A Prospective Study Evaluating Gait and Clinical Outcome Following First Metatarsophalangeal Arthrodesis for Hallux Rigidus

 , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Operative Technique
2.3. Motion Analysis
2.4. Data Analysis
2.5. Clinical Assessment
2.6. Radiographic Evaluation
2.7. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Spatiotemporal Parameters
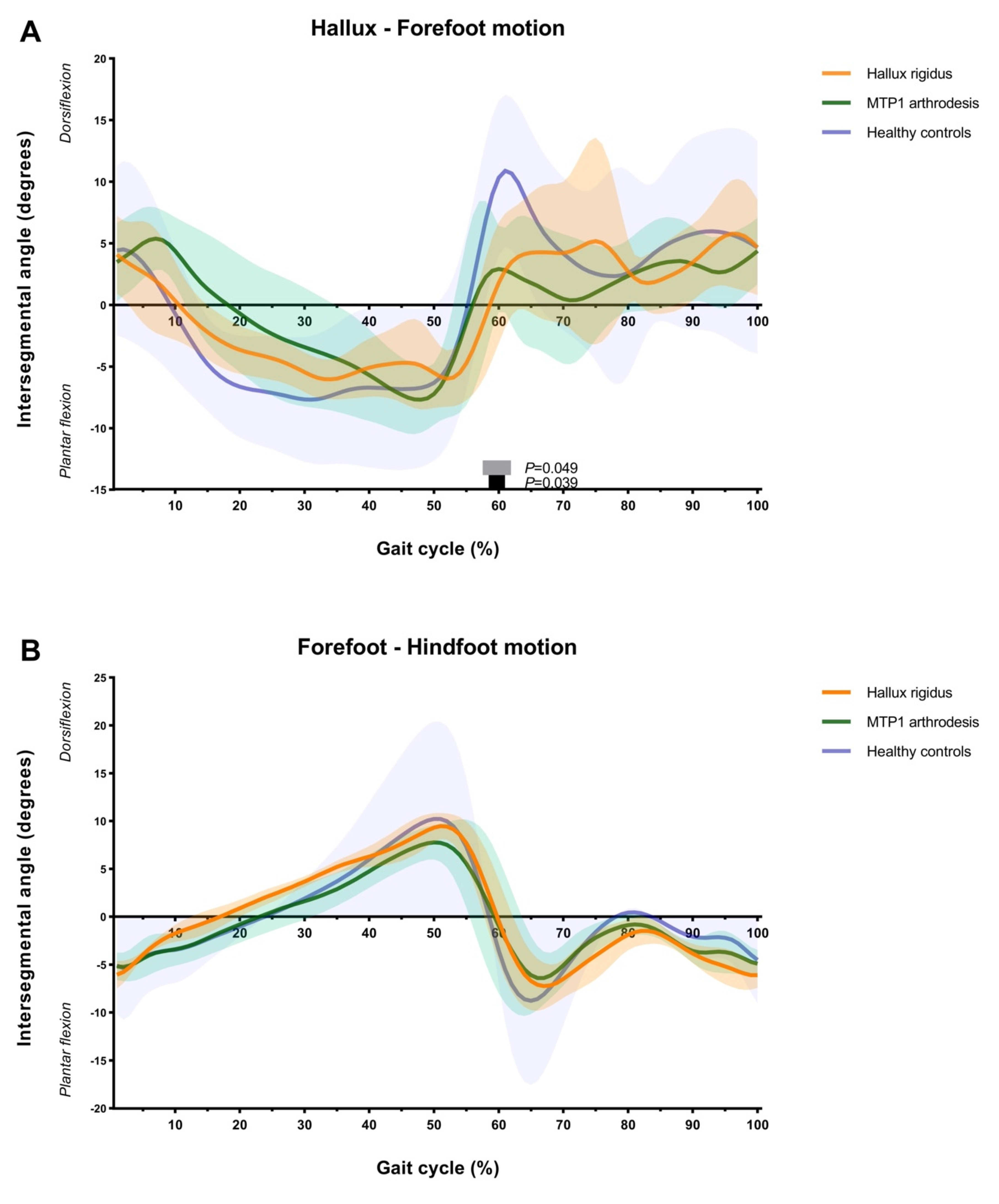
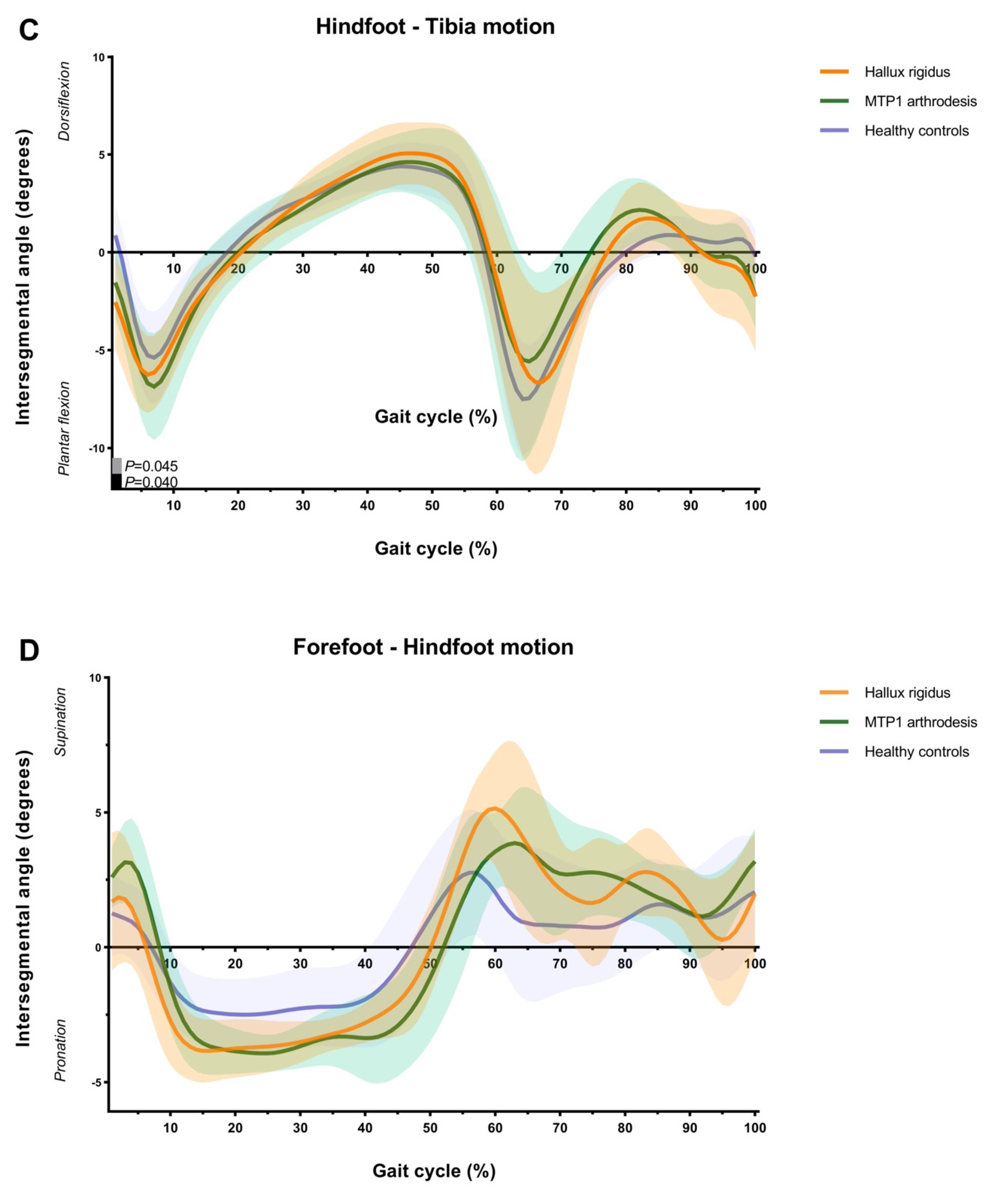
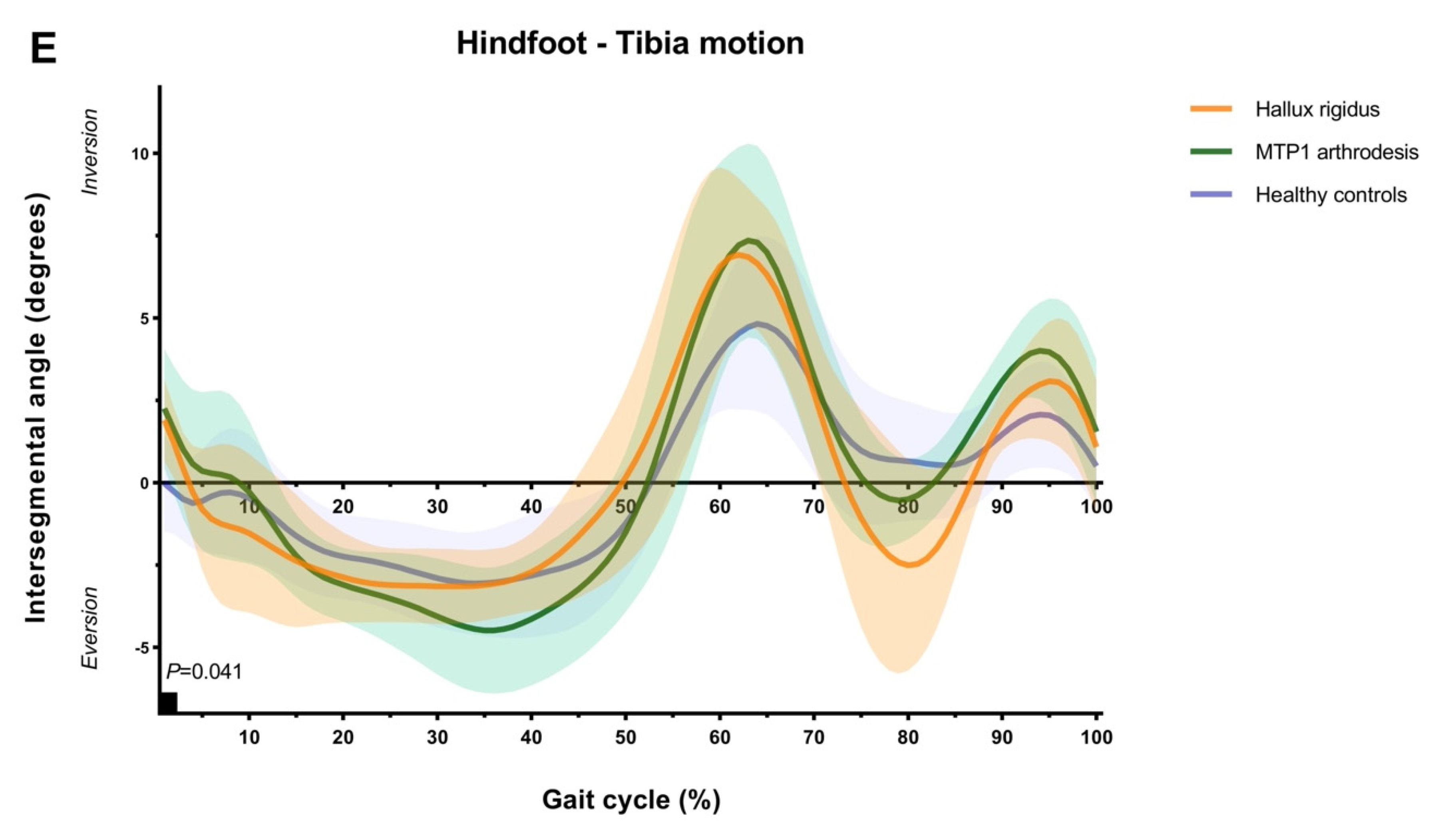
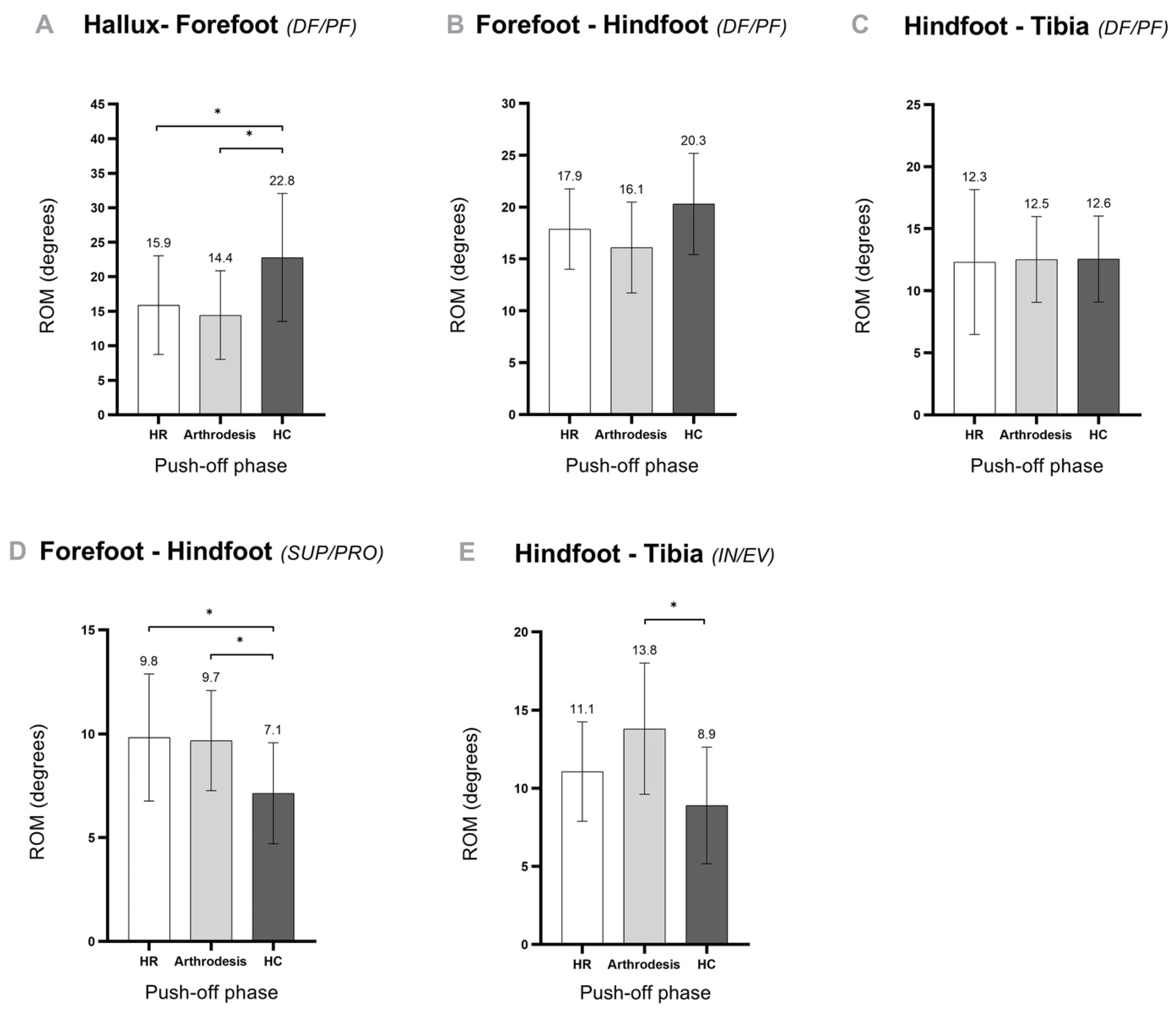
3.3. Foot and Ankle Kinematics
3.4. PROMs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AOFAS-HMI | American Orthopedic Foot and Ankle Society (AOFAS) rating system for the Hallux Metatarsophalangeal-Interphalangeal (HMI) scale |
| DF | dorsiflexion |
| EV | eversion |
| HC | healthy controls |
| HR | hallux rigidus |
| IN | inversion |
| MOXFQ | Manchester–Oxford Foot Questionnaire |
| MTP1 | first metatarsophalangeal joint |
| NPRS | Numeric Pain Rating Scale |
| OFM | Oxford foot model |
| PF | plantar flexion |
| PRO | pronation |
| ROM | range of motion |
| SUP | supination |
| T1 | first toe |
| T2-T5 | second to fifth toe |
References
- Ho, B.; Baumhauer, J. Hallux rigidus. EFORT Open Rev. 2017, 2, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Keiserman, L.S.; Sammarco, V.J.; Sammarco, G.J. Surgical treatment of the hallux rigidus. Foot Ankle Clin. 2005, 10, 75–96. [Google Scholar] [CrossRef] [PubMed]
