

Artificial Intelligence Analysis and Reverse Engineering of Molecular Subtypes of Diffuse Large B-Cell Lymphoma Using Gene Expression Data

 ,
,  , ,
, ,  and
and
Abstract

1. Introduction
1.1. Introduction to Artificial Intelligence Analysis
1.2. Machine Learnig
1.3. Types of Data Modeling in Predictive Analytics
1.3.1. Supervised Analyses
1.3.2. Association Analyses
1.3.3. Segmentation Analyses
1.3.4. Additional Analyses
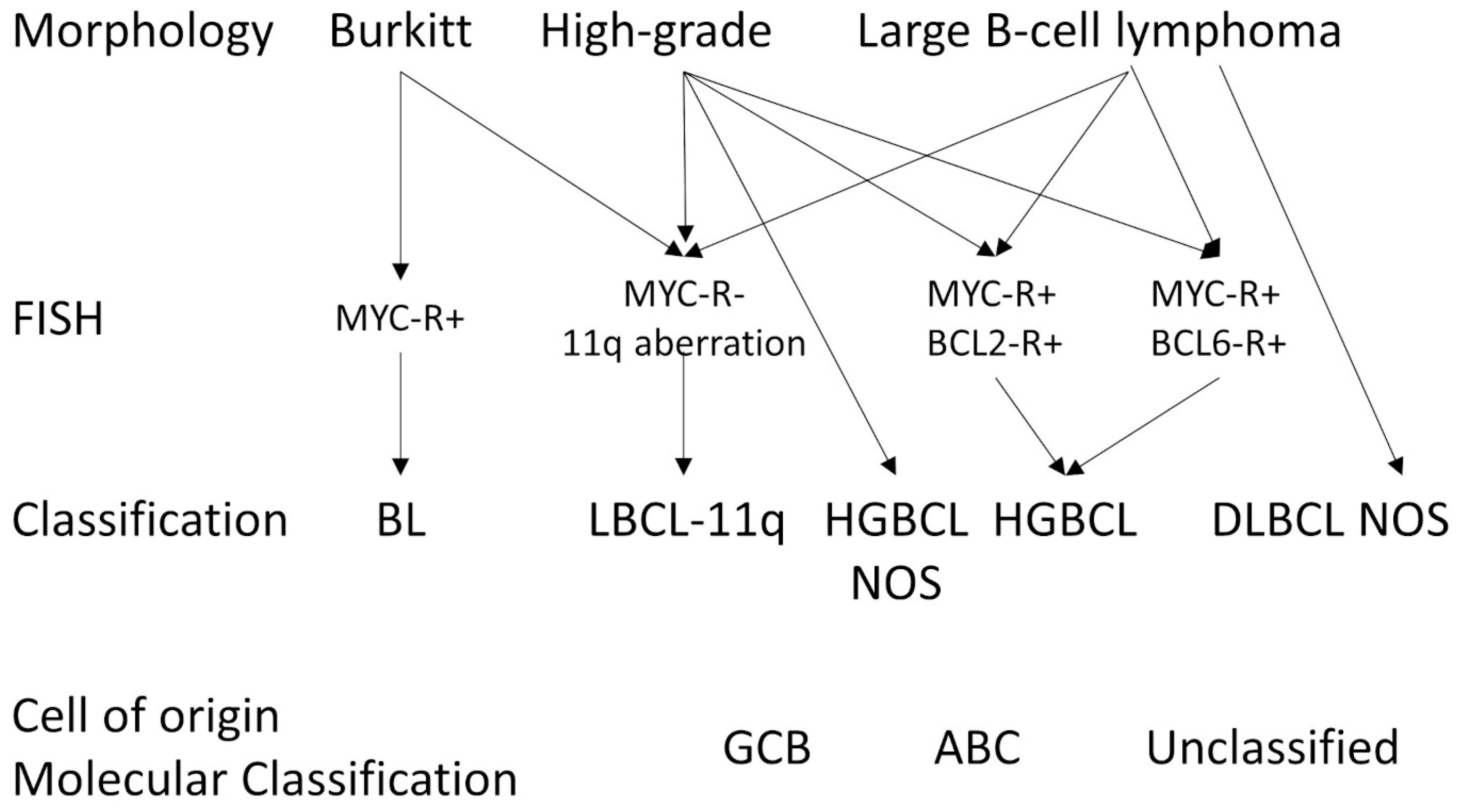
1.4. Diffuse Large B-Cell Lymphoma
- ➀
- Schmitz R. et al. identified four DLBCL subtypes: MCD (characterized by MYD88L265P and CD79B mutations), BN2 (BCL6 fusions and NOTCH2 mutations), N1 (NOTCH1 mutations), and EZB (EZH2 mutations and BCL2 translocations) [114].
- ➁
- Chapuy B. et al. identified five subtypes: a low-risk ABC-DLBCL subtype of extrafollicular/marginal zone origin; two different subtypes of GCB-DLBCLs characterized with different patients’ survival and targetable alterations; and an ABC/GCB-independent subtype with an inactivation of TP53, CDKN2A loss, and genomic instability [115].
- ➂
- Lacy S.E. et al. found six molecular subtypes: MYD88, BCL2, SOCS1/SGK1, TET2/SGK1, NOTCH2, and Unclassified [116].
- ➃
- Reddy A. et al. created a prognostic model with better performance than the conventional methods of the International Prognostic Index (IPI), cell of origin, and rearrangements of MYC and BCL2 [117].
- ➄
- Sha C. et al. defined Molecular high-grade B-cell lymphoma (MHG) using a gene expression-based machine learning classifier [118]. This MHG was applied to a clinical trial that tested the addition of bortezomib (proteasome inhibitor) to the conventional RCHOP therapy. This study found that the MHG group was biologically similar to the high-grade B-cell lymphoma of the Germinal center cell-of-origin subtype (proliferative and centroblasts), and partially with cases of MYC rearrangement [118].
- ➅
