1. Introduction
Hip extension to the appropriate extent (conditionally called the kinematic aspect) and quality (conditionally called the neuro-muscular aspect) is an important aspect of sports performance and numerous activities of everyday life [
1]. Therefore, any deficit in the mentioned movement types, kinematic and/or neuromuscular, changes the biomechanics of walking and running and, in a broader sense, dynamic posture, leading to an increased load on individual segments of the movement system. Several studies [
2,
3,
4] state that structural freedom, as well as neuromuscular control of the performance of the full range of motion in the hip joint, is important for reducing the load on the spine. Insufficient hip extension may be associated with tightness in the hip flexor muscles [
1]. Flexibility deficits of the hip flexors have been identified as potential risk factors for hamstring injuries [
5]. Mills et al. [
6] found that athletes with restricted hip flexor muscle length demonstrate significantly less gluteus maximus activation, followed by compensatory greater levels of relative hamstring co-activation, whereby hamstring muscle fatigue may allow for increased ACL loading and injury in those with hip flexor muscle tightness. The aforementioned issue creates the possibility of thinking that the optimal length–tension ratio of the hip flexor muscles, both monoarticular and biarticular, could be an important factor regarding the approach to ACL and hamstring injury prevention.
The modified Thomas test is frequently used to assess the flexibility of the hip flexor muscles; however, in practice, this test is usually subjective since, being based on observation, the results are reported dichotomously, either as positive or negative in relation to norms [
7]. The modified Thomas test quantification most often involves 2D goniometric and trigonometric methods [
8].
A modified Thomas test has already been used as an intervention for the gravity stretching of the hip flexor muscles [
9]. In such cases, it is usually performed once for 2 min, with the assessment of immediate effects only. As Lobel [
10] states, most studies that compare different types of stretching techniques use intervention periods of 1 day or 1 week at most. However, an interesting question remains as to whether such an intervention could have some prolonged (or merely postponed) effects on the flexibility of the muscles involved. This may not be so far-fetched a hypothesis as it would appear at first glance. To draw a comparison, perhaps, to muscle soreness due to acute overexertion, what we typically see, especially in untrained people, is that after an incident of overexertion (say, working out or playing sports too vigorously on an occasion), a clinical condition known as delayed-onset muscle soreness (DOMS) emerges, where peak muscle soreness occurs 48–72 h after exercise [
11], and then gradually subsides. Such an effect could also reasonably appear with muscle relaxation, i.e., stretching.
The objective of this study, therefore, was to determine whether a single application of gravity stretching in the position of the modified Thomas test could lead to a significant acute increase in the flexibility of the hip flexor muscles, which would be manifested by an increase in the hip extension range of motion, but also to check whether this potential improvement would be maintained 48 h after the intervention.
2. Materials and Methods
2.1. Participants
The present sample comprised 14 volunteers (8 women, 6 men). These were students with an average age of 22.35 ± 1.82 years, ranging from 20 to 26 years old. The mean participant height was 170.15 ± 10.04 cm, while the average weight was 74.84 ± 20.03 kg, with BMI values of 25.48 ± 4.32 kg/m2.
The inclusion criteria were an age between 18 and 30 years, being healthy, and the absence of an injury in the trunk, pelvis, and lower limbs in the last six months.
The exclusion criteria were neuromuscular diseases, musculoskeletal deformities, lumbo–pelvic–hip complex or lower extremity injuries in the last six months that could potentially interfere with the test results, pain when performing the test, and professional athlete status. The volunteers who applied to participate in this study met all the inclusion criteria. Applying the International Physical Activity Questionnaire (IPAQ) [
12], a moderate level of physical activity was determined in the sample.
Prior to the start of the testing, all participants provided written informed consent, and the protocol for this study was approved by the Faculty’s Science and Ethics Committee (decision no: 19/17). The participants were informed about the procedure and the use of the results for research purposes, including their presentation exclusively at the level of the group and the lack of individual results. Participants had the option to withdraw from the research at any time.
2.2. Procedure
Measurements and interventions were performed and controlled by one examiner, the author of this paper. Statistical processing was performed by another expert, also the author of this paper, who was blinded to the measurement and intervention protocol.
