
From Control Algorithm to Human Trial: Biomechanical Proof of a Speed-Adaptive Ankle–Foot Orthosis for Foot Drop in Level-Ground Walking


Abstract
1. Introduction
2. Motion Planning and Control Method
2.1. CGA Data of the Angular Velocity of the Ankle Joint
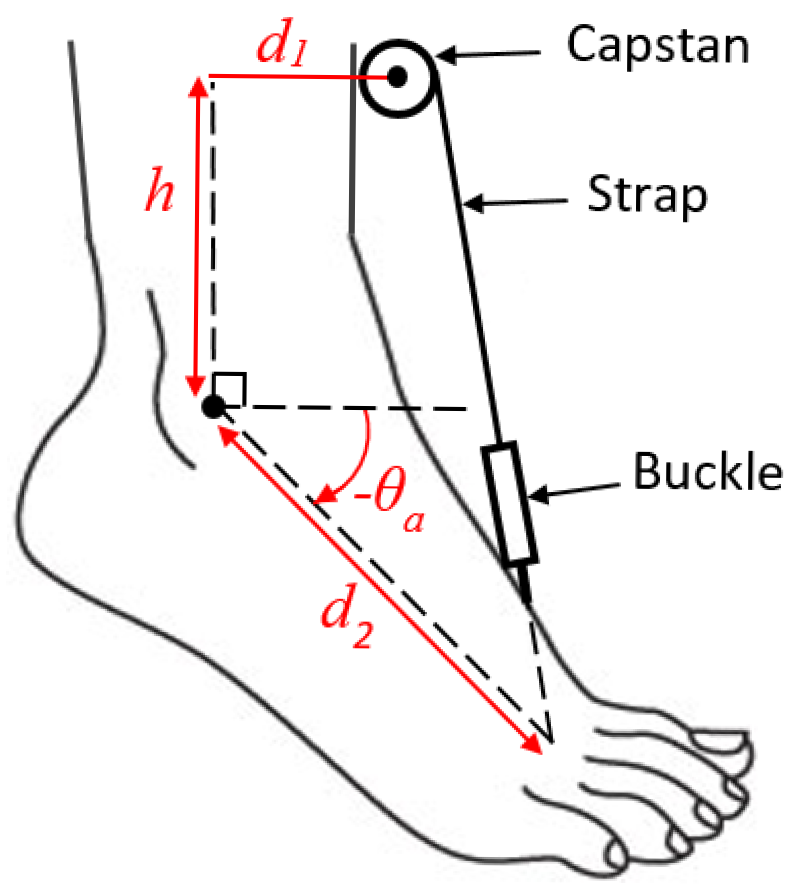
2.2. The Geometry of the Device Configuration
- Ramp-up time length: 2.7% of ;
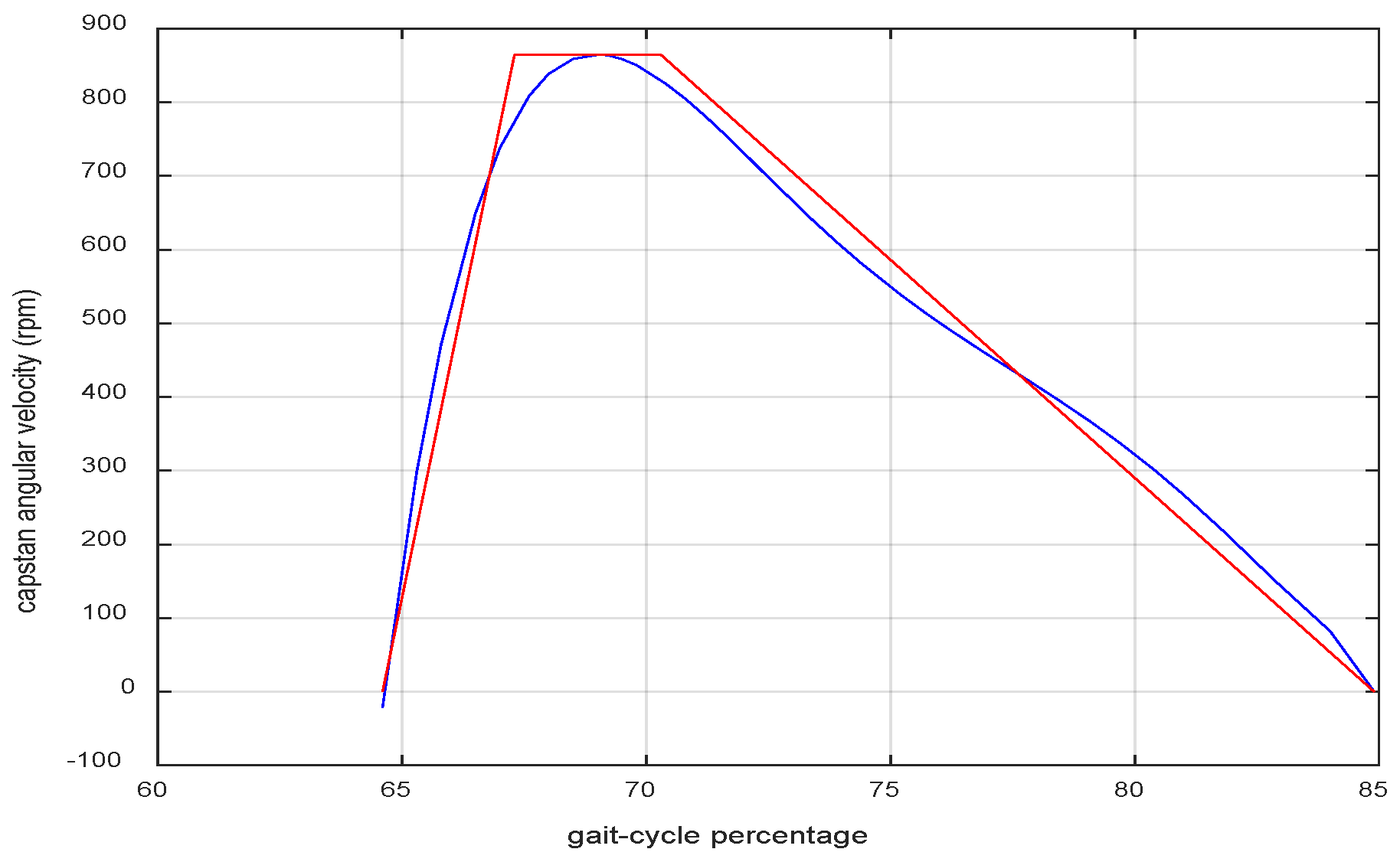
- Maximum angular velocity of the capstan in rpm: 21,610 × ;
- Constant speed time length: 3.6% of ;
- Ramp-down time length: 14.6% of .
