

Blood Pressure Estimation from Photoplythmography Using Hybrid Scattering–LSTM Networks

 , ,
, ,
Abstract
1. Introduction
2. Related Works
2.1. Challenges and Motivations
2.2. Contributions
- Scenario 1: Corresponding complete the ABP beat. Here, ABP beats are estimated from the corresponding PPG beats.
- Scenario 2: Just systolic, and diastolic BP values. In this scenario, BP values (SBP and DBP) are estimated from the corresponding PPG beats.
3. Materials Used
3.1. Data Set
3.2. Preprocessing
4. Methodology
4.1. Preprocessing Stage
4.2. Signal Segmentation
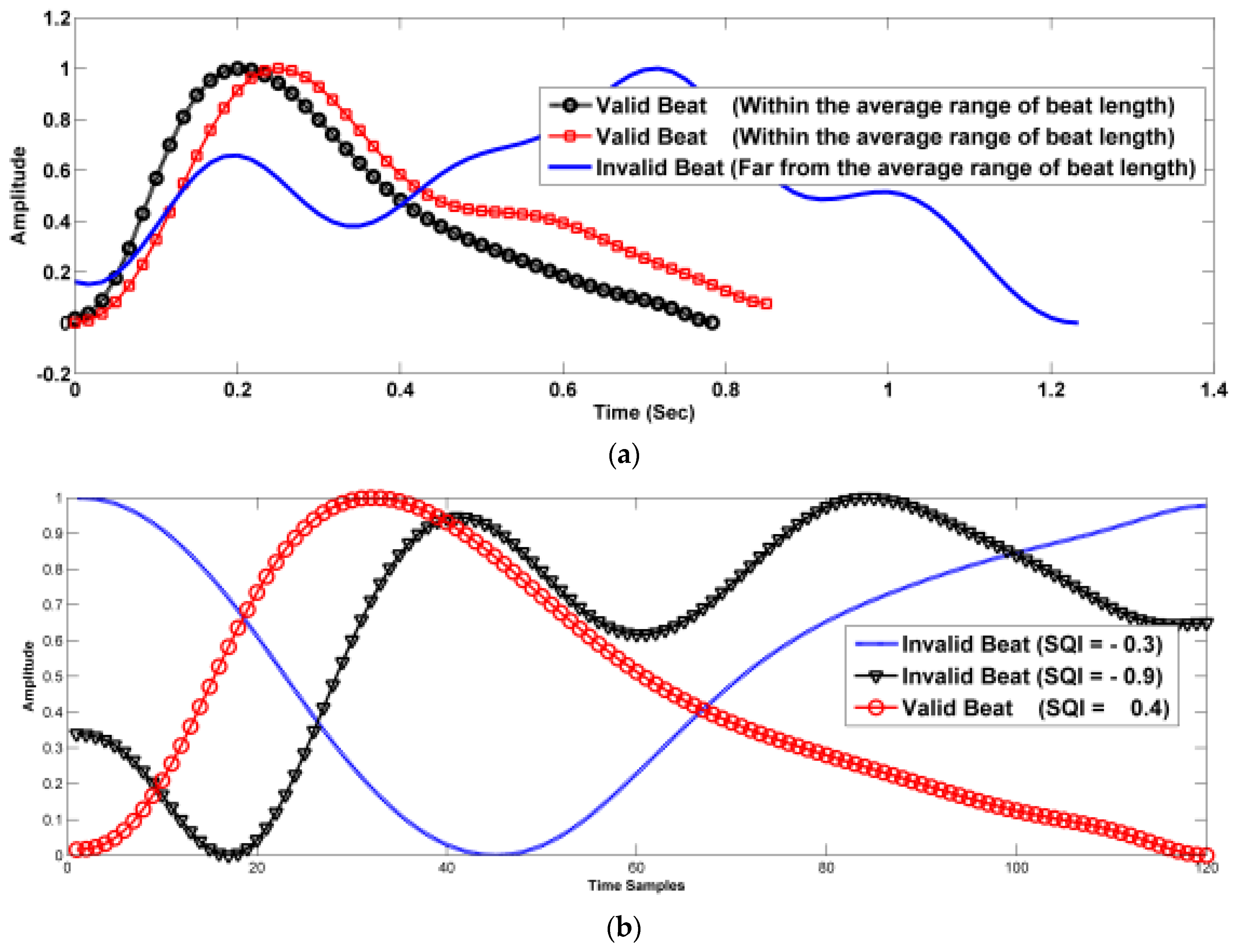
4.3. Beat Selection
4.4. Deep Learning Model
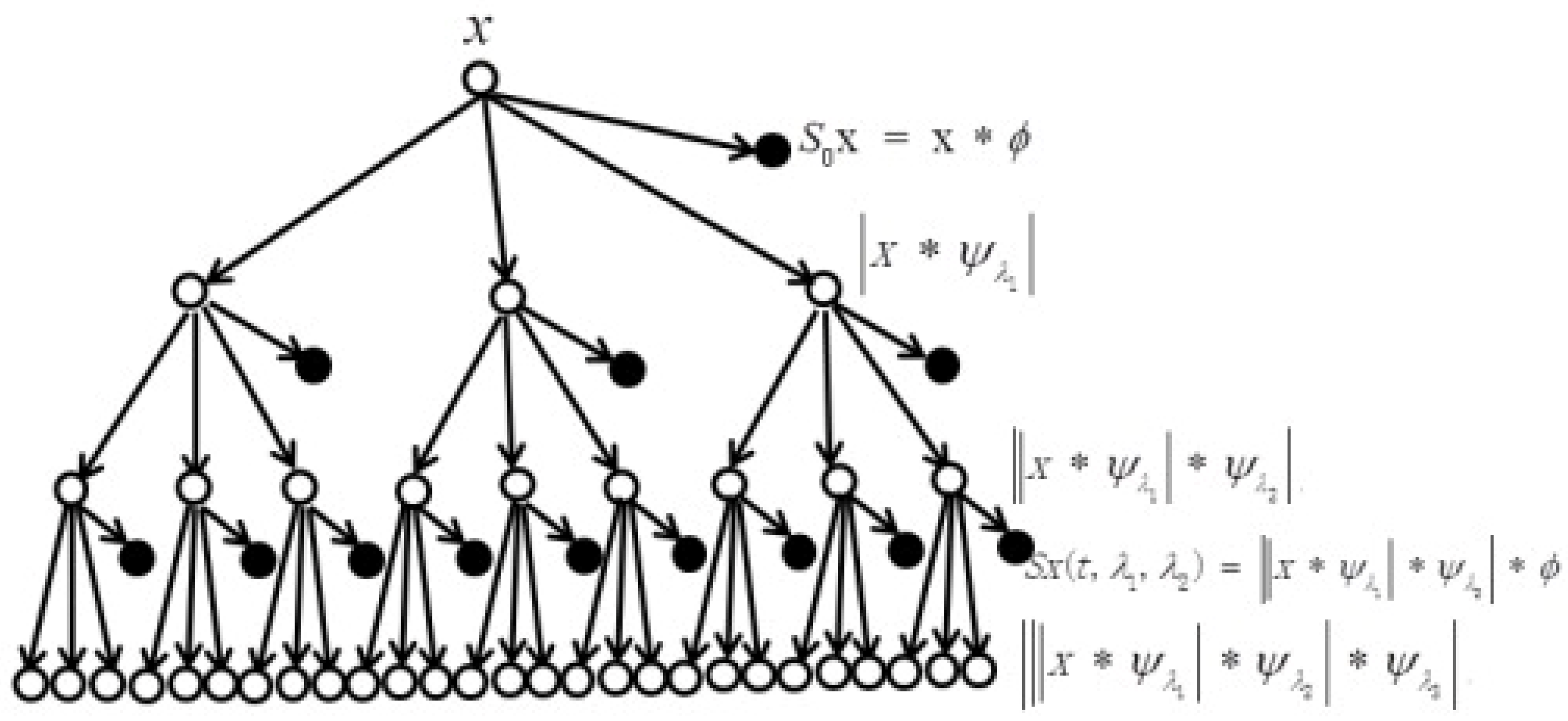
4.5. Wavelet Scattering Transform (WST)
4.6. LSTM Network
5. Experimental Results and Discussion
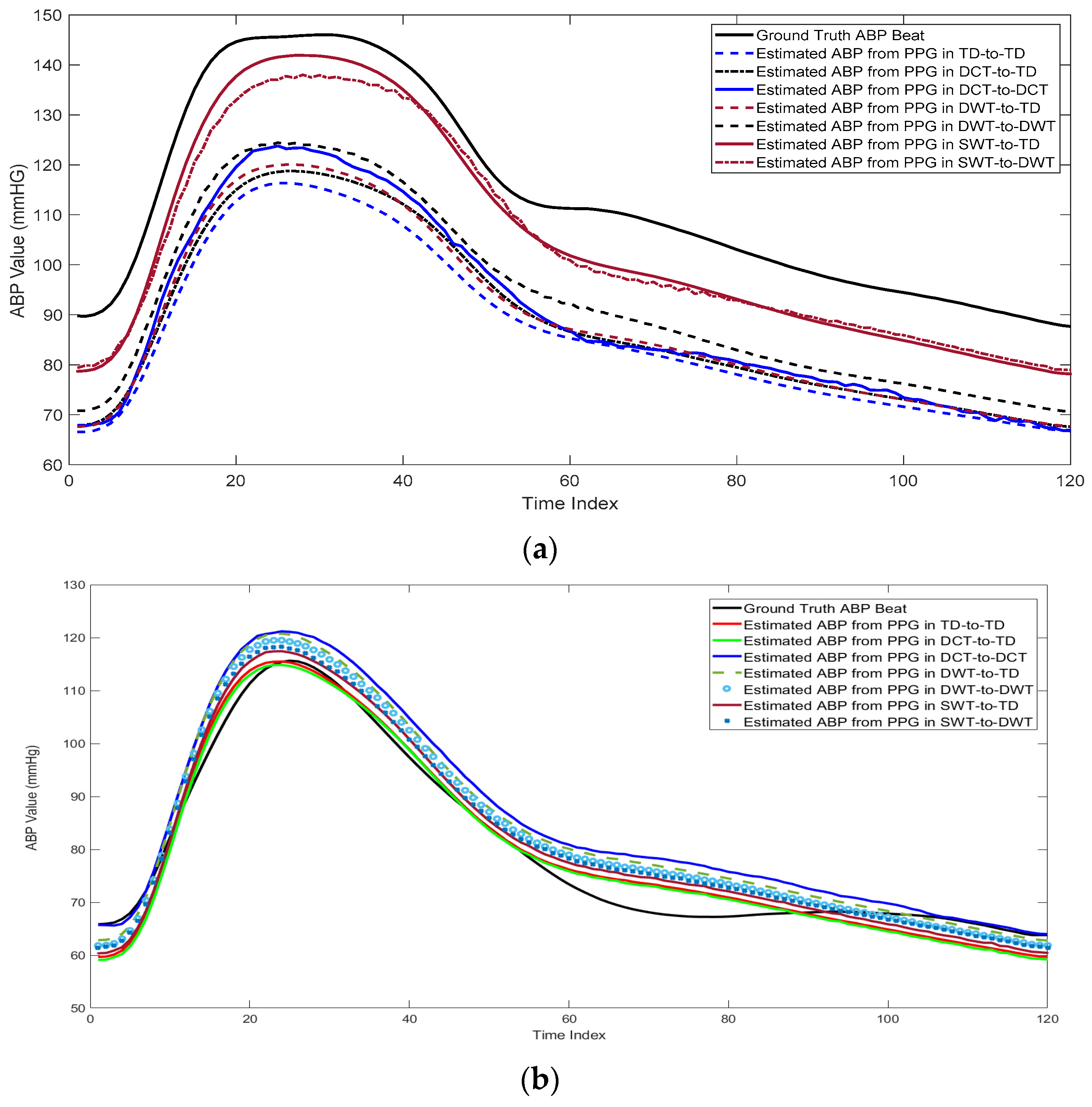