The subjects’ height and weight were measured using the measuring station (Seca GmbH & Co. KG., Hamburg, Germany). The kinematic data of the modified Thomas test performance of the dominant upper leg (i.e., evaluation of passive hip extension and knee flexion peak angles) were recorded using a camera with HD resolution (Canon EOS 550D, with a sampling frequency of 30 Hz, along with the Canon EF-S 15–85 mm lens set to focal length f = 50 mm to avoid the fish-eye effect). The camera was oriented perpendicular to the test table, with the central focus on the point where latero-lateral axis extends, around which the sagittal hip movements occur. The dominant leg was defined as the leg with which the participant stepped onto the measuring station. Passive markers were used. For that, we used self-adhesive circular white stickers with 1 cm diameters and a black dot in the center. We placed them on four prominent anatomical points: the acromion, the lateral epicondyle of the femur, the fibular head, and the lateral malleolus.
The participants were given instructions [
11,
13] for performing the test and were positioned. In order to determine realistic indicators of daily life activities, no warm-up was performed prior to the testing.
Modified Thomas Test
The extent of or deficit in hip extension and the knee flexion range of motion was measured to indirectly assess the flexibility of the hip flexors. For the aforementioned assessment, we used the modified Thomas test, a standardized [
1,
13] observational clinical test of the kinematics of the lower extremities (i.e., it is commonly used to assess passive hip extension and the knee flexion range of motion), which indirectly provides information on the flexibility of the hip and knee musculature, mainly the one-joint iliopsoas muscle along with the two-joint hip muscles (
m. rectus femoris,
m. tensor fasciae latae, and
m. sartorius). In clinical practice, the test is most often evaluated dichotomously, since based on the observation it is pass/fail test, interpreted as negative or positive, in relation to the norms [
14,
15,
16]. The quantification of the modified Thomas test most often includes goniometric [
7,
8,
13,
17,
18,
19] and trigonometric [
8,
20] methods and the digital photography method [
1,
21,
22]. Here, we also mention two attempts [
23,
24] of kinematic analysis of modified Thomas tests using a 3D automated optoelectronic system. Two-dimensional goniometry is considered the gold standard and is performed using a goniometer or inclinometer [
25]. In this research, measurements were taken using the Kinovea goniometer—a digital tool of the Kinovea computer program (Kinovea 0.8.27 software 2018), an open-source video recording, measurement, and annotation tool designed for motion analysis.