2.3. Gait Period Measurement
2.4. The Entire Motion Planning and Control Method
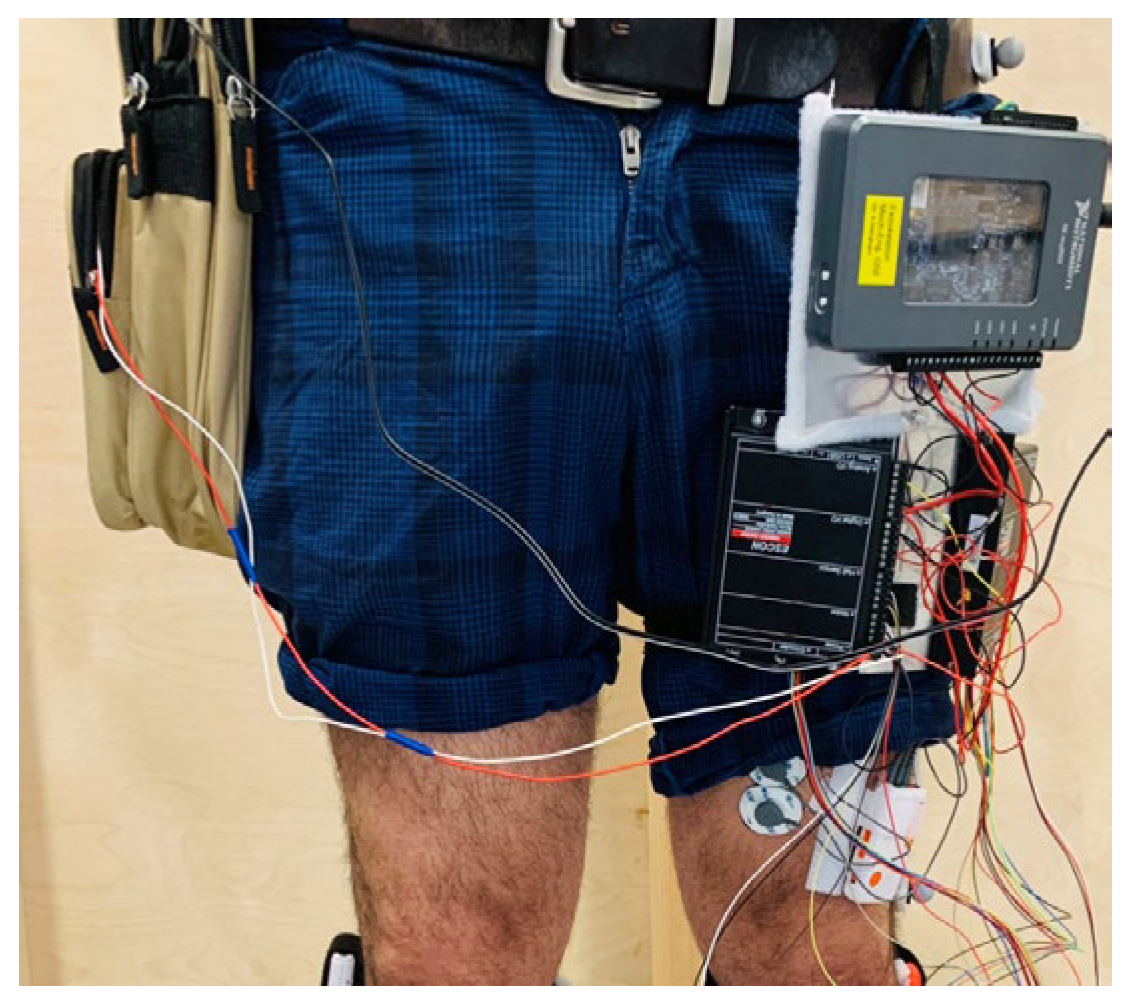
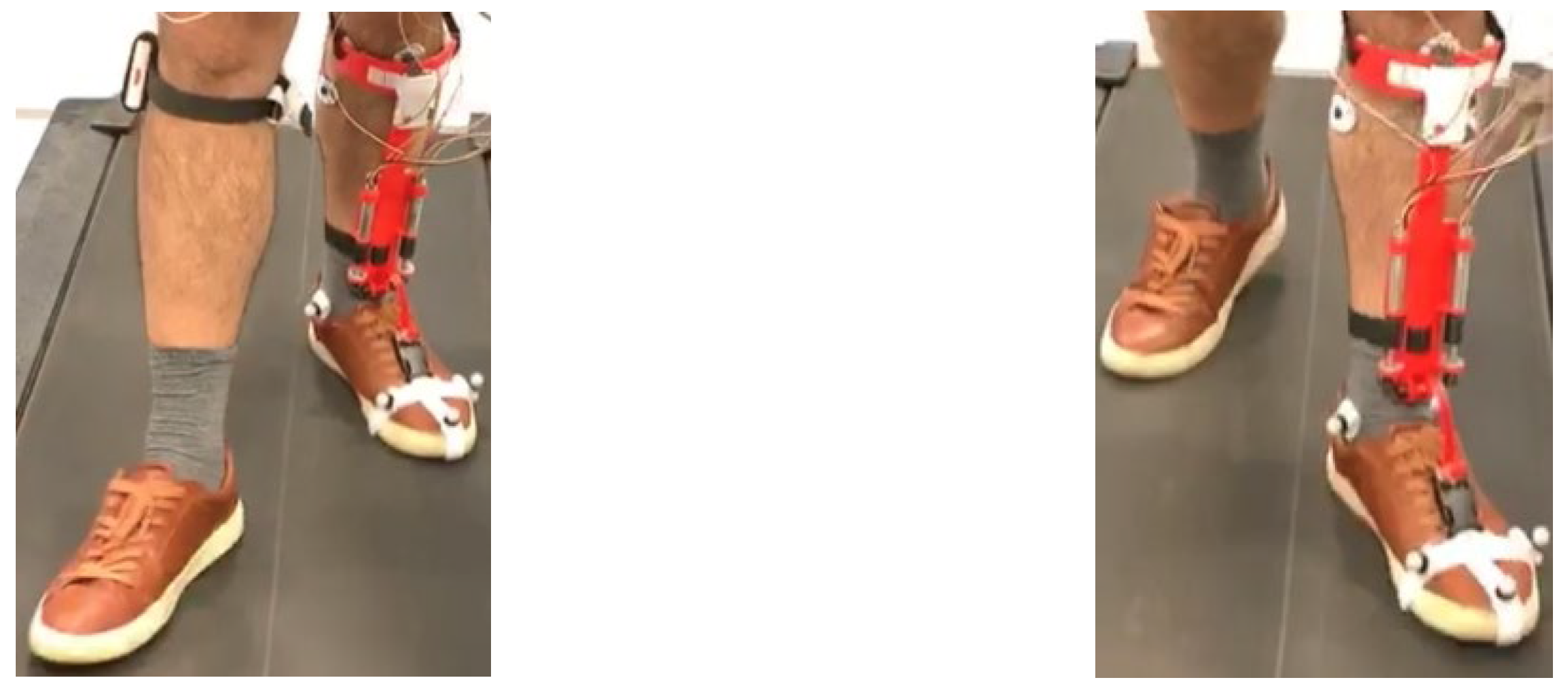
3. The User Experiments
4. Performance Assessment
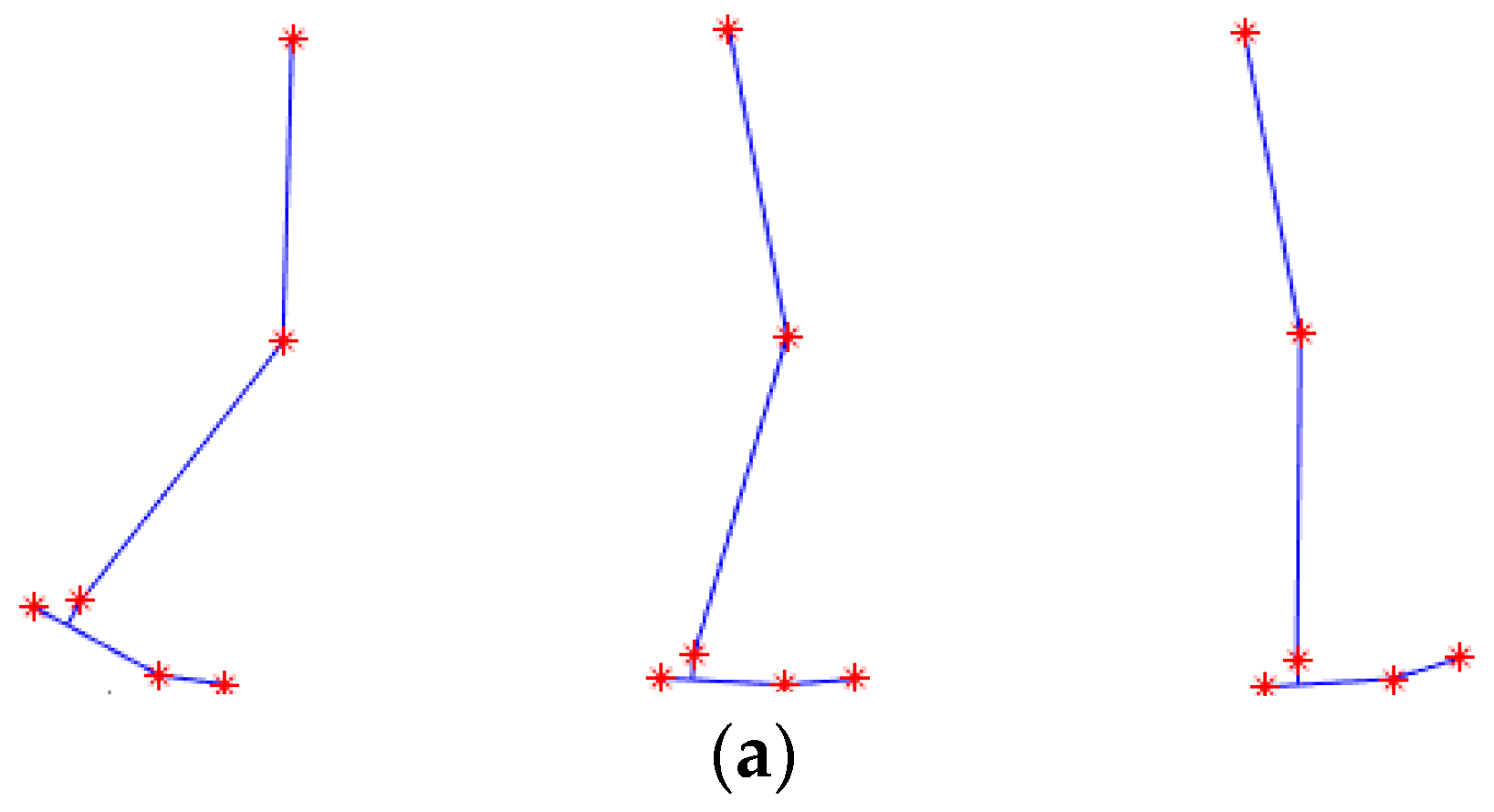
4.1. Motion Capture (MoCap) and Kinematic Analysis
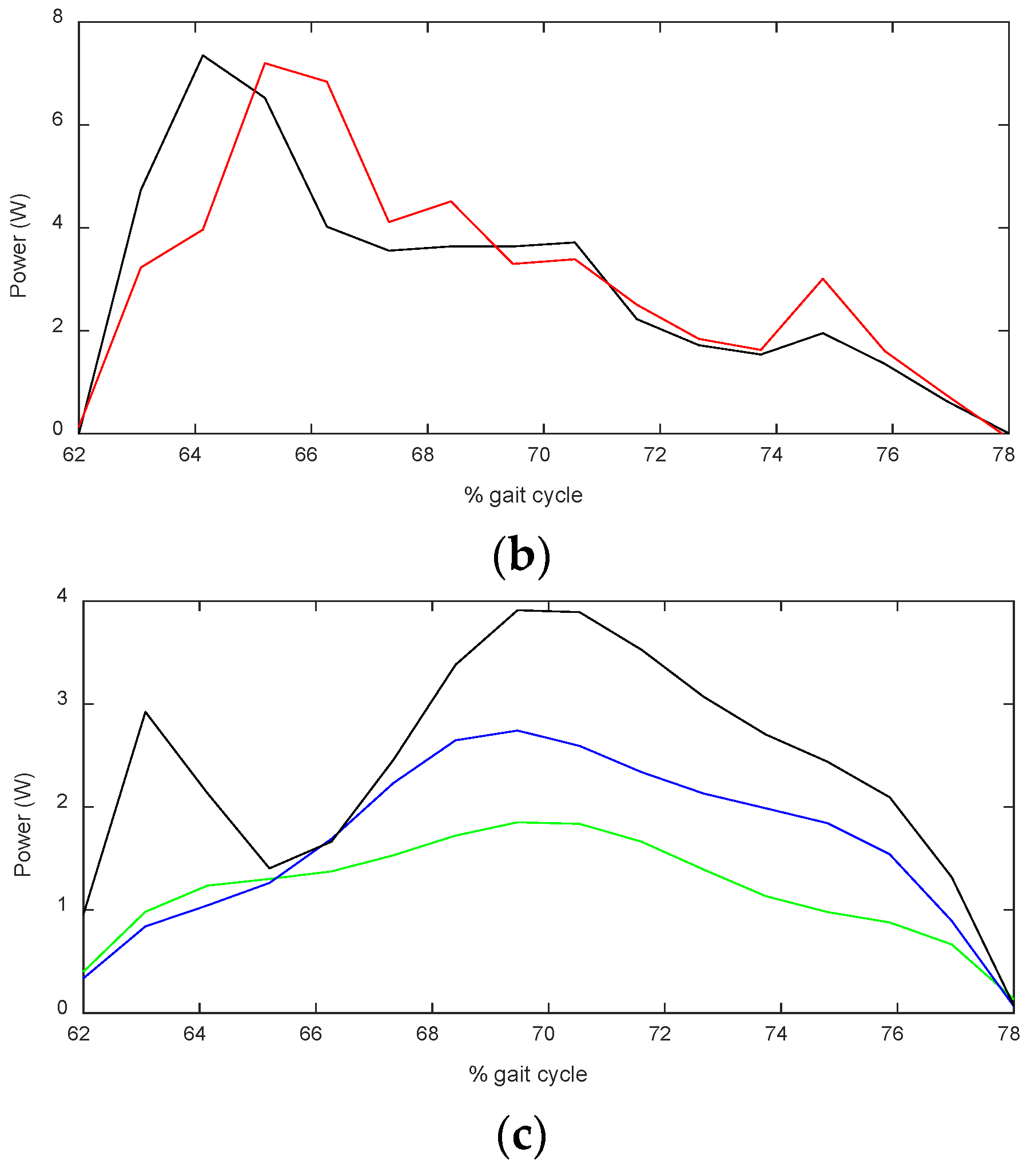
4.2. Measurement of the Output Power of the Device
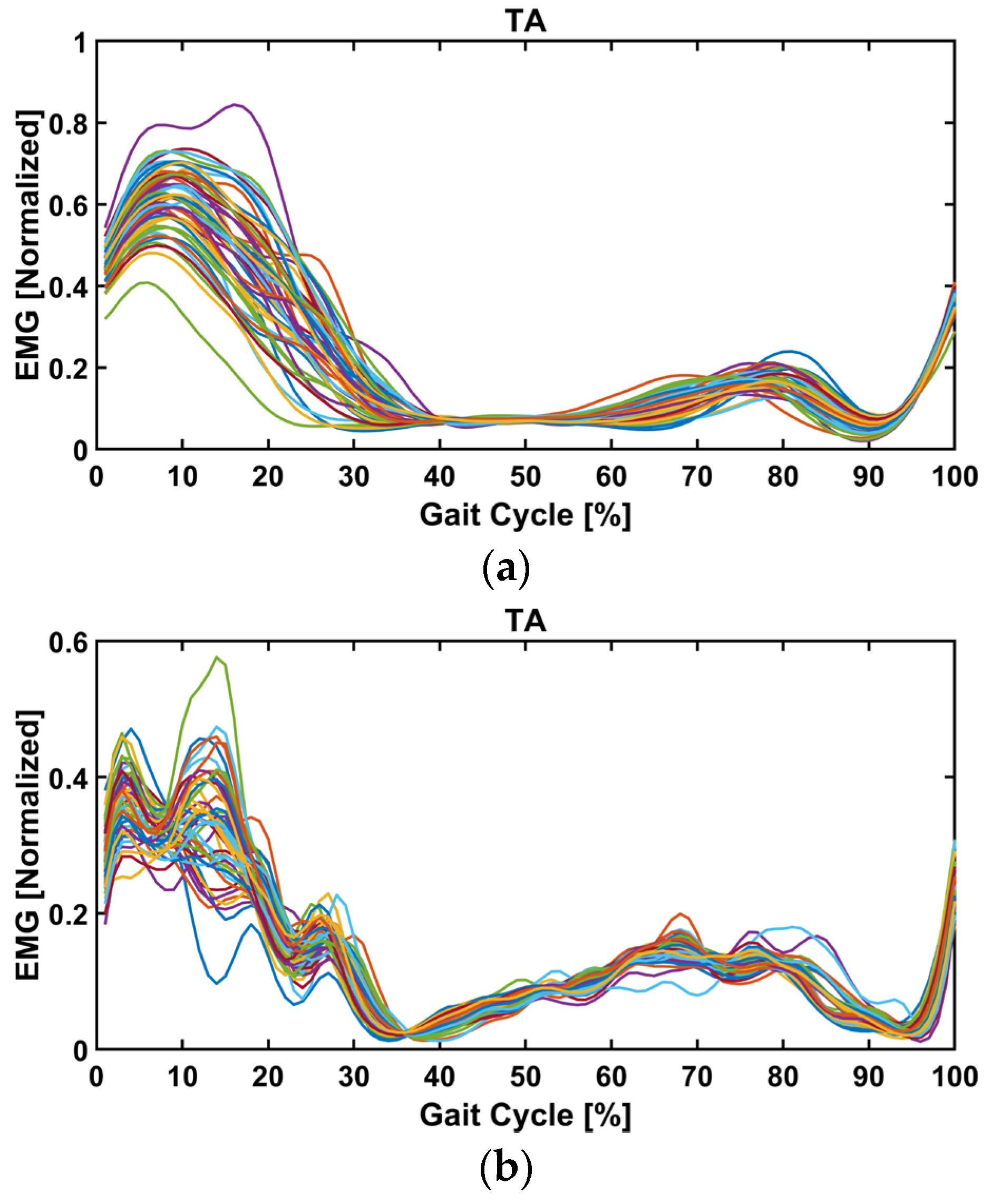
4.3. EMG Signal Measurement
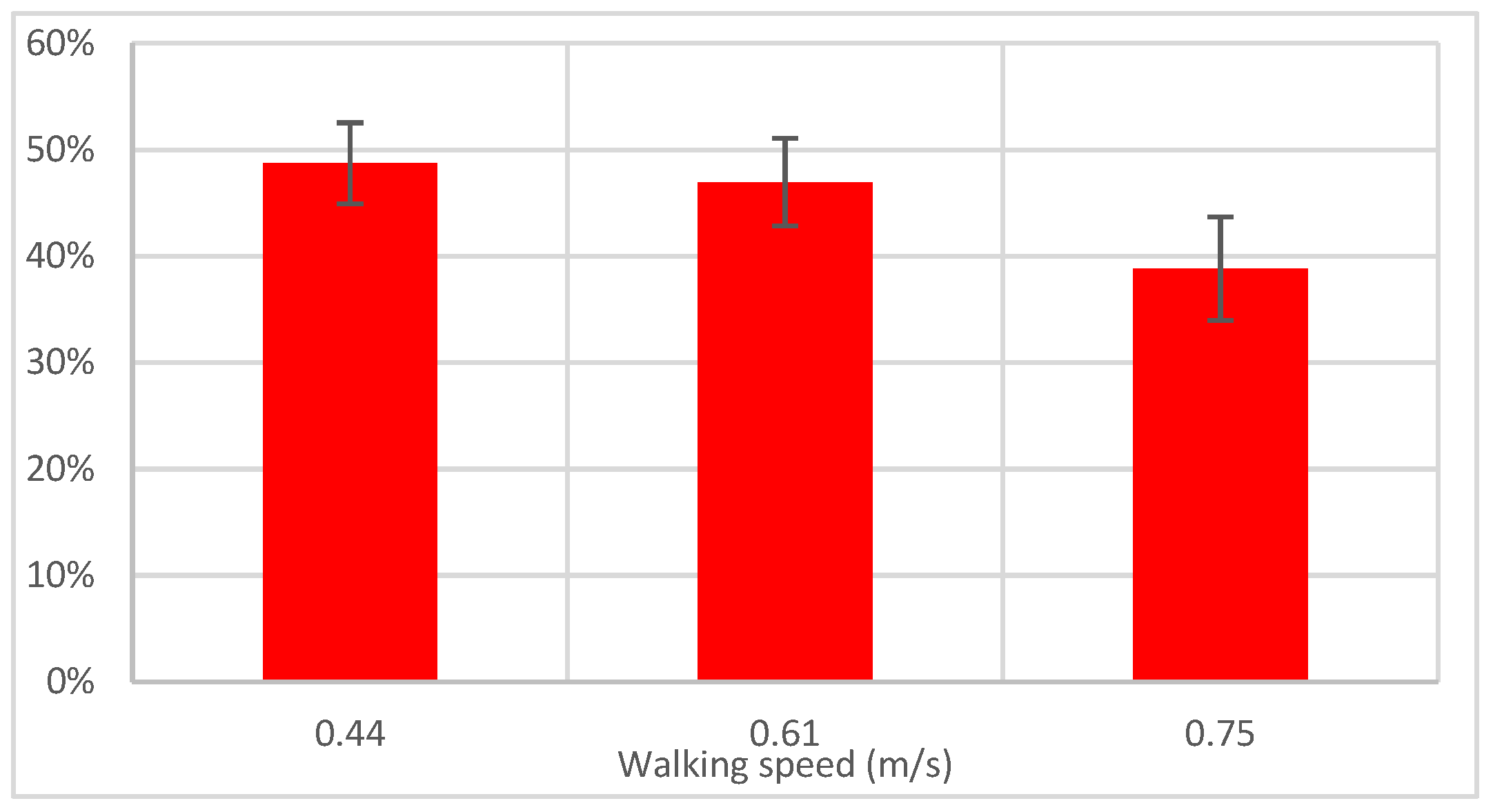
4.4. Assistance from the Device and Muscle Activation Comparison
5. Discussion, Conclusions, and Limitations of This Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stewart, J.D. Foot drop: Where, why and what to do? Pract. Neurol. 2008, 8, 158–169. [Google Scholar] [CrossRef]
- Fraser, J.J.; Koldenhoven, R.M.; Jaffri, A.H.; Park, J.S.; Saliba, S.F.; Hart, J.M.; Hertel, J. Foot impairments contribute to functional limitation in individuals with ankle sprain and chronic ankle instability. Knee Surg. Sports Traumatol. Arthrosc. 2020, 20, 1600–1610. [Google Scholar] [CrossRef]
- Lui, Z.W.; Awad, M.I.; Abouhossein, A.; Dehghani-Sanij, A.A.; Messenger, N. Virtual prototyping of a semi-active transfemoral prosthetic leg. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2015, 229, 350–361. [Google Scholar] [CrossRef]
- Carolus, A.; Mesbah, D.; Brenke, C. Focusing on foot drop: Results from a patient survey and clinical examination. Foot 2021, 46, 101693. [Google Scholar] [CrossRef]
- Thakur, S. Global Foot Drop Treatment Devices to Grow at a Substantial CAGR of 8.15% by 2027. Available online: https://www.globenewswire.com/en/news-release/2022/11/24/2562397/0/en/Global-Foot-Drop-Treatment-Devices-to-Grow-at-a-Substantial-CAGR-of-8-15-by-2027-DelveInsight.html (accessed on 24 November 2022).
