; Tsai, M.F.; Liu, Y.N.; Hsu, C.L.; Chang, Y.L.; Yu, C.J.; Shih, J.Y. IGFBP7 Drives Resistance to Epidermal Growth Factor Receptor Tyrosine Kinase Inhibition in Lung Cancer. Cancers 2019, 11, 36. [Google Scholar] [CrossRef]
- De Araujo, M.E.; Erhart, G.; Buck, K.; Muller-Holzner, E.; Hubalek, M.; Fiegl, H.; Campa, D.; Canzian, F.; Eilber, U.; Chang-Claude, J.; et al. Polymorphisms in the gene regions of the adaptor complex LAMTOR2/LAMTOR3 and their association with breast cancer risk. PLoS ONE 2013, 8, e53768. [Google Scholar] [CrossRef]
- Zhang, S.; Liu, Y.; Chen, J.; Shu, H.; Shen, S.; Li, Y.; Lu, X.; Cao, X.; Dong, L.; Shi, J.; et al. Autoantibody signature in hepatocellular carcinoma using seromics. J. Hematol. Oncol. 2020, 13, 85. [Google Scholar] [CrossRef]
- Luo, L.; Li, L.; Liu, L.; Feng, Z.; Zeng, Q.; Shu, X.; Cao, Y.; Li, Z. A Necroptosis-Related lncRNA-Based Signature to Predict Prognosis and Probe Molecular Characteristics of Stomach Adenocarcinoma. Front. Genet. 2022, 13, 833928. [Google Scholar] [CrossRef]
- Eluard, B.; Nuan-Aliman, S.; Faumont, N.; Collares, D.; Bordereaux, D.; Montagne, A.; Martins, I.; Cagnard, N.; Caly, M.; Taoui, O.; et al. The alternative RelB NF-kappaB subunit is a novel critical player in diffuse large B-cell lymphoma. Blood 2022, 139, 384–398. [Google Scholar] [CrossRef]
- Nuan-Aliman, S.; Bordereaux, D.; Thieblemont, C.; Baud, V. The Alternative RelB NF-kB Subunit Exerts a Critical Survival Function upon Metabolic Stress in Diffuse Large B-Cell Lymphoma-Derived Cells. Biomedicines 2022, 10, 348. [Google Scholar] [CrossRef]
- Sha, C.; Barrans, S.; Cucco, F.; Bentley, M.A.; Care, M.A.; Cummin, T.; Kennedy, H.; Thompson, J.S.; Uddin, R.; Worrillow, L.; et al. Molecular High-Grade B-Cell Lymphoma: Defining a Poor-Risk Group That Requires Different Approaches to Therapy. J. Clin. Oncol. 2019, 37, 202–212. [Google Scholar] [CrossRef]
- Subramanian, A.; Tamayo, P.; Mootha, V.K.; Mukherjee, S.; Ebert, B.L.; Gillette, M.A.; Paulovich, A.; Pomeroy, S.L.; Golub, T.R.; Lander, E.S.; et al. Gene set enrichment analysis: A knowledge-based approach for interpreting genome-wide expression profiles. Proc. Natl. Acad. Sci. USA 2005, 102, 15545–15550. [Google Scholar] [CrossRef]
- Mootha, V.K.; Lindgren, C.M.; Eriksson, K.F.; Subramanian, A.; Sihag, S.; Lehar, J.; Puigserver, P.; Carlsson, E.; Ridderstrale, M.; Laurila, E.; et al. PGC-1alpha-responsive genes involved in oxidative phosphorylation are coordinately downregulated in human diabetes. Nat. Genet. 2003, 34, 267–273. [Google Scholar] [CrossRef]
- Broad Institute, Inc. Massachusetts Institute of Technology; Regents of the University of California. Gene Set Enrichment Analysis. Available online: https://www.gsea-msigdb.org/gsea/index.jsp (accessed on 23 April 2024).
- Szklarczyk, D.; Kirsch, R.; Koutrouli, M.; Nastou, K.; Mehryary, F.; Hachilif, R.; Gable, A.L.; Fang, T.; Doncheva, N.T.; Pyysalo, S.; et al. The STRING database in 2023: Protein-protein association networks and functional enrichment analyses for any sequenced genome of interest. Nucleic Acids Res. 2023, 51, D638–D646. [Google Scholar] [CrossRef]
- SIB—Swiss Institute of BioInformatics; Novo Nordisk Foundation Center Protein Research; EMBL—European Molecular Biology Laboratory. STRING. Available online: https://string-db.org/ (accessed on 23 April 2024).