- This MHG gene expression profile was defined by genes of Burkitt lymphoma (BL), and conferred a bad prognosis of DLBCL [119]. The classifier was downloaded on github (https://github.com/Sharlene/BDC, accessed on 16 January 2024) and run on R statistical software [119]. Of note, the gene set tested in the classifier comprised 28 genes [119,120].
1.5. Aim of this Study
2. Materials and Methods
2.1. Materials
2.2. Methods
3. Results
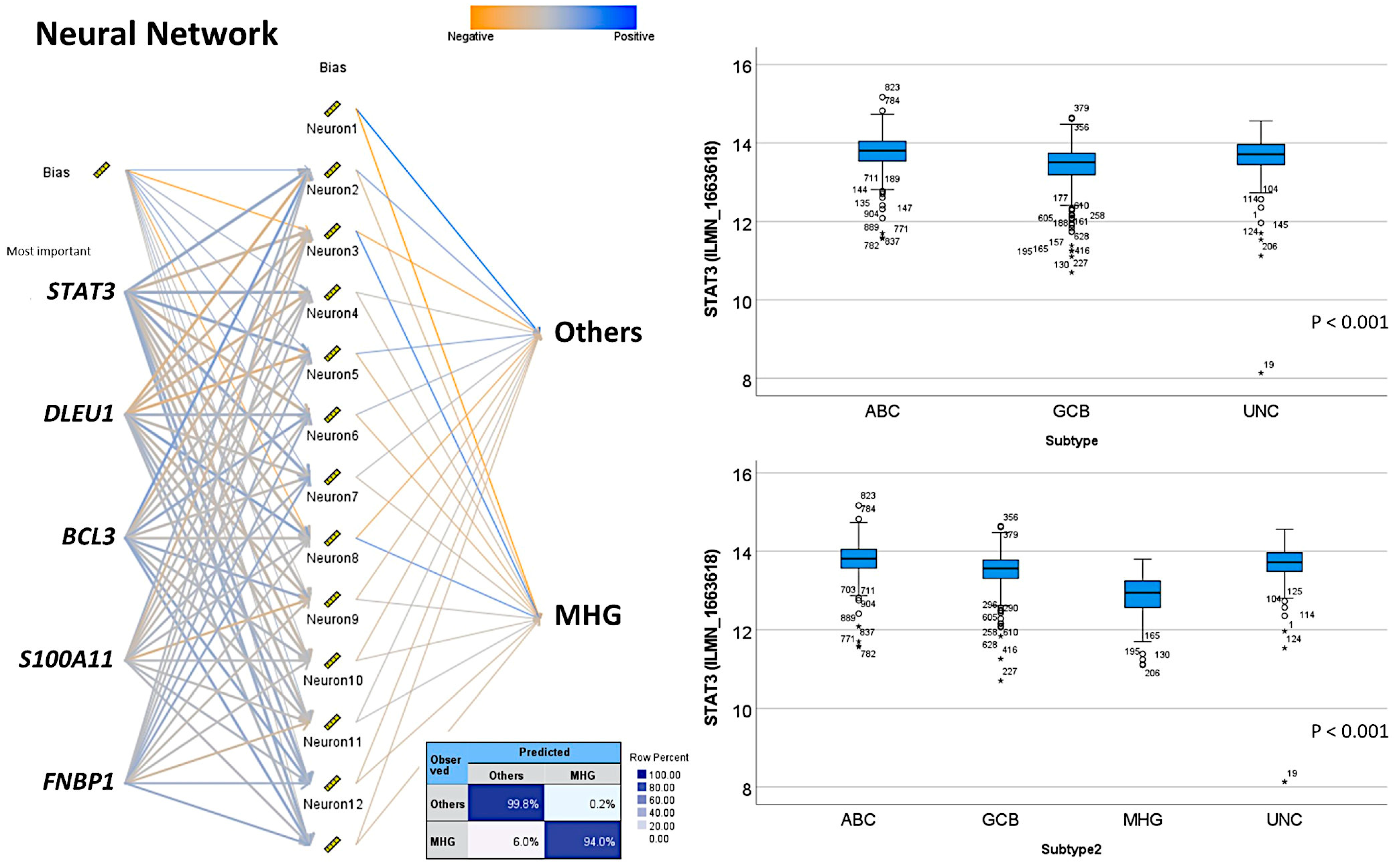
3.1. Prediction of DLBCL Subtypes Using Neural Networks
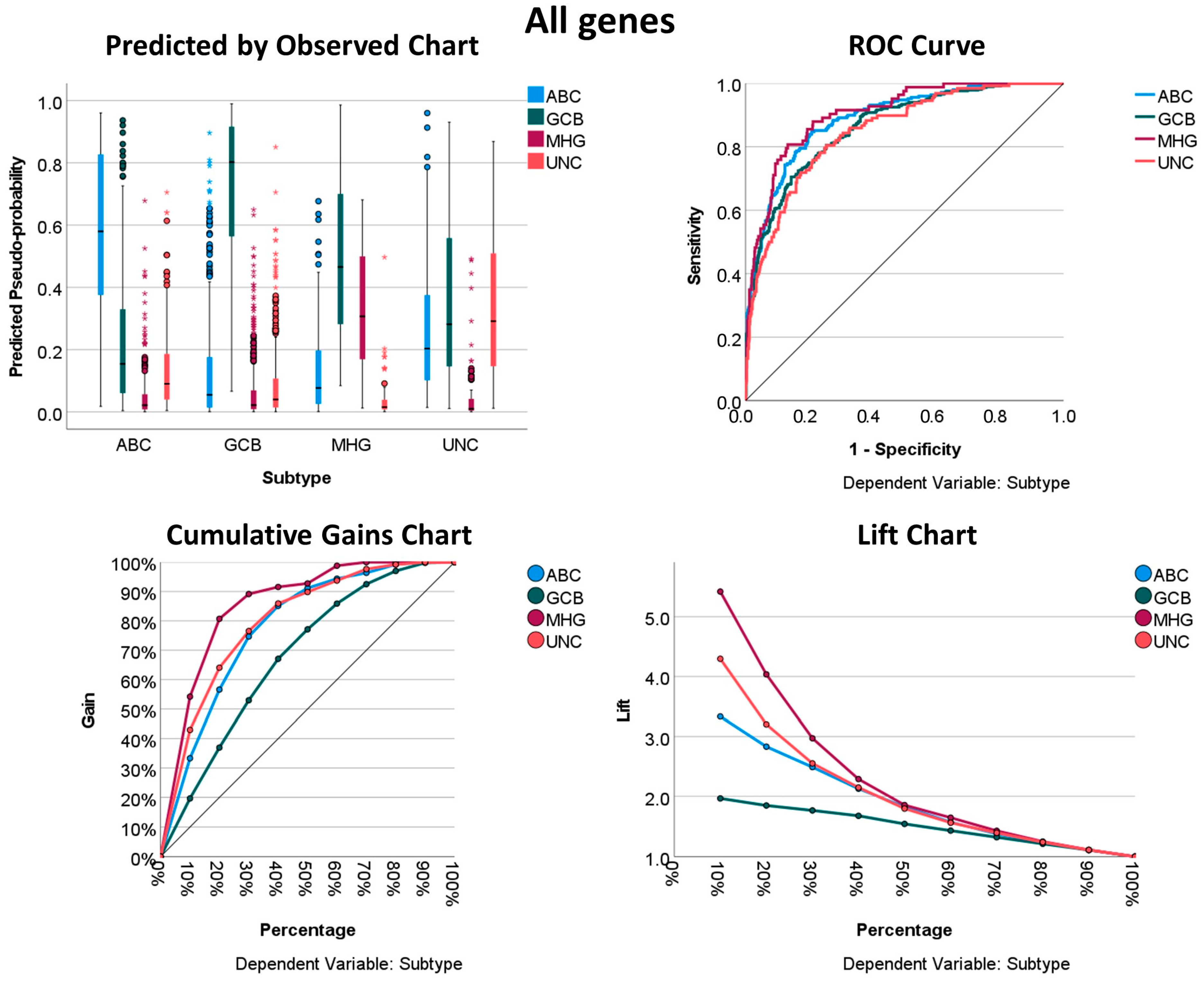
3.1.1. Prediction Using All Genes of the Array
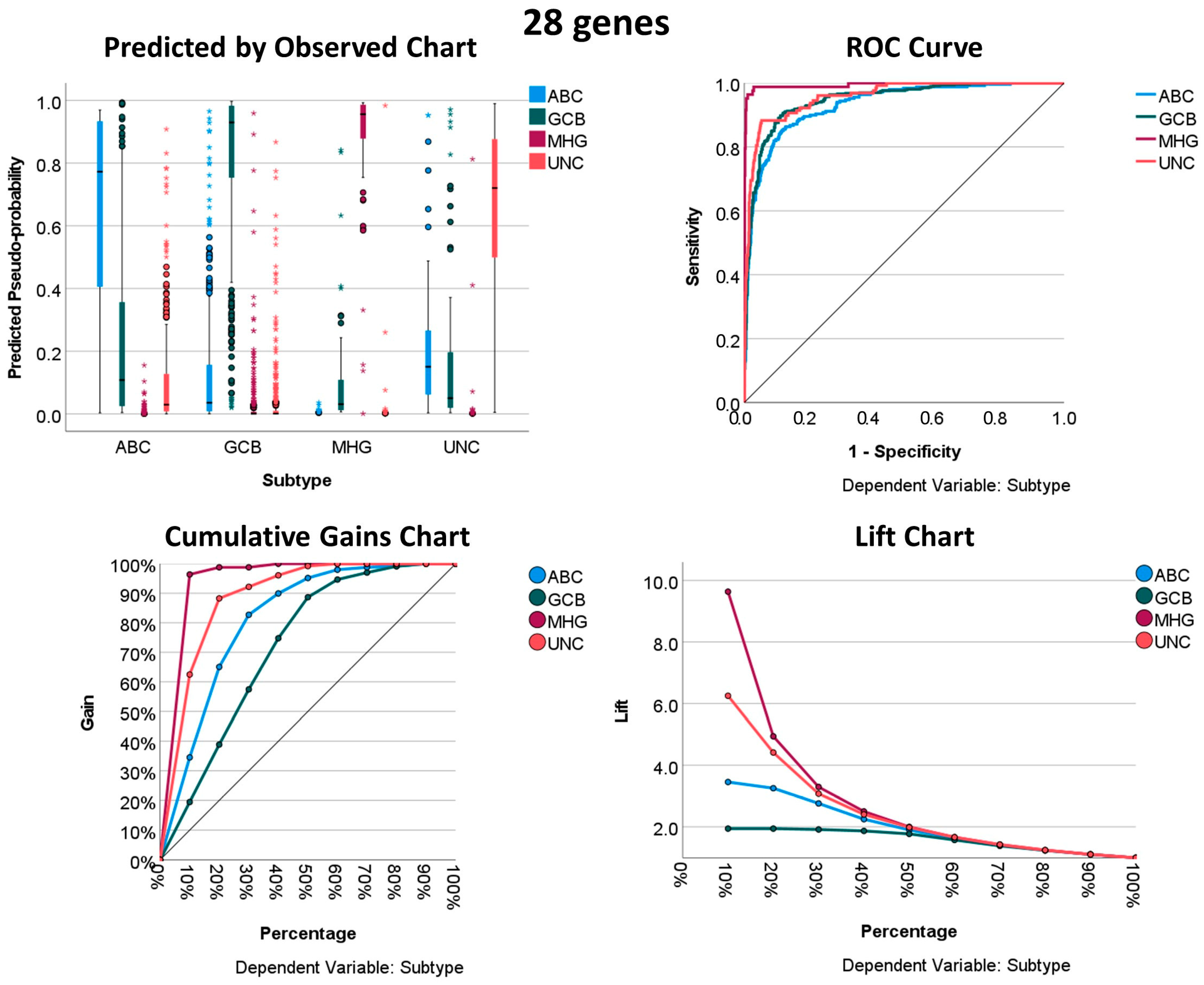
3.1.2. Prediction Using the 28 Genes
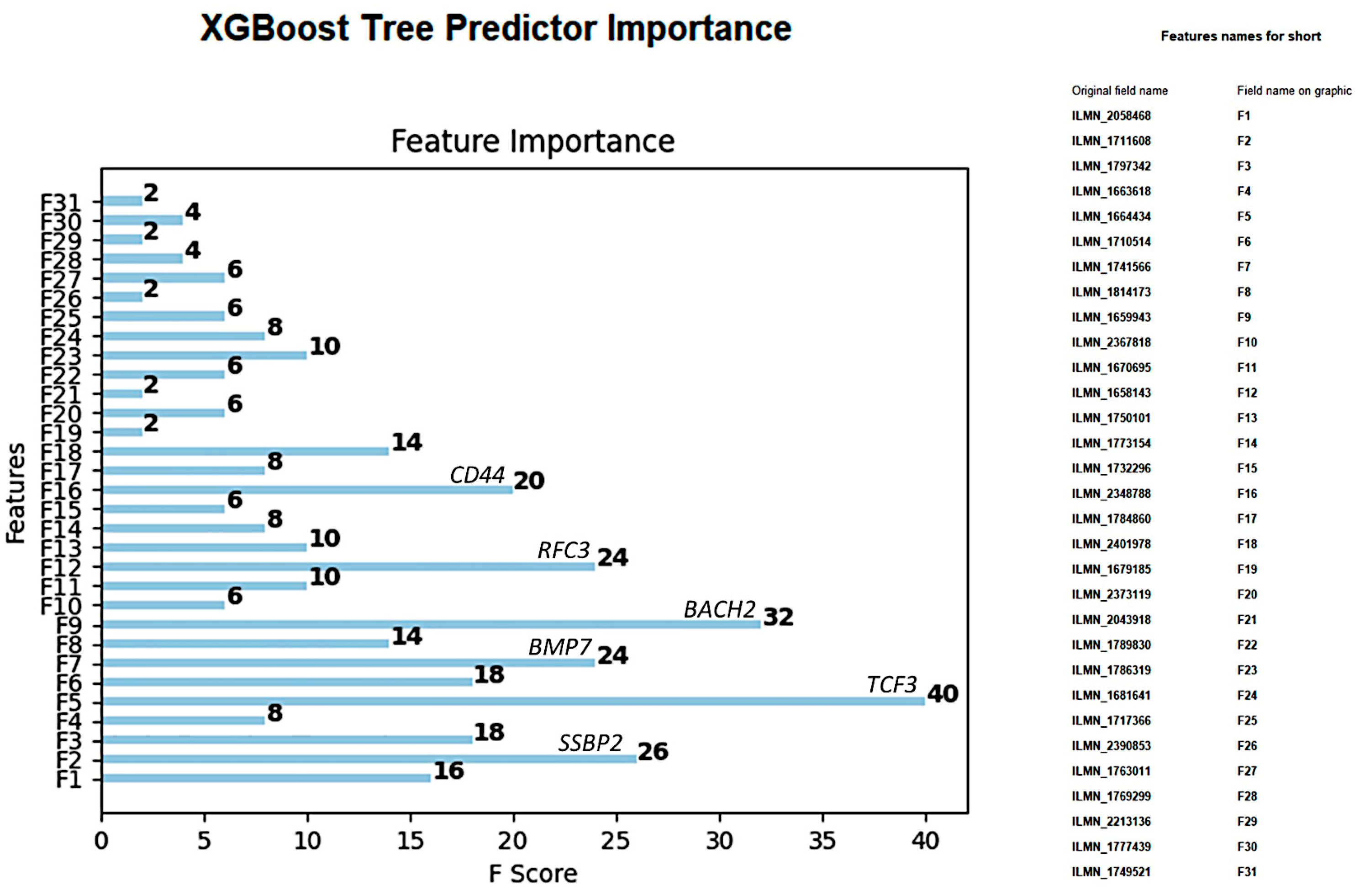
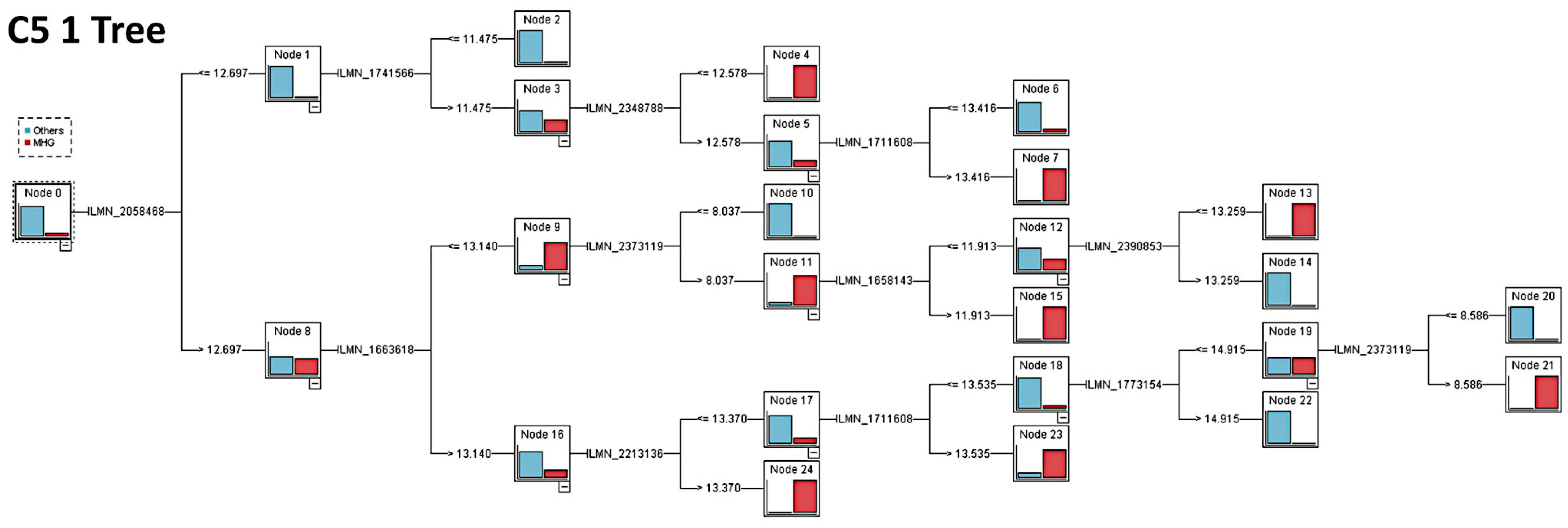
3.2. Prediction of DLBCL Subtypes Based on the 28 Genes Using Other Machine Learning Techniques
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


Appendix B. Logistic Regression
References
- Turing, A.M. Computer machinery and intelligence. Mind 1950, 49, 433–460. [Google Scholar] [CrossRef]
- McCarthy, J. John McCarthy’s Home Page. Available online: http://www-formal.stanford.edu/jmc/ (accessed on 20 November 2023).
- Anwar, S.M.; Majid, M.; Qayyum, A.; Awais, M.; Alnowami, M.; Khan, M.K. Medical Image Analysis using Convolutional Neural Networks: A Review. J. Med. Syst. 2018, 42, 226. [Google Scholar] [CrossRef]
- Mao, S.; Sejdic, E. A Review of Recurrent Neural Network-Based Methods in Computational Physiology. IEEE Trans. Neural Netw. Learn. Syst. 2023, 34, 6983–7003. [Google Scholar] [CrossRef]
- Montazeri, M.; Montazeri, M.; Montazeri, M.; Beigzadeh, A. Machine learning models in breast cancer survival prediction. Technol. Health Care 2016, 24, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Rezayi, S.; Niakan Kalhori, S.R.; Saeedi, S. Effectiveness of Artificial Intelligence for Personalized Medicine in Neoplasms: A Systematic Review. BioMed Res. Int. 2022, 2022, 7842566. [Google Scholar] [CrossRef] [PubMed]