- Kitaoka, H.B.; Crevoisier, X.M.; Harbst, K.; Hansen, D.; Kotajarvi, B.; Kaufman, K. The Effect of Custom-Made Braces for the Ankle and Hindfoot on Ankle and Foot Kinematics and Ground Reaction Forces. Arch. Phys. Med. Rehabil. 2006, 87, 130–135. [Google Scholar] [CrossRef]
- Khan, A.M.; Yun, D.-w.; Zuhaib, K.M.; Iqbal, J.; Yan, R.-J.; Khan, F.; Han, C. Estimation of Desired Motion Intention and compliance control for upper limb assist exoskeleton. Int. J. Control. Autom. Syst. 2017, 15, 802–814. [Google Scholar] [CrossRef]
- Yoon, J.; Kumar, R.P.; Özer, A. An adaptive foot device for increased gait and postural stability in lower limb Orthoses and exoskeletons. Int. J. Control. Autom. Syst. 2011, 9, 515. [Google Scholar] [CrossRef]
- Gordon, K.E.; Ferris, D.P. Learning to walk with a robotic ankle exoskeleton. J. Biomech. 2007, 40, 2636–2644. [Google Scholar] [CrossRef]
- Ferris, D.P.; Gordon, K.E.; Sawicki, G.S.; Peethambaran, A. An improved powered ankle–foot orthosis using proportional myoelectric control. Gait Posture 2006, 23, 425–428. [Google Scholar] [CrossRef]
- Young, A.J.; Ferris, D.P. State of the Art and Future Directions for Lower Limb Robotic Exoskeletons. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 171–182. [Google Scholar] [CrossRef]
- Noël, M.; Cantin, B.; Lambert, S.; Gosselin, C.M.; Bouyer, L.J. An ElectroHydraulic Actuated Ankle Foot Orthosis to Generate Force Fields and to Test Proprioceptive Reflexes During Human Walking. IEEE Trans. Neural Syst. Rehabil. Eng. 2008, 16, 390–399. [Google Scholar] [CrossRef]