5.1. Beat-by-Beat cPPG-to-ABP Mapping
5.2. Evaluation of the Proposed Method Using cPPG Signals
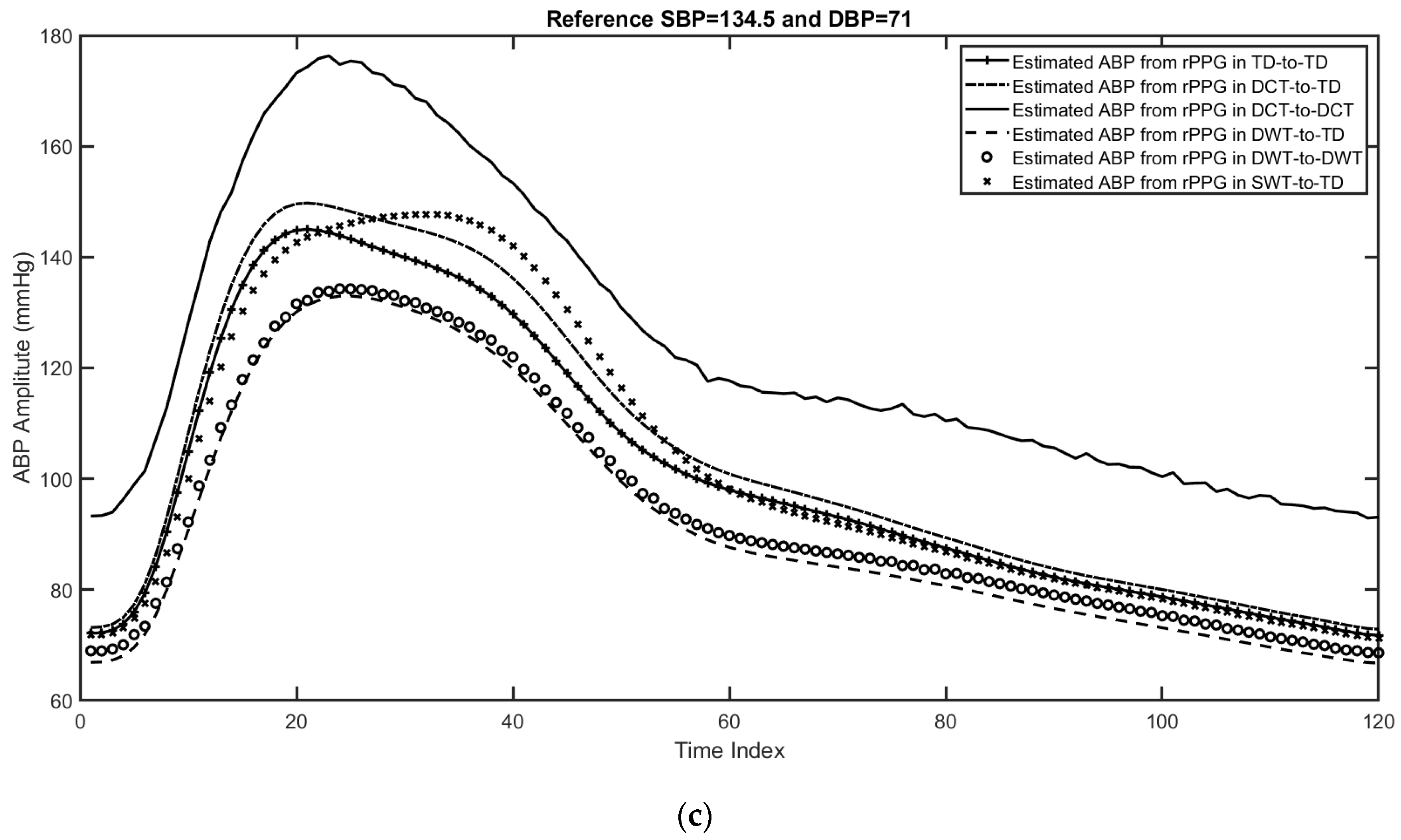
5.3. Evaluation of the Proposed Method Using rPPG Signals
5.4. Discussion
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab (accessed on 5 March 2022).