- Deist, T.M.; Dankers, F.; Valdes, G.; Wijsman, R.; Hsu, I.C.; Oberije, C.; Lustberg, T.; van Soest, J.; Hoebers, F.; Jochems, A.; et al. Machine learning algorithms for outcome prediction in (chemo)radiotherapy: An empirical comparison of classifiers. Med. Phys. 2018, 45, 3449–3459. [Google Scholar] [CrossRef] [PubMed]
- Poirion, O.B.; Jing, Z.; Chaudhary, K.; Huang, S.; Garmire, L.X. DeepProg: An ensemble of deep-learning and machine-learning models for prognosis prediction using multi-omics data. Genome Med. 2021, 13, 112. [Google Scholar] [CrossRef] [PubMed]
- Lynch, C.M.; Abdollahi, B.; Fuqua, J.D.; de Carlo, A.R.; Bartholomai, J.A.; Balgemann, R.N.; van Berkel, V.H.; Frieboes, H.B. Prediction of lung cancer patient survival via supervised machine learning classification techniques. Int. J. Med. Inform. 2017, 108, 1–8. [Google Scholar] [CrossRef]
- Sultan, A.S.; Elgharib, M.A.; Tavares, T.; Jessri, M.; Basile, J.R. The use of artificial intelligence, machine learning and deep learning in oncologic histopathology. J. Oral Pathol. Med. 2020, 49, 849–856. [Google Scholar] [CrossRef]
- Sidey-Gibbons, J.A.M.; Sidey-Gibbons, C.J. Machine learning in medicine: A practical introduction. BMC Med. Res. Methodol. 2019, 19, 64. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Vincent Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Hudson, I.L. Data Integration Using Advances in Machine Learning in Drug Discovery and Molecular Biology. Methods Mol. Biol. 2021, 2190, 167–184. [Google Scholar] [CrossRef] [PubMed]
- Sugahara, S.; Aomi, I.; Ueno, M. Bayesian Network Model Averaging Classifiers by Subbagging. Entropy 2022, 24, 743. [Google Scholar] [CrossRef] [PubMed]
- “User Guide”. Kernel Density Estimation (KDE). Web. © 2007–2018, Scikit-Learn Developers. Available online: http://scikit-learn.org/stable/modules/density.html#kernel-density-estimation (accessed on 20 November 2023).