- Jamwal, P.K.; Xie, S.Q.; Hussain, S.; Parsons, J.G. An Adaptive Wearable Parallel Robot for the Treatment of Ankle Injuries. IEEE ASME Trans. Mechatron. 2014, 19, 64–75. [Google Scholar] [CrossRef]
- Saglia, J.A.; Tsagarakis, N.G.; Dai, J.S.; Caldwell, D.G. Control Strategies for Patient-Assisted Training Using the Ankle Rehabilitation Robot (ARBOT). IEEE ASME Trans. Mechatron. 2013, 18, 1799–1808. [Google Scholar] [CrossRef]
- Rus, D.; Tolley, M.T. Design, fabrication and control of soft robots. Nature 2015, 521, 467. [Google Scholar] [CrossRef]
- Park, Y.-L.; Chen, B.-R.; Pérez-Arancibia, N.O.; Young, D.; Stirling, L.; Wood, R.J.; Goldfield, E.C.; Nagpal, R. Design and control of a bio-inspired soft wearable robotic device for ankle–foot rehabilitation. Bioinspir. Biomim. 2014, 9, 016007. [Google Scholar] [CrossRef]
- Zakria, M.; Maqbool, H.F.; Hussain, T.; Awad, M.I.; Mehryar, P.; Iqbal, N.; Dehghani-Sanij, A.A. Heuristic based gait event detection for human lower limb movement. In Proceedings of the 2017 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Orlando, FL, USA, 16–19 February 2017; IEEE: Piscataway, NJ, USA, 2017. [Google Scholar]
- Maqbool, H.F.; Husman, M.A.B.; Awad, M.I.; Abouhossein, A.; Mehryar, P.; Iqbal, N.; Dehghani-Sanij, A.A. Real-time gait event detection for lower limb amputees using a single wearable sensor. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; IEEE: Piscataway, NJ, USA, 2016. [Google Scholar]
- Martinez-Hernandez, U.; Mahmood, I.; Dehghani-Sanij, A.A. Simultaneous Bayesian Recognition of Locomotion and Gait Phases With Wearable Sensors. IEEE Sens. J. 2018, 18, 1282–1290. [Google Scholar] [CrossRef]