- Kim, J.Y.; Cho, Y.E.; Park, J.H. The Nucleolar Protein GLTSCR2 Is an Upstream Negative Regulator of the Oncogenic Nucleophosmin-MYC Axis. Am. J. Pathol. 2015, 185, 2061–2068. [Google Scholar] [CrossRef]
- Shi, Y.; Xu, X.; Zhang, Q.; Fu, G.; Mo, Z.; Wang, G.S.; Kishi, S.; Yang, X.L. tRNA synthetase counteracts c-Myc to develop functional vasculature. eLife 2014, 3, e02349. [Google Scholar] [CrossRef]
- Barrans, S.; Crouch, S.; Smith, A.; Turner, K.; Owen, R.; Patmore, R.; Roman, E.; Jack, A. Rearrangement of MYC is associated with poor prognosis in patients with diffuse large B-cell lymphoma treated in the era of rituximab. J. Clin. Oncol. 2010, 28, 3360–3365. [Google Scholar] [CrossRef]
- Kawasaki, C.; Ohshim, K.; Suzumiya, J.; Kanda, M.; Tsuchiya, T.; Tamura, K.; Kikuchi, M. Rearrangements of bcl-1, bcl-2, bcl-6, and c-myc in diffuse large B-cell lymphomas. Leuk. Lymphoma 2001, 42, 1099–1106. [Google Scholar] [CrossRef]
- Stasik, C.J.; Nitta, H.; Zhang, W.; Mosher, C.H.; Cook, J.R.; Tubbs, R.R.; Unger, J.M.; Brooks, T.A.; Persky, D.O.; Wilkinson, S.T.; et al. Increased MYC gene copy number correlates with increased mRNA levels in diffuse large B-cell lymphoma. Haematologica 2010, 95, 597–603. [Google Scholar] [CrossRef]
- Leveille, E.; Johnson, N.A. Genetic Events Inhibiting Apoptosis in Diffuse Large B Cell Lymphoma. Cancers 2021, 13, 2167. [Google Scholar] [CrossRef]
- Odqvist, L.; Montes-Moreno, S.; Sanchez-Pacheco, R.E.; Young, K.H.; Martin-Sanchez, E.; Cereceda, L.; Sanchez-Verde, L.; Pajares, R.; Mollejo, M.; Fresno, M.F.; et al. NFkappaB expression is a feature of both activated B-cell-like and germinal center B-cell-like subtypes of diffuse large B-cell lymphoma. Mod. Pathol. 2014, 27, 1331–1337. [Google Scholar] [CrossRef]
- Ok, C.Y.; Xu-Monette, Z.Y.; Li, L.; Manyam, G.C.; Montes-Moreno, S.; Tzankov, A.; Visco, C.; Dybkaer, K.; Routbort, M.J.; Zhang, L.; et al. Evaluation of NF-kappaB subunit expression and signaling pathway activation demonstrates that p52 expression confers better outcome in germinal center B-cell-like diffuse large B-cell lymphoma in association with CD30 and BCL2 functions. Mod. Pathol. 2015, 28, 1202–1213. [Google Scholar] [CrossRef]
- Yu, L.; Li, L.; Medeiros, L.J.; Young, K.H. NF-kappaB signaling pathway and its potential as a target for therapy in lymphoid neoplasms. Blood Rev. 2017, 31, 77–92. [Google Scholar] [CrossRef]
- Wu, J.; Yu, X.; Zhu, H.; Chen, P.; Liu, T.; Yin, R.; Qiang, Y.; Xu, L. RelB is a potential molecular biomarker for immunotherapy in human pan-cancer. Front. Mol. Biosci. 2023, 10, 1178446. [Google Scholar] [CrossRef]
- Modi, D.; Potugari, B.; Uberti, J. Immunotherapy for Diffuse Large B-Cell Lymphoma: Current Landscape and Future Directions. Cancers 2021, 13, 5827. [Google Scholar] [CrossRef]
- Zhang, J.; Medeiros, L.J.; Young, K.H. Cancer Immunotherapy in Diffuse Large B-Cell Lymphoma. Front. Oncol. 2018, 8, 351. [Google Scholar] [CrossRef]
- Gasparini, C.; Celeghini, C.; Monasta, L.; Zauli, G. NF-kappaB pathways in hematological malignancies. Cell. Mol. Life Sci. 2014, 71, 2083–2102. [Google Scholar] [CrossRef]
- Jayawant, E.; Pack, A.; Clark, H.; Kennedy, E.; Ghodke, A.; Jones, J.; Pepper, C.; Pepper, A.; Mitchell, S. NF-kappaB fingerprinting reveals heterogeneous NF-kappaB composition in diffuse large B-cell lymphoma. Front. Oncol. 2023, 13, 1181660. [Google Scholar] [CrossRef]