- Galois, L.; Girard, D.; Martinet, N.; Delagoutte, J.P.; Mainard, D. Optoelectronic gait analysis after metatarsophalangeal arthrodesis of the hallux: Fifteen cases. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2006, 92, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Roddy, E.; Menz, H.B. Foot osteoarthritis: Latest evidence and developments. Ther. Adv. Musculoskelet. Dis. 2018, 10, 91–103. [Google Scholar] [CrossRef]
- Kumar, S.; Pradhan, R.; Rosenfeld, P.F. First metatarsophalangeal arthrodesis using a dorsal plate and a compression screw. Foot Ankle Int. 2010, 31, 797–801. [Google Scholar] [CrossRef]
- Stevens, J.; de Bot, R.; Hermus, J.P.S.; van Rhijn, L.W.; Witlox, A.M. Clinical outcome following total joint replacement and arthrodesis for hallux rigidus: A systematic review. JBJS Rev. 2017, 5, e2. [Google Scholar] [CrossRef]
- Stevens, J.; de Bot, R.; Witlox, A.M.; Borghans, R.; Smeets, T.; Beertema, W.; Hendrickx, R.P.; Schotanus, M.G.M. Long-term effects of cheilectomy, Keller’s arthroplasty, and arthrodesis for symptomatic hallux rigidus on patient-reported and radiologic outcome. Foot Ankle Int. 2020, 41, 775–783. [Google Scholar] [CrossRef]
- Brodsky, J.W.; Baum, B.S.; Pollo, F.E.; Mehta, H. Prospective gait analysis in patients with first metatarsophalangeal joint arthrodesis for hallux rigidus. Foot Ankle Int. 2007, 28, 162–165. [Google Scholar] [CrossRef]
- DeFrino, P.F.; Brodsky, J.W.; Pollo, F.E.; Crenshaw, S.J.; Beischer, A.D. First metatarsophalangeal arthrodesis: A clinical, pedobarographic and gait analysis study. Foot Ankle Int. 2002, 23, 496–502. [Google Scholar] [CrossRef]
- Stevens, J.; Meijer, K.; Bijnens, W.; Fuchs, M.C.; van Rhijn, L.W.; Hermus, J.P.; van Hoeve, S.; Poeze, M.; Witlox, A.M. Gait Analysis of foot compensation after arthrodesis of the first metatarsophalangeal joint. Foot Ankle Int. 2017, 38, 181–191. [Google Scholar] [CrossRef]