- Staudenmayer, J.; Pober, D.; Crouter, S.; Bassett, D.; Freedson, P. An artificial neural network to estimate physical activity energy expenditure and identify physical activity type from an accelerometer. J. Appl. Physiol. 2009, 107, 1300–1307. [Google Scholar] [CrossRef]
- Khan, A.M.; Lee, Y.K.; Kim, T. Accelerometer signal-based human activity recognition using augmented autoregressive model coefficients and artificial neural nets. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008. [Google Scholar]
- Yuan, K.; Parri, A.; Yan, T.; Wang, L.; Munih, M.; Wang, Q.; Vitiello, N. A realtime locomotion mode recognition method for an active pelvis orthosis. In Proceedings of the 2015 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Hamburg, Germany, 28 September–2 October 2015. [Google Scholar]
- Huang, H.; Zhang, F.; Hargrove, L.J.; Dou, Z.; Rogers, D.R.; Englehart, K.B. Continuous Locomotion-Mode Identification for Prosthetic Legs Based on Neuromuscular–Mechanical Fusion. IEEE Trans. Biomed. Eng. 2011, 58, 2867–2875. [Google Scholar] [CrossRef]
- Thrun, S.; Burgard, W.; Fox, D. Probabilistic robotics. In Intelligent Robotics and Autonomous Agents; MIT: Cambridge, MA, USA; London, UK, 2005. [Google Scholar]
- Martinez-Hernandez, U.; Dodd, T.J.; Prescott, T.J. Feeling the Shape: Active Exploration Behaviors for Object Recognition With a Robotic Hand. IEEE Trans. Syst. Man Cybern. Syst. 2018, 48, 2339–2348. [Google Scholar] [CrossRef]
- Martinez-Hernandez, U.; Dodd, T.J.; Evans, M.H.; Prescott, T.J.; Lepora, N.F. Active sensorimotor control for tactile exploration. Robot. Auton. Syst. 2017, 87, 15–27. [Google Scholar] [CrossRef]
- Ferreira, J.; Lobo, J.; Bessiere, P.; Castelo-Branco, M.; Dias, J. A Bayesian framework for active artificial perception. IEEE Trans. Cybern. 2013, 43, 699–711. [Google Scholar] [CrossRef]