- Carreras, J. Artificial Intelligence Analysis of Ulcerative Colitis Using an Autoimmune Discovery Transcriptomic Panel. Healthcare 2022, 10, 1476. [Google Scholar] [CrossRef]
- Carreras, J.; Roncador, G.; Hamoudi, R. Artificial Intelligence Predicted Overall Survival and Classified Mature B-Cell Neoplasms Based on Immuno-Oncology and Immune Checkpoint Panels. Cancers 2022, 14, 5318. [Google Scholar] [CrossRef]
- Asadi, F.; Salehnasab, C.; Ajori, L. Supervised Algorithms of Machine Learning for the Prediction of Cervical Cancer. J. Biomed. Phys. Eng. 2020, 10, 513–522. [Google Scholar] [CrossRef]
- Jiang, T.; Gradus, J.L.; Rosellini, A.J. Supervised Machine Learning: A Brief Primer. Behav. Ther. 2020, 51, 675–687. [Google Scholar] [CrossRef]
- Pruneski, J.A.; Pareek, A.; Kunze, K.N.; Martin, R.K.; Karlsson, J.; Oeding, J.F.; Kiapour, A.M.; Nwachukwu, B.U.; Williams, R.J., 3rd. Supervised machine learning and associated algorithms: Applications in orthopedic surgery. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 1196–1202. [Google Scholar] [CrossRef]
- Uddin, S.; Khan, A.; Hossain, M.E.; Moni, M.A. Comparing different supervised machine learning algorithms for disease prediction. BMC Med. Inform. Decis. Mak. 2019, 19, 281. [Google Scholar] [CrossRef]
- Kobayashi, D.; Takahashi, O.; Arioka, H.; Koga, S.; Fukui, T. A prediction rule for the development of delirium among patients in medical wards: Chi-Square Automatic Interaction Detector (CHAID) decision tree analysis model. Am. J. Geriatr. Psychiatry 2013, 21, 957–962. [Google Scholar] [CrossRef]
- Lee, V.J.; Lye, D.C.; Sun, Y.; Leo, Y.S. Decision tree algorithm in deciding hospitalization for adult patients with dengue haemorrhagic fever in Singapore. Trop. Med. Int. Health 2009, 14, 1154–1159. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.Y.; Lu, Y. Decision tree methods: Applications for classification and prediction. Shanghai Arch. Psychiatry 2015, 27, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Algorithms Guide. IBM SPSS Modeler 18.4. IBM® SPSS® Modeler Is the IBM Corp. Orchard Rd, Armonk, NY 10504, United States. © Copyright IBM Corporation 1994, 2022. Available online: http://www.ibm.com/support (accessed on 16 January 2024).
- Chylinska, J.; Lazarewicz, M.; Rzadkiewicz, M.; Adamus, M.; Jaworski, M.; Haugan, G.; Lillefjel, M.; Espnes, G.A.; Wlodarczyk, D. The role of gender in the active attitude toward treatment and health among older patients in primary health care-self-assessed health status and sociodemographic factors as moderators. BMC Geriatr. 2017, 17, 284. [Google Scholar] [CrossRef] [PubMed]
- Fokkema, M.; Smits, N.; Zeileis, A.; Hothorn, T.; Kelderman, H. Detecting treatment-subgroup interactions in clustered data with generalized linear mixed-effects model trees. Behav. Res. Methods 2018, 50, 2016–2034. [Google Scholar] [CrossRef] [PubMed]
- Fokkema, M.; Edbrooke-Childs, J.; Wolpert, M. Generalized linear mixed-model (GLMM) trees: A flexible decision-tree method for multilevel and longitudinal data. Psychother. Res. 2021, 31, 313–325. [Google Scholar] [CrossRef]
- Chen, H.C.; Wehrly, T.E. Assessing correlation of clustered mixed outcomes from a multivariate generalized linear mixed model. Stat. Med. 2015, 34, 704–720. [Google Scholar] [CrossRef]
- Parry, R.M.; Jones, W.; Stokes, T.H.; Phan, J.H.; Moffitt, R.A.; Fang, H.; Shi, L.; Oberthuer, A.; Fischer, M.; Tong, W.; et al. k-Nearest neighbor models for microarray gene expression analysis and clinical outcome prediction. Pharmacogenom. J. 2010, 10, 292–309. [Google Scholar] [CrossRef]
- Rajaguru, H.; Sannasi Chakravarthy, S.R. Analysis of Decision Tree and K-Nearest Neighbor Algorithm in the Classification of Breast Cancer. Asian Pac. J. Cancer Prev. 2019, 20, 3777–3781. [Google Scholar] [CrossRef]
- Marston, Z.P.D.; Cira, T.M.; Knight, J.F.; Mulla, D.; Alves, T.M.; Hodgson, E.W.; Ribeiro, A.V.; MacRae, I.V.; Koch, R.L. Linear Support Vector Machine Classification of Plant Stress From Soybean Aphid (Hemiptera: Aphididae) Using Hyperspectral Reflectance. J. Econ. Entomol. 2022, 115, 1557–1563. [Google Scholar] [CrossRef]
- Razaque, A.; Ben Haj Frej, M.; Almi’ani, M.; Alotaibi, M.; Alotaibi, B. Improved Support Vector Machine Enabled Radial Basis Function and Linear Variants for Remote Sensing Image Classification. Sensors 2021, 21, 4431. [Google Scholar] [CrossRef]
- Zhang, H.; Luo, Y.B.; Wu, W.; Zhang, L.; Wang, Z.; Dai, Z.; Feng, S.; Cao, H.; Cheng, Q.; Liu, Z. The molecular feature of macrophages in tumor immune microenvironment of glioma patients. Comput. Struct. Biotechnol. J. 2021, 19, 4603–4618. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, M.C.; Song, L. Neural network analysis of lymphoma microarray data: Prognosis and diagnosis near-perfect. BMC Bioinform. 2003, 4, 13. [Google Scholar] [CrossRef]
- Xia, W.; Hu, B.; Li, H.; Shi, W.; Tang, Y.; Yu, Y.; Geng, C.; Wu, Q.; Yang, L.; Yu, Z.; et al. Deep Learning for Automatic Differential Diagnosis of Primary Central Nervous System Lymphoma and Glioblastoma: Multi-Parametric Magnetic Resonance Imaging Based Convolutional Neural Network Model. J. Magn. Reson. Imaging 2021, 54, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Chen, Z. Evaluation of Short-Term Efficacy of PD-1 Monoclonal Antibody Immunotherapy for Lymphoma by Positron Emission Tomography/Computed Tomography Imaging with Convolutional Neural Network Image Registration Algorithm. Contrast Media Mol. Imaging 2022, 2022, 1388517. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Zhao, H.; Zhong, T.; Dong, X.; Wang, L.; Han, P.; Li, Z. Adaptive deep propagation graph neural network for predicting miRNA-disease associations. Brief. Funct. Genom. 2023, 22, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Shen, T.; Wang, H.; Hu, R.; Lv, Y. Developing neural network diagnostic models and potential drugs based on novel identified immune-related biomarkers for celiac disease. Hum. Genom. 2023, 17, 76. [Google Scholar] [CrossRef] [PubMed]
- Carreras, J. Artificial Intelligence Analysis of Celiac Disease Using an Autoimmune Discovery Transcriptomic Panel Highlighted Pathogenic Genes including BTLA. Healthcare 2022, 10, 1550. [Google Scholar] [CrossRef] [PubMed]
- Carreras, J.; Nakamura, N.; Hamoudi, R. Artificial Intelligence Analysis of Gene Expression Predicted the Overall Survival of Mantle Cell Lymphoma and a Large Pan-Cancer Series. Healthcare 2022, 10, 155. [Google Scholar] [CrossRef]
- Carreras, J.; Hiraiwa, S.; Kikuti, Y.Y.; Miyaoka, M.; Tomita, S.; Ikoma, H.; Ito, A.; Kondo, Y.; Roncador, G.; Garcia, J.F.; et al. Artificial Neural Networks Predicted the Overall Survival and Molecular Subtypes of Diffuse Large B-Cell Lymphoma Using a Pancancer Immune-Oncology Panel. Cancers 2021, 13, 6384. [Google Scholar] [CrossRef]
- Cutler, D.R.; Edwards, T.C., Jr.; Beard, K.H.; Cutler, A.; Hess, K.T.; Gibson, J.; Lawler, J.J. Random forests for classification in ecology. Ecology 2007, 88, 2783–2792. [Google Scholar] [CrossRef]
- Lawson, A.; Rotejanaprasert, C. Bayesian Spatio-Temporal Prediction and Counterfactual Generation: An Application in Non-Pharmaceutical Interventions in COVID-19. Viruses 2023, 15, 325. [Google Scholar] [CrossRef] [PubMed]
- Amato, F.; Guignard, F.; Robert, S.; Kanevski, M. A novel framework for spatio-temporal prediction of environmental data using deep learning. Sci. Rep. 2020, 10, 22243. [Google Scholar] [CrossRef] [PubMed]
- Sphinx 6.6.6. Imbalanced-Learn Documentation. Available online: https://imbalanced-learn.org/stable/ (accessed on 20 November 2023).