- Rajan, R.; Mishra, A. A systematic review of total arthroplasty and arthrodesis for end-stage hallux rigidus: A biomechanical perspective. Foot 2021, 49, 101838. [Google Scholar] [CrossRef] [PubMed]
- Van Gheluwe, B.; Dananberg, H.J.; Hagman, F.; Vanstaen, K. Effects of hallux limitus on plantar foot pressure and foot kinematics during walking. J. Am. Podiatr. Med. Assoc. 2006, 96, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Shereff, M.J.; Baumhauer, J.F. Hallux rigidus and osteoarthrosis of the first metatarsophalangeal joint. J. Bone Jt. Surg. Am. 1998, 80, 898–908. [Google Scholar] [CrossRef] [PubMed]
- Miana, A.; Paola, M.; Duarte, M.; Nery, C.; Freitas, M. Gait and Balance Biomechanical Characteristics of Patients With Grades III and IV Hallux Rigidus. J. Foot Ankle Surg. 2022, 61, 452–455. [Google Scholar] [CrossRef]
- Kuni, B.; Wolf, S.I.; Zeifang, F.; Thomsen, M. Foot kinematics in walking on a level surface and on stairs in patients with hallux rigidus before and after cheilectomy. J. Foot Ankle Res. 2014, 7, 13. [Google Scholar] [CrossRef]
- Stevens, J.; de Bot, R.; Hermus, J.P.S.; Schotanus, M.G.M.; Meijer, K.; Witlox, A.M. Gait analysis of foot compensation in symptomatic Hallux Rigidus patients. Foot Ankle Surg. 2022, 28, 1272–1278. [Google Scholar] [CrossRef]
- Picouleau, A.; Orsoni, N.; Hardy, J.; Mabit, C.; Charissoux, J.L.; Marcheix, P.S. Analysis of the effects of arthrodesis of the hallux metatarsophalangeal joint on gait cycle: Results of a GAITRite((R)) treadmill test. Int. Orthop. 2020, 44, 2167–2176. [Google Scholar] [CrossRef]