- American Society of Anesthesiologists. Standards of the American Society of Anesthesiologists: Standards for Basic Anesthetic Monitoring. 2020. Available online: https://www.asahq.org/standards-and-guidelines/standards-for-basic-anesthetic-monitoring (accessed on 1 October 2023).
- Martínez, G.; Howard, N.; Abbott, D.; Lim, K.; Ward, R.; Elgendi, M. Can photoplethysmography replace arterial blood pressure in the assessment of blood pressure? J. Clin. Med. 2018, 7, 316. [Google Scholar] [CrossRef]
- Panula, T.; Sirkia, J.-P.; Wong, D.; Kaisti, M. Advances in non-invasive blood pressure measurement techniques. IEEE Rev. Biomed. Eng. 2022, 16, 424–438. [Google Scholar] [CrossRef]
- Moraes, J.; Rocha, M.; Vasconcelos, G.; Filho, J.V.; De Albuquerque, V.; Alexandria, A. Advances in photopletysmography signal analysis for biomedical applications. Sensors 2018, 18, 1894. [Google Scholar] [CrossRef] [PubMed]
- Le, T.; Ellington, F.; Lee, T.Y.; Vo, K.; Khine, M.; Krishnan, S.K.; Dutt, N.; Cao, H. Continuous non-invasive blood pressure monitoring: A methodological review on measurement techniques. IEEE Access 2020, 8, 212478–212498. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2020, 101, e215–e220. [Google Scholar]
- Slapničar, G.; Luštrek, M.; Marinko, M. Continuous blood pressure estimation from PPG signal. Informatica 2018, 42, 33–42. [Google Scholar]
- Haddad, S.; Boukhayma, A.; Caizzone, A. Continuous ppg-based blood pressure monitoring using multi-linear regression. IEEE J. Biomed. Health Inform. 2021, 26, 2096–2105. [Google Scholar]
- Yan, W.-R.; Peng, R.-C.; Zhang, Y.-T.; Ho, D. Cuffless continuous blood pressure estimation from pulse morphology of photoplethysmograms. IEEE Access 2019, 7, 141970–141977. [Google Scholar] [CrossRef]
- Khalid, S.; Zhang, J.; Chen, F.; Zheng, D. Blood pressure estimation using photoplethysmography only: Comparison between different machine learning approaches. J. Healthc. Eng. 2018, 2018, 1548647. [Google Scholar] [CrossRef] [PubMed]
- Maqsood, S.; Xu, S.; Tran, S.; Garg, S.; Springer, M.; Karunanithi, M.; Mohawesh, R. A survey: From shallow to deep machine learning approaches for blood pressure estimation using biosensors. Expert Syst. Appl. 2022, 197, 116788. [Google Scholar]
- Xing, X.; Sun, M. Optical blood pressure estimation with photoplethysmography and FFT-based neural networks. Biomed. Opt. Express 2016, 7, 3007–3020. [Google Scholar] [CrossRef]
- Schrumpf, F.; Frenzel, P.; Aust, C.; Osterhoff, G.; Fuchs, M. Assessment of deep learning based blood pressure prediction from PPG and rPPG signals. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Nashville, TN, USA, 20–25 June 2021; pp. 3820–3830. [Google Scholar]
- Slapničar, G.; Mlakar, N.; Luštrek, M. Blood pressure estimation from photoplethysmogram using a spectro-temporal deep neural network. Sensors 2019, 19, 3420. [Google Scholar] [CrossRef] [PubMed]