- Young, A.J.; Simon, A.M.; Fey, N.P.; Hargrove, L.J. Intent Recognition in a Powered Lower Limb Prosthesis Using Time History Information. Ann. Biomed. Eng. 2014, 42, 631–641. [Google Scholar] [CrossRef]
- Varol, H.A.; Sup, F.; Goldfarb, M. Multiclass Real-Time Intent Recognition of a Powered Lower Limb Prosthesis. IEEE Trans. Biomed. Eng. 2010, 57, 542–551. [Google Scholar] [CrossRef]
- Martinez-Hernandez, U.; Rubio-Solis, A.; Cedeno-Campos, V.; Dehghani-Sanij, A.A. Towards an intelligent wearable ankle robot for assistance to foot drop. In Proceedings of the 2019 IEEE International Conference on Systems, Man and Cybernetics (SMC), Bari, Italy, 6–9 October 2019. [Google Scholar]
- Martinez-Hernandez, U.; Firouzy, S.; Mehryar, P.; Meng, L.; Childs, C.; Buis, A.; Dehghani-Sanij, A.A. Human-in-the-loop layered architecture for control of a wearable ankle-foot robot. Robot. Auton. Syst. 2023, 161, 104353. [Google Scholar] [CrossRef]
- Winter, D.A. Biomechanics and Motor Control of Human Gait: Normal, Elderly and Pathological; CIRD: Seoul, Republic of Korea, 1991. [Google Scholar]
- Winter, D.A. Energy generation and absorption at the ankle and knee during fast, natural, and slow cadences. Clin. Orthop. Relat. Res. 1983, 175, 147–154. [Google Scholar] [CrossRef]
- Murray, M.P.; Drought, A.B.; Kory, R.C. Walking Patterns of Normal Men. JBJS 1964, 46, 335–360. [Google Scholar] [CrossRef]
- Krishnan, R.H.; Devanandh, V.; Brahma, A.K.; Pugazhenthi, S. Estimation of Mass Moment of Inertia of Human Body, When Bending Forward, for The Design of A Self-Transfer Robotic Facility. J. Eng. Sci. Technol. 2016, 11, 166–176. [Google Scholar]