- Rajan, R.A.; Kerr, M.; Hafesji-Wade, A.; Osler, C.J.; Outram, T. A prospective clinical and biomechanical analysis of feet following first metatarsophalangeal joint arthrodesis for end stage hallux rigidus. Gait Posture 2024, 109, 208–212. [Google Scholar] [CrossRef]
- Wright, C.J.; Arnold, B.L.; Coffey, T.G.; Pidcoe, P.E. Repeatability of the modified Oxford foot model during gait in healthy adults. Gait Posture 2011, 33, 108–112. [Google Scholar] [CrossRef]
- Carson, M.C.; Harrington, M.E.; Thompson, N.; O’Connor, J.J.; Theologis, T.N. Kinematic analysis of a multi-segment foot model for research and clinical applications: A repeatability analysis. J. Biomech. 2001, 34, 1299–1307. [Google Scholar] [CrossRef]
- Perry, J.; Burnfield, J. Gait Analysis: Normal and Pathological Function; Slack Incorporated: West Deptford, NJ, USA, 2010. [Google Scholar]
- Ibrahim, T.; Beiri, A.; Azzabi, M.; Best, A.J.; Taylor, G.J.; Menon, D.K. Reliability and validity of the subjective component of the American Orthopaedic Foot and Ankle Society clinical rating scales. J. Foot Ankle Surg. 2007, 46, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Kitaoka, H.B.; Alexander, I.J.; Adelaar, R.S.; Nunley, J.A.; Myerson, M.S.; Sanders, M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994, 15, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Morley, D.; Jenkinson, C.; Doll, H.; Lavis, G.; Sharp, R.; Cooke, P.; Dawson, J. The Manchester-Oxford Foot Questionnaire (MOXFQ): Development and validation of a summary index score. Bone Jt. Res. 2013, 2, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.; Coffey, J.; Doll, H.; Lavis, G.; Cooke, P.; Herron, M.; Jenkinson, C. A patient-based questionnaire to assess outcomes of foot surgery: Validation in the context of surgery for hallux valgus. Qual. Life Res. 2006, 15, 1211–1222. [Google Scholar] [CrossRef]