- Harfiya, L.; Chang, C.-C.; Li, Y.-H. Continuous blood pressure estimation using exclusively photopletysmography by LSTM-based signal-to-signal translation. Sensors 2021, 21, 2952. [Google Scholar] [CrossRef] [PubMed]
- Ibtehaz, N.; Mahmud, S.; Chowdhury, M.E.H.; Khandakar, A.; Salman Khan, M.; Ayari, M.A.; Tahir, A.M.; Rahman, M.S. PPG2ABP: Translating Photoplethysmogram (PPG) Signals to Arterial Blood Pressure (ABP) Waveforms. Bioengineering 2022, 9, 692. [Google Scholar] [CrossRef]
- Hsu, Y.-C.; Li, Y.-H.; Chang, C.-C.; Harfiya, L.N. Generalized deep neural network model for cuffless blood pressure estimation with photoplethysmogram signal only. Sensors 2020, 20, 5668. [Google Scholar] [CrossRef]
- Schrumpf, F.; Frenzel, P.; Aust, C.; Osterhoff, G.; Fuchs, M. Assessment of Non-Invasive Blood Pressure Prediction from PPG and rPPG Signals Using Deep Learning. Sensors 2021, 21, 6022. [Google Scholar] [CrossRef]
- McCombie, D.B.; Reisner, A.T.; Asada, H.H. Adaptive blood pressure estimation from wearable PPG sensors using peripheral artery pulse wave velocity measurements and multi-channel blind identification of local arterial dynamics. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August 2006–3 September 2006; pp. 3521–3524. [Google Scholar]
- Gesche, H.; Grosskurth, D.; Küchler, G.; Patzak, A. Continuous blood pressure measurement by using the pulse transit time: Comparison to a cuff-based method. Eur. J. Appl. Physiol. 2012, 112, 309–315. [Google Scholar] [CrossRef]
- Kachuee, M.; Kiani, M.M.; Mohammadzade, H.; Shabany, M. Cuff-less high-accuracy calibration-free blood pressure estimation using pulse transit time. In Proceedings of the 2015 IEEE International Symposium on Circuits and Systems (ISCAS), Lisbon, Portugal, 24–27 May 2015; pp. 1006–1009. [Google Scholar]
- Chen, T.; Ng, S.H.; Teo, J.T.; Yang, X. Method and System for Optical Blood Pressure Monitoring. U.S. Patent 10,251,568, 2019. [Google Scholar]
- Mahmud, S.; Ibtehaz, N.; Khandakar, A.; Tahir, A.M.; Rahman, T.; Islam, K.R.; Hossain, M.S.; Rahman, M.S.; Musharavati, F.; Ayari, M.A.; et al. A Shallow U-Net Architecture for Reliably Predicting Blood Pressure (BP) from Photoplethysmogram (PPG) and Electrocardiogram (ECG) Signals. Sensors 2022, 22, 919. [Google Scholar] [CrossRef] [PubMed]
- Brophy, E.; De Vos, M.; Boylan, G.; Ward, T. Estimation of continuous blood pressure from ppg via a federated learning approach. Sensors 2021, 21, 6311. [Google Scholar] [CrossRef]
- Senturk, U.; Polat, K.; Yucedag, I. A Novel Blood Pressure Estimation Method with the Combination of Long Short Term Memory Neural Network and Principal Component Analysis Based on PPG Signals; Springer: Berlin/Heidelberg, Germany, 2019; pp. 868–876. [Google Scholar]