Subjects were positioned for the modified Thomas test and were given instructions for performing the test according to a protocol based on information from the relevant literature [
9,
13,
14,
15,
16,
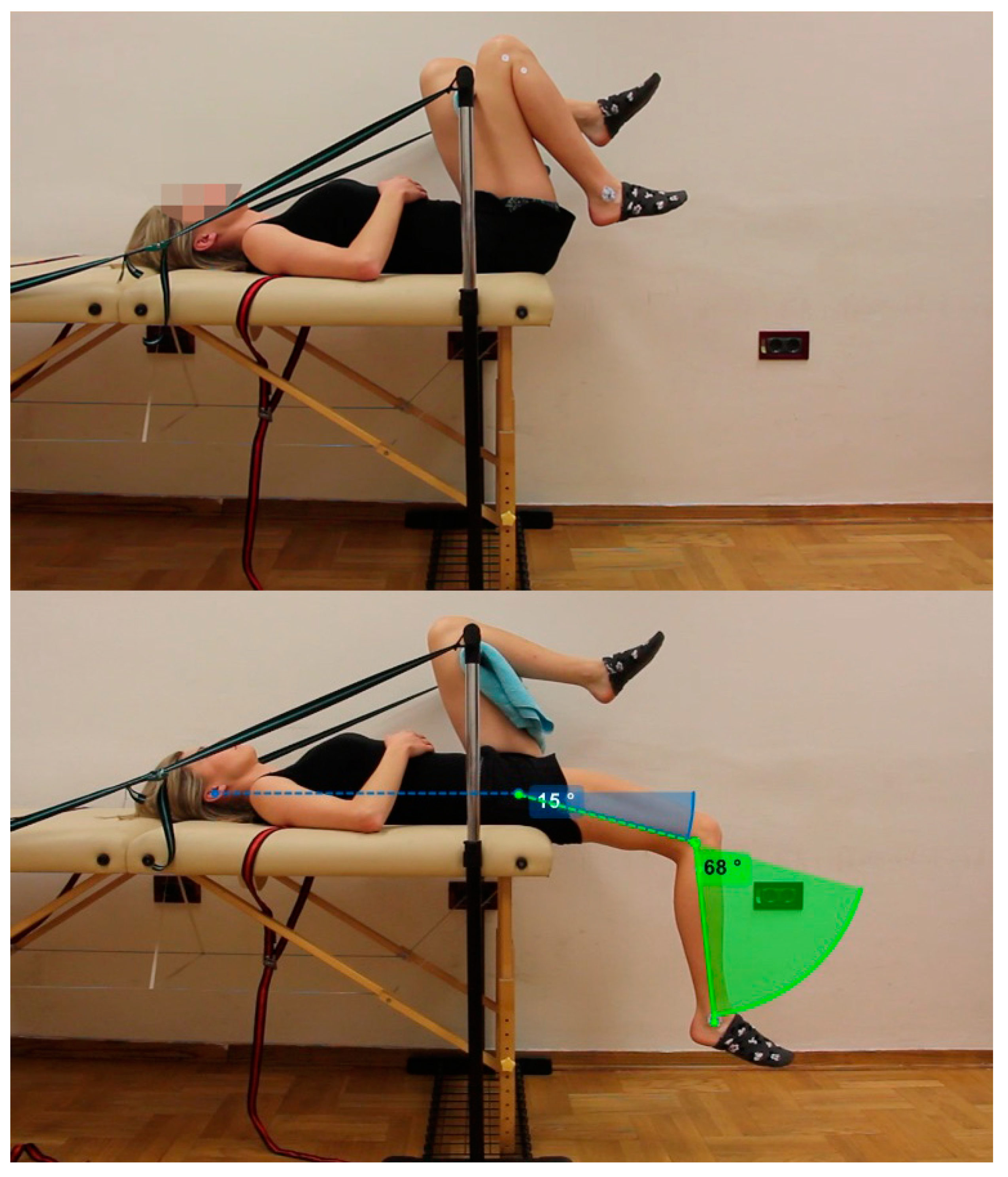
23]: the person lies in a supine position on the table, with the pelvis on the lower edge of the table, and keeps both upper legs flexed at the hips. This positioning ensures that the lumbar spine is leaning against the table, i.e., that the lumbar lordosis is aligned, with the pelvis in a posterior tilt. With a specially created adjustable (i.e., suitable for different leg lengths) construction, including a crossbar covered with a towel, the stabilization of the hip region of the untested upper leg was standardized to 120° of flexion, which ensured a flat back and the relaxation of the non-tested segments (
Figure 1). In this way, we created passive stabilization of the non-tested leg (along with its relaxation) and avoided the effect of trunk muscle co-contraction for active pelvic stabilization, as discussed by Vigotsky et al. [
1]. Pelvic stabilization was thus maintained throughout the entire modified Thomas test performance, with the prevention of its anterior tilt, which could be misinterpreted as additional hip extension range of motion. After assuming the initial position, each subject was guided to take a deep breath and, along with exhalation, allow gravity to lead to the gradual movement (i.e., hip extension) of the examined (i.e., dominant) limb.
Measurements were performed at three points: baseline, immediately after the intervention (3 min gravity stretching, through the relaxation of the participant in the modified Thomas test position, where they lie completely relaxed and allow gravity to stretch the flexor muscles of the tested limb), and 48 h after the intervention. The endpoint of the initial modified Thomas test assessment was simultaneously assigned as the starting point of the modified Thomas test intervention. A standard intervention for increasing flexibility and mobility was applied—(gravity) stretching. The intervention principles are that each participant lay completely relaxed in the modified Thomas test position for 180 s, allowing gravity to stretch the hip flexor muscles of the tested leg, as described in detail in [
9]. The endpoint of the modified Thomas test intervention was the same time as the first post-intervention measurement. We set the duration of gravity stretching according to the work of Taylor et al. [
26], Bolčević et al. [
9], and Lobel [
12], who performed 120 s stretching sessions, and we added 1 minute more for a total of 180 s since we wanted to extend the duration of the intervention by 50% compared to the longest single interventions that we, to the best of our ability, found in the literature. It seemed too ambitious to us to double that duration or attempt even more.