- Lim, S.K.; Peng, C.C.; Low, S.; Vijay, V.; Budiman, A.; Phang, B.H.; Lim, J.Q.; Jeyasekharan, A.D.; Lim, S.T.; Ong, C.K.; et al. Sustained activation of non-canonical NF-kappaB signalling drives glycolytic reprogramming in doxorubicin-resistant DLBCL. Leukemia 2023, 37, 441–452. [Google Scholar] [CrossRef]
- Oien, D.B.; Sharma, S.; Hattersley, M.M.; DuPont, M.; Criscione, S.W.; Prickett, L.; Goeppert, A.U.; Drew, L.; Yao, Y.; Zhang, J.; et al. BET inhibition targets ABC-DLBCL constitutive B-cell receptor signaling through PAX5. Blood Adv. 2023, 7, 5108–5121. [Google Scholar] [CrossRef]
- Carreras, J.; Ikoma, H.; Kikuti, Y.Y.; Miyaoka, M.; Hiraiwa, S.; Tomita, S.; Kondo, Y.; Ito, A.; Nagase, S.; Miura, H.; et al. Mutational, immune microenvironment, and clinicopathological profiles of diffuse large B-cell lymphoma and follicular lymphoma with BCL6 rearrangement. Virchows Arch. 2024, 484, 657–676. [Google Scholar] [CrossRef]

| Gene | Name | Function |
|---|---|---|
| DPM2 | Dolichyl-Phosphate Mannosyltransferase Subunit 2, Regulatory | Regulation of protein stability |
| TRAPPC1 | Trafficking Protein Particle Complex Subunit 1 | Endoplasmic reticulum-to-Golgi vesicle-mediated transport |
| HYAL2 | Hyaluronidase 2 | Positive regulation of the extrinsic apoptotic signaling pathway. Related to bladder cancer inflammation and tumor-associated myeloid cells [95] |
| TRIM35 | Tripartite Motif Containing 35 | Multiple biological processes, including cell death, glucose metabolism, and innate immune response. Correlation with high infiltration of NK cells in DLBCL [96], tumor suppressor in breast cancer [97], predicts survival in hepatocellular carcinoma, and is related to tumorigenesis |
| NUDT18 | Nudix Hydrolase 18 | Elimination of potentially toxic nucleotide metabolites |
| TMEM219 | Transmembrane Protein 219 | Apoptosis |
| CHCHD10 | Coiled-Coil-Helix-Coiled-Coil-Helix Domain Containing 10 | Positive regulation of mitochondrial outer membrane permeabilization involved in the apoptotic signaling pathway |
| IGFBP7 | Insulin-Like Growth Factor Binding Protein 7 | Prostacyclin production and cell adhesion. Related to Epstein–Barr virus tumorigenesis, mantle cell lymphoma, and lung cancer [56,98,99] |
| LAMTOR2 | Late Endosomal/Lysosomal Adaptor, MAPK, a nd MTOR Activator 2 | Activation of mTORC1, with control of cell growth and related to the risk of breast cancer [100] |
| ZNF688 | Zinc Finger Protein 688 | Negative regulation of transcription by RNA polymerase II |
| UBL7 | Ubiquitin Like 7 | Ubiquitin-dependent protein catabolic process, cellular response to stress. Autoantibody signature in hepatocellular carcinoma [101]; necroptosis-related marker in stomach adenocarcinoma [102] |
| RELB | RELB Proto-Oncogene, NF-KB Subunit | NF-kappa-B is a pleiotropic transcription factor involved in many biological processes, such as inflammation, immunity, differentiation, cell growth, tumorigenesis, and apoptosis. Pathogenic marker of DLBCL [103,104] |
| Model | No. of Genes | Overall Accuracy (%) |
|---|---|---|
| XGBoost Tree | 12 | 99.8 |
| Random Forest | 12 | 98.6 |
| Random Trees | 12 | 93.9 |
| C5 | 7 | 75.4 |
| KNN Algorithm | 12 | 73.4 |
| CHAID | 5 | 71.7 |
| Neural Network | 12 | 71.3 |
| Logistic regression | 12 | 71.0 |
| LSVM | 12 | 70.1 |
| SVM | 12 | 69.3 |
| Discriminant | 12 | 68.4 |
| C&R Tree | 12 | 68.4 |
| Tree-AS | 3 | 65.5 |
| Quest | 6 | 64.5 |
| XGBoost Linear | 12 | 60.2 |