- Huang, S.; Cai, N.; Pacheco, P.P.; Narrandes, S.; Wang, Y.; Xu, W. Applications of Support Vector Machine (SVM) Learning in Cancer Genomics. Cancer Genom. Proteom. 2018, 15, 41–51. [Google Scholar] [CrossRef]
- Noble, W.S. What is a support vector machine? Nat. Biotechnol. 2006, 24, 1565–1567. [Google Scholar] [CrossRef] [PubMed]
- Moosaei, H.; Ganaie, M.A.; Hladik, M.; Tanveer, M. Inverse free reduced universum twin support vector machine for imbalanced data classification. Neural Netw. 2023, 157, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Elshewey, A.M.; Shams, M.Y.; El-Rashidy, N.; Elhady, A.M.; Shohieb, S.M.; Tarek, Z. Bayesian Optimization with Support Vector Machine Model for Parkinson Disease Classification. Sensors 2023, 23, 2085. [Google Scholar] [CrossRef] [PubMed]
- Riva, A.; Bellazzi, R. Learning temporal probabilistic causal models from longitudinal data. Artif. Intell. Med. 1996, 8, 217–234. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Zhao, B.; Chen, T.; Hao, B.; Yang, T.; Xu, H. Multimorbidity in the elderly in China based on the China Health and Retirement Longitudinal Study. PLoS ONE 2021, 16, e0255908. [Google Scholar] [CrossRef]
- Li, Q.; Zhang, Y.; Kang, H.; Xin, Y.; Shi, C. Mining association rules between stroke risk factors based on the Apriori algorithm. Technol. Health Care 2017, 25, 197–205. [Google Scholar] [CrossRef]
- Martinez, A.; Cuesta, M.J.; Peralta, V. Dependence Graphs Based on Association Rules to Explore Delusional Experiences. Multivar. Behav. Res. 2022, 57, 458–477. [Google Scholar] [CrossRef]
- Manolitsis, I.; Feretzakis, G.; Tzelves, L.; Kalles, D.; Loupelis, E.; Katsimperis, S.; Kosmidis, T.; Anastasiou, A.; Koutsouris, D.; Kofopoulou, S.; et al. Using Association Rules in Antimicrobial Resistance in Stone Disease Patients. Stud. Health Technol. Inform. 2022, 295, 462–465. [Google Scholar] [CrossRef] [PubMed]
- Hu, L. Research on English Achievement Analysis Based on Improved CARMA Algorithm. Comput. Intell. Neurosci. 2022, 2022, 8687879. [Google Scholar] [CrossRef] [PubMed]
- Luo, G.; Xie, W.; Gao, R.; Zheng, T.; Chen, L.; Sun, H. Unsupervised anomaly detection in brain MRI: Learning abstract distribution from massive healthy brains. Comput. Biol. Med. 2023, 154, 106610. [Google Scholar] [CrossRef] [PubMed]
- Duong, H.T.; Le, V.T.; Hoang, V.T. Deep Learning-Based Anomaly Detection in Video Surveillance: A Survey. Sensors 2023, 23, 5024. [Google Scholar] [CrossRef] [PubMed]
- Tritscher, J.; Krause, A.; Hotho, A. Feature relevance XAI in anomaly detection: Reviewing approaches and challenges. Front. Artif. Intell. 2023, 6, 1099521. [Google Scholar] [CrossRef]
- Deng, H.; Li, X. Self-supervised Anomaly Detection with Random-shape Pseudo-outliers. In Proceedings of the 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, UK, 11–15 July 2022. [Google Scholar] [CrossRef]
- Demidenko, E. The next-generation K-means algorithm. Stat. Anal. Data Min. 2018, 11, 153–166. [Google Scholar] [CrossRef] [PubMed]
- McLachlan, G.J.; Bean, R.W.; Ng, S.K. Clustering. Methods Mol. Biol. 2017, 1526, 345–362. [Google Scholar] [CrossRef] [PubMed]
- Krishna, K.; Narasimha Murty, M. Genetic K-means algorithm. IEEE Trans. Syst. Man. Cybern. B Cybern. 1999, 29, 433–439. [Google Scholar] [CrossRef]
- Timmerman, M.E.; Ceulemans, E.; De Roover, K.; Van Leeuwen, K. Subspace K-means clustering. Behav. Res. Methods 2013, 45, 1011–1023. [Google Scholar] [CrossRef]
- Andras, P. Kernel-Kohonen networks. Int. J. Neural Syst. 2002, 12, 117–135. [Google Scholar] [CrossRef]
- Fort, J.C. SOM’s mathematics. Neural Netw. 2006, 19, 812–816. [Google Scholar] [CrossRef] [PubMed]
- Biehl, M.; Hammer, B.; Villmann, T. Prototype-based models in machine learning. Wiley Interdiscip. Rev. Cogn. Sci. 2016, 7, 92–111. [Google Scholar] [CrossRef] [PubMed]
- Miranda, E.; Sune, J. Memristors for Neuromorphic Circuits and Artificial Intelligence Applications. Materials 2020, 13, 938. [Google Scholar] [CrossRef] [PubMed]
- Baskin, I.I. Machine Learning Methods in Computational Toxicology. Methods Mol. Biol. 2018, 1800, 119–139. [Google Scholar] [CrossRef] [PubMed]
- Mahon, C.; Howard, E.; O’Reilly, A.; Dooley, B.; Fitzgerald, A. A cluster analysis of health behaviours and their relationship to mental health difficulties, life satisfaction and functioning in adolescents. Prev. Med. 2022, 164, 107332. [Google Scholar] [CrossRef] [PubMed]
- Kent, P.; Jensen, R.K.; Kongsted, A. A comparison of three clustering methods for finding subgroups in MRI, SMS or clinical data: SPSS TwoStep Cluster analysis, Latent Gold and SNOB. BMC Med. Res. Methodol. 2014, 14, 113. [Google Scholar] [CrossRef] [PubMed]
- Klontzas, M.E.; Volitakis, E.; Aydingoz, U.; Chlapoutakis, K.; Karantanas, A.H. Machine learning identifies factors related to early joint space narrowing in dysplastic and non-dysplastic hips. Eur. Radiol. 2022, 32, 542–550. [Google Scholar] [CrossRef]
- Mirshahi, R.; Naseripour, M.; Shojaei, A.; Heirani, M.; Alemzadeh, S.A.; Moodi, F.; Anvari, P.; Falavarjani, K.G. Differentiating a pachychoroid and healthy choroid using an unsupervised machine learning approach. Sci. Rep. 2022, 12, 16323. [Google Scholar] [CrossRef]
- “User Guide” Gaussian Mixture Modeling Algorithms. Available online: http://scikit-learn.org/stable/modules/mixture.html (accessed on 20 November 2023).
- Xu, J.; Xu, J.; Meng, Y.; Lu, C.; Cai, L.; Zeng, X.; Nussinov, R.; Cheng, F. Graph embedding and Gaussian mixture variational autoencoder network for end-to-end analysis of single-cell RNA sequencing data. Cell Rep. Methods 2023, 3, 100382. [Google Scholar] [CrossRef]
- McCaw, Z.R.; Aschard, H.; Julienne, H. Fitting Gaussian mixture models on incomplete data. BMC Bioinform. 2022, 23, 208. [Google Scholar] [CrossRef]
- Kasa, S.R.; Bhattacharya, S.; Rajan, V. Gaussian mixture copulas for high-dimensional clustering and dependency-based subtyping. Bioinformatics 2020, 36, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Melvin, R.L.; Xiao, J.; Godwin, R.C.; Berenhaut, K.S.; Salsbury, F.R., Jr. Visualizing correlated motion with HDBSCAN clustering. Protein Sci. 2018, 27, 62–75. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.Y.; Yu, C.; Husman, T.; Chen, B.; Trikala, A. Novel strategy for applying hierarchical density-based spatial clustering of applications with noise towards spectroscopic analysis and detection of melanocytic lesions. Melanoma Res. 2021, 31, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Malzer, C.; Baum, M. Constraint-Based Hierarchical Cluster Selection in Automotive Radar Data. Sensors 2021, 21, 3410. [Google Scholar] [CrossRef] [PubMed]
- Chel, S.; Gare, S.; Giri, L. Detection of Specific Templates in Calcium Spiking in HeLa Cells Using Hierarchical DBSCAN: Clustering and Visualization of CellDrug Interaction at Multiple Doses. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020. [Google Scholar] [CrossRef]
- Isotonic Regression. Regression—RDD-Based API. Apache Spark. MLlib: Main Guide. Available online: https://spark.apache.org/docs/2.2.0/mllib-isotonic-regression.html (accessed on 20 November 2023).