- Tanveer, M.S.; Hasan, M.K. Cuffless blood pressure estimation from electrocardiogram and photoplethysmogram using waveform based ANN-LSTM network. Biomed. Signal Process. Control 2019, 51, 382–392. [Google Scholar] [CrossRef]
- Esmaelpoor, J.; Moradi, M.H.; Kadkhodamohammadi, A. A multistage deep neural network model for blood pressure estimation using photoplethysmogram signals. Comput. Biol. Med. 2020, 120, 103719. [Google Scholar] [CrossRef] [PubMed]
- Hill, B.L.; Rakocz, N.; Rudas, Á.; Chiang, J.N.; Wang, S.; Hofer, I.; Cannesson, M.; Halperin, E. Imputation of the Continuous Arterial Line Blood Pressure Waveform from Non-Invasive Measurements Using Deep Learning. Sci. Rep. 2021, 11, 15755. [Google Scholar] [CrossRef] [PubMed]
- Mehrabadi, M.A.; Aqajari, S.A.H.; Zargari, A.H.A.; Dutt, N.; Rahmani, A.M. Novel Blood Pressure Waveform Reconstruction from Photoplethysmography Using Cycle Generative Adversarial Networks. arXiv 2022, arXiv:2201.09976. [Google Scholar]
- Saeed, M.; Lieu, C.; Raber, G.; Mark, R.G. MIMIC II: A massive temporal ICU patient database to support research in intelligent patient monitoring. Comput. Cardiol. 2002, 29, 641–644. [Google Scholar]
- Salah, M.; Omer, O.A.; Hassan, L.; Ragab, M.; Hassan, A.M.; Abdelreheem, A. Beat-Based PPG-ABP Cleaning Technique for Blood Pressure Estimation. IEEE Access 2022, 10, 55616–55626. [Google Scholar] [CrossRef]
- Oyallon, E.; Mallat, S.; Sifre, L. Generic deep networks with wavelet scattering. arXiv 2013, arXiv:1312.5940. [Google Scholar]
- Oyallon, E.; Belilovsky, E.; Zagoruyko, S. Scaling the scattering transform: Deep hybrid networks. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 5618–5627. [Google Scholar]
- Cotter, F.; Kingsbury, N. Visualizing and improving scattering networks. In Proceedings of the 2017 IEEE 27th International Workshop on Machine Learning for Signal Processing (MLSP), Tokyo, Japan, 25–28 September 2017; pp. 1–6. [Google Scholar]
- Oyallon, E.; Zagoruyko, S.; Huang, G.; Komodakis, N.; Lacoste-Julien, S.; Blaschko, M.; Belilovsky, E. Scattering networks for hybrid representation learning. IEEE Trans. Pattern Anal. Mach. Intell. 2018, 41, 2208–2221. [Google Scholar] [CrossRef] [PubMed]
- Salah, M.; Hassan, L.; Abdel-khier, S.; Hassan, A.M.; Omer, O.A. Robust Facial-Based Inter-Beat Interval Estimation through Spectral Signature Tracking and Periodic Filtering. In Intelligent Sustainable Systems; Springer: Berlin/Heidelberg, Germany, 2022; pp. 161–171. [Google Scholar]
- Sifre, L.; Mallat, S. Rotation, scaling and deformation invariant scattering for texture discrimination. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Portland, OR, USA, 23 June 2013–28 June 2013; pp. 1233–1240. [Google Scholar]
- Liu, Z.; Yao, G.; Zhang, Q.; Zhang, J.; Zeng, X. Wavelet scattering transform for ECG beat classification. Comput. Math. Methods Med. 2020, 2020, 3215681. [Google Scholar] [CrossRef]