- Budiman-Mak, E.; Conrad, K.J.; Roach, K.E. The Foot Function Index: A measure of foot pain and disability. J. Clin. Epidemiol. 1991, 44, 561–570. [Google Scholar] [CrossRef]
- Downie, W.W.; Leatham, P.A.; Rhind, V.M.; Wright, V.; Branco, J.A.; Anderson, J.A. Studies with pain rating scales. Ann. Rheum. Dis. 1978, 37, 378–381. [Google Scholar] [CrossRef]
- Regnauld, B. Disorders of the Great Toe; Springer: Berlin/Heidelberg, Germany, 1986; pp. 345–359. [Google Scholar]
- Coughlin, M.J. Rheumatoid forefoot reconstruction—A long-term follow-up study. J. Bone Jt. Surg.-Am. Vol. 2000, 82a, 322–341. [Google Scholar] [CrossRef]
- Pataky, T.C. Generalized n-dimensional biomechanical field analysis using statistical parametric mapping. J. Biomech. 2010, 43, 1976–1982. [Google Scholar] [CrossRef]
- Murray, M.P.; Kory, R.C.; Clarkson, B.H.; Sepic, S.B. Comparison of free and fast speed walking patterns of normal men. Am. J. Phys. Med. 1966, 45, 8–23. [Google Scholar] [CrossRef]
- Fukuchi, C.A.; Fukuchi, R.K.; Duarte, M. Effects of walking speed on gait biomechanics in healthy participants: A systematic review and meta-analysis. Syst. Rev. 2019, 8, 153. [Google Scholar] [CrossRef]
- Canseco, K.; Long, J.; Marks, R.; Khazzam, M.; Harris, G. Quantitative characterization of gait kinematics in patients with hallux rigidus using the Milwaukee foot model. J. Orthop. Res. 2008, 26, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Beertema, W.; Draijer, W.F.; van Os, J.J.; Pilot, P. A retrospective analysis of surgical treatment in patients with symptomatic hallux rigidus: Long-term follow-up. J. Foot