All tests and interventions were performed in the Faculty’s Physiology Laboratory, at the same time of day, to control, as Lobel [
12] states, the temporal flexibility changes. The participants visited the laboratory in two sessions, with an interval of 48 h between visits. The subjects were required to be completely rested for the measurements, which meant a minimum of 12 h without any intense physical activity before the initial tests, but also for the next 48 h until the end of the final measurements, in order to minimize the influence of external factors. For this purpose, the participants were additionally asked not to engage in any unusual activities or exercises in the period between measurements.
2.3. Data Analysis
Kinematic data on hip and knee range of motion during the modified Thomas test were determined by 2D quantitative kinematic analysis of video recordings, which was performed using Kinovea motion analysis software. The video recording of the modified Thomas test performance was uploaded using the Kinovea software, where it was played and stopped at the endpoint of the hip extension and knee flexion. The angles were measured using the Kinovea goniometer tool (see
Figure 1). The marker on the acromion is not visible when viewed from the sagittal plane. Therefore, we decided to use the
porus acusticus externus as an orientation point, especially because the line that forms the hip angle also passes through the acromion process in this testing position.
2.4. Statistical Analysis
The data were analyzed using SPSS software, version 22 (SPSS Inc., Chicago, IL, USA). The data were processed via the methods of descriptive and inferential statistics. Since the distribution showed deviation from normality, we decided to apply non-parametric statistical procedures. Therefore, for data processing, the Friedman test and the Wilcoxon signed-rank test were used. Statistical significance was set at the level of p ≤ 0.05.
3. Results