- Bruna, J.; Mallat, S. Invariant scattering convolution networks. IEEE Trans. Pattern Anal. Mach. Intell. 2013, 35, 1872–1886. [Google Scholar] [CrossRef] [PubMed]
- Hochreiter, S.; Schmidhuber, J. Long short-term memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Beats | 158,094 |
| Beat Length (time samples) | 120 |
| Input Feature Domain | One of the following domains:
|
| Number of Channels | 4 × 1 Layer array |
| Layer specifications |
|
| Learning Rate | 0.005 |
| Number of Iterations per Epoch | 191 |
| Optimization function | L2-Norm |
| Optimization method | ADAM |
| Per-Beat Scenario | Domain | Time | DCT | DWT | WST |
|---|---|---|---|---|---|
| PPG2ABP | Input size | 121 × 1 | 120 × 1 | 120 × 1 | 120 × 1 |
| Output size | 120 × 1 | 120 × 1 | 120 × 1 | 120 × 1 | |
| PPG2SBP/DBP | Input size | 121 × 1 | 120 × 1 | 120 × 1 | 120 × 1 |
| Output size | 2 × 1 | 2 × 1 | 2 × 1 | 2 × 1 |
| Domain | Time | DCT | DWT | WST | |||
|---|---|---|---|---|---|---|---|
| Case | TD+BI-TD | DCT-TD | DCT-DCT | DWT-TD | DWT-DWT | WST-TD | WST-DWT |
| RMSE | 11.1663 | 11.3587 | 11.5532 | 10.9905 | 10.8554 | 9.2084 | 8.9935 |
| MAE | 9.8877 | 10.0606 | 10.1669 | 9.7415 | 9.6080 | 7.7671 | 7.6257 |
| Domain | Time | DCT | DWT | WST | ||||
|---|---|---|---|---|---|---|---|---|
| BP | DBP | SBP | DBP | SBP | DBP | SBP | DBP | SBP |
| RMSE | 9.5636 | 17.6580 | 9.7477 | 17.9762 | 9.4865 | 17.3914 | 6.9164 | 14.2079 |
| MAE | 7.1212 | 13.5720 | 7.2472 | 13.9056 | 7.0517 | 13.3367 | 5.0945 | 10.8358 |
| Domain | Time | DCT | DWT | WST | ||||
|---|---|---|---|---|---|---|---|---|
| BP | DBP | SBP | DBP | SBP | DBP | SBP | DBP | SBP |
| RMSE | 11.1798 | 17.8066 | 11.7560 | 17.7062 | 11.2555 | 16.9441 | 11.2034 | 15.4742 |
| MAE | 11.1295 | 15.0720 | 11.5511 | 16.7606 | 10.0244 | 14.3486 | 9.5390 | 13.3852 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Omer, O.A.; Salah, M.; Hassan, A.M.; Abdel-Nasser, M.; Sugita, N.; Saijo, Y. Blood Pressure Estimation from Photoplythmography Using Hybrid Scattering–LSTM Networks. BioMedInformatics 2024, 4, 139-157. https://doi.org/10.3390/biomedinformatics4010010
Omer OA, Salah M, Hassan AM, Abdel-Nasser M, Sugita N, Saijo Y. Blood Pressure Estimation from Photoplythmography Using Hybrid Scattering–LSTM Networks. BioMedInformatics. 2024; 4(1):139-157. https://doi.org/10.3390/biomedinformatics4010010
Chicago/Turabian StyleOmer, Osama A., Mostafa Salah, Ammar M. Hassan, Mohamed Abdel-Nasser, Norihiro Sugita, and Yoshifumi Saijo. 2024. "Blood Pressure Estimation from Photoplythmography Using Hybrid Scattering–LSTM Networks" BioMedInformatics 4, no. 1: 139-157. https://doi.org/10.3390/biomedinformatics4010010
APA StyleOmer, O. A., Salah, M., Hassan, A. M., Abdel-Nasser, M., Sugita, N., & Saijo, Y. (2024). Blood Pressure Estimation from Photoplythmography Using Hybrid Scattering–LSTM Networks. BioMedInformatics, 4(1), 139-157. https://doi.org/10.3390/biomedinformatics4010010