- Li, W.; Fu, H. Bayesian isotonic regression dose-response model. J. Biopharm. Stat. 2017, 27, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Park, S.Y.; Lee, S.Y.; Song, J.Y.; Lee, G.Y.; Park, J.H.; Joe, H.B. Determination of the 95% effective dose of remimazolam to achieve loss of consciousness during anesthesia induction in different age groups. Korean J. Anesthesiol. 2022, 75, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Fortmann-Roe, S.; Starfield, R.; Getz, W.M. Contingent kernel density estimation. PLoS ONE 2012, 7, e30549. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, M.R.; Jung, H.; Larocque, D. Functional Kernel Density Estimation: Point and Fourier Approaches to Time Series Anomaly Detection. Entropy 2020, 22, 1363. [Google Scholar] [CrossRef]
- Yee, J.; Park, T.; Park, M. Identification of the associations between genes and quantitative traits using entropy-based kernel density estimation. Genom. Inform. 2022, 20, e17. [Google Scholar] [CrossRef]
- Pardo, A.; Real, E.; Krishnaswamy, V.; Lopez-Higuera, J.M.; Pogue, B.W.; Conde, O.M. Directional Kernel Density Estimation for Classification of Breast Tissue Spectra. IEEE Trans. Med. Imaging 2017, 36, 64–73. [Google Scholar] [CrossRef]
- Smola, A.J.; Schölkopf, B. A Tutorial on Support Vector Regression. Stat. Comput. Arch. 2004, 14, 199–222. [Google Scholar] [CrossRef]
- Liu, X.; Ouellette, S.; Jamgochian, M.; Liu, Y.; Rao, B. One-class machine learning classification of skin tissue based on manually scanned optical coherence tomography imaging. Sci. Rep. 2023, 13, 867. [Google Scholar] [CrossRef] [PubMed]
- Retico, A.; Gori, I.; Giuliano, A.; Muratori, F.; Calderoni, S. One-Class Support Vector Machines Identify the Language and Default Mode Regions As Common Patterns of Structural Alterations in Young Children with Autism Spectrum Disorders. Front. Neurosci. 2016, 10, 306. [Google Scholar] [CrossRef] [PubMed]
- Teufl, W.; Taetz, B.; Miezal, M.; Dindorf, C.; Frohlich, M.; Trinler, U.; Hogan, A.; Bleser, G. Automated detection and explainability of pathological gait patterns using a one-class support vector machine trained on inertial measurement unit based gait data. Clin. Biomech. 2021, 89, 105452. [Google Scholar] [CrossRef] [PubMed]
- Scikit Learn. Random Forests and Other Randomized Tree Ensembles. Available online: https://scikit-learn.org/stable/modules/ensemble.html#forest (accessed on 20 November 2023).
- Rigatti, S.J. Random Forest. J. Insur. Med. 2017, 47, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Wu, H.; Jin, X.; Zheng, P.; Hu, S.; Xu, X.; Yu, W.; Yan, J. Study of cardiovascular disease prediction model based on random forest in eastern China. Sci. Rep. 2020, 10, 5245. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Yang, J.; Lan, M.; Zou, T. Construction and analysis of a joint diagnosis model of random forest and artificial neural network for heart failure. Aging (Albany NY) 2020, 12, 26221–26235. [Google Scholar] [CrossRef]
- Wang, F.; Wang, Y.; Ji, X.; Wang, Z. Effective Macrosomia Prediction Using Random Forest Algorithm. Int. J. Environ. Res. Public Health 2022, 19, 3245. [Google Scholar] [CrossRef]
- Carreras, J.; Hamoudi, R. Artificial Neural Network Analysis of Gene Expression Data Predicted Non-Hodgkin Lymphoma Subtypes with High Accuracy. Mach. Learn. Knowl. Extr. 2021, 3, 720–739. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.Y.; Roncador, G.; Miyaoka, M.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; Shiraiwa, S.; et al. High Expression of Caspase-8 Associated with Improved Survival in Diffuse Large B-Cell Lymphoma: Machine Learning and Artificial Neural Networks Analyses. BioMedInformatics 2021, 1, 18–46. [Google Scholar] [CrossRef]
- XGBoost Tutorials. Available online: https://xgboost.readthedocs.io/en/stable/index.html (accessed on 20 November 2023).
- XGBoost Tutorials. Scalable and Flexible Gradient Boosting. Web. © 2015–2016 DMLC. Available online: http://xgboost.readthedocs.io/en/latest/tutorials/index.html (accessed on 20 November 2023).
- Ringner, M. What is principal component analysis? Nat. Biotechnol. 2008, 26, 303–304. [Google Scholar] [CrossRef]
- Giuliani, A. The application of principal component analysis to drug discovery and biomedical data. Drug Discov. Today 2017, 22, 1069–1076. [Google Scholar] [CrossRef]
- Campo, E.; Jaffe, E.S.; Cook, J.R.; Quintanilla-Martinez, L.; Swerdlow, S.H.; Anderson, K.C.; Brousset, P.; Cerroni, L.; de Leval, L.; Dirnhofer, S.; et al. The International Consensus Classification of Mature Lymphoid Neoplasms: A report from the Clinical Advisory Committee. Blood 2022, 140, 1229–1253. [Google Scholar] [CrossRef]
- de Leval, L.; Alizadeh, A.A.; Bergsagel, P.L.; Campo, E.; Davies, A.; Dogan, A.; Fitzgibbon, J.; Horwitz, S.M.; Melnick, A.M.; Morice, W.G.; et al. Genomic profiling for clinical decision making in lymphoid neoplasms. Blood 2022, 140, 2193–2227. [Google Scholar] [CrossRef]
- King, R.L.; Hsi, E.D.; Chan, W.C.; Piris, M.A.; Cook, J.R.; Scott, D.W.; Swerdlow, S.H. Diagnostic approaches and future directions in Burkitt lymphoma and high-grade B-cell lymphoma. Virchows Arch. 2023, 482, 193–205. [Google Scholar] [CrossRef]
- Arber, D.A.; Campo, E.; Jaffe, E.S. Advances in the Classification of Myeloid and Lymphoid Neoplasms. Virchows Arch. 2023, 482, 1–9. [Google Scholar] [CrossRef]
- Cazzola, M.; Sehn, L.H. Developing a classification of hematologic neoplasms in the era of precision medicine. Blood 2022, 140, 1193–1199. [Google Scholar] [CrossRef]
- Alaggio, R.; Amador, C.; Anagnostopoulos, I.; Attygalle, A.D.; Araujo, I.B.O.; Berti, E.; Bhagat, G.; Borges, A.M.; Boyer, D.; Calaminici, M.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia 2022, 36, 1720–1748. [Google Scholar] [CrossRef]
- Grimm, K.E.; O’Malley, D.P. Aggressive B cell lymphomas in the 2017 revised WHO classification of tumors of hematopoietic and lymphoid tissues. Ann. Diagn. Pathol. 2019, 38, 6–10. [Google Scholar] [CrossRef]
- Ott, G. Aggressive B-cell lymphomas in the update of the 4th edition of the World Health Organization classification of haematopoietic and lymphatic tissues: Refinements of the classification, new entities and genetic findings. Br. J. Haematol. 2017, 178, 871–887. [Google Scholar] [CrossRef] [PubMed]
- Falini, B.; Martino, G.; Lazzi, S. A comparison of the International Consensus and 5th World Health Organization classifications of mature B-cell lymphomas. Leukemia 2023, 37, 18–34. [Google Scholar] [CrossRef]
- Brown, J.R.; Freedman, A.S.; Aste, J.C. Pathobiology of Diffuse Large B Cell Lymphoma and Primary Mediastinal Large B Cell Lymphoma. UpToDate. 2022. Available online: https://medilib.ir/uptodate/show/4722 (accessed on 20 November 2023).
- Schmitz, R.; Wright, G.W.; Huang, D.W.; Johnson, C.A.; Phelan, J.D.; Wang, J.Q.; Roulland, S.; Kasbekar, M.; Young, R.M.; Shaffer, A.L.; et al. Genetics and Pathogenesis of Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2018, 378, 1396–1407. [Google Scholar] [CrossRef]
- Chapuy, B.; Stewart, C.; Dunford, A.J.; Kim, J.; Kamburov, A.; Redd, R.A.; Lawrence, M.S.; Roemer, M.G.M.; Li, A.J.; Ziepert, M.; et al. Molecular subtypes of diffuse large B cell lymphoma are associated with distinct pathogenic mechanisms and outcomes. Nat. Med. 2018, 24, 679–690. [Google Scholar] [CrossRef]
- Lacy, S.E.; Barrans, S.L.; Beer, P.A.; Painter, D.; Smith, A.G.; Roman, E.; Cooke, S.L.; Ruiz, C.; Glover, P.; Van Hoppe, S.J.L.; et al. Targeted sequencing in DLBCL, molecular subtypes, and outcomes: A Haematological Malignancy Research Network report. Blood 2020, 135, 1759–1771. [Google Scholar] [CrossRef]
- Reddy, A.; Zhang, J.; Davis, N.S.; Moffitt, A.B.; Love, C.L.; Waldrop, A.; Leppa, S.; Pasanen, A.; Meriranta, L.; Karjalainen-Lindsberg, M.L.; et al. Genetic and Functional Drivers of Diffuse Large B Cell Lymphoma. Cell 2017, 171, 481–494.e15. [Google Scholar] [CrossRef]
- Sha, C.; Barrans, S.; Cucco, F.; Bentley, M.A.; Care, M.A.; Cummin, T.; Kennedy, H.; Thompson, J.S.; Uddin, R.; Worrillow, L.; et al. Molecular High-Grade B-Cell Lymphoma: Defining a Poor-Risk Group That Requires Different Approaches to Therapy. J. Clin. Oncol. 2019, 37, 202–212. [Google Scholar] [CrossRef]
- Sha, C.; Barrans, S.; Care, M.A.; Cunningham, D.; Tooze, R.M.; Jack, A.; Westhead, D.R. Transferring genomics to the clinic: Distinguishing Burkitt and diffuse large B cell lymphomas. Genome Med. 2015, 7, 64. [Google Scholar] [CrossRef]
- Supplemetary Data. Gene Sets Tested in Different Classifiers. Transferring Genomics to the Clinic: Distinguishing Burkitt and Diffuse Large B Cell Lymphomas. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4512160/bin/13073_2015_187_MOESM4_ESM.pdf (accessed on 20 November 2023).