All participants completed the study, and there were no subject withdrawals or errors in data acquisition.
The main descriptive results of goniometry for the modified Thomas test for the three timepoints are presented in
Figure 2 and
Figure 3.
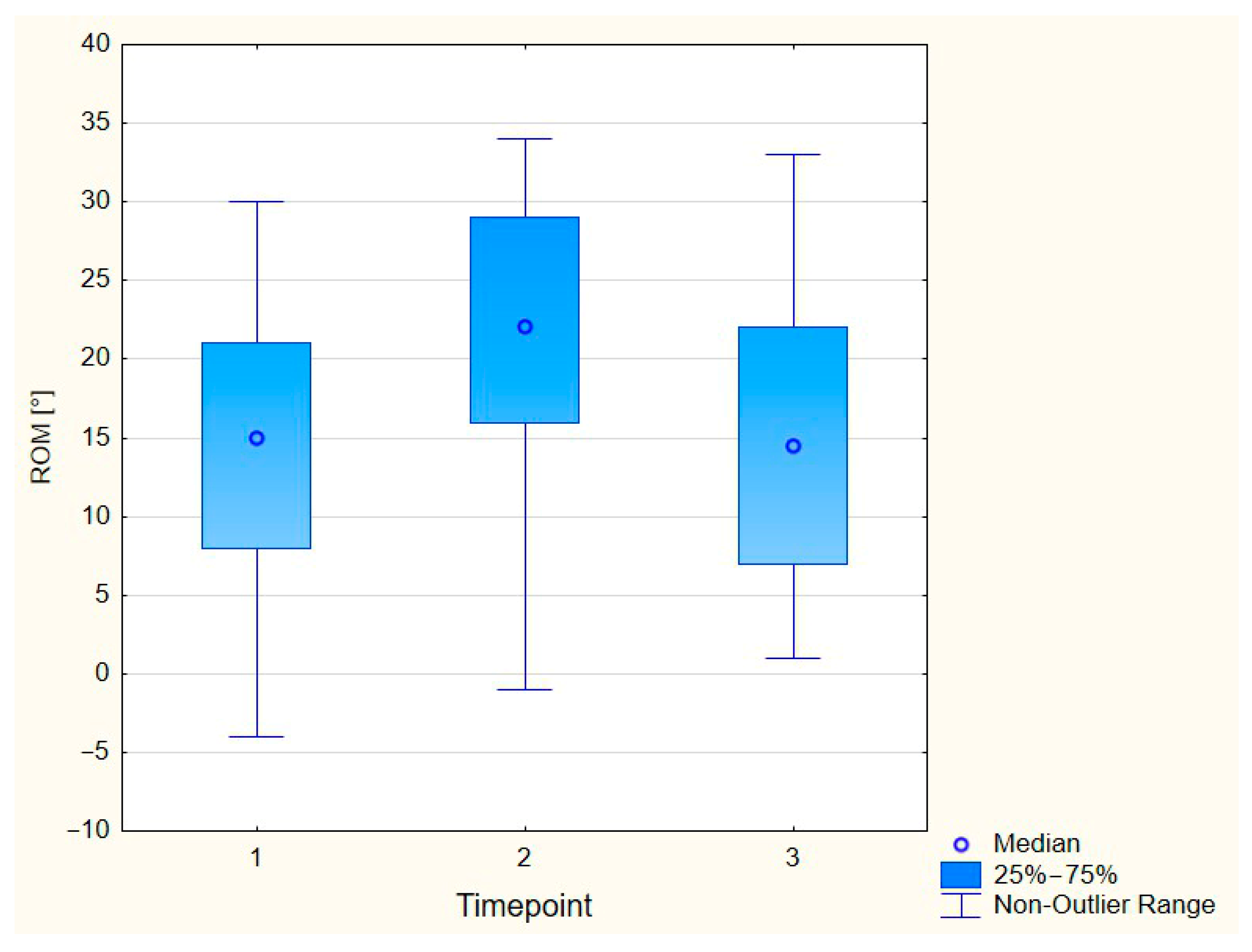
For the hip joint (see
Figure 2), at the first measurement point, the subjects showed an average extension range of motion of 14.85° ± 9.18°. The median was close to the mean value at 15°, with a range from −4° to 30°. The average range of motion at the second measurement point was 21.07° ± 9.67°, while the median was 22° (ranging from −1° to 34°). The median of the extension range of motion at the third measurement point was 14.5° (range 1° to 33°), with a mean value of 15.28° with almost the same variability; the standard deviation was 9.68°.
The Friedman test showed that the difference between the 3 measurement points was statistically significant (p < 0.001), with higher hip extension range of motion values at the second measurement point compared to the other timepoints (using the Wilcoxon signed-rank test for post hoc analysis). The difference between the baseline range of motion and the 48 h post-intervention range of motion was not significant.
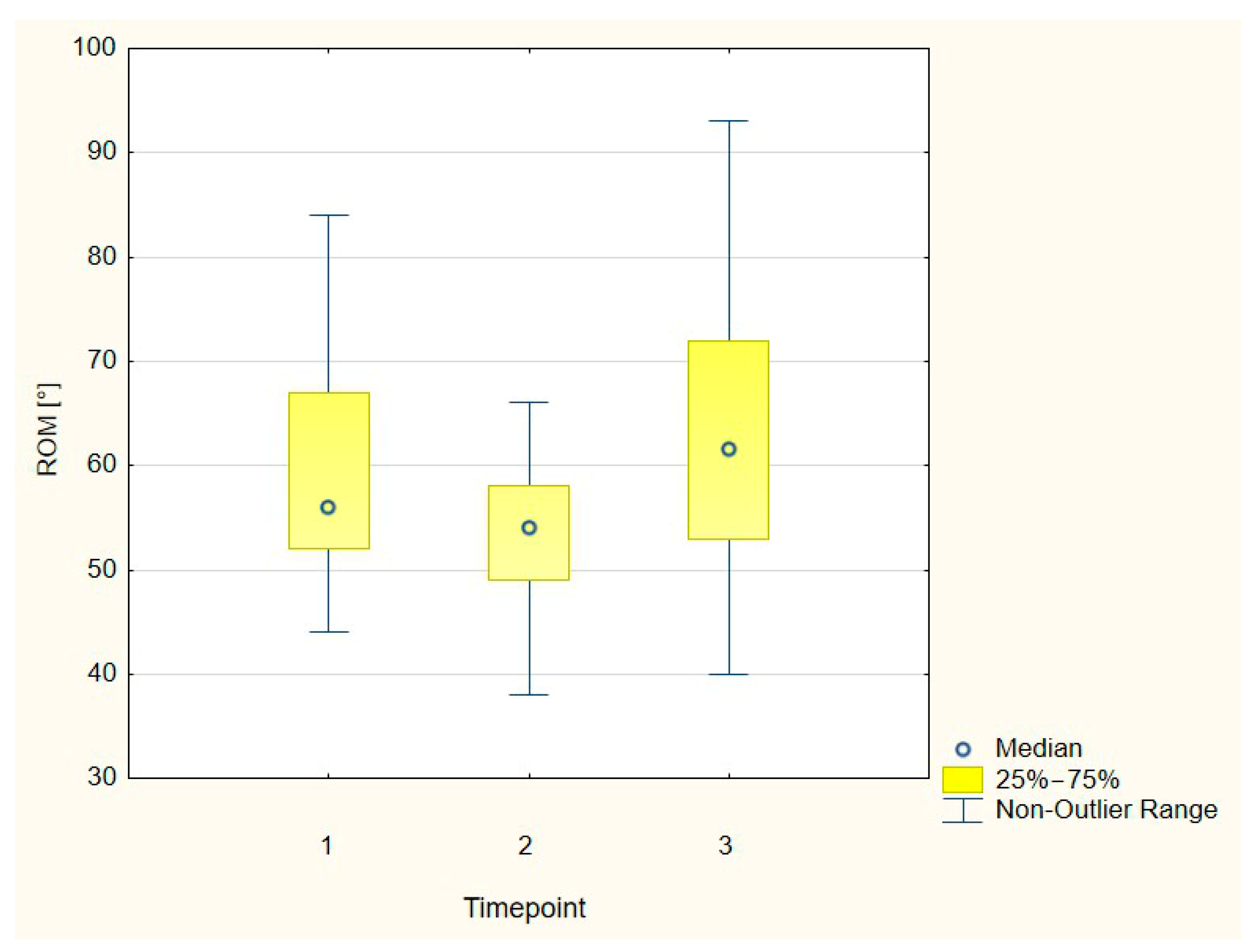
For the knee joint (see
Figure 3), at the first measurement point, the subjects showed an average flexion range of motion of 58.35° ± 11.31°. The median was close to the mean value at 56°, with a range from 44° to 84°. The average range of motion at the second measurement point was 52.92° ± 7.71°, while the median was 54° (ranging from 38° to 66°). The median of the extension range of motion at the third measurement point was 61.5° (range 40° to 93°), with a mean value of 62.07° and a standard deviation of 13.88°.
The Friedman test showed that the difference between the 3 measurement points was statistically significant (p < 0.001), with lower knee flexion range of motion values at the second measurement point, compared to the other timepoints (using Wilcoxon signed-rank test for post hoc assessment). The difference between the baseline range of motion and the 48 h post-intervention range of motion was not significant.