- Farina, D.; Merletti, R.; Enoka, R.M. The extraction of neural strategies from the surface EMG. J. Appl. Physiol. 2004, 96, 1486–1495. [Google Scholar] [CrossRef]
- Mehryar, P.; Shourijeh, M.S.; Rezaeian, T.; Khandan, A.R.; Messenger, N.; O’Connor, R.; Farahmand, F.; Dehghani-Sanij, A. Differences in muscle synergies between healthy subjects and transfemoral amputees during normal transient-state walking speed. Gait Posture 2020, 76, 98–103. [Google Scholar] [CrossRef]
- Mehryar, P.; Shourijeh, M.; Rezaeian, T.; Iqbal, N.; Messenger, N.; Dehghani-Sanij, A.A. Changes in synergy of transtibial amputee during gait: A pilot study. In Proceedings of the 2017 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Orlando, FL, USA, 16–19 February 2017; IEEE: Piscataway, NJ, USA, 2017. [Google Scholar]
- Mehryar, P.; Shourijeh, M.S.; Rezaeian, T.; Khandan, A.R.; Messenger, N.; O’Connor, R.; Farahmand, F.; Dehghani-Sanij, A. Muscular activity comparison between non-amputees and transfemoral amputees during normal transient-state walking speed. Med. Eng. Phys. 2021, 95, 39–44. [Google Scholar] [CrossRef]
- Mehryar, P.; Shourijeh, M.; Rezaeian, T.; Khandan, A.; Messenger, N.; O’Connor, R.; Farahmand, F.; Dehghani-Sanij, A. The Impact of Different Self-Selected Walking Speeds on Muscle Synergies in Transfemoral Amputees during Transient-State Gait. Biomechanics 2024, 4, 14–33. [Google Scholar] [CrossRef]
- Stegeman, D.; Hermens, H. Standards for surface electromyography: The European project Surface EMG for non-invasive assessment of muscles (SENIAM). Enschede Roessingh Res. Dev. 2007, 10, 108–112. [Google Scholar]