- Carey, C.D.; Gusenleitner, D.; Chapuy, B.; Kovach, A.E.; Kluk, M.J.; Sun, H.H.; Crossland, R.E.; Bacon, C.M.; Rand, V.; Dal Cin, P.; et al. Molecular classification of MYC-driven B-cell lymphomas by targeted gene expression profiling of fixed biopsy specimens. J. Mol. Diagn. 2015, 17, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Dave, S.S.; Fu, K.; Wright, G.W.; Lam, L.T.; Kluin, P.; Boerma, E.J.; Greiner, T.C.; Weisenburger, D.D.; Rosenwald, A.; Ott, G.; et al. Molecular diagnosis of Burkitt’s lymphoma. N. Engl. J. Med. 2006, 354, 2431–2442. [Google Scholar] [CrossRef] [PubMed]
- Deffenbacher, K.E.; Iqbal, J.; Sanger, W.; Shen, Y.; Lachel, C.; Liu, Z.; Liu, Y.; Lim, M.S.; Perkins, S.L.; Fu, K.; et al. Molecular distinctions between pediatric and adult mature B-cell non-Hodgkin lymphomas identified through genomic profiling. Blood 2012, 119, 3757–3766. [Google Scholar] [CrossRef] [PubMed]
- Harris, N.L.; Horning, S.J. Burkitt’s lymphoma—The message from microarrays. N. Engl. J. Med. 2006, 354, 2495–2498. [Google Scholar] [CrossRef] [PubMed]
- Hecht, J.L.; Aster, J.C. Molecular biology of Burkitt’s lymphoma. J. Clin. Oncol. 2000, 18, 3707–3721. [Google Scholar] [CrossRef] [PubMed]
- Hummel, M.; Bentink, S.; Berger, H.; Klapper, W.; Wessendorf, S.; Barth, T.F.; Bernd, H.W.; Cogliatti, S.B.; Dierlamm, J.; Feller, A.C.; et al. A biologic definition of Burkitt’s lymphoma from transcriptional and genomic profiling. N. Engl. J. Med. 2006, 354, 2419–2430. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, J.; Shen, Y.; Huang, X.; Liu, Y.; Wake, L.; Liu, C.; Deffenbacher, K.; Lachel, C.M.; Wang, C.; Rohr, J.; et al. Global microRNA expression profiling uncovers molecular markers for classification and prognosis in aggressive B-cell lymphoma. Blood 2015, 125, 1137–1145. [Google Scholar] [CrossRef]
- Leich, E.; Hartmann, E.M.; Burek, C.; Ott, G.; Rosenwald, A. Diagnostic and prognostic significance of gene expression profiling in lymphomas. APMIS 2007, 115, 1135–1146. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.T. Genomic diagnosis of Burkitt’s lymphoma. N. Engl. J. Med. 2006, 355, 1064. [Google Scholar] [CrossRef] [PubMed]
- Snuderl, M.; Kolman, O.K.; Chen, Y.B.; Hsu, J.J.; Ackerman, A.M.; Dal Cin, P.; Ferry, J.A.; Harris, N.L.; Hasserjian, R.P.; Zukerberg, L.R.; et al. B-cell lymphomas with concurrent IGH-BCL2 and MYC rearrangements are aggressive neoplasms with clinical and pathologic features distinct from Burkitt lymphoma and diffuse large B-cell lymphoma. Am. J. Surg. Pathol. 2010, 34, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Staiger, A.M.; Ziepert, M.; Horn, H.; Scott, D.W.; Barth, T.F.E.; Bernd, H.W.; Feller, A.C.; Klapper, W.; Szczepanowski, M.; Hummel, M.; et al. Clinical Impact of the Cell-of-Origin Classification and the MYC/ BCL2 Dual Expresser Status in Diffuse Large B-Cell Lymphoma Treated Within Prospective Clinical Trials of the German High-Grade Non-Hodgkin’s Lymphoma Study Group. J. Clin. Oncol. 2017, 35, 2515–2526. [Google Scholar] [CrossRef]
- Staudt, L.M.; Dave, S. The biology of human lymphoid malignancies revealed by gene expression profiling. Adv. Immunol. 2005, 87, 163–208. [Google Scholar] [CrossRef]
- Thomas, D.A.; O’Brien, S.; Faderl, S.; Manning, J.T., Jr.; Romaguera, J.; Fayad, L.; Hagemeister, F.; Medeiros, J.; Cortes, J.; Kantarjian, H. Burkitt lymphoma and atypical Burkitt or Burkitt-like lymphoma: Should these be treated as different diseases? Curr. Hematol. Malig. Rep. 2011, 6, 58–66. [Google Scholar] [CrossRef]
- Thomas, N.; Dreval, K.; Gerhard, D.S.; Hilton, L.K.; Abramson, J.S.; Ambinder, R.F.; Barta, S.; Bartlett, N.L.; Bethony, J.; Bhatia, K.; et al. Genetic subgroups inform on pathobiology in adult and pediatric Burkitt lymphoma. Blood 2023, 141, 904–916. [Google Scholar] [CrossRef] [PubMed]
- Carreras, J.; Kikuti, Y.Y.; Miyaoka, M.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; Hamoudi, R.; Nakamura, N. The Use of the Random Number Generator and Artificial Intelligence Analysis for Dimensionality Reduction of Follicular Lymphoma Transcriptomic Data. BioMedInformatics 2022, 2, 268–280. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.Y.; Miyaoka, M.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; Nakamura, N.; Hamoudi, R. A Combination of Multilayer Perceptron, Radial Basis Function Artificial Neural Networks and Machine Learning Image Segmentation for the Dimension Reduction and the Prognosis Assessment of Diffuse Large B-Cell Lymphoma. AI 2021, 2, 106–134. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.Y.; Miyaoka, M.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; Nakamura, N.; Hamoudi, R. Artificial Intelligence Analysis of the Gene Expression of Follicular Lymphoma Predicted the Overall Survival and Correlated with the Immune Microenvironment Response Signatures. Mach. Learn. Knowl. Extr. 2020, 2, 647–671. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.Y.; Miyaoka, M.; Roncador, G.; Garcia, J.F.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; et al. Integrative Statistics, Machine Learning and Artificial Intelligence Neural Network Analysis Correlated CSF1R with the Prognosis of Diffuse Large B-Cell Lymphoma. Hemato 2021, 2, 182–206. [Google Scholar] [CrossRef]
- Davies, A.; Cummin, T.E.; Barrans, S.; Maishman, T.; Mamot, C.; Novak, U.; Caddy, J.; Stanton, L.; Kazmi-Stokes, S.; McMillan, A.; et al. Gene-expression profiling of bortezomib added to standard chemoimmunotherapy for diffuse large B-cell lymphoma (REMoDL-B): An open-label, randomised, phase 3 trial. Lancet Oncol. 2019, 20, 649–662. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.J.; Barrans, S.; Stanton, L.; Caddy, J.; Wilding, S.; Saunders, G.; Mamot, C.; Novak, U.; McMillan, A.; Fields, P.; et al. Differential Efficacy From the Addition of Bortezomib to R-CHOP in Diffuse Large B-Cell Lymphoma According to the Molecular Subgroup in the REMoDL-B Study With a 5-Year Follow-Up. J. Clin. Oncol. 2023, 41, 2718–2723. [Google Scholar] [CrossRef]
- Mosquera Orgueira, A.; Diaz Arias, J.A.; Serrano Martin, R.; Portela Pineiro, V.; Cid Lopez, M.; Peleteiro Raindo, A.; Bao Perez, L.; Gonzalez Perez, M.S.; Perez Encinas, M.M.; Fraga Rodriguez, M.F.; et al. A prognostic model based on gene expression parameters predicts a better response to bortezomib-containing immunochemotherapy in diffuse large B-cell lymphoma. Front. Oncol. 2023, 13, 1157646. [Google Scholar] [CrossRef]
- Carreras, J.; Hamoudi, R.; Nakamura, N. Artificial Intelligence Analysis of Gene Expression Data Predicted the Prognosis of Patients with Diffuse Large B-Cell Lymphoma. Tokai J. Exp. Clin. Med. 2020, 45, 37–48. [Google Scholar]