4. Discussion
The purpose of this study was to determine the effects of a single 3 min gravity stretching procedure (i.e., in the position of the modified Thomas test) on the flexibility of monoarticular and biarticular hip flexors (measured by using the modified Thomas test) at two timepoints (immediately after intervention and 48 h after intervention).
Acutely, in our study, there was a significant increase in the hip extension range of motion (6.2° on average, and having crossed a mean value of 21°), which corresponds to the significant post-2 min modified Thomas test gravity stretching range of motion improvement of 4.9° in the research on 54 young, physically active males [
9]. Our results are even more in accordance with the research by Curry et al. [
27], where static stretching by 24 female participants was performed for 10 min (3 × 12 s) with a 12 s break each minute, resulting in a 6.5° increase in hip extension range of motion. We also found a significant immediate decrease in the knee flexion range of motion (5.4° on average), which was greater compared to that [
9], where the knee range of motion also decreased (and this change was also significant), for an average of 2.1°.
However, our results show that after 48 h, hip extension and knee flexion ranges of motion changed significantly again, but now in a negative direction, returning to approximately the original level, with an average value that did not differ significantly from the pre-intervention values. The return of the ranges of motion after 48 h to near their initial levels indicates the absence of a prolonged effect of a single stretch of the hip flexors.
It seems that, for long-term improvement of flexibility, it is necessary to select and implement another intervention protocol or modality that will lead to a prolonged increase in the range of motion.