Ankle Surg. 2006, 45, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Voskuijl, T.; Onstenk, R. Operative Treatment for Osteoarthritis of the First Metatarsophalangeal Joint: Arthrodesis Versus Hemiarthroplasty. J. Foot Ankle Surg. 2015, 54, 1085–1088. [Google Scholar] [CrossRef] [PubMed]
- Erdil, M.; Elmadag, N.M.; Polat, G.; Tuncer, N.; Bilsel, K.; Ucan, V.; Erkocak, O.F.; Sen, C. Comparison of arthrodesis, resurfacing hemiarthroplasty, and total joint replacement in the treatment of advanced hallux rigidus. J. Foot Ankle Surg. 2013, 52, 588–593. [Google Scholar] [CrossRef]
- Chraim, M.; Bock, P.; Alrabai, H.M.; Trnka, H.J. Long-term outcome of first metatarsophalangeal joint fusion in the treatment of severe hallux rigidus. Int. Orthop. 2016, 40, 2401–2408. [Google Scholar] [CrossRef]
- de Bot, R.; Veldman, H.D.; Eurlings, R.; Stevens, J.; Hermus, J.P.S.; Witlox, A.M. Metallic hemiarthroplasty or arthrodesis of the first metatarsophalangeal joint as treatment for hallux rigidus: A systematic review and meta-analysis. Foot Ankle Surg. 2022, 28, 139–152. [Google Scholar] [CrossRef]
- Schneider, W.; Jurenitsch, S. Normative data for the American Orthopedic Foot and Ankle Society ankle-hindfoot, midfoot, hallux and lesser toes clinical rating system. Int. Orthop. 2016, 40, 301–306. [Google Scholar] [CrossRef]
- van Hoeve, S.; Vos, J.; Weijers, P.; Verbruggen, J.; Willems, P.; Poeze, M.; Meijer, K. Repeatability of the Oxford Foot Model for Kinematic Gait Analysis of the Foot and Ankle. Clin. Res. Foot Ankle 2015, 3, 1–8. [Google Scholar]