- Carreras, J.; Kikuti, Y.Y.; Hiraiwa, S.; Miyaoka, M.; Tomita, S.; Ikoma, H.; Ito, A.; Kondo, Y.; Itoh, J.; Roncador, G.; et al. High PTX3 expression is associated with a poor prognosis in diffuse large B-cell lymphoma. Cancer Sci. 2022, 113, 334–348. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.Y.; Bea, S.; Miyaoka, M.; Hiraiwa, S.; Ikoma, H.; Nagao, R.; Tomita, S.; Martin-Garcia, D.; Salaverria, I.; et al. Clinicopathological characteristics and genomic profile of primary sinonasal tract diffuse large B cell lymphoma (DLBCL) reveals gain at 1q31 and RGS1 encoding protein; high RGS1 immunohistochemical expression associates with poor overall survival in DLBCL not otherwise specified (NOS). Histopathology 2017, 70, 595–621. [Google Scholar] [CrossRef] [PubMed]
- Miyaoka, M.; Kikuti, Y.Y.; Carreras, J.; Itou, A.; Ikoma, H.; Tomita, S.; Shiraiwa, S.; Ando, K.; Nakamura, N. AID is a poor prognostic marker of high-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements. Pathol. Int. 2022, 72, 35–42. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bayesian Network | C&R Tree | C5.0 | CHAID |
| Cox | Discriminant | GenLin | GLMM |
| KNN | Linear Regression | Logistic | LSVM |
| Neural Networks | QUEST | Random Trees | SLRM |
| STP | SVM | TCM | Tree-AS |
| Apriori | Association Rules | CARMA | Sequence |
| Anomaly | K-Means | Kohonen | TwoStep |
| Gaussian Mixture | GLE | HDBSCAN | Isotonic Regression |
| KDE Modeling | One-Class SVM | Random Forest | Time series |
| XGBoost Linear | XGBoost Tree | PCA/FA |
| ABC | GCB | MHG | UNC | |
|---|---|---|---|---|
| ABC | 249/255 (97.6%) | 0/255 (0%) | 6/255 (2.4%) | 0/255 (0%) |
| GCB | 0/543 (0%) | 468/543 (86.2%) | 75/543 (13.8%) | 0/543 (0%) |
| UNC | 0/130 (0%) | 0/130 (0%) | 2/130 (1.5%) | 128/130 (98.5%) |
| Age, mean ± STD | 62 ± 12.4 |
| Age > 60 | 573/905 (63.3%) |
| Male sex | 517/928 (55.7%) |
| Ann Arbor stage III-IV | 638/928 (68.8%) |
| ECOG performance status ≥ 2 | 105/928 (11.3%) |
| Serum LDH level > 230 U/L | 604/928 (65.1%) |
| International Prognostic Index (IPI) | |
| 0–1 Low | 246/928 (26.5%) |
| 2 Low-intermediate | 236/928 (25.4%) |
| 3 High-intermediate | 281/928 (30.3%) |
| 4–5 High | 165/928 (17.8%) |
| Treatment | |
| R-CHOP | 469/928 (50.5%) |
| RB-CHOP | 459/928 (49.5%) |
| Clinical response | 446/928 (48.1%) |
| Hit rearrangement * | |
| Double-hit | 35/928 (3.8%) |
| MYC-normal | 309/928 (33.3%) |
| MYC-rearranged NOS | 2/928 (0.2%) |
| n/a | 568/928 (61.2%) |
| Single-hit | 14/928 (1.5%) |
| Parameters | All Genes | 28 Genes |
|---|---|---|
| Case processing | ||
| Training | 642 (69.2%) | 667 (71.9%) |
| Testing | 286 (30.8%) | 261 (28.1%) |
| Valid | 928 (100%) | 928 (100%) |
| Input layer | ||
| No. units | 29372 | 33 |
| Rescaling method covariates | Standardized | Standardized |
| Hidden layer | ||
| No. | 1 | 1 |
| No. units | 12 | 6 |
| Activation function | Hyperbolic tangent | Hyperbolic tangent |
| Output layer | ||
| No. of dependent variables | 1 | 1 |
| No. units | 4 | 4 |
| Activation function | Softmax | Softmax |
| Error function | Cross-entropy | Cross-entropy |
| Model summary | ||
| Training | ||
| Cross-entropy error | 442.169 | 234.386 |
| Incorrect predictions % | 27.6% | 12.0% |
| Stopping rule | 1 | 1 |
| Training time | 6:49.55 | 0:00.35 |
| Testing | ||
| Cross-entropy error | 250.727 | 167.121 |
| Incorrect predictions | 35.0% | 23.8% |
| Classification | ||
| Training | ||
| ABC | 73.7% | 74.3% |
| GCB | 84.2% | 93.5% |
| MHG | 42.9% | 100% |
| UNC | 43.9% | 86.4% |
| Overall | 72.4% | 88.0% |
| Testing | ||
| ABC | 65.4% | 68.6% |
| GCB | 86.2% | 80.3% |
| MHG | 25.9% | 83.3% |
| UNC | 20.9% | 72.5% |
| Overall | 65.0% | 76.2% |
| Area Under the Curve | ||
| ABC | 0.888 | 0.932 |
| GCB | 0.862 | 0.947 |
| MHG | 0.904 | 0.994 |
| UNC | 0.850 | 0.958 |
| Predicted | ||||||
|---|---|---|---|---|---|---|
| Sample | Observed | ABC | GCB | MHG | UNC | % Correct |
| Training | ABC | 126 | 32 | 4 | 9 | 73.7% |
| GCB | 35 | 278 | 6 | 11 | 84.2% | |
| MHG | 8 | 23 | 24 | 1 | 42.9% | |
| UNC | 17 | 28 | 3 | 37 | 43.5% | |
| Overall% | 29.0% | 56.2% | 5.8% | 9.0% | 72.4% | |
| Testing | ABC | 51 | 24 | 1 | 2 | 65.4% |
| GCB | 12 | 119 | 2 | 5 | 86.2% | |
| MHG | 1 | 19 | 7 | 0 | 25.9% | |
| UNC | 13 | 20 | 1 | 9 | 20.9% | |
| Overall% | 26.9% | 63.6% | 3.8% | 5.6% | 65.0% |
| Predicted | ||||||
|---|---|---|---|---|---|---|
| Sample | Observed | ABC | GCB | MHG | UNC | % Correct |
| Training | ABC | 133 | 30 | 0 | 16 | 74.3% |
| GCB | 16 | 319 | 1 | 5 | 93.5% | |
| MHG | 0 | 0 | 59 | 0 | 100.0% | |
| UNC | 7 | 5 | 0 | 76 | 86.4% | |
| Overall% | 23.4% | 53.1% | 9.0% | 14.5% | 88.0% | |
| Testing | ABC | 48 | 14 | 0 | 8 | 68.6% |
| GCB | 15 | 102 | 4 | 6 | 80.3% | |
| MHG | 0 | 3 | 20 | 1 | 83.3% | |
| UNC | 2 | 8 | 1 | 29 | 72.5% | |
| Overall% | 24.9% | 48.7% | 9.6% | 16.9% | 76.2% |
| Prediction of 4 DLBCL Subtypes | MHG vs. Others | |||
|---|---|---|---|---|
| Model | No. of Genes | Overall Accuracy | No. of Genes | Overall Accuracy |
| XGBoost tree | 33 | 99.56% | 33 | 100.00% |
| Random forest | 33 | 98.92% | 33 | 99.46% |
| Random trees | 33 | 94.18% | 33 | 99.88% |
| C5 | 28 | 88.04% | 10 | 98.28% |
| Bayesian network | 33 | 86.42% | 33 | 99.14% |
| SVM | 33 | 83.62% | 33 | 99.35% |
| Logistic regression | 33 | 80.93% | 33 | 99.03% |
| KNN algorithm | 33 | 80.93% | 33 | 98.06% |
| Neural network | 33 | 79.74% | 33 | 99.25% |
| LSVM | 33 | 79.63% | 33 | 98.28% |
| Discriminant analysis | 33 | 75.43% | 33 | 95.69% |
| CHAID | 19 | 74.25% | 9 | 95.91% |
| C&R tree | 26 | 70.37% | 11 | 94.94% |
| Tree-AS | 6 | 61.53% | 6 | 93.43% |
| Quest | 17 | 58.51% | 24 | 94.50% |
| XGBoost linear | 33 | 50.43% | 33 | 91.06% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carreras, J.; Yukie Kikuti, Y.; Miyaoka, M.; Miyahara, S.; Roncador, G.; Hamoudi, R.; Nakamura, N. Artificial Intelligence Analysis and Reverse Engineering of Molecular Subtypes of Diffuse Large B-Cell Lymphoma Using Gene Expression Data. BioMedInformatics 2024, 4, 295-320. https://doi.org/10.3390/biomedinformatics4010017
Carreras J, Yukie Kikuti Y, Miyaoka M, Miyahara S, Roncador G, Hamoudi R, Nakamura N. Artificial Intelligence Analysis and Reverse Engineering of Molecular Subtypes of Diffuse Large B-Cell Lymphoma Using Gene Expression Data. BioMedInformatics. 2024; 4(1):295-320. https://doi.org/10.3390/biomedinformatics4010017
Chicago/Turabian StyleCarreras, Joaquim, Yara Yukie Kikuti, Masashi Miyaoka, Saya Miyahara, Giovanna Roncador, Rifat Hamoudi, and Naoya Nakamura. 2024. "Artificial Intelligence Analysis and Reverse Engineering of Molecular Subtypes of Diffuse Large B-Cell Lymphoma Using Gene Expression Data" BioMedInformatics 4, no. 1: 295-320. https://doi.org/10.3390/biomedinformatics4010017
APA StyleCarreras, J., Yukie Kikuti, Y., Miyaoka, M., Miyahara, S., Roncador, G., Hamoudi, R., & Nakamura, N. (2024). Artificial Intelligence Analysis and Reverse Engineering of Molecular Subtypes of Diffuse Large B-Cell Lymphoma Using Gene Expression Data. BioMedInformatics, 4(1), 295-320. https://doi.org/10.3390/biomedinformatics4010017