Our results relating to hip extension range of motion prior to the intervention (a mean of 14.85° with a standard deviation of 9.18°) align with those of the relevant literature, suggesting that a “normal” hip extension range of motion ranges between 10 and 15° [
15,
16]. The initial hip range of motion values in our study are also comparable to the results obtained by Harvey [
13], at 11.9° ± 5.5°; Ferber et al. [
18], at 10.6° ± 9.6°; Kiseljak et al. [
23], at 10° ± 10°; and Neves et al. [
28], at 12° ± 10° (males) and 9° ± 9° (females). These authors used a similar positioning of the subjects, but with a different stabilization of the non-tested leg, with the subject passively holding the lower leg in a maximally flexed position [
13,
18,
28], or with 120° flexion while passively holding the non-tested leg using an immobilizer strap that the subjects held with their hands [
23], preventing the complete relaxation of the untested segments. Kim and Ha [
21] point out the importance of stabilization for standardization, being one of the conditions for precise measurement. This reduces measurement errors that can lead to inadequate evaluations using a modified Thomas test. Vigotsky et al. [
1] emphasize that when pelvic tilt is controlled, the modified Thomas test appears to be a valid test with which to assess the peak hip extension angle. In our experimental study, the flexed position of the lower leg at the hip was standardized at 120°, which ensured a flat back without lordosis, but also without kyphosis, which occurs above 120° of flexion, and the position was ensured by a specially created adjustable construction that simultaneously enabled stabilization and relaxation of the untested leg, as well as stabilizing the pelvis, trunk, and arms.
Our results regarding knee flexion range of motion prior to the intervention (a mean of 58.35° with a standard deviation of 11.31°) align with those of four studies whose evaluation via the modified Thomas test showed mean values greater than 50° for the knee flexion angle (53.91° ± 12.36° [
9]; 52.5° ± 7.56° [
13]; 53.5° ± 11° [
17]; 56.7° ± 11.2° [
23]; and 50° ± 12° [
29]). In contrast to the hip extension values, our knee range of motion results, as well as all the average peak angles reported by other researchers, are quite reduced compared to those found in relevant research such as that of Magee [
15], who specified 90° as normal for this test, or Peterson-Kendall et al. [
16], who described an angle of 80°.
The results were processed in a two-dimensional form with the goniometer of the Kinovea computer program. The application of the modified Thomas test via Kinovea has already been investigated by Neves et al. [
28], who analyzed recorded images to obtain hip extension ranges of motion measurements. The shortcoming of this research is that the authors used the principle of self-stabilization of the unexamined leg, with full hip flexion, which made it impossible to ensure the complete exclusion of the influence of non-tested segments, e.g., their muscle co-contactions, on the results.
In addition to the use of Kinovea motion analysis software, which is considered a reliable tool for performing angular measurements [
30], the advantage of our research is that it was conducted through three measurement points. This allows it to contribute to filling a gap in the existing research, which includes cross-sectional studies. We believe that we have contributed to the more objective application of this frequently used clinical test by equipping the test table with a special adjustable construction to ensure the relaxation of the non-tested leg, improving the stabilization. This method, to the best of our knowledge, was only used by Wakefield et al. [
8], but in a much more robust way using the plyo boxes.
Our research also has certain limitations. The examiner was not blinded, and the sample was convenient and consisted of young, healthy students, and so it does not represent a much more heterogeneous population. The measuring instrument was not an automated optoelectronic system, but an open-source video recording, measurement, and annotation tool designed for motion analysis, where the arms and center of the goniometer were placed on the markers by the researcher.
Another obvious limitation is the small sample size, as the cohort consisted of only 14 participants. It would, of course, always be preferable to have a larger sample size, which was unfortunately not feasible in this instance; as the research was conducted within the framework of a much larger project, and due to time constraints and organizational limitations, this was the only sample we were able to obtain at this point. This small sample by itself does not necessarily mean that the study is statistically underpowered; our results show a clear and significant improvement in flexibility when measured immediately after the intervention, which is consistent with the literature. Therefore, it would seem that the statistical power of the study was sufficient to at least detect this expected and well-established effect. Failure to obtain significant prolonged effects should not, therefore, be automatically dismissed as simply a result of low power. However, the presence of either statistical significance or non-significance in a study with a sample as small as this one can depend on a multitude of factors, such as higher potential levels of error variance in the measurement, and even perhaps possible the presence of a systematic error of some kind. Both of these have a larger impact on the final results when the sample size is smaller. Therefore, our results should be interpreted with caution, keeping in mind the sample size. Future researchers interested in this topic could improve upon this study design by having results drawn from a larger, and therefore more robust, sample of participants. This would help clear up possible doubts about the results.
As another future research recommendation, but also as a practical implication of our paper, we emphasize the imperative of quantifying the range of motion instead of the still quite common dichotomous assessment (i.e., positive or negative) of the modified Thomas test.



{kind=link}
{kind=link}
{kind=link}