- Schallig, W.; van den Noort, J.C.; McCahill, J.; Stebbins, J.; Leardini, A.; Maas, M.; Harlaar, J.; van der Krogt, M.M. Comparing the kinematic output of the Oxford and Rizzoli Foot Models during normal gait and voluntary pathological gait in healthy adults. Gait Posture 2020, 82, 126–132. [Google Scholar] [CrossRef]
- Schallig, W.; van den Noort, J.C.; Piening, M.; Streekstra, G.J.; Maas, M.; van der Krogt, M.M.; Harlaar, J. The Amsterdam Foot Model: A clinically informed multi-segment foot model developed to minimize measurement errors in foot kinematics. J. Foot Ankle Res. 2022, 15, 46. [Google Scholar] [CrossRef]
- Aarts, S.; van den Akker, M.; Winkens, B. The importance of effect sizes. Eur. J. Gen. Pract. 2014, 20, 61–64. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HR | Healthy Controls | p-Value b | |
|---|---|---|---|
| Number of participants (number of feet) | 10 (10) | 15 (30) | - |
| Male/female | 3:7 | 9:6 | - |
| Left/right feet | 3:7 | 15:15 | - |
| Age (y) | 65 ± 9.5 (52–79) | 59 ± 5.0 (53–70) | 0.16 |
| Height (m) | 1.66 ± 0.09 | 1.74 ± 0.09 | 0.04 |
| Weight (kg) | 72.8 ± 14.7 | 83.0 ± 11.9 | 0.06 |
| BMI | 26.2 ± 4.3 (20.4–33.2) | 27.4 ± 3.9 (20.2–33.3) | 0.37 |
| Leg length (cm) | 89.0 ± 5.0 (82–98) | 91.6 ± 4.9 (84–104) | 0.21 |
| Preoperative HR grade c | II = 7, III = 3 | ||
| Postoperative DFA | 25.0 ± 5.66 (19.0–38.0) |
| HR (1) | MTP1 Arthrodesis (2) | Healthy Controls (3) | p-Value | p-Value b | p-Value b | |
|---|---|---|---|---|---|---|
| 1–2 | 1–3 | 2–3 | ||||
| Gait speed (m/s) | 1.01 ± 0.19 | 1.07 ± 0.29 | 1.14 ± 0.19 | 0.30 | 0.09 | 0.65 |
| Step width (m) | 0.12 ± 0.05 | 0.10 ± 0.04 | 0.13 ± 0.04 | 0.27 | 0.64 | 0.05 |
| Step length (m) | 0.56 ± 0.02 | 0.60 ± 0.09 | 0.64 ± 0.07 | 0.21 | 0.002 | 0.33 |