- Pataky, T.C.; Vanrenterghem, J.; Robinson, M.A. Zero-vs. one-dimensional, parametric vs. non-parametric, and confidence interval vs. hypothesis testing procedures in one-dimensional biomechanical trajectory analysis. J. Biomech. 2015, 48, 1277–1285. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Speed (m/s) | No-Load Power (W) | Gross Power (W) | Pure Assistive Power (W) | Estimated Required Power (W) |
|---|---|---|---|---|
| 0.44 | 1.54 | 2.12 | 0.58 | 1.19 |
| 0.61 | 2.29 | 3.06 | 0.77 | 1.64 |
| 0.75 | 2.57 | 3.49 | 0.92 | 2.37 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mehryar, P.; Firouzy, S.; Martinez-Hernandez, U.; Dehghani-Sanij, A. From Control Algorithm to Human Trial: Biomechanical Proof of a Speed-Adaptive Ankle–Foot Orthosis for Foot Drop in Level-Ground Walking. Biomechanics 2025, 5, 51. https://doi.org/10.3390/biomechanics5030051
Mehryar P, Firouzy S, Martinez-Hernandez U, Dehghani-Sanij A. From Control Algorithm to Human Trial: Biomechanical Proof of a Speed-Adaptive Ankle–Foot Orthosis for Foot Drop in Level-Ground Walking. Biomechanics. 2025; 5(3):51. https://doi.org/10.3390/biomechanics5030051
Chicago/Turabian StyleMehryar, Pouyan, Sina Firouzy, Uriel Martinez-Hernandez, and Abbas Dehghani-Sanij. 2025. "From Control Algorithm to Human Trial: Biomechanical Proof of a Speed-Adaptive Ankle–Foot Orthosis for Foot Drop in Level-Ground Walking" Biomechanics 5, no. 3: 51. https://doi.org/10.3390/biomechanics5030051
APA StyleMehryar, P., Firouzy, S., Martinez-Hernandez, U., & Dehghani-Sanij, A. (2025). From Control Algorithm to Human Trial: Biomechanical Proof of a Speed-Adaptive Ankle–Foot Orthosis for Foot Drop in Level-Ground Walking. Biomechanics, 5(3), 51. https://doi.org/10.3390/biomechanics5030051