| Bayesian Network | 12 | 0.0 |
| Gene | B | p Value | Hazard Risk | 95% CI for HR | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| TRAPPC1 | −0.391 | 0.023 | 0.676 | 0.483 | 0.946 |
| HYAL2 | 0.757 | 0.000 | 2.133 | 1.461 | 3.113 |
| IGFBP7 | −0.683 | 0.000 | 0.505 | 0.400 | 0.637 |
| UBL7 | 0.507 | 0.001 | 1.660 | 1.234 | 2.233 |
| RELB | −0.361 | 0.003 | 0.697 | 0.549 | 0.885 |
| No. | Symbol | Title | Running Enrichment Score (ES) | Core Enrichment |
|---|---|---|---|---|
| 1 | REL | REL proto-oncogene, NF-kB subunit | 0.0879 | Yes |
| 2 | LTB | Lymphotoxin beta | 0.1807 | Yes |
| 3 | RELB | RELB proto-oncogene, NF-kB subunit | 0.2316 | Yes |
| 4 | TRAF2 | TNF receptor-associated factor 2 | 0.2571 | Yes |
| 5 | NFKB2 | Nuclear factor kappa B subunit 2 | 0.2892 | Yes |
| 6 | CD40 | CD40 molecule | 0.3301 | Yes |
| 7 | MALT1 | MALT1 paracaspase | 0.3536 | Yes |
| 8 | NFKBID | NFKB inhibitor delta | 0.3914 | Yes |
| 9 | NFKBIA | NFKB inhibitor alpha | 0.3964 | Yes |
| 10 | RELA | RELA proto-oncogene, NF-kB subunit | 0.4062 | Yes |
| 11 | IKBKG | Inhibitor of nuclear factor kappa B kinase regulatory subunit | 0.4174 | Yes |
| 12 | BCL3 | BCL3 transcription coactivator | 0.4145 | Yes |
| 13 | TAB1 | TGF-beta activated kinase 1 (MAP3K7) binding protein 1 | 0.4192 | Yes |
| 14 | TANK | TRAF family member-associated NFKB activator | 0.4068 | No |
| 15 | NFKBIB | NFKB inhibitor beta | 0.3919 | No |
| 16 | EZH2 | Enhancer of zeste 2 polycomb repressive complex 2 subunit | 0.3875 | No |
| 17 | TNFRSF1A | TNF receptor superfamily member 1A | 0.3872 | No |
| 18 | NFKBIE | NFKB inhibitor epsilon | 0.3934 | No |
| 19 | IKBKB | Inhibitor of nuclear factor kappa B kinase subunit beta | 0.3868 | No |
| 20 | SKP1 | S-phase kinase-associated protein 1 | 0.3765 | No |
| 21 | CHUK | Component of inhibitor of nuclear factor kappa B kinase complex | 0.3782 | No |
| 22 | NFKB1 | Nuclear factor kappa B subunit 1 | 0.3747 | No |
| 23 | KPNA1 | Karyopherin subunit alpha 1 | 0.3685 | No |
| 24 | MAP3K14 | Mitogen-activated protein kinase kinase kinase 14 | 0.2468 | No |
| 25 | LTBR | Lymphotoxin beta receptor | 0.106 | No |
| 26 | NFKBIZ | NFKB inhibitor zeta | 0.082 | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carreras, J.; Hamoudi, R. Anomaly Detection and Artificial Intelligence Identified the Pathogenic Role of Apoptosis and RELB Proto-Oncogene, NF-kB Subunit in Diffuse Large B-Cell Lymphoma. BioMedInformatics 2024, 4, 1480-1505. https://doi.org/10.3390/biomedinformatics4020081
Carreras J, Hamoudi R. Anomaly Detection and Artificial Intelligence Identified the Pathogenic Role of Apoptosis and RELB Proto-Oncogene, NF-kB Subunit in Diffuse Large B-Cell Lymphoma. BioMedInformatics. 2024; 4(2):1480-1505. https://doi.org/10.3390/biomedinformatics4020081
Chicago/Turabian StyleCarreras, Joaquim, and Rifat Hamoudi. 2024. "Anomaly Detection and Artificial Intelligence Identified the Pathogenic Role of Apoptosis and RELB Proto-Oncogene, NF-kB Subunit in Diffuse Large B-Cell Lymphoma" BioMedInformatics 4, no. 2: 1480-1505. https://doi.org/10.3390/biomedinformatics4020081
APA StyleCarreras, J., & Hamoudi, R. (2024). Anomaly Detection and Artificial Intelligence Identified the Pathogenic Role of Apoptosis and RELB Proto-Oncogene, NF-kB Subunit in Diffuse Large B-Cell Lymphoma. BioMedInformatics, 4(2), 1480-1505. https://doi.org/10.3390/biomedinformatics4020081