| Stance time (s) | 0.71 ± 0.10 | 0.75 ± 0.13 | 0.71 ± 0.11 | 0.11 | 0.85 | 0.71 |
| HR | MTP1 Arthrodesis | p-Value b | |
|---|---|---|---|
| AOFAS-HMI score c | 55.7 ± 8.7 (42–70) | 79.1 ± 15.5 (52.2–100) | 0.002 |
| NPRS | 5.7 ± 2.5 (1–8) | 1.5 ± 1.8 (0–5) | 0.004 |
| MOXFQ | 51.0 ± 15.6 (22.5–78.8) | 20.0 ± 13.5 (0–43) | 0.002 |
| Standing or walking (%) | 43.1 ± 23.9 (5.7–80) | 19.1 ± 15.5 (0–45.6) | 0.027 |
| Pain (%) | 53.2 ± 14.9 (20–76) | 25.6 ± 18.8 (0–64) | 0.004 |
| Social interactions (%) | 50.8 ± 8.2 (40–64) | 28.0 ± 17.0 (0–44) | 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Bot, R.T.A.L.; Stevens, J.; Staal, H.M.; Meijer, K.; Witlox, A.M. A Prospective Study Evaluating Gait and Clinical Outcome Following First Metatarsophalangeal Arthrodesis for Hallux Rigidus. Biomechanics 2025, 5, 46. https://doi.org/10.3390/biomechanics5030046
de Bot RTAL, Stevens J, Staal HM, Meijer K, Witlox AM. A Prospective Study Evaluating Gait and Clinical Outcome Following First Metatarsophalangeal Arthrodesis for Hallux Rigidus. Biomechanics. 2025; 5(3):46. https://doi.org/10.3390/biomechanics5030046
Chicago/Turabian Stylede Bot, Robin T. A. L., Jasper Stevens, Heleen M. Staal, Kenneth Meijer, and Adhiambo M. Witlox. 2025. "A Prospective Study Evaluating Gait and Clinical Outcome Following First Metatarsophalangeal Arthrodesis for Hallux Rigidus" Biomechanics 5, no. 3: 46. https://doi.org/10.3390/biomechanics5030046
APA Stylede Bot, R. T. A. L., Stevens, J., Staal, H. M., Meijer, K., & Witlox, A. M. (2025). A Prospective Study Evaluating Gait and Clinical Outcome Following First Metatarsophalangeal Arthrodesis for Hallux Rigidus. Biomechanics, 5(3), 46. https://doi.org/10.3390/biomechanics5030046